upper gastro-intestinal hemorrhage
TRANSCRIPT

UPPER GI HEMORRAGE
Presenter: Dr. Thaha Rashid P TModerator: Dr. Gyan Singh
Introduction
• Acute gastrointestinal (GI) hemorrhage is a significant cause of morbidity and mortality in the emergency setting.• The source of GI bleeding can range from the esophagus through to
the colon and is classified into upper or lower GI bleeding depending on the site of bleeding relative to the ligament of Treitz.• Hemorrhage persisting or recurring after negative endoscopy is
termed obscure bleeding• Occult bleeding is when there are no signs of overt bleeding, but the
presenting symptoms are due to chronic blood loss and anemia• Mortality from upper GI bleeding is 5–14%

Approach to the patient

Initial assessment and resuscitation
• Initial evaluation should focus on rapid assessment of the magnitude haemorrhage• Less than 20% - Postural changes in BP & pulse• 20–30% - Tachycardia (>100 beats/min) and a reduced pulse pressure• Greater than 40% - impairment of conscious level (obtundation
/agitation), cool, clammy peripheries, & systolic BP less than 90 mm Hg• Fluid resuscitation in unstable patients should be commenced with a
2-L bolus of crystalloid
• Success of fluid resuscitation should be monitored using parameters such as heart rate, blood pressure, and urine output• Supplemental oxygen will maximize oxygen delivery to tissues• Blood test – CBC, LFT, KFT, Coagulation profile, Grouping and cross
matching• Blood transfusion• Decreased response to fluid resuscitation• Presence ongoing bleeding• Cardiopulmonary comorbidities• Old age- hematocrit below 30%• Young age- hematocrit below 20%• Suspected likelihood of rebleeding - esophageal varices
• Packed red cells are the optimal form of transfusion

History and examination
• Time of onset, volume, and frequency of bleeding are key aspects of the history in determining amount of blood loss• Hematemesis may be bright red when fresh, but older blood will
resemble coffee grounds• Melena is passage of offensive, black, tarry stool (60 ml of UGI
bleeding)• Hematochezia usually results from bleeding from the left side of the
colon• Syncope, angina - end-organ symptoms suggestive of reduced oxygen
delivery

• Antecedent vomiting - Mallory-Weiss tear• Recent weight loss or loss of appetite – malignancy• Recent epigastric pain - peptic ulceration• Alcohol intake or liver disease - variceal bleeding• Previous aortic surgery - Aortoenteric fistula• Drug history – NSAIDs, SSRIs - peptic ulceration• Use of anticoagulants• Physical examination
• Nasopharynx and oropharynx• Pigmented lesions in the oral mucosa - Peutz-Jeghers disease• Tender epigastrium - Peptic ulceration• Lymphadenopathy – malignancy• Splenomegaly, ascites, jaundice, palmar erythema – Variceal• Rectal examination – Melena, rectal cancer, hemorrhoids

Identification of source of bleeding
• Nasogastric Aspiration• Confrm upper GI bleeding• Assesses the rate of bleeding• Removal of blood from the stomach – Better visualisation in Endoscopy
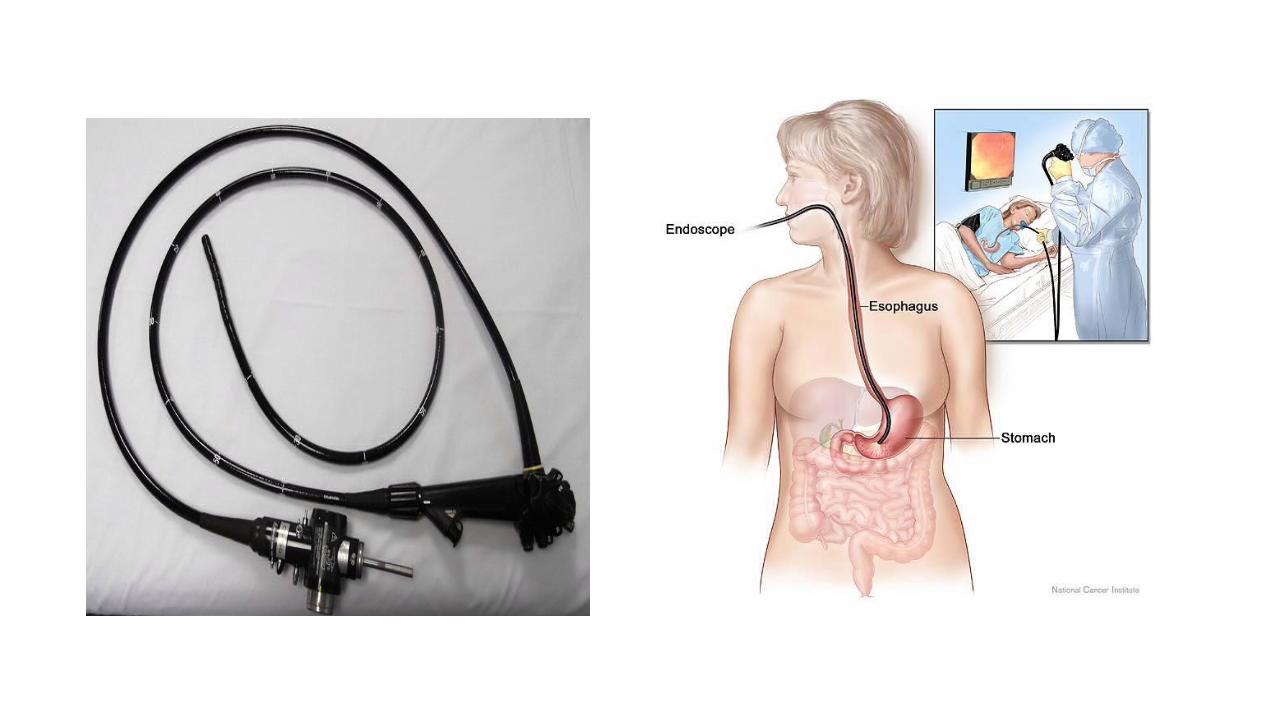
• EGD• Gold standard investigation for UGI bleeding• Should be performed within 24 hours of presentation• Identification of the source of bleeding• Determine the underlying etiology• Achieving hemostasis• Provides prognostic information
• Colonoscopy or Flexible sigmoidoscopy

