validation of new ajcc exclusion criteria for subepithelial prostatic stromal invasion from pt4a...
TRANSCRIPT

Validation of New AJCC Exclusion Criteria for Subepithelial
Prostatic Stromal Invasion from pT4a Bladder Urothelial Carcinoma
Amit R. Patel, Joshua A. Cohn, Ahmed Abd El Latif, Ranko Miocinovic,Gary D. Steinberg,* Gladell P. Paner and Donna E. Hansel†From the Section of Urology (ARP, JAC, GDS, GPP) and Department of Pathology (GPP), University of Chicago, Chicago, Illinois, andGlickman Urological and Kidney Institute (AAEL, RM), and Department of Pathology and Laboratory Medicine (DEH), Cleveland Clinic,Cleveland, Ohio
Purpose: In 2010 the AJCC (American Joint Committee on Cancer) excludedurothelial carcinoma with subepithelial prostatic stromal invasion from the pT4abladder cancer staging class, which is otherwise defined by direct prostaticinvasion transmurally from the bladder. We determined if the new guidelineswere reflective of differences in survival between subepithelial prostatic stromalinvasion and transmural pT4a disease.Materials and Methods: A retrospective, multi-institutional cohort of cystectomycases with subepithelial prostatic stromal invasion from the University of Chi-cago and Cleveland Clinic were compared to a cohort with transmural pT4adisease. All pathological specimens were rereviewed at the respective institu-tions. Patients were excluded from the final cohort if variant bladder cancerhistology, pT3 bladder disease or extraprostatic extension of urothelial carcinomawere identified. The primary end points were cancer specific and overall survival.Results: Our study sample consisted of 48 patients with subepithelial prostaticstromal invasion and 49 patients with transmural pT4a disease. Median followupwas 12.8 months (IQR 4.9 to 31.4). Patients with subepithelial prostatic stromalinvasion had lower rates of lymph node involvement than those with transmuralpT4a disease (14.6% vs 61.2%, p �0.001) and lower rates of positive surgicalmargins (18.7% vs 61.2%, p �0.001). Rates of perioperative chemotherapy weresimilar in both groups. When comparing subepithelial prostatic stromal invasionand transmural pT4a groups, overall survival was 64.0 vs 9.8 months and mediancancer specific survival was not achieved vs 16.5 months, respectively (p �0.001).Conclusions: Subepithelial prostatic stromal invasion from urothelial carcinomahas more favorable outcomes compared to transmural pT4a disease. Our resultssupport the exclusion of subepithelial prostatic stromal invasion from the pT4abladder urothelial carcinoma staging class.
Key Words: carcinoma, transitional cell; prostate; neoplasm invasiveness;
Abbreviations
and Acronyms
BCG � bacillus Calmette-Guérin
CSS � cancer specific survival
LN � lymph node
OS � overall survival
SM � surgical margins
SSI � subepithelial prostaticstromal invasion
UC � urothelial carcinoma
Accepted for publication July 17, 2012.Study received institutional review board ap-
proval.* Financial interest and/or other relationship
with Endo, Abbott Molecular and Predictive Bio-sciences.
† Correspondence: Department of Pathologyand Laboratory Medicine, Cleveland Clinic, 9500Euclid Ave., Cleveland, Ohio 44195 (telephone:216-444-5893; e-mail: [email protected]).
urinary bladder neoplasms; cystectomy
IN 2012 there will be an estimated73,510 new cases and 14,880 deathsfrom bladder cancer in the UnitedStates.1 The estimated lifetime prob-ability of bladder cancer developing inCaucasians in the United States and
Western Europe is estimated at 1 in0022-5347/13/1891-0053/0THE JOURNAL OF UROLOGY®
© 2013 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RES
25 for men and 1 in 80 for women.2
The incidence is increasing in indus-trialized and in developing nations,with 386,000 incident cases world-wide in 2008.3
Tumor grade, stage and lymph
node status are important prognostichttp://dx.doi.org/10.1016/j.juro.2012.09.006Vol. 189, 53-58, January 2013
EARCH, INC. Printed in U.S.A.www.jurology.com 53

SUBEPITHELIAL PROSTATIC STROMAL INVASION VERSUS TRANSMURAL BLADDER DISEASE54
factors, and have implications in patient counselingand management, including decisions regardingperioperative chemotherapy. Locally advanced dis-ease portends a poorer prognosis, with estimated5-year survival rates of 77% for pT2 LN negativedisease vs 44% for pT4a, LN negative disease.4 Ad-vanced T stage is generally associated with LN in-volvement. Pathological T4a disease was associatedwith a LN positive rate of 42% compared to only 18%for pT2 disease. These data illustrate the tendencyof poor prognostic factors to be grouped and under-score the prognostic differences between locally ad-vanced and organ confined invasive disease.4
Prostatic stromal invasion is not uncommon andhas typically been associated with poor prognosis.5–7
Urothelial carcinoma of the prostate has an inci-dence of 12% to 48%, of which approximately 7.6% to25% have prostatic stromal invasion.5–7 Risk factorsfor prostatic invasion include multifocal UC, carci-noma in situ and tumor location at the trigone orbladder neck.8 Many cases are associated with con-current or previous tumors in the bladder and his-tory of intravesical BCG therapy.
