usaarl report' no. '71-22 - dtic.mil · usaarl report no. 71-22 the neurological effects...
TRANSCRIPT
2 00 AD_ _
0
USAARL REPORT' NO. '71-22
THE NEUROLOGICAL EFFtIXTS OF INH
BY
MAJ J. E. Jordan,. MCMr. 2Stephen Shields
Mr. Dan Bochneak
jc, December 1971
U. S. ARMIY AEROMEDICAL RESEARCH LABORATORY
Fort Rucker, Alabama
. NA'flIiIAL TECHNICAL
IPINV") ',%AATION SERVICE ,
NOTICE
Qualified requesters may obtain'copies from rhe Defense Documentation,Center (DDý), Camern, Station, Alexandria, Virginia. Orders-,will'beexpedited if placed through the librarian or owaer person designated A
to .request documents from DDC (formerly ASTIA).
Change of Address 4
Organization receiving reports from the USArmy Aeromedical ResearchLaboratory on automatic .iailing lists should confirm correct address.when corresponding about laboratory reports.
Disposition
Destroy this report when it is no longer needed. ,Do not returnit tothe originator.
Distribution Statement
This-document has been approved for public release and-sale; its dis-tribution is unlimited.
Disclaimer
The findings• inthis report arc nbt to be construed as, an oificial De-partment cf the-Army -position. .unles so designated- by other authorized-documents.
r .. .

"l•, :,S.• :Army.:Aeromed£cal Research Laboratory •.ou•Unc!assAf+ed'
-,,•b9 Ndurological• Effects-pf' INH
(. O•SC m P T, V • NO'r!S (PYPe.of •'•#m'l •md l.€lusl•e dlies) " *
_Paper for publication
J,'. E, .jORDAN, .H•., MC
Stephen ShieldsDan Bochneak
e, Rs'I•OFIT DAT[ " ' ?,. TOTAL, ,O.'OIr I)AGZ$ [7b; N•O;-O'F'•*•I)
December 1971 ..... 106 [ ],07S141. CONTRACT OR GRANT NO. I•h ORIGINATOP)I •IKPORT NUFA'I•FiR{I|
•. p.o;•c,,o. 3A0 6211 0A 819 ;[: 71-22
this •por0
d.•to, 0iSv•,UVION SVAV:•:NV
This< document has been approved for public rei'ease and sale; its distribu:ion isunlimited. ]
''.'$UPPLKEAENTAY NOTE. ll. 2. |PON$OING MII-ITAY ACTIVITY
US Army Medical R&D Command
Washington, D. C. 20314
il3/ A• TRACT ,. ........ i
INH was given for one year to a group of 28•,volunteer civilian aviators. Neuro- [logical examinations) mental status examinations, EEG's and visual evoked poten-tials uere monitored at control) Six months and twelve months. Hinor changes were [observed in all the measures; none of these changes were •evere enough to be o•great concern. No evidence was found to Justify restriction of flying during inn
administration, although the results of this study suggest that careful moniteria5of patients taking INH is indicated.
D• • •473 IlllPl'&€lllDl•[•Olllit14711'lJANi•4'11Hl!=HIll) 0, oo•oL•vi{ •)o• -mw u•z. Unclassified

'Unclassified,Security-Clussification
14; LINK 'A" LINK S LIN C
K RL T . R O L E I ' O L E WT 4
INHVitamin 'B6Neurological Examination .•
Mental Status Examination IElectroencephalograph ,V.isual Evoked Potentials &6Aviators
Neuropathy
UcsiI
ii
S... I~ II I II -2 .. . .• :-- ... . ... .---SUnclasifle
AD _ - __
USAARL REPORT NO. 71-22
THE NEUROLOGICAL EFFECTS OF ,INH'
-BY-
MAJ J. E. Jordan, MCMr. Stephen Shields
Mr. Dan Bochneak
December 1971
U. S. ARMY AEROMEDICAL RESEARCH LABORATORY
Fort Rucker, Alabama
U. S. Army Medical Research -afid Development Command
P)ibLribution Statement: This document has been approvedi for public re-lease and sale; its distribution is unlimited.
-1/

"ABTRACT'
INH was given for one year to a group of 28 volunteer civilianaviators. Neurological examinations, mental status, examinations, EEG'sand' visual evoked potentials were monitored at control, six months andtwelve mbnths. Minor changes were observed in all the measures; none,of these changes were severe enough to be of great concern. No evidencewas found to justify restriction of flying during INH administration,although the results of this study suggest that careful monitoring ofpatients taking INH is indicated.
-APPR6VED.. ROBERTAM "A.-WtColonel, MSCW. BCommanding
I-

ACKNOWLEDGMENTS "1
Special thanks goes to Dr. Andrew S. Martin for invaluable assistancein statistidal analysis of the data and for many hours spent in ,criticalreview'of the manuscript.
The authors also w sh to express grateful appreciation to ,Mrs. J4aniceSpeigner for typing the manuscript and 'to Mr. David Morris for assistancein data. analysis.

tA3LU`QF- CONTENTS:
INTRODUCTION . . .. . . . . ... . . . .. .. .
Subjects ........... .......... . . . .. . . . 1Experimental Design 2. • ... .... .
LITERATURE REVIEW . ..... . . ................ 2
STUDY 1 - NEUROLOGICAL EXAMINATION AND CLINICAL NEUROLOGICALEXAMINAT ION . ... 22
rocedure ... .. .. .. .. . 22
History . .. .. . . . . . . . . 222
Neurological'Examination . ............ ..... 22
Data Analysis............... . .............. . . . . 23"
Results .. ....... . . . . . . . . . ......... .... . . 94
History . . . . . . . . . . . ....... .. . . . .24
Autonomic Nervous System Function . .. .......... .. 24Reflexes . . . .... ..... .... . . . . . . . 24'Sensory Nervous System Function........... ...... . . . 2bCranial Nerve Function. . . . . . . ...... .... .. . . . 26Muscle Power . . . . . . .. .. ............ .... . 26Functional Tests . . . ...................... 27Cerebellar Function . .. ........ .27
Gai t ........... . . .......... .... 27.. .nwr .tin. ..g . . . 27
Ijiscussion ......... ....................... ... .. .. . . . . 32
Summary. . .. ....... . 37
STUDY 2 - MENTAL STATUS EXAMIIATION ............................. 30
Procedure .. ....... . .. .. ................... .9
'Serial Subtraction... .... ... ...... . ... .. 39Oral Recall, . . . . . . . . . . . . 39Judgment . .. . . . ................ 39
Results ..... ... . . . . . .. . . . 39
Seirial Subtraction 39'Oral R Scall . . . . . . . . . .. . .. 31Judginent . . . . . . . . ., . . . . . . 4
Discussion . • . . . .. .. . . • . .. . ... 41
STUDY 3 - ELECTROENCEPHALOGRAPHIC EXAMINATION . . .. . . ....... 43
Phase 2 .. .. .. . . .. . . .. . .. . . . . . . . *. . o . . . . 47Chlin ia. ........................................ 48
Phsubcinca.. .. .. ... . ....... . . . . ... .. .. .. .... 50Apparatus and Procedure........... . . . . . . . . 6048
DtAnialysis . . . .y. . . . ........ ..... 64
Phsebl ni .. .. . . . . . . . *I. . . .. . .. . . . .4 . . . .. .. . 50
Reasults .............................. 62Discussion . . . . . . . . . . . . . . . . . . . . ... . .. 69
DscussiYNDonC................ ..... *.. ...... 71
STUDY 4- VISUAL EVOKED POTENTIAL ... . . .. . .. .... 60
Method . . . . . . . . . ..... . . . .. .. . . . . . . . . . 60
Apparatus and Procedure ............... 60Data Analysis . . . . . . . . . ... . ...... . . . . . . 61
Results ... . . . . . . . . . . . . . . . . . . . . .. . .. . 62
Discussion . . ... . . . . . . 0.. 0. . . . . .. . . . .. . . 69
S U*11ARY 0ZD CONCLUSIONS o.. ..... .. . ... ....... 71
REFERENCES ..o . .. . . . . . . . . . . . .. . ... . . . . .. . 72

LIST OF TABLES AND FIGURES
Page
TABLE 1 - Reported Side Effects of INH . . . . . . . . . . . . . 14
TABLE 2 - Summary of Selected Case Histories With an Overdoseof INH . . . . . . . . . . . . . . . ....... . .. . '18
TABLE 3 - Neurological-Symptoms .. ............ . 25
TABLE 4 - Neurological Findings .d.g. ......... .. .. . . 28
TABLE 5 - Multiple System Involvement . ...... . . . ... 31.
TABLE 6 - Time of Appearance of Neurological Findings and*Symptoms .0.. . .. . .. . . . . . . 3
TABLE 7 - Statistical Analysis of Mental Status Test . . . . . 40
FIGURE 1A - Well Developed Alpha o . . . . . .... . . . . . . . . 44
FIGURE-iB - Other Alpha ................... .. . 45
FIGURE 2 - Paroxysmal Bursts of Subject ............. . . . .49'
TABLE 8 - Changes in EEG Parameters .............. . 51
TABLE 9 - Parameter Shifts . ............................ . 55
TABLE 10 - Zhanges in EEG, Parameters by Area ..... . . . . . 5
1ABLE 11 - Visual Evoked Potentials . ....... .... . . . 03
-----------

,7 APPENDICES
APPENDtX I - Summary of Clinical Signs and Symptoms..,..8.
,APfitNDIX 2 - S~unýiary of Analysis of Variance - SerialS'ubtraction- Score ............... ... 82
APPENDIX 3 - Summary of Aaalysis of Variance - SerialSubtracion - Total Time .... ........... . . . .. 82
APPENDIX +4 - Summary of Analysis of Variance - Oral Recall -Score .......... ..... ......... ......... 83
APPENDIX 5 - Tests on )ifferencec Between Totals - Oral Recall -Score .... ....................... ........... 83
APPENDIX 6 - Paragraih Stimuli Lor the Oral Recall Test ....... 84
APPENDIX 7 - Summnary of Aralysis ,5f Variance - Ampltitude ofAfter Discharge - Channel 1 ........ .. . . . . . 85
A?" ' .42 1 - Summary of Aralysis of Variance - Amplitude ofAfter Discharge - Channel 2 ...... ............ ... 85
APPENDIX 9 - Sumnauy O6 Aualysis of Varvance - Amplitude ofAfter Discharge - Channel 3 .................... 86
APPENDIA 10 - Summnary (if taiysis of Variance - Amplitude ofAfter Discijargc - Channel 4 ..... ......... . . ... .86
APPENDIX 11 - Summary of Aaa,.•i,si of Variance -- Amplitude o fSecondary Complex - Channel I ..... ........ ..... 87
APPFLNDiX 12 - ýurmmary vi Aai~s .z of Variance - Amplitude ofSecoadar\ ,'wx -Channel 2 .............. .... 87
APPENDIX 13 - Summary of An.J of Variaiine - Amplitude ofSecondary Cot•x - Channel 3 .... ........ ..... 88
APPENDIX 14 - Summary of -)z:l * vt of Variance - Amplitude ofSecondar:! Complex - Channel 4 .......... ........ 88
Page
APPENDIX 15 - Summary of.Afia2ysis of Variance - Width ofSecondary Complex ",'Channel I ............. . -89,
AFPENDIX 16 - Summary ,of Analysis .of Variance - Width. ofSecondary Complex - Channe~l 2 ..... ........ .... . 89
APPENDIX 17 " Sununary of Anriaysis of Variance - Width ofSecondary Coiplex - Channel 3 . . . . .. .. .. . . 90
APPENDIX 18 - Summary of Analysis ulf Variance - Width 6fSecondary Complex - Channel 4 .......... .......... 90
APPENDIX 19 - Summary of Analysis of Variance - Complexity ofPrimary Complex - Channel 1' . . . . . . .. . 91
?YPENDIX 20 - Summary of ý)nalysis of ,'ariance - Complexity ofPrimary Complex - Channel 2 ............. ........ 91
APPENDIX 21. - Sumnmarv &I i.alysis of Variance - Complexity ofPrimanry -Coiplex - Channel 3 ... ... .. ......
APPENDIX 22 - Summary of Akna]ysis of WVarjiance - CoMpIexiLy ofPrima-cy Complex - Channel 4 ... ......... ..2
APPENDIX '23 S;ummary of Analysis of Variance Complexity ofSecondary Complex - Channel I .. ...... . . . . 93
APPENDIX 24! - Summary Of Analysis of Variance - Complexity ofSecondary Complex - Channel 2. ..... . .... 93
APPENDIX, 25 - Sumt-uiy of Analysis of Variance - Complexity ofSecondary Comp3.ex - Channel 3 ... ........... . . 94
WAIPENDI. 26 - Sunuwar~y of Analysis of Variance - Complexity ofSecun6ary Complex - Channel 4 .... ......... . ... 94
API'E4NDJý 27 'l:Iur,,y of Analysis of Variance - Complexity ofib o .)i.scarge - Channel A.. . .. . .......... 95
ij'PNDI,', 2S - Summary of Analysis ,of Variance - Complexity oft. Discharge - Channel 2 .... ........ . . . 95
APPENDX /9 - Sum'u.r: of lunalysis of Variance - Complexity ofAVtou Dischar•ge - Chcnnel 3 ...... ........... ... 96
,V'NPLAWU 30 - Summaiy of Analysis of Variance - Complexity of10 1 D:ischarge Channel 4 .... .......... 96

APPENDIX 31 - bummary oi i,!aLysis of Variance - Latency to PeakDeflecc.oi -ýnannel I .. ....... .............. .. 97
APPENDIX 32 - Sumnary of Afwsiysios of Variance - Latency to PeakDefilcta.on - "rmmixul 2 ....... .......... 97
APPENDIX 33 - $suiyruci Cf C >,II -)0 Var :Wiance - Latency to PeakD-fIsdC t -'. o ' ýhrv- 98~fL~fzt:<' -- (hn. vn'&l....-....... ......... .9
APPENDIX 34 - Summaýy, of vi -- ,s of Variarnce - Latency t.'• Peak,. . . . .. . . . 98
APPENDIX 35 - Suu.na , ','..'-' €. Va.ac.,nce - Amplitude ofPrimr C', " .- .hannel 1 ... ......... ....... 99
APPENDi{ 36 - Suwn-, , vis of Var ance - tAmplitwde of, ,,] amei 2 . . ... . . . . . . . 99
7( •; - c . ,si oi Variinc(e - Amplitude of:ltj n, , - Cnannel 3 .... ......... ...... 100
rIPE11.: 3 -16 i..y s uf Variance - Amplitude of,', ( ,: ,, - an ....C..annel 4 ................ 100
SAPPLN:X 39 - - ,rianrte - SecondaryCoIy.,. - - Channel I ...... ... 101
APP EtINX f X - .1 . . .,C - 3c,:oldary• '1,), , . .. * • )•, ' i'.u' g - (~~n.. ?1
- - ? . .Ol . .9 it']
,XPYiNOE{ 4£ -- 6:, ,, ..I N. 0 I -1,aoondary
,2P12.,',DLv 4.' - '.,.a m, " - V \,'ri :;,c - ., nd r2 CANI'' 3 . . .
APPENDIX 43 - Ttr.u.' s o,, ;,. - , Votals - Amplitudeul n c, . . ... .... ... 103
A4. ,� , , %2 ', , t,.,Q l ,.t-Ie -. MIDI!iLude1 ' ,"r. 3....... . ........... 103
APPENDii.% 45 - A. )re 2re! ces ,ecer. 'fotIa)s - Compiexityr1 i imcry AV )L.,,):. - Channel 1 ........... ........ 104
r6
Page
APPENDIX 46 - Tests on Differences Between Totals Width of
Secondary Complex - Channel 1 ............ . . . 104
APPENDIX 47 - Tests on Differences Betweent Totals - Amplitudeof Secondary Complex - Channel 3 ......... . . . ... 105
APPENDIX 48 - Tests on Differences Between Totals- Amplitudeof Secondary Complex - Channel 1 .. ............ . 105
APPENDIX 49 - Tests on Differences Between Means - Amplitudeof Secohdary Complex - Channel 2 .......... . 106
CX Z

THE NEUROLOGICAL EFFECIS OF INH
INTRODUCTION
For several years the drug isoniazid (INH) has been empi.6yed-in thetherapjeutic and prophylactic toreatment of tuberculosis. As a result,• ourknowledge of the drug's actions and side effects is considerable. Amongthe various effects, the ,effects on the nervous system are ,of prime im-portance and are most frequent.
The aviation environment demands a leyel of performance that is seldon,required elsewhere. Consequently, subclinical problems and side eff:•"zts v"T1 11 or iiiy other drug miy ,ause difficulty in the a4,ator which would iotbe manlfesz: in the general population. This leads to the conclusion thatreurrenr knowledge of drugs should not be applied witnout reservation lo
• Ind that drug effects in this linique envw.runment should be inten,sively !,'O.ied.
An opportunity to pursue thib obj",tLive aro~U a,. Fuit Rucker. Sevei-al civil ian instructor pilots were expo,-eu to a .as' of active pulmonarytuberculosis. Subsequent tuuerculirn skin test. cecealed a positive reac-tion in each case. In accordance with accepted me'Ldtcal standards, theywere put on a program ,of I[H therapy whLtch was lo last Ior one year. Manyvolunteered' to participate in a 3tudy of Lhe C fft• ;i this program on"-heir flying performance. Neurological, general medi.:aj, psychomotor andophthaL.,ologic studies were done. The results or thse studies are icport-Pd elsewhere.7 38 86 The study by Shub, et. al.,'"' ineiely sununarizud thErourological results, The purpooe of 6bi, papc.- ite present these inmore detail. Computational i.rrors which were dscove-pd after public-tio,
" thr- VI r't paper and a differeiv.,. 1iu Llt Ii. -' t-,ect: popiil r~,• '.:h j,'Iidonr ! figures are oased w[Llt hi-, j , •,De..iscrepat is.
METHOD
t ,z t, were 5A civilian ini.;ttu o, oi lot,, whO volunteevrei toS.. .. • tudy. Tweity-one (21-•.| ' l•, ý .- - Ieted the , oi Le
' ri,,nr14. 'If therapy (12--month subje¢.rs). ,Suver (7) s.ul1jects complete'dT It". 1.f therapy (6-vionth nub i e- 1-) . ';&? dat., presented' in rhi.
•h, *, ,h' esulting ý% subject. [he *,.it. pre',nted are prindi-v-, I 1, ,t ir.wi 0 we 12-month sub ;ct s. When ,,atA rrom I'he 6-month ,.IŽjec. -
,. .- y will be soe(.l bl kv i.L,•.
16

'The -mean age .of the 28-subjedts was 47.2 yeats (range 39-57).. Themedian age ,was 48 years. 'The meafi, ages Of the i2- and 6-imonth. subjeptswere 48.1 yea6s and 44.4 years respectively.
To bL ixicluded, in this study subjects had to be in reasonably good-health, free of tuberculosis and :sh6w :a positive reaction to intradermalintermediate strength ppd (i0' mm of induration after A48 to, 72 hours). Foradditional details see Shub, et, a1.8 6
There was-no non-drug control group included- in the study.
Experimental Design - The design of ,the study was that subjecta were eval-uated three times during the course of therapy.:, Once before taking INH(referred to as control or baseline), once 6 months after being on the-drug(6-month exam) and once 12 months after being on the drug (12-month exam).The INH therapy consisted of a,300, mg daily oral dose (3-5 mg/kg body weight).Ten subjects also took or were given Vitamin B6 (pyridoxine-lO0 mg/day) forvarious reasons.
The. design of the study was that each of the following measures would betaken at each examination period: Neurological history, clinical neurolog-ical examination, mental status examination, clinical electroencephalographicexamination (EEG) and visual evoked potential (VEP).
Because of the complex nature of the methods and procedures employed ineach of these examinations, the paper is organized into four separate studies.
LITERATURE REVIEW
A considerable amount of literature exists describing the variousneurological side effects of INII. For clarity thes, are preseuced insummary form in Table I where the effects aro lunipea into nine k9) majorcategories. It will be noted that this categorization j.. not enitirelyadequate in that many of the entries miight be class.iied in several waysand considerable overlap is unavoidable. The appropriate references areindicated. This list is not exhaustive; perhaps 50. vF Lhe ex.bting lit-erature is cited. The authors are not aware, howe'utr, of any other neu-rological complications not included in the table or discussed below.Some effects are not strictly neurological but included because of theirinterest to neurologists.
Various dosage levels and species have been employed in the studiescited. For completeness, all the effects are listed, but special attention
2

is given, to the effects found in humans taking an amount of INHW similar tothis study and tO effects found only with iNH overdose.
Since its introduction in 1951 as a chemotherapeutic agent for tuber-culosis, INH has been extensively used and studied. After an oral dose,peak serum levels are noted at 30 minutes 7 0 76 to one hour. 3 5 48 At fivehours the level is 66% of peak 7 6 and at six hours it is 50% of the peaklevel. 32- The reported time required for complete serum clearance variesamong authors. Twelve (12) hours, 3 5 16 hours, 7 6 24 hours 7 0 and over ,24hours 4 8 are reported. Elimination is via the renal route 3 5 48 95 and comi-mences ten minutes after oral administration. 4 8 No accumul'ation of thedruý-in the ~human body occurs, 7c, '#8 although Barlow, et. al.,.. report accumulat.ion*in ,the cat hippocarpus. 6 It is also reported that nc protein binding occursin the serum.,5 Peak excretion races are noted fr6,n ewo to four hours afteroral dosing. 7 0
INH is excreted unchwigWd as the acetyl derivative. The respective:)aLt entaies of secretion in each state- .te 4 to 32% and 5 to 65%.70 T"3.re
-s a direct' corrlation of serum INHi with free urine ENI! and an inverse. ckeelation with acetyl-INI.0 41 An interesting aberration )f INH metabolismhas been noted in mongolism. Compared to matched controlq, mongoloids havebectn noted to have lower serum levels following the same oral dose. Theirurine contained a lower than expected percentage of acetyl.-INH.100
No localization of INH in the body is seen. There is equal distribu-tion between the blood, brain, cerebospinal fluid and the visceral organs.8 :
St is well known that the population d&,splays two patterns of metabo-1' 4ith a less-well-defin~'d group between the extremes, characterized as
cow, intermediate and fast inactivacors. 3 2 ' This distinction is made onIe plasma INH level measurable six hiours after an oral test dose. Six-
"-.b, miL.rograms per ml seems to be the acc ptaulk, Aividing point. s.ib-,'s ti, '-vels under 0.6 are classLfied As fa-;L; over 0.6 as slow; and
,.' " ntermediate.19 35 It has bnt,e 'tci hat this Jdi-f: .rom varying genetic conaSItuL .*o- . Kast inactivation I.
i ,,.r, i,-tno•omal dominant and slow in ',t vartion as an autosoma]. , ( .24 35 W, A slim majority of tht. population can be expeLced
'k~)xq jna.Iivatorsi and only 7% intet odi,•'".e '5 SO.ow inactivators__.e u ý.ttater percentage of 11NH in ,be uný-etylated state8 4 and, as
-<,eztod, hovp more side effects fronm the drug ('" ind below).
.'t rio dV.sage levels employed in the presunt study nost authors re-
t-. f.w -,- no side effects. Most rate, -i si lo eff,'cts 'reported are int0,0 iange of .2% to 1%.- i 2 lower, Late is tigh ias 42% are reported.

At dosag. levels-of 10. mg1kg r5%. incidence is noted; if 16 to 20mg/kg, 22.5%;' and, if 12 mg/kg, 51%,5'
The reason for this, discrepancy, is unclear. One factor certainly mustbe, thr severity of the •symptoms, On-e author might consider a mild symptomworthy . of note; another might not. For example, the American Trudeau Societynotes an 'overall incidence of 5%, but only 1% were serious enough that dis-continuance of the idrug was considered to be advisable. 9 5 Another likelyfactor is "the ,means of diagnosis. Hanson, et. al',,t report 6.2% overallincidence ,of Side effects, ,but base this figure on subjective reports. Thehazards. of this ,are illustrated by Ferebee-2 who found i.. i.9% overall io-cidenc& but also 'an incidence of 1.5% with a plaeebo. True side effectsoccurred earlier. Other authors have noted as well Uiat side effects aremore- common• in ,unstable •people. 1 0 1
SFerebee 2 6 and Vysniauskas and BruecknerI0i raport gretex side effectswith increasing age. This would not be unexpecred since it is known .hatolder individuals tend. to• have more drug-lndu~ed side effects.
Most symptoms take one and one-half to three months to develop. 2 6 101One author reports a 12% incidence in his population six weeks after beingon a dose of 20 mg/kg. 7 5 This increased to 51% at 20 weeks. The corres-ponding incindencse when vitamin B6 was added were 10% to 25% respectively.Toxic reactions are more fraquent with concomitant Ulcohol ingestion 3 andless frequent with concomitant phenobirbital. 01 These factors as well asthe dosage and type of inactivation nt:ed Lo b.: consi.lereo it evaluating anystudies of the incidence of side LiZcL. M ,diei, such as the monumentalPHS trials using large populations vidi ,(,acc,! Q4,, cr.,s rwould be quitedesirable. 2 6
Although nearly all S'iudieS repo-c ,viuv w,,1I6 c *ipLions with 3-5img/kg dose of INH, Vysniauskas aant i -&i .c,,o re side effectsat this level. Therefore, it cannot bu &,ssy,.d tw,• tlo Irog i ceally asinnocuous as claimed.
Side effects related to :hi . '' ,tj , , o ,; ',,ur 1o0L fre-quently. 2 95 Thirteen and six-tonchs pereent of ,l .' roctons to INH notedin one study were neurologic. yj v ,z . t .-,f , %4 r,-a,.t-tion'; aro re-lated to the CNS. 10 1
The incidence of neurolglcal 'g-W&ii•A o . .:Veucd in any seriesof cases is comparable to tine •~rideuce o o -. , of t, Workers employ-ing a 3-5 mg/kg dose find no neurologic•, - , 5.5, 2%and 3-4%8 incidence. Ferebee't' found that the p cceutage or complaintswhich were neurologica- was 16.8%. IIowcv':, ': ,_ o1•c~Tu gtoup, the inci-dence was 7%.

