urn: stemi clinical pathwaysdc858063671d84c6.jimcontent.com/.../name/pathway_stemi_st.pdf ·...
TRANSCRIPT
DO
nO
t wr
ite in
this
bin
Din
g m
ar
gin
DO
nO
t w
rit
e in
th
is b
inD
ing
ma
rg
inÌSW
043b
\Îv5
.00
- 0
2/20
12m
at. n
o.: 1
0217
515
sw
043b
Page 1 of 12
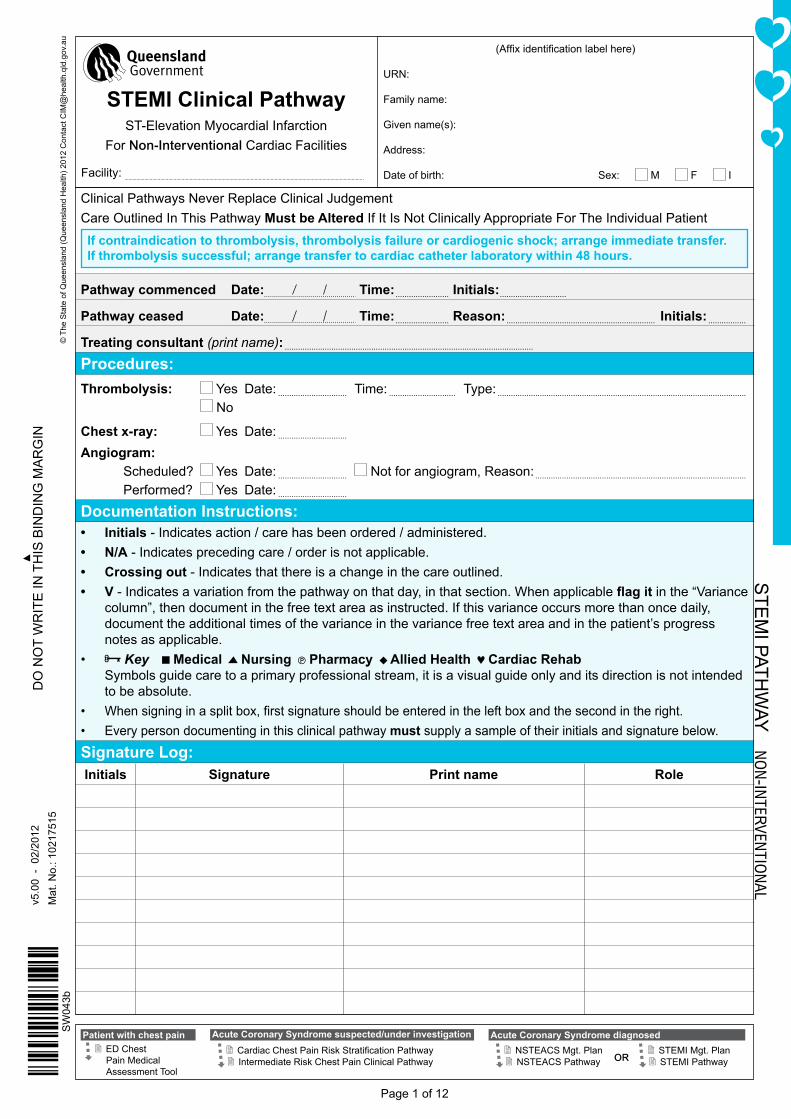
Clinical Pathways Never Replace Clinical JudgementCare Outlined In This Pathway Must be Altered If It Is Not Clinically Appropriate For The Individual Patient
If contraindication to thrombolysis, thrombolysis failure or cardiogenic shock; arrange immediate transfer.If thrombolysis successful; arrange transfer to cardiac catheter laboratory within 48 hours.
Pathway commenced Date: Time: ........................ Initials: ..............................
Pathway ceased Date: Time: ........................ Reason: ................................................................... Initials: .................
Treating consultant (print name): ................................................................................................................
Procedures:Thrombolysis: Yes Date: ............................... Time: .............................. Type: ................................................................................................................ No
Chest x-ray: Yes Date: ...............................
Angiogram: Scheduled? Yes Date: ............................... Not for angiogram, Reason: ...............................................................................................
Performed? Yes Date: ...............................
Documentation Instructions:• Initials - Indicates action / care has been ordered / administered.• N/A - Indicates preceding care / order is not applicable.• Crossing out - Indicates that there is a change in the care outlined.• V - Indicates a variation from the pathway on that day, in that section. When applicable flagit in the “Variance
column”, then document in the free text area as instructed. If this variance occurs more than once daily, document the additional times of the variance in the variance free text area and in the patient’s progress notes as applicable.
• Key Medical Nursing Pharmacy Allied Health Cardiac Rehab Symbols guide care to a primary professional stream, it is a visual guide only and its direction is not intended to be absolute.
• Whensigninginasplitbox,firstsignatureshouldbeenteredintheleftboxandthesecondintheright.• Every person documenting in this clinical pathway must supply a sample of their initials and signature below.