• Capsule Enteroscopy• Endoscopic access to the small bowel is difficult• Capsules measure 11 ×26 mm• Contain a lens• White LED for illumination• Silver oxide batteries• Radio transmitter
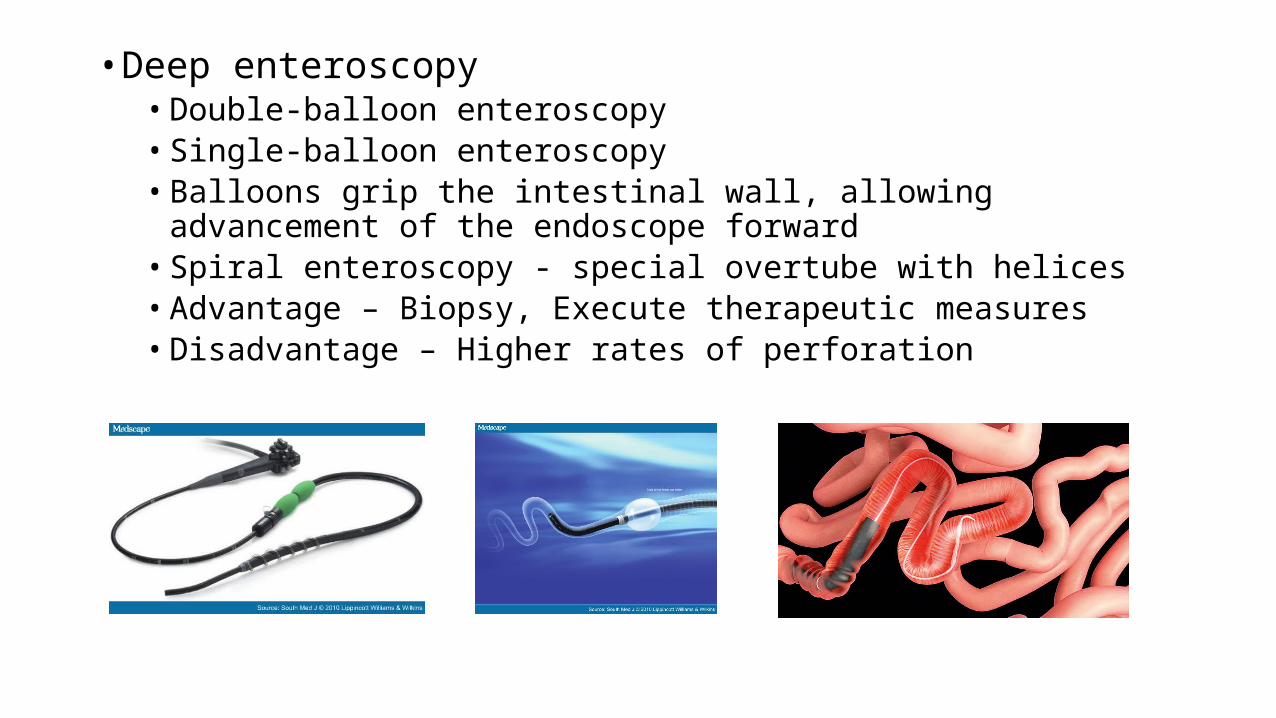
• Deep enteroscopy• Double-balloon enteroscopy• Single-balloon enteroscopy• Balloons grip the intestinal wall, allowing advancement of the endoscope
forward• Spiral enteroscopy - special overtube with helices• Advantage – Biopsy, Execute therapeutic measures• Disadvantage – Higher rates of perforation
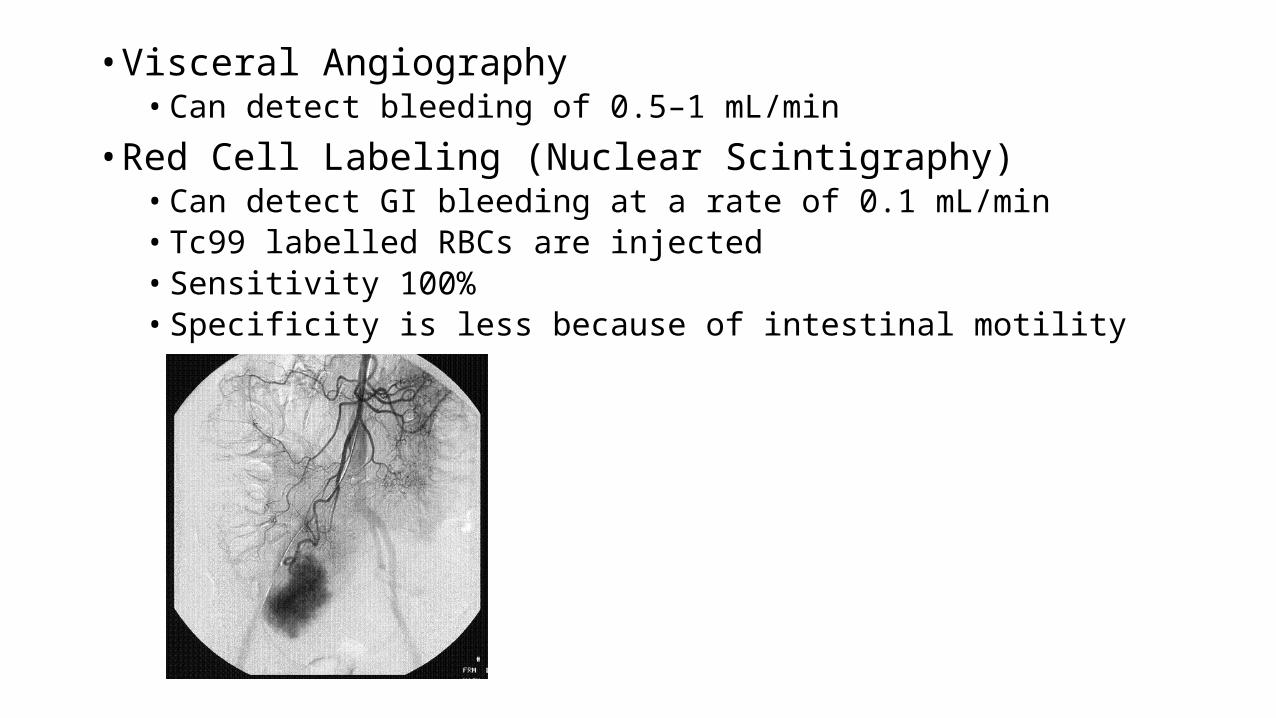
• Visceral Angiography• Can detect bleeding of 0.5–1 mL/min
• Red Cell Labeling (Nuclear Scintigraphy)• Can detect GI bleeding at a rate of 0.1 mL/min• Tc99 labelled RBCs are injected• Sensitivity 100%• Specificity is less because of intestinal motility


