vaginal birth after cesarean delivery
TRANSCRIPT
Candidate : Dr Nandini JahagirdarGuide : Prof Neerja BhatlaSenior resident guide : Dr Praveen Kumar
Vaginal Birth After Cesarean delivery
(VBAC)
Cragin’s dictum,1916 “once a cesarean, always a cesarean”
In 1910, Mason and Williams – The strength of healed cesarean section scars
of guinea pigs & cats tested by subjecting to increasing weights.
Rupture was noted in the muscle but not the scar in 100% cases.
Kerr’s low transverse uterine incision – 1921 – reduced maternal mortality from sepsis & hemorrhage
-Gave greater strength to healed incision site
Background
Cragin himself witnessed VBAC in a woman in whom he did the cesarean NY Med . 1916;104:1–3
Rethinking the Dictum : Case in 1930s gave an excellent review on VBAC showing 70% success rate in British population J Obstet Gynaecol Br Commonw. 1971;78:203–14
In U.S., till 1970, patients with previous cesarean were mostly delivered by elective repeat cesarean – leading to Five-fold increase in rate of cesarean deliveries
From 1980 onwards, reappraisal of the situation, careful selection of candidates for VBAC began
First guideline was formed by ACOG in 1999
Elective repeat cesarean Delivery (ERCD) – Also called ERCS (Elective Repeat Cesarean Section)
Trial of labor after cesarean (TOLAC) This can have 2 outcomes
Successful TOLAC – Vaginal Birth After Cesarean Delivery (60 to 80%)
Failed TOLAC - Emergency cesarean Delivery
Options for a patient with previous cesarean
The available data is limited by 3 important factors
No Prospective, Randomized trials of TOL V/S ERCD available so far
Adverse maternal or perinatal outcomes are rare & large study populations are necessary to observe a significant difference in outcomes
The woman’s choice to attempt a TOLAC is heavily influenced by her health-care provider & local resources - leading to selection bias in published reports
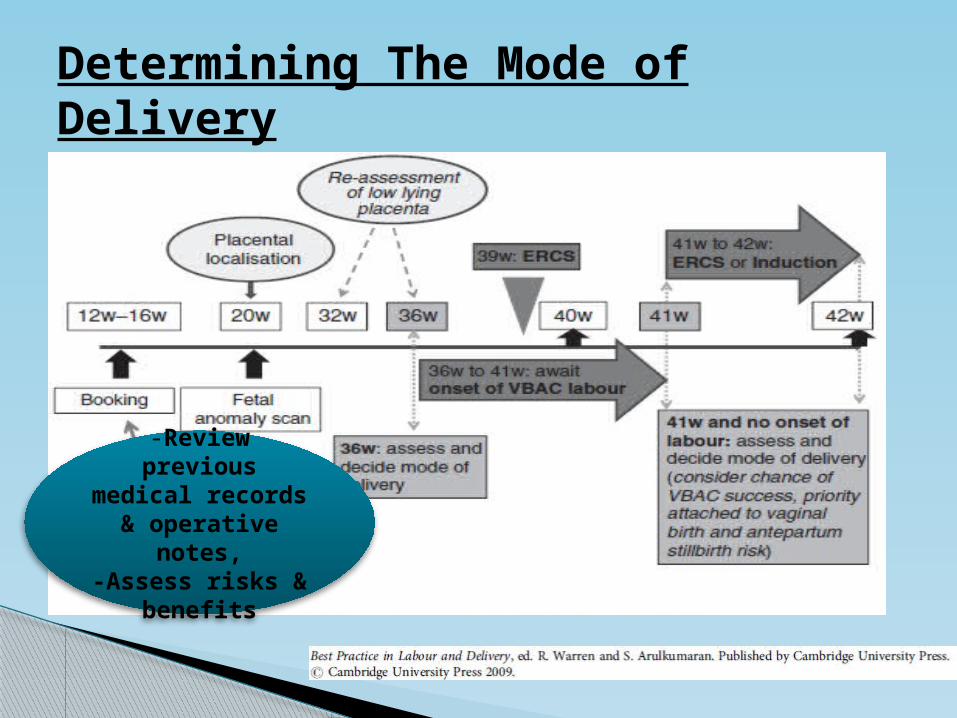
Determining The Mode of Delivery
-Review previous
medical records & operative
notes,-Assess risks &
benefits
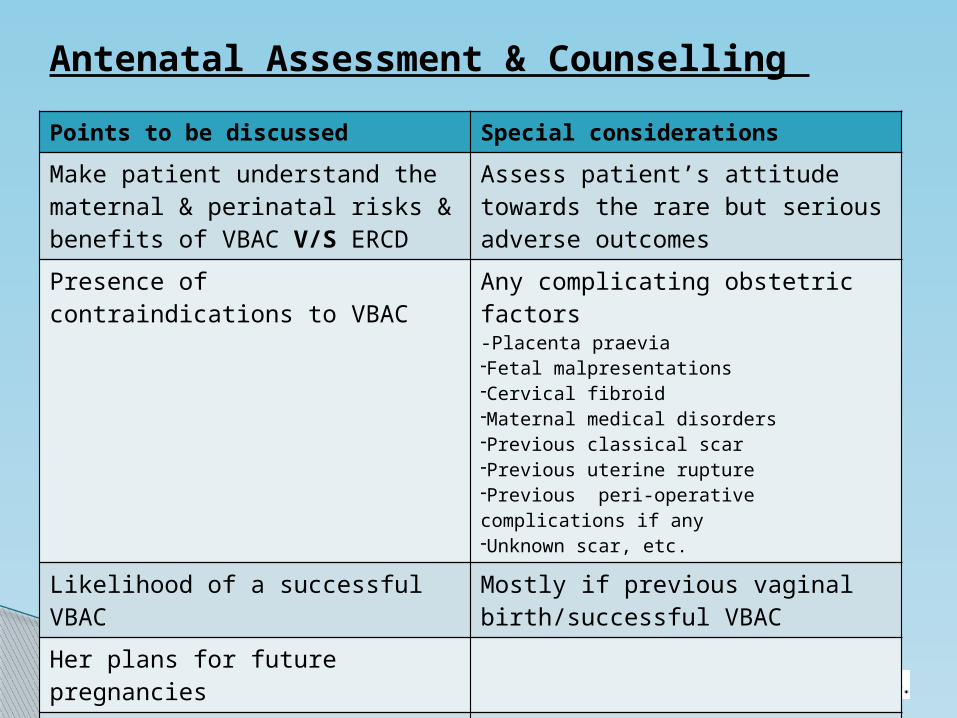
Antenatal Assessment & Counselling Points to be discussed Special considerationsMake patient understand the maternal & perinatal risks & benefits of VBAC V/S ERCD
Assess patient’s attitude towards the rare but serious adverse outcomes
Presence of contraindications to VBAC
Any complicating obstetric factors-Placenta praevia-Fetal malpresentations -Cervical fibroid -Maternal medical disorders -Previous classical scar -Previous uterine rupture -Previous peri-operative complications if any -Unknown scar, etc.