Signature Log:Initials Signature Print name Role
STE
MI PATh
WAY
No
N-IN
terveN
tIoN
al
© T
he S
tate
of Q
ueen
slan
d (Q
ueen
slan
d h
ealth
) 201
2 C
onta
ct C
IM@
heal
th.q
ld.g
ov.a
u
Patient with chest pain ED Chest Pain Medical Assessment Tool
CardiacChestPainRiskStratificationPathway
Acute Coronary Syndrome suspected/under investigation
Intermediate Risk Chest Pain Clinical Pathway
Acute Coronary Syndrome diagnosed NSTEACS Mgt. Plan NSTEACS Pathway STEMI Pathway
STEMI Mgt. PlanOR
(Affixidentificationlabelhere)
URN:
Family name:
Given name(s):
Address:
Date of birth: Sex: M F I
STEMI Clinical PathwayST-Elevation Myocardial Infarction
For Non-Interventional Cardiac Facilities
Facility:
DO
nO
t wr
ite in
this
bin
Din
g m
ar
gin
DO
nO
t w
rit
e in
th
is b
inD
ing
ma
rg
inÌSW
043b
\Îv5
.00
- 0
2/20
12m
at. n
o.: 1
0217
515
sw
043b
Page 2 of 12
Signature Log (continued):Initials Signature Print name Role
(Affixidentificationlabelhere)
URN:
Family name:
Given name(s):
Address:
Date of birth: Sex: M F I
STEMI Clinical PathwayST-Elevation Myocardial Infarction
For Non-Interventional Cardiac Facilities
DO
nO
t wr
ite in
this
bin
Din
g m
ar
gin
DO
nO
t w
rit
e in
th
is b
inD
ing
ma
rg
inÌSW
043b
\Îv5
.00
- 0
2/20
12m
at. n
o.: 1
0217
515
sw
043b
Page 3 of 12
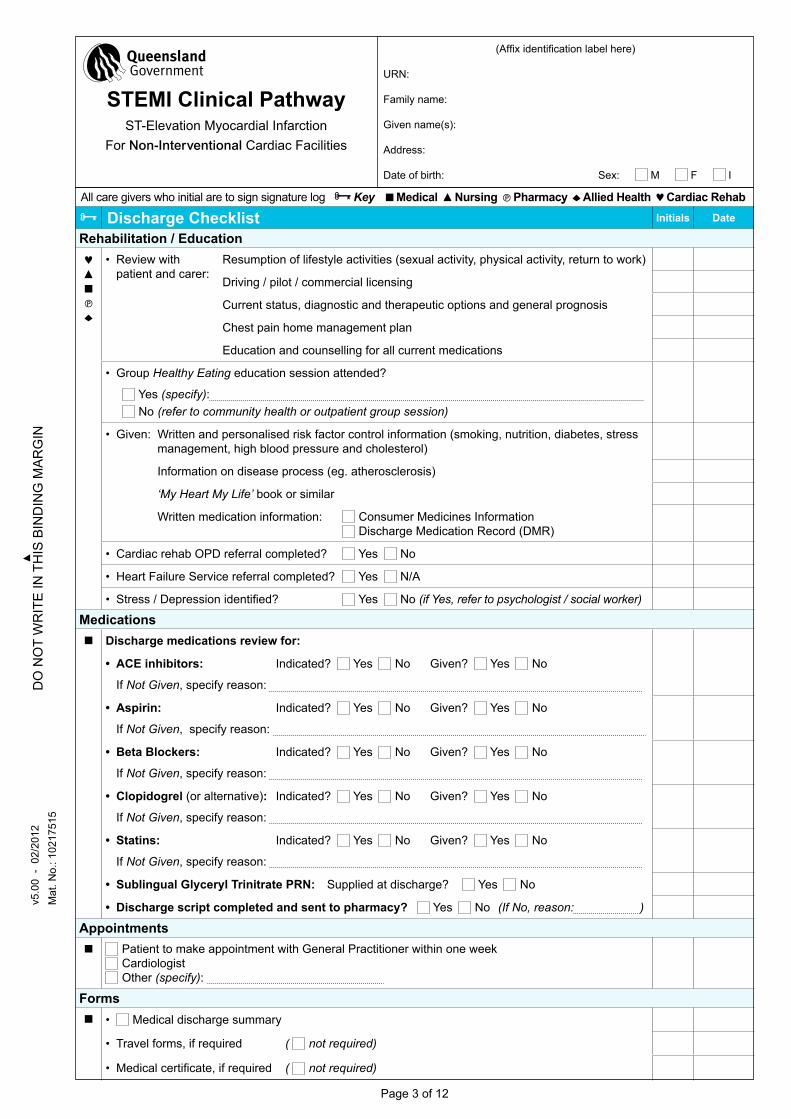
All care givers who initial are to sign signature log Key Medical Nursing Pharmacy Allied Health Cardiac Rehab
Discharge Checklist Initials Date
Rehabilitation / Education• Review with
patient and carer:Resumption of lifestyle activities (sexual activity, physical activity, return to work)
Driving / pilot / commercial licensing
Current status, diagnostic and therapeutic options and general prognosis
Chest pain home management plan
Education and counselling for all current medications
• Group Healthy Eating education session attended?
Yes (specify): No (refer to community health or outpatient group session)
• Given: Written and personalised risk factor control information (smoking, nutrition, diabetes, stress management, high blood pressure and cholesterol)
Information on disease process (eg. atherosclerosis)
‘My Heart My Life’ book or similar
Written medication information: Consumer Medicines Information Discharge Medication Record (DMR)
• Cardiac rehab OPD referral completed? Yes No
• heart Failure Service referral completed? Yes N/A
• Stress/Depressionidentified? Yes No (if Yes, refer to psychologist / social worker)
Medications Discharge medications review for:
• ACE inhibitors: Indicated? Yes No Given? Yes No
If Not Given, specify reason:
• Aspirin: Indicated? Yes No Given? Yes No
If Not Given, specify reason:
• Beta Blockers: Indicated? Yes No Given? Yes No
If Not Given, specify reason:
• Clopidogrel (or alternative): Indicated? Yes No Given? Yes No
If Not Given, specify reason:
• Statins: Indicated? Yes No Given? Yes No
If Not Given, specify reason:
• Sublingual Glyceryl Trinitrate PRN: Supplied at discharge? Yes No
• Discharge script completed and sent to pharmacy? Yes No (If No, reason: )
Appointments Patient to make appointment with General Practitioner within one week
Cardiologist Other (specify):
Forms • Medical discharge summary
• Travel forms, if required ( not required)
• Medicalcertificate,ifrequired ( not required)
(Affixidentificationlabelhere)
URN:
Family name:
Given name(s):
Address:
Date of birth: Sex: M F I
STEMI Clinical PathwayST-Elevation Myocardial Infarction
For Non-Interventional Cardiac Facilities
DO
nO
t wr
ite in
this
bin
Din
g m
ar
gin
DO
nO
t w
rit
e in
th
is b
inD
ing
ma
rg
inÌSW
043b
\Îv5
.00
- 0
2/20
12m
at. n
o.: 1
0217
515
sw
043b
Page 4 of 12
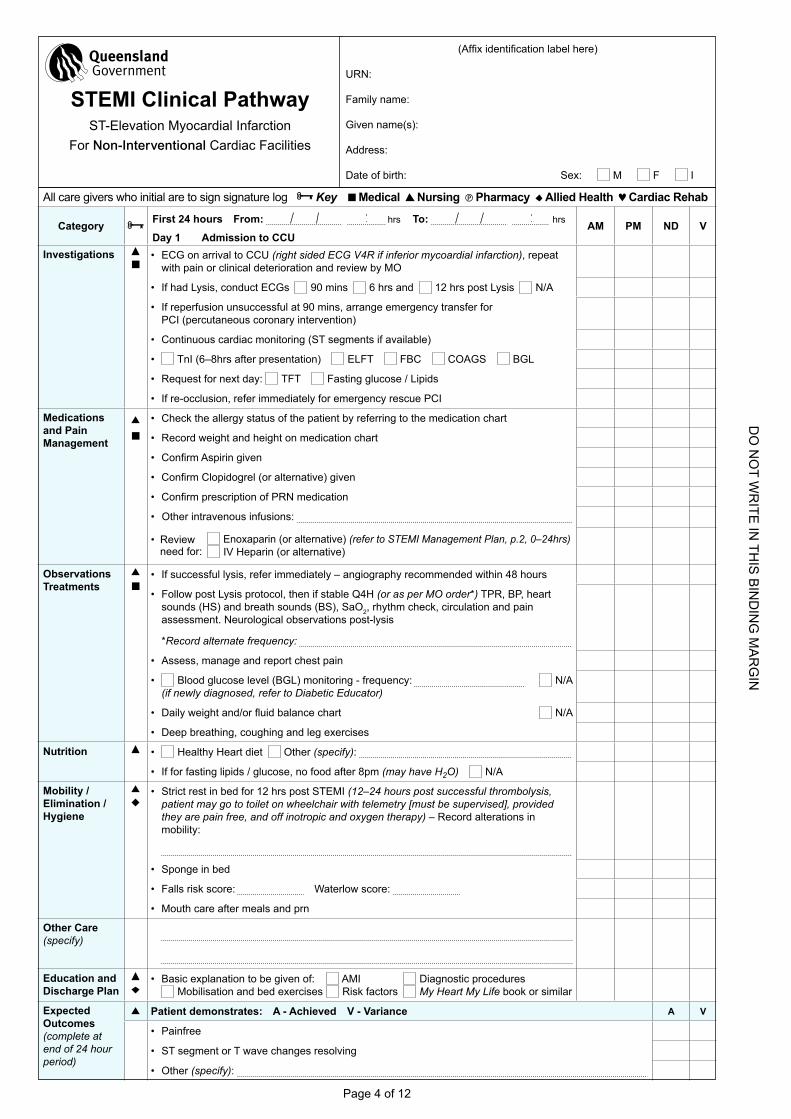
All care givers who initial are to sign signature log Key Medical Nursing Pharmacy Allied Health Cardiac Rehab
Category First 24 hours From: hrs To: hrs
Day 1 Admission to CCU AM PM ND V
Investigations • ECG on arrival to CCU (right sided ECG V4R if inferior mycoardial infarction), repeat
with pain or clinical deterioration and review by MO
• If had Lysis, conduct ECGs 90 mins 6 hrs and 12 hrs post Lysis N/A
• If reperfusion unsuccessful at 90 mins, arrange emergency transfer for PCI (percutaneous coronary intervention)
• Continuous cardiac monitoring (ST segments if available)
• TnI (6–8hrs after presentation) ELFT FBC COAGS BGL
• Request for next day: TFT Fasting glucose / Lipids
• If re-occlusion, refer immediately for emergency rescue PCI
Medications and Pain Management
• Check the allergy status of the patient by referring to the medication chart
• Record weight and height on medication chart
• ConfirmAspiringiven
• ConfirmClopidogrel(oralternative)given
• ConfirmprescriptionofPRNmedication
• Other intravenous infusions:
• Review need for:
Enoxaparin (or alternative) (refer to STEMI Management Plan, p.2, 0–24hrs) IV heparin (or alternative)
Observations Treatments
• If successful lysis, refer immediately – angiography recommended within 48 hours
• Follow post Lysis protocol, then if stable Q4h (or as per MO order*) TPR, BP, heart sounds (hS) and breath sounds (BS), SaO2, rhythm check, circulation and pain assessment. Neurological observations post-lysis
*Record alternate frequency:
• Assess, manage and report chest pain
• Blood glucose level (BGL) monitoring - frequency: N/A (if newly diagnosed, refer to Diabetic Educator)
• Dailyweightand/orfluidbalancechart N/A
• Deep breathing, coughing and leg exercises
Nutrition • healthy heart diet Other (specify):
• If for fasting lipids / glucose, no food after 8pm (may have H2O) N/A
Mobility / Elimination / Hygiene
• Strict rest in bed for 12 hrs post STEMI (12–24 hours post successful thrombolysis, patient may go to toilet on wheelchair with telemetry [must be supervised], provided they are pain free, and off inotropic and oxygen therapy) – Record alterations in mobility:
• Sponge in bed
• Falls risk score: Waterlow score:
• Mouth care after meals and prn
Other Care(specify)
Education and Discharge Plan
• Basic explanation to be given of: AMI Diagnostic procedures Mobilisation and bed exercises Risk factors My Heart My Life book or similar
Expected Outcomes (complete at end of 24 hour period)
Patient demonstrates: A - Achieved V - Variance A V
• Painfree
• ST segment or T wave changes resolving
• Other (specify):
(Affixidentificationlabelhere)
URN:
Family name:
Given name(s):
Address:
Date of birth: Sex: M F I
STEMI Clinical PathwayST-Elevation Myocardial Infarction
For Non-Interventional Cardiac Facilities
DO
nO
t wr
ite in
this
bin
Din
g m
ar
gin
DO
nO
t w
rit
e in
th
is b
inD
ing
ma
rg
inÌSW
043b
\Îv5
.00
- 0
2/20
12m
at. n
o.: 1
0217
515
sw
043b
Page 5 of 12
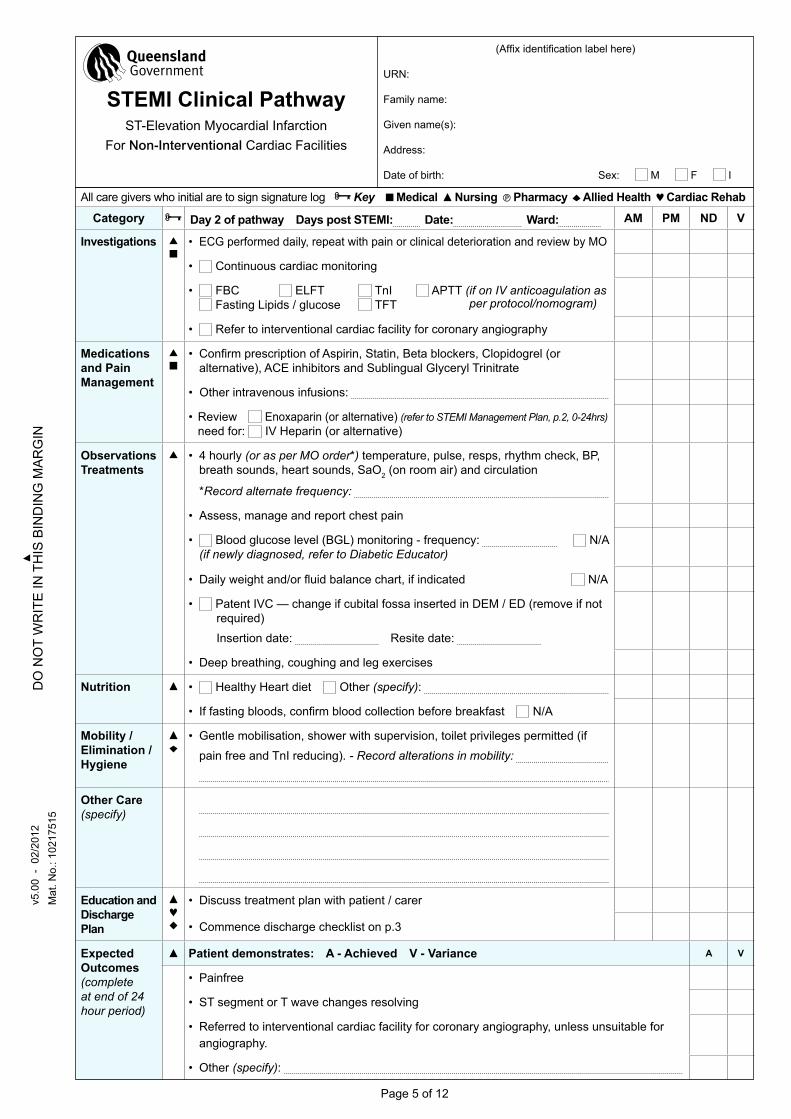
All care givers who initial are to sign signature log Key Medical Nursing Pharmacy Allied Health Cardiac Rehab
Category Day 2 of pathway Days post STEMI: Date: Ward: AM PM ND V
Investigations • ECG performed daily, repeat with pain or clinical deterioration and review by MO
• Continuous cardiac monitoring
• FBC ELFT TnI APTT (if on IV anticoagulation as Fasting Lipids / glucose TFT per protocol/nomogram)
• Refer to interventional cardiac facility for coronary angiography
Medications and Pain Management
• ConfirmprescriptionofAspirin,Statin,Betablockers,Clopidogrel(or
alternative), ACE inhibitors and Sublingual Glyceryl Trinitrate
• Other intravenous infusions:
•Review need for:
Enoxaparin (or alternative) (refer to STEMI Management Plan, p.2, 0-24hrs) IV heparin (or alternative)
Observations Treatments
• 4 hourly (or as per MO order*) temperature, pulse, resps, rhythm check, BP, breath sounds, heart sounds, SaO2 (on room air) and circulation
*Record alternate frequency:
• Assess, manage and report chest pain
• Blood glucose level (BGL) monitoring - frequency: N/A (if newly diagnosed, refer to Diabetic Educator)
• Dailyweightand/orfluidbalancechart,ifindicated N/A
• Patent IVC — change if cubital fossa inserted in DEM / ED (remove if not required)
Insertion date: Resite date:
• Deep breathing, coughing and leg exercises
Nutrition • healthy heart diet Other (specify):
• Iffastingbloods,confirmbloodcollectionbeforebreakfast N/A
Mobility / Elimination / Hygiene
• Gentle mobilisation, shower with supervision, toilet privileges permitted (if
pain free and TnI reducing). - Record alterations in mobility:
Other Care(specify)
Education and Discharge Plan
• Discuss treatment plan with patient / carer
• Commence discharge checklist on p.3
Expected Outcomes(complete at end of 24 hour period)
Patient demonstrates: A - Achieved V - Variance A V
• Painfree
• ST segment or T wave changes resolving
• Referred to interventional cardiac facility for coronary angiography, unless unsuitable for angiography.
