use of drugs in cardiogenic shock due to acute...
TRANSCRIPT
Use of Drugs in Cardiogenic Shockdue to Acute Myocardial Infarction
By ROLF M. GUNNAR, M.S., M.D., AND HENRY S. LOEB, M.D.
SUMMARYAs a plan of therapy for shock associated with acute myocardial infarction in a
general hospital and assuming that septic and hemorrhagic shock has been eliminatedas diagnostic possibilities we would suggest the following:
(1) Pain should be relieved using morphine or pentazocine, and atropine if brady-cardia is present. Oxygen by mask should be administered to bring the arterial oxygentension to about 100 mm Hg. The airway must be examined and, if air exchange ispoor and the artelial oxygen very low or carbon dioxide high, respiratory assistanceand occasionally intubation may be required.
(2) Blood pressure must be stabilized at an adequate level for perfusion of vitalorgans, or progression may be so rapid that death will occur before proper evaluationcan be made and more rational therapy started. For this purpose we would start anorepinephrine infusion at a rate just sufficient to keep the systolic blood pressure near100 mm Hg. If the shock syndrome is present but arterial pressure is normal or onlyslightly reduced, we would eliminate this step in therapy.
(3) Arrhythmias or heart block should be corrected by methods discussed elsewherein this symposium.
(4) A venous catheter should be inserted so that the catheter tip is just within thethorax. If the central venous pressure (CVP) is below 10 cm H20 we would begin aregimen of plasma volume expansion giving 100 cc of 40dextran over a peliod of 10min, waiting 10 min, and if the CVP has not risen 1 cm H20 repeat the process untilshock is relieved, the CVP continues to increase or is above 15 cm H20, or 1000 ccof 40dextran has been given. If the patient accepts more than 1000 cc of fluidin this manner without elevating the CVP it is most likely that some othermajor process causing fluid loss is complicating the myocardial infarction.
(5) If or when CVP is above 10 cm H20, and if the patient remains in shock and ishypotensive, we would add norepinephrine infusion at a rate just sufficient to bringthe systolic pressure between 100 and 110 mm Hg. If this cannot be accomplishedwith small amounts of norepinephrine then intraarterial pressure must be measuredsince the discrepancy between the cuff pressure and actual pressure may be increasingwith further pressor infusion.
(6) If the patient is normotensive and has a CVP above 10 cm H20 but manifeststhe shock syndrome, an isoproterenol infusion should be instituted, but to use thisregimen one must be able to measure intraarterial pressure. If CVP falls, simultaneousplasma volume expansion may be necessary. If arterial pressure begins to fall, nor-epinephrine should be substituted. We would use dopamine first in this particularsituation, but this agent is not as yet generally available.
(7) With the CVP elevated and blood pressure stable, arterial oxygenation estab-lished, and arrhythmias corrected, if the patient is still in a low cardiac output state withcontinued oliguria and poor tissue perfusion, digsalization with about half to twothirds the normal digitalizing dose should be undertaken.
(8) If a further inotropic response is needed glucagon may be added at this point.With an initial bolus injection efficacy should be established and if found helpful aconstant infusion should follow. Aminophylline should be given simultaneously topotentiate the action of glucagon.
(9) The patient who at this point remains oliguric and with a small pulse pressuremay be benefited by cautious vasodilation with chlorpromazine or phentolamine andsimultaneous further plasma volume expansion.
(10) A patient who remains pressor-dependent or responds poorly to pressors willprobably need circulatory assistance. However, unless some definitive measure can be
Circulation, Volume XLV, May 1972 1111
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

GUNNAR, LOEB
undertaken to restore or replace inonfunctioninig myocardium this too will be of littlebenefit.
(11) A patient wlho stabilizes well but experiences a fall in blood pressure as thepressor infusion is being discontinued should have plasma volume expansion as thepressor infusion is decreased. The physician must resist the temptation to restart theinfusion as the pressure falls, unless the shock syndrome accompanies the hypotension.
SHOCK IS A CLINICAL syndrome whichincludes obtundation, oliguria (urine
flow<30 cc/hour), cold cyanotic extremities,and small pulses. Blood pressure as measuredby the standard cuff method is usually low butintraarterial pressure measured directly mavbe low, normal, or high. Since the clinicalsyndrome is not dependent on a low intraarte-rial pressure one should classify shock as beingwith or without intraarterial hypotension. Theshock syndrome associated with acute myo-
cardial infarction has multiple factors in itsetiology,' and although ventricular dysfunc-tion is usually the most significant componentthe terms myocardial infarction shock andcardiogenic shock must not be used inter-changeably. Cardiogenic shock refers to thatportion of the syndrome which is due tomalfunction of the heart as a pump butignores the reflex changes in the peripheralvascular system, the effective plasma volumedeficit, and ventilatory abnormalities whichoccasionally become dominant.Myocardial infarction results in decreased
cardiac output.2 3 The ischemic myocardiumbulges with systole4 and the remaining func-tioning muscle not only has to substitute forthe nonfunctioning, tissue but also mustovercome the damping effect of the expandinginfarcted area. The resultant decreased rate ofpressure rise5 activates the baroreceptors ofthe carotid sinus and aorta thus calling forvasoconstriction to maintain arterial pressure.
The surprising finding is that more than halfof the patients with myocardial infarction,shock, and hypotension have normal ratherthan elevated systemic vascular resistance."
Agress called attention to this lack ofvasoconstriction, and by injecting beads intothe coronary arteries to produce infarctionconstructed an experimental model to simulatethe clinical syndrome.7 In his animals thecardiac output and arterial pressure fell whilethe vascular resistance remained constant. If,in addition, the animals had dorsal sympa-thectomy and vagotomy, the decrease incardiac output was accompanied by vasocon-
striction and arterial pressure was maintained.He attributed the inhibition of vasoconstric-tion to a reflex arising in the coronary arteriesbut differing from the Jarish-Bezold reflex innot being abolished by vagotomy. Morerecently, it has been postulated that ischemiaactivates receptors in the ventricular myocar-
dium causing inhibition of the vasoconstrictorresponse.Y These receptors may be stretchreceptors activated when the ischemic musclebulges during systole.9 The afferent fibershave been located as being vagal10 or
sympathetic" and cause central inhibition ofsympathetic tone. In addition to these studiesin the experimental animal, it has recentlybeen demonstrated that patients with acutemyocardial infarction have decreased vaso-
constriction during head-up tilt, again indicat-ing inhibition of normal sympathetic re-
sponses.'12The lack of vascular response to a fall in
cardiac output seen in the patient with acutemyocardial infarction is not easily recognizedclinically.'3 14 Such patients without general-ized vasoconstriction demonstrate the bestrecovery rate with pressor infusion, havehigher cardiac outputs, and may have lesseramounts of myocardial damage.15 Since long-term survival is most likely to occur in thepatients with the least myocardial destruction,identification of the patient in shock withnormal resistance is important.
