upper limb amputation rehabilitation
TRANSCRIPT
Upper limb amputees
MBBS(Mal),AM(Mal),FRCS(Ed),FRCS(Glasg),FICS(USA),MBA(USA), Dip Hand Surgery(Eur),Dip MedEd(Dundee),
FHEA(UK), FFSTEd, FAcadMEd(UK)
Senior Consultant Hand Surgeon, KTPH Alexandra Health,Honorary Senior Lecturer, YYL School of Medicine, National
University of Singapore,Core Faculty for Orthopaedic Surgery and Hand
and Reconstructive Micro Surgery, NHG Residency Program , SINGAPORE
Dr Vaikunthan Rajaratnam

The issues and challenges
• 2 million people living with limb loss in the United States
• main causes are vascular disease (54%) – including diabetes and peripheral arterial disease –
• trauma (45%) and • cancer (less than 2%) 185,000 amputations/yearhospital costs associated with amputation totaled more than $8.3 billionhalf of the individuals who have an amputation due to vascular disease will die within 5 years

• Trauma accounted for 54 per cent of these of which mechanical trauma was most common. Neoplasia accounted for 14 per cent of referrals. There has been an increase in the number of referrals following upper limb amputation due to a primary malignancy from 7 per cent in 2002/03 to 13 per cent in 2003/04. Dysvascularity as a cause of upper limb amputation was recorded in 8 per cent of referrals.Trauma was the most common cause within the 16 – 54 age group, but in the older age groups more referrals are made due to neoplasia.T
reasons for an upper extremity amputation• Trauma• Correction of a congenital deformity• Tumor• medical disease
Based on the Academy Upper Limb Society enrollment in summer 2005, approximately
66 individuals in the United States pursue upper limb prosthetics as a specialty
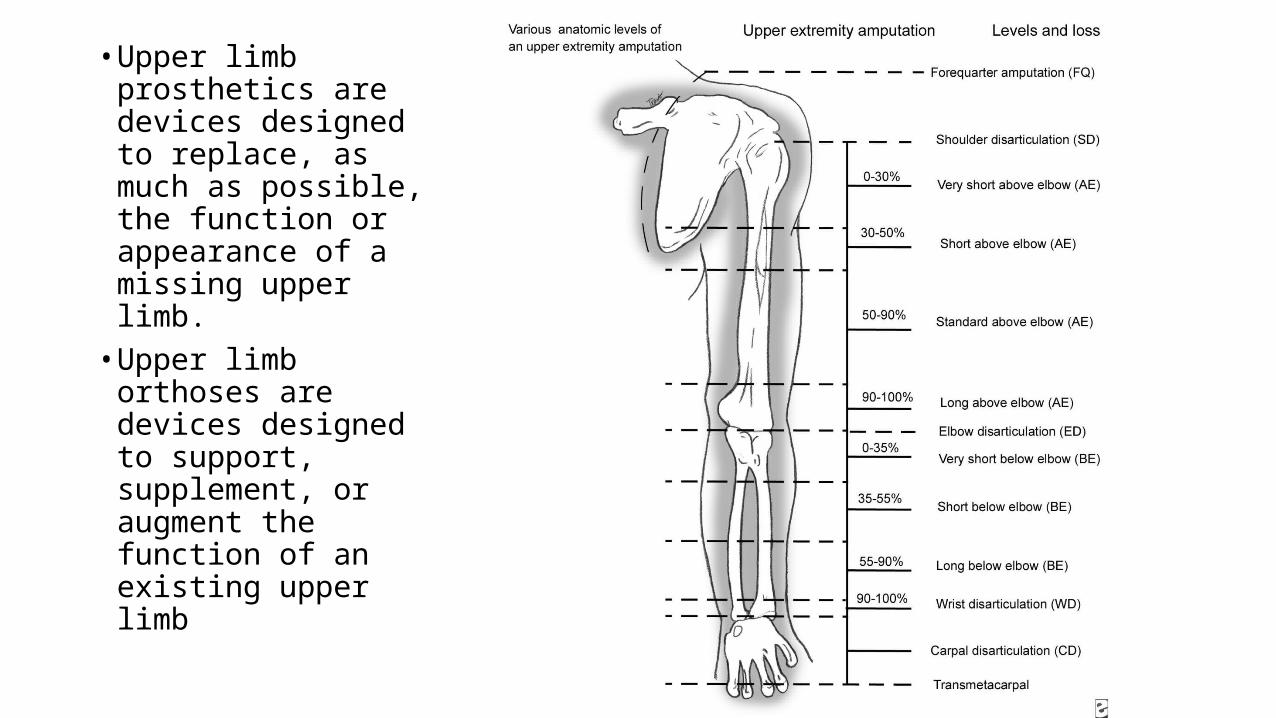
• Upper limb prosthetics are devices designed to replace, as much as possible, the function or appearance of a missing upper limb.
• Upper limb orthoses are devices designed to support, supplement, or augment the function of an existing upper limb