THERAPEUTIC OPTIONS
• Pharmacologic• Preventing recurrence of bleeding• Proton pump inhibitors• H.pylori eradication• Hemostatics
• Endoscopic• Thermal coagulation• Injection therapy - Epinephrine• Mechanical devices - metallic clips and band ligation• Argon plasma coagulation – Non contact coagulation• Laser-mediated coagulation

• Interventional Angiography• Embolization of the bleeding vessel• Microcoils• Gelfoam (gelatin sponge)• Polyvinyl alcohol• May also be coupled with selective infusion of a vasoconstrictor such as
vasopressin
• Surgery• When all modalities of hemorrhage control have failed• Treatment of choice - Malignancy

Causes of Upper GI bleeding
• NONVARICEAL BLEEDING – 80%• Peptic ulcer disease 30%-50%• Mallory-Weiss tears 15%-20%• Gastritis or duodenitis 10%-15%• Esophagitis 5%-10%• Arteriovenous malformations 5%• Tumors 2%
• PORTAL HYPERTENSIVE BLEEDING – 20%• Gastroesophageal varices >90%• Hypertensive portal gastropathy <5%• Isolated gastric varices

Peptic Ulcer Disease
• Most frequent cause of upper GI hemorrhage• 40% of all cases• Bleeding is the principal cause for death in PUD• Bleeding develops as a consequence of peptic acid erosion of the
mucosal surface• Usually chronic blood loss• Significant bleeding results when there is involvement of an artery of
the submucosa, gastroduodenal artery or left gastric arteries

Management
• Medical Management • Stop any causes (Drugs)• Ulcerogenic medications : NSAIDs, Salicylates, SSRI• Non ulcerogenic alternatives : COX-2 inhibitors• Proton pump inhibitors – Control bleeding and reduce rebleeding• Anti H.pylori treatment – 2 antibiotics