Circulation, Volume XLV, May 1972
From the Department of Adult Cardiology,Division of Medicine, Cook County Hospital andHektoen Institute for Medical Research, and from theDepartment of Medicine, University of Illinois Collegeof Medicine, Chicago, Illinois.
1112
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

DRUGS IN CARDIOGENIC SHOCK IN MI
Myocardial infaretion is in general associat-ed with diffuse disease of the coronaryarteries.'6 Partial occlusion of a vessel causes apressure gradient over the narrowing and,therefore, a significant pressure difference mayexist between aortic diastolic pressure and theperfusion pressure at the level of the arteri-oles. It is probable that vessels distal to areasof partial occlusion as well as vessels in theischemic zone will be maximally vasodilated.17For these reasons very significant amounts ofthe myocardium may have a blood supplywhich is pressure-dependent and no longerable to adjust by autoregulation.18 This samesituation may also pertain to cerebral andrenal blood flows if there is partial occlusionof the major arteries to these organs.Hypovolemia may be a significant factor in
shock associated with myocardial infaretion.19A loss of intravascular volume may occur notonly as a result of reduced fluid intake but alsodue to prolonged vasoconstriction, vomitingassociated with the pain of infarction ormedication, sweating, or the use of potentdiuretic agents which can reduce intravascularvolume precipitously. Circulatory arrest mayproduce such profound acidosis at the capil-lary level that vascular integrity is lost, fluidrapidly leaves the intravascular compartment,and dilatation of the capacitance vesselsoccurs. Since the injured myocardium needs ahigher filling pressure to maintain an adequatecardiac output the reduced filling pressureassociated with hypovolemia may result inshock in a patient with acute myocardialinfarction even though the extent of myocar-dial damage is only moderate. Sudden loss ofintravascular volume in acute myocardialinfarction therefore may set off a chain ofevents (hypotention -* use of pressor agents ->further loss of intravascular volume -> decreas-ing cardiac output) which will increase theextent of myocardial damage.The appearance of clinical shock in a
patient with acute myocardial infaretionshould not preclude considering noncardiaecauses of shock such as sepsis or hemorrhage.The clue may not be obvious but a lowcentral venous pressure (CVP), a fever out ofCirculation, Volume XLV, May 1972
proportion to the myocardial necrosis, asudden fall in hematocrit, shock in a patientlacking electrocardiographic changes of trans-mural infaretion, or shock associated with anormal or high cardiac output should allinitiate a search for additional nonmyocardialcauses of shock.13
Plasma Volume Expansion in Shockof Myocardial Infarction
Most patients with shock and myocardialinfaretion have severe myocardial damage andhave an elevated CVP. However, there aresome patients who, as noted above, have aninadequate effective blood volume. If the CVPis below 10 cm H20, fluid challenge shouldprecede all forms of therapy unless hypoten-sion is so profound that immediate stabiliza-tion of arterial pressure is mandatory. Langs-joen et al. reported a reduced mortality rate inpatients treated with low molecular-weightdextran after acute myocardial infarction.20Although the therapy was designed to de-crease intravascular sludging, the authorspostulated that correction of undetected hypo-volemia might have contributed to the im-proved survival. Nixon et al. pointed out theneed for fluid to elevate the cardiac fillingpressure of patients in shock with myocardialinfaretion and advocated infusion of dextrosesolution as initial therapy of all patients withthis syndrome.21 Allen et al. reported hypo-volemia to be present in 20% of patients withcardiogenic shock and advocated initial dex-trose infusion as therapy.22Normal or slightly reduced blood volumes
have been reported in patients with shock andmyocardial infaretion.23 However, withoutknowing the individual's normal blood volumeprior to shock it is difficult to use bloodvolume measurements in adjusting fluid ther-apy. For this reason Weil et al. haveadvocated fluid challenge and careful monitor-ing of the CVP for diagnosis and treatment ofhypovolemia.24 The information needed tomonitor fluid infusion in myocardial infarc-tion, in order to be certain that pulmonaryedema is not precipitated, is the left atrial orpulmonary venous pressure. At the same time
1113
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from
GUNNAR, LOEB
a measure of left ventricular end-diastolicpressure (LVEDP) must be known in orderto assure that the left ventricle is working atpeak performance on the function curve,utilizing the Frank-Starling mechanism.Scheinman et al. used pulmonary artery end-diastolic pressure as an equivalent of meanleft atrial pressure.25 Swan and Ganz haveconstructed a catheter with a balloon cuff nearthe tip. This catheter can be floated into thepulmonary artery and by inflating the balloonthe pulmonary artery is occluded and pulmo-nary venous pressure as transmitted throughthe pulmonary capillaries can be measuredfrom the tip of the catheter distal to theballoon.26 Both of these methods assesspulmonary venous pressure and fulfill therequirements for monitoring to avoid thedanger of pulmonary edema, but neithermethod gives a measure of the pressure whichis a determinant of ventricular function(LVEDP).We have been impressed with the ease of