• Other (specify):
(Affixidentificationlabelhere)
URN:
Family name:
Given name(s):
Address:
Date of birth: Sex: M F I
STEMI Clinical PathwayST-Elevation Myocardial Infarction
For Non-Interventional Cardiac Facilities
DO
nO
t wr
ite in
this
bin
Din
g m
ar
gin
DO
nO
t w
rit
e in
th
is b
inD
ing
ma
rg
inÌSW
043b
\Îv5
.00
- 0
2/20
12m
at. n
o.: 1
0217
515
sw
043b
Page 6 of 12
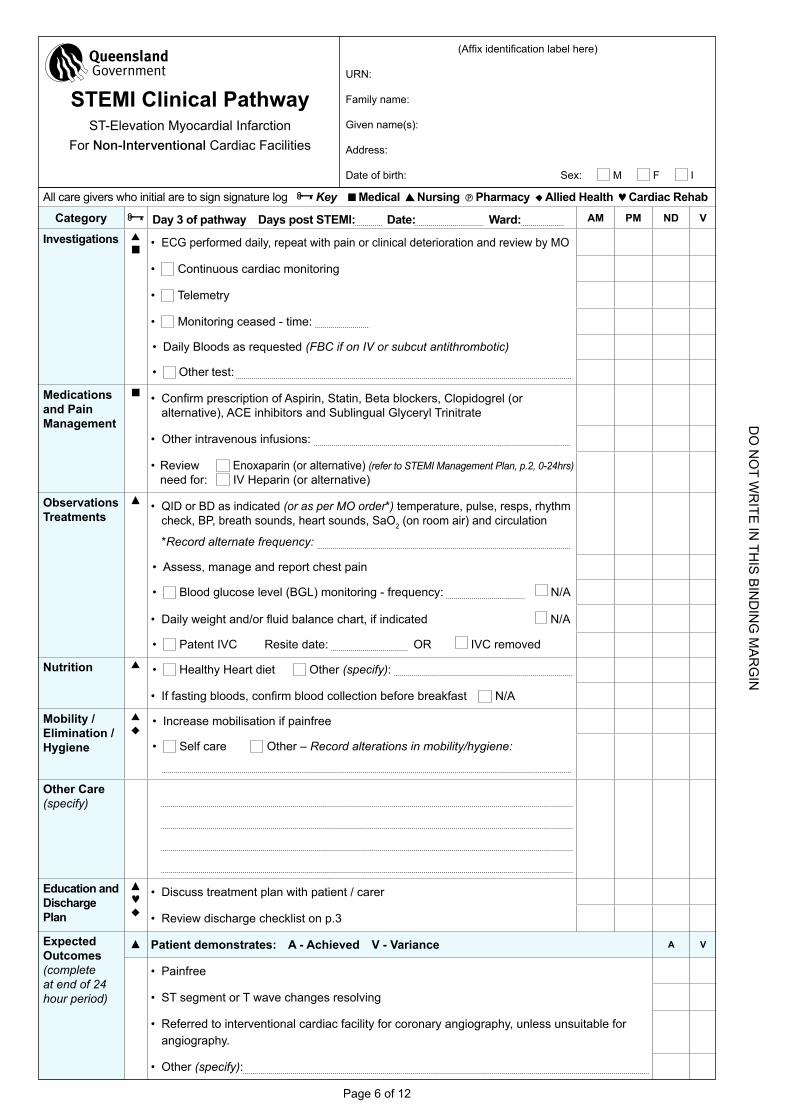
All care givers who initial are to sign signature log Key Medical Nursing Pharmacy Allied Health Cardiac Rehab
Category Day 3 of pathway Days post STEMI: Date: Ward: AM PM ND V
Investigations • ECG performed daily, repeat with pain or clinical deterioration and review by MO
• Continuous cardiac monitoring
• Telemetry
• Monitoring ceased - time:
• Daily Bloods as requested (FBC if on IV or subcut antithrombotic)
• Other test:
Medications and Pain Management
• ConfirmprescriptionofAspirin,Statin,Betablockers,Clopidogrel(oralternative), ACE inhibitors and Sublingual Glyceryl Trinitrate
• Other intravenous infusions:
•Review need for:
Enoxaparin (or alternative) (refer to STEMI Management Plan, p.2, 0-24hrs) IV heparin (or alternative)
Observations Treatments
• QID or BD as indicated (or as per MO order*) temperature, pulse, resps, rhythm check, BP, breath sounds, heart sounds, SaO2 (on room air) and circulation
*Record alternate frequency:
• Assess, manage and report chest pain
• Blood glucose level (BGL) monitoring - frequency: N/A
• Dailyweightand/orfluidbalancechart,ifindicated N/A
• Patent IVC Resite date: OR IVC removed
Nutrition • healthy heart diet Other (specify):
• Iffastingbloods,confirmbloodcollectionbeforebreakfast N/A
Mobility / Elimination / Hygiene
• Increase mobilisation if painfree
• Self care Other – Record alterations in mobility/hygiene:
Other Care(specify)
Education and Discharge Plan
• Discuss treatment plan with patient / carer
• Review discharge checklist on p.3
Expected Outcomes(complete at end of 24 hour period)
Patient demonstrates: A - Achieved V - Variance A V
• Painfree
• ST segment or T wave changes resolving
• Referred to interventional cardiac facility for coronary angiography, unless unsuitable for angiography.
• Other (specify):
(Affixidentificationlabelhere)
URN:
Family name:
Given name(s):
Address:
Date of birth: Sex: M F I
STEMI Clinical PathwayST-Elevation Myocardial Infarction
For Non-Interventional Cardiac Facilities

DO
nO
t wr
ite in
this
bin
Din
g m
ar
gin
DO
nO
t w
rit
e in
th
is b
inD
ing
ma
rg
inÌSW
043b
\Îv5
.00
- 0
2/20
12m
at. n
o.: 1
0217
515
sw
043b
Page 7 of 12
All care givers who initial are to sign signature log Key Medical Nursing Pharmacy Allied Health Cardiac Rehab
Category Day 4 of pathway Days post STEMI: Date: Ward: AM PM ND V
Investigations • ECG performed daily, repeat with pain or clinical deterioration and review by MO
• Continuous cardiac monitoring
• Telemetry
• Monitoring ceased - time:
• Daily Bloods as requested (FBC if on IV or subcut antithrombotic)
• Other test:
Medications and Pain Management
• ConfirmprescriptionofAspirin,Statin,Betablockers,Clopidogrel(oralternative), ACE inhibitors and Sublingual Glyceryl Trinitrate
• Other intravenous infusions:
•Review need for:
Enoxaparin (or alternative) (refer to STEMI Management Plan, p.2, 0-24hrs) IV heparin (or alternative)
Observations Treatments
• QID or BD as indicated (or as per MO order*) temperature, pulse, resps, rhythm check, BP, breath sounds, heart sounds, SaO2 (on room air) and circulation
*Record alternate frequency:
• Assess, manage and report chest pain
• Blood glucose level (BGL) monitoring - frequency: N/A
• Dailyweightand/orfluidbalancechart,ifindicated N/A
• Patent IVC Resite date: OR IVC removed
Nutrition • healthy heart diet Other (specify):
• Iffastingbloods,confirmbloodcollectionbeforebreakfast N/A
Mobility / Elimination / Hygiene
• Increase mobilisation if painfree
• Self care Other – Record alterations in mobility/hygiene:
Other Care(specify)
Education and Discharge Plan
• Discuss treatment plan with patient / carer
• Review discharge checklist on p.3
Expected Outcomes(complete at end of 24 hour period)
Patient demonstrates: A - Achieved V - Variance A V
• Painfree
• ST segment or T wave changes resolving
• Referred to interventional cardiac facility for coronary angiography, unless unsuitable for angiography.