Likelihood of a successful VBAC Mostly if previous vaginal birth/successful VBAC
Her plans for future pregnanciesPersonal preference & motivation to achieve vaginal birth or ERCD

Risks And Benefits
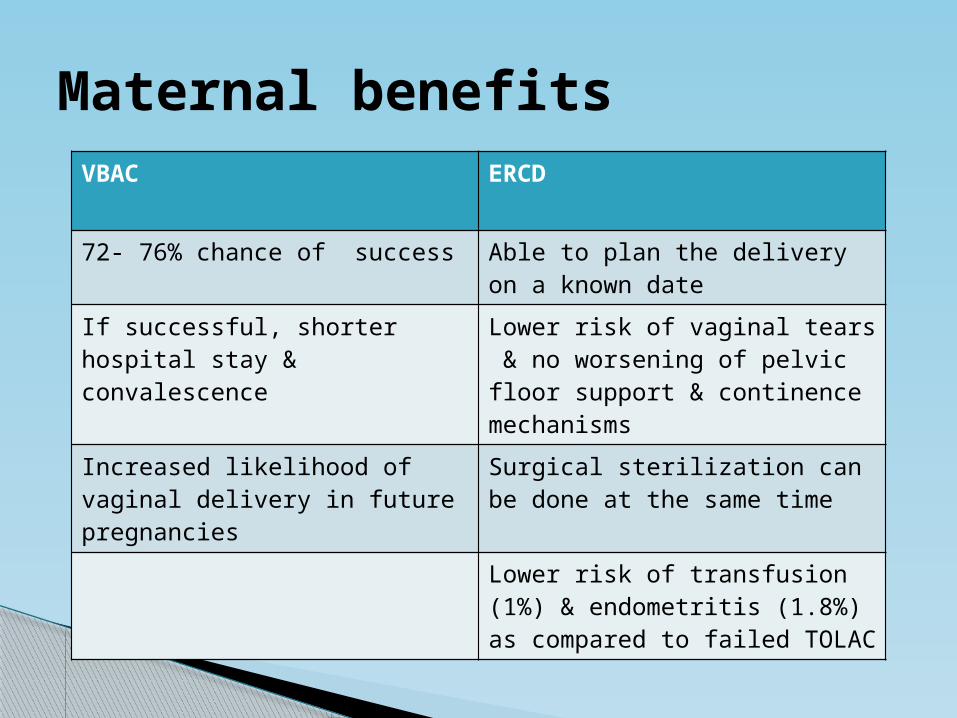
Maternal benefitsVBAC ERCD
72- 76% chance of success Able to plan the delivery on a known date
If successful, shorter hospital stay & convalescence
Lower risk of vaginal tears & no worsening of pelvic floor support & continence mechanisms
Increased likelihood of vaginal delivery in future pregnancies
Surgical sterilization can be done at the same timeLower risk of transfusion (1%) & endometritis (1.8%) as compared to failed TOLAC
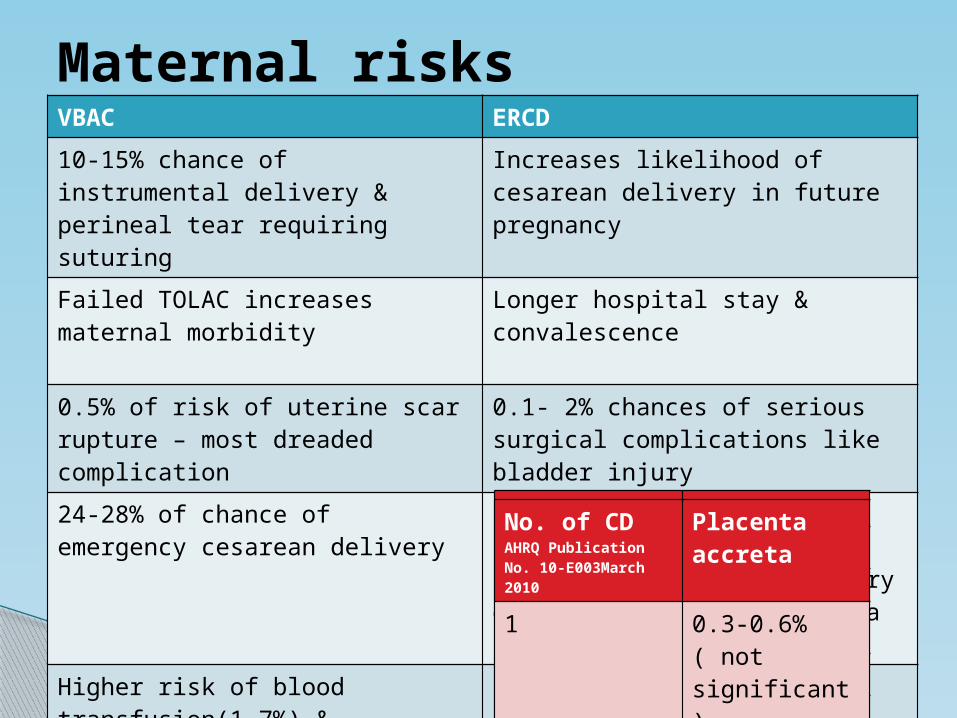
Maternal risksVBAC ERCD10-15% chance of instrumental delivery & perineal tear requiring suturing
Increases likelihood of cesarean delivery in future pregnancy
Failed TOLAC increases maternal morbidity
Longer hospital stay & convalescence
0.5% of risk of uterine scar rupture – most dreaded complication
0.1- 2% chances of serious surgical complications like bladder injury
24-28% of chance of emergency cesarean delivery
Increased risk of surgical complications with each subsequent cesarean delivery due to adhesions, placenta praevia/accreta
Higher risk of blood transfusion(1.7%) & endometritis(2%)
No . Of CD Placenta praevia
1 1%2 1.7%3 2.3%>3 2.8%Any no. 1.2%
No. of CD AHRQ Publication No. 10-E003March 2010
Placenta accreta
1 0.3-0.6%( not significant)
2 or more 1.4%5 or more 6.74%
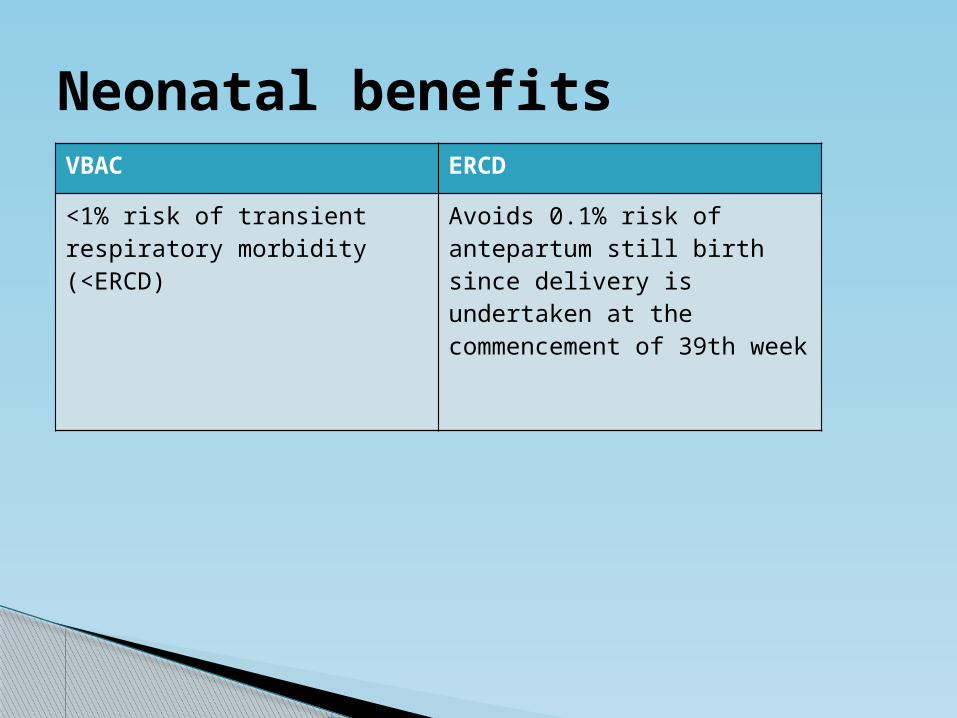
Neonatal benefitsVBAC ERCD
<1% risk of transient respiratory morbidity (<ERCD)
Avoids 0.1% risk of antepartum still birth since delivery is undertaken at the commencement of 39th week
