upper quarter consists of - asht.org 2016_htrc... · wrist complex: base ... 1st cmc joint or basal...
TRANSCRIPT

Hand Therapy Review CourseCurtis National Hand Center
Baltimore, MD
October 7-9, 2016
Anatomy and Kinesiology of the Hand
Jane Fedorczyk, PT, PhD, CHT, ATC
Upper Quarter Consists of:
Cervical Spine & Thorax Provide Support for Upper Limb Function
Shoulder Complex: Hand Placement
Elbow Complex: Hand Placement
Wrist Complex: Base for Prehension
Hand: Prehension or Grasp
The Hand: Complex Motor Tasks,
Interaction/Perception with Environment Hand Osteology
• 19 bones distal to the carpus• 5 Metacarpals (I‐V)
• 3 Phalanges (II‐V)• 2 Phalanges (I)
Arthrology of the Hand
• Interphalangeal (IP) Joints
• Metacarpal Phalangeal (MCP) Joints
• Carpometacarpal (CMC) Joints
CMC Joints
• Saddle Joints (2 df)• Thumb & Digit V
• Flex/Ext (ll to palm)
• Abd/Add ( to palm)• Opposition net effect
• Plane Joints (1 df)• Digits II‐IV• Flexion/Extension

CMC Joints: function
• Saddle joints are responsible for positioning thumb and little finger for opposition or prehension.
• In the digits, CMC motion increases from radial to ulnar side of the hand; contributes to hollowing/cupping of palm to conform to objects.
• Less mobility of the II and III is thought to be a functional adaptation to enhance ECRL/ECRB and FCR muscle activity.
1st CMC Joint or Basal Joint or Trapeziometacarpal Joint
Thumb OsteokinematicsMotion of the CMC Joint of the Thumb: Extension, Flexion, Abduction
Composite FlexionHitchhiking
Grasping Wide Jar
Thumb Arthrokinematics

Extrinsic and Intrinsic Tendon Forces Cooney, et al. 1977
• Joint compression forces averaged 12 kg at the CMC joint during simple pinch with 1 kg of applied force
• Compression forces of as much as 120 kg may occur at the CMC joint during strong grasp
Palmar/Volar Ligament of the 1st CMC
MCP Joints
Condyloid Joints:
flexion/extension
abduction/adduction
Digits II‐V
• Motion increases radial to ulnar in digits
• 0/90‐110 degrees
• Hyperextension consistent across digits;
varies among individuals
MC P1
MCP Joints: Thumb
• MP joint motion varies widely amongst individuals
• Abduction, adduction, and long axis rotation function to provide additional range for opposition to enhance grasp and prehension.
• Axial rotation allows for pad to pad prehension.UCLTear
rotation

Ligaments of the MCP Joints
• Loose Joint Capsule
• Volar Plate
• Collateral Ligaments
• Proper• Accessory
MCP Joint: Collateral Ligaments
• Due to cam‐shaped metacarpal head, the collateral ligaments are:
• Taut in Flexion• Slack in Extension
• Collateral ligament length maintained @ 45‐70° flexion
IP Joints: Structure and Function
Amount of DIP
motion varies
Among
individuals;
60‐80°common
PIP and DIP joint have similar configuration
Supporting structures:joint capsule collateral ligamentsvolar plate
PIP most important jointfor hand function
Volar Plate
• Enhances joint stability
• With flexion, proximal portion buckles/folds like accordion
• Stability of volar plate enhanced by attachment of collateral ligaments