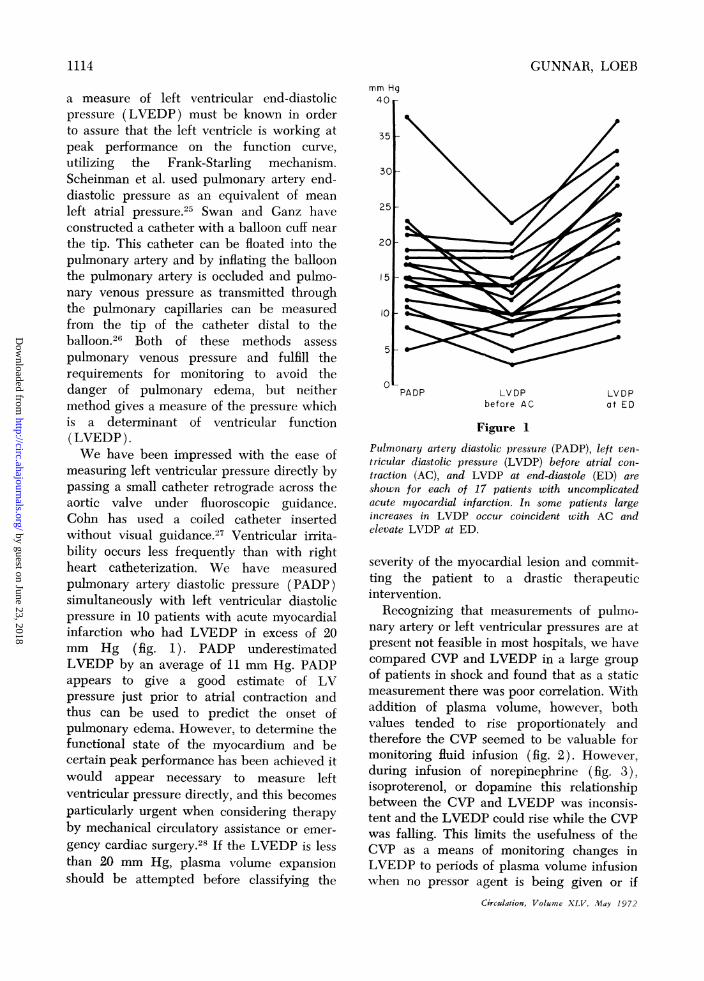
measuring left ventricular pressure directly bypassing a small catheter retrograde across theaortic valve under fluoroscopic guidance.Cohn has used a coiled catheter insertedwithout visual guidance.27 Ventricular irrita-bility occurs less frequently than with rightheart catheterization. We have measuredpulmonary artery diastolic pressure (PADP)simultaneously with left ventricular diastolicpressure in 10 patients with acute myocardialinfarction who had LVEDP in excess of 20mm Hg (fig. 1). PADP underestimatedLVEDP by an average of 11 mm Hg. PADPappears to give a good estimate of LVpressure just prior to atrial contraction andthus can be used to predict the onset ofpulmonary edema. However, to determine thefunctional state of the myocardium and becertain peak performance has been achieved itwould appear necessary to measure leftventricular pressure directly, and this becomesparticularly urgent when considering therapyby mechanical circulatory assistance or emer-gency cardiac surgery.28 If the LVEDP is lessthan 20 mm Hg, plasma volume expansionshould be attempted before classifying the
mm Hg40
35
30_
251
201
15 v1
10-
5
0PADP LVDP
before ACLVDPat ED
Figure 1
Pulmonary artery diastolic pressure (PADP), left ven-tricular diastolic pressure (LVDP) before atrial con-traction (AC), and LVDP at end-diastole (ED) areshown for each of 17 patients with uncomplicatedacute myocardial infarction. In some patients largeincreases in LVDP occur coincident with AC andelevate LVDP at ED.
severity of the myocardial lesion and commit-ting the patient to a drastic therapeuticintervention.
Recognizing that measurements of pulmo-nary artery or left ventricular pressures are atpresent not feasible in most hospitals, we havecompared CVP and LVEDP in a large groupof patients in shock and found that as a staticmeasurement there was poor correlation. Withaddition of plasma volume, however, bothvalues tended to rise proportionately andtherefore the CVP seemed to be valuable formonitoring fluid infusion (fig. 2). However,during infusion of norepinephrine (fig. 3),isoproterenol, or dopamine this relationshipbetween the CVP and LVEDP was inconsis-tent and the LVEDP could rise while the CVPwas falling. This limits the usefulness of theCVP as a means of monitoring changes inLVEDP to periods of plasma volume infusionwhen no pressor agent is being given or if
Circulation, Volume XLV, May 1972
1114
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

DRUGS IN CARDIOGENIC SHOCK IN MI
Changes in CVP and LVEDP following Infusion ofWeight Dextran in 17 Patients
15LVEDP mm. Hg
Low Molecular
* = Pre LMWD
o = Post LMWD
30
Figure 2
Central venous pressure (CVP) and left ventricular end-diastolic pressure (LVEDP) beforeand after infusion of low molecular-weight dextran (LMWD) in patients with various typesof shock. Although the CVP and LVEDP did not correlate well before LMWD, withLMWD infusion LVEDP and CVP showed parallel changes.
Changes in CVP and LVEDP during Infusion of Norepinephrinein 12 Patients
* = Pre - norepi neph r ne
o=During norepinephrine
'P
I5 105 10 15
LVEDP mm. Hg
Figure 3
20 25 30
CVP and LVEDP before and during norepinephrine infusion in 12 patients with shock. Noclear relationship between changes in CVP and LVEDP is apparent during infusion ofnorepinephrine.
m
E
0
25r
20p
I 5
EE
> 100
5
1115
)25
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

GUNNAR, LOEB
pressors are being infused to periods whenthe rate of pressor infusion is not altered.We have used 4"dextran as the agent forvolume expansion as have Cohn et al.29This agent has the advantage of dispersingred-cell aggregates and preventing plateletclumping. Nixon et al. have advocated the useof 5% dextrose solution21 as have Swan et al.0who suggested monitoring pulmonary arterypressure and giving 20 cc/min of 5% dextrosefor 5-15 min or until the pulmonary arterydiastolic pressure increased more than 4 mmHg. Dextrose solutions, if used, must be givenrapidly so that they challenge the extent towhich the intravascular compartment is filled.When dextrose solutions are given slowly thefluid may leave the intravascular compartmentas rapidly as the infusion adds volume andthereby edema may develop and the cardiacfilling pressure not rise. A 3.5% solution ofserum albumin would also be an adequatesubstitute for dextran and might not leave theintravascular compartment as rapidly as eitherdextrose or dextran. We have used a modifi-cation of Weil's method for volume challengeby giving 100 cc of 40dextran over a 10-minperiod, waiting 10 min, and then if CVP hasnot increased by more than 1 cm of H20repeating the process. This is continued untilthe CVP continues to increase, exceeds 15 emH1,0, or shock is relieved, or 100 cc has beengiven. With treatment of 10 patients in thismanner we witnessed recovery from shock inseven and long-term survival in five.19 A 50%survival is so remarkable in this illness that itsuggests that myocardial damage in thesepatients was only moderate and that hypo-volemia was the added complication whichproduced the shock syndrome.