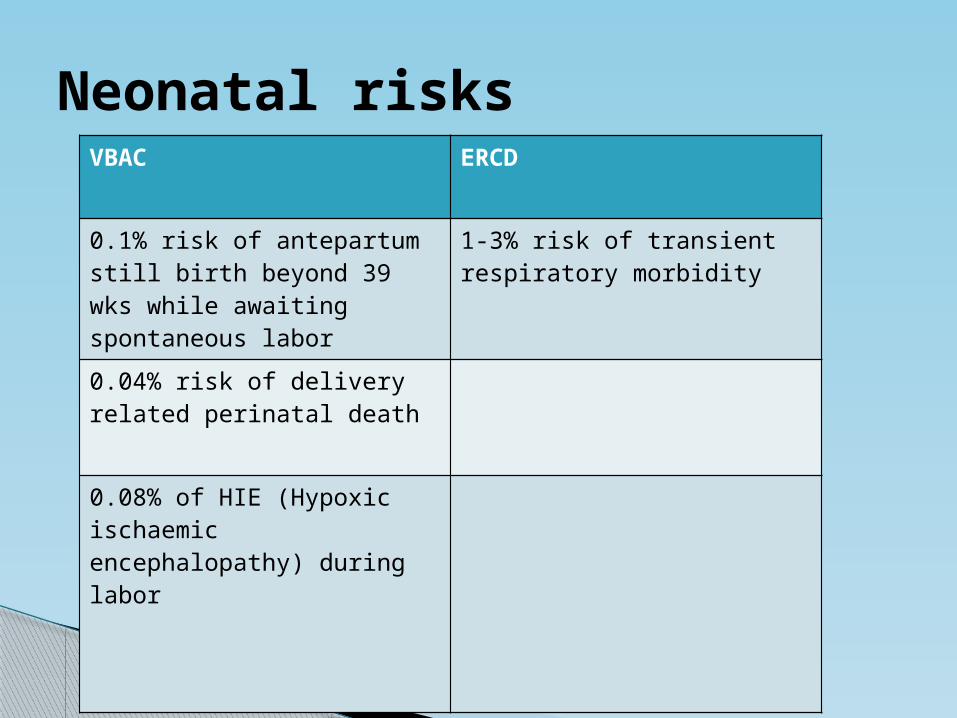
Neonatal risksVBAC ERCD
0.1% risk of antepartum still birth beyond 39 wks while awaiting spontaneous labor
1-3% risk of transient respiratory morbidity
0.04% risk of delivery related perinatal death
0.08% of HIE (Hypoxic ischaemic encephalopathy) during labor
Largest & most comprehensive Study is conducted by Landon et al Done in women enrolled in NICHD Maternal-Fetal
Medicine Units Network, 1999-2002 In TOLAC group , n= ~18000 In ERCD group, n= ~16000 This study includes all women who had a prior
cesarean delivery & who had a singleton pregnancy at 20 weeks or more of gestation or whose infant had a birth weight of at least 500 g
Women undergoing Cesarean for other indications were excluded
Maternal & perinatal outcomes in VBAC V/S ERCD
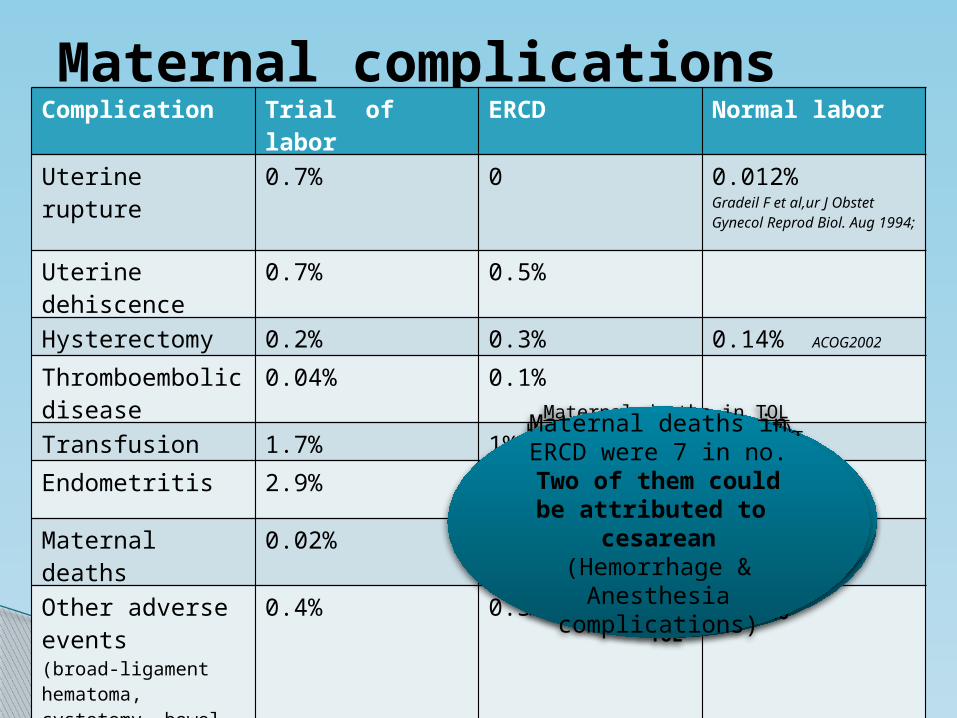
Maternal complications
N Engl J Med 2004,351:2581
Complication Trial of labor ERCD Normal laborUterine rupture 0.7% 0 0.012%
Gradeil F et al,ur J Obstet Gynecol Reprod Biol. Aug 1994;
Uterine dehiscence
0.7% 0.5%
Hysterectomy 0.2% 0.3% 0.14% ACOG2002
Thromboembolic disease
0.04% 0.1%
Transfusion 1.7% 1%Endometritis 2.9% 1.8% 1-2% Parkland
Hospital
Maternal deaths 0.02% 0.04%Other adverse events(broad-ligament hematoma, cystotomy, bowel injury, and ureteral injury)
0.4% 0.3%
Maternal deaths in TOL were 3 in no. & were due to
1.Severe PIH with hepatic failure2.Sickle cell crisis with cardiac arrest3.PPH
None of them could be directly attributed to TOL
Hysterectomy in ERCD(47)-1.Atony(17) 2.Placenta accreta(12)3.Unexplained hemorrhage(5)4.Extension / laceration(2)5.Myoma (3) 6.cancer(5) 7.Others (3)
Maternal deaths in ERCD were 7 in no.