Amputation levels• Transphalangeal amputation: Resection of the thumb or fingers at distal interphalangeal (DIP),
proximal interphalangeal (PIP), or metacarpophalangeal (MCP) levels, or at any level in between• Transmetacarpal amputation: Resection through the metacarpals• Transcarpal amputation: Resection through the carpal bones; transmetacarpal and transcarpal
amputations are less advised because, except for select circumstances, they provide for decreased functional outcomes
• Wrist disarticulation: Transection between the carpals and radius/ulna• Transradial amputation: Below-elbow amputation (may be classified as long, medium, or short)• Elbow disarticulation: Transection through the elbow joint• Transhumeral amputation - Above-elbow (Standard length is 50-90% of humeral length.)• Shoulder disarticulation: Transection through the shoulder joint• Interscapulothoracic disarticulation (forequarter): Amputation removing the entire shoulder girdle
(scapula and all or part of the clavicle) (some surgeons choose to leave part of the medial clavicle)

relevant terminology• Residual limb: The preferred term for the remaining portion of the amputated limb• Relief: A concavity within the socket that is designed for areas that are sensitive to
high pressure (bony prominences)• Buildup: A convexity that is designed for areas that are tolerant to high pressure
(such as a bulge)• Terminal device: The most distal part of a prosthesis that substitutes for the hand;
it may be a prosthetic hand, a hook, or another device.• Myodesis: Direct suturing of residual muscle or tendon to bone/periosteum• Myoplasty: Suturing of agonist-antagonist muscles pairs to each other• Prehensile: Grasp

Upper limb transplantation• Issues• Challenges
Ethics
Immunology
Risk
considerations when choosing a prosthesis
• Amputation level• Contour of the residual limb• Expected function of the prosthesis• Cognitive function of the patient• Vocation of the patient (eg, desk job vs manual
labor)• Avocational interests of the patient (ie, hobbies)• Cosmetic importance of the prosthesis• Financial resources of the patient






43 year-old female, right-handed, cook
Traumatic amputation of right thumb and index finger
Underwent emergency debridement on day of injury

Unreplantable thumb

Underwent right thumb reconstruction with right big toe osteoplastic wrap-around flap 1 week post-injury, after counseling and consenting

Toe wrap based on dorsalis pedis

10 months post op: flap debulking and scar revision


timeline for an amputation/prosthesis fitting
• Preamputation• Surgical procedure• Acute postsurgery• Prosthesis fitting and
testing• Preparatory vs definitive
prosthesis
Characteristics of a successful prosthesis• comfortable to wear• easy to put on and remove• light weight, • durable, and • cosmetically pleasing• function well mechanically and • require only reasonable maintenance• motivation of the individual

Principlesbest type of surgical technique for an upper limb–deficient individualis a myodesis approach, in which the surgeon sutures the residual muscles to the bone rather than to one another