The 3 described patterns of prostatic stromal inva-sion from urothelial carcinoma are extravesical, trans-mural and subepithelial stromal invasion (fig. 1).9 His-torically, invasion of the prostatic stroma, whetherthrough transmural invasion or subepithelial invasionvia the prostatic urethra, had been classified as a sub-set of pT4a disease. In 2010 the AJCC reclassifiedprimary staging for bladder cancer to exclude SSI fromthe pT4a staging status, reserving the pT4a classifica-tion for those tumors extending into the prostate byway of transmural invasion through the bladderwall.10
Figure 1. Prostatic invasion from UC via transmural and ex-
travesical route (A), and subepithelial invasion (B).We investigated the validity of the new AJCCguidelines using patient cohorts from the ClevelandClinic and University of Chicago. We determinedwhether the changes in the AJCC guidelines werereflective of more favorable pathological parame-ters, such as margin and LN status, and cancerspecific and overall survival for patients with SSIcompared to transmural pT4a disease.
METHODS
With the approval of the institutional review boards atUniversity of Chicago and Cleveland Clinic, the patientcohorts were extracted from institutional databases. TheUniversity of Chicago study sample contained all patientswho underwent radical cystectomy for UC between De-cember 1994 and October 2011, and were diagnosed withpT4a disease (extravesical/transmural and SSI). TheCleveland Clinic provided a cohort of patients from March2004 to March 2010 who were diagnosed with pT4a dis-ease based on the finding of SSI rather than transmuralinvasion. All pathology was reviewed by GPP and DEH atthe respective institutions. We included in study onlycases considered to be urothelial carcinoma, and excludedthose that had nonurothelial morphology such as pureadenocarcinoma, squamous cell carcinoma and small cellcarcinoma. We also excluded cases that demonstrated apredominant variant morphology of urothelial carcinomasuch as micropapillary or nested urothelial carcinoma. Inaddition, patients were excluded upon review if they hadSSI and additionally had pT3 disease in the bladder orextraprostatic extension of subepithelial UC. The ratio-nale for eliminating pT3 bladder disease was derived frompreviously published studies that demonstrated survivaloutcomes to be more strongly dependent on bladder stag-ing alone than SSI.11
Following review of pathology, the pT4a study samplewas divided into 2 cohorts of transmural pT4a and SSI.Demographic factors collected included age, ASA (Ameri-can Society of Anesthesiologists) score and smoking his-tory. Clinical data included history of intravesical BCG,history of radiation therapy and history of perioperativechemotherapy. Pathological data included tumor histol-ogy, T stage, LN status and margin status (urethral, ure-teral or soft tissue margin). Time of last followup and timeto death were obtained by review of the medical recordsand the Social Security Death Index. Primary end pointswere overall and cancer specific survival. The likelihood ofLN positive disease and margin status was analyzed as anestimate of the extent of disease at surgery.
