urinary calculi
TRANSCRIPT
1
Dr sumer yadav
INTRODUCTION• The diagnosis and management of urolithiasis
have undergone considerable evolution in recent years. The application of noncontrast helical computed tomography (CT) in patients with suspected renal colic is one major advance. The superior sensitivity and specificity of helical CT allow urolithiasis to be diagnosed or excluded definitively and expeditiously without the potential harmful effects of contrast media.
2
INTRODUCTION (cont.)
• Initial management is based on three key concepts: (1) the recognition of urgent and emergency requirements for urologic consultation, (2) the provision of effective pain control using a combination of narcotics and nonsteroidal anti-inflammatory drugs in appropriate patients and (3) an understanding of the impact of stone location and size on natural history and definitive urologic management.
3
4
EPIDEMIOLOGY• One person in 10 develops kidney stones during
his/her lifetime in North India. Renal stone disease accounts for 7-10 of every 100 hospital admissions. Most common form of urinary calculi in India is pure Calcium Oxalate 86.1%.
• Stone disease is two to three times more common in males than in females. It occurs more often in adults than in elderly persons, and more often in elderly persons than in children.
5
• In addition, urolithiasis occurs more frequently in hot, arid areas than in temperate regions. • Decreased fluid intake and consequent urine
concentration are among the most important factors influencing stone formation. Certain medications, such as triamterene (Dyrenium), indinavir (Crixivan) and acetazolamide (Diamox), are also associated with urolithiasis.
EPIDEMIOLOGY cont.
6
ETIOPATHOGENESIS OF STONE DISEASE• Supersaturation of urine is the key to stone
formation
• Intermittent supersaturation - Dehydration
• Crystal aggregation
• Anatomic Abnormailities – PUJ
• Bacterial Infection
• Defects in transport of Calcium and Oxalate by Renal epithelia
E.Coli infection increases matrix content in urine . Proteus makes urine alkaline 7
TYPES OF KIDNEY / URETER STONES
• OXALATE (CALCIUM OXALATE)
• PHOSPHATE
• URIC ACID & URATE
• CYSTINE
8
UNCOMMON STONESXANTHINE STONES
– (Autosomal Recessive . Def of Xanthine Oxidase leading to Xanthinuria)
DIHYDROXYADENINE STONE
– ( Def. of enzyme adenine phospo ribosyl transferase )
SlLICATE STONES
– Rare in humans ( excess intake of Antacid with Mg Trisilicate. Mostly in cattle due to ingestion of Sand )
MATRIX
- Infection by Proteus - Radiolucent (all calculi have some amt ( 3%) of matrix but matrix calculus has 65% Matrix content in calculi)
9
Uncommon StonesTRIAMTERENE
– Anti-hypertensive used with hydroclorothiazide – spare Potassium. Mostly found as a nucleus in Ca oxalate or uric acid calculus
Indinavir Stones
- Drug to treat AIDS (4 to13%)
Ephedrine or Guifenesin
– Cough medicine - Radiolucent
10
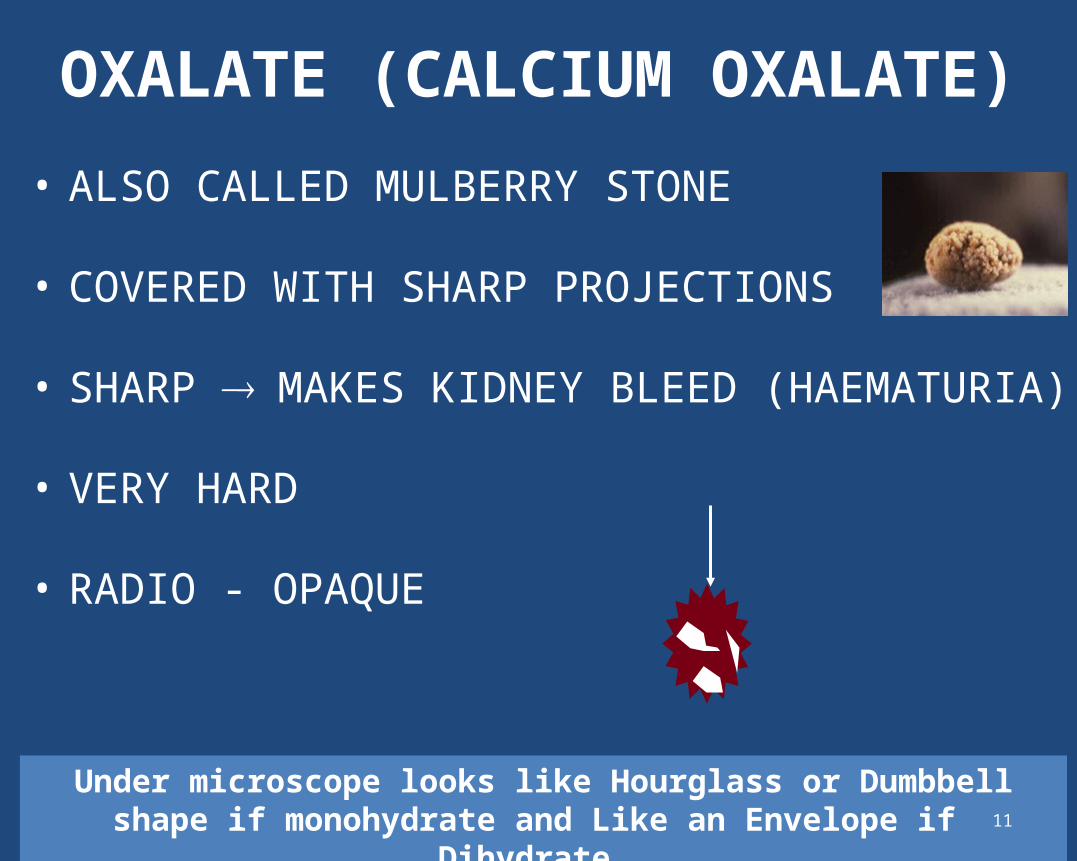
OXALATE (CALCIUM OXALATE)
• ALSO CALLED MULBERRY STONE
• COVERED WITH SHARP PROJECTIONS
• SHARP MAKES KIDNEY BLEED (HAEMATURIA)
• VERY HARD
• RADIO - OPAQUE
Under microscope looks like Hourglass or Dumbbell shape if monohydrate and Like an Envelope if Dihydrate 11
PHOSPHATE STONE
• USUALLY CALCIUM PHOSPHATE
• SOMETIMES CALCIUM MAGNESIUM AMMONIUM PHOSPHATE OR TRIPLE PHOSPHATE
• SMOOTH MINIMUM SYMPTOMS
• DIRTY WHITE
• RADIO - OPAQUE
Calcium Phosphate also called ‘Brushite’ appears like Needle shape under microscope 12
PHOSPHATE STONES
IN ALKALINE URINE
ENLARGES RAPIDLY
TAKE SHAPE OF CALYCES
STAGHORN
Struvite can form Stag-horn and appear like coffin lid under microscope 13
URIC ACID & URATE STONE• HARD & SMOOTH
• MULTIPLE
• YELLOW OR RED-BROWN
• RADIO - LUCENT (USE ULTRASOUND)
Under microscope appear like irregular plates or rosettes
pKa of uric acid 5.75 – at this pH 50% of uric acid insoluble.If pH falls further - uric acid more insoluble 14
CYSTINE STONE
• AUTOSOMAL RECESIVE DISORDER
• USUALLY IN YOUNG GIRLS
• DUE TO CYSTINURIA -
• CYSTINE NOT ABSORBED BY TUBULES
• MULTIPLE
• SOFT OR HARD – can form stag-horns
• PINK OR YELLOW
• RADIO-OPAQUE
Under microscope appears like hexagonal or benezene ring – ask for first morning sample 15
DIAGNOSIS AND INITIAL MANAGEMENT OF KIDNEY STONES
16
DIAGNOSIS• Diagnosis of renal stone disease involves a
medical history, physical examination, laboratory evaluation, and imaging tests. The physician determines if the patient has a history of kidney stones, documents past medical conditions, and evaluates present symptoms. Fever may indicate a urinary tract infection that requires antibiotics.