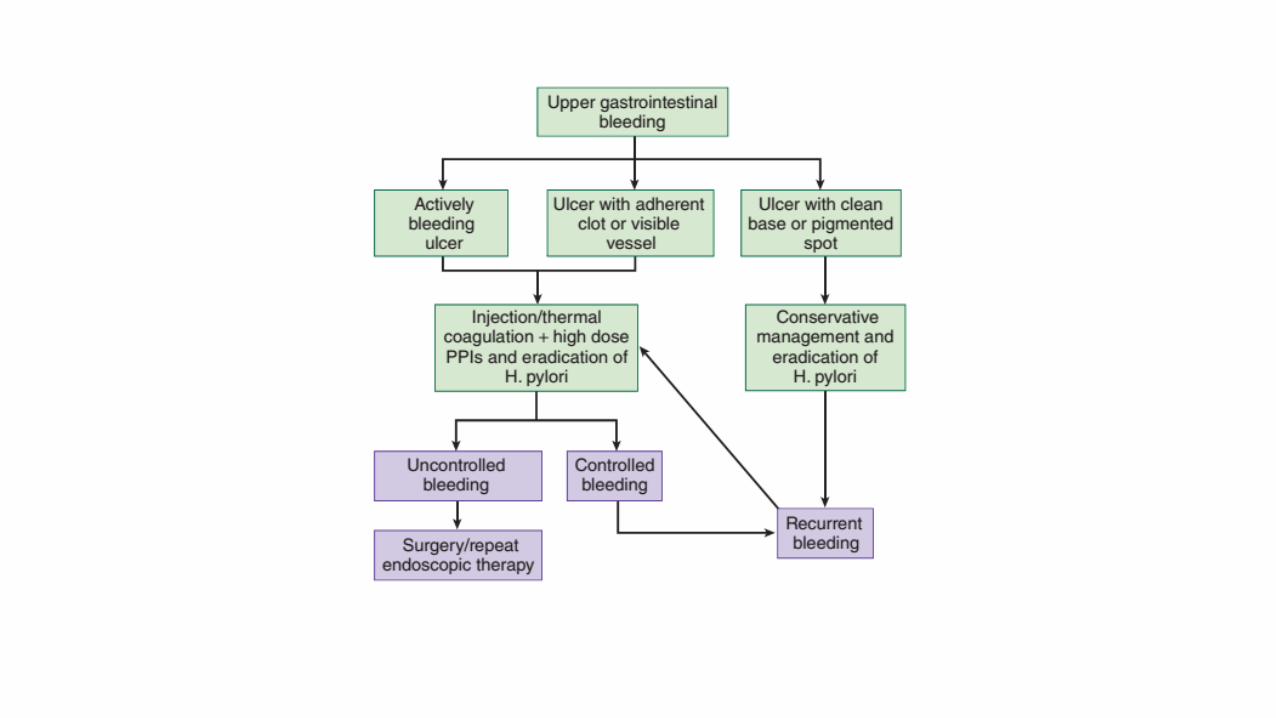
Endoscopic Management
• Endoscopy within 24 hours

• Endoscopic therapy is recommended in cases of active bleeding as well as those with a visible vessel (Forrest I to IIa)• In case of an adherent clot (Forrest IIb), the clot is removed and the
underlying lesion evaluated• Epinephrine injection (1 : 10,000) to all four quadrants of the lesion• Thermal therapy with heater probes, monopolar or bipolar
electrocoagulation, or laser or argon plasma coagulation• A combination of injection with thermal therapy achieves hemostasis
in 90% of bleeding PUDs• Hemoclips, which is difficult to apply is helpful with a spurting vessel