Two of them could be attributed to
cesarean (Hemorrhage &
Anesthesia complications)
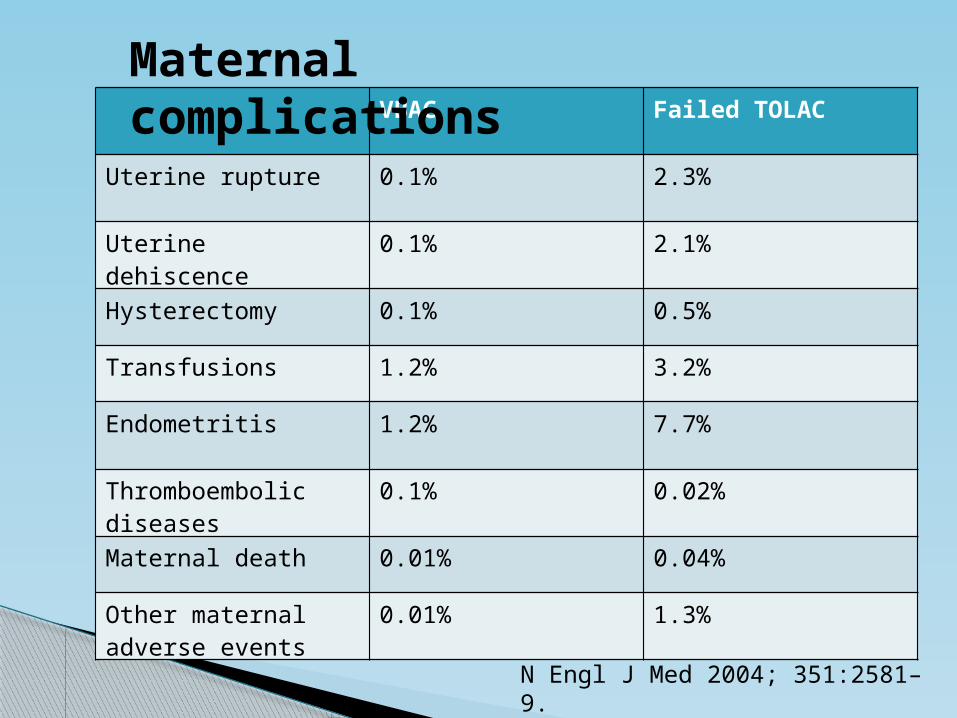
N Engl J Med 2004; 351:2581–9.
VBAC Failed TOLAC
Uterine rupture 0.1% 2.3%
Uterine dehiscence 0.1% 2.1%
Hysterectomy 0.1% 0.5%
Transfusions 1.2% 3.2%
Endometritis 1.2% 7.7%
Thromboembolic diseases
0.1% 0.02%
Maternal death 0.01% 0.04%
Other maternal adverse events
0.01% 1.3%
Maternal complications
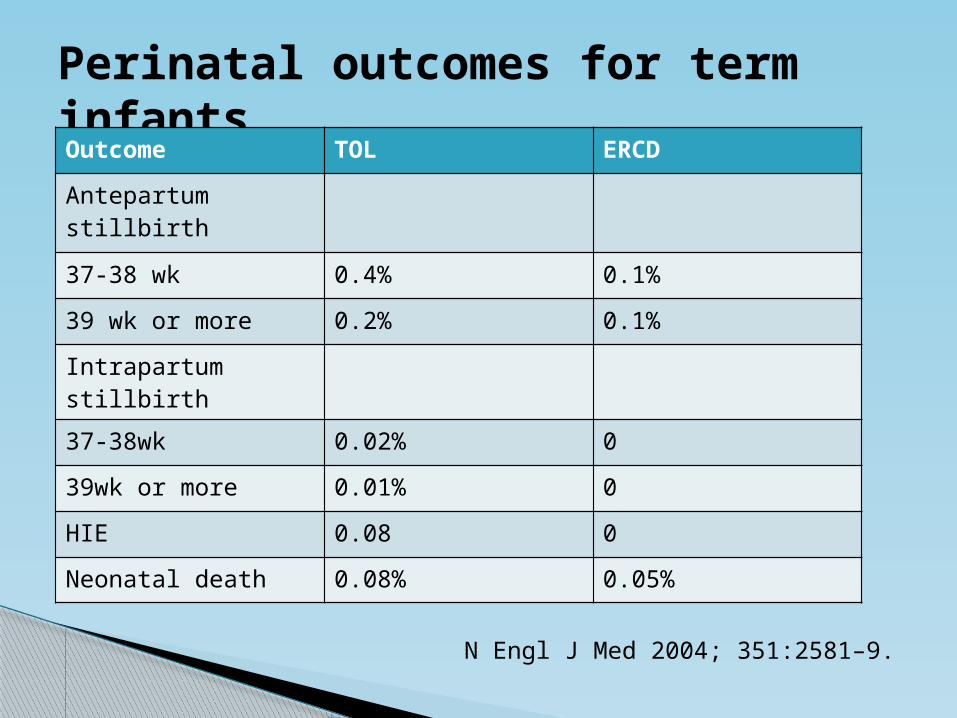
Perinatal outcomes for term infantsOutcome TOL ERCDAntepartumstillbirth
37-38 wk 0.4% 0.1%39 wk or more 0.2% 0.1%Intrapartum stillbirth37-38wk 0.02% 039wk or more 0.01% 0HIE 0.08 0Neonatal death 0.08% 0.05%
N Engl J Med 2004; 351:2581–9.