17
18
THE DIAGNOSIS• The various presentations of renal colic and
its broad differential diagnosis, an organized diagnostic approach is useful.
• Symptomatic stones essentially present as abdominal pain.
• Renal colic may be suspected based on the history and physical examination, but diagnostic imaging is essential to confirm or exclude the presence of urinary calculi.
19
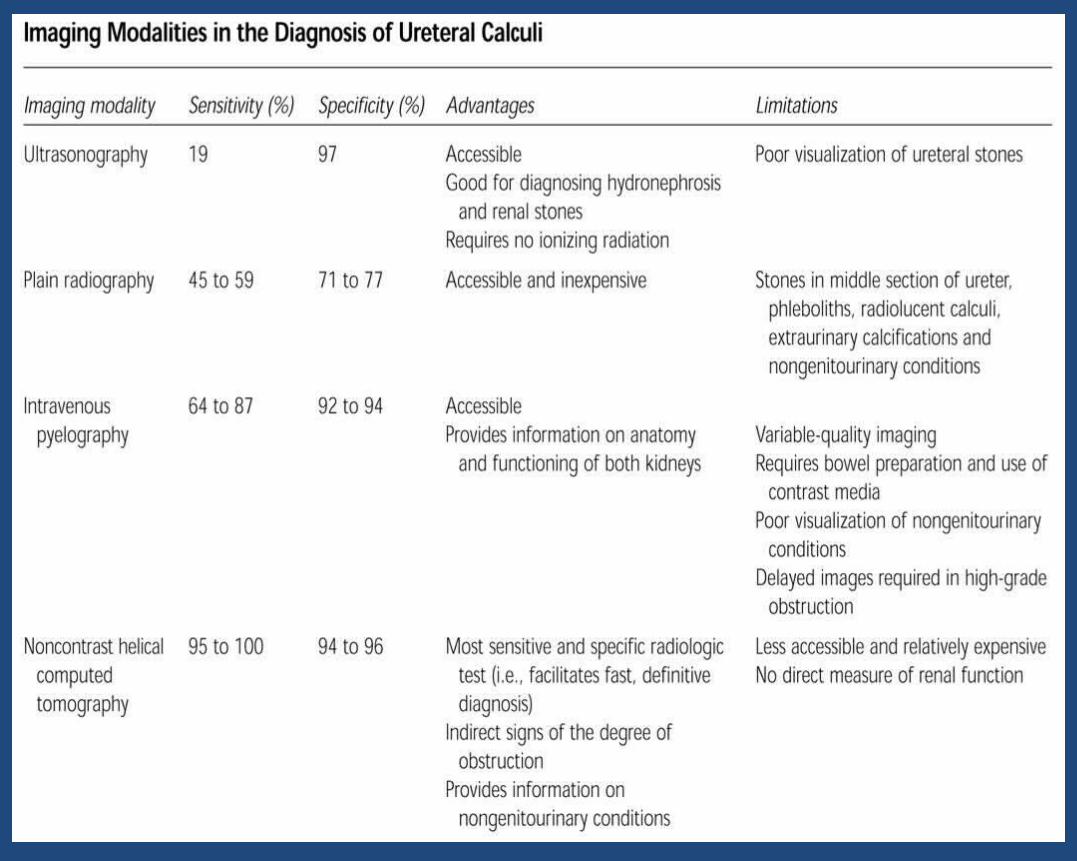
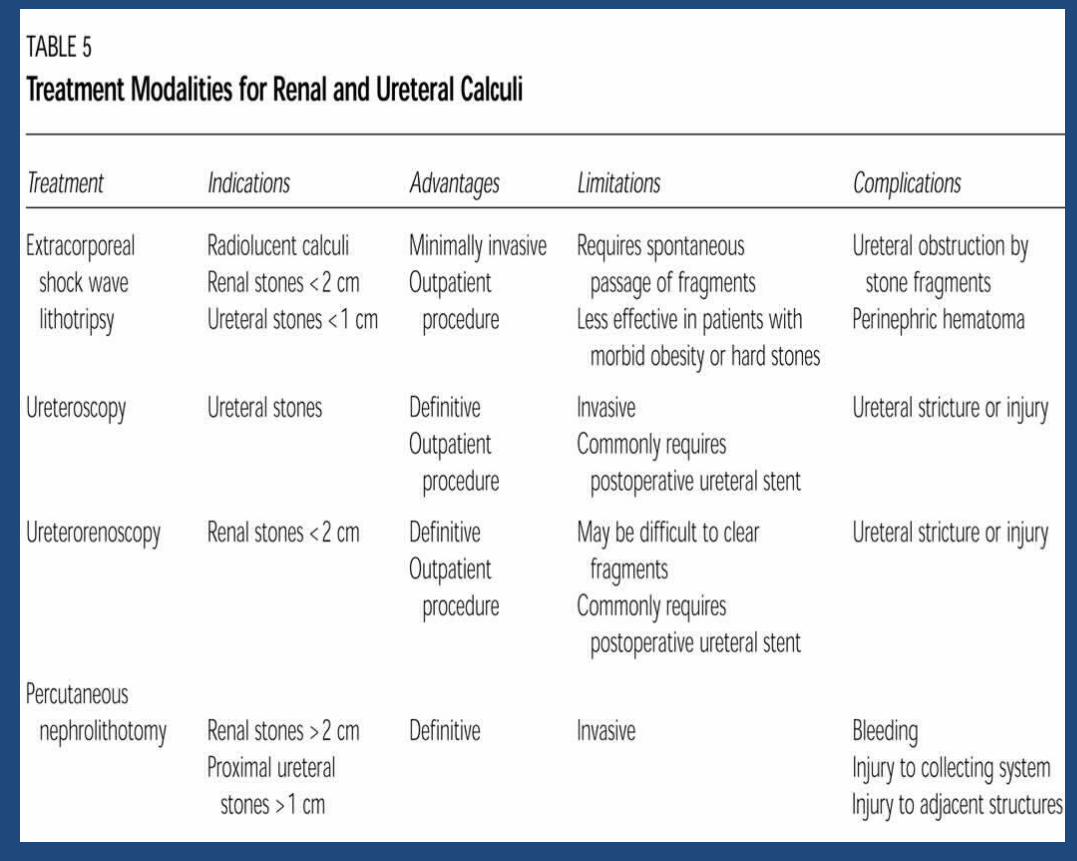
THE DIAGNOSIS cont.
