utilizing science & technology and innovation for development impact of sms on improving...
TRANSCRIPT
Utilizing Science & Technology and Innovation for Development
Impact of SMS on improving Medication Adherence among Diabetes Mellitus Type-2 in Jordan
Marriott Hotel- Amman, August 13th, 2015
Project Team
Fadi M. Alkhateeb, BSPharm, MBA, Ph.D. Director of Assessment & Associate
Professor of Pharmacy Texas A&M Health Science Center College of Pharmacy
Texas, USA
Lara Tutunji, BSPharm, Ph.D. Assistant Professor of Pharmacy The University of Jordan College of
Pharmacy Amman, Jordan
Brief Description
• Poor adherence to treatment of chronic disease is worldwide problem of striking magnitude. Recently, the world health organization stated that only 50% of patient diagnosed with chronic illness were fully compliant with their treatment regimen, in developing country the rate are even lower.1
• It is undeniable that many patient experiences difficulty in following treatment recommendations
• Several studies suggest that a large proportion of people with diabetes have difficulty managing their medication regimens (oral hypoglycemic agents [OHAs] and insulin) as well as other aspects of self-management 1
• Worldwide, adherence rate for medication for diabetes vary between 36 and 93%2
• Adherence to prescribed medication is crucial to reach metabolic control as non adherence with blood glucose lowering drug is associated with higher HbAIc levels
Brief Description
• Poor medication adherence (i.e., failure to take the proper medication at the correct time) is a causative factor for diminished control of type 2 diabetes mellitus (T2DM) in patients.
• Poor adherence is also correlated with an increased incidence of vascular, nephrologic, neurologic and ophthalmological complications as well as a higher cost burden1.
• One of the chief causes for suboptimal adherence is patients’ inability to recall and act upon dosage regimens2.
• Other variables associated with a lack of compliance in T2DM include socioeconomic status, and low health literacy 3,4.
• Low health literacy is also significantly associated with hypoglycemic episodes 5.
Justifications
• Due to the high penetration of mobile phones across socioeconomic groups and the high read rate for mobile SMS (short message service), text message medication reminders offer a promising intervention for improving medication adherence in T2DM patients.
Objectives
• The primary objective of this study is to improve medication adherence in patients with T2DM via use of daily SMS medication reminders.
• Secondary objectives include: 1) to assess health literacy levels in an
ethnically diverse, patient population, 2) to examine the predictive potential of
measured health literacy and disease knowledge for medication adherence, and
3) to perform a test-retest with health literacy and disease knowledge assessment tools.
Scope of work/DurationEstimated Budget
Scope of work: Health & Environment / Pharmaceutical Outcomes
Duration: One year
Estimated Budget: 42,500 JOD ($70,000)
Research Team
• Nurse as research assistant to fill out the questionnaires, collect baseline data, and make sure that SMS messages are being sent
• Internist for evaluation of results compared to baseline data
• Statistician for statistical evaluation of results
Methodology of Implementation
A randomized, open-label, controlled study will be conducted at the Health Center / Nazzal, Amman, Jordan with a diverse patient population.
The intervention is daily SMS medication reminders. Participants will be
randomized to either the SMS + standard care group (intervention) or standard care alone (control) group for 6 months.
Baseline data, including HbA1C, demographics, and medication regimens will be collected for all patients at the initial visit. Other measures employed at baseline and month 6 in this study include health literacy via the REALM-SF (Rapid Estimate of Adult Literacy in Medicine – Short Form) instrument and disease knowledge with the DKT (Disease Knowledge Test) – T2DM subset tool to allow for test-retest validation.
Medication adherence will be assessed at months 3 and 6 via refill records, the MMAS (Morisky Medication Adherence Scale) and measured by hemoglobin A1C (HbA1C).
Methodology of Implementation
Baseline data, including HbA1C, demographics, and medication regimens will be collected for all patients at the initial visit.
Those patients randomized to the SMS group will receive daily text messages which will be administered by use of the SMS by research personnel. The daily text message will be delivered to participants cell phones to read, “It’s that time”.
