user involvement in the act now study maximising recruitment to a randomised controlled trial gill...
TRANSCRIPT

User involvement in the ACT NoW Study
Maximising recruitment to a
Randomised Controlled Trial Gill Pearl Liz Royle
Alys Young, Audrey Bowen

Reasons for the ACT NoW study
• Stroke affects communication:Aphasia, Dysarthria
• Speech & Language Therapy services: poorly resourced, variable and vulnerable service
• NHS needs robust research evidence to improve services – ‘proof’
• NHS commissioned ACT NoW study using Health Technology Assessment ‘HTA’ funding
• Randomised controlled trial• Enhanced therapy vs attention control
• Early – available on admission to hospital• ‘Intensive’ – sufficient ‘dose’ to affect outcome• Continuous – no gap from hospital to home• Pragmatic – delivered by NHS therapists• Multiple strategies – many types of therapy• Replicable – can be done by others in the future
What is different about the speech and language therapy in this
study?
How is it measured?Three research methods:• Compare the communication
• Qualitative study of selected people from each half of the trial. Ask people about the therapy
• Health economics – the cost, preferences and values for the outcomes
Challenges• Can be difficult to recruit people, this
is a threat to validity
• HTA Wanted to do a pilot study to see if the main study would work
• The management group wanted involvement from ‘users’ to make it work better. Users = people who have aphasia, dysarthria or are carers
Learning from others -key problems• Language – unfamiliar words, jargon,
misunderstanding • Difficult to grasp research concepts• Presentation of information- style,
format• Engaging users- process,
communication• Mismatch of purpose – what is needed
by ethics is not necessarily what someone wants to make a decision

Also …..• Problems of understanding are
complicated by aphasia –difficulties with understanding and using verbal language and print.
• Physical and emotional problems also may make the process of recruitment difficult
• The communication problems are highly variable and unpredictable
What did we do?
• Built the problem into the pilot study phase
• Put the solution firmly within the experience of those who had aphasia and/or dysarthria following stroke
• Made a long term commitment to work with a user group through the life of the research project

The RUG-Research User group
• 10 people were in the group• We were asked to join the study from
knowing Gill, through aphasia organisations and through speech and language therapy departments
• We met once a month at a community hall for 3 hours

photograph

How we joined in?
• Lots of staff to help– Alys -a researcher, – Gill - speech and language
therapist/researcher,– One other person from the research team
• Each meeting was very carefully planned with changes to the written information, pace, how things were explained, support for people

• In asking the group to do this work we had to work with the very difficulties that the task was seeking to overcome
• supporting the group to understand their jobs meant engaging with the problems of understanding, of using print and pictures
• The process became the objective and the objective became the process
The basics
• A belief that the users are competent, knowledgeable, experts who are equal partners in the process
• Attention to the environment, timing and pacing of meetings
• Support and changes to communication to allow access to the conversations for both understanding and expressing views
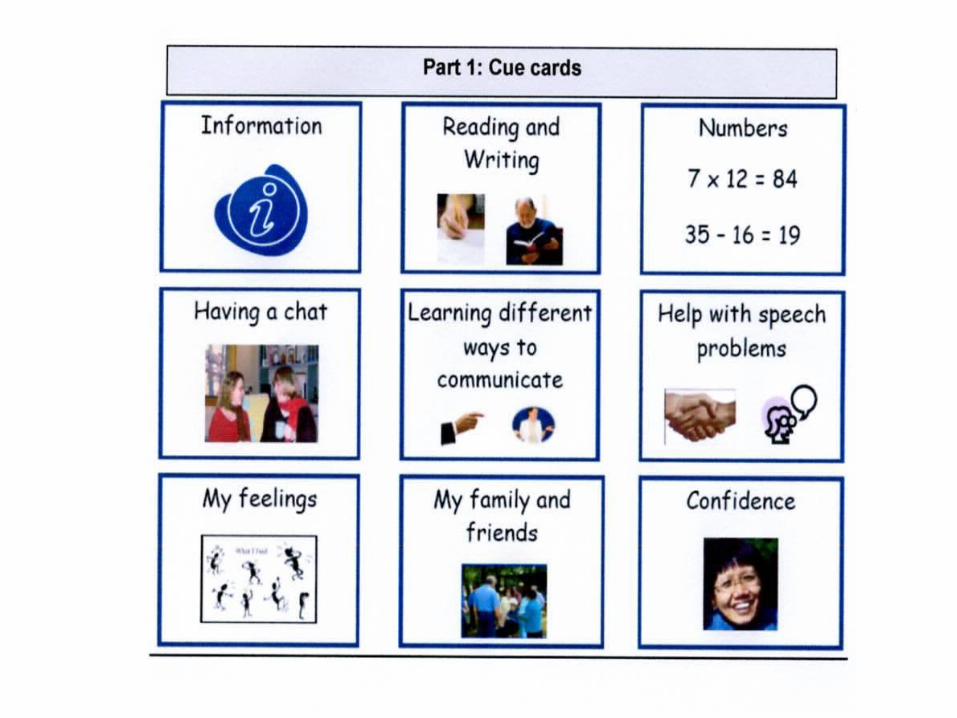
Communication support• Range of materials to allow engagement
and communication using a variety of ways – speech, writing, drawing, pictures, gestures, facial expressions
• Group rules• Meeting cards• Flexible and inventive• Power point
– Throughout the meetings to help check back as the discussion is happening
– Use it for drawings and diagrams– Print it out to go into members folders for
future reference