NorepinephrineUsing a definition of shock in myocardial
infarction which includes systolic blood pres-sure below 80 mm Hg, Binder et al. found thesurvival rate without vasopressors to be about10%.31 If patients with volume depletion areexcluded, the survival rate with the use ofpressor agents in most series has been between20 and 30%.32 Pure vasoconstrictors such asmethoxamine, neosynephrine, or angiotensin
are not of value in the treatment of shock withacute myocardial infarction.15 Increasing af-terload merely increases the work of the heart,and since these agents are without inotropiceffects the ventricle dilates. As this increaseswall tension and oxygen needs, the ventricle isthereby required to work from an even greatermechanical disadvantage.The first hemodynamic studies of response
to pressors were by Malmcrona, Schroder, andWerko who reported on nine patients withrecent myocardial infarction, five of whomhad periods of systolic blood pressure below100 mm Hg.33 They showed increases incardiac output during metaraminol infusion inseven of the nine patients. Smulyan, Cuddy,and Eich studied seven patients in shock withmyocardial infarction measuring the effects ofnorepinephrine in five and metaraminol in twopatients.34 Cardiac output increased in onlytwo patients although in most of the patientssystemic arterial pressure was brought above110 mm Hg during treatment. Shubin andWeil treated 10 patients with either norepi-nephrine or metaraminol and demonstrated anincrease in cardiac output and arterial pres-sure.35 They made the very important obser-vation that when the arterial pressure wasbrought above 90 mm Hg there was adecrease in cardiac output and an increase insystemic vascular resistance. We have report-ed on the use of norepinephrine in 33 patientsin shock with acute myocardial infarction andall except one had control mean arterialpressure below 75 mm Hg.' Cardiac outputincreased an average of 18%, arterial pressureincreased 43%, and systemic vascular resistanceincreased 37%.We have reviewed our experience with the
use of norepinephrine in patients with variousforms of medical shock (table 1) and haveconfirmed the observations of Weil andShubin36 that increasing the arterial pressureabove levels just adequate to perfuse the vitalorgans (brain, heart, and kidney) merelyincreases the work of the heart at the expenseof a decrease in blood flow. Laks et al. havedemonstrated in the intact dog that at verysmall infusion rates norepinephrine increases
Circuclation, Volume XLV, May 1972
1116
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from
DRUGS IN CARDIOGENIC SHOCK IN MI
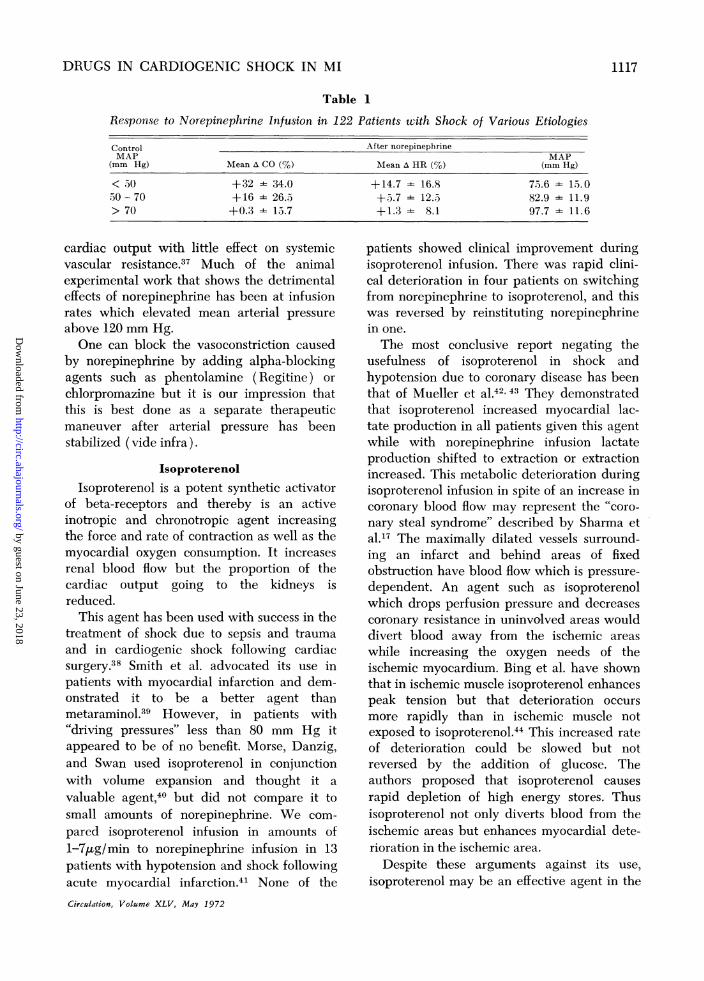
Table 1
Response to Norepinephrine Infusion in 122 Patients with Shock of Various Etiologies
Control After norepinephrineMAP MAP
(mm Hg) Mean A CO (%) Mean A HR (%) (mm Hg)
< 30 +32 - 34.0 +14.7 - 16.8 73.6 - 13.030 70 +16 - 26.3 +5.7 - 12.3 82.9 - 11.9> 70 +0.3 - 13.7 +1.3 - 8.1 97.7 - 11.6
cardiac output with little effect on systemicvascular resistance.37 Much of the animalexperimental work that shows the detrimentaleffects of norepinephrine has been at infusionrates which elevated mean arterial pressureabove 120 mm Hg.One can block the vasoconstriction caused
by norepinephrine by adding alpha-blockingagents such as phentolamine (Regitine) orchlorpromazine but it is our impression thatthis is best done as a separate therapeuticmaneuver after arterial pressure has beenstabilized (vide infra).
IsoproterenolIsoproterenol is a potent synthetic activator
of beta-receptors and thereby is an activeinotropic and chronotropic agent increasingthe force and rate of contraction as well as themyocardial oxygen consumption. It increasesrenal blood flow but the proportion of thecardiac output going to the kidneys isreduced.
This agent has been used with success in thetreatment of shock due to sepsis and traumaand in cardiogenic shock following cardiacsurgery.38 Smith et al. advocated its use inpatients with myocardial infaretion and dem-onstrated it to be a better agent thanmetaraminol.39 However, in patients with"driving pressures" less than 80 mm Hg itappeared to be of no benefit. Morse, Danzig,and Swan used isoproterenol in conjunctionwith volume expansion and thought it avaluable agent,40 but did not compare it tosmall amounts of norepinephrine. We com-pared isoproterenol infusion in amounts of1-7,gg/min to norepinephrine infusion in 13patients with hypotension and shock followingacute myocardial infarction.41 None of theCirculation, Volume XLV, May 1972
patients showed clinical improvement duringisoproterenol infusion. There was rapid clini-cal deterioration in four patients on switchingfrom norepinephrine to isoproterenol, and thiswas reversed by reinstituting norepinephrinein one.The most conclusive report negating the
usefulness of isoproterenol in shock andhypotension due to coronary disease has beenthat of Mueller et al.42 3 They demonstratedthat isoproterenol increased myocardial lac-tate production in all patients given this agentwhile with norepinephrine infusion lactateproduction shifted to extraction or extractionincreased. This metabolic deterioration duringisoproterenol infusion in spite of an increase incoronary blood flow may represent the "coro-nary steal syndrome" described by Sharma etal.17 The maximally dilated vessels surround-ing an infarct and behind areas of fixedobstruction have blood flow which is pressure-dependent. An agent such as isoproterenolwhich drops perfusion pressure and decreasescoronary resistance in uninvolved areas woulddivert blood away from the ischemic areaswhile increasing the oxygen needs of theischemic myocardium. Bing et al. have shownthat in ischemic muscle isoproterenol enhancespeak tension but that deterioration occursmore rapidly than in ischemic muscle notexposed to isoproterenol.44 This increased rateof deterioration could be slowed but notreversed by the addition of glucose. Theauthors proposed that isoproterenol causesrapid depletion of high energy stores. Thusisoproterenol not only diverts blood from theischemic areas but enhances myocardial dete-rioration in the ischemic area.