At higher doses ~the incidence inc-rcases. Withi 6 1.0 v&~/kg 8%,8 - -19%, 1-ar5 reported. With 11-i5 inglkg A8) 17 CZ'ý Jh 6t 2
K kg, 44%,8 37%,75 17%,7' 29%.50 'maniy (--1 tbese figuircs art. aot c~pec.fical1ymentioned byý the authors involved but -;tr"ed 1ro... zhir data as accurate-ly as possible. The reasons for th*p divcti~pal)cies ý,u'lo include ~hose aiis-cussed above. In addition, the prev.ious Jrug Hit~torl ~n to pl~ay an m?ortant part. The incidence increaseo, U- TAU 1lad beeii takea precviously.8qAnother faccor is the way in whiceb the dru-g !. adrjninisiere~d, D1iiding t~ledoses results in lower neurologic side effe~cLs), presuN.ibly an indicationthat the .peak levels achieved in the sei!.m have oticlogic s.,gnificance.
LMoney 58 reported a 20% in~cidence i-ihj.. iii- ec.' tat;Lng 4. to 6 mg/kgbut most were alcoholics and undernourished--factors which. many agree havebearing oil the problemý.
In nearly all the studies cited perlphe.ca, J~~a.~ zw tL t, t~i an wythe most common finding. flyperreflexGi~, cuiztchiog, i4,tiessnx~ss1 and dizzi-ness" are also mentioned as being cominoa. lthe. iitcieciteo inc'r,ýases Ulitii thetime the drug is taken as. in the i#4~~:~i gen~ara 6U ~ects S Id~effects are generally noted within Zour snonth8i." '
'Little doubt exists at the p~resent. time that .:'ne or rior' ofT the analogsof vitamin B6 is intimately related to the nio.iiiA ah fcto INHMany authors report that B6 eithur dvedts o;oecri toe izicidenct: andseverity of neuropathy. 9 1 2SO G2 'hiph.t"i i seen even ifas much as 2.0 mg/kg of INH11 is give-n. 9 75 Aa INII~e v, level aliwost:invariably produces neuropathy. The vitamrin apj.ý:aro. to be aoce effectLv'c .14a prophylactic agent than a therapeutic orne. 9 Near*. :1!) of-er iteutolvi-ic~iIproblems related to INMI are reported i.0 Show, Ztl1AiýLioO V-, a L'6.question ~of whether B6 is ef fective ia seiziiýes L.. Ie.' SOI..wI.rb
report no-, ef fect and leel that the vitamin has Only po:ýiA eff-.LCtU. cýfd
no0 effeact on seizures or other CNIS prob] ein,,.~ - : te~pct Cbie VQ"bitc-7 1 'P 32 E, It is even report~ed Lbaiý B6 ~~g~c. 'C a b"~b
FN. A correlation betwceen Cht: se,,'mr tW. tze~ "li;res and 1wpresence of neuropathy has been Shown. I' l~~.:o.. efetose~izures would be expected for aiiothez 1teuaon. 'Tvi'~eny4 ~~which occurs in early childhood I., jarce buL ai wv OjlI~l t.Ihal
whlere dramatic reversal of cl~ini.cal scizu~tei j,.d C'- uot EEW.f*:oJALi(!!3thereof is seen with B16 adniinistrar.i.01o'Y hL; 1Iýs )c0JL' t'dly(COI '- ~by demonisrration of the fact that: 136 is ..% acc1--L"y, ct ii ý'-r "tie svnLttsiof GABA, a presuimed inhibitor transmwu.ter. jF 11~.o.1- itOf :.ikfi%- to decj-,-ass2brain CAB3A,,7 although this effect i~j Ctnia aaat :ý ~I '..-aeatsd 17,Uvr."A thurapeutic trial of this compound o:. g uLIfi ' -:C 1't Az iot ou' ean done, butwould be oe interest.
Why should this relationship of JidlI ai)d B16 VC1~ " ~ rs ppearSto be that a B16 deficiency is producýed by IN'.. 'ilic vw.:o'I of thih- inter-action has been studied extensively AceesL' ~ ~ nOf 86

is reported. 9 55 39 DirecLx metabolic antagonism has been shown, 3975including depletion of tissue vitamin. 14 Presumably this results from 'thestructural similarity of the two moLicules resulting in analog formation.48Pyridoxal and pqridoxa) phosphate as.ist penetration of the blood brainbarrier by IN1. 8 b3 It appears thae -this action accounts in part for someof the side effects seen eird for the beneficial effects of supplemental B6given with INH. .An additional observotion amplifying this point is the factthat conditions where subclinical B6 deficiency would be anticipated alsoshow a higher incidence of oide effects, such as malnutrition,5U alcohol-"ism,58 old agel01 "C avd deb-.litating disease, specifically TB. 9 Also,the neuropathy of INN is stt-ed to be similar to the neuropathy produced bya B6 antagonist. 9
In-spite of the evidence. _his suggestion is doubted by some, 3 9 becauseother .signs of B6 defic -erny are not seen with INH administration, such asglossitis and skin lesiolu.. These have been reported with INh, however,even on low doses ot 30 rPg/day. 19 20 89 92 It is also suggested by somethat the dietary deiciency is !ifferent than that produced by INH. Thebiochemical raact2.ons, for axa•il•e, are &ifferent. -One other possib'lityhas beere suggested. Caverawug-1' iotes that clinically, the neuropathy of B6deficiency and porphyria. a-, ,o M L~ I and' that B6 deficiency has been shownin porphyria. 'He sugJeir #,h| p.ossiblxy the metabolic defect in porphyriaand INH side effects is 4he sam.e_ rINH has been shown to interfere with,porphyrin metabolism.3
Other metabolic ino:,iactP..s .- ( !1q1 wth other drugs have -been noted.It. has been obs.erved tCit P•tietits taiing both INH and diphenylhydanroindevelop toxicity whereas or, ar iodentical dose of diphenylhydantoin alone,they do not.1 26 21 This ph,3nemenoa is seen more often in slow inacti-vators.1 52iasr. 6.ino.tivat- - a'w : steep rise of diphenylhydantoin plasmalevels up to 7 aays, whic¢.1 teaJd thereafter. ln slow inactivators theinitial rise ws steepet ind 010 plCaveau dt a higher Jovel. Those in the.latter group who devuloý)ed .1p0eiylihyJalitoin toxi.eity showed a continuousrise of diphenyihydarto:&i uJ.'a,, wit.hb no plateau and the slope of the in-crease was far steeper than ; v"he' two groups. In all cases the di-phenylhydantoin level was I-gher at :. times than when no INH was given.
In cats with vario.As d.k's;Lgz- or MIR, a direct cor-kelation has beenshown between the amount ow L*1 gi-,).t and the blood level of diphenyl-hydantoin, "n vico nttdi^. ,o.,t-e Lhar the mechanism of this effect:appears to be tFon.-cotnp.tý FtI,, le iiihibition of thl- enzyme systemmetabo~l-irig dipheiy~hydait.o~ p-.rohydroxy1&;ion. ' 2 Inhibition wascomplete with 137 itiicrogc'm. /w , l il ond 18% with 5 micrograms/ml.
Para-amirosalicyelic x•vi • r quenLly given with INH. It has beenshown char this rvstie.s I., o",- ot•aon ot the half life and flattening of
the peak levels of INH.9 8 Ceriloplasmin oxidase. is inhibited by INH, re-sulting in decreased degradation of serontonin.31 Plasma, but Not platelet
monoamine oxidase, is also inhibited. 7 2 A possible synergistic effect withdisulfiram exists. 102 Another interaction which may explain some effectsis that INH inhibits intestinal transport of amino acids.b0 15
Peripheral neuropathy- is generally considered to be the most com monneurological side effect of INH. As seen, it usually responds to• adminis-tration of vitamin B6. Vitamin preparations containing all the vitaminsexcept B6 have no effect but, interestingly, glutamic acid does appear torender preventive effects. 1 7 The incidence and severity is (lose relat-e, 16 32 7 75' increased in slow inactivators,32 33 so 16 and correlated,with the serum INH levels. 1 9 Symptoms regress when INH is stoppedi 2 8although prompt and complete regression is observed only if no findingson the neurological exam are noted. The time of onset of symptoms is alsodose related; higher doses cause earlier symptoms, 8 dividing the doses maydelay the onset, 9 and the incidence is greater if the patient has takenINH earlier. 8 It is reported that the incidence of neuropathy is in-creased 8 1 9 and decreased 32 in individuals whose urine, contaihs more freeINH and iess •acetylated INH. One interesting report 50 describes decreasedSGOT levels in patients developing, neuropathy on high doses of INH withreturn to normal upon clinical clearing of symptoms by discontinuance ofthe drug or B6 administration.
By the time a, patient has been on INH for ten months, it would be ex-pected that symptoms or signs of neuropathy would be noted if they are goingto appear at all, 19 8 9 30 although the delay may be in terms of years.0Initial symptoms are sensory--burning, numbness, paresthesia, etc.30 8 Ill 88
Only one study could be found which measures nerve conduction time. 8 8
This is regrettable since it is recognized that suggestibility and other non-neurological factors are important. 8 26 Yet, a decreased conduction time wasseen. Cavenaugh1 '• suggests that ,motor involvement occurs but is compensatedearly by regeneration and collateral sprouting of nerve fibers at the- Milusclelevel. This has indeed been demonstrated to occur in experimental animalsoin INH. 36 This might be reflected in physiologic measurements. More studieswith careful control of stimulus parameters are necessary to settle the issue.
Symptoms begin, distally and more proximal invoivcment is seen later.c'Devadalta, et. al.,19 studied patients taking 7.8 to 9.b mg/kg/day of 1Nil.Spontaneous complaints appeared after 2 to 10 month,. SabjectS were examinedif complaints continued and were follo,.ed-. Distal parestne,,ias were ini-tially seen primarily in the feet. Dista. weakness wao noed by their pa-tients but only in the hands even though all extrvtAile. a,)ptared to be in-volved on examination. Other physical signs were .Iurgtl i±Lnited to the
7

lower part of the body and consisted of hyperesthesia, hypaigesia, posteriorcolumn findings and loss of deep -t&ndon reflexes.-, One patient had anesthesiaof the right face, shoulder arid sca-pular area. Initial signs were loss of
vibration and ankle jerks followed by hypesthesia and loss of positi6n sense.The severest cases had Lbss of iknl'e jerks and weakness. A slow progressionand spread, of findings were- notad4i
Bienl and Nimetz, 8 in iavc *tigating peripheral neuropathy, noted anearly and late stage of develoment. The early stage consisted of only
sensory symtpoms and were reversible. The late stages were seen only insubjects 7,eceiving 20 mg/kgý ani consisted of subjective and objective finid-ings. Discont4nuance of NR, in these subjects produced some regression butabnormalities persisted for months. One year afterward some subjects stillcomplained of ourning, had atrophy, fasiculations and weakness, implyingstructural nerve damage. Some of their subjects developed contractures,but t•hey felt this could not be definitely attributed 'to INU.
Seizures, when seen, arc usua.l.ly found in known epileptics or are"nimcre frequent in these patients.. %I It is rare to find a case in pa-tients taking 300 mg/day. Yet cases of status epilepticus hav been re-ported at these l'evels.)v" These have been, again, in previous epilep-
" ~r4cs.
In view of the meiaboliz i r.ýractions of INH and diphenylhydantoin,it is quite Lurprising zhat dipher.y1hydantoin is almost universally foundto be ineffective in control of seizures induced by INH (71 and below).Phenobarbital has been recomecnded, ' 01 but usually is only slightlybetter than diphehylhydantoin (see below). The ,effectiveness of B6 hasbeen discussed, and in general is superior to conventional anticonvulsants.Pyruvic acid is scated to have a 1)coective effect against seizures. 3 9
Dizaepam and depressant drugs hate been employed with some successs (70 71and below). Susceptibility to seizures increases with. steroids. 5 9
Reilly, et. aJ..,11 ne' lura,,o a carefully controlled stldy where theseizures producing effect of) 1,\a was quantified. It was noted that sub-.jects who were Lakin8 L'X exper..ratced a lowered threshold for seizures, pro-duced by photic and aud',,ory *Orauli. The subjects all progressed througha characteristic photogel, Ls. SI; re pattern starting with facial, seizures.In doses ranging from 20 to 4.) m6/kkg only 35% of the trltais produced 9,gizures.Even 45 mg/kg did not alwavo. cause seizures. The authors concluded thnt areliable convulsant dose co,"J not be found within their dose range. En-hancement of photo-s•ensiLivity is also noted in epileptic baboons with 50-150 mg/kg. fb
The above results are quit,- surprising in view of the rest of the lit-erature,. The authors considec careful study of reports,/of INH toxiiity from

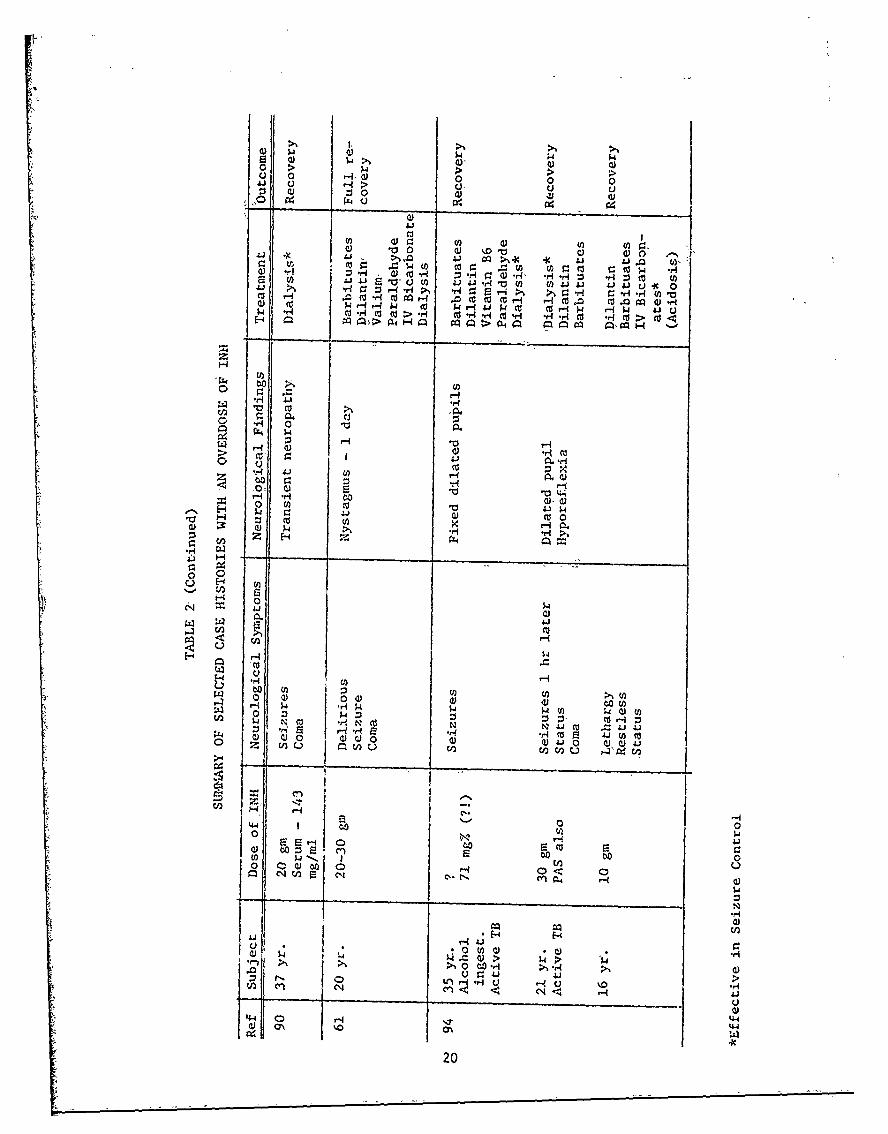
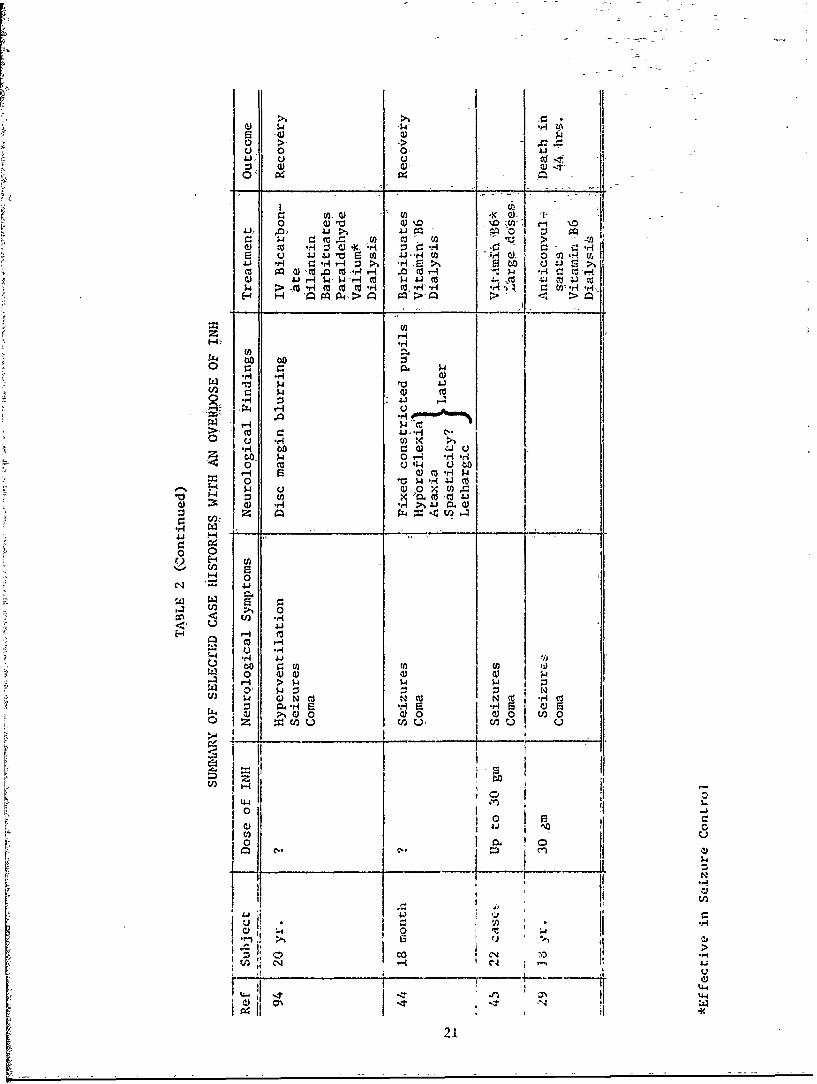
overdose to be particularly instructive. The, pertinent facts in severalcases in the literature are su~mmarized in Table 2. It will be noted thatseizures are a feature of all cases. Assuming an'average weight of 70 kgfor the subjects in the--study reported by Reilly, the dose of"INH used wouldbe over 3 gm. This, dose produced status and death in one case.
Table 2 is not intended to be exhaustive--merely representative. Terfiianand Titelbaum9 4 present an excellent literature review on this subject.Wherever known, the dose of INH is presentedz in mg/kg.
Several interesting features of this summary are appaient. First isthe striking clinical similarity of'toxic manifestations although a widelydiverse group of patients is presented'.
Coma and intractable seizures are seen in nearly all cases. Othersimilarities as discussed by Terman and Titelbaum include respiratory dis-tress, metabolic acidosis, hyperglycemia and acetonuria. The acidosis seenin several cases is remarkable and often severe.- -Lactic acidosis is- reported-in dOnventional doses as well 1
Another feature is the notable lack of effect of the tisual anticonvul-sants to control the seizures, although diazepam is occasionally effective.Often the acidosis is responsible for this and correction of it results incontrol. It is notsfelt, howevet, that the acidosis per se causes seizures. 91 lIt seems that B6 is occasionally effective, sometimes dramatically so. 5 Thismay relate to the dose of B6 employed. It continues to be recommended, incases of ingestion of more than 10 gm2 9 and on a gram for gram. basis withINH.56 Another interesting point is that the interval between ingestionand seizures, when given, corresponds quite-closely to the time when peaklevels are noted -on metabolic studies. Perhaps, as suggested, the rapidityof change of serum levels and resulting penetration of the blood-brain bar-rier is the basic pathogenesis invoived. The range of dosages involvedreveals a wide individual tolerance. The case of death following 3 gm8 5 isthe lowest lethal dose of which the authors are aware. Perhaps the alcoholhistory contributed, in concert with earlier.observations in this paper.However,, the opposite, appears to be true when alcohol ingestion was presentin patients ingesting extremely massive doses with recovery.
It is stated that acute toxicity occurs after ingestion of 80 to i00mg/kg, 2 3 and that certain death occurs with ingestion of 200 mg/kg. 1 2 In-spection of Table 2 will reveal that the last statement Is untrue, Morethan twice that amount has been taken with favorable outcome. More than8 grams has been consumed with absolutely no CNS effects.bZ
The cases reported by Nelson 6 2 in Navajo Indlans are especially in-teresting because of the rapid recovery following sizable doses. However,all the children vomited some time after taking Ehe drug, and they may have
9
absorbed only a sm§l1 amcunt. Another unique feature is that the dose wascqrefully counted before iiigestion and, therefore, quite reliable. Theais est dose ever taken,, ,too-the author's knowledge, 1 was 40 gm, cited. by
Terman and Titelbaum. 9 4 The details were not. presented.
Large doses In animals' produce mucA th• same picture-with a good cor-relation, between the plasma level and. the toxic effects. 7 1 76 The animalsappear to be more susceptible to INH 'Lhan humans. One hundred fifty (150),mg/kg7 1 or 9-35 microgram/ml 7 6 causes death. Transient CNS stimulation
occurred with 6 to 8 microgram/ml,
In regard to the mental efflcts of INH, much less literature is avail-able. A Scandanavian group64 99 has done the greatest amount of work. Im-pairment of memory was noted in' a majority of subjects taking conventionaldqoes of INH. This effect was more prominent with higher doses. It wasonly partially reversible. Further investigation revealed this effect tobe a combination of confusion a:nd .a subtle inability to concentrate onmore than one task at a time,, revealed by a test of their own design.Some of the-psychophystologi•Al measures in our Fort Rucker study were de-signed to specifically inveseigate this point• 37 38 In, contrast to thisreport, no change in mental.<function 3 7 or a suggestive improvement havebeen noted. 26 97
The issue of mood and personality changes is likewise controversial.Mood changes are said to be the earliest sign of toxic encephalopathy. 1
It is often noted that INli-caused ,psychosis is related to a previous un-stable personality, 1 0 1 95 but not' strictly limited to this.I01 It is oftensevere enough to require hospitalization. 5
Some of the literature on experimental INH pathology in animals a;-hllbe summarized in relation to the clinical problems discussed above. Thesestudies were done on rats, mice, and ducks who were givlen IN1l-in doses ranpingfrom 125-360 mg/kg in rodentj and 1000 to 1500 mg/kg in ducks. 15 3G 54 65 49
91 107 67 81 83 5
In studies concerned with the peripheral nervous system, with onlyone exception,6 5 clinical changes were noted after pathologic changes hadoccurred or were not noted (presumably because '-.e experiment was terminat-ed before the would be expected). The delay Was as long as 7 to 8 monthsin one case. Severe pathologic changes were frequently seen, yet theanimal was clinically normal 36 or only minimally involved. 1 5 65
In contrast, early changes occur in the electromyogram and nerve con-duction Lime. Hildebrand, et. al., 3Ib studied rats given 330-360 mg/kg. Anearly slowing in nerve conduction time was seen; at first only sensory.
10
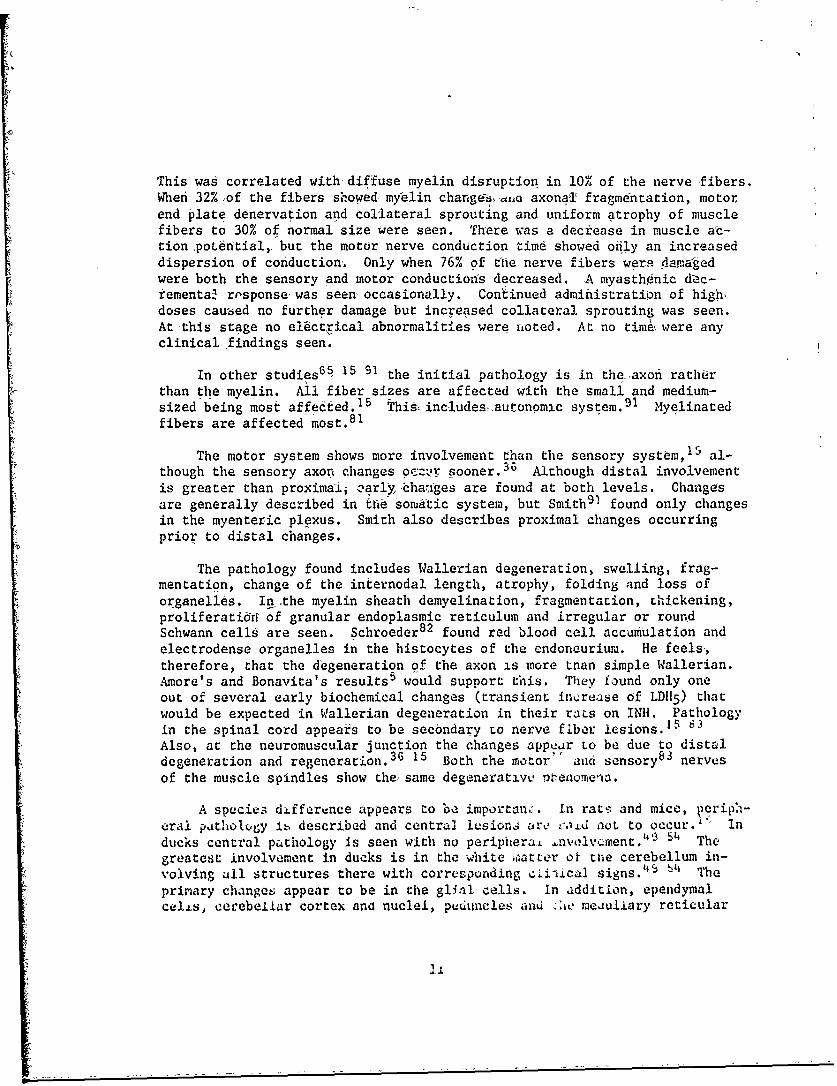
This was correlated with-diffuse myelin disruption in 10% of the nerve fibers.When 32%,of the fibers showed myrelin changedioa axonal fragmentation, motorend plate denervation and collateral sprouting and uniform atrophy of musclefibers to 30% of normal size were seen. There was a decrease in muscle ac-tion~potdftial, but the motor nerve conduction time showed ofily an increaseddispersion of conduction. Only when 76% of the nerve fibers were damagedwere both the sensory and motor conductions decreased. A myasthinic dec-rementaW risponse-was seen occasionally. Continued administration of hig&,doses caused no further damage but increased collateral sprouting was seen.At this stage no elictrical abnormalities were noted. At no time were anyclinical findings seen.
In other studies65 15 91 the initial pathology is in the. axont ratherthan the myelin. All fiber sizes are affected with the small and medium-sized being most affected. 1 5 This includesý.autqnomic system. 9 1 Myelinatedfibers are affected most. 8 1
The motor system shows more involvement than the sensory system, 1 5 al-though the sensory axon changes oc•r sooner. 3 6 Although distal involvementis greater than proximaii :arly,ýhaiges are found at both levels. Changesare generally described in erie somatic system, but Smith9O found only changesin the myenteric plexus. Smith also describes proximal changes occurringprior to distal changes.
The pathology found includes Wallerian degeneration, swelling, frag-mentation, change of the internodal length, atrophy, folding and loss oforganelles. In.the myelin sheath demyelination, fragmentation, thickening,proliferati•a of granular endoplasmic reticulum and irregular or roundSchwann cells are seen. Schroeder 82 found red blood cell accumulation andelectrodense organelles in the histocytes of the endoneurium. He feels,therefore, that the degeneration of the axon is more tnan simple Wallerian.Amore's and Bonavita's results 5 would support this. They found only oneout of several early biochemical changes (transient in,.rease of LD115 ) thatwould be expected in Wallerian degeneration in their rats on INH. Pathologyin the spinal cord appea~s to be secondary to nerve fiber lesions.15 81
Also, at the neuromuscular junction the changes appear to be due to distaldegeneration and regeneration. 3 6 15 Both the motor aud sensory83 nervesof the muscle spindles show theysame degenerativu PTAenomena.
A species difference appears to be importan.:. In rat• and mice, •eriph-era! putholcqy i•. described and central lesions are 00,-d not to occur.' Inducks central pathology Is seen with no periphera. •nvolvcmient. 4 51', Thegreatest involvement in ducks is in the white matter of tue cerebellum in-volving all structures there with corresponding c.i-ical signs.'$ 4" Theprimary changes appear to be in the glial cells. in addition, ependymalcelis, eerebellar cortex and nuclei, peduncles and •-.i meauliary reticular
Jii