Surgical Management
• Indications for Surgery• Hemodynamic instability despite vigorous resuscitation (>6 U) transfusion• Failure of endoscopic techniques to arrest hemorrhage• Rebleed after initial stabilization (with up to two attempts at obtaining
endoscopic hemostasis)• Shock associated with recurrent hemorrhage• Continued slow bleeding with a transfusion requirement >3 U /day
• The first priority - Control of the haemorrhage• Definitive acid-reducing procedure
Surgery for duodenal ulcer
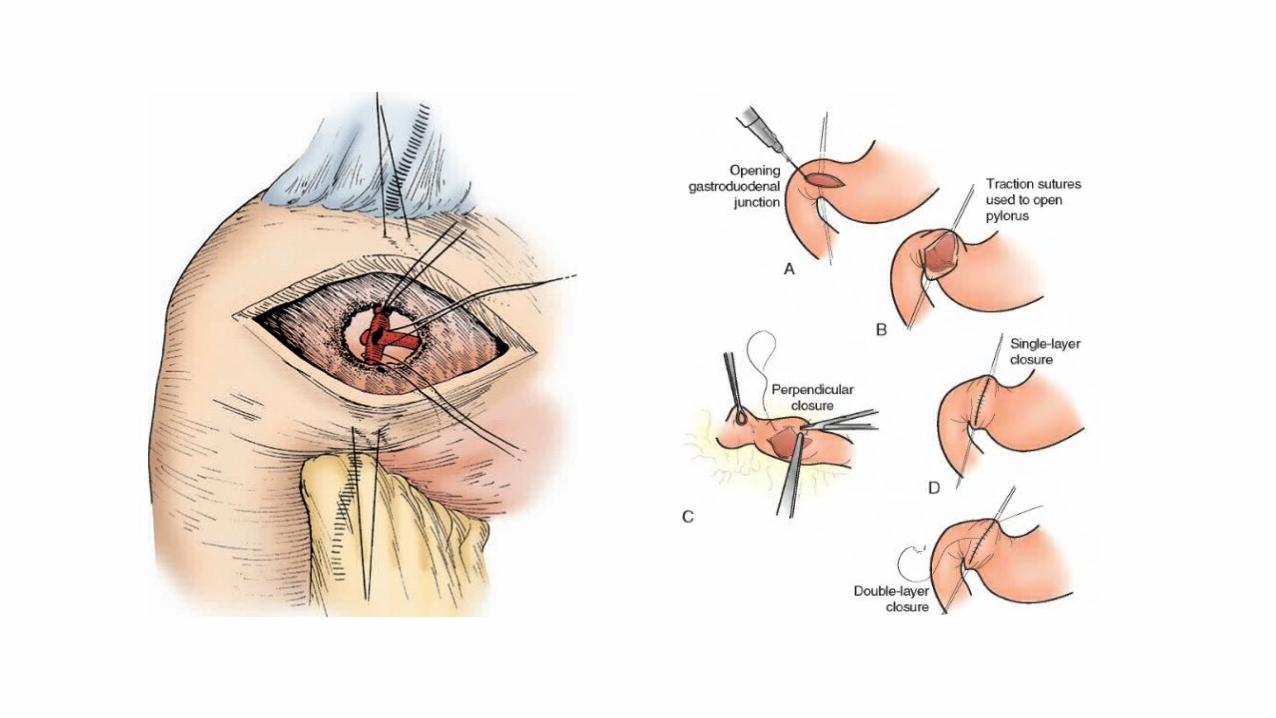
• Exposure of the bleeding site by longitudinal duodenotomy or duodenopyloromyotomy• Anterior ulcer- four-quadrant suture ligation with nonabsorbable
suture• Posterior ulcer eroding into the pancreaticoduodenal or
gastroduodenal artery- suture ligation of the vessel proximal and distal to the ulcer + U stich underneath the ulcer to control the pancreatic branches

Acid reducing operation
• Usefulness has been questioned because simple closure and H. pylori control is sufficient to prevent recurrence• Pyloroplasty, combined with truncal vagotomy, is the most frequently
used operation• Antrectomy with truncal vagotomy- In refractory duodenal ulcer
disease or who has failed conservative surgery

Surgery for gastric ulcer
• Gastrotomy and suture ligation• Because of a 10% incidence of malignancy, gastric ulcer resection is
generally indicated• Simple excision alone is associated with rebleeding in as many as 20%
of patients so distal gastrectomy is generally preferred• Ulcers of the proximal stomach-• near-total gastrectomy• distal gastrectomy combined with resection of a tongue of proximal stomach
to include the ulcer
Mallory-Weiss Tears
• 15% to 20% of cases• Mucosal and submucosal tears that occur near the gastroesophageal
junction• Usually develop in alcoholic patients after a period of intense retching
and vomiting following binge drinking• Occur in any patient who has a history of repeated emesis• Forceful contraction of the abdominal wall against an unrelaxed
cardia, resulting in mucosal laceration of the cardia as a result of the increase intragastric pressure

• Usually diagnosed based on history• Endoscopy is frequently used to confirm the diagnosis• Retroflexion maneuver• Most tears occur along the lesser curvature• Supportive therapy- 90% of bleeding episodes are self limited and the
mucosa often heals within 72 hours• Severe ongoing bleeding• Endoscopic therapy with injection or electrocoagulation• Angiographic embolization with gelatin sponge• high gastrotomy and suturing of the mucosal tear

Stress Gastritis
• Commonly encountered lesion in critically ill patients• Multiple superficial erosions of the entire stomach• Combination of acid and pepsin injury in the context of ischemia from
hypoperfusion states• Head injury -Cushing’s ulcers• Burns -Curling’s ulcers• Significant hemorrhage from stress ulceration is a common
phenomenon
• Patients with these risk factors should be given prophylactic therapy with antacids, histamine-2 (H2) receptor antagonists, PPIs, or sucralfate• Management of shock and sepsis• Acid suppressive therapy• Endoscopic therapy- Doubtful benefit• Selective infusion of vasopressin into the splanchnic circulation
through the left gastric artery• Angiographic embolization of left gastric artery• Surgery- Oversewing with figure-of eight stitches, Total gastrectomy in
life threatening refractory cases

Esophagitis
• Esophageal inflammation secondary to GERD• Crohn’s disease, radiation• Various infectious agents may also cause esophagitis, particularly in
the immunocompromised• Acid suppressive therapy• Endoscopic control of the hemorrhage, usually with
electrocoagulation or a heater probe• Infectious cause- targeted therapy


