using human factors to achieve high reliability in
TRANSCRIPT

Insert name of presentation on Master Slide
30.4.14
Using Human Factors to Achieve High
Reliability in Healthcare Organisations
Chris Hancock

Cycle for Sepsis
• Sennedd to Houses of Parliament
• 178 miles
• 3 days

Human Factors – just a sexy ‘on trend’ subject Or A tool to enable the right thing to be done, every time?


Human Error Reduction
• ‘the paradox at the heart of the patient safety problem.... is that Medical education, almost uniquely, is predicated on an assumption of trained perfectibility’
– Dr James Reason

Education is necessary but not sufficient
• Human Factors encompasses all those factors that can influence people and their behaviour. In a work context, human factors are the environmental, organisational and job factors, and individual characteristics which influence behaviour at work.
• Based on UK Health & Safety Executive: Reducing error and influencing behaviour, HSG48, HMSO (2005)

Insert name of presentation on Master Slide


Insert name of presentation on Master Slide

Insert name of presentation on Master Slide
Insert name of presentation on Master Slide

Insert name of presentation on Master Slide

Insert name of presentation on Master Slide

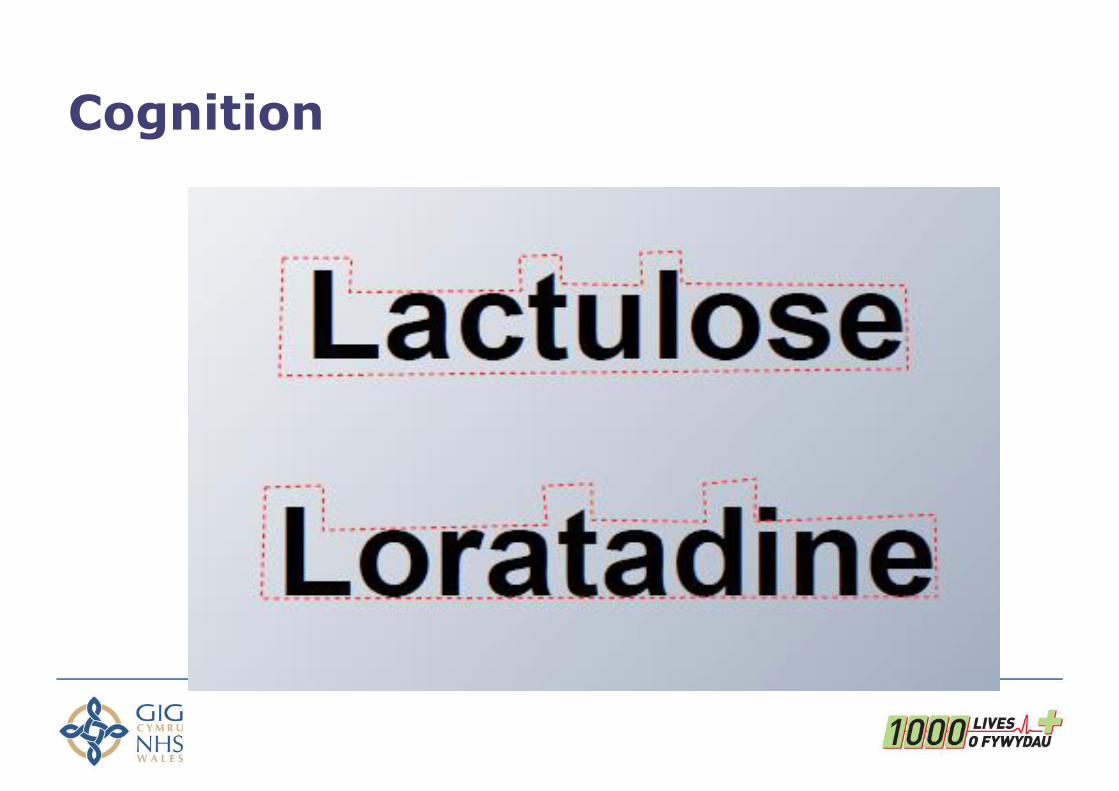
Cognition
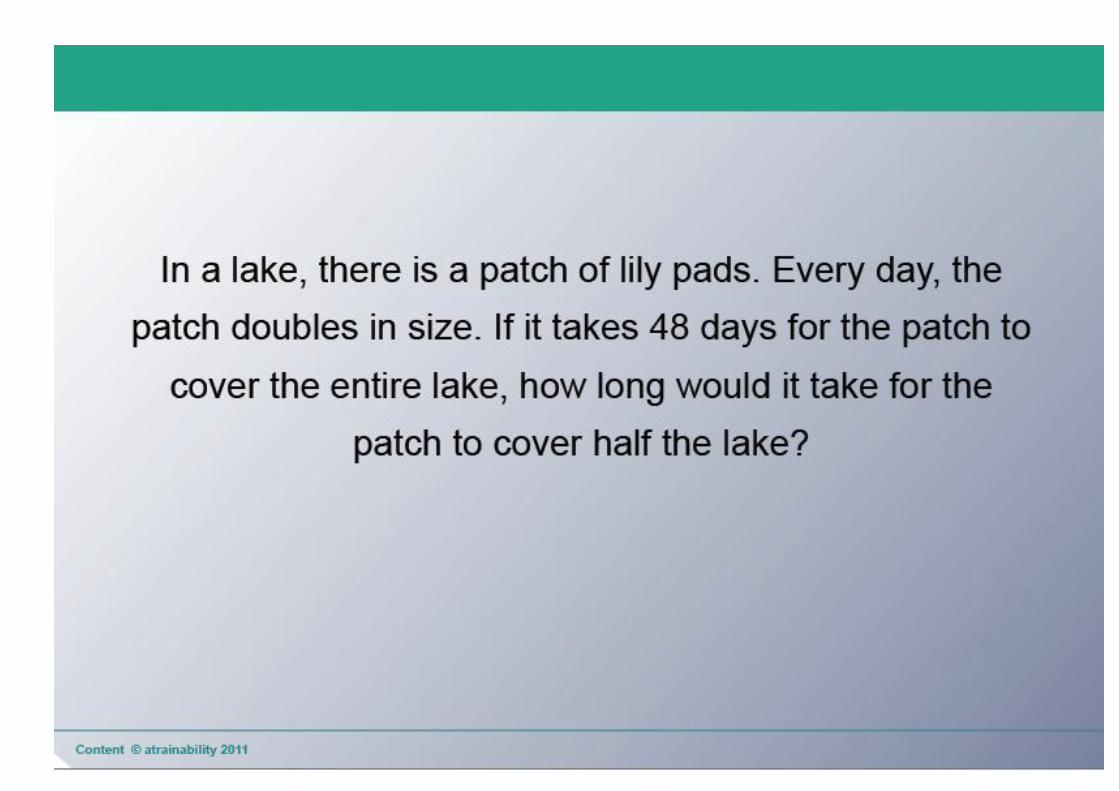
• Human error is an inevitable consequence of being human