• Several imaging modalities are available, and each has advantages and limitations (Table).• Diagnostic imaging is essential to
confirm the size and location of urinary tract calculi. A diagnosis of renal colic cannot be based on the clinical findings alone.
20
21
URINALYSIS• Urinalysis will be performed to look
for blood, infection or crystals in the urine. It is common to see microscopic traces of blood in the urine when a kidney stone is present, especially when it is moving down the ureter.
22
Of currently available imaging techniques, non-contrast helical computed tomography has the highest sensitivity and specificity for the identification of urinary tract stones. In the future, it will probably become the imaging technique of choice for suspected renal colic. 23

MANAGEMENT STRATEGY
24
INTRODUCTION• The management of urinary calculi
has undergone dramatic changes since the early 1980s with the introduction of extracorporeal shock-wave lithotripsy (ESWL) using the Dornier HM3 device and with the popularization of percutaneous nephrolithotomy (PNL).
25
• After emergency situations have been ruled out and adequate analgesia has been achieved, the next step is to formulate a strategy for managing the stone. Clinical experience with urolithiasis has been refined with statistical analysis to provide sound principles for definitive management.
• The two major After emergency situations have been ruled out and adequate analgesia has been achieved, the next step is to formulate a strategy for managing the stone.
26
• The development of minimally invasive surgical techniques for stone surgery has depended heavily on technologic advances in several areas, including fiberoptics; imaging; and development of shock wave, ultrasonic, electrohydraulic, and laser lithotriptors. Available technology accelerated development of modern techniques for stone removal including, ureteroscopic stone removal (URS), PNL, and most importantly, ESWL. The term endourology was coined to encompass antegrade and retrograde techniques for the closed manipulation of the urinary tract.
27
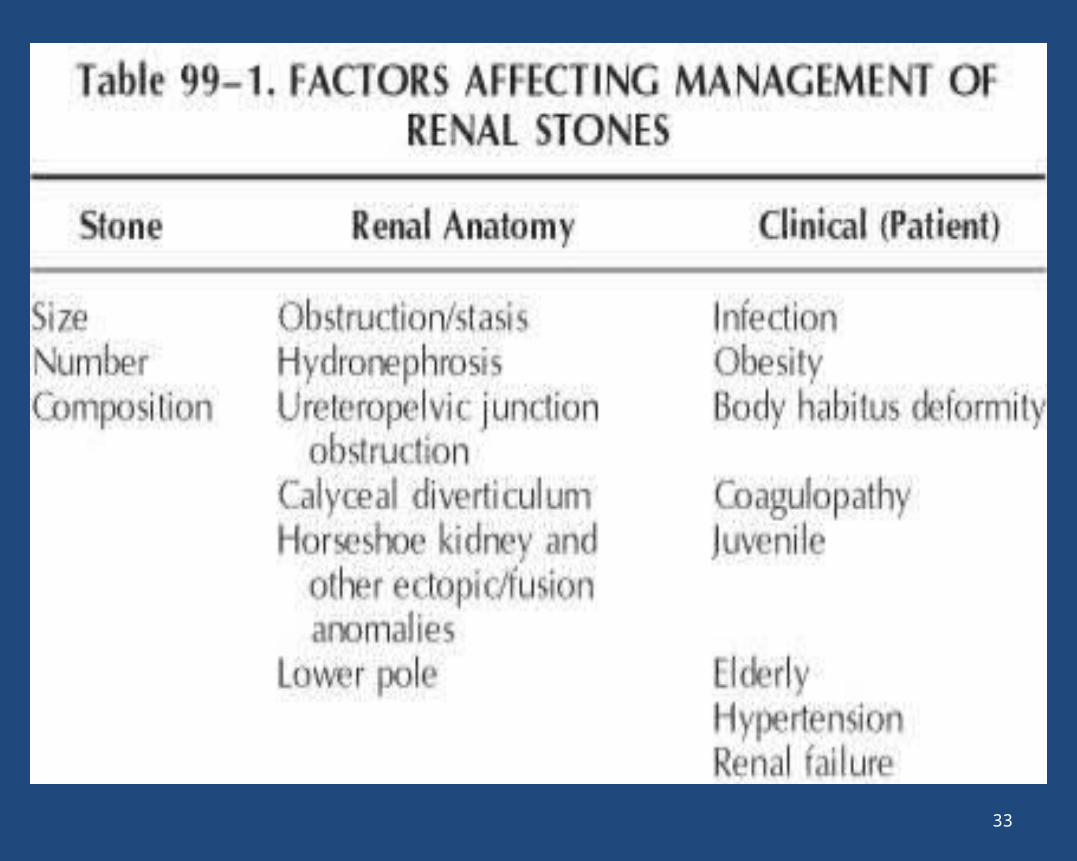
MANAGEMENT OF RENAL STONE
• The characteristics of the stones (size, number, location, and
composition), renal anatomy, and clinical factors are all considered
when selecting a treatment approach for renal calculi.
28
GENERAL MEDICAL TREATMENTMedical therapy for stone disease serve two purposes: -Treatment of Acute Episode: - Specific guidelines for emergency management are as follows: -
• Supranormal Hydration• Analgesia: narcotic or nonsteroidal anti-
inflammatory drug (NSAIDs)• Antiemetic agents such as metoclopramide HCI
and prochlorperazine may also be added as needed.