Diagrams and pictures
• Pre-prepared diagrams don’t work • Pictures built from within the group
do work
• An example of what not to do
? ? ?? ? ?? ? ?? ? ?
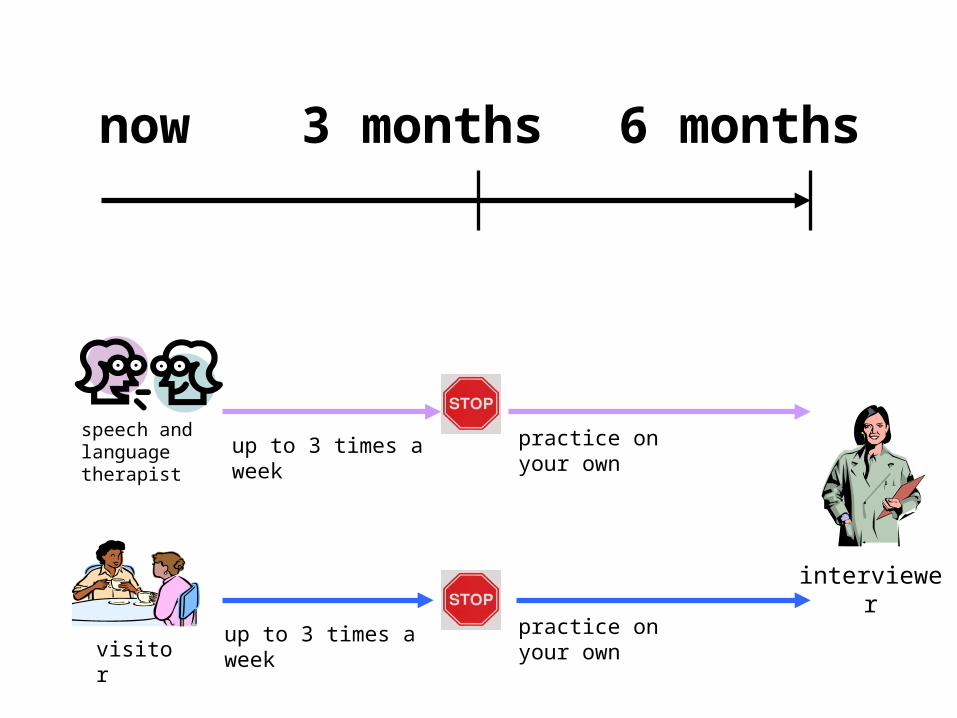
now 3 months 6 months
interviewer
practice on your own
practice on your own
up to 3 times a week
up to 3 times a week
speech and language therapist
visitor