formation are involved. IL rabbits, uc reased dutec.aLle neurotransmitterand neurone degeneration is seen in tnc iiypethalamur', mostly in the para-ventricular nucleua.67 A material not furrtha chi avasrrized was a,*s3 seenin the pituitaýy.
Pathoiogi, bcaoie- in the human nervous, systvM , .aiot ý.-aC.tSent.PerivascutoL: aemorrhages, optic tract demylination- . ýeaing, of Ohe vreymatter,ý.- cerebral edema and degeneration1 0 3 were not u lnp:r.pieats who, ,ledfrom an overdose of INII.
Simmons and Ambler 8 8 conducted the one study which ms, sely approx-imates the present study, Fifteen (15) healcLy aviators, ab% -it 4ocif2 ed,were given baseline exams includin, EEC, median ner~ye motor cftductiG-I time,physical exam and INH blood levels. Following this 300 rig of U0" were givenorally in one morning dose and subjects were reexaminet, twice a waul- for thefirst two weeks and once a maonna thereafter. Subjects were studied tor oroyear. No serious side effects necessitating removal from flying dutieb Yereencountered. All subjects were found to be rapid inactiveors. Nerve c'a.-ducticn times were done oi L3 of the subjects, but rep:atvd on only three it-the third montn. Of these three, one snowea 4 change from 82.5 to 53.3meter/sec; one from 67.5 to 61.25 and 60 meter/see; ana one from 70.5 to 88.5meter/sec. Both the subjects withi the large decrease and the one with theincreasie in conduction time complained of paresthesias with the first rerporting headaches as well. T complaints disappeared when INH was stopped.No other neurological tomplainr• are ",)Lad. The EEG :esults are not men-tioned.
The literature on ELG -handcs of INH is quite sparse. Few studies in-clude the EEG as a p.,-4::mm-tec. Nv ipecific change appears other tlhan one re-port of increased amplitude Yf occipitat alpha and front41 s~iking. 3 2 Tri-phasic waves were seen, buL chv patient also had cxrchosis. A photoniyo-clonic or photoconv•ls.,Lv :,uFase has already been voteJ.,'ý 71 A loweredthreshold here is tnlm onLv CUOLL that mig~ht be attributed to INH.
Other findings , , -pe.;•epced :.n seizures iromi any Cause and oc-curred in subjtccb experienk.ing, 6eizures. They iaciude paroxysma. slow-ing, 5 7 60 64 six anu 14 poSiitiva spikes, 7 0 unchqracteLized patterns consis-tent with seizures. '2 £.orL i rheta 7 0 9' and a temporal focus (ofspikes?)'2 are noted ouL xmaN resuit from anoxia. due to the seizures ratherthan INH. Sharp tI~tAI ,ie: ru:,ng ,coxyswal dischirges described in thisgroup as part of an aie.-gic reacLLQ' miy have a aidtcront significance."
Even less iiceratur: exisc. uu v;.ual evoked potential changes. A de-crease in threshold or rctponse Lu auuiturv and visual stimuli has beennoted previously.7' > T i: a1 iso seen in b6 deficiency. - A changein the evoked poCenuai. U:ouiG rDe expected, but this poinL has not been
12

studied. To the author's knowledge, no study of the evoked potential inINH exists.
A few additional interesting reports are worthy of note. In ratsgiven. enough INH to result in peripheral neuropathy a decremental responseis seen on the electromyogram.' 0 This implies, decreased myoneural trans-mission and 'needs to be considered in the workup of myastherria gravis.Spastic'ity, although a rare complication, may be a presenting feature of INHside effects.
In addition to the side effects, an allergic reaction has been reportedwith INH. Burning and flushing are a feature of this. 8 4
Finally, clinicians need to recall that many of the phenomena of INNmay'be duplicated by the disease for which it is given, tuberculosis. Anexcellent review of some of the more unusual presenting features of TB arepresented by Kocen and Parsons.47
13

TABLE 1
REPORTED SIDE EFFECTS OF ZNH
I. PERIPHERAL NEUROPATHY
**Paresthesia 8 9 19 26 30 31 8P 69**Numbness 8 9 19 26 30 69**Burning8 9 19 30 89' 6••**Weakness 8 9 19 30 6'8 69 1**Leg Pain8 9
**Calf Tenderness 8 19 89**Decrease Nerve Conduction Time 8 8 69**"Peripheral Neuropathy" 50 66 90 93 95 75
Stiffness8
Hypalgesia 8 19Deep Tenderness 8
Decreased Vibration Sense Distally8 19 30Atrophy
8
Fasiculations8
Prickling Pain 1 9
Hyporeflexia8
Decreased Position Sense'Hypesthesia
8 19 30
II. CRANIAL NEUROPATHY
**Optic Neuritis & Optic AtrophyZ 42 (4 32*Decreased Corneal Reflex 1 3
*Dilated Pupils 1 3 70 94?*Constructed Pupils44-*Decreased Pupillary Light Reflex2 3 13 80 44i**Iridoplegia 2
**Cycloplegia2*Blurring of Disc69 32 64
BurnLng in Face 1 9
III. AUTONOMIC DISORDERS
Postural Hypotensiont'**Flushing]9 96
*Reported with ovecdose only**Dose of 5 mg/kg/day or less in humans
14

TABLE I.
REPORTED SIDE EFFECTS OF INH (Continued)-
ýDryness oqf MouthP8 73
Synco'pý.95
**Diffictilty with Urination95 96Tachycardia:,75
*,Irregiiiar p'ilsd7 6
Bradycardia69 33
Sweating1 9
IV. VESTIBULO CEREBELLAR DISORDERS
*ty~ertigo2 G 34 414 32 48 33 73**Giiddiner~sGb**Dizziness 2 6 34 42 75 48 96
Ataxia49 75 76 44 69 32 33*Intention Tremor49 48
Tinnitis"~ 32Dysarthria10
Decrea~sed Fine Coordination of Hands19
*Nys tagmus80
V. ONS STIMULATION
**Hyperreflexia8 80 48 73 1 95 96**Clonus 8O 1**Seizuresl 23 42 46 50 51 13 62 68 70 71 75 76 77 79 80 90 9~4
101 44 32 48 33 57 73 29 45S 1 95**Tremors7 69 33 96
Hyperventilation914 693Respiratory Dites9
**-wirchin If 101 69 32 ;ý3 73 95 96
**Insomnia93 101 414 69 95Lower Sensory Thre'shold7 ,
**Restlessness8O 94 1(#' 69 95 96Excitability76
**Spasticityl*Running Movement (Animals)7f,
**NervouslOl 95 96**Involunltary Movements1
15

TABLE 1
REPORTED SIDE EFFECTS OF INH (Continued)
VI.1 CNS DEPRESSION
Stupor"'2 75 32**Lethargy 3 31 46 13 75 90 94 44 32 33 96
,Coma1O 23 46 68 90 103 44 45*Respiratory Depression 1 3 76 90 41 69
**Pyramidal Tract Signs 1 0 1*Hyporeflexial 3 70 94 44
**Decreased Superficial Reflexes1
**Paraplegial
VII. MENTAL CHANGES
**ConfusioniO 75 85 101 69 32 99 1**Psychosis4 2 51 75 101 69 32 95**Korsakoff Syndrome]
"Toxic Encaphalopathy•"4 2 68 32**Disoriented for Time and PlaceI 01
Euphoria4 2 32**Agitation1.Memory Disturbance 80 'tit 32 99
**DeliriumlSeparation of Ideas and Reality 3 2
Loss of Self Control 3 32**Irritability93 101 1 96**Depression101 69 '2 106
"Unbalanced State of Mind"'"I0**Apathy1*Illusion""t
**Hal]ucinationsIl0*lDelus.Lon44
**IrraLiona. 1•**Incoherent :0A**Uncoopcracivei i
Personality Change" 9
**Emotional Lability3 1 101
,Decreased IQ3-2
Apprvhensionl' ý'-5**Argumentitivel 01
Premonition of Death 1 9
**Paranoid Ideation1 01 I
16
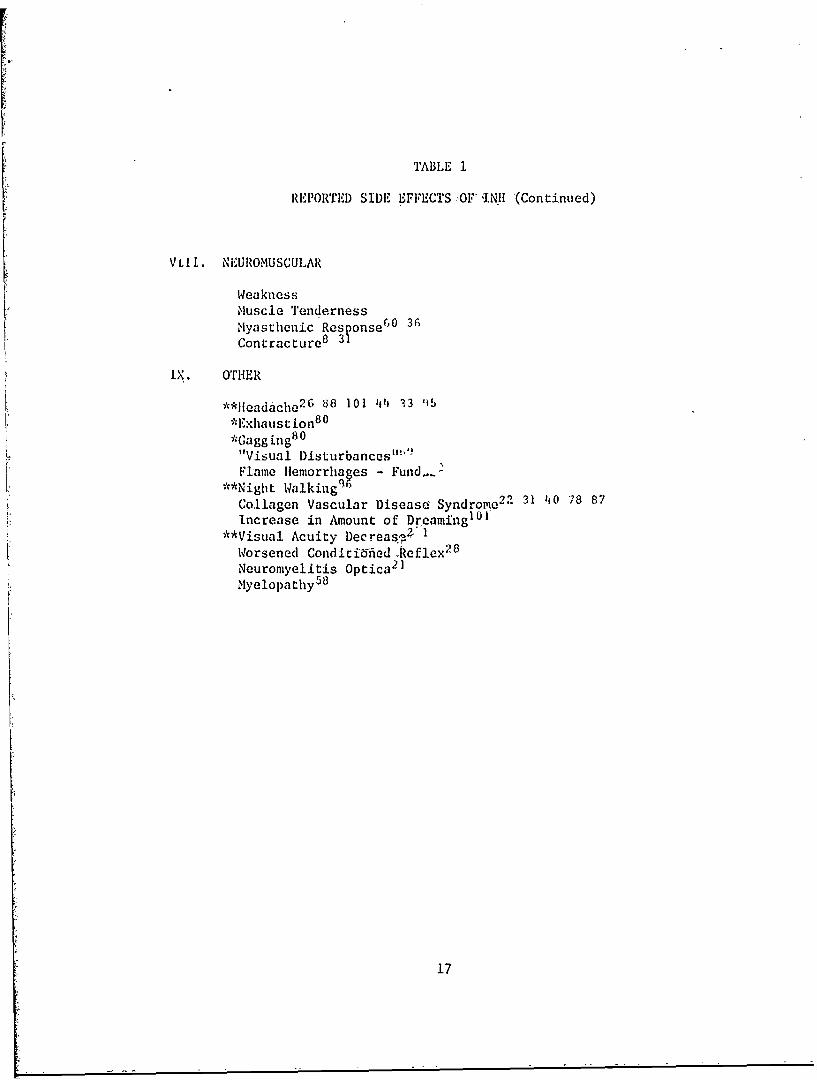
TABLE 1
REPORTED SIDE EFFECTS ,OF INII (Contintied)
V LI. NEUROMUSCULAR
WeaknessMuscle TendernessMyasthenic Res onse6O 30Contractureo 3 '
iX. OTHER
**H1eadache2G 838 101 44 33 115*Exhaust ion 8 0
*Gagging 8 0
"L "Visual Disturbances"'Flame llemorrhages - Fund." .
**Night Walking2 1Collagen Vascular Disease Syndrome 2 2 31 -i0 78 87Increase in Amount of Dreaming1 0 1
**Visual Acuity Decreas.,2Worsened Conditid-ied .Reflex2 8
Neuromyelitis Optica 2 1
Myelopathy58
17

j 0 0 0 0 C'J 0(N 0 CNI
ciuciU u
U) ().3C U)~ ) H
U) I-:1 rq e U) C
a)J 1.0 W kok 0 1041 0
tn~~/ Cl C ) o 0
co~ .t.4 4jt
CeOa) 0 ~c
0 a)I m )UH I 0 ; : 4c
0 ~ ~ ~ ~ -[2H 411i4
U IV)l
~ HK ~~'- *41 41
__ V1 V_ VH4 $
$4 14 N rd N (:44 ri-ri r- ri F
C) Q) 0 41
V) VH
)-4 i toIV;to8

$4 4) 44 ;4 T
4) w ) Lo wi w) w 120 1 > i' $4a > ~ 14 > 1 >u 0 r 0 4 30J0JN 0 0 0 $
4) 0 U 0 > Li rq tU V Ul
o C4 N i CAi-Cf rn u (a
U'H ( (A U C))C
~PQ ~ 41 4.)~~ .
200) 0H C: 1 C: z01 0i 41 H J
t r= -i -:4 * 4j rq P. 4JJr4 ~ ~ u .
4J. 41 W -H 0. 'r- 'd H 44 *r-4 m41
H1 '>.r0 . C'.~ t>1 >, M. EJ-(4 0. >~4J p > m
000 4H
to E-4 x 0. r0 u a).44 C)
00 :J 4 ) ( (
aOWt Ci 4~J 00~4a 0~ COo W up4 1
ý- CO 44 4 C$4 060 W
a1~H ) C0P. U 'Hi 4.4
0 __H_ W___ 0
4J30L)O
0 0UJ $4 ) 4-1S-0.j -L 01 00 C
PI Uo H co'
01 00 -. 4
H u P H) 1.4 UUw rj $4 Cn
rC i 0 41lu Q1 H)41
-14~O' C4 g.!e1 H1 E' Hý
01)cs 04 0
L In or-i19
8. 0) w ~ 0 00 > >~u 0 ~ 00
:j
re, 44 0) ce
~0 0 d ) 00 -?
:) - H 0) (aU tq~ :07- z*,-4 t0 4 41 c U 4 41 "dH *41 0 41u 9>ýJJ C - Pw q Ui -r U)4Jq 4 V cn -0cl r-i 4 (~~~~~.0*,-40com -q . O 0 4 comH r40oZ c ap )-cc-4 0 al wH 1 c 0H w H .J 41 ujq W~0 *. > d'O -r4, M >
z Ha))
cc~0 4
*.f- 4J UI) H 0)
H r
z Uo 0 H 0.
CL Q
HC) 0
S C$)
WC/ 0 H)0ir H
W) 0) D : zoUm)0 001 0 0)0 q ) 0 41
LO V) u0 P40 Ad O U J O
00 NH 41a) O -. :3
0d0 00 0 H ) ~C C)2 ' C*MU
U0> w~ 0=00* Q) > 4 0
V0 C4 " 41U') . 4.)u
%0 44
20
Cl 44 4 I I
r .)
co rq0 ) C: ) C- H -
0. CJq 4)C . oIir4 .0 conl -!1, to -4ji $4 WJ.J 0 41J 0W 'w 1
;> ,c ma co c i cd f
E-4 9z pq 04 =
zH
00 00r..
H 60 rC) zi
r_:j 4 Hz 0) (1-A$
0 H4 -H j C
o~ 0 (o4 C
CC 4
C'.4 41a --4--0C (L) 4)C
~P H 40ClrWP
0 0
Oo CoC14 1-1 C
Cl I ~ ~ C 'I
CC Wi 0
Preo
STUDY 1.
NEUROLOGICAL EXAMINATION AND' CLINICAL NEUROLOGICAL EXAMINATION
PROCEDURE
History - Subjects were asked tocoumplete a prepared questionnaire whichcontaified questions relating to all the neurological side effects of INH.Subsequent interviews were held with.each subject to define further anyanswer suggesting relevant symptomatology.
Neurological Examination - The neurological examination consisted of ninesubtests as4detailed below:
1. Autonomic Nervous Systr-m FUnction " Autonomic nervous system fund-tion was evaluated by measuring the resting vital signs after lying at least30 seconds, the vital signs immediately after rapid assumption of the stand-ing& position and by inspection of the mucous membranes.
2. Reflexes - All the usual deep. tendon reflexes and all four abdominalreflexes were elicited and graded on a scale of -4 to +4 (-4 = no response,,0 = n6rmal and +4 = sustained clonus). The plantar response was recorded.
3. Sensory Nervous System Function - Pain and light touch sensibilitywere evaluated in ail dermatomes. Vibration and proprioception were eval-uated bilaterally ,at the level of the great toe.
4. Cranial Nerve function - The function of all the cranial nervesexcept the first was tested including a fundoscopic examination.
5. Muscle Powvr - Distal muscle power was eva& .ated by testing theinterosseous, toe dor.iflexor, flexor digitorum profundus and superficialis,pronation and suppination function bilaterally; proximal muscle power byforearm flexion ann e:•tension, as described below. The results were gradedon a scale of 0-i00/ (04" is no measuraole contraction, 50% is just enoughpower to overcome ýihc force of gravity and 100% is the full power an indi-vidual of comparable "ge would possess),
6. Functional Te1sS - T'emicag wai accomplished by having subjectsstand and hop first on one foot and then stand on the toes of that samefoot. This was done for both thu left and right foot. The time requiredto do 20 pushups and 20 deep knee bends was recorded. If the subjects wereunable to do 20 pushups the number they could do was recorded. Finally,
22

the subject was required to lie: supine ind maintain all limbs at a 450
angle from th6 horizontalposition. The limbs were not allowed-to contacteach other, and the knee aad elbow joints had t
a had o be in full extiension. Thesubject was timed fr6m-,,the dnset to the point where any limb touched theexamining table and this time recorded. Observation for muscle twitchingwas done at all times.
7. Cerebellar Function - Cerebellgr function was evaluated by the
finger to nose test, ability to mako iapid alterisating movements, the Rhom-
berg Test, observation for nystagtG'; and' intention tremor and by observation.of responses in the oatler tests whidh bear on carebellar function.
8. Gait - The subjects were observed, while ambulating normally. with
eyes open and eyes closed. Heel, toe and tandem walking was observed,.
9. Handwriting - Subjects were -asked to copy a few sentences from t,,i-
terial which remained the same at each evaluation. This test was designed
to assess handwriting and observational accuracy.
10. Peripheral Neuropathy - Evidence for the existence of peripheral
neuropathy was derived from four areas: Dc.-sed deep tendon reflexes,
corresponding muscle weakness, corresponding seusory complaints and ,.orres-
ponding symptoms. Changes were required in two of these four areas before
a subject was considered for a diagnosis,
DATA ANALYSIS
Each of the measures taken in this study was compared at 6 and 2months, for each subject, to his pre-dzug baseline, measure in order to
determine the presence or absence of a clinical change. In most cases a
progressive increase or decrease was required.
When either the 6 or 12 month exam showed more c]l.iCally notable
findings or when several measures at one examination period showed a pat-
tern which, when considered together, suggescs a valid clinical problem a
change was recorded.
An attempt was made subjectively to assess thu relationship ("subjec-
tive correlacion") between various c.,inical measures, the kitamin B6 admin-
istration, system involvement and the INH inactivation levels.
"Multiple system involvement" means that the subject showed a change
in more than one subtest.
22

The INH inactivation levels were determined as part of the overallstudy done by Shub, et. al. 8 6 Each subject was classified as a rapid, slowor intermediate inactivator.
RESULTS
History - The subjective symptoms reported by the subjects in Ehe question-naire and in the subsequent interviews are summarized in Table 3. All symp-toms reported are listed along with the number of subjects reporting the
.symptom, their mean age and the percentage. of the total group represented.The last column shows uhe number of subjects, with neuri ,l i findings re-lated to the symptom. These are called associated find',,o,- Associatedmeans a symptom 'which would be expected to occur with a particular diseaseprocess and probably related to it. For example, paresthesias would beconsidered an associated symptom of peripheral neuropathy.
The mean age of the 17 subjects with, symptoms was 46.7 compared to tliemean age of the entire group which was' 47.2. This difference -was not stamtistically significant.
Inspection of the table reveals that the deviations of the meanl age ofthe subjects reporting various symptoms, from the mean age of the group arein the directions expected for the nature of the symptom. An exception tothis was in the case of blurring of vision. It would be anticipated thatolder subjects would report more blurring but the data reveal that 14.3% ofthe subjects reportea this, symptom and had a mean age two years below thegroup mean.
Paresthesia w'as the most frequent symptom by far (28.6%). Almost 40/of the group with associated neurological findings, were represented by thesubjects with paresthesias.
Autonomic Nervous System Function - Definite orthostatic changes in vitalsigns occurred in two subjects. In one subject this change was seen onlyat the six month exam. The changes in the remaining subjects were withinnormal limits.
Reflexes - As mentioned previously reflexes were graded on a scale from-4 to +4. All subjects showed some variation in grading. For this reasona difference of t3 from baseline had to be reached or maintained in accor-dance with, wae criter.za outlined :in the data analysis section.
Nineteen (19) subjects showed reflex ch'anges in accordance with thesecriteria. Eighteen (18) showed decreases and one showed an increase. Twoof the 19 subjects showed reflex changes only at the six month exam. All
24"

Qc .1 Lro
:30 w~)
0 .0AJ~i 44.
;4 0r d0C4H I- i
(j) *r-4l0
0) 00 00 fC! S'riC1 n n% % 1%0 I
4J 4J 4-4
0 E! 4J
U 41
r. 0 (10 0~0fC
010
()0 U) 040)H141 4J 0 C:
0) 0;* 0
E-4 0..' ) C,~'
od0 0 (.0'r
tq0 0 U)
0~4- 0 J 00U0 04-Jt24C
-u 00H4 0r 0 to
r40 z 0 010 03 rd In' 0 0 0 -
0 1 C 0 ;> 'H > w~w~ U) 4 m) U0)0z
4 0.4 'r JE4)'r4 ) 0 _0 -CYu) 0 U) U 0'p
CI U) cn a U) 0 :3 U) 0) >1 0- P4 ZJ U -4 4 ~J 0 0 Cdj(nC% 14 o F 'i 4 0' 'a li I ý z oZ J4
0) C Ic H0 u".:1p ý 0 p 05 -j0) U
CO~ ~~~~~~~~~U $4 0 )M0ZWri0 H- .W0, 4
LA 0) AU 4-j m
HHr-l rl-jiJ '
25

these" changes were marginal ,or "suggestive" and would not be consideredsignificant in the-usual clinical situation.
Three subjects showed reflex asymmetry, two in the abdominal and onein the brachioradialas and ankle jerk.
Sensory Nervous System Function - Two subjects showed hypesthesia. In onesubject this was located in the anterior tibial area only and in the otherit was located in the distal leg. No subjects showed decrease in iig: ttouch sensation. Eight subjects showed decrease in vibration sense and sixshowed decrease in proprioception.
Of the subjects chac showed sensory changes, five had changes inmmorethan one modality.
In all,, 11 subjects showed changes in sensation. in tlhrce subjects thechange was noted only at the six month exam, and in one ani± at tne 12 monthexam.
These findings were barely detectable and in and of themselves wouldnot be considered its rupre-3entative of clinical difficulty.
Cranial Nerve Functiot - No stoject showed any detectable change in cranialnerve function on trr- c.iiical exam.
Eighth cranial nerve iunecion was evaluated on all subjects by Shub,et. al., 8 6 using au"o~o:,a•, •ni ice water calorics. Two subjects hadtinnitus. The zinr-iLiiY one subject showed marked progression and changeswere noted on his "uai,. anu ice water calorics. For this reason, thissubject was considered to ,,awt 8th nerve involvement. This was the onlyincident of any cranial aoe've involvement noted.
Muscle Power - .,even buojeCts bnowed decrease in muscle strength. Of these,five were consi-..ireu to be a possible clinical change; "possible" in Chat nosubjects approached a level of weakness that would be indicative oi clinicaldisease.
In the otnef Lwo case.- the scores were indicative of a change but werewithin the range o. 6cozing ecror and, therefore, could be no more than nor-mal. variation. bnc, .1 OotDC exists, these cases have been included.
The weakne iz aotuL was ulifuse in five cases and localized to the armin one case. One subject showed only proximal weakness.
In all cases except one, the weakness was persistent throughout thestudy.
26