29
• The traditional out patient treatment indicated above has recently been improved by the application of active medical explosive therapy MET.
1. The calcium channel blocker nifedipine relaxes ureteral smooth muscle and enhances stone passage.
2. The alpha blotters, such as terazosin, and the alpha-1 selective blockers, such as tamsulosin, also relax musculature of the ureteral and lower urinary tract, markedly facilitating passage of ureteral stones.
3. Analgesic therapy combined with MET dramatically improves the passage of stones, addresses pain, and reduces the need for surgical treatment.
30
MANAGEMENT OF RENAL CALCULI
• The goal of surgical stone management is to achieve maximal stone clearance with minimal morbidity to the patient.
• Four minimally invasive treatment modalities are available for the treatment of kidney stones ESWL, PNL, retrograde ureteroscopic intrarenal surgery (RIRS), and laparoscopic stone surgery.
31
RENAL CALCULI cont.• The majority (about 80% to 85%) of "simple"
renal calculi can be treated satisfactorily with ESWL. Several factors were associated with poor results of ESWL, including large renal calculi (mean, 20 mm), stones within dependent or obstructed portions of the collecting system, stone composition (mostly calcium oxalate monohydrate and brushite), obesity or a body habitus.
32
33
PREOPERATIVE EVALUATION• Patients who have radiographic or clinical
features suggestive of struvite, or in whom infection is suspected, should receive 2 weeks of broad-spectrum antibiotics before surgery to reduce the risk of sepsis. Parenteral antibiotics should be administered preoperatively in any patient in whom urinary infection is suspected.
34
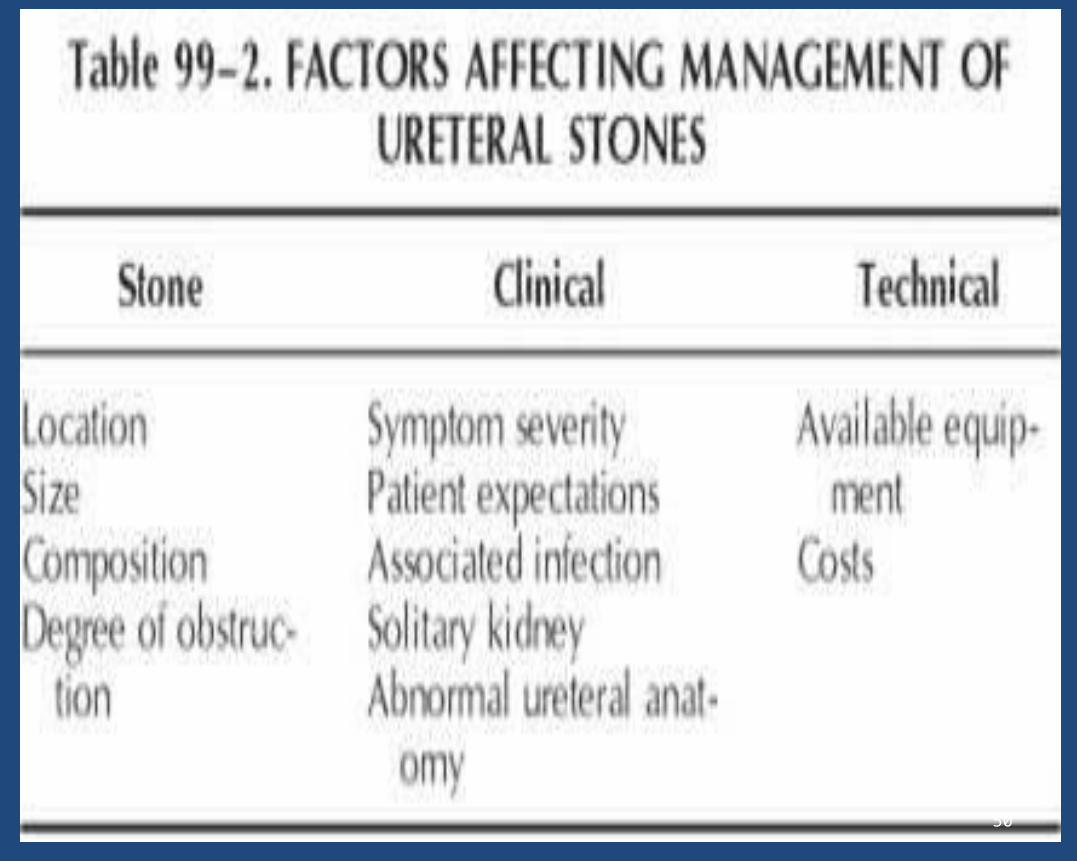
STONE FACTORS
• Stone factor included stone burden (size and number), stone composition, and stone location.
35
STAGHORN STONES• The ideal management of staghorn calculi is
threefold. First, complete surgical removal of the entire stone burden is essential. If all the infected material is not removed, urea-splitting bacteriuria may persist, leading to eventual stone regrowth. The procedure or combination of procedures most likely to render the patient free of stone material with the lowest morbidity should be selected. Second, any metabolic abnormalities need to be identified and treated appropriately.
36
Surgical Management of Staghorn Calculi
• OPEN STONE SURGERY (OSS) : - Overall, the stone-free rate after OSS for struvite stones is about 85%.
37
VARIOUS OPEN SURGICAL TECHNIQUES
• PYELOLITHOTOMY: - Is effective, especially with an extra renal pelvis.
• ANATROPHIC NEPHROLITHOTOMY: - Is used with complex staghon calculi.
• RADIAL NEPHROTOMY: - Given access to limited calyces of the collecting system.
• EXTENDED PYELOLITHOTOMY
38
• URETEROLITHOTOMY: - Long standing ureteral calculi those inaccessible with endoscopy and those resistant to ESWL can be extracted with this technique.
• COAGULUM PYELOLITHOTOMY: - Is mainly indicated in cases of multiple stones, soft and crumbly stone or stones, small, mobile caliceal stones, and as an aid to fixing caliceal stone or stones in the calix prior to partial resection of the kidney or nephrolithotomy.
39
Surgical Management of Staghorn Calculi Cont.• SANDWICH THERAPY: - The most frequently used
regimen was described by Streem and coworkers (1987) as sandwich therapy, consisting of primary percutaneous debulking followed by ESWL of residual inaccessible infundibulo-calyceal stone extensions or fragments. After ESWL, a secondary percutaneous procedure is performed (Streem, 1997b).