Why do diagrams built from within the group work?
• Interactive- contributory knowledge from all people in the group
• Can ‘see’ understanding being modified• OK to say that don’t understand a diagram
when may not be OK to say don’t understand
• Pictures are different, real photos, diagrams, cartoons, icons
• Some require shared cultural understanding to be meaningful
• Open discussion helped to get the right diagrams
The user group helped the study with 3 jobs
1.Developed information and consent materials
2.Developed ‘interviews’3.Interviewed staff
1. Developing information and consent materials
• The group was asked to think about different ways to give information
• The information was for people who had just had a stroke, and their carers
• The research assistants used the information to ask patients to take part in the study (to recruit)
We needed to consider…
• The information itself, how much, what was important
• The words• How it looked• All people who have aphasia are different • Different ways of presenting the information• It needed to be ‘aphasia accessible’ • Group very strong on
– Cant assume how a patient may prefer to communicate– Give choice of ways to present materials– Must make sure that information builds on patients
strengths and not just addresses weaknesses
in this study you would see
•a speech and language therapist
•an ACT NoW visitor
or
visitor
speech and language therapist
this is decided by chance

will I see a speech and language therapist or a
visitor?• we do not know for sure which will be better for you
• we will not decide who you will see, it will be decided by chance
• a computer will pick names
• half the people will see a speech and language therapist
• half the people will see an ACT NoW visitor
therapist visitor
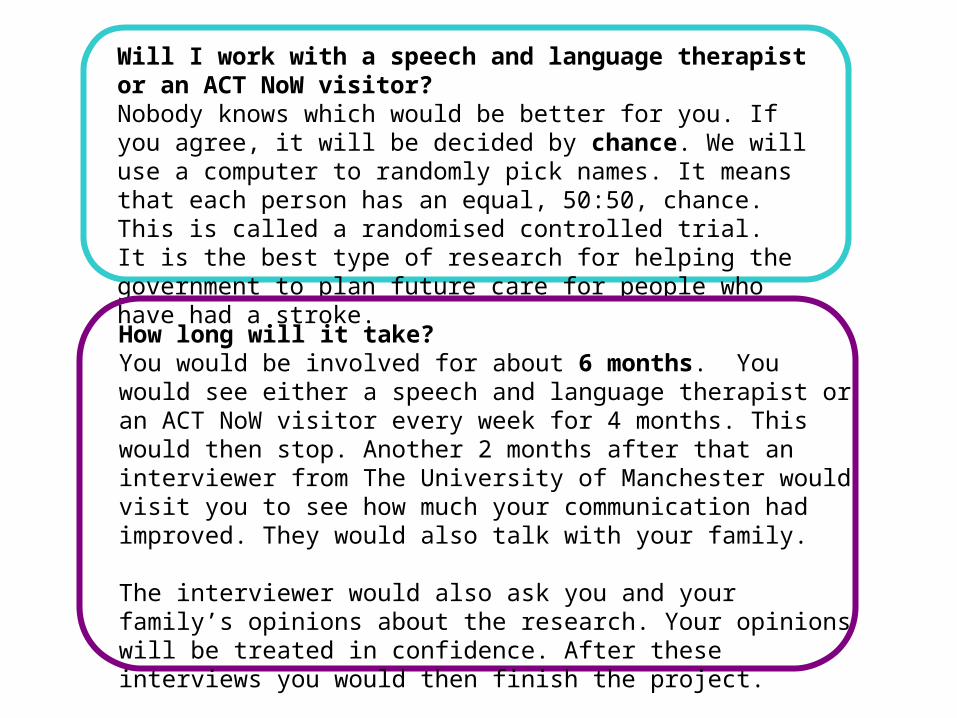
Will I work with a speech and language therapist or an ACT NoW visitor?Nobody knows which would be better for you. If you agree, it will be decided by chance. We will use a computer to randomly pick names. It means that each person has an equal, 50:50, chance. This is called a randomised controlled trial. It is the best type of research for helping the government to plan future care for people who have had a stroke.
How long will it take?You would be involved for about 6 months. You would see either a speech and language therapist or an ACT NoW visitor every week for 4 months. This would then stop. Another 2 months after that an interviewer from The University of Manchester would visit you to see how much your communication had improved. They would also talk with your family.
The interviewer would also ask you and your family’s opinions about the research. Your opinions will be treated in confidence. After these interviews you would then finish the project.