Selection of candidates for VBAC
Previous 1 LSCS Clinically adequate pelvis No other uterine scar / previous rupture Physician immediately available throughout
active labor, capable of monitoring labor, performing an emergency cesarean delivery
Availability of anesthesia & personnel for emergency cesarean delivery
ACOG practice bulletin 2010
Special circumstances
VBAC success rate - 75.3% (in 2 or > previous LSCS) Uterine Rupture rate – 1.7% Miller et al.
(1994) In a meta-analysis, VBAC success rate – 71.1% ( Previous 2 LSCS ) Uterine rupture rate – 1.4% S Tahseen, M Griffiths -BJOG
2010;117:5–19.
No conclusive evidence available on methods of induction or augmentation of labor
More than one previous LSCS
Comparison of outcome of trial of labor after previous two Caesarean sections V/S previous one Cesarean sections – A Prospective clinical Trial is undergoing
at AIIMS by Dr Prerna under guidance of Prof Neerja Bhatla So far, 2 women with previous 2 LSCS have
had successful Trial of labor Both of them were induced with PGE2
(0.5mg) at 39-40wks
Several studies support VBAC in Twins with a success rate 69-84%
Rate of uterine rupture was not found significantly high - Miller et al and Strong et al
ACOG 2010 - “Women with one previous cesarean delivery with a low transverse incision, who are otherwise appropriate candidates for twin vaginal delivery, may be considered candidates for TOLAC”
Multiple pregnancy
“ERCD is associated with better perinatal outcome in a previous LSCS with Breech presentation in current pregnancy”
-A large multicentric trial by Hannah et al.-
External Cephalic Version (ECV) is not contraindicated – ACOG 2010 Flamm BL, Am JObstet Gynecol
1991;165:370–2, Sela HY, Eur J Obstet Gynecol Reprod Biol
2009;142:111–4
SOGC (Society of obstetricians & gynaecologists of Canada) discourages VBAC in Breech
Breech presentation
Suspected macrosomia (>4000g) is not a contraindication for TOL but decreases success rate of VBAC -Elkousy et al(2003)
Success rate of 60% is observed -Zelop et al. Am J Obstet
Gynecol 185:903, 2001
Macrosomia
No significant difference in the outcome of the next pregnancy
Chapman et al, Ohel et al, Hauth et al
Few studies although found increased risk of uterine rupture, no sufficient data available
Durwald & Mercier, Bujold et al Longterm outcomes of CORONIS Trial (A large
randomised multicentre fractional, factorial trial) & CAESAR Trial (Caesarean section surgical techniques: a
randomised factorial trial) are awaited
Single v/s Double layer closure of Uterus
Other Factors
Maternal obesity – Decreases probability of VBAC - BMI >40 associated with 61% chances of successful VBAC Hibbard et al, Juhas et al
History of postpartum fever after Caesarean section - 3 fold increase in rupture Shipp T et al Am J Obstet
Gynecol.2001;184:S71
Mullerian duct anomalies – 8% risk of rupture
Ravasia et al, Am J ObstetGynecol. 1999;181:877–881
Maternal age - <30yrs (Decrease risk of uterine rupture : 0.5% v/s 1.4%)
Shipp T et al Am J Obstet
Gynecol.2001;184:S71.-Their relationship to the risk of uterine rupture have been examined in
small studies, but definitive conclusions cannot yet be drawn.
Related to Previous Cesarean Delivery
Previous classical or T /J shaped uterine incision Previous uterine rupture Uterine surgeries involving full muscle thickness (Hysterotomy, Preterm LSCS, myomectomy with cavity
opened. No consistent evidence available for incidence of uterine
rupture in Laparoscopic v/s open myomectomy) Previous >2 LSCS (VBAC in previous 3 LSCS has been reported as early as in1979 but not enough evidence
available) Unknown scar – In the absence of previous operative
records, a detailed history may be taken Most common incision, however is, low transeverse & VBAC
is reasonable Obstet Gynecol.1994;84:255–258
Contraindication to trial of labor after cesarean (TOLAC)
Obstetric or Medical complication
Malpresentation Antepartum hemorrhage- Placenta praevia, Placenta
accreta Severe PIH/eclampsia Placental insufficiency (IUGR, Oligohydramnios) Medical disorders like HTN, Heart disease, Renal disease,
Asthma, Seizure disorders, Thyroid disorders (Grobmann et al – Inconsistent evidence, VBAC can be
given)
Contracted pelvis/CPD
Inability to perform emergency cesarean due to insufficient staffing / facilities