Despite these arguments against its use,isoproterenol may be an effective agent in the
1117
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

GUNNAR, LOEB
presence of the shock syndrome when intraar-terial pressure is normal. Under these circum-stances, isoproterenol should be given in smallamounts of 0.5-2.0 gg/min and discontinued ifarterial pressure falls or if arrhythmias appear.In patients with severe mitral insufficiencyand acute myocardial infarction any increasein systemic vascular resistance only enhancesthe regurgitant flow and, therefore, isoprotere-nol is the catecholamine to be used first.
Isoproterenol can also be used after atro-pine in the presence of bradycardia but inmost instances this will be a temporarymeasure while placing a pacing catheter.Idioventricular rhythms should not be broughtmuch above 60 beats/min with this drugbecause of the danger of inducing ventriculartachycardia or fibrillation.
DopamineDopamine is a precursor of norepinephrine
and activates both the beta- and alpha-adrenergic receptors.45 In addition this drughas vasodilator effects on the renal andmesenteric vessels not mediated throughadrenergic receptors.46 Dopamine, by increas-ing myocardial oxygen consumption, reducescoronary vascular resistance.4 A direct effectof dopamine on the coronary circulation hasnot as yet been demonstrated. Because itsaction on the adrenergic receptors is interme-diate between norepinephrine and isoprotere-nol and due to its renal vasodilator properties,dopamine has been considered a useful agentin the treatment of various shock states.48Dopamine has been shown to improve hemo-dynamic abnormalities caused by experimen-tal myocardial infarction as it tends to reversethe depression of myocardial function thatfollows coronary artery ligation.49 MacCannellet al. reported improvement in urine flow aswell as arterial pressure and cardiac outputduring dopamine infusion in patients withshock of several etiologies.50 Talley et al.reported seven patients who had a betterhemodynamic response to dopamine than toisoproterenol.51We have reported on the effects of dopa-
mine on 62 patients with shock.52 In 13patients, five of whom had acute myocardial
infarction, the shock was primarily cardio-genie. In patients with cardiogenic shockdopamine increases cardiac output andLVEDP and can increase mean arterialpressure if it is reduced. Systemic vascularresistance tends to fall as cardiac outputincreases in those who are initially vasocon-stricted. When compared to norepinephrineand isoproterenol, dopamine increases cardiacoutput more than norepinephrine and lessthan isoproterenol and increases arterial pres-sure more that isoproterenol and less thannorepinephrine. Urine flow appears to im-prove as often with norepinephrine as withdopamine. Comparison of the latter twoagents by therapeutic trial is often necessary ifimproved urine flow is the object of therapy.Dopamine can be infused at rates of 0.1-1.6
mg/min, and careful ECG monitoring isnecessary because ventricular arrhythmiasmay be precipitated.
DigitalisDigitalis has been used in treatment of
shock with myocardial infarction but fewstudies of the hemodynamic effects have beenpublished. Gorlin measured cardiac output intwo patients before and after rapid digitaliza-tion and found increases in both patients.53 Inan experimental model of cardiogenic shockCronin and Zsoter showed that digitalis causesan increase in blood pressure, a slight increasein cardiac output, and a very significantincrease in stroke volume with a fall inLVEDP.54 The increase in blood pressurepreceded the increase in cardiac output andthey suggested that the direct vasoconstrictoreffects of digitalis preceded the inotropicaction.We have reported the effects of acute
digitalization in a group of patients in shockwith myocardial infarction and the averagesof the changes in cardiac output, arterialpressure, CVP, and systemic vascular resis-tance tended to show no effect of the digitalison any of these parameters.' Some patientsimproved but others deteriorated or continuedto deteriorate following administration ofdigitalis. Morrison and Killip have stressed the
Circulation, Volume XLV, May 1972
1118
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

DRUGS IN CARDIOGENIC SHOCK IN MI
increased ventricular irritability induced bydigitalis in acute myocardial infarction,55 andtherefore it should be used judiciously andonly after elevating the arterial pressure andby ensuring an adequate filling pressure byfluid infusion, if necessary. It should be givenin amounts calculated to be one half to twothirds of the accepted "digitalizing" doses. Thebest effects will be in the patients in overtfailure, but almost all patients with acutemyocardial infarction given digitalis willdecrease LVEDP and increase LV stroke workand rate of pressure development.The question remains as to whether this
effect is of benefit to the heart. The increase instroke work and the increase in rate ofpressure development would be at the expenseof an increase in myocardial oxygen consump-tion.56 However, the decrease in LVEDP, if itrepresents a decrease in diastolic volume andnot just a change in myocardial compliance,should decrease myocardial oxygen needs.The law of LaPlace indicates that the pressurein the ventricle varies directly with the tensionin the wall and inversely with the radius of thecavity. Therefore, if left ventricular pressuredevelops from a smaller ventricular radius,myocardial tension, a major determinant ofmyocardial oxygen consumption, could de-crease even as pressure rises. It is probablethat the dilated heart benefits from adminis-tration of digitalis while the normal-sizedheart does not. The answer to whether theeffects in acute myocardial infarction arebeneficial awaits studies of changes in ventric-ular volume or measurements of myocardialoxygen consumption. There is some indicationfrom clinical observations that changes inventricular volume may determine the efficacyof digitalis in ischemic heart disease, sincepatients with angina and small hearts notinfrequently accelerate their angina withdigitalization while patients with big heartsmay be relieved of angina when givendigitalis.57 Digitalis should not be given in thepresence of heart block unless a pacemakercatheter is in place.