Volar Plate Structure
Critical Corner
Critical Corner
Disruption of the Critical Corner leads to dorsal dislocation (PIP Joint Instability)
Volar Plate
• Fixed flexion, redundant layers thicken; lead to contracture
• Flexor tendons may adhere to volar plate
• Hyperextension injury• Flexor tendon injury
Protected Position of the Hand
• MCPs 40‐70° Flexion
• Maintain Length of Collaterals
• IPs 0° Extension• Prevent Volar Plate Contracture
• Wrist 0°
• Avoid Increased CT Pressure
• Open 1st Web Space
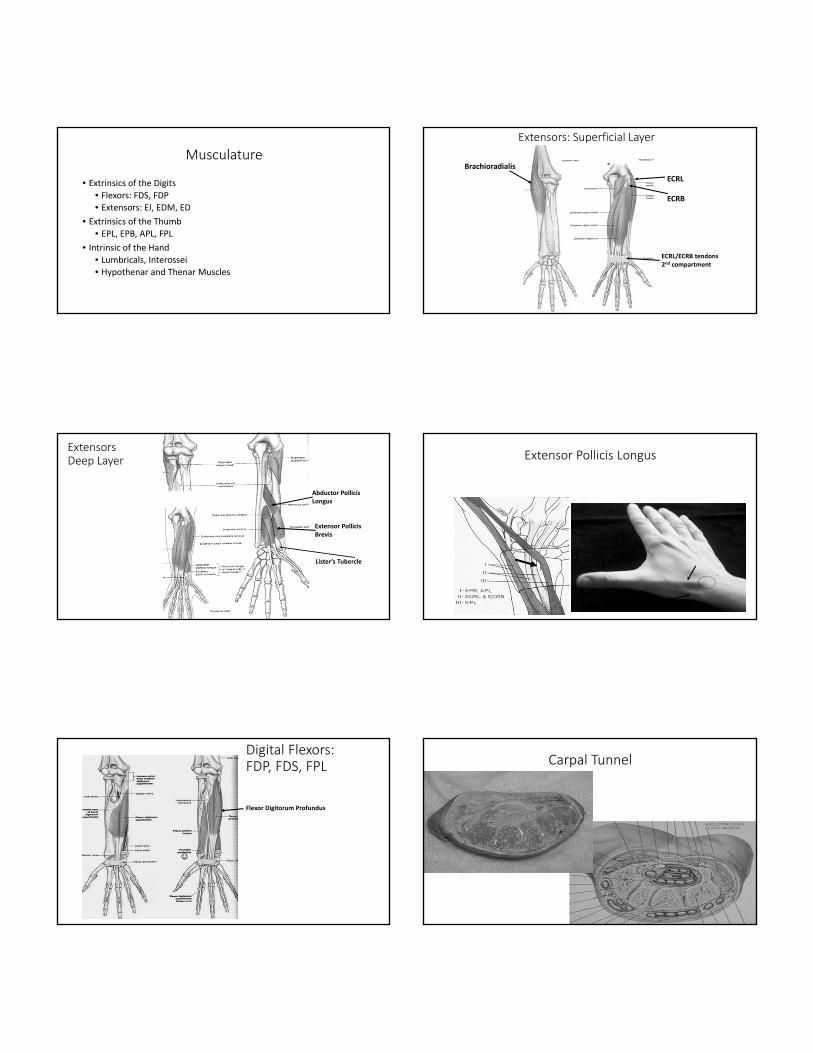
Musculature
• Extrinsics of the Digits• Flexors: FDS, FDP• Extensors: EI, EDM, ED
• Extrinsics of the Thumb
• EPL, EPB, APL, FPL
• Intrinsic of the Hand • Lumbricals, Interossei
• Hypothenar and Thenar Muscles
Extensors: Superficial Layer
Brachioradialis
ECRL
ECRB
ECRL/ECRB tendons2nd compartment
ExtensorsDeep Layer
Abductor PollicisLongus
Extensor PollicisBrevis
Lister’s Tubercle
Extensor Pollicis Longus
Digital Flexors: FDP, FDS, FPL
☺
Flexor Digitorum Profundus
Carpal Tunnel

Extrinsic Flexors: FDS and FDP
• Synovial linings decrease friction in tight places (CT and FDS bifurcation)
• Function is dependent on intact gliding structures; sheaths and pulley system can enhance or impede gliding
Tendon Sheath
Extrinsic Flexors: FDS and FDPLength Tension Issues
• FDS and FDP are dependent on wrist position to enhance function;35°‐40°ext for maximum grip
• ECRB provides counterbalance to prevent wrist flexion; ECRL contributes with power grip
General Observation: Tenodesis
Flexor Tendon Pulley System
Maintains tendons and sheath close to bone to prevent bow stringing and enhance mechanical advantage
Flexor Tendon Pulley System
• A2 and A4 most crucial
• Loss will result in decreased flexion ROM and grip strength
A2
A4