Predicting the success v/s failure
of Trial of Labor
ACOG practice bulletin 2010
Increased probability of success of TOLACPrior vaginal birthSpontaneous onset of Labor
Decreased probability of successRecurrent indication for initial cesarean delivery ( Dystocia, CPD)Increased maternal AgeNonwhite ethnicityGestational age > 40 weeksMaternal obesityPre-eclampsiaShort interpregnancy intervalIncreased neonatal birth weight
Factors increasing likelihood of successMaternal age < 40Prior vaginal deliveryFavorable cervix, spontaneous laborPrior cesarean for non recurrent indication
Factors decreasing likelihood of success Increased no of prior cesarean deliveriesGestational age > 40 weeksBirth weight > 4 kg Induction or augmentation of labor
Criteria for success (American academy of family physicians)
Factors decreasing risk of failure Age <40 Prior vaginal delivery Indication for previous cesarean other than failure
of progress Cervical effacement at admission > 75% Cervical dilatation at admission > 4cm
Score 0-2 has success rate of 49% & for 8-10, 95% Flamm ,Obstet gynecol 1994;83:927-32
Scoring system to predict Success v/s Failure of VBAC
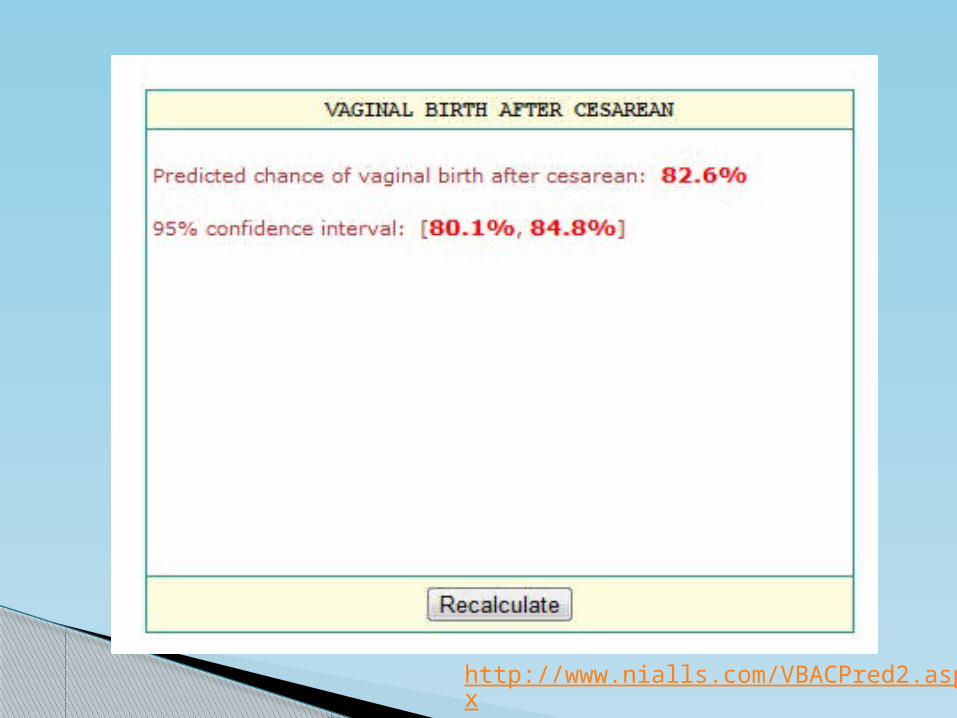
Grobman & colleagues (2007) Developed a nomogram to predict a
successful TOL & maternal morbidity based on a questionnaire in a term gestation with previous 1 LSCS
-A score >60 has a 75-80% chances of a successful vaginal delivery
Obstetrics and Gynecology, volume 109, pages 806-12, 2007
E-Calculator
Defined as “A primary cesarean delivery at maternal request in the absence of any medical or obstetrical indication”.
(ACOG–American College of Obstetrician and Gynecologists, Committee Opinion, Number 394, December 2007)
Cesarean Delivery by Maternal Request (CDMR)
-ACOG states Elective cesareans are justified options
-FIGO(2003) entails CDMR ‘a positive right of women’
Lower incidence of endometritis/ transfusions Lower Neonatal / Perinatal Morbidity Fewer Infant Birth Injuries during Delivery Better Maternal Postpartum Satisfaction &
Psychological Wellbeing Better Sexual Health in the Immediate
Postpartum Period & in some cases, long term Reduced or Avoided Urinary Incontinence & Fecal
Incontinence Less damage to pelvic floor, vaginal tearing,
episiotomy, and risk of future pelvic organ prolapse
Factors influencing CDMR

Intrapartum management
Take detailed informed written consent
To be conducted in a suitably staffed & equipped setting with the facility for emergency cesarean delivery 24x7 & neonatal resuscitation
An Obstetrician, Anesthesiologist & pediatrician should be immediately available
PGE 2 may be used to induce labor with caution.
IV access, adequate blood cross matched
Monitor maternal BP, PR & ST every 15 min
Intrapartum management
Continuous fetal monitoring by CTG (II A)
Intrauterine pressure catheters - not routinely useful
Oxytocin should be used with caution (In AIIMS - low dose, starting from 1mIU/min is being used for augmentation)
No contraindication for epidural analgesia – does not reduce success or mask signs of rupture
Regular review of partogram by senior obstetrician
Routine postpartum exploration of scar - not needed
Most Dreaded complication of TOLAC
Relative risk of uterine rupture in TOL compared to ERCD is 2.07
Maternal and or fetal morbidity of rupture 10-25%
In rupture, 1.5/10,000 risk of perinatal death &
4.8/10,000 risk of hysterectomy
Uterine rupture
Uterine rupture – Complete disruption of all layers of uterus associated with one/more of the following-
Hemorrhage requiring surgical exploration Hysterectomy, Injury to the bladder Extrusion of any part of feto-placental unit Cesarean delivery for suspected uterine rupture Cesarean delivery for fetal distress
Uterine dehiscence – Asymptomatic uterine disruption (complete or incomplete) having no effect on mother or neonate
Uterine rupture V/S Uterine dehiscence
Most Reliable First sign is - “Non reassuring fetal heart tracing”
Most Specific sign is - Persistent variable fetal heart deceleration.
Clinical signs of uterine rupture
Classical signs (Unreliable) Maternal tachycardia, Hypotension, Hematuria, Pain over previous incision site Vaginal bleeding
Dramatic loss of station Low sensitivity, high specificity
Clinical signs of Uterine Rupture….