Data collected at subsequent patient visits at months 3 and 6 will include patient counseling, HbA1c, and all standard labs along with assessment of adherence (MMAS) in both groups.
In the intervention group only, a brief, 3-item questionnaire will be administered to assess satisfaction and to evaluate SMS alert fatigue at months 3 and 6
Methodology of Implementation
For both groups, disease state knowledge and health literacy assessments will be administered again at month 6 in order to allow for test-retest validation. The data will be evaluated using logistic regression analysis
A sample size of 300 patients was calculated to be sufficient to provide a power of 80% to detect a 10% (absolute value 0.75%, estimated SD 1.0) change in HbA1c at the 5% level of significance, assuming a dropout rate of 10%.
Baseline data, including HbA1C, demographics, and medication regimens will be collected for all patients at the initial visit and the REALM-SF and DKT-T2DM will similarly be administered in both arms at that time.
Inferential statistical tests will be used to assess the effect of SMS on adherence.
Multivariable linear regression will be used to explore associations between health literacy and HbA1C levels
Summary
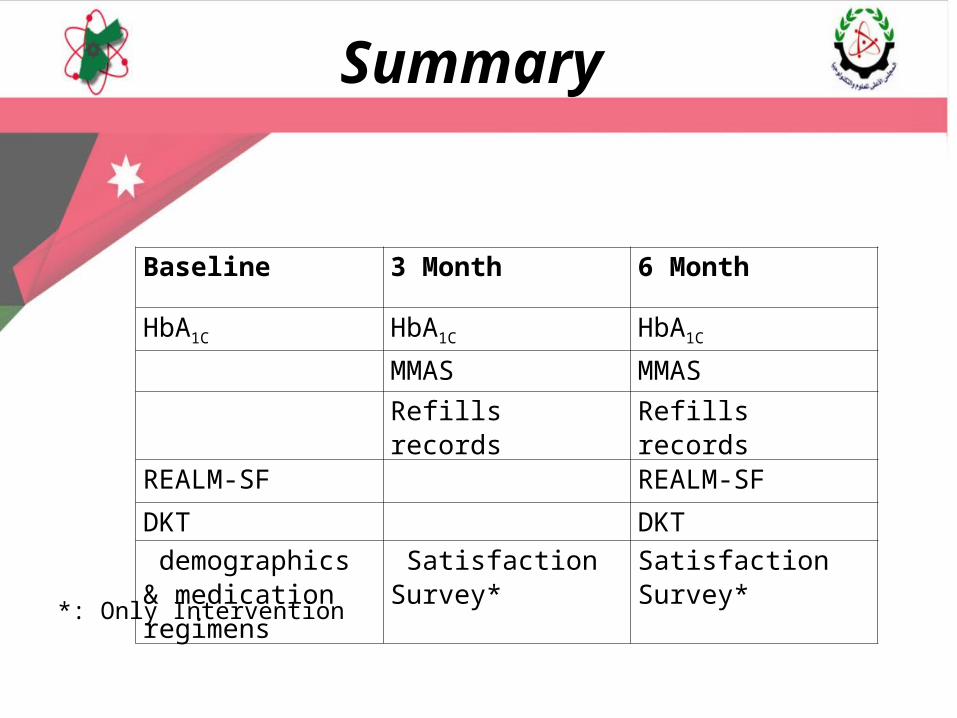
Baseline 3 Month 6 Month
HbA1C HbA1C HbA1C
MMAS MMASRefills records Refills records
REALM-SF REALM-SF
DKT DKT demographics & medication regimens
Satisfaction Survey* Satisfaction Survey*
*: Only Intervention
Methodology of ImplementationPatient Population
• The patients will be randomly selected from the Outpatient Clinics of healthcare centre in Nazal area, Amman, Jordan. Patients’ consent should be obtained according to the regulations of the Ministry of Health in Jordan.