• Other (specify):
(Affixidentificationlabelhere)
URN:
Family name:
Given name(s):
Address:
Date of birth: Sex: M F I
STEMI Clinical PathwayST-Elevation Myocardial Infarction
For Non-Interventional Cardiac Facilities
DO
nO
t wr
ite in
this
bin
Din
g m
ar
gin
DO
nO
t w
rit
e in
th
is b
inD
ing
ma
rg
inÌSW
043b
\Îv5
.00
- 0
2/20
12m
at. n
o.: 1
0217
515
sw
043b
Page 8 of 12
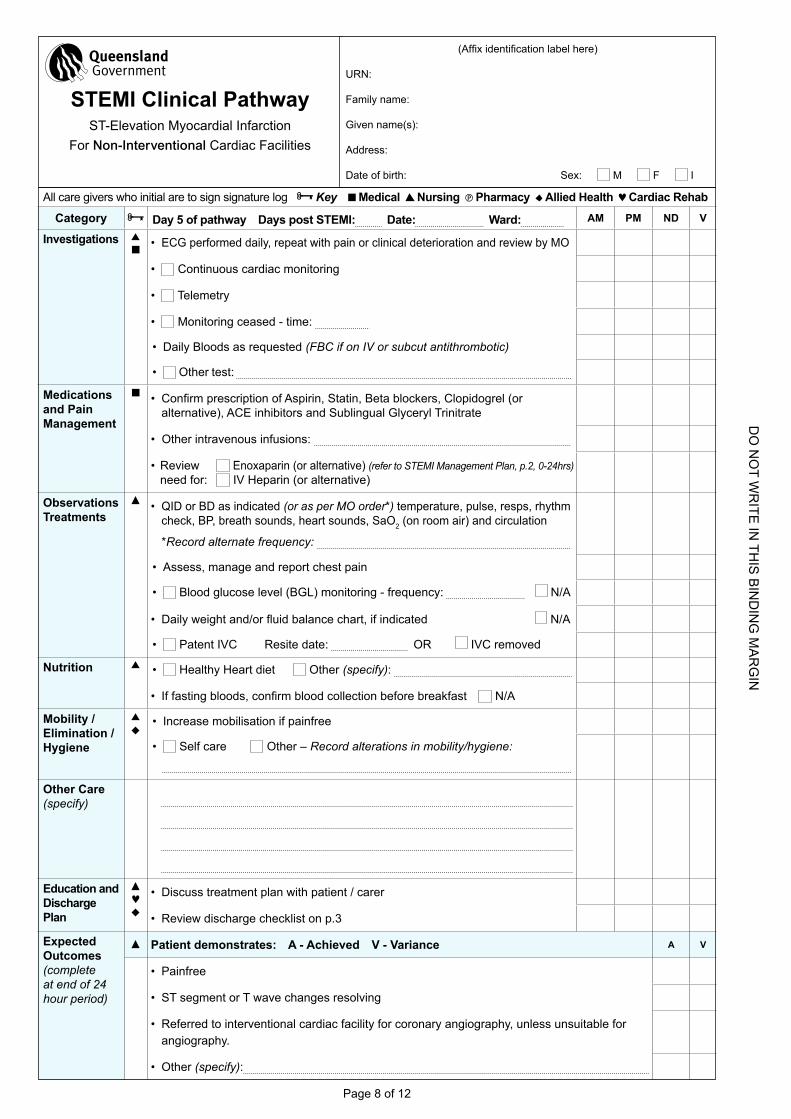
All care givers who initial are to sign signature log Key Medical Nursing Pharmacy Allied Health Cardiac Rehab
Category Day 5 of pathway Days post STEMI: Date: Ward: AM PM ND V
Investigations • ECG performed daily, repeat with pain or clinical deterioration and review by MO
• Continuous cardiac monitoring
• Telemetry
• Monitoring ceased - time:
• Daily Bloods as requested (FBC if on IV or subcut antithrombotic)
• Other test:
Medications and Pain Management
• ConfirmprescriptionofAspirin,Statin,Betablockers,Clopidogrel(oralternative), ACE inhibitors and Sublingual Glyceryl Trinitrate
• Other intravenous infusions:
•Review need for:
Enoxaparin (or alternative) (refer to STEMI Management Plan, p.2, 0-24hrs) IV heparin (or alternative)
Observations Treatments
• QID or BD as indicated (or as per MO order*) temperature, pulse, resps, rhythm check, BP, breath sounds, heart sounds, SaO2 (on room air) and circulation
*Record alternate frequency:
• Assess, manage and report chest pain
• Blood glucose level (BGL) monitoring - frequency: N/A
• Dailyweightand/orfluidbalancechart,ifindicated N/A
• Patent IVC Resite date: OR IVC removed
Nutrition • healthy heart diet Other (specify):
• Iffastingbloods,confirmbloodcollectionbeforebreakfast N/A
Mobility / Elimination / Hygiene
• Increase mobilisation if painfree
• Self care Other – Record alterations in mobility/hygiene:
Other Care(specify)
Education and Discharge Plan
• Discuss treatment plan with patient / carer
• Review discharge checklist on p.3
Expected Outcomes(complete at end of 24 hour period)
Patient demonstrates: A - Achieved V - Variance A V
• Painfree
• ST segment or T wave changes resolving
• Referred to interventional cardiac facility for coronary angiography, unless unsuitable for angiography.
• Other (specify):
(Affixidentificationlabelhere)
URN:
Family name:
Given name(s):
Address:
Date of birth: Sex: M F I
STEMI Clinical PathwayST-Elevation Myocardial Infarction
For Non-Interventional Cardiac Facilities

DO
nO
t wr
ite in
this
bin
Din
g m
ar
gin
DO
nO
t w
rit
e in
th
is b
inD
ing
ma
rg
inÌSW
043b
\Îv5
.00
- 0
2/20
12m
at. n
o.: 1
0217
515
sw
043b
Insert additional days here if applicable.