Risk factors for uterine rupture
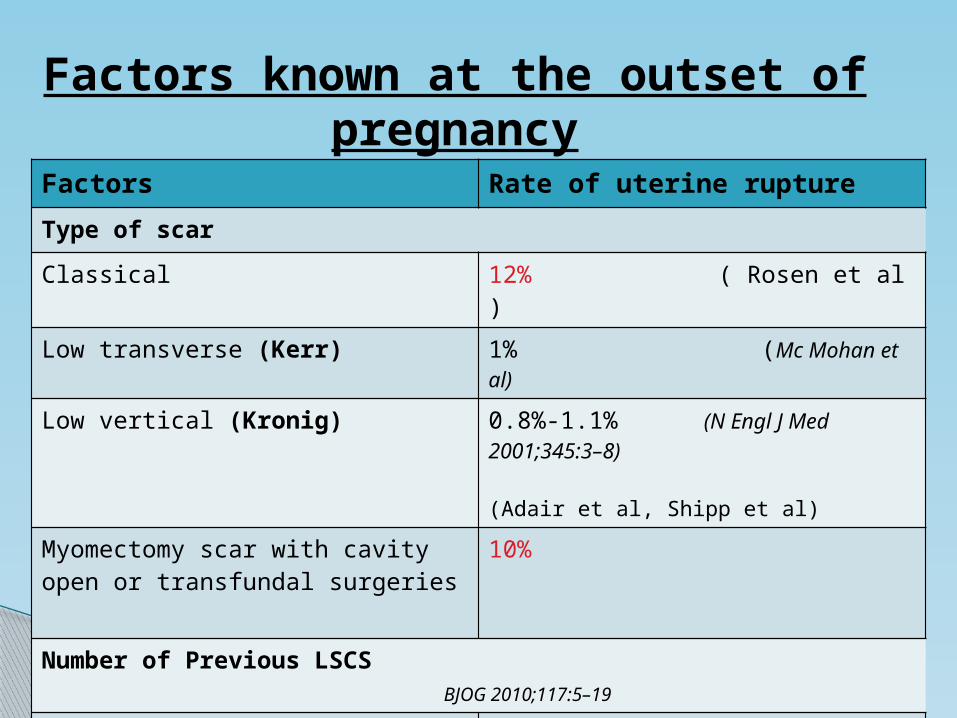
Factors known at the outset of pregnancy
Factors Rate of uterine ruptureType of scarClassical 12% ( Rosen et al ) Low transverse (Kerr) 1% (Mc Mohan et al)
Low vertical (Kronig) 0.8%-1.1% (N Engl J Med 2001;345:3–8) (Adair et al, Shipp et al)
Myomectomy scar with cavity open or transfundal surgeries
10%
Number of Previous LSCS BJOG 2010;117:5–19
1 LSCS 0.8%2 LSCS 1.4%
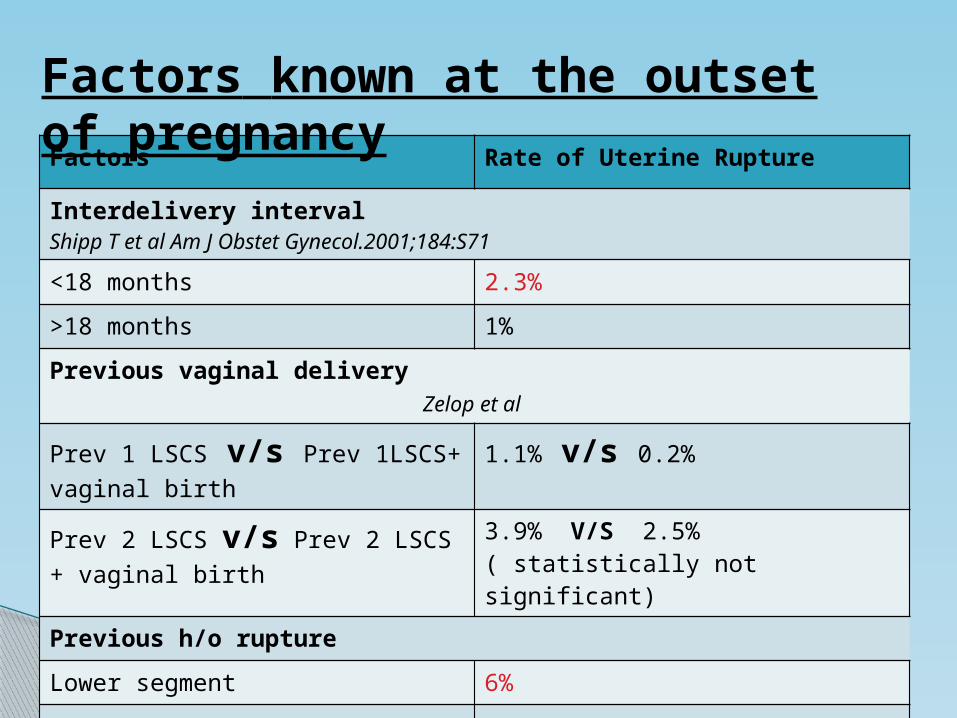
Factors Rate of Uterine Rupture
Interdelivery interval Shipp T et al Am J Obstet Gynecol.2001;184:S71<18 months 2.3%>18 months 1%Previous vaginal delivery Zelop et al
Prev 1 LSCS v/s Prev 1LSCS+ vaginal birth
1.1% v/s 0.2%
Prev 2 LSCS v/s Prev 2 LSCS + vaginal birth
3.9% V/S 2.5% ( statistically not significant)
Previous h/o ruptureLower segment 6%Upper segment 32%
Factors known at the outset of pregnancy
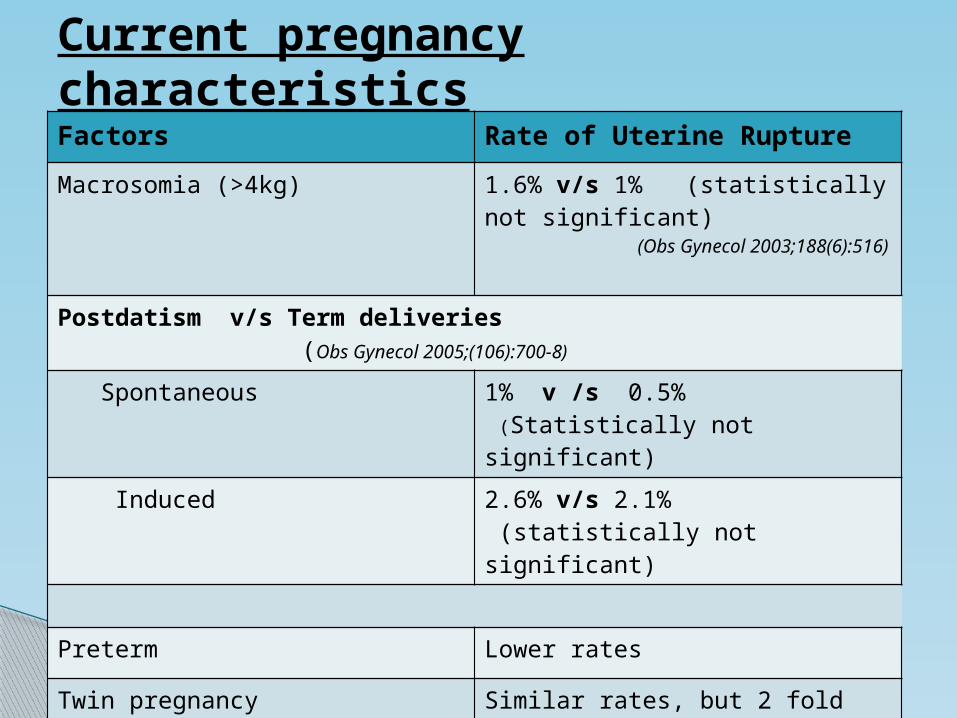
Current pregnancy characteristicsFactors Rate of Uterine RuptureMacrosomia (>4kg) 1.6% v/s 1% (statistically not
significant) (Obs Gynecol 2003;188(6):516)
Postdatism v/s Term deliveries (Obs Gynecol 2005;(106):700-8)
Spontaneous 1% v /s 0.5% (Statistically not significant)
Induced 2.6% v/s 2.1% (statistically not significant)
Preterm Lower rates
Twin pregnancy Similar rates, but 2 fold increased risk of dehiscence
Breech & ECV Results not definitive
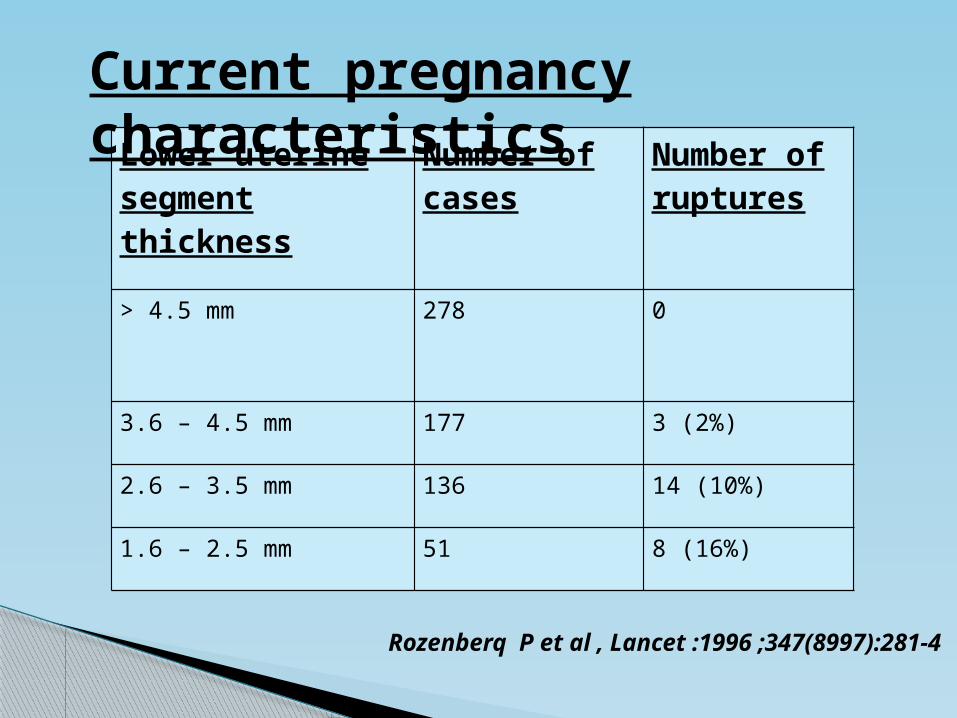
Rozenberq P et al , Lancet :1996 ;347(8997):281-4
Lower uterine segment thickness
Number of cases
Number of ruptures
> 4.5 mm 278 0
3.6 – 4.5 mm 177 3 (2%)
2.6 – 3.5 mm 136 14 (10%)
1.6 – 2.5 mm 51 8 (16%)
Current pregnancy characteristics
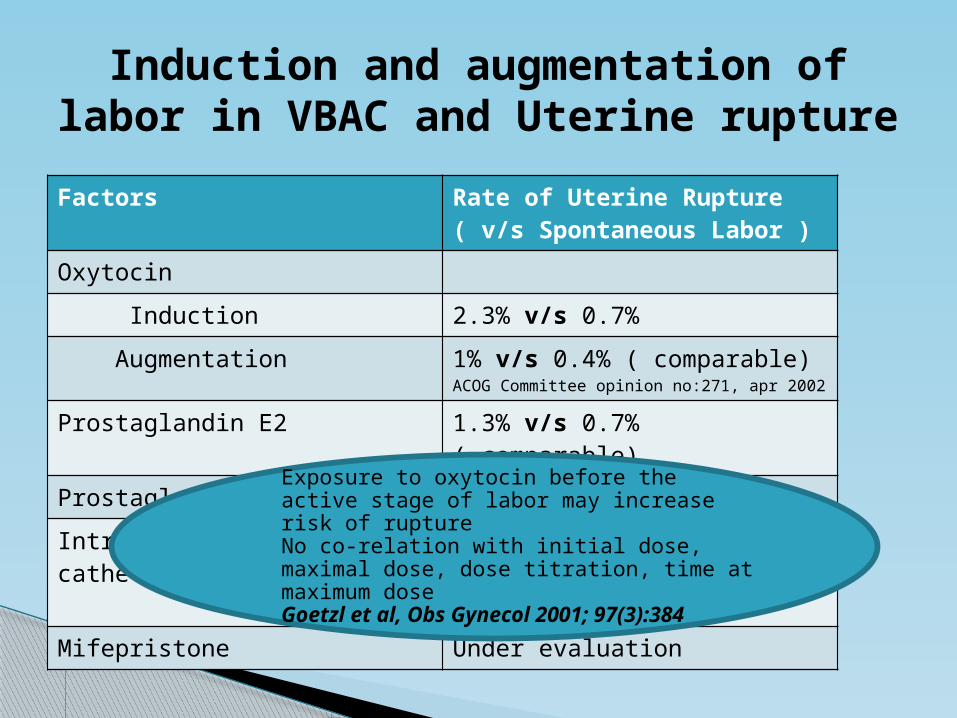
Induction and augmentation of labor in VBAC and Uterine ruptureFactors Rate of Uterine Rupture
( v/s Spontaneous Labor )Oxytocin Induction 2.3% v/s 0.7% Augmentation 1% v/s 0.4% ( comparable)