• Clinicians at the Health Center / Nazzal, Amman, Jordan will screen, recruit and determine eligibility for adult patients who are newly diagnosed with type 2 diabetes mellitus (T2DM),
• Inclusion criteria for all participants will include: o Patients 18 years of age, who have been newly diagnosed with T2DM
at least 1 year earlier,o Who received oral hypoglycemic medication (sulphonylurea or/and
biguanide), o Who did not use insulin or suffer from chronic complications, o have SMS-capable cell phones, and who are Arabic literate.
Expected output
• Our study will show an evidence on the effectiveness of SMS interventions to enhance adherence in patients suffering type 2 diabetes mellitus.
• The outcomes of this study indicates that SMS could have an influential and important role in improving adherence in patients taking type 2 diabetes mellitus medications
Impact
If significant improvement is detected in the intervention group, it could be the basis for a large, multi-center study to be used as guidance for a low cost, high impact method to increase medication adherence, improve patient outcomes, and help address the $1.0 billion cost burden of the this public health issue in Jordan.
Action Plan
Funding •Estimated Budget: 42,500 JOD ($70,000)• Salaries for a physician and a nurse.• Reimbursement for 300 patients for their time
(20JD)• Cost for sending SMS messages (3*180*150) • Statistician for statistical evaluation of results
(1000JD)
•Texas A&M University Division of Research Program to Enhance Scholarly and Creative Activities (PESCA) Grant, ($25,000) and will be applying to the
•Scientific Research Fund (SRF) ($45.000).
References 1. Vermeire E, Wens J, Van Royen P, Biot Y, Hearnshaw H, Lindenmeyer A.
Interventions for improving adherence to treatment recommendations in people with type 2 diabetes mellitus. Cochrane Database Syst Rev. 2005;(2):CD003638.2. Odegard PS, Capoccia K. Medication taking and diabetes: a systematic review of the literature. Diabetes Educ. 2007;33(6):1014-29; 1030-1.3. Cabellero AE, Tenzer P. Building cultural competency for improved diabetes care: Latino Americans and diabetes. J Fam Pract. 2007;56(9 Suppl Building):S7-13.4. Schillinger D, Grumbach K, Piette J, Wang F, Osmond D, Daher C, Palacios J, Sullivan GD, Bindman AB. Association of health literacy with diabetes outcomes. JAMA. 2002;288(4):475-82.5. Sarkar U, Karter AJ, Liu JY, Moffet HH, Adler NE, Schillinger D. Hypoglycemia is More Common Among Type 2 Diabetes Patients with Limited Health Literacy: The Diabetes Study of Northern California (DISTANCE). J Gen Intern Med. 2010;25(9):962-8.6. Brunton S. Implementing treatment guidelines for type 2 diabetes in primary care. Postgrad Med. 2009;121(2):125-38.7. Ajlouni K1, Khader YS, Batieha A, Ajlouni H, El-Khateeb M. An increase in prevalence of diabetes mellitus in Jordan over 10 years. J Diabetes Complications. 2008 Sep-Oct;22(5):317-24.