• Nephrectomy: - This is a reasonable option for a poorly functioning kidney bearing a staghorn stone.
40
Treatment Decisions by Stone Composition
• Cystine and brushite stones are the most resistant to ESWL, followed by calcium oxalate monohydrate stones.
• Generally, stones that fragment with difficulty (i.e., brushite, cystine, calcium oxalate monohydrate) should be treated with ESWL only when they are small (i.e., less than 1.5 cm). Larger stones are preferentially treated with PNL or RIRS.
41
Treatment Decisions by Renal Anatomy• Anatomic factors, congenital or acquired, that
hinder stone clearance adversely affect the results of ESWL.
• Ureteropelvic Junction Obstruction: Although, patients with stones and concomitant ureteropelvic junction obstruction have traditionally been treated by open pyeloplasty and stone extraction, PNL with concomitant endopyelotomy can achieve good results with less morbidity.
42
Treatment Decisions by Renal Anatomy Cont.• Horseshoe Kidney and Renal Ectopia: -
ESWL can achieve satisfactory results in properly selected patients (i.e., those with stones less than 1.5 cm) in the presence of normal urinary drainage. For larger stones or when there is evidence of poor urinary drainage, PNL should be used as the primary approach.• Ectopic Kidney : - Treatment of choice ESWL
Alternatively, percutaneous transperitoneal nephrolithotomy can be done.
43
• Lower Pole Stones: - Overall stone-free rate for ESWL when applied to LPS was 60%. In comparison, the results of ESWL for upper and middle pole calyces range from 70% to 90%.
44
• The efficacy of PNL was shown to be independent of stone size (approximately 90% stone-free rate), whereas the efficacy of ESWL dropped rapidly as stone size increased (from 74% to 56% to 33% for stones 10 mm or smaller, 11 to 20 mm, and larger than 20 mm, respectively).
• The results of the Lower Pole Study Group suggest that PNL should be considered the primary approach for LPS larger than 10 mm.
45
TREATMENT DECISIONS BY CLINICAL FACTORS• Morbid obesity: - RIRS may be the preferred
treatment for morbidly obese patients when the stone burden is not excessively large.
• Patients with spinal deformity or limb contractures may also be difficult to position within the lithotriptor. Alternative treatment modalities, including PNL and ureteroscopy using flexible instruments, may be preferable in these patients.
46
URETERAL CALCULI• The goal of surgical management of ureteral
calculi is to achieve complete stone clearance with minimal morbidity to the patient.
• Most ureteral calculi are 4 mm or smaller and pass spontaneously, although not without discomfort and expense to the patient. Ureteral calculi of any size are often associated with renal obstruction, and care must be taken to prevent irreversible damage to the kidney, whether choosing expectant or active treatment.
47
48
Referral to a urologist is appropriate for patients with a ureteral stone more than 5 mm in greatest diameter or a stone that has not passed after two to four weeks.
49
50
• Ureteral calculi are stones that usually form in the renal collecting system, then progress down the ureter. They tend to become lodged at sites where the ureter narrows. The three most common entrapment sites are at the ureteropelvic junction, over the iliac vessels and at the ureteral meatus.
51
FACTORS AFFECTING TREATMENT DECISIONS
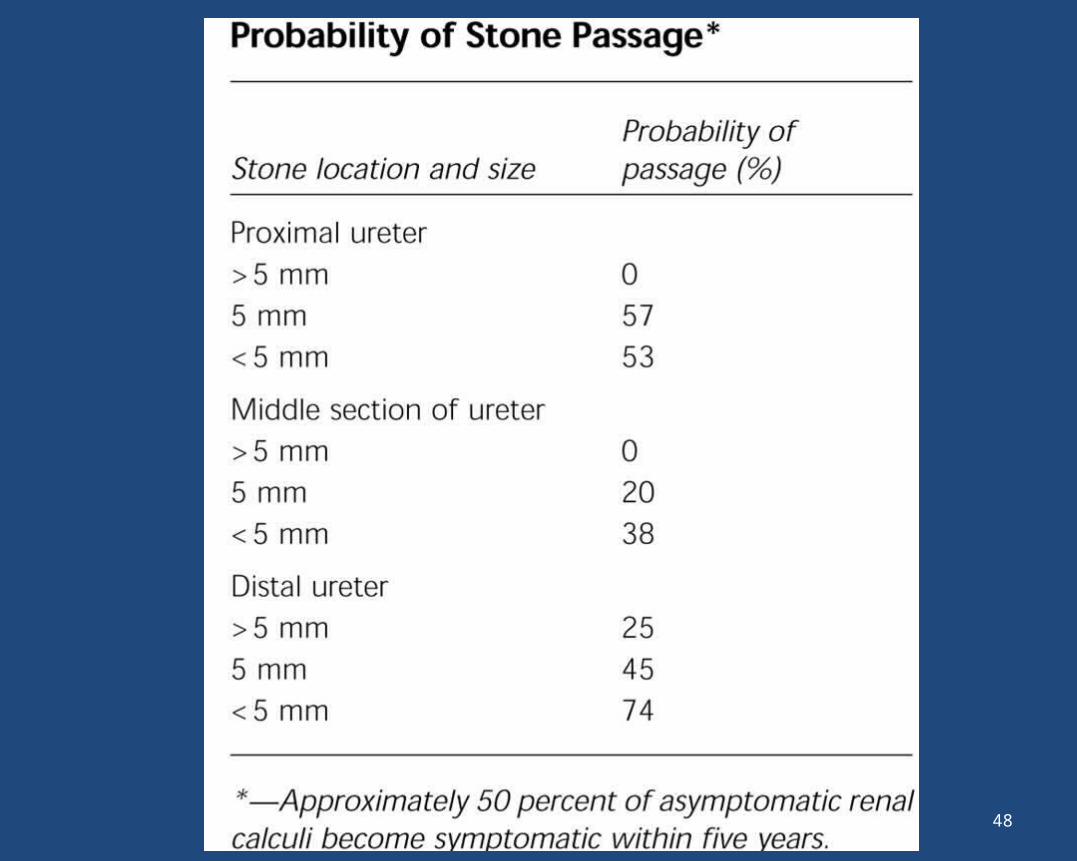
1) Location: - the statistical probability of spontaneous ureteral stone passage is inversely related to stone size and proportional to the distance of the ureter traversed.
2) Size and number: - stones less than 5 mm in diameter pass spontaneously. Stones larger than 8 mm require ESWL or Ureterscopy removal.
52
Cont.
4) Stone composition: - Brushite, cystine, and calcium oxalate monohydrate are relatively resistant to ESWL.