Complications
• postoperative pain• Phantom sensation• telescoping

Challenges• upper limb amputations result from a traumatic event - no
preoperative stage• difficult to disguise the loss of an upper limb• extremely high expectations• seeking counseling
Passive prosthesesvariable rejection rates 6% (Kejlaa 1993) to 100% (van Lunteren et al. 1983)Recent evidence suggests that cosmetic prostheses tend to have a higher rate of permanent use both in adult and pediatric populations (Dudkiewicz et al. 2004; Crandall and Tomhave 2002)
life-like silicone glovinghigher prevalence of passive devices in UK /Swedenmyoelectric/body-powered more in West Germany /United Stateselicit the fewest user concerns wear temperature glove problems, excessive weight, wear on clothes, and strap irritation osseointegration may in the future alleviate many areas of user dissatisfaction related todiscomfort with sockets and sleeves,
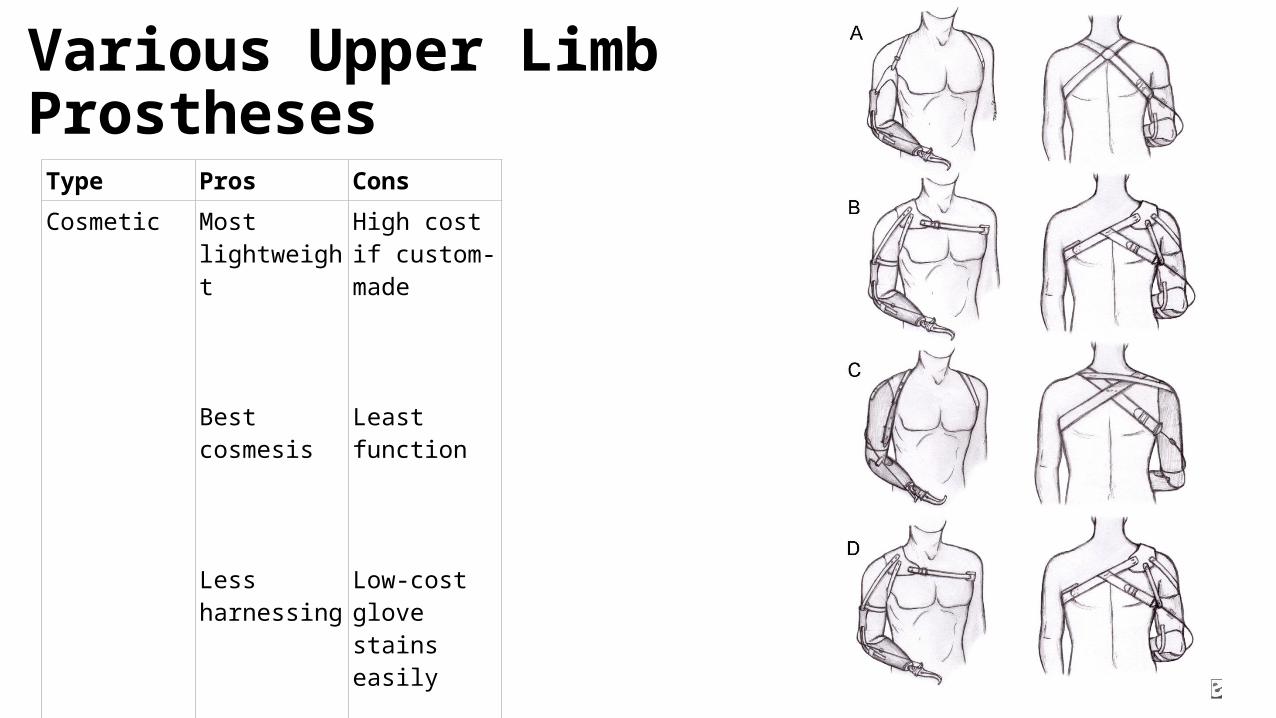
Various Upper Limb Prostheses
Type Pros ConsCosmetic Most
lightweight
Best cosmesis
Less harnessing
High cost if custom-made
Least function
Low-cost glove stains easily
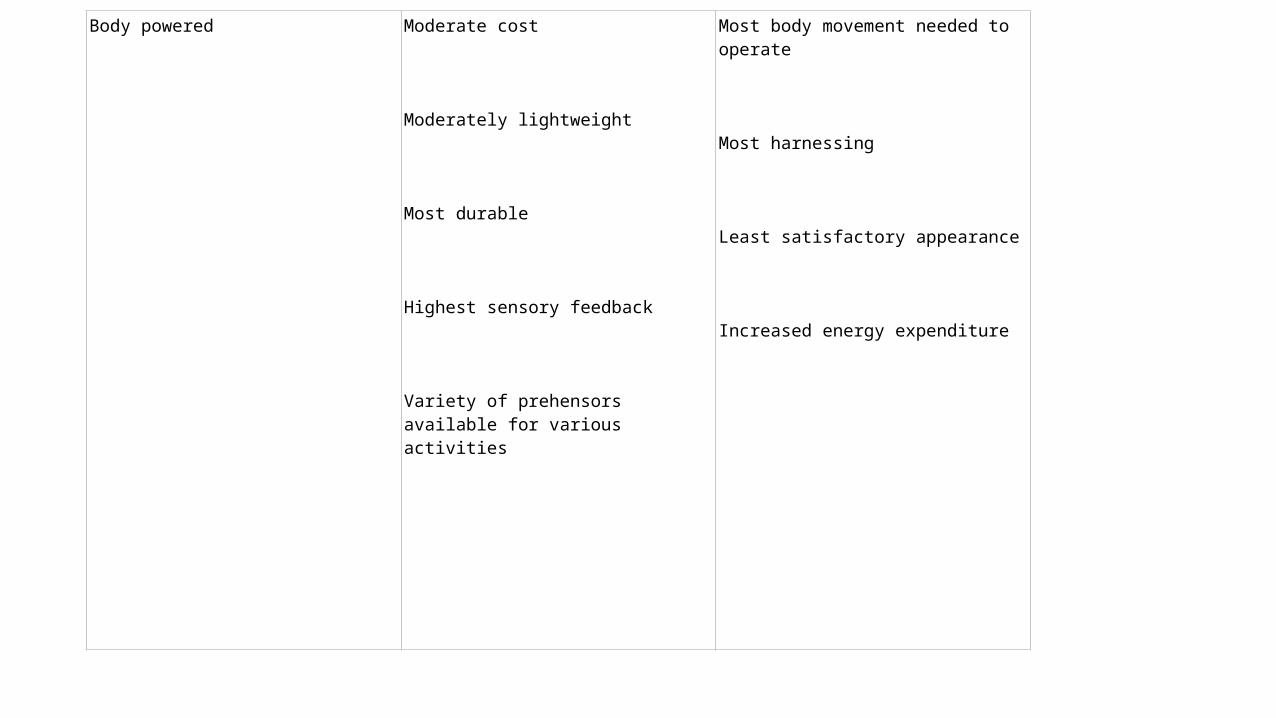
Body powered Moderate cost
Moderately lightweight
Most durable
Highest sensory feedback
Variety of prehensors available for various activities
Most body movement needed to operate
Most harnessing
Least satisfactory appearance
Increased energy expenditure