2. Developing qualitative ‘interviews’
• The study also included qualitative interviews with people who have aphasia or dysarthria
• The group was asked to think about the sort of questions the research assistant might ask– What are the questions– How should they be asked– What support materials might help
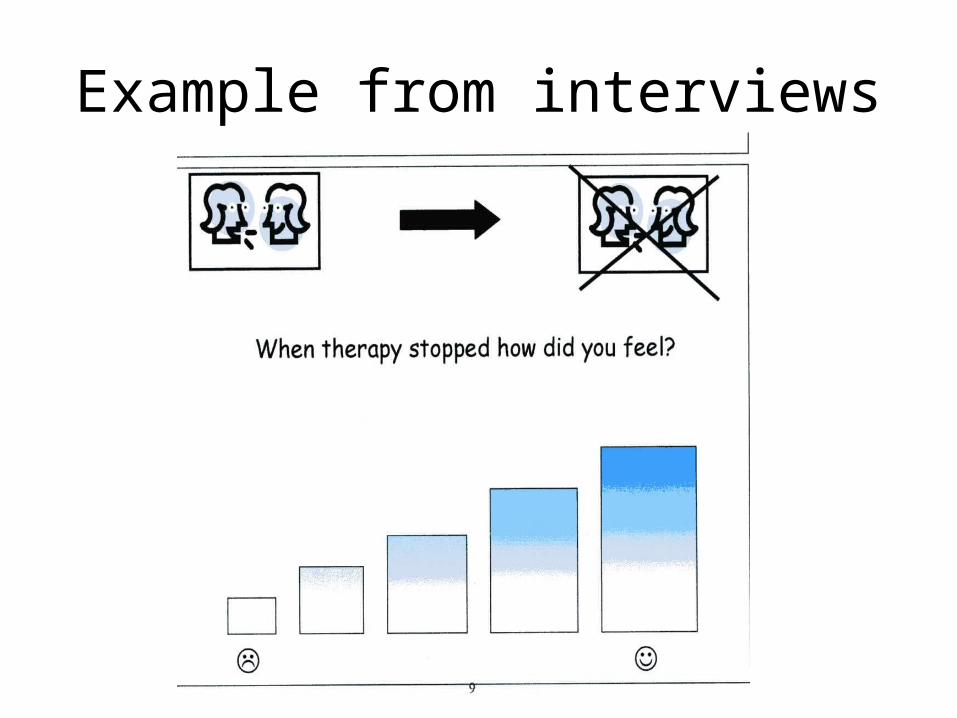
Example from interviews

3. Interviewing research assistants
• I was invited to join the University interview panel with Sean Crosby.
• We spent 2 days interviewing 10 candidates and chose 3
• We asked questions• We also answered questions • We commented on their
communication skills

What makes the RUG work – Gill and Alys’ view
• Planning• Preparation• Attention to detail
• Not a tick box approach but a collaborative process

What makes the group work? Liz’ view
• Alys and Gill facilitated the meetings. They prepared things in advance like an activity for role-playing the qualitative interviews. .
• Members brought ideas to the group and were given time to explain them
• Everyone had ideas because we are all from different backgrounds and brought different skills to the group. I owned my own business.
• We “brain stormed” our ideas• We took ideas from each other and expanded
on them• Alys and Gill coaxed ideas out of us without
putting words in our mouth.• They did not lose our ideas. They took notes on
the laptop. We received the notes before the next meeting
• We followed the discussions using a lap top and projector
• There were materials to help communication

User involvement: benefits to the study
•Accessible ‘information’ materials
•Ethics approval and praise “…Videos/Tapes helpful… would look to recommend their use in other studies ”
•Recruiting and training research staff
•71% consented to pilot
•Insider perspective on Qualitative interviews
•Sharing the information of ACT NoW

Benefits -What did I get out of it?• I made new friends with my group and the
researchers • I got involved with the research and it interested
me• It stretched my imagination• It was as though I had a job to do. It gave me a
sense of purpose.• It felt good to be doing something useful. I want to
help.• Confidence• I had fun doing the role-play video• I learnt to be patient with the other users• I value speech therapy and think its an important
study
User involvement: costs to ACT
NoW •Meetings: room hire, subsistence, travel
•Fee: an honorarium per user
•User representation services – Gill Pearl
•Meeting facilitation – 3 staff and preparation
•Approximately £12,000 for pilot study
•In main study + 0.3FTE Research Assistant
•Dissemination – 7 preparatory meetings (fee, travel, staff time, subsistence)
The future
• Continue to meet, but less frequently• Help with any problems, a resource
for other aspects of the study• Recruitment and training for new
staff • Ambassadors for the study• Share information about what we
have learned

For further information contactGill Pearl [email protected]
This project is funded by the Health Technology Assessment Programme
02/11/04
The views and opinions expressed therein are those of the authors and do
not necessarily reflect those of the Department of Health