GlucagonGlucagon has been noted to have an
Circulation, Volume XLV, May 1972
inotropic effect in isolated muscle preparationsand in the intact animal.58 In man it has beenshown to be effective in increasing cardiacoutput, rate of pressure development, andheart rate.59 It was first used therapeutically asan inotropic agent by Linhart who reportedimprovement in a patient with depressedcardiac function after heart-valve replace-ment.60 With administration of glueagon tothis patient he noted that the blood pressurereturned to normal, heart rate increasedslightly, and further pharmacologic supportwas unnecessary. Parmley reported on theadministration of this agent to 16 patients inthe first postoperative day after prosthetic-valve replacement and found an increase inmean arterial pressure, heart rate, and cardiacindex.61 There was no change in systemicvascular resistance, although Glick had pre-viously shown glueagon to be a mild vasodila-tor.62 Vander Ark and Reynolds treated 16patients with cardiogenic shock for 1-12 dayswith continuous glueagon infusions.63 Theynoted improvement in 12 of the patients whoexperienced increased blood pressure, de-creased heart rate, and increased urine flow.Murtagh et al. gave glueagon to eight patientswith myocardial infaretion and noted anincrease in pulmonary and systemic vascularresistances.64 Diamond et al. treated 10patients with acute myocardial infarction, nineof whom had left ventricular failure.65 Theynoted an increase in heart rate, cardiac output,and arterial pressure. There was a consistentincrease in pulmonary vascular resistance, andthey attributed this to a direct effect ofglucagon on the pulmonary vasculature. Theyalso report the use of glucagon in treating twopatients with severe myocardial infarction andshock, and credited survival in one of thepatients to the use of glucagon. Studies inpatients with chronic congestive failure havebeen less conclusive than studies in patientswith acute failure.66 In studies of papillarymuscles from patients having mitral-valvereplacement Goldstein et al.68 found glucagonhad no inotropic effect on muscles frompatients who had prolonged cardiac failure,
1119
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

GUNNAR, LOEB
90 -
80 FE MMAP:
70
80j.
E £0
470
601
260 - L Dl
S~ ~ ~Fgr400
50'-
20E0
The effects of isoproterenol (ISP), phentolamine, andglucagon in a patient with chronic congestive heartfailure. Cardiac output (CO) increased more withisoproterenol thanz with glucagon hut urine flow (UF)was greater during glucagon infusion. Phentolamineinfusion had little effect on either CO or UF. Changesin mean arterial pressure (MAP), heart rate (HR),and left ventricular end-diastolic pressu4re (LVEDP)are also show)n.
although these same muscles responded posi-tively to norepinephrine. Papillary musclefrom patients with mitral stenosis and no leftventricular failure showed an inotropic re-sponse to both glucagon and norepinephrine.This discrepancy is probably due to uncou-pling or disruption of the glucagon receptormechanism in chronic congestive heart fail-ure.67Glucagon acts by activating adenyl cyclase
which converts adenosine triphosphate tocyclic AMP (adenosine 5'-monophosphate )and this in turn activates the contractilemechanism.67 Catecholamines also activate
adenyl cyclase but through a different recep-tor mechanism. Aminophylline will potentiatethe effects of glucagon by blocking phospho-diesterase which deactivates cyclic AMP.69Glucagon, therefore, has the advantage ofacting through a nonadrenergic receptormechanism and can be effective in the patientwvho has received beta-receptor blockingagents. It does not cause arrhythmias and canbe used in the patient with digitalis excess. Ithas also been shown to reverse the prolonga-tion of action potential produced by quini-dine.70
Administration is either by single injectionof 4-5 mg intravenously or by constantintravenous infusion at the rate of 4-12mg/hour. The single injection shows onset ofaction almost immediately, peak action at 10min, and action is dissipated within 30 min.71Hyperglycemia is a constant finding, but isusually only to levels of 140 mg% and seldomexceeds 200 mg%. Hypoglycemia may occur,particularly on discontinuance after prolongedinfusion. Hypokalemia occurs consistently andshould be prevented by K-' supplementationduring glucagon infusion. Glucagon infusionshould be augmented by simultaneous amino-phylline infusion. Nausea and vomiting areuncomfortable side effects and the resultantvagal stimulation may decrease cardiac out-put. By limiting the infusion rate or keepingthe single injection below 5 mg this side effectusually can be avoided.Glucagon has a direct effect on the renal
tubules leading to diuresis and natriuresis.72 Inchronic intractible cardiac failure we havenoted marked diuresis far in excess of thehemodynamic effect and suggest that thedirect renal effects deserve further study (fig.4).
Chlorpromazine and PhentolamineChlorpromazine73 and phentolamine have
been used as vasodilators in myocardialinfarction. They can be used in conjunctionwith norepinephrine to decrease the vasocon-strictor activity of the latter agent and thusallow more inotropic activity. Both agents alsocause a decrease in venous tone and should be
Circulation, Volume XLV, May 1972
1120
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

DRUGS IN CARDIOGENIC SHOCK IN MI
accompanied by volume administration unlessthe vasodilator is being used in managementof pulmonary edema. Chlorpromazine is givenin amounts of 5-10 mg intravenously in a singleinjection and may be repeated only once at20-30 min. Larger amounts of this agent willincrease drowsiness and may enhance arrhyth-mias. Phentolamine is given as a constantintravenous infusion at a rate of 2-4 mg/hour.Phenoxybenzamine, although a very potentalpha-adrenergic blocking agent, is not avail-able for general use and its action is soprolonged that we would not think it shouldbe used in acute myocardial infarction.