DO
nO
t wr
ite in
this
bin
Din
g m
ar
gin
DO
nO
t w
rit
e in
th
is b
inD
ing
ma
rg
inÌSW
043b
\Îv5
.00
- 0
2/20
12m
at. n
o.: 1
0217
515
sw
043b
Page 10 of 12
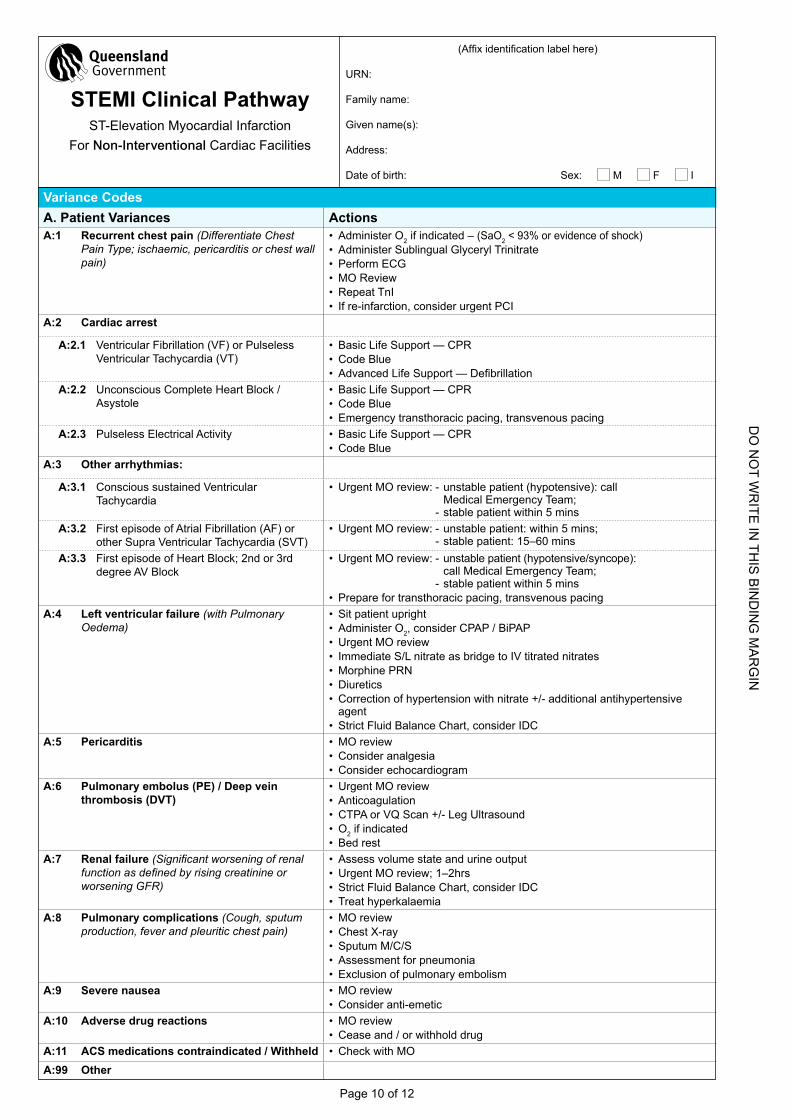
Variance CodesA. Patient Variances ActionsA:1 Recurrent chest pain (Differentiate Chest
Pain Type; ischaemic, pericarditis or chest wall pain)
•Administer O2 if indicated – (SaO2 < 93% or evidence of shock)•Administer Sublingual Glyceryl Trinitrate•Perform ECG •MO Review•Repeat TnI• If re-infarction, consider urgent PCI
A:2 Cardiac arrest
A:2.1 Ventricular Fibrillation (VF) or Pulseless Ventricular Tachycardia (VT)
•Basic Life Support — CPR•Code Blue• AdvancedLifeSupport—Defibrillation
A:2.2 Unconscious Complete heart Block / Asystole
•Basic Life Support — CPR•Code Blue•Emergency transthoracic pacing, transvenous pacing
A:2.3 Pulseless Electrical Activity •Basic Life Support — CPR•Code Blue
A:3 Other arrhythmias:
A:3.1 Conscious sustained Ventricular Tachycardia
•Urgent MO review: - unstable patient (hypotensive): call Medical Emergency Team; - stable patient within 5 mins
A:3.2 First episode of Atrial Fibrillation (AF) or other Supra Ventricular Tachycardia (SVT)
•Urgent MO review: - unstable patient: within 5 mins; - stable patient: 15–60 mins
A:3.3 First episode of heart Block; 2nd or 3rd degree AV Block
•Urgent MO review: - unstable patient (hypotensive/syncope): call Medical Emergency Team; - stable patient within 5 mins
•Prepare for transthoracic pacing, transvenous pacingA:4 Left ventricular failure (with Pulmonary
Oedema)•Sit patient upright•Administer O2, consider CPAP / BiPAP•Urgent MO review• Immediate S/L nitrate as bridge to IV titrated nitrates•Morphine PRN •Diuretics•Correction of hypertension with nitrate +/- additional antihypertensive
agent•Strict Fluid Balance Chart, consider IDC
A:5 Pericarditis •MO review•Consider analgesia•Consider echocardiogram
A:6 Pulmonary embolus (PE) / Deep vein thrombosis (DVT)
•Urgent MO review•Anticoagulation•CTPA or VQ Scan +/- Leg Ultrasound•O2 if indicated•Bed rest
A:7 Renal failure (Significant worsening of renal function as defined by rising creatinine or worsening GFR)
•Assess volume state and urine output•Urgent MO review; 1–2hrs•Strict Fluid Balance Chart, consider IDC• Treat hyperkalaemia
A:8 Pulmonary complications (Cough, sputum production, fever and pleuritic chest pain)
•MO review•Chest X-ray•Sputum M/C/S•Assessment for pneumonia•Exclusion of pulmonary embolism
A:9 Severe nausea •MO review•Consider anti-emetic
A:10 Adverse drug reactions •MO review•Cease and / or withhold drug
A:11 ACS medications contraindicated / Withheld •Check with MO