Dieulafoy’s Lesion
• Vascular malformations found primarily along the lesser curve of the stomach within 6 cm of the gastroesophageal junction• Unusually large vessels (1 to 3 mm) in the gastric submucosa• Erosion of the gastric mucosa overlying these vessels leads to
haemorrhage• Dieulafoy’s lesions appear as reddish-brown protrusions on
endoscopy with no ulceration• The mucosal defect is usually small (2 to 5 mm) and may be difficult to
identify

• Endoscopic control- Application of thermal or sclerosant therapy• Angiographic coil embolization• Surgical intervention• Gastrostomy with oversewing of the lesion• Partial gastrectomy- if bleeding point is not identified
• Surgical intervention may require prior endoscopic tattooing
Gastric Antral Vascular Ectasia
• Collection of dilated venules appearing as linear red streaks converging on the antrum in a longitudinal fashion• Watermelon stomach• Acute severe hemorrhage is rare• Patients present with persistent iron deficiency anemia from
continued occult blood loss• Endoscopic therapy- APC• Antrectomy


Malignancy
• Chronic anemia or hemoccult-positive stool rather than episodes of significant hemorrhage• Malignancies that present as ulcerative lesions will bleed persistently• Endoscopic therapy is often successful in controlling these bleeds• As rebleeding rate is high, surgical resection is indicated• Extent of resection is dependent on the specific lesion• Palliative resections for control of bleeding usually entail wedge
resections
Aortoenteric Fistula
• Previous abdominal aortic aneurysm repair• May occur as a result of an inflammatory or infectious aortitis• Development of a pseudoaneurysm at the proximal anastomotic
suture line in the setting of an infection, with subsequent fistulization into the overlying duodenum• Hemorrhage is often massive and fatal• Typically, patients with bleeding from an aortoenteric fistula will
present first with a sentinel bleed, a self-limited episode that heralds the subsequent massive, and often fatal, hemorrhage
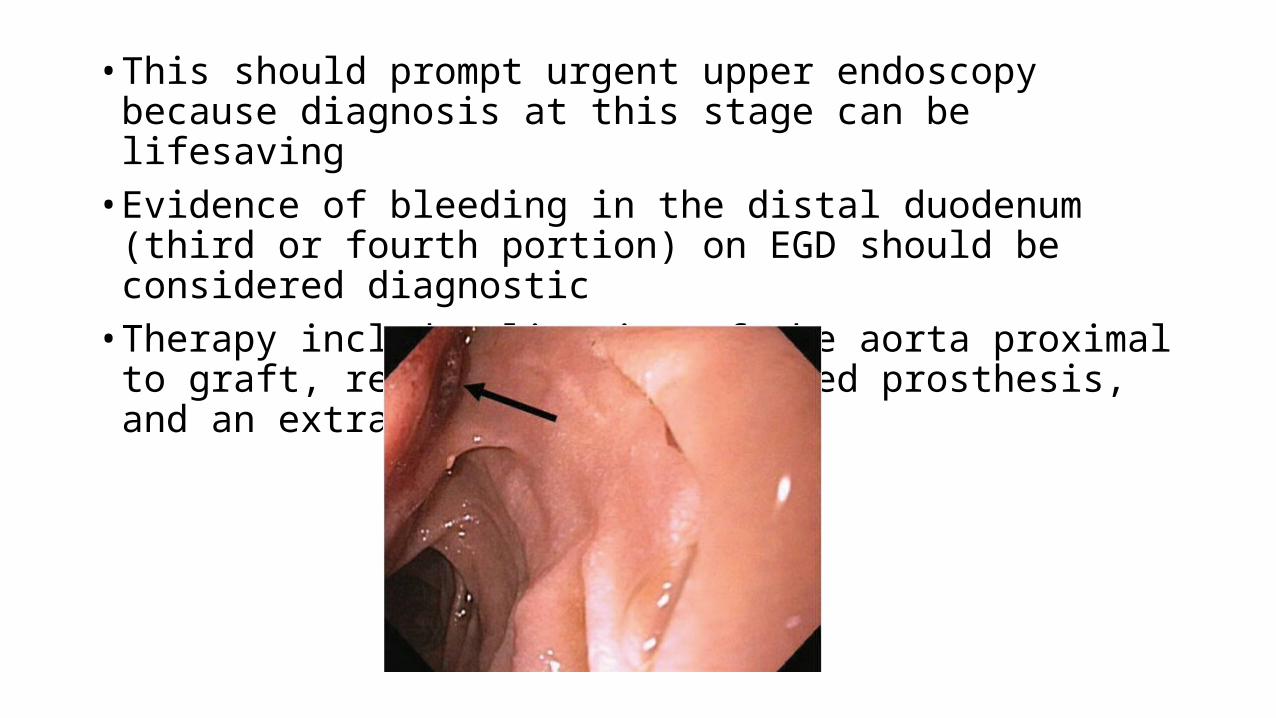
• This should prompt urgent upper endoscopy because diagnosis at this stage can be lifesaving• Evidence of bleeding in the distal duodenum (third or fourth portion)
on EGD should be considered diagnostic• Therapy includes ligation of the aorta proximal to graft, removal of
the infected prosthesis, and an extra-anatomic bypass.