53
CLINICAL FACTORS• Pain: - The pain of ureteral colic is
mediated by prostaglandins released by the ureter in response to obstruction. • Infection associated with ureteral
stones or obstructed pyelonephritis is a relatively common and potentially life-threatening urologic emergency.
54
Infection associated cont.• Patients are typically febrile and may
present with hypotension or septic shock. Urgent drainage of the obstructed portion of the urinary tract by either ureteral catheter or percutaneous nephrostomy is essential. A urine culture from the obstructed segment will aid in directing antibiotic therapy.
55
SOLITARY KIDNEY
• A ureteral stone obstructing a solitary kidney demands prompt attention with drainage internally via a stent and definitive stone treatment (ESWL or URS).
56
57
• Accepted alternatives for treating patients with ureteral calculi can be grouped into five general categories:
1)Observation (also termed “expectant management” and “watchful waiting”);
2)Shock wave lithotripsy (SWL);3)Ureteroscopy (URS);4)Percutaneous nephrolithotomy (PNL); and5)Open surgery (referring to any method of open
surgical exposure of the ureter and removal of stones)
58
PROXIMAL URETERAL STONES• The surgical treatment options for proximal
ureteral stones include ESWL with or without stone manipulation; ureteroscopy; PNL; and, rarely, open and laparoscopic stone surgery.
• ESWL, by whatever technique (push back or in situ), should be the primary approach for stones of less than 1 cm in the proximal ureter. For stones larger than 1 cm in diameter, ESWL, PNL, and ureteroscopy are all acceptable choices.
59
PROXIMAL URETERAL STONES cont.
• Ureteral stenting is appropriate for other indications, such as management of pain, relief of obstruction, and difficult-to-visualize stones, and is mandatory in patients who have a solitary obstructed kidney.
60
DISTAL URETERAL STONES• Surgical treatment options for distal
ureteral stones include ESWL with or without a stent; ureteroscopy with extraction or intracorporeal lithotripsy; and, rarely, open and laparoscopic stone surgery.• ESWL and ureteroscopy were both
considered acceptable treatment options.
61
BLADDER CALCULI• Vesical calculi affect men predominantly and
account for 5% of urinary calculi in the Western world. In the United States, bladder stones usually occur in men older than 50 years and are often associated with bladder outlet obstruction.
• Risk factors for bladder calculi include bladder outlet obstruction; neurogenic bladder; chronic bacteriuria (urea-splitting organisms); foreign bodies; bladder diverticula; and, rarely, upper tract stones.
62
BLADDER CALCULI CONT.• Cystoscopy is essential to evaluate
the bladder and the bladder outlet, both to determine the etiology of the stone and to plan the most appropriate treatment approach.
63
TECHNIQUE• As with any urinary tract stone, the
first priority in treatment is to render the patient stone free. However, relief of bladder outlet obstruction, elimination of urinary infection, and correction of urinary stasis should also be addressed as part of the treatment plan.
64
TECHNIQUE cont.• Several modalities exist for the
treatment of bladder calculi, including cystolitholapaxy; cystolithotripsy with electrohydraulic, ultrasonic, laser, or pneumatic lithotripsy; percutaneous cystolithotomy; and open cystolithotomy. Shock-wave lithotripsy may be another option.
65
• Cystolitholapaxy: - with stone-crushing forceps or the optical lithotrite has been used to crush stones since the late 1800s. Contraindications to this procedure include small-capacity bladders, multiple stones, stones larger than 2 cm that cannot be engaged, hard stones, bladder stones in children, and inadequate urethras.
• cystolitholapaxy can be technically difficult and is associated with a complication rate of between 9% and 25%.
66
• Percutaneous cystolithotomy has been advocated as an alternative to open cystolithotomy in pediatric patients with narrow urethras and in patients with impassable or surgically ablated urethras and bladder necks, large stone burdens, or multiple stones with anticipated prolonged operative times.
• Contraindications to this approach include history of bladder malignancy, prior abdominal or pelvic surgeries, prior pelvic radiotherapy, active urinary or abdominal wall infection, and pelvic prosthetic devices
67
• Open cystolithotomy may be indicated in cases of large stone burdens or hard stones refractory to an endoscopic approach, abnormal anatomy precluding safe access, or concomitant open prostatectomy or diverticulectomy.• ESWL is safe and effective in non-
obstructed patients.
68
REVIEW OF MANAGEMENT IN STONE (RENAL, URETERAL & BLADDER )
69
• IN BRIEF MANAGEMENT OF STONE IS DONE BY FOLLOWING PROCEDURES: -–MEDICAL TREATMENT –OPEN SURGERY–NON INVASIVE TECHNIQUE (ESWL)–MINIMAL INVASIVE TECHNIQUE (RIRS,
PCNL, LAP.)
70
OPEN SURGICAL TREATMENT INDICATIONSome type of surgery may be needed to remove a kidney stone if the stone:
• Does not pass after a reasonable period of time and causes constant pain,is too large to pass on its own.
• Blocks the urine flow.• Causes ongoing urinary tract infection.• Damages the kidney tissue or causes constant
bleeding, or has grown larger (as seen on follow up x-ray studies).
71
• Until recently, surgery to remove a stone was very painful and required a lengthy recovery time (4 to 6 weeks). Today, treatment for these stones is greatly improved. Many options exist that do not require major surgery.