Flexor Tendon Pulley System
Loss will result in
decreased flexion
ROM and
grip strength
Vincula
Trigger Finger
Flexors vs. Extensors
• Extensor do not have
a pulley system
• “Bow stringing” at extensor retinaculum
• All extensor tendons are extrasynovial except for zone 7
Extrinsic Extensors: 6 Compartments
I APL and EPB
II ECRL and ECRB
III EPL
IV EDC and EIP
V EDMQ
VI ECU
Separation occurs at retinaculum.
1st Dorsal Compartment: Site of DeQuervain’s

Extrinsic Extensors
• EIP and EDM add independent function not strength
• ED can produce IP extension if MPs blocked in slight flexion
Juncturae Tendinae
• Link EDC to prevent independent function
• Maintain dorsal placement of extensors tendons over MPs during flexion
http://www.lambchop.tv/
Bet You Can’t Extensor Mechanism
• EDC flattens into extensor hood just distal to MCP joint
• Central tendon inserts onto base
of middle phalanx
• Lateral bands arise at PIP joint and reunite into terminal tendon

Extensor Mechanism
• ORL arises from the A2 pulley near proximal phalanx
• ORL lies volar to PIP joint and dorsal to DIP joint
• Intrinsics contribute
to the lateral bands
Extensor Mechanism
• Oblique Retinacular Ligaments (ORL)• Synchronous IP flexion or extension
Boutonniere Deformity is a clinical example of a disruption of the extensor mechanism
Swan Neck Deformity

Intrinsics of the Digits
• Support Arches of the Hand:transverse, longitudinal, oblique
• Contribute to production of grip strength; about 50%
• Small muscles with large cross‐sectional area; capable of large force production
Intrinsics of the Digits Lumbricals
Originate from FDP
tendons and insert
into lateral bands
Hypothenar
• AbDM• FDM• ODM
Transverse Carpal Ligament (TLC) serves as point of attachment of some intrinsic muscles
ThenarEminence
HypothenarEminence
Intrinsics of the Digits • Interossei
(Dorsal and Palmar)• With MCPs extended primarily abd/add
• With MCPs flexed primarily MP flexors

Intrinsics of the Thumb
Thenar Muscles (median nerve)
• Abductor Pollicis Brevis• Flexor Pollicis Brevis• Opponens Pollicis
• Involved in placement and stabilization for prehension
Adductor Pollicis (ulnar nerve)
• responsible for power/strength
Thenar
AdductorPollicis
FBP
OP deep to FBP and ABP
Hard to separate these muscles outfunctionally – therefore recommendtesting as a group
Froment’s Sign
• FPL substitutes for weak AdP
• Indicates ulnar nerve lesion
Arches of the Hand
• Proximal Transversce Arch
• Distal Transverse Arch
• Longitudinal Arch
Prehension
• Grasp and Pinch
Grasp
• Types of Grasp• Hook• Spherical• Cylindrical
Types of Pinch
• Tip to tip
• Pulp to pulp
• Lateral or key
• Chuck • three‐point chuck
Components of Grip and Pinch
• Strength• Extrinsic and Intrinsic
• ROM
• Tendon Gliding
• Lymphatic Function
• Motor Control
• Motor plan
• Timing• Recruitment
• Coordination
• Stable Base especially wrist and thumb
• Load Transfer• Quality of bone and articular cartilage
• Innervation• Sensation• Vascularity• Skin Integrity
Median Nerve Innervation
• FDS
• Lumbricals (II, III)
• AbPB
• OP
• FPB (superficial head)
• Pronator Teres (PT)
• FCR
Anterior Interosseous
• FDP II (III)
• FPL
• Pronator Quadratus
Ulnar Nerve Innervation
• DI and PI
• Lumbricals IV, V
• AdP
• FPB (deep head)
• Hypothenar:• AbDM• FDM• ODM
• FCU
• FDP IV, V (III)
Radial Nerve Innervation
Posterior Interosseous
• EDC
• EPL
• EPB
• APL
• EIP
• EDM
• ECU
• Supinator
• ECRL
• ECRB