References1. GUNNER RM, LOEB HS, PIETRAS RJ, TOBIN JR
JR: The hemodynamic effects of myocardialinfarction and results of therapy. Med Clin NAmer 54: 235, 1970
2. GUNNAR RM, PIETRAS RJ, STAVRAKOS C, LOEBHS, TOBIN JR JR: The physiologic basis fortreatment of shock associated with myocardialinfarction. Med Clin N Amer 51: 69, 1967
3. GILBERT RP, ALDRICH SL, ANDERSON L: Cardiacoutput in acute myocardial infarction. J ClinInvest 30: 640, 1951
4. WIGGERS CJ: The functional consequences ofcoronary occlusion. Ann Intern Med 23: 158,1945
5. LOEB H, SINNO MZ, CHUQUIMIA R, ROSEN K,RAHIMTOOLA SH, GUNNAR R: Correlates ofleft ventricular contractility in patients withuncomplicated acute myocardial infarction.Clin Res 19: 325, 1971
6. KUHN L: The treatment of cardiogenic shock.Amer Heart J 74: 578, 1967
7. AGRESS CM, ROSENBERG MJ, JACOBS HI, BINDER
MJ, SCHNEIDERMAN A, CLARK WG: Protractedshock in the closed chest dog followingcoronary embolization with graded micro-
spheres. Amer J Physiol 170: 536, 19528. CONSTANTIN L: Extra cardiac factors contribut-
ing to hypotension during coronary occlusion.Amer J Cardiol 11: 205, 1963
9. SLEIGHT P, WIDDICOMBE JG: Action potentialsin fibers from receptors in the epicardium andmyocardium of the dog's left ventricle. JPhysiol 181: 235, 1966
Circulation, Volume XLV, May 1972
10. KEZDI P, MISRA SN, KORDENAT RK, SPICKLERJW, STANLEY EL: The role of vagal afferentsin acute myocardial infarction. Amer J Cardiol26: 642, 1970
11. BROwN AM: Excitation of afferent cardiacsympathetic nerve fibers during myocardialischemia. J Physiol (London) 190: 35, 1967
12. HUGHES JL, AMSTERDAM EA, MASON DT,MANSOUR E, ZELIS R: Abnormal peripheralvascular dynamics in patients with acutemyocardial infarction: Diminished reflex arte-riolar constriction. Clin Res 19: 321, 1971
13. GUNNAR RM, LOE.B HS, PIETRAS RJ, TOBIN JRJR: Hemodynamic measurements in a coronarycare unit. Progr Cardiovase Dis 11: 29, 1968
14. COHN JN, LUIuA MH: Studies in clinical shockand hypotension: IV. Variations in reflexvasoconstriction and cardiac stimulation. Circu-lation 34: 823, 1966
15. GUNNAR RM, CRUZ A, BOSWELL J, Co BS,PIETRAs RJ, TOBIN JR JR: Myocardialinfarction with shock: Hemodynamic studiesand results of therapy. Circulation 33: 753,1966
16. BLUMGART HL, SCHLESINGER MJ, DAVIS D:Studies in the relationship of the clinicalmanifestations of angina pectoris, coronarythrombosis and myocardial infarction to patho-logic findings. Amer Heart J 19: 1, 1940
17. SHARMA GV, KUMAR RK, MOLOKHIA F, MESSER
JV: Coronary steal: Regional myocardial bloodflow studies during isoproterenol infusion in
acute and healing myocardial infarction. ClinRes 19: 339, 1971
18. BERNE RM: Regulation of coronary blood flow.Physiol Rev 44: 1, 1964
19. LOEB HS, PIErntS RJ, TOBIN JR JR, GUNNAR
RM: Hypovolemia in shock due to acutemyocardial infarction. Circulation 40: 653,1969
20. LANGSJOEN PH, FALCONER HS, SANCHEZ SA,LYNCH DJ: Observations in treatment of acutemyocardial infarction with low molecularweight dextran. Angiology 14: 465, 1963
21. NIXON PGF, IKROM H, MORTON S: Cardiogenicshock treated with infusion of dextrosesolution. Amer Heart J 73: 843, 1967
22. ALLEN HM, DANZIG R, SWAN HJC: Incidence andsignificance of relative hypovolemia as a cause
1121
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from
GUNNAR, LOEB
of shock associated with acute myocardialinfarction. Circulation 36 (suppl II): II-50,1967
23. FREIs ED, SCHNAPER HW, JOHNSON RL,SCHREINER GE: Hemodynamic alterations inacute myocardial infarction: I. Cardiac output,mean arterial pressure, total peripheral resis-tance, "central" and total blood volumes,venous pressure and average circulation time. JClin Invest 31: 131, 1952
24. WEIL MH, SHUBIN H, ROSOFF L: Fluidrepletion in circulatory shock: Central venouspressure and other practical guides. JAMA192: 668, 1965
25. SCHEINMAN MM, ABBOTT JA, RAPAPORT E:Clinical use of a flow-directed right heartcatheter. Arch Intem Med (Chicago) 124: 19,1969
26. SWAN HJC, GANZ W, FORRESTER J, MARCUS H,DIAMOND G, CHONETTE D: Catheterizationof the heart in man with use of a flow-directedballoon-tipped catheter. New Eng J Med283: 447, 1970
27. COHN JN, KHATRI IM, HAMOSH P: Diagnosticand therapeutic value of bedside monitoring ofleft ventricular pressure. Amer J Cardiol 23:107, 1969
28. LEINBACH RC, MUNDTH ED, DINSMORE RE,HARiTHORNE JW, BUCKLEY MJ, KANTROWITZ A,AUSTEN GW, SANDERS CA: Selective coronaryand left ventricular cineangiography duringintra-aortic balloon assist for cardiogenic shock.Amer J Cardiol 26: 644, 1970
29. COHN JN, LURIA MH, DADDARIO RC, TRISTANIFE: Studies in clinical shock and hypotension:V. Hemodynamic effects of dextran. Circula-tion 35: 316, 1967
30. SWAN HJC, FORRESTER JS, DANZIG R, ALLENHN: Power failure in acute myocardialinfarction. Progr Cardiovasc Dis 12: 568,1970
31. BINDER MJ, RYAN JA JR, MARCUS S, MUGLER FJR, STRANGE D, AGREss CM: Evaluation oftherapy in shock following acute myocardialinfarction. Amer J Med 18: 622, 1955
32. HADDY FJ: Pathophysiology and therapy of theshock of myocardial infarction. Ann Intern Med73: 809, 1970
33. MALMCRONA R, SCHIIODER G, WERKO L: Hemo-
dynamic effects of metaraminol: II. Patientswith acute myocardial infarction. Amer JCardiol 13: 15, 1954
34. SMULYAN H, CUDDY RP, EICH RH: Hemody-namic effects of pressor agents in septic andmyocardial infarction shock. JAMA 190: 188,1964
35. SHUBIN H, WEIL MH: Hemodynamic alterationsin patients after acute myocardial infarction. InShock and Hypotension, edited by Mills,Moyer. New York, Grune & Stratton, 1965, p499
36. SHUBIN H, WEIL MH: The hemodynamic effectsof vasopressor agents in shock due tomyocardial infarction. Amer J Cardiol 15: 147,1965
37. LAKS M, CALLIS G, SWAN HJC: Hemodynamiceffects of low doses of norepinephrine in theconscious dog. Amer J Physiol 220: 171,1971
38. CAREY JS, BROWN RS, MoHR PA, MONSON DO,YAO ST, SHOEMAKER WC: Cardiovascularfunction in shock: Responses to volumeloading and isoproterenol infusion. Circulation35: 327, 1967