ACOG Committee opinion no:271, apr 2002
Prostaglandin E2 1.3% v/s 0.7% ( comparable)Prostaglandin E1 5.6%Intracervical foley’ catheter Safe
Also recommended in second trimester induction
Mifepristone Under evaluation
Exposure to oxytocin before the active stage of labor may increase risk of ruptureNo co-relation with initial dose, maximal dose, dose titration, time at maximum doseGoetzl et al, Obs Gynecol 2001; 97(3):384
Cost of failed TOLAC is more than successful TOL or repeat cesarean
If rupture rate > 3.2%, the increased infant morbidity/mortality of attempted TOLAC exceeded the benefits of reduced cost
TOLAC is cost effective if the rate of successful vaginal delivery >74%
So careful patient selection is necessary before planning TOL
Obs Gynecol 2001;97:932-41
Economics of VBAC
ACOG practice bulletin 2010
Most women with previous 1 LSCS are candidates for VBAC & Should be counseled about VBAC & offered TOLAC
Epidural analgesia for labor may be used as part of TOLAC
Misoprostol should not be used for 3rd trimester cervical ripening or labor induction in patients with previous cesarean delivery or major uterine surgeries
ACOG Guidelines Level A Evidence

VBAC is recommended in previous 2 LSCS with low transverse scar and previous 1 LSCS with twins
ECV for breech is not contraindicated in previous LSCS Scars other than low transverse/ low vertical scars or those
in whom Vaginal delivery is contraindicated (eg.placenta accreta) are contraindications for VBAC
Induction of labor for maternal/fetal indication remains an option
Previous unknown uterine scar is not a contraindication unless there is high suspicion of classical cesarean delivery
Level B evidence
ACOG practice bulletin 2010
There are no areas of significant difference as compared to RCOG
Guidelines -2007 -RCOG also encourages trial in 3
or more previous cesarean deliveries

THANK YOU