ursodeoxycholic acid (udca), a hydrophilic bile acid, is concentrated in the water soluble fraction...
TRANSCRIPT
April 1995 Biliary Disorders A405
• SPHINCTEROTOMY FOR AN EMPTY DUCT?.. AB Ballinger, E Barnes, EM Alstead, PD Fairclough. Digestive Diseases Research Centre, St Bartholomew's Hospital, London, UK.
Laparoscopic cholecystectomy has become the routine treatment modality for patients with symptomatic gallstones. Preoperative endoscopic retrograde cholangiography (ERC) is performed in patients with clinical, biochemical or radiological indicators of choledocholithiasis. Sphincterotomy is undertaken in patients with common bile duct (CBD) stones on cholangiogram However, it is not known if sphincterotomy should be performed if the cholangiogram show no stones. In a retrospective review of 1469 consecutive ERCP records 336 patients were suspected (transient jaundice, increased alkaline phosphatase or dilated ducts on ultrasound), prior to ERCP, to have CBD stones. Patients with acute pancreatitis were excluded from this study. In 76 patients (23%) CBD stones were not found on ERC and sphincterotomy was not performed. The clinical course after ERC has been documented by review of the hegpital records and by a questionnaire sent to the patients and their GPs. In 14 patients (18%) follow up was inadequate and the remaining 62 patients are the basis of this study. There were 32 women and the mean age was 64 years (range 23 - 92). At the onset of illness median serum alkaline phosphatase was 193 iU/L (interquartile range 146-296) and it was > 250iU/L in 20 patients (32%). The bile duct was dilated (>8mm) on ultrasound examination in 22 (35%) patients. During follow up, (median 24 months [interquartile range 9-31]) 38 patients have had a cholecystectomy and 10 are on the waiting list. There have been no further complications of gallstones and only two (3%) patients have subsequently been found to have CBD stones. Both patients were asymptomatic at the time and stones were found on operative cbolangiogram. In one, cholecystectomy was 13 months al~er ERCP and CBD stones may well have developed after the original illness. In conclusion, two year follow up suggests that if the ERC shows no stones sphincterotomy in unnecessary in most patients.
SCLEROSING CHOLANGITIS AS RISK FACTOR FOR GASTRO- INTESTINAL CANCER. Pradeen BansaL Amnon Sonnenberg. VA Medical Center and The Medical College of Wisconsin, Milwaukee, WI.
Background: While studying the epidemiologic association between inflammatory bowel disease and colorectal cancer, it was noticed that presence of sclerosing cholangitis represented a general risk factor for gastrointestinal cancer even in the absence of inflammatory bowel disease. Methods: The present investigation tested the association of sclerosing cholangitis with esophageal, gastric, small intestinal, and colorectal cancer. Bronchopu!monary and renal cancer, as well as cancer of the urinary bladder were used for comparison. The comorbid occurrences of sclerosing cholangitis and various cancer types were analyzed in the population of 3.41 million military veterans who were discharged from VA hospitals distributed throughout the US between 1981 and 1993. Comorbidity was calculated as the ratio between the observed and expected number of hospitalized veterans with sclerosing cholangitis plus cancer. A 95% Confidence interval was calculated based on the Poisson distribution of the observed number of patients with comorbidity. Results: In the veterans population from 1981 to 1993, 2330 individuals with sclerosing cholangitis were found, 15644 with esophageal cancer, 12110 with gastric cancer, 1745 with cancer of the small intestine, 52620 with colorectal cancer, 159154 with broncho- pulmonary cancer, 12439 with renal cancer, and 26566 with cancer of the urinary bladder. The ratio of their comorbid occurrence with sclerosing cholangitis was 1.09 (0.58-1.87) for esophageal cancer, 4.15 (2.95- 5.67) for gastric cancer, 12.91 (7.52-20.67) for cancer of the small intestine, 2.01 (1.60-2.49) for colorectal cancer, 0.53 (0.41-0.68) for bronchopulmonary cancer, 1.69 (0.97-2.75) for renal cancer, and 0.76 (0.44-1.24) for cancer of the urinary bladder. Compared with the expected mortality of each individual cancer type, the increase in mortality by the comorbid occurrence of sclerosing cholangitis was 1.57 (0.51- 3.65) for esophageal cancer, 10.42 (6.75-15.39) for gastric cancer, 44.43 (22.96-77.61) for cancer of the small intestine, 6.20 (4.56-8.25) for colorectal cancer, 1.34 (0.95-1.83) for bronchopulmonary cancer, 3.84 (1.41-8.36) for renal cancer, and 3.30 (1.58-6.07) for cancer of the urinary bladder. Conc lus ions : Sclerosing cholangitis represents a significant risk factor for the occurrence of gastric, small intestinal, and colorectal cancer. Moreover, the presence of sclerosing cholangitis is associated with an increased cancer-related mortality. Such risks do not apply to esophageal cancer or much less to cancers affecting extra- intestinal organs.