Battery powered (myoelectric and/or switch controlled)
Moderate or no harnessing
Least body movement needed to operate
Moderate cosmesis
More function-proximal areas
Stronger grasp in some cases
Heaviest
Most expensive
Most maintenance
Limited sensory feedback
Extended therapy time for training

Hybrid (cable to elbow or TD and battery powered)
If excursion to elbow and battery-powered TD
If excursion to TD and battery-powered elbow
All-cable excursion to elbow or TD
All-cable excursion to elbow
Increased TD pinch
All-cable excursion to TD
Low effort to position TD
Low-maintenance TD
Battery-powered TD weights forearm (harder to lift but good for elbow disarticulation or long THA)
Lower pinch for TD and least cosmetic

Body-powered prosthesespopular choice in upper limb prostheticsOverall rejection rates 16% to 66% (Bhaskaranand et al. 2003, Kruger and Fishman 1993) Body-powered hands rejection rates as high as 80% (Millstein
et al. 1986) and 87% (Kejlaa 1993), complaints targeting • slowness in movement, • awkward use, • difficulty in cleaning and maintenance, • excessive weight, • insufficient grip strength and • high-energy expenditure needed to operate (Millstein et al.
1986; Kejlaa 1993). Body-powered hooks on the other hand are • functional value, • durability, • lower weight and • good visibility of objects being handled and, overall, • are more acceptable to users (Millstein et al. 1986)

Suspension Options
Harness Figure-8 Transradial
Transhumeral
Light to normal activities
Simple, durable, adjustable Axillary pressure produces discomfort
Shoulder saddle and chest strap Transradial
Transhumeral
Heavy lifting
Greater lifting ability, more comfortable than figure-8 harness
Reduced control compared with figure-8 harness; difficult to adjust in women, because straps cross breasts
Self-suspending Munster Northwestern Supracondylar
Wrist disarticulation
Elbow disarticulation
Short transradial Myoelectric transradial
Ease of use Limited lifting capacity compared with harness systems, compromised cosmesis, reduced elbow flexion
Suction Suction socket with air valve Transhumeral with good soft-tissue cover
Secure suspension, elimination of suspension straps
Requires stable residual volume, harder to put on than other suspension systems
Gel sleeve with locking pin Transradial
Transhumeral Compromised limbs with scarring or impaired skin integrity
Accommodate limb volume change with socks,
reduced skin shear
Greater cleaning and hygiene requirements,
can be uncomfortable in hot climates
Osteintegration
Issues body-driven prostheses
• excessive wear temperatures, • abrasion of clothes, • wire failure, • unattractive appearance, • harness discomfort and/or
breakage