72
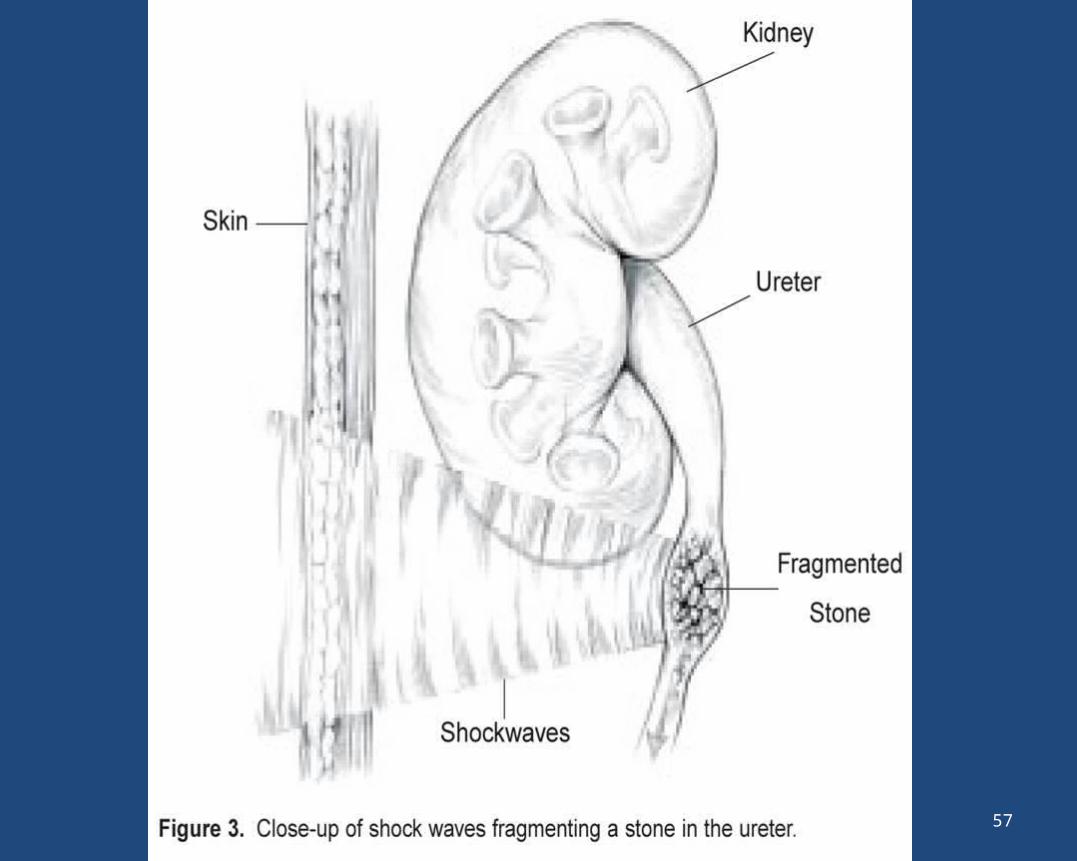
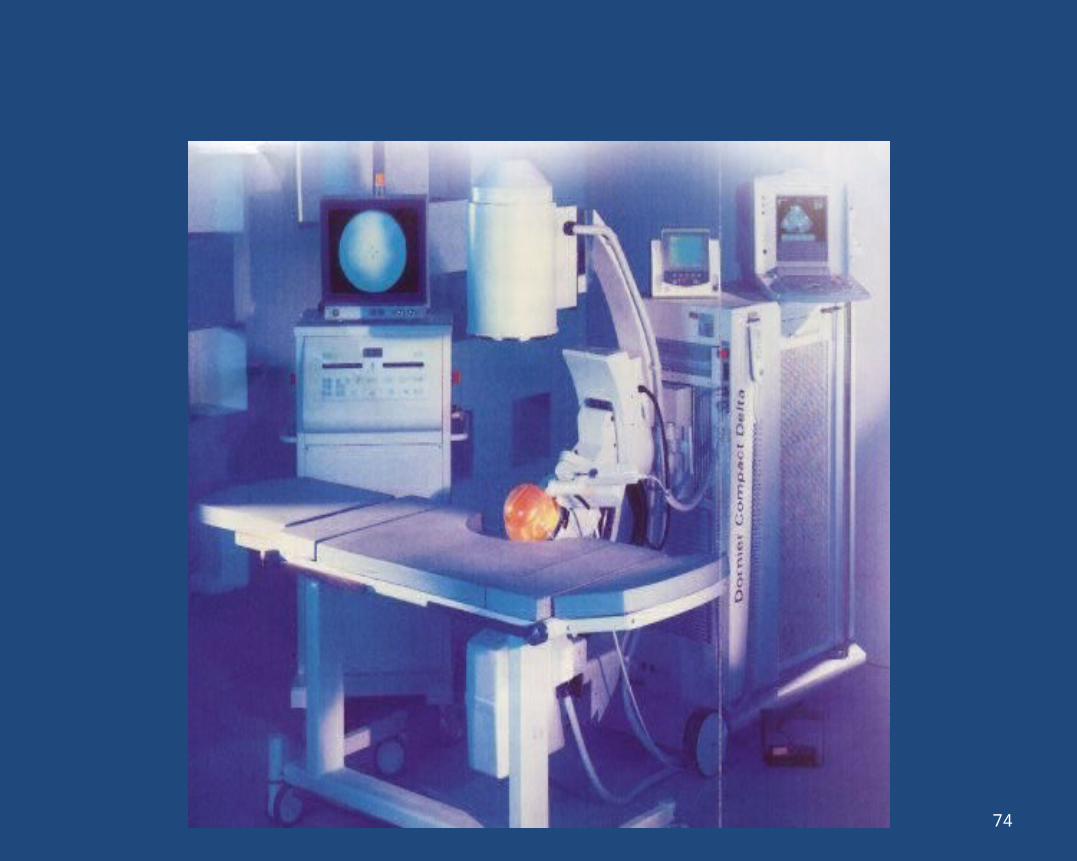
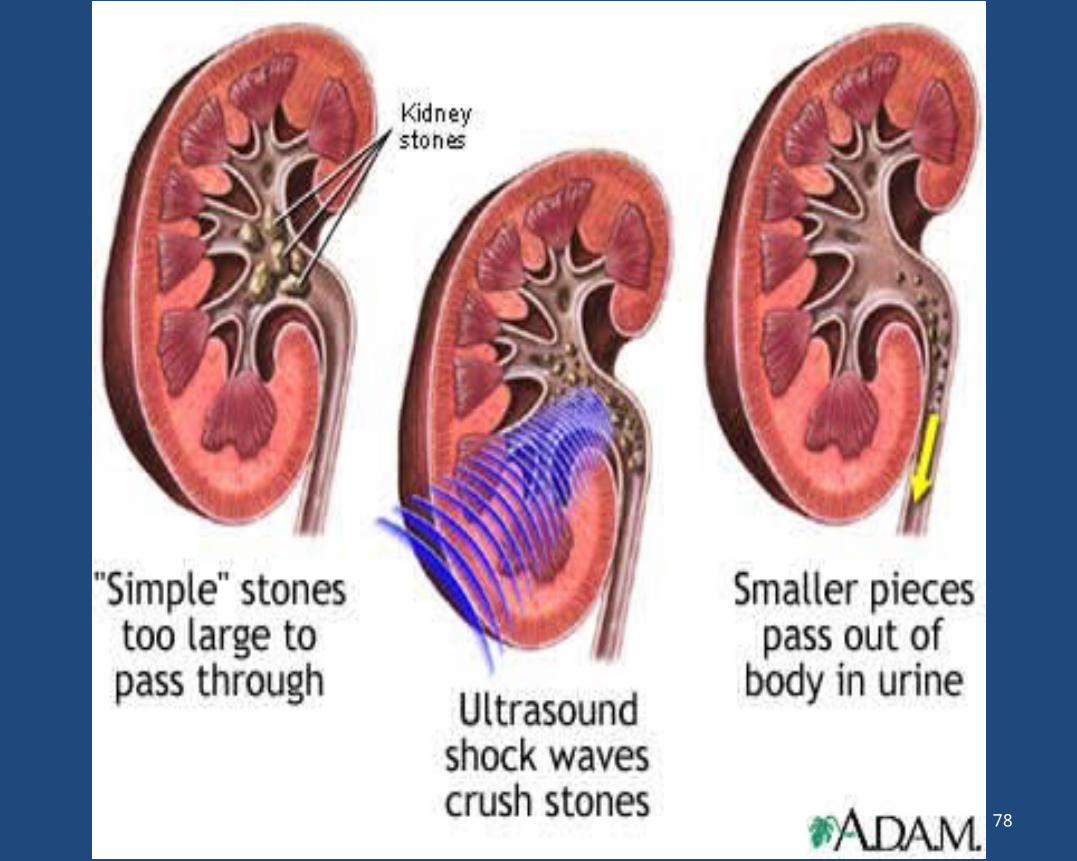
EXTRACORPOREAL SHOCKWAVE LITHOTRIPSY• Extracorporeal shockwave lithotripsy (ESWL)
is the most frequently used surgical procedure for the treatment of kidney stones. ESWL uses shockwaves that are created outside of the body to travel through the skin and body tissues until the waves hit the dense stones. The stones become sand-like and are easily passed through the urinary tract in the urine.