Functional Tests - The role of the functional muscle tests was to provideadditional information on muscle power. The results paralleled those, foundin the conventional muscle power tests.
Cerebellar Function - Eight subjccts showed 6cme finding, on the cereb.?J.lartesting. The findings consisted of an unsteady )hoiiberg in four, intentionitremor in five, drifting of the arms in two apeo dysdiado':hoklnesia in one.One of the eight subjects had cerebellar fin6i,tgs only at the six monthexam. One other subject showed an unsteady Rhowberg ot. the six month examonly, but had intention tremor at the six ao'. 12 mont.. exam.
Three of these eight subjec-ts showed a mna3'ud,. of change great enoughthat a clinical impression of "bossible" cereLeiJ1.:r j,-,fronction was dranm.In the remaining five subjects a "chanb.c" was flu.-u which co,!,Id easily haverepresented a variation of normal.
Nystagmus was seen in four sublects. J, .<;J , the nystarmus wajmore than just end point nystagmus. I: t: ,,. ciL-, , ,o subjects,present only at 12 months in one, and p,-.en- o-aiy -t sixý months in the
other.
The nystagmius was horizontal bf -A,) .. t xt ia the subject withnystagmus at six months only, where it w+s vunLiua ano obLique.
The findiag of nystagmus wus considered i :al'id clinical change in allthe cases except the subject: with nyý.tagmis tt 1. iionthý.. In that case itwas merely considered as suggestive and aol -urchv j. further considerationdue to thu small magnx'ude of the finding jau tite ,of Ippearance.
Gait - No abc.ormalities of gait were roteo i- i- .., subbect.
fianowritinr - Analysis of the hadv tieiu •,r,!l c r.aiti Ivo consistentchange in accuracy of motor c-,) odut-L.Loni -it,-.'C •nDGt,,' tdalI or iln thegroup as a wnoie.
A sumiaary of the findings and symp.,omns c eaoh ,.mbjcc- will be foundin Apuend.x 1. 'fable 4 ineJudes only 0,t',V e,1a•, .c were V o,asidered
to be 'poS,,.ibl.," changes add ,xclud . , '., were mei,' e+iiid is changeswithin the r,.age of corai vakciation, . wv.-., "marginal"
cnan~es, cha; %iitairn the range of scortng -iL; uk "vhi ;t." The
findings 6ua•riarized in Table 4 ace those~ whici ,oe ildicated in AppendixI with i dark llne.
The question still remainec about -1, .,.At,., ! -1, ,,il. .ioLTiizing these
findings in t•iJc. manner. An assumptic-a -.. , d 'r , i valld clinical

-00
EU ;W - r
a41 C
*t0 I -uN I ~H I 0
0U)
z
4)~ '03 00 co %Do 0z ~ -~'~ L.n- - -T - n
u H(
N -H H is -s ON r- In)
0i >i f- N4 0 0 0* cnH ~j H Hi b~ H H H
~-H H
UU
~o )U.4 4J,
0. O'3 N C Ci I)C0.
0 U
JJ CJ
C) 0 +) U
t >1zq co +- ) 1
041-
-w w H4 cw >1 H 41
0. Z- co
2 8

change occurred it should be accompanied• by associated symptoms. Therefore,the "possible" changes were compared tO the more questionable changes in re-spect to associated symptoms. It was found that there were no associatedsymptoms with any "questionable" finding and that all the associated symptomswere in the group of subjects with "possible" findings. This finding lentsome credence to the dichotomy of "cnanges."
Table 4 should not be construed ar' '.esenting definite clinicalchanges, because the findings report e dre r extremely small magnitude andmight better be denoted as "subclini, a1" ftnd. ;s. No LI)Jnges which wouldbe expected to cause difficulty with occupatioi 1I or daily activities werefound.
Nine (9) subjects •(32.1%) were fr Ac L_ ..CVQ some evidence of periph-eral neuropathy. In six of these cas-s (21.4%) this evidunce was insuffi-cient to make a diagnosis of anything other tian "evidence for peripheralneuropathy." In the other three (10.7%) caseý more evidence was present,but the magnitude of this evidence was still insufficient to make a firmclinical diagnosis. These cases are therefore refe•rred to as "possibleneuropathy," and are described below.
Subject 20: The subject had marked progression of vibration andproprioceptive loss, far more apparent than in other cases. He also de-veloped deep tendon reflex asymmetry and an unsteady Rhomberg. Althoughthere were no subjective complaints, the !ýensory I,.ogrcssion was so com-pelling that a diagnosis of "possible neuro;'athy" was made.
Subject 26: Weakness and a decreased %;bratory sense were seenon the neurological exam. Paresthesias developed ,aite early and wererelieved by Vitamin 86. Primarily because ok thib istory, the diagnosiswas made.
Subject 13: Although a few physici f Lndingr we-,:, present, theyappeared to be time-related to rather severe iý It,-sis Vich were com-pletely reversed with B6. The diagnosis was raauwe kIsiazLily on the samegrounds as it was for subject 26.
Unfortunately, neither ,ubj.ct I iýuo z ':a ... ocn "t the timeof his greatest difficulty when a ,o poz w.e i, i .ight have beenpossible.
As in the case of symptomatology an a;. -. 'tot , 2-atae to determine ifthe mean age ot the subjects with the vofio tyc, -" rindings differedfrom the group mean. The greatest diitefunct. foun,' that the group
_4

with cerebellar findings was alm-ost four years younger than the mean.Although this difference appeared significant, the small number of sub-jects precluded statistical testing.
The mean age of the subjects with "evidence" of neuropathy was almostthree years above rbe group mean. However, this difference is not main-tained in the case of subjects with "possible" neuropathy who are slightlyyounger than the group mean. Therefore, it appears that there is no con-sistent relationshir between age and neuropathy.
The mean age of all che subjects with findings (those listed on Table4) was 47.8 years, 0.6 years above the mean. This difference was not sta-tistically significant.
Table 4 shows the number of subjects with associated Ond non-associ-ated symptoms. Approximately 50% of the subjects in each category ofneurological findings had associated symptoms.
Several subjectb ihad involvement of more than one system (See Appendix1). The data on multiple system involvement are summarized in Table 5. Itmight be expected that older subjects would show a greater tendency towardmultiple system involvement. However, this did not seem to be the caseconsidering the mean ages. There was a tendency for the mean age to in-crease from one- to two-system involvement. The failure to maintain thistrend may be due to the small number of subjects with three systems involved.
The symptoms and signs are also, noted- i• Table 5. Table 5 indicatesthat most subjects showed involvement of only one systam. The total numberof signs and symptoms was also greatest in the one-system grop. The datado not indicate that involvement of multiple systems is accompanied bygreater numbers of either signs or symptoms.
Although not detailed in the table, certain individuai signs and symp-toms were predominantly concentrated in one group. The two-Eystem grouphad most of the paresthes.as. Weakness;i both subjectivc and objective, wasalso most prevalent in this group. All the orthostaLic findings were inthe one-system group.
Ten subjects (35.7%) Look Vitamin B6. These subjectb accounted for38% of the neurolo.ic-al findings and 41% of the symptoms. The differencesin percentage figurc' were insufficient to permit a conclusion that thisgroup differred from the rest of the subject population. This assumesthat symptoms and findings should be randomly distributed among the sub-jects.
30.

TABLE 5
MULTIPLE SYSTEM INVOLVEMENT
NO. OF SYSTEMS INVOLVED
__2 3
LNo. of Subjects 9 (56%) 5 (31%) 2 (13%)
Mean Age 45.4 51.4 45.5
No. of Symptoms 10 (42%) 12 (50%) 2 (8%)
No. of Neurological Findings 10 (38%) 10 (38%) 6 (23%)
Total No. of Signs & Symptoms 36 (50%) 26 (37%) 9 (13%)
No. on Vitamin B6 2 4 0
31
The assumption was applied tO each individual sign and symptom sincelumping them together may have obscured more specific effccts. This meansthat one out of three subjects with any finding or symptom would be takingB6. This distribution was found in all cases except: None of the sub-jects with cerebellar findings, only one of the foir subjects with blurr-ing, none of the subjects with back paini and only ,ne of the six subjectswith "evidence" of neuropathy were taking B6.
Another way of looking at the effects of B6 is to see if there is anycorrelation between the administration of B6 and a change in a finding orsymptom. This was found in three cases: Two of the three subjects •with"possible" neuropathy and one subject with weakness. RIprovement wasreported in all three cases when B6 was taken,
The eff~ect of B6 on multiple system involvement was vxamined. Table5 shows that none of the subjecrs• with three-system involvement were tal:ingB6, but four of the five with ewo-system involvemenc were. Tha Lrýonsietef,nature of these findings and 0the small number of subjectL invoivud precludeany definite conclusions.
Since INH inactivat±on patterns were unavailable in many cases, thedata are insufficient to postulate any correlations betweea INK levels andclinical difficulties. However, a few findings of Lnterest are uoted. Twiceas many of the symptomatic 5ubjects with known INH inactivation patterns wereslow inactivators as fast or intermediate; two of the three subjects withpossible neuropathy were rapid inactivators. In the remaining measurea, thLnumber of subjects with rapid, slow and intermediate inactivation patternswere about equal.
The time of appearance of symptoms and signs was studied. The resultsare presented in Table 6. It will be noted that all the neurologic find-ings were seen by six months and three quarters were persistent and thatnearly all the symptoms were noted by six months but most were not persis-tent. In both cases very little was noted ar 12 months. Blurring of visionwas the only symptom or sign which did not follow che gener•al rule of ap-pearing at six months. One subject of three with blurring; e;xperienced itat six months; two of tne three experienced it initially at 12 months.
DISCUSSION
The most frequent 6ympto,01us was paresthesias wh;.ch was reported by 29%of the subjects. Thc 6mosc iequernt sign was peripherai neuropathy, foundin 32% of the subjects. Oth.±r studies have also reporttcd leov a' Uie mostfrequent sign and symptoms actisough the incidence figures 2ported in thepresent study are higher than generally reported.

TABLE 6
'TIME AND APPEARANCE OF NEUROLOGICAL FINDINGS AND SYMPTOMS
TIME NOTED
6 Mos. Only 6 & 12 Mos. 12 Mos. Only
Neurological Findings 3 (25%) 9 (75%)
Symptoms 17 (55%) 9 (29%) 5 (16%)
33,

The literature indicates that when minimal,changes are sought, inci-dence figures will increase. The reason for this is obvious. The clinicalfindings in this study were indeed minimal. Because of this. it is possiblethat experimenter error was introduced which could account for some of thechanges seen.
Very few studies in the literature indicare the amount of clinicalchange accepted as a valid change or the minuteness of the effort employedin examination. Consequently, it is impossible to compare directly theincidence figures in this study to other studies. Assuming that the pres-ent study employed greater scrutiny, the higher figures would be understand-able.
A second possible reason why the incidence figures in this study arehigher than those previously reported is that the subjects in this studywere older. It is frequently pointed out in the literature that higherfrequency of side effects is associated with older age.
A third possibility is the fact that the subject population. in thisstudy consisted solely of aviators. Part of the character traits of avia-tors might cause them to react differently to minor changes in their phys-iology (i.e., they may show more concern about their health). In addition,
the demands of the aviation environment would be expected to accentuateminor clinical abnormalities.
On the other hand, Army flight surgeons know that aviators flying forthe military are very reluctant to report medical problems for fear of beinggrounded. This is especially important in the case of our subjects whoselivelihood is dependent on flying. This factor may have worked to bias theincidence figures in a conservative direction.
Another possible conservative bias operating in this study was the in-completeness of the examination. Certainly it cannot be said that it wascomplete, and it might better be termed a screenin6 examination. The lim-ited time allotted for examination of the subjects precluded the use of amore complete clinical assessment, but it was felt thaL the examinationemployed at least sampled the major areas of neurological involvement.
Since the literature indicates that older subjects would be expectedto develop more clinical problems while taking INH, an attempt was made inthis study to find correlation between age and various symptoms and signs.No obvious correlation was found. There were some trends noted in the ex-,pected direction. The negative correlation found between age and cerebellarfinding and non-specific CNS symptoms was unexpected.
Any attempt to establish a definite relationship between age and these
34

measures in this study suffers 'from two limitations: Marked attenuation ofthe age range of the subjects and the small number of subjects at each ageand in each clinical category.
The literature amply demonstrates an ameliorating effect of Vitamin B6on the side effects of INH. Since the intent of this study was not inves-tigation of felationship of B6 to INH, our subject should not have been"allowed to take B6 without a clinical indication. lHowever, as mentionedpreviously, 35% of the group were taking it and the administration was notclosely controlled so that the dosage and total amount taken was not knownin most cases.
Normally these subjects would be eliminated from the study. It wasdecided, however, to include them and attempt tv study the effects of B6.
Study of the data revealed no clear differences between the grouptaking B6 and the remaining subjects. However, in three cases, the sub-jects reported an amelioration of symptoms related to BM. These were twocases of possible neuropathy and one case of weakness.
A proper design for study of this problem would have included a randomselection of the group designated to take B6. This was not the case in thisstudy. It is known that subjects who received B6 received it because ofclinical symptomatology, although the nature of the complaint and the re-sults of the B6 are not known. Taken together, thase facts preclude anydefinitive statemeht about B6 effects in this study.
Correlation of INH inactivation patterns and other muasures taken wasalso attempted. It is wel l known that individuals with slow inactivationpatterns have more side effects. Confirmation of this fact was nat obtainadbecause of the marked incompleteness of the cata collection. This situationresulted from the fact that the support laboratory ,L up)ped making INRH de-terminations and from the fact that many of the Known inactivation patternswere in subjects with no symptoms or signs.
Review of the literature revealed that many authurb studied the clin-ical effects of INk in many ways, but none ýt the sti~die& employed a dataanalysis technique based on the number of ,,vstems involvvd. It was hy-pothesized in the present study thaL multipl,ý system invwlvement might becorrelated with other clinical measures. This hypothesis did not receiveany support from the data.
While there were nine subjects that showed sign: and/or symptoms ofperipheral neuropathy, it must be kept in mind thaL six of these had whatcould only be described as "evidence" of peripheral neuropathy. Thesecases are equivalent to findings in other systems conbidered as marginal
35

but are included with the data on possible' changes because of the high inaterest of most readers in neuropathy related to INH.
The significance of the three cases of "possib-3'" neuropathy and thesix cases of "evidence" of neuropathy cannot be ascertained due to the, lackof a suitable non-drug control group and the ' ack of data on the variationsof the neurological findings over the course of a year.
The validity of classifying subjects as "possible" or "evidence" ofneuropathy on the Vasis of marginal findings or symptoms primarily mightbe questioned. Previous studies have provided support for this procedure.The normal progression of disease is that subjects. first have symptomsalone, then symptoms plus marginal findings, then symptoms plus definitefindings.8 14 A Studies on INH have shown that by the time symptomsoccur, structural damage is present. The study by Simmons and Ambler 8 8
supported ,this, since slowing of nerve conduction time was seen at thisstage.
A nerve conduction time would have been the most helpful measure chatcould have been added to this study. Inclusion of these data W6ald havepermitted a much more positive diagnosis of neu~opathy and permitted acorrelation of the data from this study with the data from other studies.Although inclusion of this measure was strongly desired, thb logistics ofthe overall study did not permit this.
In view of the above, it does not seem unwarranted, to suggest thatthe diagnosis is justified in the three cases of "possible" neuropathy.
-One subject had father definite scapular paresthesias and part ofthe history suggested radiculopathy. A paucity of findings was presenton physical exam. Devadalta, et. al., 1 9 report a similar case. Thisraises the suggestion that scapular paresthesias may represent a more un-usual and overlooked side effect of !NH.
Nearty all the signs and symptoms were noted at the six month examin good agreement w:Lth the literature. The fact that symptoms appearedto be largely transitory also agrees with the literature, but then theclinical findings shQuld parallel the symptoms. The results of this studydo not show this to be the case. No simple explanation is readily apparent.
The operation of any of several factors is possible. The clinicalfindings may have been overinterpreted at both the six and 12 month exam-ination. The symptoms n'ay have been spuriously elevated at six months ordecreased at 12 months. It is also possible that the clinical findingsrepresented pathology due to INH and that the subjects had adapted so thatat 12 months they were less aware of their difficulties.
36

Blurring of vision appeared to be a unique symptom. It stood• outfrom the other symptoms in its delayed development. Wrnile the data sug-gest that the latency of development of visual blurring may be prolongedover other symptoms, the number of subjects involved does not permit thisconclusion. If all four of the subjects with blurring developed it at 12months,. perhaps more could be said.
Two subjects volunteered a history of alcoholism. While the side ef-fects in these individuals were not particularly greater than the rest of•the group, in, contrast to what the literature would suggest, no conclusionsregarding the interactions of alcohol and INH are justified from data withonly two subjects involved.
Thi! study was an "experiment of opportunity" and certain limitationsand deficiencies in the experimental dezign were univoidable. Several prob-lem areas were encountered in analyzing the data. These have been alludedto previously and will be summarized here.
The lack of adequate control data was one of the principle obstaclesin data interpretation. This resulted partially from the absence of a non-d'ug control group. Of greater importance perhapa is the fact that onlyone examination served as the baseline for all parameters. In order toadequately establish the true baseline plus the repeatability .of the mea-sures, more control exams should have been done. This is particularlyapplicable in the area of EEG and eVokedl -p-tential where considerablevariability is known to exist. For examnple, it is not possible to identifyand label the individual deflections of the evoked potent~ial with certaintywithout these repeated baseline measures. Only one baseline examinationwas obtainable due to the clirvical indications for prompt initiation oftherapy.
The second major problem area over which the authors had no controlwas the fact that iýý S.pervision of the adminiscration of the INH was ex-ercised. Subjects were merely given a supply of Li131 with instructions.In some cases the assurance that directions were followed was in question.
A third factor which could have been oF ixuza! 1;istanee in data in-terpretation would be follow-up data aftc: tM•e subjecLs discontinued INH.Most subjects were not available for furLher c.
Several neurological signs ind sy.iptoms are reported in subjectstaking INH in this study. Although the incidutce figures are high in
3-7

some cases, in all cases but one they represented subclinical difficulties.No definite evidence was found to support the idea of restricting flyingduties when INH is taken.

STUDY 2
MENTAL STATUS EXAMINATION
PROCEDURE
Three mental status tests were performed--serial subtraction, oralrecall and judgment. Although these and other similar tests are not stan-dardized, they are part of a cofiplete neurological examination.
Serial Subtraction - Subjects were instructed to begin at 100 and subtractby 7 serially and progress to zero. They vere instructed to perform thismentally and give the examiner the answer for ejch subtraction. The re-sponses were recorded along with the time required.
A score of one point was awarded for each correct answer given by thesubject, Points wdre accumulated until an error was committed. For exam-ple, if a subject gave the following sequence: 93-86-79-72-53, his score
would be four.
Oral Recall - Oral re-call was tested by reading aloud to the subjects aparagraph-containing 26 items of information. The paragraphs were similarin structure but varied in content at each test. The presentation was madein a standardized manner with no repetition of any part. At the 12 month-test a paragraph of 27 items was inadvertently used. Subjects were askedto recall everything they could. A score of one point was given for eachfact recalled correctlyand with the proper association, or for an accept-able synonymous fact, showing retention of the basic nature of the fact.No score was given for any other response.
Judgment - Judgment was tested by present.Lng the subjects withra situa-tional problem. They were requested to relate the idtizon they would takeif placed in that situation. The response was evaluated in terms of theresponses usually obtained, and a rating of normal, dbove normal or belownormal was made.
RLSULTS
Serial Subtraction - The means and standard cieviattoni for the serial sub-traction scores are presented in Table 7. The data for the 6- and 12-monthsubjects are presented separately.
3ý0

Ho coM
0 rq
U) 0 U)
%H 0
0; U) 0UU)
0 co Ui0-
C--zU)4U
M Or- 00

The results indicate a slight improvement ir serial subtraction scoresfrom control to 6 months in both the 6- and 12-month subjects. This im-provement is maintained at 12 months. None of thes, ditfforences were foundto be statistically significant in a one-way clwsiTficatien analysis ofvariance (ANOVA).
The serial subtraction time scores albo .-howea imDrov•;nent from c,,n-trol to 6 months in both subject groups. In the i2-rrntb stibjects the ifrv.-provement was not maintained. These differences were again not statisti-cally significant in an ANOVA. Summary tables or t1•e iNOVA will befound in Appendices 2 and 3.
Oral Recall - Table 7 presents the mean., acod -o.ard deviations of theoral recall test for the 6- and 12-month •,ub-ie(cr. The rr;uits indicaitean improvement in oral recall from control to h o•no•C1:z Iich was not" min-rained at 12 months. A one-way classificariou ANOVA showed a significantdifference in recall scores over trials (p<.Ol). ludividual tests of meanrecall scores showed that the source o; t-,.-i lifforence was that the 6-month scores differed from the control and 12-monk scoree (p<.01) andthat the control and 12-month scores did not differ from ea'Th other (SeeAppendix 5).
An accuracy score was also derived by subtracting the number of syn-onymous answers from the number of correct answers and dividing the dif-ference by the total number recalled. The resulting score was expressedas a percentage.
The mean percent recalled scores for boct the 6- and 12-month sub-jee-s was about 37%. Scores for botn groups paixa.,-eled the results shownfo7 oie raw scores which showed an, incroase ar t, monous. The mean accuracy..cores ranged from 95 to 9r7%. There was no chan•e from tne control scoresin either group.
Judgment - Only two subjects out 01 tMe ent. re gXoup of 28 showed a slightdecrease in judgment over the 12 raoanhs of therapy.
0,I ,4AjSSIOX
Tise ot.J CeCali Lees," was eri- ,! Lc: a,., t o ,m memory andserial recall. Although thle paragraph Sfio1:A ."t ,, p,.L of a stan-dardized test, an attempt was made to eq,,,ce '•.I . , .,pe, and orderof presentation of na.e.', dc-es And ?Lact, tue , n he paragraph(See Appendix 6 for the pnragraphlb eoploycd).
There is no ri adily apparent expiaa P .... , ,ftcant increase
'9

in the 6-month scores which were not maintained. One or both of the follow-ing factors may account for the difference.
First, the 6-month stimulus material may have been less difficultthan the others.
Second, several subjects showed greater interest in this test thanin other mental status tests. This could account for an increase at 6months, out additional explanations would be required to explain the de-crease at 12 months.
4-41

STUDY 3
ELECTROENCEPHAIOGRAPHIC EXAMINATION
METHOD
Apraratus and Procedure - Routine clinical EEG's were performed on a GrassModel 3, eight channel electroencephalograph. Grass cup electrodes wereapplied and secured to the head with bentonite paste aceordinf to the iO-241jInternational System of electrode placement. Seven montages includingmonopolar, bipolar, anterior to posterior, lateral. parasagittal and coron-al runs covering all areas of t~he head were made. The monopolar referenceelectrodes were affixed to tbý-e.ars. Three minutes of hyperventilationwere recorded. The subjects were not sleep deprived and no attempt wasmade to obtain sleep tracings. Attempts were made in all cases to maintainfilter settings of HLF 70, LLF 1.
Data Analysis - Two types of analyses were performed. First, a routine
clinical analysis was done in which the tracings were read as noimal,borderline or abnormal. Second, a subclinical analysis was done in whichmore detailed and quantified measures of the EEG were sought.
For the subclinical analysis, the following criteria were employed:
Delta Rhythm - 0-4, Hz
Theta Rhythm - 4-.8 11%
Well Developed Alpha - Rhythm in the 8-13 H. range whichis more or less sinusoidal, smooth in wavforin and :lear-ly discernible from the other rhythms present. (See Fig-uro 1A.)
Other Alpha - Rhythm in the 8-13 liz range of low amplitude,contaminated with other rhythms, irregular and not clearlyseen. A clear distinction with well dcveloped alpha wasusually obvious. (See Figure lB.)
Beta Rhythm - More than 13 Hz.
Organization - EEG daca often contain several rhythms whichmix or override each other, producing an irregular pattern
A3
FIGURE 1A
WELL DEVELOPED ALPHA
NI 4 -s-- -"•'
I I 4
Si i !
LJL

FIGURE iB
OTHER ALPHA
"Low V ., , ,.
5r
I1•c
"WN ,VV

of frequency and amplitude. On the other hand, there isoften a dominant frequency with little variation in ampli-tude which ýroduces a smooth, regular appearance. Theterm "organization" is used to denote this difference.Thý fi:•t example would be classified as poorly organized;L'e second as well organized.
Focuo - The area where a rhythm is most prominent andhignesc in amplitudeP.
Extent - The total area where a rhythm is seen.
buildup - The EEG response to three minutes of hyper-vcntilation which consists of slowing of frequency andincrease in amplitude.
A~y,=,uc,:, - A uiffereace in EEG patterns over homologousbrain areas. The side containing the greatest degree ofthe paramater is considered to be the side possessingthe asymretry.
Shift - A change in location from one area of a hemisphereto another of an EEC barameter. To be considered a shift,the size of the area had to remain the same.
* Phase 1 - Three typep of ob6ervacions were made on the data inPhase 1. The fir.ýr cif these involved recording the presence of variousfrequencies of asyrLietri',: (right and left) in each channel. In the caseof beta rhythm nearly all channels cuntalneG trequencies in this range.Therefore, only beti.. !iyVCi, whitch was h ghe=r tan the background in am-plitude and stood alona, was counte.d.
ThL seconi invo0veq a forcea choice canking procedure which wasapplied to the data on buildup, organization, .iplitude and the amount ofSeach frequency, ThŽ ior~eci choice ranking involved direct comparison of
each-montage of che control, 6-;4ionch and 12-month record for each subject.
The third involved ten measurements of alpha frequency in thefirst montage (laterai monopoari).
Sumcetime:ý artft•corr !ep ),.:curred throughout a channel. When
this occurred the data were hanciled -cs it the activity in question werepresent, but -no ranklng was done for the montage in which it occurred.