Challenges -body-powered prostheses• provision of more durable cables, • more comfortable harnesses• improved gloving material, • increased wrist movement • improved control mechanisms requiring less visual attention and • Enabling coordination of multiple joints.
Electric prostheses advantagesPros
appearanceincreased pinch strength, ease of operation, and lack of harnesssensory feedback, overall function, and comfort,
Consincreased maintenanceglove and battery replacement, higher costhigher weight
The main reasons reported for primary non-wear were a perceived lack of need and discrepancies between the perceived need and the prostheses
The main reasons reported for secondary prosthesis rejection were dissatisfaction with prosthetic comfort, function and control.
Implications for Rehabilitation• Major upper-limb amputees (ULAs) are fitted with prostheses after the amputation.• This population-based study shows that proximal ULAs, elderly ULAs and women have an increased risk of prosthesis rejection.• Emphasising individual needs may facilitate successful prosthetic fitting.• Improved prosthesis quality and individualised prosthetic training may increase long-term prosthesis use.
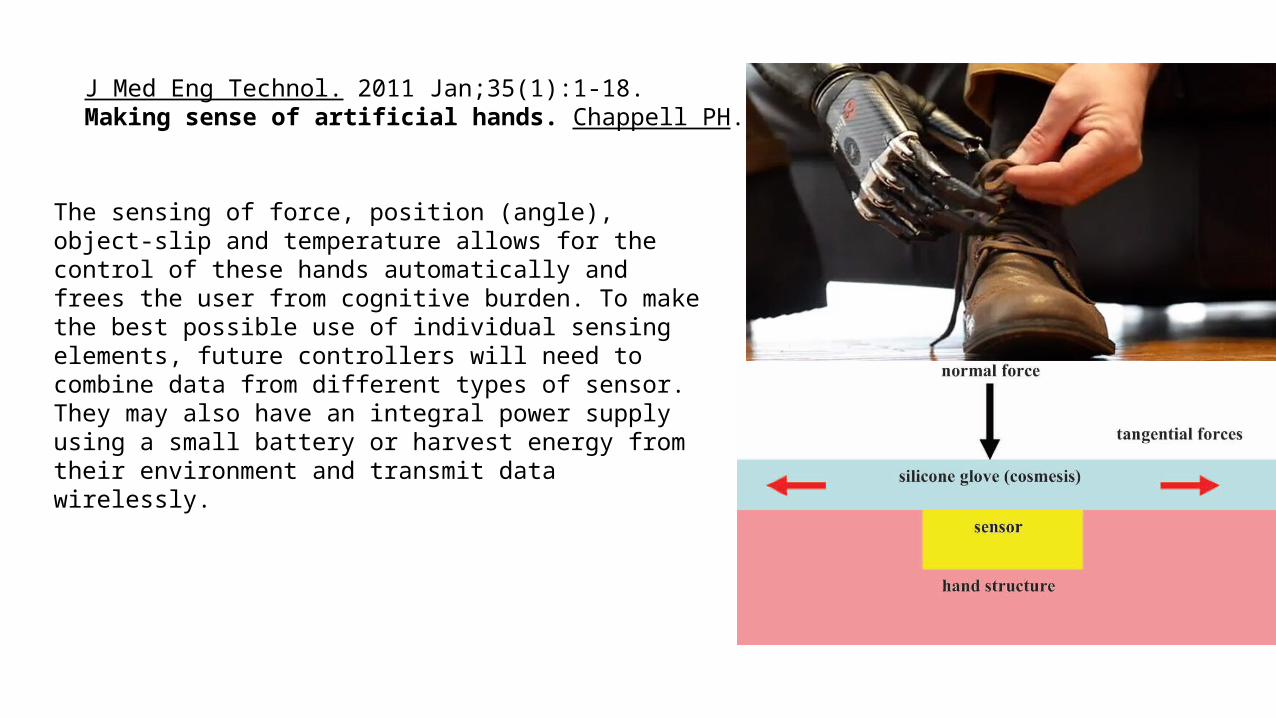
J Med Eng Technol. 2011 Jan;35(1):1-18. Making sense of artificial hands. Chappell PH.
The sensing of force, position (angle), object-slip and temperature allows for the control of these hands automatically and frees the user from cognitive burden. To make the best possible use of individual sensing elements, future controllers will need to combine data from different types of sensor. They may also have an integral power supply using a small battery or harvest energy from their environment and transmit data wirelessly.
sensing of force, position (angle), object-slip and temperature allows for the control of these hands automatically and frees the user from cognitive burden.
Journal of Medical Engineering & Technology
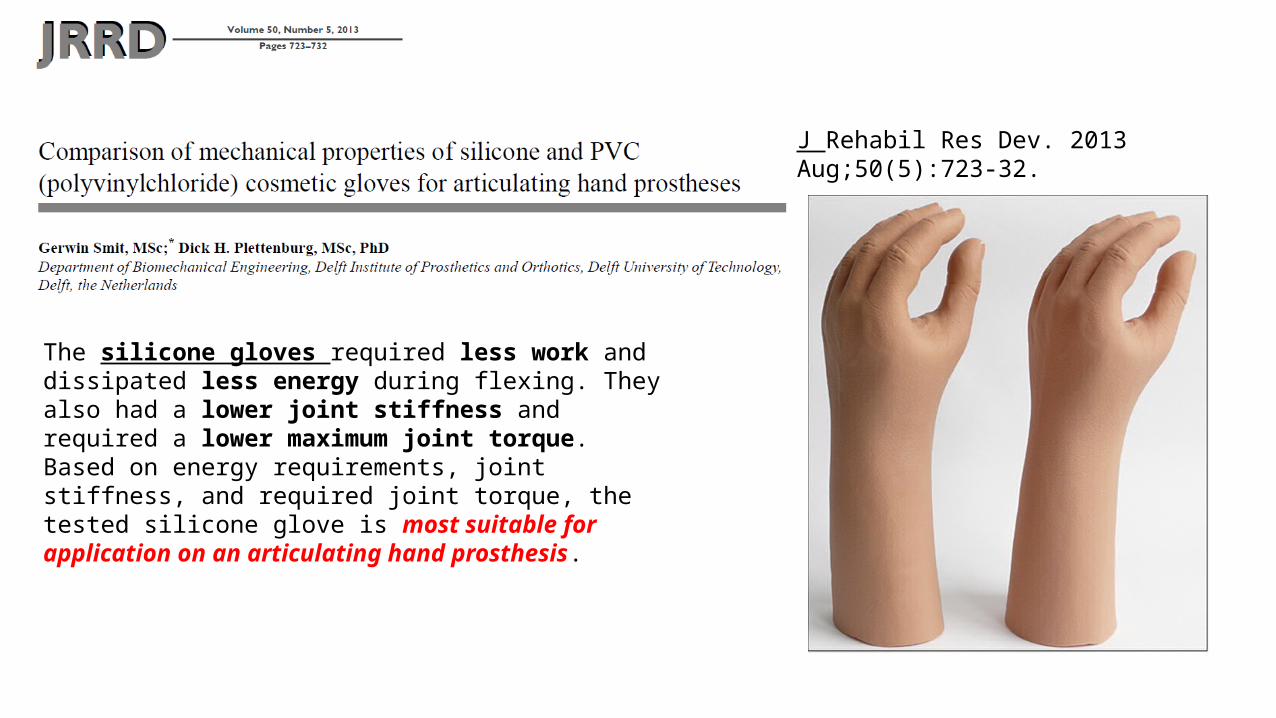
The silicone gloves required less work and dissipated less energy during flexing. They also had a lower joint stiffness and required a lower maximum joint torque. Based on energy requirements, joint stiffness, and required joint torque, the tested silicone glove is most suitable for application on an articulating hand prosthesis.
J Rehabil Res Dev. 2013 Aug;50(5):723-32.