73
74
EXTRACORPOREAL SHOCK-WAVE LITHOTRIPSY
• That sound waves are focusable has been known for centuries.
• Simple renal calculi are those with a stone burden of <2 cm (aggregate diameter) and normal renal anatomy. Most simple renal calculi (80-85%) can be treated successfully with shock wave lithotripsy (fig.).
75
• Lithotripsy may fail or be less effective when stones are larger; stones are located in dependent or obstructed parts of the collecting system; stones are made up of calcium oxalate monohydrate, brushite, or cystine; the patient is obese or has a body build that inhibits proper imaging; or it is difficult to target the stone for shock wave
delivery and subsequent fragmentation.
76
• A retrospective comparison of percutaneous nephrolithotomy and shock wave lithotripsy found that as stone burden increased, the number of lithotripsy treatments and ancillary procedures increased, but stone-free
rates decreased.
77
78
• There are several types of ESWL devices. One device positions the patient in the water bath while the shock waves are transmitted. Other devices have a soft cushion or membrane on which the patient lies. Most devices use either x-rays or ultrasound to help the surgeon pinpoint the stone during treatment. For most types of ESWL procedures, some type of anesthesia is needed.
79
• In some cases, ESWL may be done on an outpatient basis. Recovery time is short, and most people can resume normal activities in a few days.
• Complications may occur with ESWL. Most patients have blood in the urine for a few days after treatment. Bruising and minor discomfort on the back or abdomen due to the shockwaves are also common. To reduce the chances of complications, doctors usually tell patients to avoid taking aspirin and other drugs that affect blood clotting for several weeks before treatment.
80
• In addition, the shattered stone fragments may cause discomfort as they pass through the urinary tract in the urine. In some cases, the doctor will insert a small tube called a stent through the bladder into the ureter to help the fragments pass. Sometimes the stone is not completely shattered with one treatment and additional treatments may be required.
81
PERCUTANEOUS NEPHROLITHOTOMY
• Percutaneous nephrolithotomy is recommended to remove a stone. This treatment is often used when the stone is quite large or in a location that does not allow effective use of EWSL.
82
• In this procedure, the surgeon makes a tiny incision in the back and creates a tunnel directly into the kidney. Using an instrument called a nephroscope, the stone is located and removed. For large stones, some type of energy probe (ultrasonic or electrohydraulic) may be needed to break the stone into small pieces. Generally, patients stay in the hospital for several days and may have a small tube called a nephrostomy tube left in the kidney during the healing process.
83
• One advantage of percutaneous nephrokithotomy over ESWL is that the surgeon removes the stone fragments instead of relying on their natural passage from the kidney.
84
URETEROSCOPIC STONE REMOVAL• Although some ureteral stones can be
treated with ESWL, urethroscopy may be needed for mid- and lower ureter stones. No incision is made in this procedure. Instead, the surgeon passes a small fiberoptic instrument called a ureteroscope through the urethra and bladder into the ureter.
85
• The surgeon then locates the stone and either removes it with a cage-like device or shatters it with a special instrument that produces a form of shockwave. A small tube or stent may be left in the ureter for a few days after treatment to help the lining of the ureter heal.
86
OPEN SURGICAL TECHNIQUES • General/Indications - With the advent of ESWL
and PCNL techniques, open surgical procedures on the kidney have been made virtually obsolete. There are, however, specific indications warranting open surgery. These include: failure of ESWL or PCNL to fragment the entire stone
• Large stone burden that would require multiple ESWL and/or PCNL procedures
• Certain anatomic abnormalities of the urinary tract.
87
POSTOPERATIVE• Hospital stays range from 3 to five
days depending on the type of surgery. Postoperative pain is typically mild to moderate and is easily controlled with intravenous or oral pain medication. An epidural anesthetic can also be used to control postoperative pain.
88
PREVENTION OF STONE RECURRENCE • General Measures of PreventionA.HYDRATION: - high fluid intake results in
reduction of saturation of calcium phosphate calcium oxalate
B.DIET A. Control Dietary protein B. Control Dietary calcium C. Control Dietary sodiumD. Control Dietary oxalateE. Control Dietary phosphate
89
90
SUMMARY POINTS• Unenhanced helical computed
tomography is the best radiographic technique for diagnosing urolithiasis• Shock wave lithotripsy,
ureteroscopy, and percutaneous nephrolithotomy have replaced open surgery for treating urolithiasis
91
SUMMARY POINTS• Most simple renal calculi (80-85%) can be
treated with shock wave lithotripsy• Percutaneous nephrolithotomy is the
treatment of choice for complex renal
calculi• Staghorn calculi should be treated, and
percutaneous nephrolithotomy is the preferred treatment in most patients
92
SUMMARY POINTS
• Ureteroscopy is the preferred treatment in pregnant, morbidly obese, or patients with coagulopathy.• Most ureteral calculi <5 mm in
diameter will pass spontaneously within four weeks of the onset of symptoms.
93

THANKS94