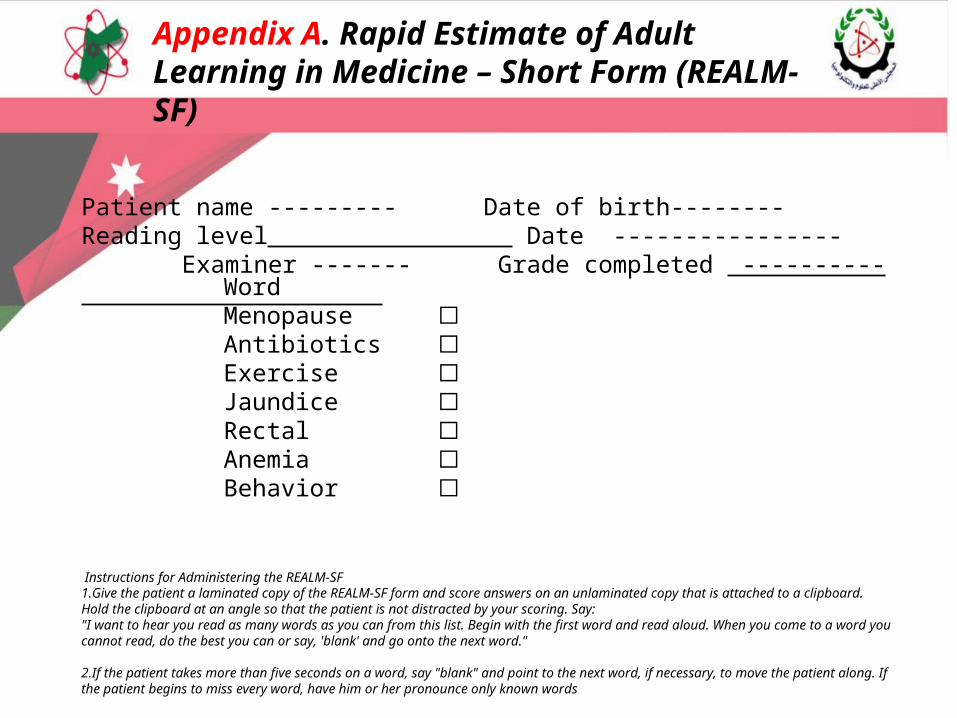
Patient name --------- Date of birth-------- Reading level Date ---------------- Examiner ------- Grade completed ----------
Instructions for Administering the REALM-SF1.Give the patient a laminated copy of the REALM-SF form and score answers on an unlaminated copy that is attached to a clipboard. Hold the clipboard at an angle so that the patient is not distracted by your scoring. Say: "I want to hear you read as many words as you can from this list. Begin with the first word and read aloud. When you come to a word you cannot read, do the best you can or say, 'blank' and go onto the next word."
2.If the patient takes more than five seconds on a word, say "blank" and point to the next word, if necessary, to move the patient along. If the patient begins to miss every word, have him or her pronounce only known words
Permissions: REALM-SF was developed by researchers via a the Agency for Healthcare Research and Quality (AHRQ), a publicly funded agency which is not copyrighted. Per AHRQ, “These tools can be used for research, clinical, or program planning purposes“ (http://www.ahrq.gov/populations/sahlsatool.htm)