* Phase 2 - In Phase 2 of the analysis the following concept of"change" was employed. Since the 6- and 12-month measures may be higheror lower than control and vary independently of eacn other, many combi[na-tions of conditions may result. Only three were considered in this stud'yas a valid change over the course of therapy.
1. Progressive i.ncrease or decrease.
2. Control and 6-month measures were identical,but the 12-month measure was increased or de-creased.
3. A change from control at six months with thechange persisting at some degree at 12 months(a constant shift).
The data on presence of each frequency and on asymmetries(which were recorded for each channel) were then organized according to
the location on the head. Using this organization the following parameterswere derived: Shifts, determination of focus and extent of focus, deter-mination of extent of the various frequencies. The areas of the head weredefined by the position of the EEG electrodes.
For the data on the forced choice ranking (involving amplitude,organization and amount of each frequency), each montage of each EEG wasclassified as showing a "change" or "no change" according to the followingscheme.
Since there were seven montages in each EEG, many combinationsof scores for each parameter were possible. In order to determine whetheran overall change in the parameter should be noted, all the possible com-binations were listed in descending order from tue situation where allseven montages showed the same change, and an overall change was obvious tothe situation where all montages showed no changu. The number of EEG'sshowing each combination was tabulated as well ab the number of montagesshowing progressive changes in each combination.
in order to determine whether or not aa overall change occurred,a cutoff point was sought. A cutoff was made at tha point where 50% ormore of the montages showed the change. Sinac Laere was no obvious gapthere and since nearly half the number of observations lay below the line,it was decided to search for an additional discriminator. An obvious onewas found and used.
According to this scheme, if a change waF- noted in more than
50% of the montages and two or more of the change- were progressive (12
: .ii

mo > 6 mo > control), an overall change was recorded for the EEG. If not,no change was recorded,.
Since the data on-bijldup involved only one measurement, theseand the data of the third observation involving alpha frequency, were re-corded as a change or no change, according to the definition outlined inthe beginning of this section.
* Phase 3 - In Phase 2 the data were categorized according towhether a change occurred. In Phase 3 the nature of the change was exam-ined (increase or decrease). These determinations were recorded in tabularform for each of the parameters.
The data which were organized according to location on the headwere recorded as a change from one area to another, rather than an increaseor decrease in one area.
Since the EEG electrodes defined a number of subdivisions of thehead in the anterior to posterior direction and since medial or lateralshifts-could occur in any or all subdivisions, several medial-lateral shiftscould occur. Rather than attempting to derive an overall medial-lateralshift measure, a shift was recorded in each area where it occurred.
The nature of this data was such that no meaningful statistical anal-ysis could be performed. Therefore, overall changes in the EEG were con-sidered according to two criteria: (I) More than 50% of the subjectshad to show a change and (2) Since changes in opposite and mutually ex-clusive directions occurred, twice as many subjects had to show a change inone direction as the number of subjects showing a change in the oppositedirection. Both the above criteria had to be met for a change to be con-sidered to have occurred in a given parameter. For example, if eight of 20subjects showed no change in alpha frequency, seven showed an increase andfive showed a decrease, no overall change in alpha frequency would be con-sidered to have occurred. However, if five subjects out of 20 showed nochange in alpha frequency, 11 showed an increase and four showed a decrease,an overall increase in alpha frequency would be recorded.
RESULTS
Clinical - Only one subject showed an EEG abnormality. Two others showedsome abnormality at some time during the study.
The first subject had a normal control EEG. At six months a definiteburst of slow activity was noted, which was labeled "paroxysmal." This is

FIGURE 2
PAROXYSMAL BURSTS OF SUBJECT
F8 FP2 2170
vwvF `IIIIIý3- p ý7 IV
FP2-FPI
FPl-F7
vw
A2-T4
T4-F4
IvW% IN,
IF4- F3
S
i
IF3-T3
ýlF3-Tý3ý
50 PVT T -Al3 1 SEC3-Al
49

illustrated ineoFigure 2. Considerably more buildup was noted on hyperven-tilation at this time. This record was considered suspicious. At 12 months,two paroxysmal bursts of slowing were seen in the resting record and sevTeral more during hyperventilation. This record was considered as "border-line abnormal." Thus, 7ne EEG abnormality was found, yielding an incidenceof 3.6%.
The other subjects th~at showed some abnormality only showed it at oneoi the three, testing periods, The nature of the abnormality in each casewas slowing, at the control EEG in one case, and at the 6-month EEG in theother. All other EEG's on these subjects were normal.
Subclinical - The results of the subclinical analyses are presented inTables 8 to 10. The derivation of this information and definitions ofterms are given in the data analysis section.
In general, the following changes. were noted:
Alpha - There was an increased extent of alpha focus, principallyin the medial and parasagittal areas.
Beta - There was an increased amount seen with no change in ex-tent. More asymmetry was noted. The asymmetry was widespread,'seen inthe frontopolar, frontal, postei~ior temporal and parietal areas. Themedial, lateral and parasagittal areas all demonstrated the increase.
Theta - An increased amount was noted.
Buildup - Buildup was increased in the 6-month group only, al-though the change was noted in 86% of that group.
DISCUSSION
One subject had a clearly abnormal pattern of EEG's in the study.Two other subjects had what would be considered abnornal EEG's, but theywere of a transient nature. It could be argued that these subjects shouldhave been considered to have abnormal patterns. In the clinical domaintransient abnormalities are reported.
However, it was elected not to consider this as an EEG change dueto INH because the EEG is a variable measure within the same subject, andthe transient changes may be reflecting just this. In the one subjectmanifesting a clear progression of change, the possibility of this beinga normal variation was much smaller.
r'

>Ig
0 l r 00
T0 In w ~ 00
0r CO I0 00
In I -T H
r-4
0)10
0),~~~~ 00 0C c00 c' 0oo 0-0 0 00' t
IN %DcJ Clq In N cON '- N. C",
--
44.00
0 1

0IT 0 00 Hi Cl IT00 0 00 c c r-ý a% L
C1~4
0 0 00NICC)C %0..
C) 0 I 0 0) 0 H- 0 1 Cirn C14J 1 1
00
X: OH 00 ON ~ C)-7 LO0 OHr- 00 Or- Vr)0 LI) ONC) CN -.TC' N H r- o l0 % or- Cl) ml r 0' m C-4
CO H
CC) 00
4-ii
X ej
C) p a U')r-q ?-I H H~ oo ) or- r-r N A 0. ~j ri f90 u4 L'~4 t~' - N (C) *tA I)H c- A
0 (D 0~Lu
000 z U)
H IjW 1) 0 N f)r- -L)r- L r L N L Hbcn)4 inN n n l " Y)C4 T n n -i M-,52 -

ýqH H r \0
0 H
.[0 C) C 0 0 1 C-4
C: +1
-- =-
a) H) H C
p
C% ) 00. 0-2 0-? tiI 00-.?- m O 000 O n r-4h'
C 4 .- UI
10 E-4 0(~
- ~ 0 100 LA0 LA.T LAý . 0 T t)0 0-. Cci 00't4j4 4 r4H rI : -. H H- N~ c'4e
0
a)10 0~ 00 90 nCl n13 0C 00-. 00m 00a
00
0q)1
U~ H J
0J Xi 0)4
P4-

00 0 0 I I
* 0 * I I.O r-4 I I
0 0 O
0)
00
0 --0 0,-t
I x
C) 4
0 M
H 0
hi-t
11 0%0 0 0 0 0 inOq% 0 Vmo1 ~o 00 Ln LAn 4 00O
C: 0
LZk0
41 1 N H H 17
00
o0 z
c) tn oo t %o oz o
lA-07 00 0A~ 0 0 0
N.0 04%0 N \. C14 N1 %
0 4
to 1440 02
.4 0)Hca r40)4 # '

v1iHL. C00 00 00 0 --T 00 t(A 17 'in- l ZI) '), 0 ~-7cx'f w H C', -
00
iLg00 Ifn0 If4.. 00 00 00 1fa0 Uan-T L110 0- IT n0.
H HH4 H CA'iH
4~1i
1-1 tn -T Lf) 0 Ln ýT 00 0 C~ 00 f- 0 0 00 0Tt T0
00 I 0 On V- -T00 00 00 C 0 L)0 t)ý
100
C14c
0' 0' 0' 0' .-* 0 0,7- X. 07 :7.
CII%0 C'' C4I' C1 0 0 %D. C.i- 4% 0 D C4% N ýo C4-1 .-i .:I 1-4 a)r a4
:h H o
0. 0. > > a -. 02 02 0Pk 2 2 , V ~.
ct IM cc r

"T0 0 'T 00 H ~r-l HCV)a.O nfl ll ko e 0r0 -- ri00 a
T~l3SL'SUv~ Nco ) 100'0 I l cLAC\1.0- n Nr 0 cn HO'0
T 0 n M Nr-iL~( C1 jc 9 - riHC1
HC'H CJN Cl LnC I c'Jc'H q '. N 4t
-' To zodw Li 0 0 LAOO 000n nL ý Cl 0L0 O IT c a n % O C O-T p-uV i JH -.T cl) -w MI (N J 1-1N NH
r- 4 H m~~- 'T C*N ~-H C' ClC4JHc'J
w Tv IIl 0A -Tor-0 0N000 0 m n N 0m-.T' t C-,A.. 0Ou c0NTc ~O~ H H Z Nf IT CIT Cl4 H %D IT H C14 cn ,4H
o -T000 0000 000 T tnC\C0 C\OOO%0 J7
t-T03 0) 0 0 3 C0 C00C T C - n 0 ONCi
H .~ H r- j ý H H4 -
r. ci 0 0 ) Z w a a
ý4Ju0
00
xH 0
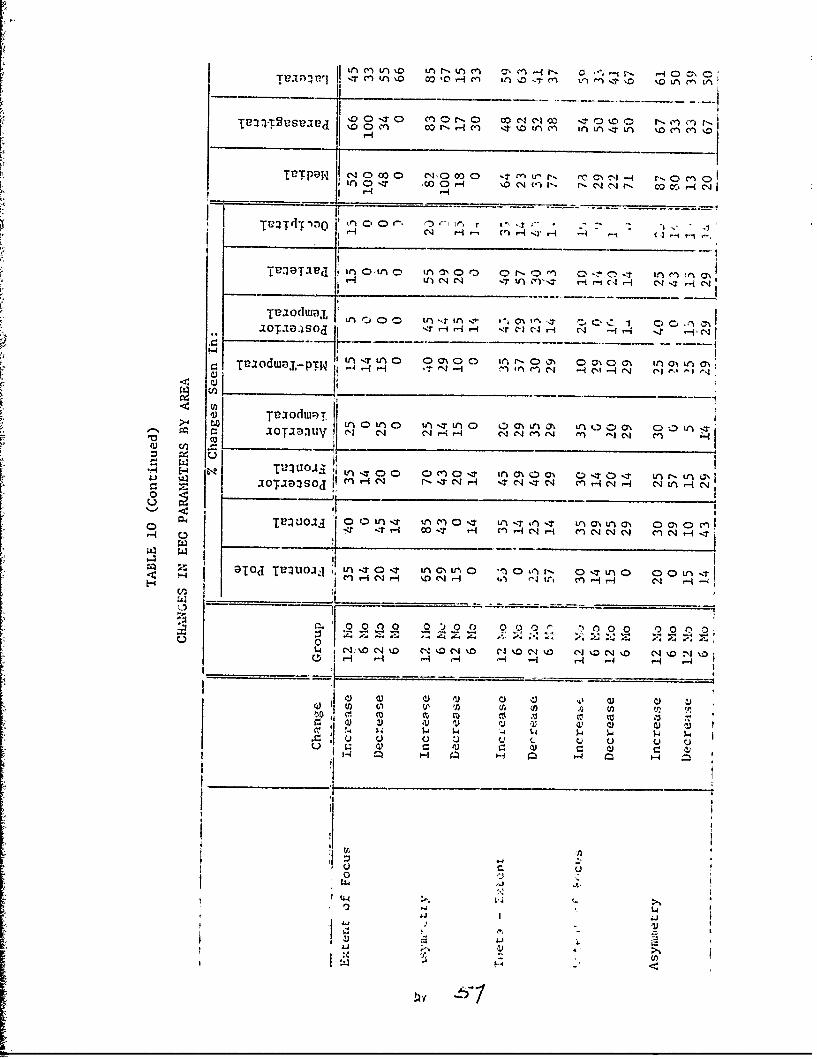
ILT91 H NN 0T cI 0 Hc -JHi -~ 0 co0 "T
In 0 00 0 -i %D 14rIO NH N~l NIH t" c-.j -4.cN~
c itWJ)TW I CN H" HT in Cy '-4 r- e r -i -.4r C NT ( -i C
0010 In IOl-.1 0~H O~~N 0 ON ON-In ONIa\Lv o w),P W f' 2 ýqLn T ^ ic ir ' o,0 .
u, ~ ~ ~ 7 o uý T__ _ _ _ _ __ _ _ _ _ _ _ __ _ _ _ _ _ _ _in 0-40 i T n0 0O n ý t n-10 -- IUVVAr-4-17N -. cri rTN C~IHn -1 CSHc
Cn1 - l 7C --r ITc~O C~~r-4 j ýT Oo mr- C4c'C1 i I
0 0
r zrfl o r- C) H r C 14 CN C) 04r-
Sl " 14r i %D N Hi fA Li tiEn) ~ (
r 0 C, C) ,0 C) 0 0Hj 42 He Z X-I __________________________ N, %0C4t I 0Cik 1 0 C4N I 0C4\ ' 0 qk
4)C
1-4 1= C l -
ýy

Tuulq C0Lq 0rý I 00UmMA Ln L 000
cn0- r-,0 cn0 Nc c4 4oo 0000Hi L1 00 Ln O.T ,t LIT -T~ Lr 0 0
U.P~ X, -1 r 0000 all 0 00000
I~~- cCj c'Jl; rLf
CH IT~TP3 Ltooý 000 ooona. ntn nr '100
HiC-'4Hý cq C'4 cn ?-4 H
Tvowa- o 06 00o o~ Hn - 0C
0 T'e0tdiua
0 4 ol) - _____ 0_ D 0 z_ t 0 O)G% 0_0 0
Joaoso HIcq cn q q H C14 H C-4 NC-4 cqJ
0T12IUOIJI 0 ON 0d\ 'L o~~ ~0 0in-. 00 )00NH4m C - 1 - *
DT~d TTU0UIA I 'T 0 o-T o-T 0oo ' o-,T 000
-qC4 -q-,r- -
00000 0 0 0 0
z 0 C 0
H H)
0 ~4-
.10 0I' ~iLA

In this one subject with progres:ivi- Aicýrw1.i _ '.t , the changu con-sisted of the appearance of paroxysmal burstb -t th,i 6 and 12 monthexams. Paroxysmal bursts are non-speelfic i h io'xi2noei defined as suddenshort appearances of activity, obviously di ffrent t;.,n rive other activ-ity on the page ana usually present in 11l 1-. 1 .. .rmot oases theparoxysmal activity consists of slower f,'o', '. ", and/or spikes.It is most compatible with sei'urc Pt,,, ,* i- -,.,"hyperventilation in the normal individo l . X' Fn .!I -11C phon ",change may be seen in an individual who o .pr•fe,,y rorm,'1 clinicqllyand does not imply that the subject has seizures.
Paroxysmal slowing as well as ut.uer LEG torrviptes of se.zuretb .fltreport.ed to occur with 1ll adminQ:i rauton. ii rhi pro.;ent study onlyone case of progre.,sive paroxysmal slowing w, ,.r 1"ot~iad. ft is not: knownwhether or not this change might not have occured normailv, or whetherit was due to some other cause. This subject also wa', classified as"possible" ne,,ropathv, and thi. clinical evidence, I ,,ether with thefact rhat t:• EEG change wos progres~iv,-, .-n,•lcates thAt he was indeedexperiencing neurological side effects )F INH.
The remaining EEG analysis which has been called subclinical anal-ysis was done in an effort to extract the maximum amount of informationfrom the data on hand. Short of spectral analysis or some other com-puterized techniques, the authors are unaware of another study utilizingthis approach. 'While the results of the p•est:it study may not have anyparticular clinical significance, it is hoped ta.at as our knowledge ofEEG expands we may one day understand the meaning of changes such as wedescribe here. With this hope of contrcibution to our knowledge in thefuture and for the interest it may have for. :he present reader, theanalysis was under-taken. We emphasi.,e agaiv that the significance ofthis analysis is unknown and no valid U.G change is being suggested.
In addition to tie above, azothe- factr of umporcance should benoted. Throughout the analysis, subject. ,i ry is dominant. The defini-tions of change and significance as -ailtd Cie t'e report were purelya, bitCary. A knowledge of varibt.l•n of oo,.al i1EG pdati.,:rns over timedoes not eXit at this level 4nd a coatco- gwiul ,.,s ,rt included forcmpari.son. Jud;rnentis about rhe EkL,'s. wrre taI ly .uIjllcrive. Thedesignations of ell-devclopl-A 'pb.*ri .', ainc, iv were generatedoy the autho's for purposez of d i', . ,;,,. be taken in thatlight oniy.
For all these reasons no statL:,t:,1 ', :1., " .,-u- on the final"d"ta, since more significance wou~d aav.• ol c a J than was warranted.The fina] results were merely pre..,-t l " , tY I, at ).nterpretation.

STUDY 4
VISUAL EVOKED POTENTIAL
METHOD
Apparatus and Procedure - Visual evoked potentials were recorded on eachsubject. The stimulus consisted of 100 flashes of light from a Grass PST2100 bulb at the rate of one flash per second. The flashes were controlledby a Grass PS3 photo stimulator unit. The intensity was set at 16, whichcorresponds to a maximum flash intensity of 1,500,000 candella. The lampwas placed directly in front of the subject's face, 15 cm from the nose.No shielding of the face of the lamp nor interval filtering of the flashwas done. The subject was requested to keep his eyes closed and to lookthrough his eyelids in the direction of the flash. An attempt was mde tomaintaip alertness by the use of high ambient noise levels and verbalS~~stimulation. •
Only 100 -ight stimuli were given, and the VEP's were recorded fromfour different areas simultaneously. Recordings were made in the bipolarmode from four electrodes placed as follows: Oz - over the inion; Pz -in the midline parietal area corresponding exactly to the placement ofthe 10-20 International System; 01 and 02 - 3 cm lateral and 3 cm supe-rior to 0,. VEP's were recorded between 0I and 02, 02 and Oz, 01 and Q.and OZ an(IP z (Channels 1, 2, 3 and 4 respectively).
A pulse artifact corresponding to each flash from the PS3 stimulatorand the subject's EEG response were recorded on paper and magnetic tape.
,%u Ampex SP300 recore - was employed with recordings made in the FM
mode. The output from the Grass EEG machine was fed through a voltagedivider system to the input of the recorder. The input sensitivity ofthe recorder was adjusted so that a 100 microvolt calibration signal fromthe ,EEG machine produced a peak to peak voltage deflection of 1.5 v asmeasured on a CRO monitor at the output of the recorder. The stimulusartifact was recorded, on a sepacaze data channel, with the input sensi-tivity level adjusted in the same manner.
The raw data were procesbcd off-line. The output of the Ampex re-corder wab ied into a Nuclear Da,'a Inc. Aodel ND-800 Enhancetron 1024for averagiag. The output of toe averager was viewed on a TektronixType 503 oscilloscope. The potential was written out on a Hewlett-Packard Model 7000 AM XY recorder.

Data Analysis - The potentials were inspected visually to detect anyobvious changes. None were detected. Consequently, a more criticalanalysis was undertaken.
First, a baseline was drawn for each VEP. Since there was apparentdrift in some cases, the best-fitting baseline was selected. In mostcases it was an obvious one. A straight horizontal or nearly horizontalline was the best fit in most cases. Most potentials contained sinusoidaldeflections. The points that bisected these deflections, along with theinitial. starting point of the deflection, were used to determine the base-line.
Second, the potentials were divided into three parts correspondingto the: (1) Specific, early or primary complex; (2) non-specific, secon-dary complex or "main" discharge; (3) the afte" daseharge. In many casesthe points of division were obvious, based on a change in character ofthe complexes, amplitude of the waves, baseline width of the waves, etc.When the division was not obvious the points were located by identifyingthe wave which corresponded to wave -five (r.c'ýording to Gestaut) and,with this, locating waves three and six. Wave f~ve was identified asthe one with the largest amplitude, the most complexity or the latencyof approximately 130-200 mSec.
Vertical lines were drawn bisecting wavws three and 'six, and theselines were used as division points. Boch syscems resulted in approximatelythe same division points.
When the VEP was thus divided, the amplitude, complexity and widthof each section ware determined. The -JMpLACud;2 Ir:uasurements were in ar-bitrary units and reprezented the peak ro peal- ampli.ude of the largestwave within trw complex. "Compplexity" ,,e dt-i- , as the number ofchanges in poilcity in the def!,;±(:. or oc•- ifutg '.~hin the division. Indeterinin.Lng wThether a change, in polarity o: oefl,ýCcion represented a wave,it was required that it either crossed •, badlin9 or wa_. the point ofan obvious coange in overall zrencl. ' O-med without reversal ofpolarity w;re nuot counted, nor we.. s&.Lrple nc'OiUes on A large wave.Latenu3.es co trne peak deflect..ort of the VEP w !:e A1•o determined.
in the ,,iezsureaevL: ok peak def0 , lc, .. a,1 i• ir wA., found that,in general, cne w~ve was largesL in .rnMpLOio,'. ý two deflectionsof equal anmpiitude w'..ru found. in .za.. t.• ,awc correspondingmost ciostly to the sblbshed pr:,eri- ). K', chainel was selectedfor n.s-e:,,*nt. The peak aeflec.oi1 .-' -,tnn,'.o but not always, wavefive as defined by previous criteria.
% ..od from each channel wer.: ; r~i"zwd , A mean and
a
standard deviation were computed for each measurement. A separate, one-wa- classification ANOVA was performed on the data from the 12-monthsubjects. where two or more measures were derived, they were analyzedseparately by trials (0, 6, 12 months).
In one VEP reliable measurement of the latency to peak deflectioncould not be made. A valu& was estimated for the analysis according tothe method outlined in Winer.1 014
Tu .y-four VEP's were suitable for analysis. Eighteen in the 12-month group and six in the 6-month group.,
RESULTS
The means and standard deviations of the nine (9) measurements arepresented in Table 11. Significant differences between means are indi-:cated. The analysis of variance and post hoc tests on which these dif-ferences are based are presented in Appendices 2 to 49.
No grossly vdisible differences were noted in any of the VEP's.
Primary complex amplitude - There was an increase in primary complexamplitude in channels two and threeat six and 12 months. The differencein channel three was significant (p<.05). Post hoc tests demonstrated thatthe source of the difference was that both the 6 and 12 month scores dif-fered significantly from control (p<.05), but not from each other. Inchannel two-, the control amplitude was higher than either 6 or 12.months.
Primary complex complexity " There was a significant increase at6 and 12 months in channel one (p<.05). All other channels showed an in-crease at 6 and 12 months, but none of these differences were significant.
Secondary complex latency -No significant changes nor trends wereseen.
Secondary complex width - A significant decrease (p<.05) at decreasewas found in channel one compared to the 12 month and control values.Channels three and four of the 12-month group and all channels of the 6-month group show the same decrease at 6 months.
Secondary complex latency to peak deflection - No significant changesnor trends were seen.
Secondary complexity amplitude - A significant increase at 12 months

TABLE 11
VISUAL EVOKED POTENTIALS
12 Month Group 6 Month Groupn 8 n 6
Parameter . ' Mean SD Mean SD
Primary Complex
Amplitude1
Channel 1Control 12.33 8.68 11.17 7.176 Months 11.00 7.03 27.00 15.0i12 Months 15.78 1.4.01
Channel 2Control 12.39 9.08 17.33 14.056 Months 20.94; 14.24 18.00 9.1012 Months 21.50 16.92'
Channel 3Control 14.89 8.11 16.33 14.646 Months 22.44* 11.13 16.J.7 9.3312 Months 23.78* 11.64
Channel 4Control 33.44 28.94 23.00 16.596 Months 27.61 22.97 44.17 14.7312 Months 28,11 36.08
Complexity
Channel 1Control. 2.44* 1.04 2.33 1.376 Mondhs 3.67 3.85 3.67 1.0312 Monlths 3.78 1.96
Channe t 2Control 3.17 . 25 2.00 .636 Months 3.67 1,85 3.83 .7512 Months 3.50 L.69
Channel 3Control 3.06 .87 1.67 .82
6 Months 3.83 ,.'2 4.00 .8912 Months 3.28 /,I ___