• MECltANISM OF BOTULINUM TOXIN A EFFECT ON TIlE SPHINCI'ER OF ODDL SA Barnes. A Nakeeb, TH Magnuson, PJ Pasricha, AN Kalloo, PA Lipsett, HA Pitt, and KD LiHomoe. Departments of Surgery and Gastroenterology, The Johns Hopkins Medical Institutions, Baltimore, MD.
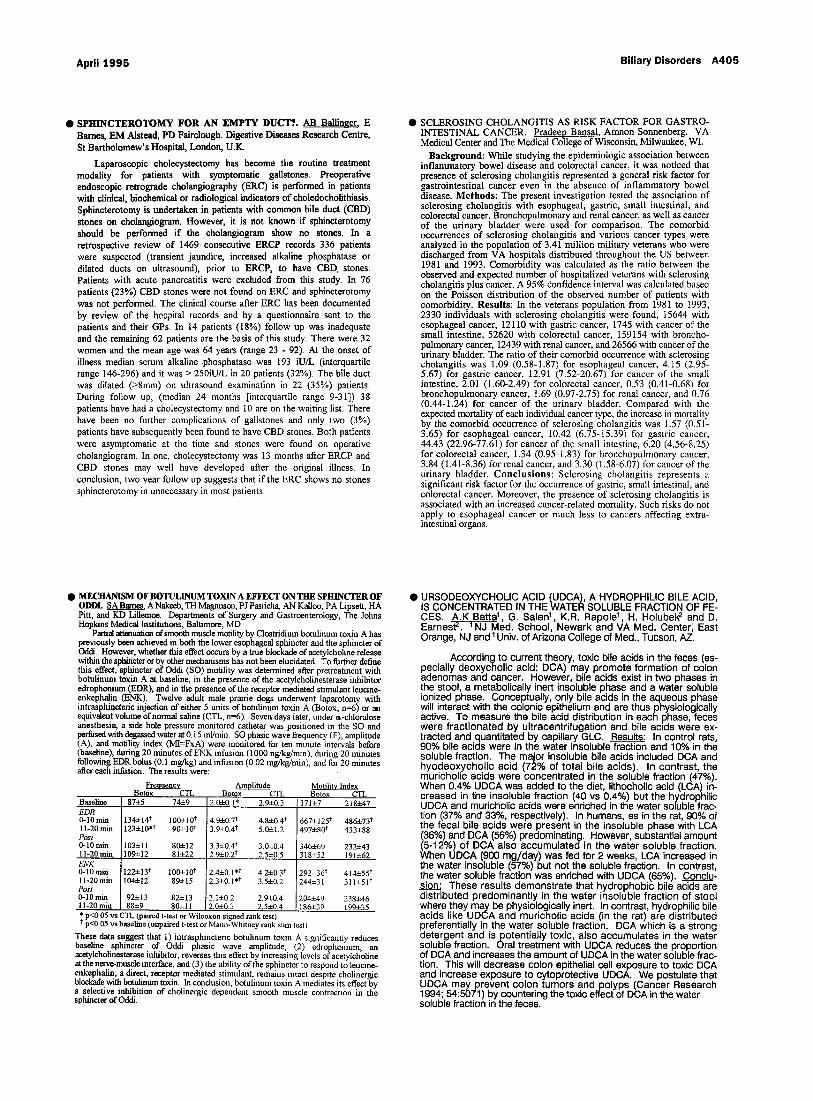
Partial attenuation of smooth muscle motility by Clostridium botulinum toxin A has previously bean achieved in both the lower esophageal sphincter and the sphincter of Oddi. However, whether this effect occurs by a true blockade of acetyleholine release within the sphincter or by other mechanisms has not been elucidated. To further define this effect, sphincter of Oddi (SO) motility was determined after pretreatmant with hotulinum toxin A at baseline, in the presence of the acetylcholinesterase inhibitor edrophonium (EDK), and in the presence of the receptor mediated stimulant leucine- enkephalin (ENK). Twelve adult male prairie dogs underwent laparotomy with intrasphinctoric injection of either 5 units of botulinum toxin A (Botox, n=6) or an equivalent volume of normal saline (CTL, n=6). Seven days later, under a-chloralose anesthesia, a side hole pressure monitored catheter was positioned in the SO and perfused with degassed water at 0.15 ml/min. SO phasic wave frequency (F), amplitude (A), and motility index (MI=FxA) were monitored for ten rmnute intervals before (baseline), during 20 minutes Of ENK infusion (1000 ng/kg/min), during 20 nunutes following BDR bolus (0.1 mg/kg) and infusion (0.02 mg/kg/min), mad for 20 minutes aider each infusion. The results were:
Baseline 87±5 74±9 EDR 0-10 mm 11-20 min Post 0-10 rain 11-20 rain ENK 0-10 rain 11-20 min Post 0-10 rain 11-20 min
Frequency Amplitude Motility Index Botox CTL Botox CTL Botox CTL
2.0±0.l* 2.9a:0.3 171:t:7 218±47
134±141- 100-J:10 ? 123±10.? 90-a:10 t
103±11 80a:12 109-a:12 81±22
122.a:131- 100±10 t 104.412 89-2=15
92~13 82±13 88±9 80=11
4.9±0.7 ? 4.8±0.4 ? 3.9f-0.47 5.0~1.2
3.3±0.4 ? 3.0~0.4 2.9-x0.21- 2.5±0.5
2.4±0.1"* 4.2±0.3 ? 2.3:i:0.1.1- 3.5±0.2
2. I:i:0.2 2.9a:0.4 2.0i-0.3 2.5±0.4
667±1251- 486±73 ? 497±80 ? 433±88
346~69 232~43 318±52 191~62
292±36 ? 414±55 ? 244±31 311±51 ?