Hemobilia
• Associated with trauma, recent instrumentation of the biliary tree, or hepatic neoplasms.• Should be suspected in anyone who presents with hemorrhage, right
upper quadrant pain, and jaundice• Endoscopy- blood at the ampulla• Angiography- diagnostic procedure of choice• Angiographic embolization is the preferred treatment

Hemosuccus Pancreaticus
• Erosion of a pancreatic pseudocyst into the splenic artery• Bleeding from the pancreatic duct• Diagnosis requires a high index of suspicion in patients with
abdominal pain, blood loss, and a past history of pancreatitis• Angiography is diagnostic and permits embolization, which is often
therapeutic• Distal pancreatectomy, often results in cure

Bleeding Related to Portal Hypertension
• Usually the result of bleeding from varices• Dilated submucosal veins develop in response to the portal
hypertension, providing a collateral pathway for decompression of the portal system into the systemic circulation• They are most common in the distal esophagus and can reach sizes of
1 to 2 cm• Overlying mucosa becomes increasingly tenuous, excoriating with
minimal trauma

• May also develop in the stomach and hemorrhoidal plexus of the rectum• Gastroesophageal varices develop in approximately 30% of patients
with cirrhosis and portal hypertension• Compared with nonvariceal bleeding, variceal hemorrhage is
associated with an increased risk of rebleeding & mortality• Hemorrhage is frequently massive, accompanied by hematemesis and
hemodynamic instability

Medical Management
• Vasopressin produces splanchnic vasoconstriction and has been shown to reduce bleeding significantly• Octreotide, is the vasoactive agent of choice• Continuous IV infusion of these agents results in temporary control of
bleeding and allows time for resuscitation and appropriate diagnostic and therapeutic maneuvers.
Endoscopic Management
• Early EGD is critical to evaluate the source of bleeding because more than 50% of bleeding is caused by nonvariceal sources• If bleeding esophageal varices are identified, sclerotherapy and
variceal banding have been shown to control hemorrhage effectively• Sclerotherapy-perforation, mediastinitis, and stricture• Banding- Need for expertise

Other Management
• Balloon tamponade• Sengstaken-Blakemore tube consists of a gastric tube with esophageal
and gastric balloons• Inflation of the balloons compresses the esophagogastric venous
plexus, arresting bleeding• Deflation can be associated with recurrent bleeding in 50% of patients• Hence this technique is reserved as a temporizing measure


Prevention of Rebleeding
• Approximately 70% of patients will have a rebleed within 2 months without further definitive therapy• Medical therapy• Non-selective beta blocker, such as nadolol• Antiulcer agent, such as a PPI or sucralfate
• Endoscopic band ligation repeated every 10 to 14 days until all varices have been eradicated

Radiologic or Surgical Portal Decompression
• In 10% of cases of when endoscopic management is unsuccessful• TIPS• Artifcial anastomosis between the hepatic and portal veins• Under fluoroscopic guidance, using a covered stent• Control bleeding in 95% of cases• Disadvantage- hepatic encephalopathy from diversion of blood away from the
liver parenchyma
• Surgical shunting- More morbidity and mortality than TIPS