Pattern recognition
• Aoccdrnig to a rscheearch at Cmabrigde Uinervtisy, it deosn‘t mttaer in waht oredr the ltteers in a wrod are, the olny iprmoatnt tihng is taht the frist and lsat ltteer be at the rghit pclae. The rset can be a toatl mses and you can sitll raed it wouthit porbelm. Tihs is bcuseae the huamn mnid deos not raed ervey lteter by istlef, but the wrod as a wlohe.
Cognition

Situations associated with an increased risk of error
• unfamiliarity with the task*
• inexperience*
• shortage of time
• inadequate checking
• poor procedures
• poor human equipment interface Vincent
* Especially if combined with lack of supervision

Individual factors that predispose to error
• limited memory capacity
• further reduced by: ○ fatigue
○ stress
○ hunger
○ illness
○ language or cultural factors
○ hazardous attitudes


Ergonomics and process reliability
• Put a good person in a bad system and the bad system wins, no contest
– W. Edwards Deming

The Gap Between Perception and
Practice What We Think We
Do
Vs.
What We Actually Do
Mitchell Levy,
Director, Surviving Sepsis Campaign

• Overall the reported reliability in the clinical systems studied was between 81% and 87%.
• In everyday life this would mean your car not starting 1 day every week or your luggage being lost once in every four overseas trips you take.
• Would you still use email if you knew that one email in seven would not reach its intended recipient?
– Burnett et al. 2012.

Time to Intervene - Key findings • Assessment on admission was considered deficient in
47% of the cases under review.
• 38% of in-hospital cases of cardiac arrests (and subsequent resuscitation attempt) could have been avoided if patient care had been properly managed.
• 75% of cases displayed clear warning signs that the patient was deteriorating. Of these patients the signs were not recognised in 35%, not acted on in 56% and not communicated to senior doctors in 55% of cases.

Exercise 2
• Using your own or the example provided identify how human and system error have contributed to patient harm.