I
TABLE 11 (Continued)
VISUAL EVOKED POTENTIALS
12 Month Group 6 Month Groupn 18 n= 6
Parameter Mean SD Mean SD
Channel 4Control 2.83 1.10 2.33 1.036 Months 3.28 1.07 2.67 1.2112 Months 3.00 1.14
Secondary Complex
Latency to Beginning3
Channel 1Control 74.72 19.96 65.83 11.586 Months 76.67 21.07 85.00 18.1712 Months 70.00 29.46
Channel 2Control 77.50 16.56 74.17 8.016 Months 72.22 19.50 87.50 12.1412 Months 67.22 21.50
Channel 3Control 71.39 16.96 70.00 8.946 Months 71.11 15.20 82.50 18.6412 Months 68.61 19.99
Channel 4Control 63.33 16.09 62.50 15.736 Months 70.56 23.45 77.50 31.1012 Months 59-.17 16.29
Width3
Channel 1Control 162.50 33.00 179.17 38.526 Months 14 6 . 9 4L"* 36.83 i43.33 26.9612 Months 163.33 38.39
Channel 2Control 150.00 34.39 150.00 33.916 Months 152.22 37.78 144.17 37.0712 Months iE'- 44 43.99

TABLE 11 (Continued)
VISUAL EVOKED POTENTIALS
12 Month Group 6 Month Groupn=18 n=6
Parameter Mean SD Mean SD
Channel 3Control 147.22 40.04 161.67 28.756 Months 134.72 34.28 140.83 34.2712 Months 142.22 40.81
Channel 4Control 161.39 35.31 150.67 9.836 Months 160•.28 36.60 136.67 16.9312 Months 162.50 41.56
Latency to Peak Deflection 3
Channel 1Control 152.78 27.07 157.50 33.586 Months 150.00 35.31 175.83 37.6112 Months 158.61 57.77
Channel 2Control 147.17 42.35 148.33 29.446 Months 144.17 41.03 170.83 20.3512 Months 1,48.61 54.58
Channel 3Control 135.83 27.08 126.6-7 23.596 Months 152.78 38.81 150.83 28.8812 Months 130.56 51.27
Channel 4Control 143.06 ý"2.50 150.00 18.176 Months 152.78 59.88 141.67 42.0312 Months 141.39 40.83
Amplitude
Channel 1Control 40.94 3t. 9 0 5b.67 33.016 Months 32.17 19.03 42.00 21.8812 Months 82.28"* 74.27

TABLE 11 (Continued)
VISUAL EVOKED POTENTIALS
12 Month Group 6 Month Groupn = 18 n 6
Parameter Mean SD Mean SD
Channel 2Control 30.22 19.52 44.17 25.956 Months 34.11 17.91 41.33 21.2012 Months 60.89* 47.56
Channel 3Control 42.39 26.67 57.33 33.396 Months 38.28 23.27 41.83 33.8712 Months 63.33* 34.25
Channel 4Control 119.78 50.61 81.17 27.246 Months 79.78 41.11 93.33 54.3712 Months 93.39 79.27
Complexity
Channel 1Control 4.56 1.76 4.00 1.106 Months 4.50 2.01 3.83 .9812 Months 5.28 1.53
Channel 2Control 4.39 1.94 3.33 .526 Months 4.56 1.85 4.83 1.7212 Months 5.44 2.12
Channel 3Control 5.50 1.72 4.83 1.606 Months 5.06 1.89 4.33 1.5112 Months 4.72 1.45
Channel 4Control 5.17 1.69 4.67 1.516 Months 5.44 1.46 4.33 1.2112 Months 5.28 1.99

TABLE 11 (Continued')
VISUAL- EVOKED POTENTIALS
"12 Month Group 6 Month ,Groupn =18 nI6
Parameter Mean SD Mean SD
After Discharge
Amplitude
Channel 1Control 1.7.00 11.92 24.33 12.406 Months 21.28 12.02 25.83 11.2512 Months 33.82* 24.92
Channel 2Control 19.33 12.15 25.67 17.49
Months 21.56 13.61 26.00 17.2612 Months 26_.07 21.00
Channel 3Control 23.94 13.93 37.00 34.626 Months 26.78, 13.55 29.00 19.9112 Months 34.50 18.87
Channel 4Control 1 64.17 32.32 46.67 24.556 Months 46.06 26.78 63.67 41.0212 Months 51.67 50.04
Complexity
Channel 1Control 6.50 2.,68 6.00 1.906 Months 8.33 2.45 6.83 .4112 Months 7.83 2.62
Channel 2Control 6.89 2.49 5.67 1.036 Months 8.17 3.31 6.50 2.0712 Months 8.56 4.26
Channel 3Control 8.00 2.59 6.67 2.586 Months 8 ,6 .104 8.50 1.2212 Months 9.44 3.90
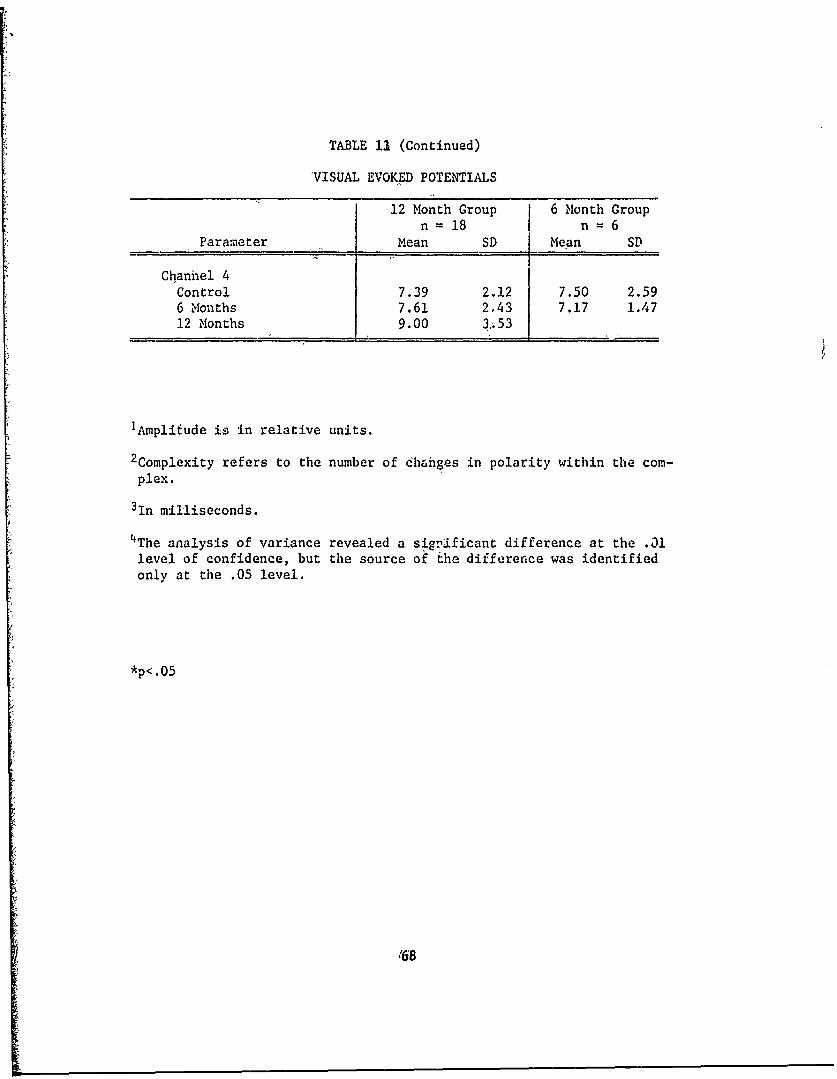
TABLE 13 (Continued)
VISUAL EVOKED POTENTIALS
12 Month Group 6 Month Groupn = 18 n = 6
Parameter Mean SD Mean SD
Chanhel 4Control 7.39 2.12 7.50 2.596 Months 7.61 2,43 7.17 1.4712 Months 9.00 3'ý53
IAmplifude is in relative units.
2Complexity refers to the number of ch&nges in polarity within the com-plex.
3In milliseconds.
4The analysis of variance revealed a sign1ficant difference at the .31level of confidence, but the source of the difference was identifiedonly at the .05 level.
*p<. 0 5
'68

compared to control on 6 monLhs was seua 1r ,satc clo-incl,: Channel 2(p<.O1), channel 3 (p4.05), channel 4 (p-.05).
Secondary complex complexity - .o .U d fferences nor trendswerv iutn.
After dIscharge amplitude A $igri , ,. , . (p .05) at 12months compare" to control and 6 mornths . jrouwuo )j, ,aannel one. Chan-nels two anc three also showed an iicle ý,' i:, , tcr diLcharge amplitude,but the increase was not statisticall% •,;n3Ucar,.
After discharge complexity - The 6 ana 12 monLh values were higherthan the controi values in al' chun1;eib 0o bt,! ' ,uup•. These differ-ences were not found to be stati.stica])y ýýig.glu.1,A.L, however.
The ..cattvred significa.it dicr,,' Al ah' %,cy, found in the visualevoked potentJal data are difficuL.L Lo _ue~p ti. ,. coms reasonableto expvct that any real change ocourrii.g wsWuJ1 oe )ound in all channels.This was found tzo be the casre regaru.Z;,g t.le r,• ny of the primarycomplex and Cie after discharge, buz only in tlic p1i;..Jry complex wereany of the differences significait. 'the fo)lLa tr,3d~tional measures oflatency ax'd amplitude did not sliow (ý :ba Ll •ec consistently in allchannels.
One other (fnding ts b s'- ,.,. the three channelsshowlng arn eva!-i c in the anp: i I a. ýA , , -,ry iooplex at twelve-,.oftis, Alth ;, the fourth dh.,n,,c .,. • , change, the over-all trend hngi~t he considered u • o LM on the evoked poten-
c';t, i', ae . r, if ol ýupport in,h.nl the changv.ý
A :I ` ":!V. -it Ll., ;. k.t'.d potentialsS,:.Ut haw.,- .I-cs, , . 0.,)t :ntial would
, e , -u : , ." , : a,) I, tk•c enld. Coa-t , '¼,.. Lxptriencv
,- -*•. lopoida: ,licrC I. -,, v.c, d have beenp,'t , fr. tt, ,, .,ccurately. Ai-
t'hou~sh ,ýt( t.•ta ' ,,,o-w ado 4v nut,,,.;'o' a, . t, t, s, certain
j._f ,r., ,, the lo'fr Ot " ', -O I (ions, ctc.,
69

col /o e-irle n a aeinlecdtefnlptnil
Vai~tLo f 'a )~oolgc, taeo* .h sbec s nwnt hvcosiurb'.. l ti -\,kdpceta. hsvaibe/a n
could oe -aitro.ile i nd mayq1 c hare dinfcluece th nepe t Tinal po enal.inVar§athniqof e,'s'.'c-ologicbcu datieso aihe- subjectete is knintoferecconherab'. nonee,,;d. , try be co ed pocntin. This variabed was uhn-ekn owntic ýan werr sbct.ctapliy :nois or sfevea differen pyilevelc of stinulusver :.a. uroul: the rba:n ix-ýc~ .thaty or, secuencay cmipl aex wouddeon,ao a- aaach oth. 2Ci-1A andUy hzv be-,;,nsna. should hntI ave been mpOyedtile r:~.vr L.--- uime res of thi ,tudycannoty beodirectliy compMredwtlh cA-ýer; rin i~ SUC abISoue aOfima de mLeaasuresý were3 not avai.ýlal.
Therii cu- cb'iesI caaamplý j,, art difficut .Zobu inepe . Th - asur-Ikngwtevigu tae underyi.ae yhyloo~ o;.a bc cdres ieiy hav crpeatdal diff;.er~penc.
i Ihre on reaisons 1c the oter signfiat de changs aere untledas. changs
however, tr wau they hrtdjeaL~v te that thewhsccondary hoaplebewouldund,hadnda~ierent methe: ýPe :cioploynd inv ten. presn udyChne in the ~ri a.O
tose ofne 1N ý-vc r Like. .o~ipitodoog as n dfcndile abovpe would beinie~c.1u Sinc c obcralig sL'i Wa)isC Uot nsa)iakhed ý rt isliely tha these
chalg.e ,cc toe unriyohg wAhyi.ýog oi. rthe~ nvormal variat ions.noptc
Tn~ reasons 2o V the 01hc siiicn thnes are uncllSear.iC is
ion uf I., u ivc o~r, , Iw _ý,i%~td aese *.c~ad abovie wold baLe.mi
Becau.,e "ý .thodo~ký tý_L coj~rd osoa t:io fact that no grosslyvisii~ a~w cei, . uiuJl rmethoa.s oý data! arhoIvs.L were
not 10.~:.~ i .'c~ :uui' btý fouaJ 'Or tioc P~resen~t methodof dato . ŽJ .t~~ewrx~ ew. of looking at
Tb.!C ýU.c -ý "" 1ý _ro .c -1 iiai _yse .~~t.W1re performod, itis pc.-s io1,2 t,,. z,, in c aý A o l, of ti-oz ýignificant dif-ferencvbs wL! .,, - ffec¾,
70

SUMLARY AND CONCLUSIONS
Careful study of the results has disc~oced several changes basedon inspection of the data and on stati.iical analysis. Although it isimpossible, f r -Leasons detailed in this serieb of studies, to establishwith certainty -That INH was responsible for changes found, it is notpossible to exclude INII as a cause either. The changes which were foundwere minimal and scattered and may have little or no significance. Theclinical data probably raise the greatest q.,estlon. Althougii the c'fin-ical findings were minimal inmost cases, the significance is apparent,especially for aviators. The incidence of neuropathy is especially dis-turbing. Most flight surgeons would not want to allow aviators to flywith the probability of side effects which were found. Therefore, fur-ther studies are needed in order to estabLt`si whether the present dataare spurious or would hold up for larger populations.
Meanwhile, although the resultj o! r.ýe )r. -int stu y do not indicatethat INlI is innocuous and causes only noyisi.ýDificant effects, they alsooffer no conclusive evidence that should cause aviators co be groundedsimply because IN}{ is being administered.
In the final analysis iz would seem wise to mjke judgment on an in-dividual basis. The data strongly suggest that r.rvfuJ. study of treatedaviators is indicated. Policy stacements on LMI oho,:ld await furtherstudies.
7,I
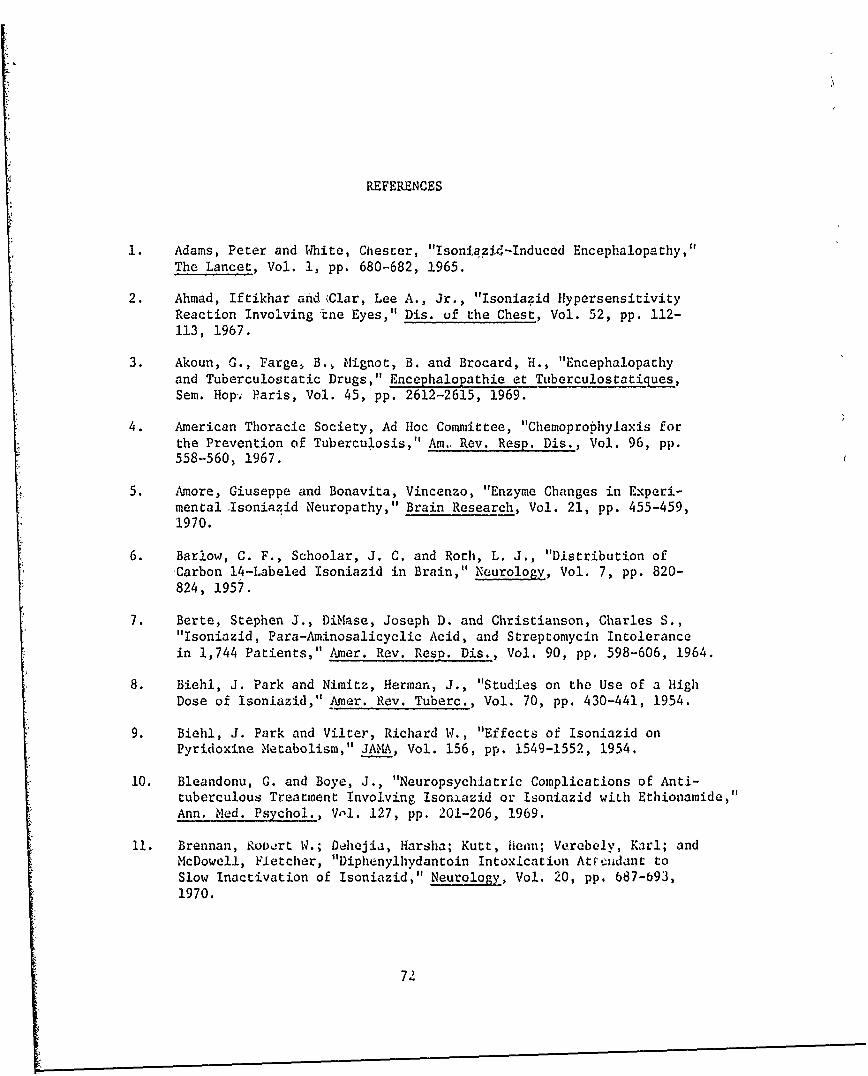
REFERENCES
1. Adams, Peter and 1White, Chester, "IsoniaziM-Induced Encephalopathy,"The Lancet, Vol. 1, pp. 680-682, 1965.
2. Ahmad, Iftikhar and Clar, Lee A., Jr., "Isoniazid HypersensitivityReaction Involving mne Eyes," Dis. uf the Chest, Vol. 52, pp. 112-113, 1967.
3. Akoun, G., Farge, B., Mignot, B. and Brocard, H., "Encephalopathyand Tuberculostatic Drugs," Encephalopathie et Tuberculostatiques,Sem. Hop.ý Paris, Vol. 45, pp. 2612-2615, 1969.
4. American Thoracic Society, Ad Hoc Committee, "Chemoprophylaxis forthe Prevention of Tuberculosis," Am., Rev. Resp. Dis., Vol. 96, pp.558-560, 1967.
5. Amore, Giuseppe and Bonavita, Vincenzo, "Enzyme Changes in Experi-mental Isoniazid Neuropathy," Brain Research, Vol. 21, pp. 455-459,1970.
6. Barlow, C. F., Schoolar, J. C. and Roth, L. J., "Distribution ofCarbon 14-Labeled Isoniazid in Brain," Neurology, Vol. 7, pp. 820-824, 1957.
7. Berte, Stephen J., Diiase, Joseph D. and Christianson, Charles S.,"Isoniazid, Para-Aminosalicyclic Acid, and Streptomycin Intolerancein 1,744 Patients," Amer. Rev. Resp. Dis., Vol. 90, pp. 598-606, 1964.
8. Biehl, J. Park and Nimitz, Herman, J., "Studies on the Use of a HighDose of Isoniazid," Amer. Rev. Tuberc., Vol. 70, pp. 430-441, 1954.
9. Biehl, J. Park and Vilter, Richard W., "Effects of Isoniazid onPyridoxine Metabolism," JAMA, Vol. 156, pp. 1549-1552, 1954.
10, Bleandonu, G. and Boye, J., "Neuropsychiatric Complications of Anti-tuberculous Treatment Involving Isonxazid or Isoniazid with Ethionamide,"Ann. Med. Psychol., Vol. 127, pp. 201-206, 1969.
11. Brennan, Rowxrt W.; Dehejia, Harsha; Kutt, fiean; Verebely, Karl; andMcDowell, Fletcher, "Diphenylhydantoin Intoxication Atttcidant toSlow Inactivation of Isoniazid," Neurology, Vol. 20, pp. 687-693,1970.
72
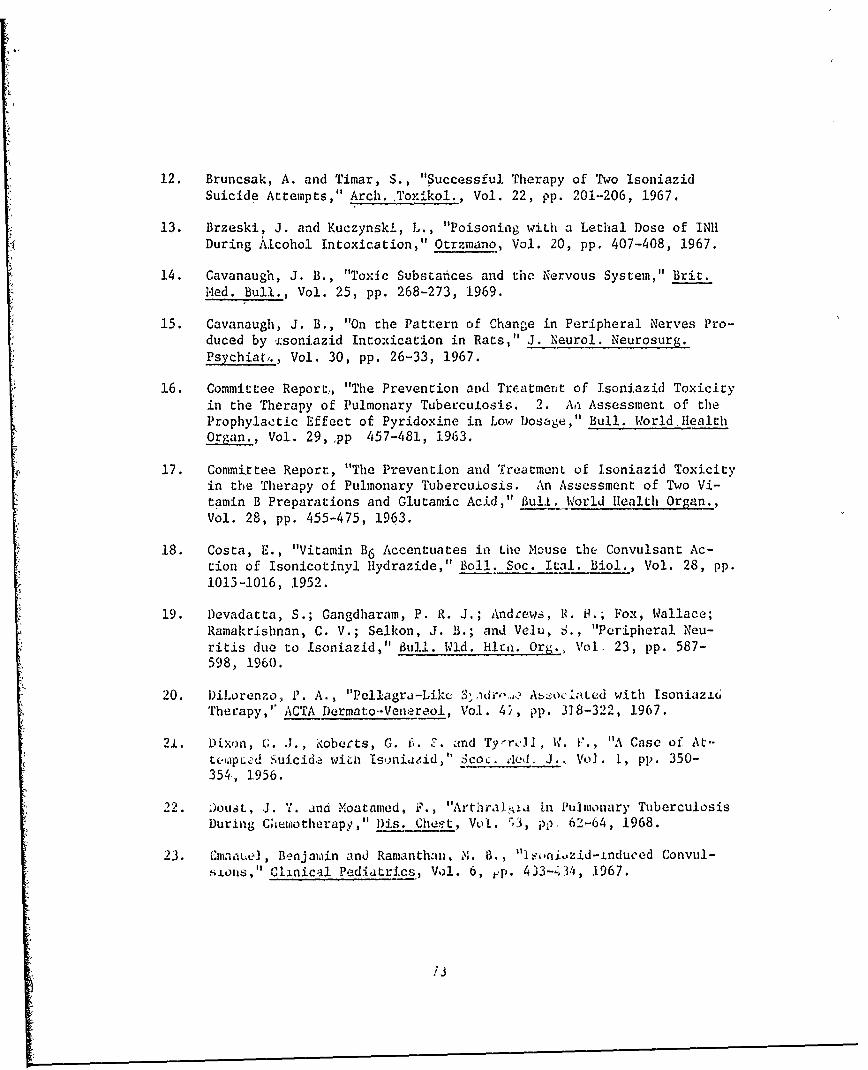
12. Bruncsak, A. and Timar, S., "Successful Therapy of Two IsoniazidSuicide Attempts," Arch. Toxikol., Vol. 22, pp. 201-206, 1967.
13. Brzeski, J. and Kuczynski, L., "Poisoning with a Lethal Dose of INIIDuring Alcohol Intoxication," Otrzmano, Vol. 20, pp. 407-408, 1967.
14. Cavanaugh, J. B., "Toxic Substazces and the Nervous System," Brit.Med. Bull., Vol. 25, pp. 268-273, 1969.
15. Cavanaugh, J. B., "On the Pattern of Change in Peripheral Nerves Pro-duced by 'i:soniazid Intoxication in Rats," J. Neurol. Neurosurg.Psychiat,., Vol. 30, pp. 26-33, 1967.
16. Committee Report,, "The Prevention and Tre.atment of Isoniazid Toxicityin the Therapy of Pulmonary Tuberculosis. 2. An Assessment of theProphylactic Effect of Pyridoxine in Low Dosage," Bull. World.ilealthOrgan., Vol. 29, 'pp 457-481, 1963,
17. Committee Report, "The Prevention and Treatment of Isoniazid Toxicityin the Therapy of Pulmonary Tuberculosis. An Assessment of Two Vi-tamin B Preparations and Glutamic Acid," Bull. World Health Organ.,Vol. 28, pp. 455-475, 1963.
18. Costa, E., "Vitamin B6 Accentuates in Lhe Mouse the Convulsant Ac-tion of Isonicotinyl Hydrazide," Boll. Soc. Ital. Biol., Vol. 28, pp.1013-1016, 1952.
19. Devadatta, S.; Gangdharam, P. R. J.; Andrews, R. H.; Fox, Wallace;Ramakrishnan, C. V.; Selkon, J. B.; and Velu, S., "Peripheral Neu-ritis due to Isoniazid," Bull. Wld. HI. Org., Vol. 23, pp. 587-598, 1960.
20. l)iLorenzo, P. A., "Pellagra-Likc ">,dr'.,, Azocltcd with Isoniazi6Therapy,'" ACTA Dermato--Venereol, Vol. 4', pp. 318-322, 1967.
21. Dixon, G. J., ',oberts, G. f,. F. and Tyr•Jl, W. i., "A Case of At-t•eJLpL¢d Suicide wih Isniazid," Scoc. a,'d. J., Vo]. 1, pp. 350-354., 1956.
22. Doust, J. 'I. and Moatamed, F., "Arthraiia in Pulmonary TuberculosisDuring Chimotherapy," Dis. Chesýt, Vol. -3, pp, 62-64, 1968.
23. Cmaauie, Benjamin and Ramanthan, M. B., "leo.niozid-induced Convul-slons," Clinical Pediatrics, Vol. 6, jp. 433-'3/4, 1967.
/'
24. Evans, David A. Price, "Genetic Factors in Drug Therapy," In Scien-tific Basis of Medicine, British Medical Federation, Oxford U. Press,1.969.
25. Favez, G., Mailiard, J. M. and Vouilloz, M., "Resultats Comparesde Doses Moyennes et Elevees d'Isoniazide Dans le Traitement Triplede la Tuberculose," Achweiz. Med. Wschr., Vol. 98, pp. 1392-1395,1968.
26. Feroee, S. H., "Controlled Chemoprophylaxis Trials in Tuberculosis,A General Review," Adv. Tuberc. Res., Vol. 17, pp. 28-106, 1970.
27. Fetcurhoff, K. I., Holmes, C. X. and Martin, G. E., "Hazards of!soniazid Therapy in Epileptics," mun. Rev. Tuber., Vol. 66, pp.501-509, 1952.
28. Foldi, N., Zolcan, 0. T. and Maurer, M., "Influence of Isoniazid onthe Central Nervous System and the Antagonism Between this Substanceand Pyridoxine, Panthothenic Acid," Arzneim. Forsch., Vol. 20, pp.1620-1623, 1970.
29. Friedmann, S. A., "Death Following Massive Ingestion of Isoniazid,"Amer. Rev. Resp. Dis., Vol. 100, pp. 859-862, 1962.
30. Gibson, Francis, D., Jr. and Phillips, Samuel, "Peripheral NeuritisAfter Long-Term Isoniazid," Geriatrics, Vol. 21, pp. 178-180, 1966.
31. Good, Armin E., Green, Robert A. and Zarafonetis, Chris J. D.,"Rheumatic Symptoms During Tuberculosis Therapy, A Manifestationof Isoniazid Toxicity?" Ann. Intl. Med., Vol. 63, pp. 800-807, 1965.
32. Goodman, Louis S. and Gilnan, Al-red, TYŽ Pharmacological Basis ofTherapeutics, The Macmillian Company, New iork, 1965.
33. Grollman, Arthur, Pharmacology and Thorapeutics, Lea & Febiger,
Philadelphia, Pennsylvania, 1962.
34. Hanson, Mary L., Comstock, G. Iv. and Halcy, C. E., "CommunityIsoniazic Prophylaxis Program in ai Undvraevuloped Area of Alaska,"Public Heaith ikeports, Vol. 82, pp. 1045-1056, 1907.
35. Harris, hi. WI.liam, "Currert Concfprs of the Metabolism of Anti-tuberculous Agents," Amer. NY Acad. Sei., Vol. 106, pp. 43-47, 1963.
36. Hildebrand, J., Joffrov, A. and Cuers, C., "Myoneural Chanis in Ex-perimental lsoniazid NeuropatLy - Electrophysiological and H|istolog-ical Study," Arch. Neurol., Vol. 19, pp. 60-70, 1968.
74