A:99 Other
(Affixidentificationlabelhere)
URN:
Family name:
Given name(s):
Address:
Date of birth: Sex: M F I
STEMI Clinical PathwayST-Elevation Myocardial Infarction
For Non-Interventional Cardiac Facilities
DO
nO
t wr
ite in
this
bin
Din
g m
ar
gin
DO
nO
t w
rit
e in
th
is b
inD
ing
ma
rg
inÌSW
043b
\Îv5
.00
- 0
2/20
12m
at. n
o.: 1
0217
515
sw
043b
Page 11 of 12
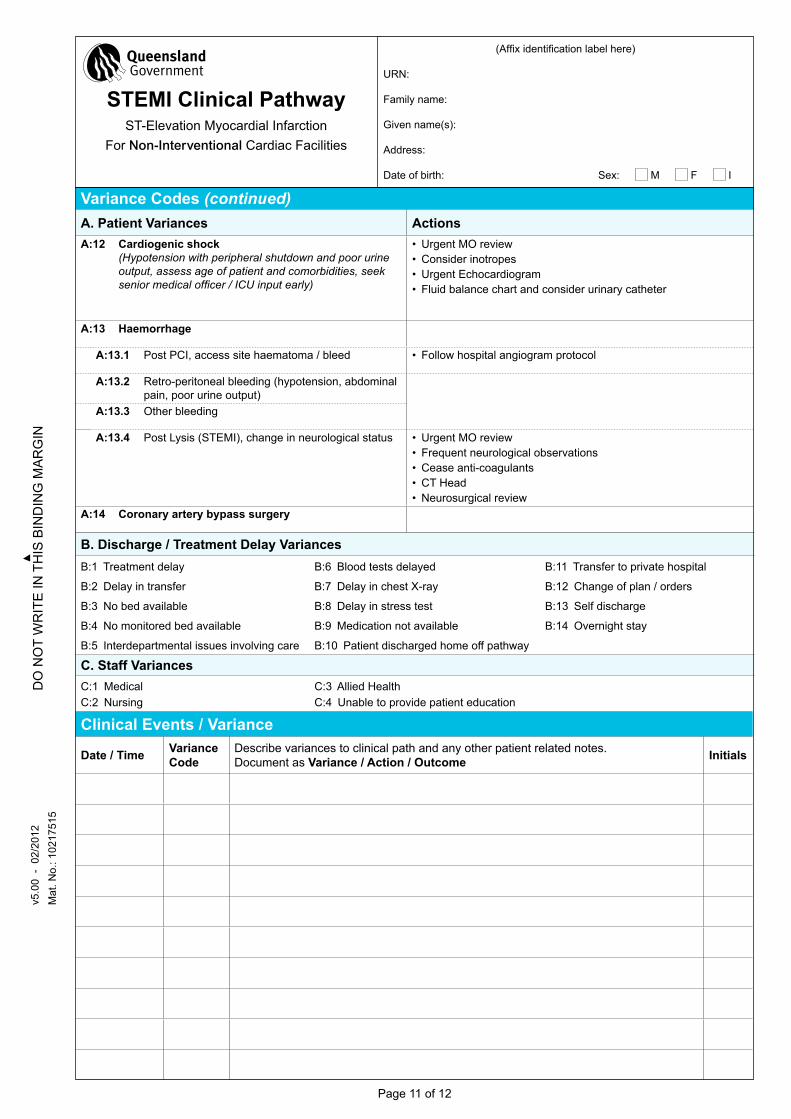
Variance Codes (continued)A. Patient Variances ActionsA:12 Cardiogenic shock
(Hypotension with peripheral shutdown and poor urine output, assess age of patient and comorbidities, seek senior medical officer / ICU input early)
•Urgent MO review•Consider inotropes•Urgent Echocardiogram• Fluid balance chart and consider urinary catheter
A:13 Haemorrhage
A:13.1 Post PCI, access site haematoma / bleed • Follow hospital angiogram protocol
A:13.2 Retro-peritoneal bleeding (hypotension, abdominal pain, poor urine output)
A:13.3 Other bleeding
A:13.4 Post Lysis (STEMI), change in neurological status •Urgent MO review• Frequent neurological observations•Cease anti-coagulants•CT head•Neurosurgical review
A:14 Coronary artery bypass surgery
B. Discharge / Treatment Delay VariancesB:1 Treatment delay
B:2 Delay in transfer
B:3 No bed available
B:4 No monitored bed available
B:5 Interdepartmental issues involving care
B:6 Blood tests delayed
B:7 Delay in chest X-ray
B:8 Delay in stress test
B:9 Medication not available
B:10 Patient discharged home off pathway
B:11 Transfer to private hospital
B:12 Change of plan / orders
B:13 Self discharge
B:14 Overnight stay
C. Staff VariancesC:1 Medical C:2 Nursing
C:3 Allied health C:4 Unable to provide patient education
Clinical Events / Variance
Date / Time Variance Code
Describe variances to clinical path and any other patient related notes.Document as Variance / Action / Outcome Initials
(Affixidentificationlabelhere)
URN:
Family name:
Given name(s):
Address:
Date of birth: Sex: M F I
STEMI Clinical PathwayST-Elevation Myocardial Infarction
For Non-Interventional Cardiac Facilities
DO
nO
t wr
ite in
this
bin
Din
g m
ar
gin
DO
nO
t w
rit
e in
th
is b
inD
ing
ma
rg
inÌSW
043b
\Îv5
.00
- 0
2/20
12m
at. n
o.: 1
0217
515
sw
043b
Page 12 of 12
Clinical Events / Variance (continued)
Date / Time Variance Code
Describe variances to clinical path and any other patient related notes.Document as Variance / Action / Outcome Initials
(Affixidentificationlabelhere)
URN:
Family name:
Given name(s):
Address:
Date of birth: Sex: M F I
STEMI Clinical PathwayST-Elevation Myocardial Infarction
For Non-Interventional Cardiac Facilities