• targeted muscle reinnervation, surgeons transfer nerves that previously carried signals to the amputated limb to muscles in the chest and upper arm.
• http://www.technologyreview.com/view/411996/patients-test-an-advanced-prosthetic-arm/

Brain. 1996 Apr;119 ( Pt 2):593-609.
Action recognition in the premotor cortex.Gallese V, Fadiga L, Fogassi L, Rizzolatti G.Istituto di Fisiologia Umana, Università di Parma, Italy.
• Visualization , mental practice, visuo-motor imagery• ventral pre-motor area are motor "command" neurons,
inferior frontal gyrus,making muscles do certain things; • any given mirror neuron will also fire when one observes
another performing the same action• Action words

Surgical skill acquisitionMirror neurons

Electromyogram pattern recognition for control of powered upper-limb prostheses: State of the art and challenges for clinical use. Erik Scheme, MSc, PEng; Kevin Englehart, PhD, PEng*
Institute of Biomedical Engineering, University of New Brunswick, Fredericton, Canada
JRRD Volume 48, Number 6, 2011 Pages 643–660Journal of Rehabilitation Research & Development
DEKA• The DEKA Arm is an advanced upper limb prosthesis, not yet available
for commercial use• three configurations: radial configuration, humeral configuration, and
shoulder configuration. • 6 preprogrammed grip patterns and four wrist movements.
Defense Advanced Research Project Agency to design a prosthetic arm system that would be a dramatic improvement compared with the existing state of the art

Psychology graduate student /Congenital below elbow left arm amputee
http://aannggeellll.tumblr.com/post/56878186543/testing-out-the-new-deka-luke-arm-videos-will


Thank you• www.handsurgeryedu.com• www.handtherapyedu.com• www.mbamedicine.com• http://www.linkedin.com/gro
ups/Hand-Surgery-International-3804094