Errors In Aviation
% of
Accidents
Time (The History of Powered Flight)
2011 Human Failure
Aircraft Failure

NoTechs – non technical skills
• Communication
• Situational Awareness
• Management
• Leadership
• Problem solving
• Decision making

Tools for Comms and Situational Awareness

Achieving higher reliability Apply human factors thinking to your work environment (WHO, 2010)
1. Avoid reliance on memory
2. Make things visible
3. Review and simplify processes
4. Standardize common processes and procedures
5. Routinely use checklists
6. Decrease the reliance on vigilance

1. Avoid reliance on memory
5.3
Rehearse, train and prepare for ‘worst case’ scenarios (eg. Simulation)
• Train as teams
• Train as close to the work place as possible

Before After
2. Make things visible

Communication – make it visible
• In your house, where do you put information you want the family to know?

RRAILS
The Fridge Door – the PSAG Board
Why do we hide important
information at the foot of the
bed?

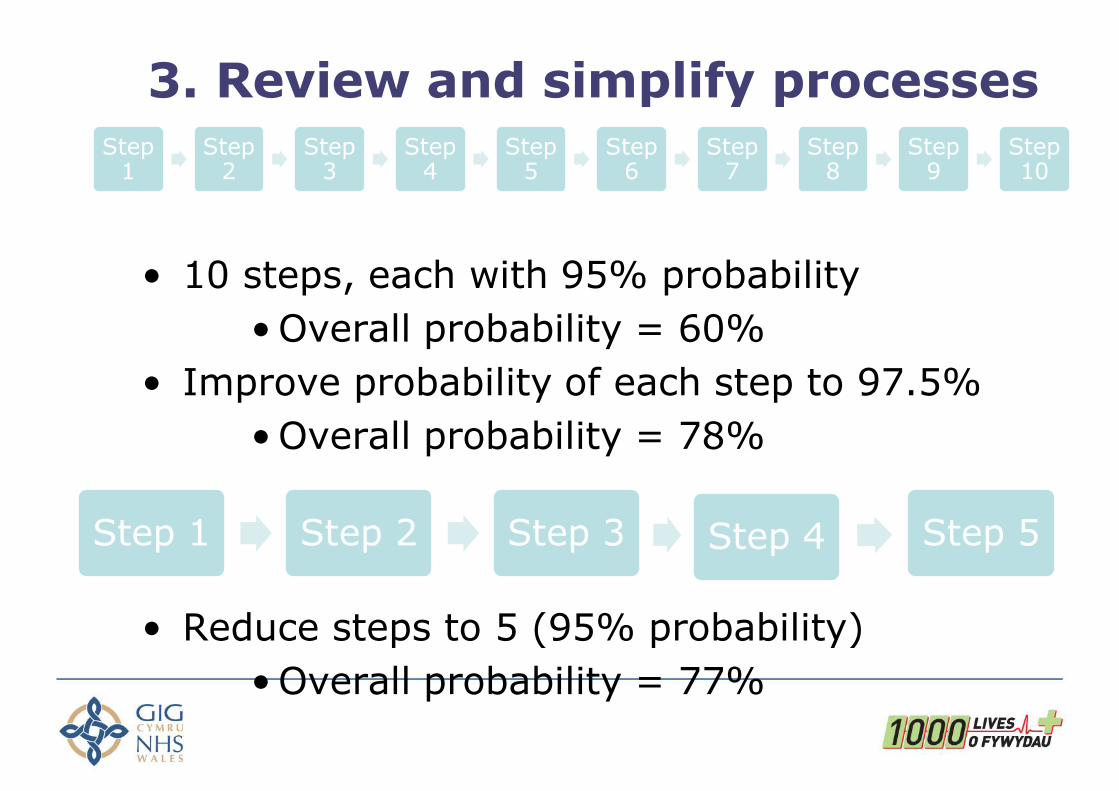
3. Review and simplify processes
• 10 steps, each with 95% probability
• Overall probability = 60%
• Improve probability of each step to 97.5%
• Overall probability = 78%
• Reduce steps to 5 (95% probability)
• Overall probability = 77%
Step 1
Step 2
Step 3
Step 4
Step 5
Step 6
Step 7
Step 8
Step 9
Step 10
Step 1 Step 2 Step 3 Step 4 Step 5