204±49 238±46 186±39 199±35
* p<0.05 vs CTL (paired t-test or Wilcoxon signed rank test) 1- p<0.05 vs baseline (unpaired t-test or Maml-Whitney rank sum test)
These data suggest that 1) intrasphincteric botulinum toxin A significantly reduces baseline sphincter of Oddi phasic wave amplitude. (2) edrophonium, an acetyleholinast0rase inhibitor, reverses this effect by increasing levels of acetylcholine at the nerve-muscle interface, and (3) the ability of the sphincter to respond to lancine- enkephalin, a direct, receptor mediated stimulant, remains intact despite cholinergie blockade with batulinum toxin. In conclusion, botulinum toxin A mediates its effect by a selective inhibition of cholinergic dependent smooth muscle contractmn in the sphincter of Oddi.
• URSODEOXYCHOLIC ACID (UDCA), A HYDROPHILIC BILE ACID, IS CONCENTRATED IN THE WATER SOLUBLE FRACTION OF FE- CES. A.K Batta 1 , G. Salen 1, K.R. Rapole ~ , H. Holubek 2 and D. Earnest ~. ~NJ Med. School, Newark and VA Med. Center, East Orange, NJ and ~ Univ. of Arizona College of Med., Tucson, AZ.
According to current theory, toxic bile acids in the feces (es- pecially deoxycholic acid; DCA) may promote formation of colon adenomas and cancer. However, bile acids exist in two phases in the stool, a metabolically inert insoluble phase and a water soluble ionized phase. Conceptually, only bile acids in the aqueous phase will interact with the colonic epithelium and are thus physiologically active. To measure the bile acid distribution in each phase, feces were fractionated by ultracentrifugation and bile acids were ex- tracted and quantitated by capillary GLC. Results: In control rats,
o Q 90~ bile acids were in the water insoluble fraction and 10~ in the soluble fraction. The major insoluble bile acids included DCA and hyodeoxycholic acid (72% of total bile acids). In contrast, the muricholic acids were concentrated in the soluble fraction (47%). When 0.4% UDCA was added to the diet, lithocholic acid (LCA) in- creased in the insoluble fraction (40 vs 0.4%) but the hydrophilic UDCA and muricholic acids were enriched in the water soluble frac- tion (37% and 33%, respectively), tn humans, as in the rat, 90% of the fecal bile acids were present in the insoluble phase with LCA (36%) and DCA (56%) predominating. However, substantial amount (5-12%) of DCA also accumulated in the water soluble fraction. When UDCA (900 mg/day) was fed for 2 weeks, LCA increased in the water insoluble (57%) but not the soluble fraction. In contrast, the water soluble fraction was enriched with UDCA (65%). Conclu- sion: These results demonstrate that hydrophobic bile acids are distributed predominantly in the water insoluble fraction of stool where they may be physiologically inert. In contrast, hydrophilic bile acids like UDCA and muricholic acids (in the rat) are distributed preferentially in the water soluble fraction. DCA which is a strong detergent and is potentially toxic, also accumulates in the water soluble fraction. Oral treatment with UDCA reduces the proportion of DCA and increases the amount of UDCA in the water soluble frac- tion. This will decrease colon epithelial cell exposure to toxic DCA and increase exposure to cytoprotective UDCA. We postulate that UDCA may prevent colon tumors andpolyps (Cancer Research 1994; 54:5071) by countering the toxic effect of DCA in the water soluble fraction in the feces.