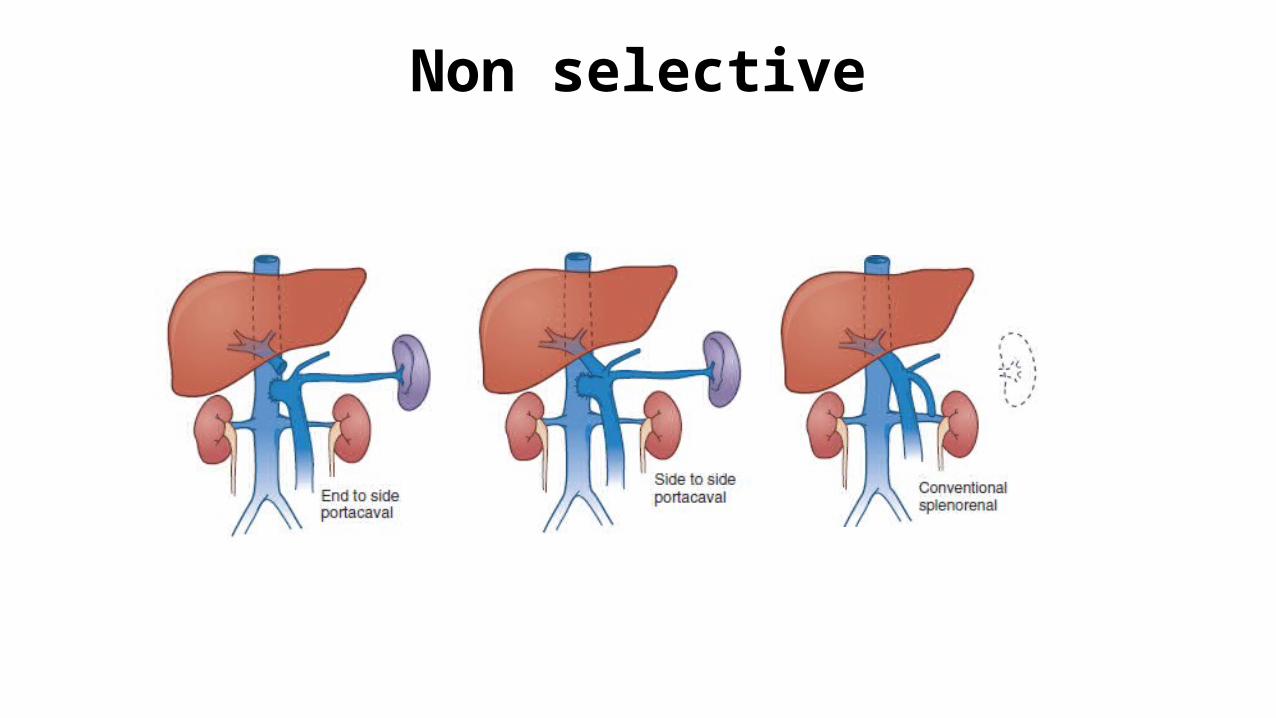
Shunt surgery
• Non selective• End to side portacaval• Side to side portacaval• Conventional splenorenal
• Selective• Left gastric vena caval shunt• Distal splenorenal shunt
• Partial Shunts• Portacaval shunt using small diameter PTFE graft (10mm)
Non selective

Distal spleno renal shunt
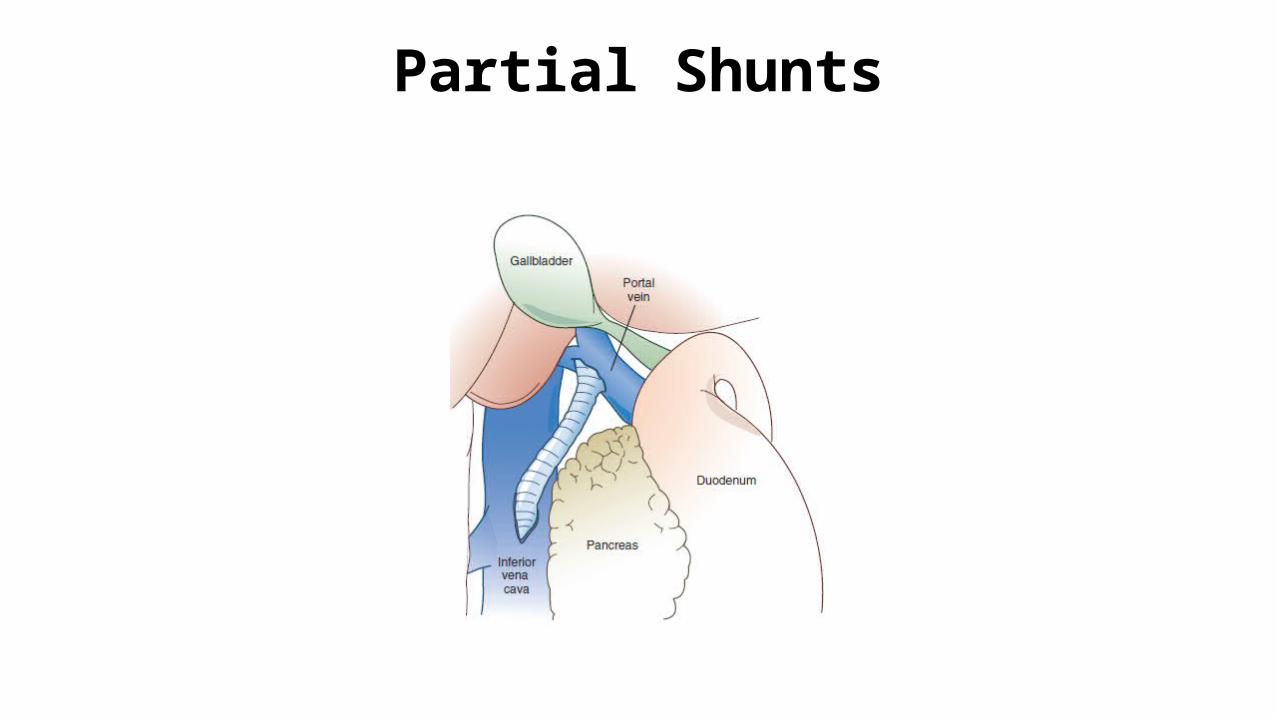
Partial Shunts

• Gastric varices are managed much the same way as esophageal varices• Isolated gastric varices – Splenic vein thrombosis – Splenectomy• Portal hypertensive gastropathy• Diffuse dilation of the mucosal, and submucosal venous plexus• Snake-skin appearance with cherry-red spots
Thank you