Appendix A. Rapid Estimate of Adult Learning in Medicine – Short Form (REALM-SF)
Word Menopause ☐Antibiotics ☐Exercise ☐Jaundice ☐Rectal ☐Anemia ☐Behavior ☐
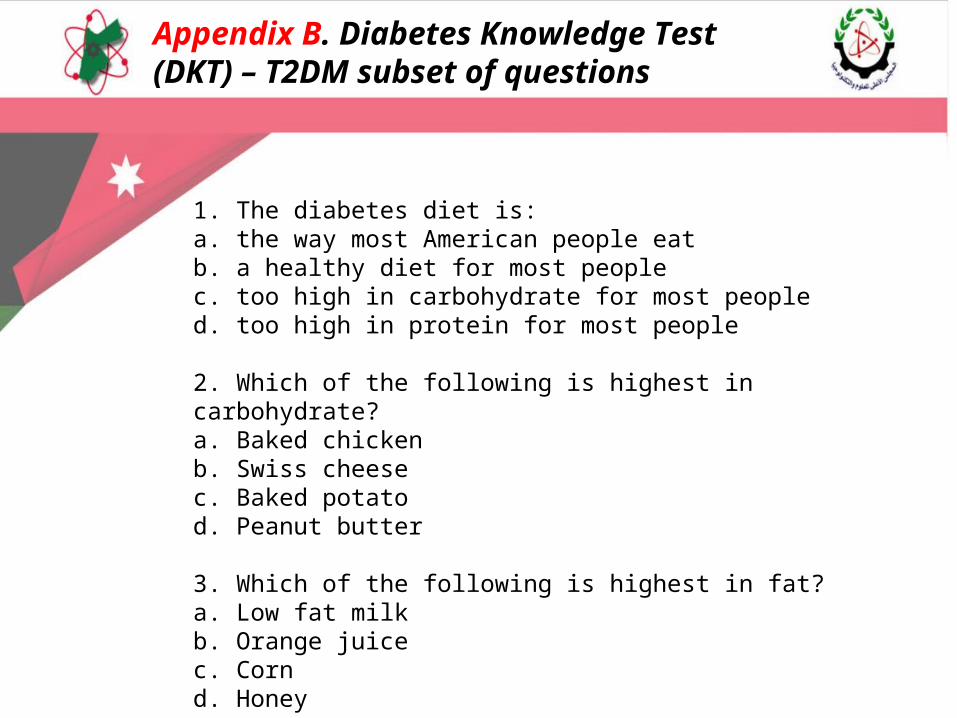
Appendix B. Diabetes Knowledge Test (DKT) – T2DM subset of questions
1. The diabetes diet is:a. the way most American people eatb. a healthy diet for most peoplec. too high in carbohydrate for most peopled. too high in protein for most people 2. Which of the following is highest in carbohydrate?a. Baked chickenb. Swiss cheesec. Baked potatod. Peanut butter 3. Which of the following is highest in fat?a. Low fat milkb. Orange juicec. Cornd. Honey
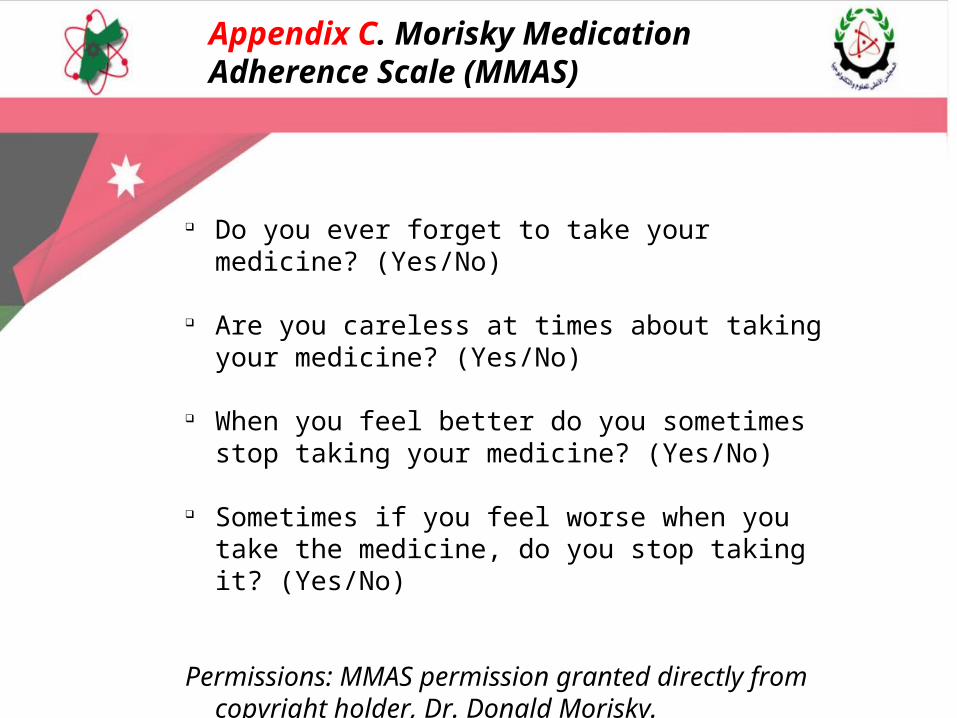
Do you ever forget to take your medicine? (Yes/No)
Are you careless at times about taking your
medicine? (Yes/No) When you feel better do you sometimes stop
taking your medicine? (Yes/No) Sometimes if you feel worse when you take the
medicine, do you stop taking it? (Yes/No) Permissions: MMAS permission granted directly
from copyright holder, Dr. Donald Morisky.
Appendix C. Morisky Medication Adherence Scale (MMAS)