39. SMITH HJ, ORIOL A, MORCH J, MCGREGOR M:Hemodynamic studies in cardiogenic shock:Treatment with isoproterenol and metaraminol.Circulation 35: 1084, 1967
40. MORSE BW, DANZIG R, SWAN HJC: Effect ofisoproterenol in shock associated with acutemyocardial infarction. Circulation 36 (supplII): II-172, 1967
41. GUNNAR RM, LOEB HS, PIETRAS RJ, TOBIN JRJR: Ineffectiveness of isoproterenol in thetreatment of shock due to acute myocardialinfarction. JAMA 202: 1124, 1967
42. MUELLER H, AYRES SM, GREGORY JJ, GIANNELLIS JR , GRACE WJ: Hemodynamics, coronaryblood flow and myocardial metabolism incoronary shock: Response to l-norepinephrineand isoproterenol. J Clin Invest 49: 1885,1970
43. MUELLER H, AYRES SM, MAZZARA JT, GIANNELLIS, CONKLIN EF, GRACE WJ, NEALON T: Coro-nary flow-pressure relation and its role formyocardial metabolism in human coronaryshock. Amer J Cardiol 26: 651, 1970
Circulation, Volume XLV, May 1972
1122
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from
DRUGS IN CARDIOGENIC SHOCK IN MI
44. BING OHL, BRooKs WW, MESSER JV: Mechani-cal benefits and hazards of isoproterenol duringmyocardial hypoxemia. Clin Res 19: 305,1971
45. MCNAY JL, GOLDBERG LI: Hemodynamic effectsof dopamine in the dog before and after alphaadrenergic blockade. Circ Res 18 (suppl I): I-
110, 196646. McNAY JL, McDONALD RH JR, GOLDBERG LI:
Direct renal vasodilation produced by dopa-mine in the dog. Circ Res 16: 510, 1965
47. BROOKS HL, STEIN PD, MATSON JL, HYLAND
JW: Dopamine induced alterations in coronary
hemodynamics in dogs. Circ Res 24: 699,1969
48. MCDONALD RH JR, GOLDBERG LI, McNAY JL,TUTTLE EP JR: Effects of dopamine in man:
Augmentation of sodium excretion, glomerularfiltration rate and renal plasma flow. J ClinInvest 43: 1116, 1964
49. NEVATT GW, NELSON JM, GOLEY DE, BOWYER
AF: Dopamine reversal of the abrupt hemody-namic abnormalities of myocardial infarction.Clin Res 18: 117, 1970
50. MACCANNELL KL, MCNAY JL, MEYER MB,GoLDBERG LI: Dopamine in the treatment ofhypotension and shock. New Eng J Med 275:1389, 1966
51. TALLEY RC, GOLDBERG LI, JOHNSON CE, MCNAYJL: A hemodynamic comparison of dopamineand isoproterenol in patients in shock. Circula-tion 39: 361, 1969
52. LOEB HS, WINSLOW EBJ, RAHIMTOOLA SH,ROSEN KM, GUNNAR RM: Acute hemodynamiceffects of dopamine in patients with shock.Circulation 44: 163, 1971
53. GORLIN R: Modern treatment of coronary
occlusion and insufficiency. Med Clin N Amer46: 1243, 1962
54. CRONIN RFP, ZSOTER T: Hemodynamic effects ofrapid digitalization in experimental cardiogenicshock. Amer Heart J 69: 233, 1965
55. MORRISON J, KILLIP T: Serial serum digitalislevels in patients with acute myocardialinfarction. Clin Res 19: 353, 1971
56. BRAUNWALD E: Control of myocardial oxygen
consumption. Amer J Cardiol 27: 416, 1971
57. SONNENBLICK EH, SKELTON CL: Oxygen con-
sumption of the heart: Physiological principles
Circulation, Volume XLV, May 1972
and clinical implications. Mod Conc Cardio-vasc Dis 40: 9, 1971
58. FARAH A, TUTTLE R: Studies on pharmacology ofglucagon. J Pharmacol Exp Ther 129: 49,1960
59. PARMLEY WW, GLICK G, SONNENBLICK EH:Cardiovascular effects of glucagon in man.
New Eng J Med 279: 12, 1968
60. LINHART JW, BAROLD SS, COHEN LS, HILDNERFJ, SAMET P: Cardiovascular effects ofglucagon. Amer J Cardiol 22: 706, 1968
61. PARMLEY WVW, MATLOFF JM, SONNENBLICK EH:Hemodynamic effects of glucagon in patientsfollowing prosthetic valve replacement. Circu-lation 39 (suppl I): 1-163, 1969
62. GLICK G, PARMLEY WW, WECHSLER AS,SONNENBLICK EH: Glucagon: Its enhancementof cardiac performance in the cat and dog andpersistence of its inotropic action despite beta-
receptor blockade with propranolol. Circ Res22: 789, 1968
63. VANDER ARK CR, REYNOLDS EW JR: Clinical
evaluation of glucagon by continuous infusionin the treatment of low cardiac output states.
Amer Heart J 79: 481, 1970
64. MURTAGH JG, BINNION PF, LAL S, HUTCHISON
KJ, FLETCHER E: Hemodynamic effects ofglucagon. Brit Heart J 32: 307, 1970
65. DIAMOND G, FORRESTER J, DANZIG R, PARMLEY
WW, SWAN HJC: Hemodynamic effects of
glucagon during acute myocardial infarctionwith left ventricular failure in man. Brit HeartJ 33: 290, 1971
66. NORD HJ, FONTANES AL, WILLIAMS JF JR:
Treatment of congestive heart failure with
glucagon. Ann Intern Med 72: 649, 1970
67. EPSTEIN SE, LEVEY GS, SKELTON CL: Adenylcyclase and cyclic AMP: Biochemical links in
the regulation of myocardial contractility.Circulation 43: 437, 1971
68. GOLDSTEIN RE, SKELTON CL, LEVEY GS, GLAN-CEY DL, BEISER GD, EPSTEIN SE: Effects of
glucagon on contractility and adenyl cyclaseactivity of human papillary muscle. Circulation42 (suppl III): III-158, 1970
69. MARCUS ML, SKELTON CL, PRINDLE KH JR,EPSTEIN SE: Influence of theophylline on the
inotropic effects of glucagon. Circulation 42
(suppl III): III-181, 1970
1123
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

GUNNAR, LOEB
70. STEWART JW, MYERBURG RJ, HOFFMAN BF: Theeffect of glucagon on quinidine-inducedchanges in Purkinje fibers. Circulation 40(suppl III): III-196, 1969
71. PARMLEY WW, SONNENBLICK EH: Glucagon: Anew agent in cardiac therapy. Amer J Cardiol27: 298, 1971
72. PULLMAN TN, LAVENDER AR, AHO I: Direct
effects of glucagon on renal hemodynamics andexcretion of inorganic ions. Metabolism 16:
358, 1967
73. LoE HS, PIETRAS RJ, NINOs N, TOBIN JR JRGUNNAR RM: Hemodynamic responses tochlorpromazine in patients in shock. ArchIntern Med (Chicago) 24: 354, 1969
Circulation, Volume XLV, May 1972
1124
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from
ROLF M. GUNNAR and HENRY S. LOEBUse of Drugs in Cardiogenic Shock due to Acute Myocardial Infarction
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1972 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation
doi: 10.1161/01.CIR.45.5.11111972;45:1111-1124Circulation.
http://circ.ahajournals.org/content/45/5/1111located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer
of the Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle columnClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from