37. Hofmann, Mark A. and Nossaman, Richard 0., "EffevL of Isoniazid' onPerformance," USAARL Report No. 71-14, US Army Aeromedical ResearchLaboratory, Fort Rucker, Alabama, February 1971.
38. Nossaman, Richard 0. and Hofmann, zark A., "Effect of Isoniazid inPerformance ii," USAARL Report No. 71-23, US Army Aeromedical RvsearoalLaboratory, Fort Rucker, Alabama, June 1971.
39. Holtz, Peter and Palm, Dieter, "Pharmacological Aspects of VitaminB6 ," Pharmacol. Reviews, Vol. 16, pp. 113-178, 1964.
40. Hothersall, T. E., Mowat, A. G., Duthie, J. J. R., and Alexander,W. R. M., "Drug-Induced Lupus Syndrome - A Case Report ImplicatingIsoniazid," Scot. Med. J., Vol. 13, pp. 245-247, 1968.
41. Ito, Susumu, "Studies on Mechanism of Psycho-Neurotic DisturbancesCaused• by INA1I Administration. ii. On the Antagonistic Action Be-tween INAI (Isonicotinic Acid Hydrazide) and Vitamin B6 ,," SapporoMed. J., Vol. 273, pp. .13'6-142, 1965.
42. Johnston, Robert F. and Hopewell, Philip C.., "Diagnosis and Treat-ment -- Chemotherapy of Pulmonary Tuberculosis," Ann. of Int. Med.,Vol. 70, pp. 359-367, 1969.
43. iKarkalitsdy, I. M., "Comparative Biochemical Characteristics ofB6 -Vitamin Deficiency Caused by Alimentary Iasufficiency of Pyri-doxine and by Isoniazid," VYp. i'itan.. Vol 30, pp. 37-44, 1971.
44. Kasprzak, Scanislaw, Jagielskil, Stefan and Piziewica, Urszula,"Pr:zylv.dkow" Ostre Zatrucie Hkin 1,5-Rocznego Chlopea," Otrzymano,Vol. 19, pp. 284-287, 1968.
45. Katz, Gary A. and Jobii', Gary C., "l:-rgo ooses of Pyridoxine in theTreatment of Massive Lngestion of isoniafLd," Letter to the Editor,Am. Nwvi.t;, of Resý)irato,'y D.s.za~e, Vol. 101, pi. 991-992, 1970.
46 . ,')#:., "Troo,,.. :;, Toll, Henry1 W., Jr., Ce u, D. C. and Kier, L.L,. "u:•tU iiu to W nt,,ýn..ional ,vduo:x•e of .soniazid: A Case Re-po,-t,' eo. , a:sic Sc*, V%;. i0, p,'). j-._-_338, 1965.
47. Kot-un, i\. S. and Parsons, M., "Nutro.o.ic.A Cor.mplications of Tuber-culo-U. Scrv Unusual Manifestationý,' "i.ýh (U.Irterly Journal ofmediinu, Vol. 39, pp. 17-31, 1970.
48. Kra.Lz., ,1i. ;., Jr. anJ Carr, C. Jol.f, kYr.•iaologoýc PrinciplesOf , a] -4'l 'icl ce, 5ch E.it•r•i.n, Thu e tiera & W Tkins Company,
73
L
49. Kreutzberg, Georg W. and Carlton, William W., "Pathogenic Mechanismof Experimentally-Induced Spongy Degeneration," Acta Neuropathologica,Vol. 9, pp. 175-184, 1967.
50I n D. V., Selkon, J. B., Ramachandran, K., Devadatta, S.,~.i•:ci1n, D. A., Radhakrishna, S. and Stot-t, H., "Effect of Pyri-uo.;iax on Vitanin B6 Concentrations and Glutamic-Oxaloacetic Trans-ann~.s¢, Accivity in Whole Blood of Tuberculous Patients Receiving
g- g Isoniazid," Bull. Wld. Hlth. Org., Vol. 36, pp. 853-870,1967.
51. Kubicki, S., Ibe, Karla and Gotze, W., "EiectroencephalographicChanges in an Isoniazid Psychosis and a Suicide Attempt with Nico-teben," Arch. Toxikol., Vol. 20, pp. 197-209, 1964.
52. Kutt, Henn, Brennan, Robert, DeHejia, Harsha and Verebely, Karl,"Diphenylhydantoin Intoxication - A Complication of Isoniazid Therapy,"American Rev. .of Resp. Dis., Vol. 101, pp. 377-384, 1970.
53. Kutt, H. Verebely, K. and McDowell, F. H., "Inhibition of Diphenyl-hydantoin Metabolism in Rats and in Rat Liver Microsomes by Anti-tubercular Drugs,Neurolo, Vol. 18, pp. 706-712, 1968.
54. Lampert, Peter W. and Schochet, Sydney, S., "Electron MicroscopicObservations on Experimental Spongy Degeneration of the CerebellarWhite Matter," J. of Neuropathology and Experimental Neurology, Vol.27, pp. 210-220, 1968.
55. Levy, Louis, Higgins, Lucy J. and Burbridge., Thomas N., "Isoniazid-Induced Vitamin B6 Deficiency - Metabolic Studies and PreliminaryVitamin B6 Excretion Studies," Amer. Rev. Resp. Dis., Vol. 96, pp.910-917, 1967.
56. Meldrum, B. S., Balzano, E., Gadea, M6 and Naquet, R., "Photic andDrug-Induced Epilepsy in the Baboon (Papio Papio): The Effects ofIsoniazid, Thiosemicarbazde, Pyridoxine and Amino-Oxyacetic Acid,"Electroencephalogranhy and Clinical Neurophys., Vol. 29, pp. 333-347, 1970.
57. Mellerio, M. F., "Into.%.caticns Aigues et Crises Convulsives. EtudeElectroencephalographiques de trois Pfoduits tres Differents: Rimifon,Chlorolase, Metaldehyde," Rev. Neurol., Vol. 117, pp. 495-498, 1967.
58. Money, G. L., "Unusual Ma•nifestations of Isoniazid Toxicity," J.Trop. Med. Hyg., Vol. 62, plp. 198-209, 1959.

59. Mrozikiewica, Aleksander and Strzyzewski, Wlodzimierz, "Effect ofLong-Term Administration of ACTH and Adrenocortical Hormones on theCourse of Hydrazide Convulsions," Archivum Immunologiae Et TheraviaeExperimentalis, Vol. 15, pp. 909-911, 1967.
60. Munck, B. G., "Amino-Acid Transport by Small Intestine of the Rats,"Biochem. Biophys. Acta, Vol.. 94, pp. 136-142, 1965.
61. Neff, Thomas A., "Isoniazid Toxicity: Reports of Lactic Acidosisand Keratitis," Chest, Vol. 59, pp. 245-248, 1971.
62. Nelson, Leslie G., "Grand Mal Seizures Following Overdose of Isoniazid,"Amer. Rev. Resp. Dis., Vol. 91, pp. 600-604, 1965.
63. Nishizawa, Y., Kodama, T. and Sugahara, S., "Brain y-AminobutyricAcid During and on Suppressing of the Running Fit)" J. Vitaminol,Vol. 6, pp,. 236-239, 1960.
64. Olsen, Pov! Zancer and Torning, Kjeld, "Isoniazid and Loss of Memory,"Scand. J. Resp. Dis., Vol. 49, pp. 1-8, 1968.
65. Olsson, Yngve, "Mast Cells in INII-Induced Neuropathy of the Rat,"Acta Neurol. Scandinav., Vol. 44, pp. 457-466, 1968.
66. Patel, R. B., Patel, T. L. and Mehta, H. C., "Comparative Studieswith Isoniazid Alone, Isoniazid with Thiacetazone and Isoniazid withPara-aminosalicyclic Acid in Ambulatory Treatment of Pulmonary Tuber-culosis," J. Indian Med. Ass., Vol. 48, pp. 471-478, 1967.
67. Pawlaczyk, J., Banaszkiewica, W., Kowalski, E. and Walczak, M.,"Changes in the Neurosecrecive Sysr-em of Rabbits During ConvulsionsCaused by Isonicotinic Acid Hydrazide," Acta Physiologic Polonica,Vol. 21, pp. 401-409, 1970.
68. Phatak, A. T. and Shah, S. it., "Encephalopathy Following AccidentalIsoniazid Poisoning," C±Linical Pediatrics, Vol. 10, pp. 356-358, 1971.
69. Physicians' DesK 0efvrencL to Pharamaceutical Specialties and Bio-logicals, Medicai Lconomics, Inc., Oradell, N. J., 1970.
70. Ramakrishna, Tallapragada and Smith, Bernard, H., "Seizures Secondaryto Isoniazid Ingestion," Neurology, Vol. 20, pp. 1142-1145, 1970.
71. Rellly, Rich.ard Ii., Killam, Keith F.; Jenney, Elizabeth If.; Marshall,William H.; Tausig, Theodore; Apter, Nathaniel S.; and Pfeiffer, CarlC., "Convulsant Elfects of isoniazid," JAMA, Vol. 152, pp. 1317-1321,1953.
77
72. Robinson, Donald S., Lovenberg, Walter, Keiser, Harry and Sjoerdsma,Albert, "Effects of Drugs on Human Blood Platelet and Plasma AmineOxidase Activity In Vitro and In Vivo," Biochemical Pharmacol., Vol.17, pp. 109-119, 1968.
73. Robitzek, E. l. -and Selikoff, I. J., "Hydrazene Derivatives of Iso-nicotinic Acid in, the Treatment of Active Progressive Caseous-Pneu-monic Tuberculosis: Preliminary Report," Am. Rev. Tuberc., Vol. 65,pp. 402-428, 1952.
74. Robson, 3. M. and Sullivan, F. M., "Antituberculosis Drugs," Pharma-
col. Rev., Vol. 15, pp. 182-185, 1963.
75. Ross, Raymond R., "Use of Pyridoxine hydrochloride to Prevent IsoniazidToxicity;" JAMA, Vol. 168, pp. 273-275, 1958.
76. Rubin, Bernard, Ilassert, G. Lee, Jr., Thomas, Bernard G. H. and Burke,John C., "Pharmacology of Isonicoei-nic Aciu, Hydrazide (Nydrazid),Am. Rev. Tuberc., Vol. 65, pp. 392-401, 1952.
77. Saad, Samir Fahmy, "The Effect of Isoniazid and Some AnticonvulsantDrugs on the y-Aminobutyric Acid Content of Mouse Brain in InsulinHypoglycaemia," J. Pharm. & Pliarmacoi., Vol. 22, pp. 372-374, 1970.
78. Saslaw, Samuei and Klainer, Albert S., "Rheumatoid Syndrome DurinlgIsoniazid Therapy," Am. Rev. Resp. Dis., Vol. 100, pp. 221-223, 1969.
79. Sbarbaro, J. A. and Johnson, S., "Tuberculosis Chemotherapy forRecalcitrant Outpatients Adminai.tered Directly Twice Weekly," Amer.Rev. Res. Dis., Vol. 97, 'pp. 895-904, 1968.
80. Schncider, E., Jungbluch, H. an",i O•Ži,.aL:•n, F., "Die Akute Isoniazid-Intoxikaczion. Fin Netic,!ogi e, f1-ektro.;acepnalographische andTox:ikolog-Lche Verlatzfsunter rcnhun:g" LJ]in. . Vol, 49, pp.904-910, 1971.
81. Scl,rod.3r, 1. M., "Die 7!iusLr• kcuii ,i ý..e• (R2 Ž.nF'cher) Nerven-fasern bei der Isoniiazid-~iieuroaatzu •," Acta NqcupýyLth., Vol. 15,pp. )56-175, 1970.
82. Schrodec. J. M., IZur 1ahoget•. dt £nL•z~e-.eL'r•pathie. I. LineFeinstrukturell5 Diffarenzie:.ua, Ggenuiv: ,aer Wadlerschen Degenera-tion," Ac \, Neuropatin. Vol. <10, ',. 3•01-0, 197.).
83. Schroaer, J. M., "Zur Patnoiens- de," l=,.izid-i-uropathie. II.Phasvnkoncias.. und Ele ronciakroio i' •',, ' ucuugon am Rucken-
.wi.,1 -,~p.- aal g..n,ýieni und LO.~t'~'it N~aropath. , Vol.AU, #*. 32--341, 1970.
i

84. Seidell, Martin, "Isoniazid Induced Life-Threatening Neurologic Re-action in ano Allergic Individual," Ann. of Allergy, Vol. 28, pp.276-281, 1970.
85. Sfitkakis, Paul, "Isoniaiid and Alcohol," Letter to the Editor, Am.Rev. Resp. Dis., Vol. 101, p. 991., 1.970.
86. Shub, Clarence, Salmonsen, Paul C., Jordan, J. E., llofmann, Mark A.and Alexander, Byron B., "Safety of INH Chemoprophylaxis in AviationPersonnel," Aerospace Medicine, Vol. 42, pp. 1325-1335, 1971.
87, Siegel,. Morris, Lee, Stanley, L. and Peress, Nancy S., "The Lpidem-iology of Drug-Induced Systemic' Lupus Erythematosus," Arthritis andRheumatism, Vol. 10, pp. 407-415, 1967.
88. Simmons, William W. and Ambler, Rosalie K., "Isonjazid Prophylaxisas an Aviation Risk: Preliminary Report," Naval Aerospace Medicineinstitute Technical Report, NAMI-1095, November 1969.
89. Singh, A. and Bawa, Y. S., "Isoniazid-Induced Vitamin B Deficiency'State," J. Indian Med. Ass,.., Vol. 48, p. 504, 1967.
90. Sitprija, Visith and Holmes, Joseph H., "Isoniazid Intoxication,"Amer. 'Rev. Resp. Dis., Vol. 90, pp. 248-254, 1964.
91. Smith, Barbara, "The Myenteric Plexus in Drug-Induced Neuropathy,"J. Neurol. Neurosurg. Psychiat., Vol. 30, pp. 506-510, 1967.
92. So=nnichsen, N., Zoeliner, E. and Random€, U., "INH-induced Pellagrain Pulmonary Tuberculosis," Z. Tuberk Erkrar,,en, hroaxorgane, Vol.124, pp. 224-227, 1965.
93. Steinfield, L. 1. and Cohen, ' C., "Experienc¢! ý,'ici IsoniazidProphylaxis in a Large City anaith Department," D)is. Chest, Vol.51, pp. 406-411, 1967.
94. Torman, kivid S. and Teicelbaum, DanietL Y. "Ijoni, d Self-Poisoning,"Neurology, Vol. 20, pp. 299-304, 1970.
95. "Tne To,:i.;ty of isoniazio '" ReporL 01 . ue O io(:,•n on Thecapy,American Trudeau Society, Am. Re,. Tubei:., Vol. 66, pp. 302-305,1953.
96. "The Trc•a•ment of Pulmonary Tub.rcuio.bi., ,.%iti ifsa.iazid," An InterimReport to the Medical Research Council Ioy Thior Tuberculosis Chemo-therapy Trials Cowmittee, brit. •ed. 1., \.'±. i, ps'. 735-746, 1952.
79
97. Theodore, Andrew and Wolff, Marion, "The Effect of Isoniazid on Per-formance in School," Am. Rev., of Resp. Dis., Vol. 101, pp. 252-257,1970.
98. Tiitinen, H. and Mattila, M. J., "Modification of the Serum IsoniazidLevels by Different Preparations of Para-aminosalicyclic Acid,"Arzneimittelforschung, Vol. 18, pp. 623-625, 1968.
99. Torning, K. and Olsen, P. Z., "Isoniazid and Impairment of Memory,"Dis. Chest, Vol. 53, pp. 675-678, 1968.
10. Turpin, R., Bergongne-Berezin, E., Camille, B. and Salmon-Bonnereau,D., "Inactivation of Isoniazid in Down's Syndrome," Lancet, Vol. 2,p. 1369, 1967.
10]. Vysniauskas, Constantine and Brueckner, Harold H., "Severe Reactionsof the Central Nervous System Following Isoniazid Treatment," Am.Rev. of Tuberc., Vol. 69, pp. 759-765, 1954.
102. Whittington, H. G. and Grey,-L.., "Possible Interaction Between Di-sulfiram and Isoniazid," Amer. J. Psychiat., Vol. 125, pp. 1725-1729,1969.
103. Widomska-Czekajska, Teresa, "A Case of Decerebration in the Courseof Acute Intoxication with Isonicotinic Acid Hydrazide," Pol. Tyg.Lek., Vol. 20, pp. 533-534, 1965.
104. Winer, B. J., Statistical Principles in Experimental Design, McGraw-Hill Book Company, 1962.
105. Wood, J. D. and Peesker, S. J., "Sequential Lowering and Raising ofBrain y-Aminobutyric Acid Levels by Isonicotinic Acid Hydrazide,"Canadian J. of Physiol. and Pharmacol., Vol. 49, pp. 780-781, 1971.
106. Year Book of Drug Therapy, Edited by Harry Blackman, M. D., Year BookMedical Publishers, Inc., Chicago, Illinois, 1969.
107. Zbinden, G. and Studer, A., "Experimenteller Beitrag zur Frage desIsoniazid--Neuritis und ihrer Beeinflussung durch Pyridoxin," Z.Tuberk., Vol. 107, pp. 97-107, 1955.
80

ii• I -I
4 V
K-nco4
2c~2r
Lu

APPENDIX 2
SUM4IARY OF ANALYSIS OF VARIANCESERIAL SUBTRACTION - SCORE
Source SS df MS f
Between Subjects 773.94 20
Within Subjects 1108.67 42
Trials 80.03 2 40.02 1.56
Residual 1028.63 40 25.72
TOTAL 1882.62 62
APPENDIX 3
SUMMARY OF ANALYSIS OF VARIANCESERIAL SUBTRACTION - TOTAL TIME
Source SS df MS f
Between Subjects 27916.41 20
Within Subjects 15412.67 42
Trials 345.27 2 172.64 0.46
Residual 15067.40 40 376.69
TOTtT, 43329.08 62

APPENDIX, 4
SUMMARY OF ANALYSIS OF VARIANCEORAL RECALL - SCORE
Source SS dc' MS f
Between Subjqets 435.27 ,20
Within, Subjects 264.00 42
Trials 106.13 2 53. 07 13.45**
Residual 157.87 40 3.95
TOTAL 699.27 62'
**p< .01
APPENDIX 5
TESES ON DIFFERENCES BETWEEN TOTALSORAL RECALL - SCORE
Ordered -Tests Control 12 Mo. 6 Mo.
TOTALS 181 188 242
Control 181 --- 7 61**12 Mo. 188 --- 54**
6 Mo. 242 ---
Truncated Range r 2 3
q.99 (r, 40) 3.82 4.37
/nMSrds q.99 (r, 40) 34.791 39.8002
**p<.O 1

APPENDIX 6
PARAGP•PH STIMULI FOR THE ORAL RECALL TEST -
CONTROL Mary Jones, age 23, of 157 North Walnut Sý,reet, Pbiladel-phia, Pennsylvania,. -was seen. wandering on the 3500 blockof South Main Street, at 3:00 a.m. yesterday, the,13th ofAugust 1959, -having wrecked .her 1957 Buick on the JohnsonBridge,.
6 MONTHS John Smith, age 46, of, 235 South Cherry Street,, Chicago,Illinois, was apprehended at the 1600 block of NorthDevon Street, at 1:00 a.m; -yesterday, the 23rd:;of July1969, aftdr stea-ling a 1968 Cadi1lac from Nicho1as.MotorCompany.
12 MONTHS Bill Morrisý ,age 29, of 758 West Holly Lane,, Baltimore .Maryland', wa\s observed at 2900', East Lombard Street at5:00 p.m. yesterday, the 16th of October 1970. He hadjust left the 301 Club located next to the First Nation-al Bank Building.

APPENDIX 7
SUMMARY 'OF ANALYSIS OF VARIANCEAMPLITUDE OF AFTER DISCHARGE - 'CHANNEL 1
Source SS df MS f
Between Subjects 5796 17
Within Subjects 12388 36
Trials 2756 2 1378 4.85*
Residual 9652 34 284
TOTAL 53
'*p<. 0 5
APPENDIX 8
SUMMARY OF ANALYSIS OF VARIANCEAMPLITUDE OF AFTER DISCHARGE - CHANNEL 2
Source SS df MS f
Between Subjects 41-54.81 17
Within Subjects 9018.67 36
Trials 509.04 2 254.52 1.02
Residual 8509.63 34 250.28
TOTAL 13665.48 53
85,•
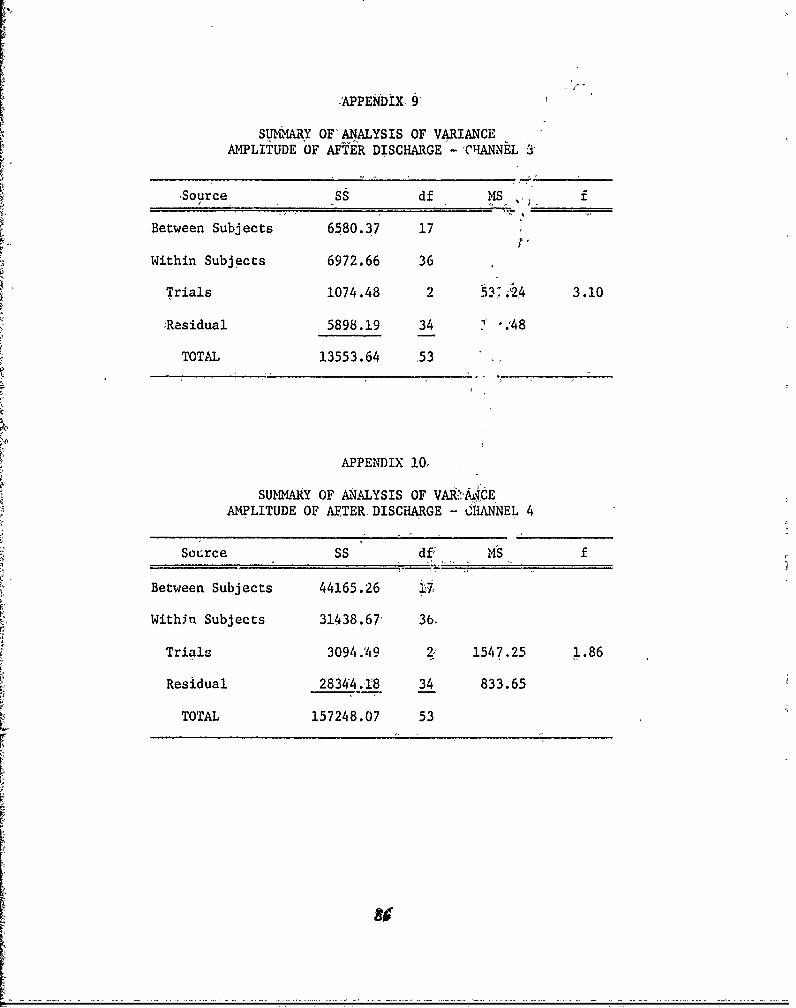
APPENDIX, 9
SUIVMARY OF ANALYSIS OF VARIANCEAMPLITUDE OF AFTER DISCHARGE - 'CHANNEL a
Source SS df MS f
Between Subjects 6580.37 17 ,
Within Subjects 6972.66 36
Trials 1074.48 2 53i24 3.10
)Residual 5898.19 34 -. ,48
TOTAL 13553.64 53
APPENDIX 10O
SU mmRY OF ANALYSIS OF VAR>*jCEAMPLITUDE OF AEFTER DISCHARGE - CHANNEL 4
Source SS df, MS f
Between Subjects 44165.26 ;J
Within Subjects 31438.67 3b.
Trials 3094.49 2; 1547.25 1.86
Residual 28344.18 34 833.65
TOTAL 157248.07 53
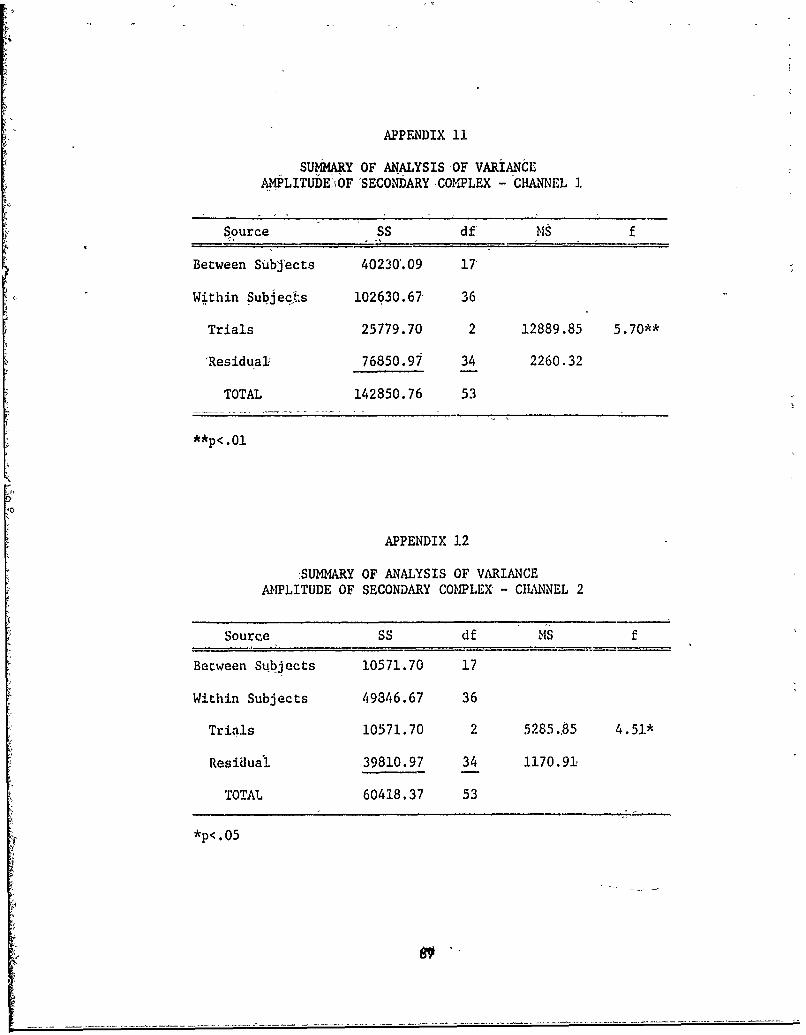
APPENDIX 11
suMMARY OF ANALYSIS-OF VARIANCEAMPLITUDEI•OF SECONDARY ,COMPLEX - CHANNEL 1
Source SS df MS f
Between Subjects 40230'.09 17
Within Subjeqt.s 102630.67, 36
Trials 25779.70 2 12889.85 5.70**
'Residual, 76850.90 34 2260.32
TOTAL 142850.76 53
**p< .01
APPENDIX 12
:SUMMARY OF ANALYSIS OF VARIANCEAMPLITUDE OF SECONDARY COMPLEX - CHANNEL 2
Source SS df MS f
Between Subjects 10571.70 17
Within Subjects 49346.67 36
Trials 10571.70 2 5285.85 4.51*
Residual 39810.97 34 1170.91,
TOTAL 60418.37 53
*p<. 0 5