4. Standardise common processes and procedures
NEWS card & iPhone App available
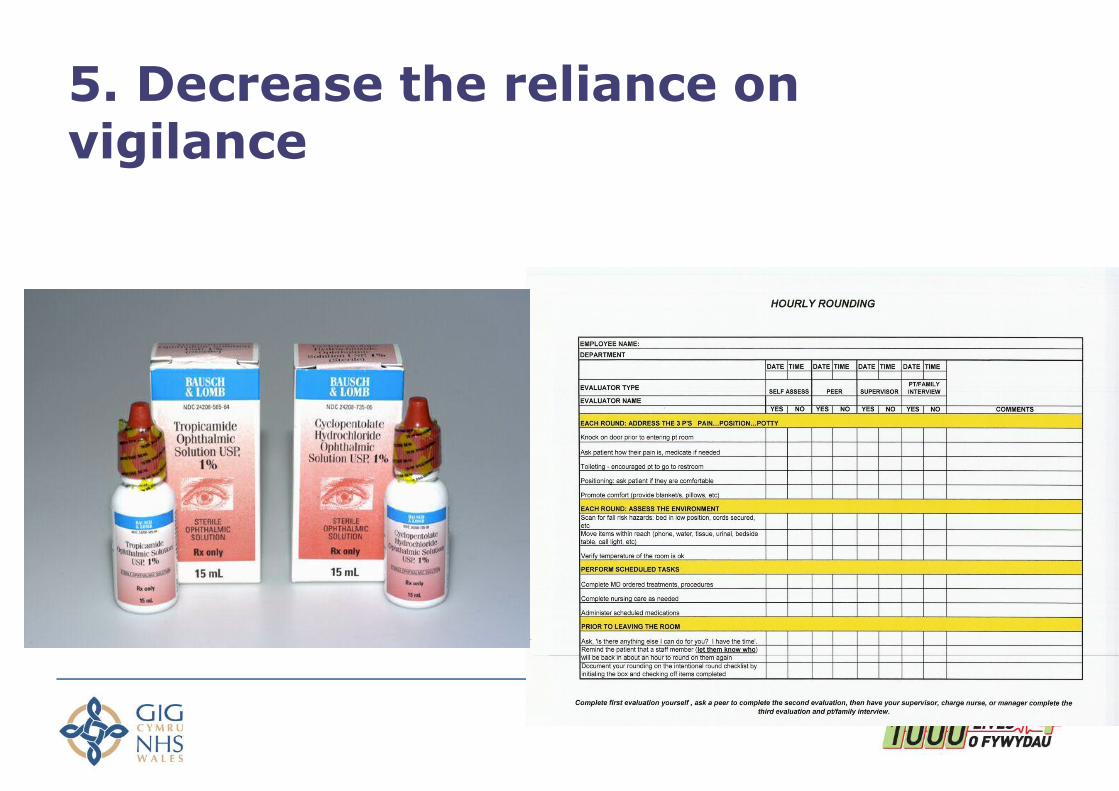
5. Decrease the reliance on vigilance

6. Routinely use checklists

All Wales Endoscopy Checklist
Insert name of presentation on Master Slide

Briefings
• Booklet users felt Briefings to be an integral part of preventing problems, better teamwork and making improvements
• Also, other benefits; ... the proportion of late starts had reduced by more than 15% in that time compared with the previous 12 months
An audit between Mar and Dec 2012 found 71% of lists had briefings in one theatre and …

Error proofing

@chris23han
@MikeFealey
Give Permission to Act
• 76% Patients remained on ward care.
• 17.5% Patient care escalated to ITU/HDU
• 6.5% DNAR or RIP. – Burke et al. ESICM 2013

DESIGN DESIGN DESIGN DESIGN APPROVE
Conference Room
Real World
‘Good enough’ now beats future perfection
IMPLEMENT

DESIGN
TEST & MODIFY
TEST & MODIFY
APPROVE IF NECESSARY
Conference Room
Real World TEST &
MODIFY START TO
IMPLEMENT
The Quality Improvement Approach


Weick’s Characteristics of High Reliability Organisations
• Preoccupation with failure
• Reluctance to simplify
• Sensitivity to operations
• Commitment to resilience
• Deference to expertise

Exercise 3
• How could you redesign your process using human factors principles to achieve greater reliability?

Summary
• Human factors broadly addresses cognitive and ergonomic issues to change behaviour
• Improving system reliability by ‘making it easier to do the right thing’
• Applies equally to ‘basic’ systems as to ‘high tech’
• Improving communication and situational awareness yields greatest results
• Give Permission to Act
• Good enough now beats future perfection
• Always events
• Application of human factors principles is an essential part of becoming a High Reliability Organisation

Questions?
• http://www.1000livesplus.wales.nhs.uk/
• Follow me on Twitter @chris23han – #Sepsis
– #RRAILS
– #NEWS_Wales