APPENDIX. 1:3
SUMMARY OF 0ANALYSIS OF VARIANCEAMPLITUDE OF SECONDARY COMPLEX - CHANNEL 3
Source SS df MS f
Between ,Subjects 12780 17
Within Subjects 34960 36
Trials 6500.11 2 3250.06 3.88*
Rcsidual 28459.89 34- 837.06
TOTAL 76i99,.89 53
*p<.05o
APPENDIX 14
SUMMARY OF ANALYSIS OF VARIANCEAMPLITUDE OF SECONDARY COMPLEX - CHANNEL 4
Source SS df MS f
Between Subjects 65884.31 i7
Within Sub-j'e6ts 12810. 36
Trials 14889.81 2 7444.91 2.24
Residual 113218.19 34 3329.95
TOTAL 193992.31 53
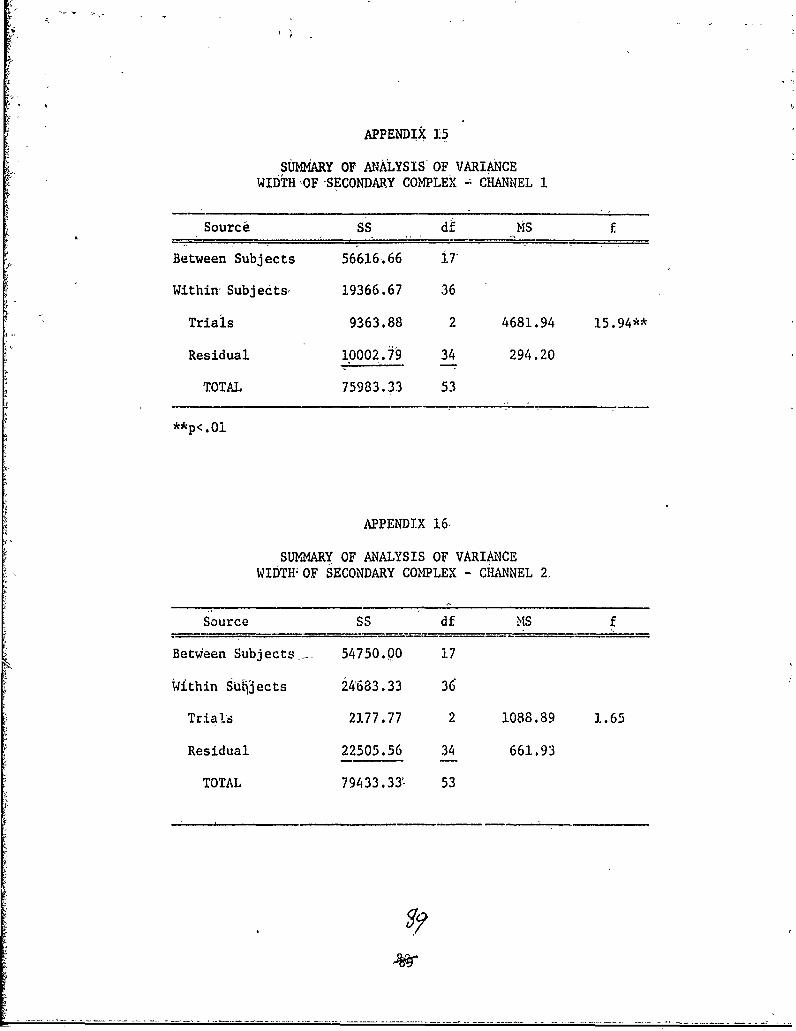
APPENDIX 15
SUMMARY OF ANALYSIS OF VARIANCEWIDTH OF SECONDARY COMPLEX - CHANNEL 1
Source SS df MS f
Between Subjects 56616.66 i7'
Within Subjects, 19366.67 36
Trials 9363.88 2 4681.94 15.94**
Residual 10002.79 34 294.20
TOTAL 75983.33 53
**p<.O 1
APPENDIX 16
SUMM&ARY OF ANALYSIS OF VARIANCEWIDTH OF SECONDARY COMPLEX - CHANNEL 2.
Source SS df MS f
Between Subjects,. 54750.00 17
Within S§U1ects 24683.33 36
Trials 2177.77 2 1088.89 1.65
Residual 22505.56 34 661.93
TOTAL 79433.331 53

APPENDIX.17
SUMMARY, OF ANALYSIS OF VARIANCEWIDTH OF SECONDARY COMPLEX - CH'NNEL 3
Source SS df MS f
Between Subjects 45870.83 17
'Within Subjects 31100.00 36
T-.:ials 1425.00 2 h12.50 .82
Recidual 296Z5.00 34 872.79
TOTAL 76970.83 53
APPENDIX 18
SUMMARY OF ANALYSIS OF VARIANCEWIDTH OF SECQNDARY COMPLEX - CHANNEL 4
Source SS df MS f
Between Subjects 56987.50 17
Within Suibj edts 16•383.33 36
Trials 44.44 2 22.,22
Res•Ldual 16338.89 34 430.56 .05
TOTAL 7337C,83 53
90
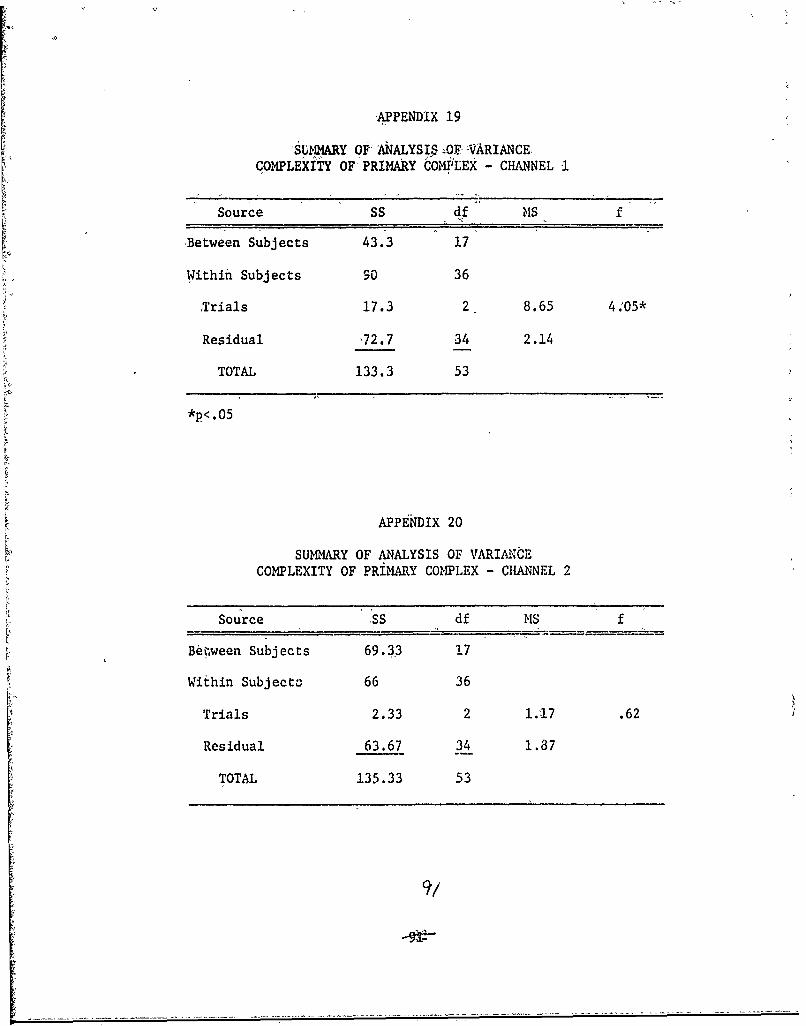
ýAPPENDIX 19
SUMMARY OF ANALYSI$ AOF• VARIANCE.COMPLEXITY OF PRIMARY COMJ!LEX - CHANNEL I
Source SS df MS f
Between Subjects 43.3 17
Within Subjects 90 36
•Trials 17.3 2 8.65 4.05*
Residual -72.7 34 2.14
TOTAL 133.3 53
*p<. 0 5
APPENDIX 20
SUMMARY OF ANALYSIS OF VARIANCECOMPLEXITY OF PRIMARY COMPLEX - CHANNEL 2
Source SS df MS f
Beiween Subjects 69.33 17
Within Subject: 66 36
Trials 2.33 2 1.17 .62
Residual 63.67 34 1.87
TOTAL 135.33 53
9,/

APPENDIX 21
-SUYIiARY OF ANALYSIS OF- VARIANCECOMPLEXITY OF PRIMARY COMPLEX CHANNEL 3
Source SS df MS f
-Between Subjects 62.83 17
Within Subjects 42 36
Trials 5.77 2 2.89 2'.70
Residual 36.23 34 1.07
TOTAL 104,83 53
APPENDIX 22
SUMMARY OF ANALYSIS OF VARIANCECOMPLEXITY OF PRIMARY COMPLEX - CHANNEL 4
Source SS df MS f
Between Subjects. 17.26 17
Within Subjects 46.67 "• 36
Trials 1.82 2 .91 .69.
Residual 44.85 34 1.32
TOTAL 63.95 53

APPENDIX 23
SUMMARY OF ANALYSiS OF VARIANCECOMPLEXITY OF SECONDARY COMPLEX - CHANNEL 1
'Source, SS df MS f
Between Subjects 98.66 J.7
Within Subjects 68.67 36
Trials 6.1' 2 3.39 il86,
Residual 61.90 34 1.82
TOTAL 167 .,3 53
APPENDIX 24
SUMMARY OF A1'ALYSIS OFtVARIANCECOMPLtXITY OF SECONDARY COMPLEX - CHANNEL 2
'Source SS MS f
Between Subjects 68,.j/6 17
Within Subjects 142.00 36
Trials 11. 59 2 5.80 1. 51[
Residual 130.41 34 3.84
TOTAL 210.76 53
935
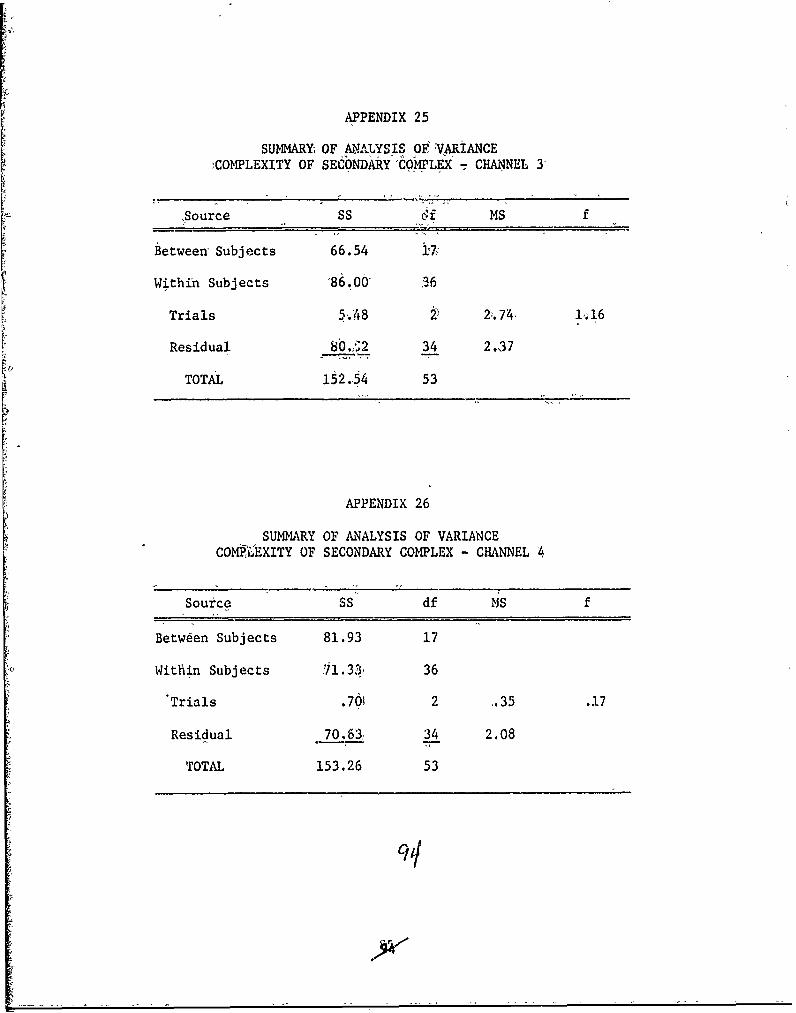
APPENDIX 25
SUMMARY OF ANALYSIS OF VARIANCE)COMPLEXITY OF SECONDARY COMPLEX CHANNEL 3
Source SS 6cf MS f
Between Subjects 66.54 i7i
Within Subjects -86.06' 36
Trials 5.4 8 2;. 74 i, 16
Residual 8b.,2 34 2.37
TOTAL 152.54 53
APPENDIX 26
SUMMARY OF ANALYSIS OF VARIANCECOMPLEXITY OF SECONDARY COMPLEX - CHANNEL 4
Source SS df MS f
Between Subjects 81.93 17
Within Subjects 71.33, 36
"Trials .761 2 .35 .17
Residual 70,63, 34 2.08
TOTAL 153.26 53

APPENDIX 27
SUMMARY OF ANALYSIS OF VARIANCECOMPLEXITY OF AFTER DISCHARGE - CHANNEL 1
Source SS df NS f
Between Subjects 155.33 17
Within Subjects 2Y'; . 36
Trials )'2.33 2 16.11 :.96
Residual 185.67 34 5.46
TOTAL 373.33 53
APPENDIX 28
SUMM1ARY OF ANALYSIS OF VARIANCECOMPLEXITY OF AFTER DISCHARGE - CIANNEL 2
Source SS df MS f
Between Subjects 300.76 17
Within Subjectb 327.33 36
Trials 27.37 2 13.69 i.51
Residual 299.96 34 8. t,
TOTAL 628.09 53

APPENDIX 29
SUMMARY OF ANALYSIS OF VARIANCE.-COMPLEXI-TY OF AFTER DISCHARGE - CHANNEL 3
Source SS df MS f
Between Subjects 246.67 17
Within Subjects 215.33 36
Trials 19.11 2 9.56 1.66
Residual 196.22 34 507
TOTAL 462.00 53
APPENDIX 30
SUMMARY OF ANALYSIS OF VARIANCECOMPLEXITY OF AFTER DISCHARGE - CHANNEL 4
Source SS df MS f
Between, ,Subjects 236.67 17
Within Subjects 179.33 36
Trials 27.44 2 13.72 3.07
Residual 151.89 34 4.47
TOTAL 416.00 A
96

APPENDIX 31
SUMMARY OF ANALYSIS OF VARIANCELATENCY TO PEAK DEFLECTION -,CHANNE'L 1
Source SS df MS f
Between Subjects 55630.09 17
Within Subjects 35466.67 36
Trials 695.37 2 347.69 .34
Residual 34771.30 34 1,022.69
TOTAL 91096.76 53
APPENDIX 32
SUMI*MY OF ANALYSIS OF VARIANCELATENCY TO PEAK DEFLECTION - CRANNEL 2
Source SS df MS f
Between Subjects 36163.64 17
Within Subjects 73760.67 36
Trials 185.03 2 92-52 .04
Residual 73575.64 34 2163.99
TOTAL 109924.31 53
97

APPENDIX 33
SUMMARY 'OF'ANAYSIS OF- VARIANCE'LATENCY TO ,PEiAK DEFLECTION -- CHANNEL 3
Source 'SS df Ms' fi
Between Subjects 20870.83 17
Within Subjects ,66750.00 36
Trials 4852.77 2426.39 1.33
Residual 61897.23 34 1820.51
TOTAL 87620.83 53
APPENDIX 34
SUMMARY OF ANALYSIS OF VARIANCELATENCY TO PEAK DEFLECTION - CHANNEL 4
Source ss df MS f
Between Subjects 55687.04 17
Within Subjects 51933.33 36
Trials 1362.04 2 681.02 .46
Residual 50571.29 34 1487.39
TOTAL 108620.37 53
98

APPENDIX 35
SUMMARY OF ANALYSIS OF VARIANCEAMPLITUDE OF PRIMARY COMPLEX - CHANNEL 3
'Source SS df MS f
Between Subjects 1.556.60 17'
Within Subjects 4117.33 36
Trials 318.82 2 109.41 95
Residual, 3898.51 34 114.66
TOTAL 5673.93
APPENDIX 36
SUMM•RY OF ANALYSIS OF VARIANCEAMPLIhUDE OF PRIMARY COMPLEX - CHANNEL 2
Source SS df MS f
Between Subjects 2420.1b 17
Within Subjects 8462.67 36
Trials 939..11 2 1169.5o 2. L_
Residual 7523.56 34 22i.28
TOTAL 10882.83 511

APPENDIX 37
SUkHARY OF ANALYSIS OF VARIANC.AMPI'rUDE oF PRIMARY COMPLEX -,CHANNEL 3
'Source SS df MS f
Betweeni2Subjects 2205.92 17
Within, Subjects 4146.67 36
Trials 827. 26 2 413.63 4.24*
Residual 3319.41 34 97.63
TOTAL 6352.59 53
/*pi.05
APPENDIX 38
SU•MARY OF ANALYSIS OF VARIANCEAMPLITUDE OF PRIMARY COMPLEX - CHANNEL 4'
Source SS df MS f
Between Subjects 16514.83 17
Within Subjects 29200.00 36
Trials 376.33 2 188.17 .22
Residual 28823.67 34 847.76
TOTAL 45714.83 53
100

APPENDIX 39
SUMMARY OF ANALYSIS OF VARIANCESECONDARY COMPLEX - LATENCY TO ,BEGINNING - CHANNEL 1
Source SS df MS f
Between Subjects 14396.76 17
Within Subjects 15100.00 36
Trials 423.15 2 211.58 .49
Residual 14676.85 34 431.67
TOTAL 29496.7b 53'
APPENDIX 40
SUMMARY OF ANALYSIS OF VARIANCESECONDARY COMPLEX - LATENCY TO BEGINNING - CHANNEL 2
Source SS df MS
Between Subjects 8385.6: 17
Within Subjects 11550.00 36
Trials 950.93 2 475.47 1.53
Residual 10559.07 34 311.74
TOTAL 19935.65 53
101

APPENDIX 41
SUMMARY OF ANALYSIS OF VARIANCESECONDARY COMPLEX - LATENCY TOý BEGINNING- CHANNEL 3
Source SS df MS, f
Between Subjects 10075.92 17
Within Subjects 5616.67 36
Trials 8M .26 2 42.13 .26
Residual 553 .41 34 162.72
TOTAL 15692.59 53
APPENDIX 42
SUMMARY OF ANALYSIS OF VARIANCESECONDARY COMPLEX - LATENCY TO BEGINNING;- CHANNEL 4
Source SS, df MS, f
Between Subjects 9468.98 17
Within Subjects 9983.33 36
Thials 1195.37 2 597.69 2.31
Residual 8787.96 34 258.47
"TOTAL 19452.31 53
102

APPENDIX 43
TESTS ON, DIFFERENCES BETWEEN TOTALSAMPLITUDE OF AFTER DISCHARGE - CHANNEL 1
Ordered Measures Control 6 1o. 12 No.
TOTALS 306 383 609
Control 306 --- 7,7 303*6 Mo. 383 --- 226*12 Mo. 609
Truncated Range r 2 3
q.9 5 (r, 30) 2.89 1.49
N7Src s q95 (r, 30) 206.37 249.22
*p<.05
APPENDIX 44
TESTS ON DIFFERENCES BETWEEN TOTALSAMPLITUDE OF PRIMARY COMPLEX- CHANNEL 3
Ordered Measures Control r mo. 12 Mo.
TOTALS 268 404 428
Control 268 --- 136* 230*6 No. 404 --- 24.12 4,io. 428 ---
Truncated Range r 2 3
q.95 (,r, 30) 2.89 3.49
/nMSres q95 (r, 30,) 83.84 125.76
*p<.0 5
103

~APPEilbIX 45
TESTS ON ,DIFFERENGES BETWEEN TOTALS,COMPLEXITY OF PRIMPtV 'COMPLEX - CHANNEL 1
Ordered Measures Control- 6 Mo'. i2 Mo.
TOTALS 44 62 68
Control 44 18* 24*6 Mo. 62 -- 6
12 Mo. 68
Truncated Range r 2 3
q.95, (,r, 30) 2.89 3.49
n/nMSTesF q95 (r, 30) 17.49 21.66
*p< .05
APPENDIX 46
TESTS ON DIFFERENCES ,BETWEEN TOTALSWIDTH OF SECONDARY 'COM4PLEX - CHANNEL 1
Ordered Measures 6 Mo. Control 12 Mo.
TOTALS 2645 2925 2940
6 Mo. 2645 --- 280* 295*Control 2925 1512 Mo. 2940
Truncated Range r 2 3
q95 '(r, 30) 2;89 3.49
vGnMSres q95 (r, 30) 210,31 253.97
*P-,.05
104

APPENDIX 47
TESTS ON DIFFERENCES BETWEEN TOTALSAMPLITUDE OF SECONDARY COMPLEX - CHANNEL 3
Ordered Measures 6 Mo. Control :1.2 Mo.
TOTALS 689 763 1140
6 Mo. 689 --- 74 451.*Control 763 --- 377-12 Mo. 1140
Truncated Range r 2 3
q9 5 (r, 30) 21.89 3.49
"nMSres q95 (r, 30) 354.74 428.39
*p<. 0 5
APPENDIX 48
TESTS ON DIFFERENCES BETWEEN 'TTALSAMPLITUDE OF SECONDARY COMPLEX -'CMANNEL 1
Ordered Measures. 6 Mo. Con•trol 12 Mo.
TOTALS '579 737 14 18
6 Mo. 579 --- 1-58 , 02-zControl 737 --- 744*12 Mo. 1,48].
Truncated Range r 2 3
q95 (r, 30) 2.89 3.49
iVnM res q95 (r, 30) 583.42 704."
*p< .05
105

APPENDIX 49'
TESTS ON DIFFERENCES BETWEEN MEANSAMPLITUDE OF SECONDARY COýIPLEX - CHANNEL 2
Ordered •Measures Control 6 Mo. 12 Mo.
TOTALS 544 614 1096
Control, 544 70 552*6 Mo., 614 --- 482*12 Mo. 1096
Truncated Range r 2 3
q.95 (r, 30) 2.89 3.49
Cýffsres -q95 (ri 30)- 419.56 506.67
*p< .05
106