Statistical analysis was performed with MedCalc® ver-sion 11.5.1.0 and the chi-square test was used to comparecategorical values. Medians were compared via the Mann-Whitney U test. Kaplan-Meier curves were generated tocompare OS and CSS between the 2 groups using the logrank test. Multivariate Cox proportional hazards modelswere developed using Stata® 11 to estimate the effect ofeach covariate (age, group, total LN, positive LN and SM)on survival. Additional analysis was performed to evalu-ate factors (primary bladder stage, SM and LN status)
influencing survival in the SSI group.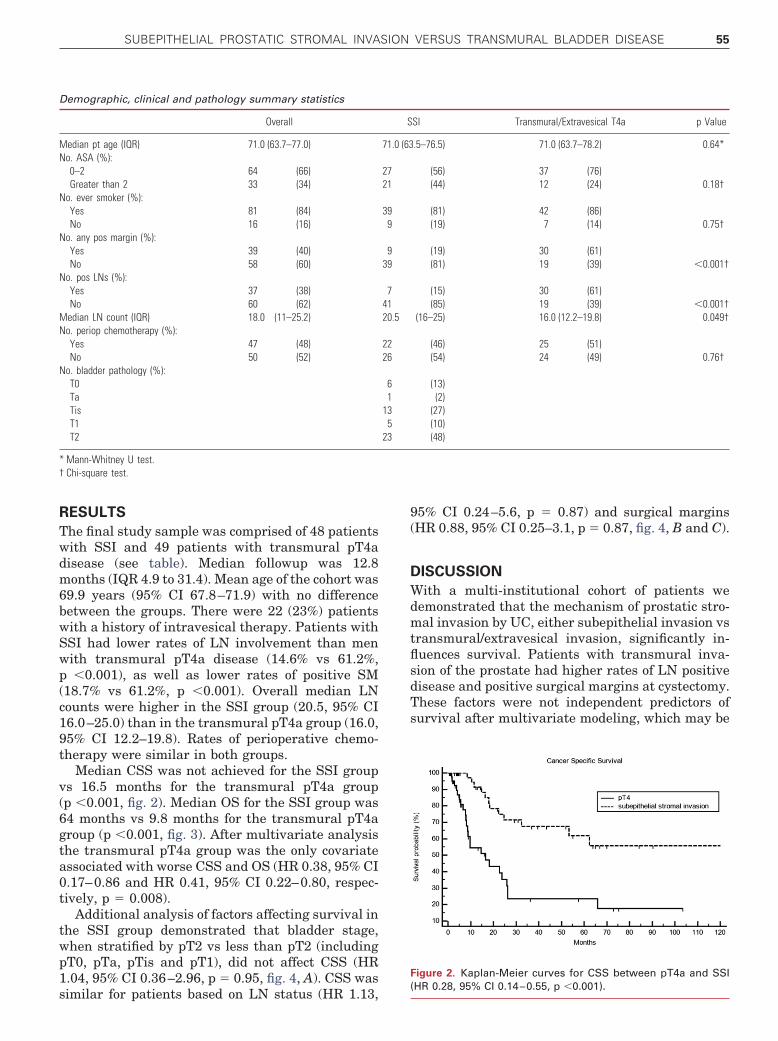
SUBEPITHELIAL PROSTATIC STROMAL INVASION VERSUS TRANSMURAL BLADDER DISEASE 55
RESULTS
The final study sample was comprised of 48 patientswith SSI and 49 patients with transmural pT4adisease (see table). Median followup was 12.8months (IQR 4.9 to 31.4). Mean age of the cohort was69.9 years (95% CI 67.8–71.9) with no differencebetween the groups. There were 22 (23%) patientswith a history of intravesical therapy. Patients withSSI had lower rates of LN involvement than menwith transmural pT4a disease (14.6% vs 61.2%,p �0.001), as well as lower rates of positive SM(18.7% vs 61.2%, p �0.001). Overall median LNcounts were higher in the SSI group (20.5, 95% CI16.0–25.0) than in the transmural pT4a group (16.0,95% CI 12.2–19.8). Rates of perioperative chemo-therapy were similar in both groups.
Median CSS was not achieved for the SSI groupvs 16.5 months for the transmural pT4a group(p �0.001, fig. 2). Median OS for the SSI group was64 months vs 9.8 months for the transmural pT4agroup (p �0.001, fig. 3). After multivariate analysisthe transmural pT4a group was the only covariateassociated with worse CSS and OS (HR 0.38, 95% CI0.17–0.86 and HR 0.41, 95% CI 0.22–0.80, respec-tively, p � 0.008).
Additional analysis of factors affecting survival inthe SSI group demonstrated that bladder stage,when stratified by pT2 vs less than pT2 (includingpT0, pTa, pTis and pT1), did not affect CSS (HR1.04, 95% CI 0.36–2.96, p � 0.95, fig. 4, A). CSS was
Demographic, clinical and pathology summary statistics
Overall
Median pt age (IQR) 71.0 (63.7–77.0)No. ASA (%):
0–2 64 (66)Greater than 2 33 (34)
No. ever smoker (%):Yes 81 (84)No 16 (16)
No. any pos margin (%):Yes 39 (40)No 58 (60)
No. pos LNs (%):Yes 37 (38)No 60 (62)
Median LN count (IQR) 18.0 (11–25.2)No. periop chemotherapy (%):
Yes 47 (48)No 50 (52)
No. bladder pathology (%):T0TaTisT1T2
* Mann-Whitney U test.† Chi-square test.
similar for patients based on LN status (HR 1.13,
95% CI 0.24–5.6, p � 0.87) and surgical margins(HR 0.88, 95% CI 0.25–3.1, p � 0.87, fig. 4, B and C).
DISCUSSION
With a multi-institutional cohort of patients wedemonstrated that the mechanism of prostatic stro-mal invasion by UC, either subepithelial invasion vstransmural/extravesical invasion, significantly in-fluences survival. Patients with transmural inva-sion of the prostate had higher rates of LN positivedisease and positive surgical margins at cystectomy.These factors were not independent predictors ofsurvival after multivariate modeling, which may be
SI Transmural/Extravesical T4a p Value
.5–76.5) 71.0 (63.7–78.2) 0.64*
(56) 37 (76)(44) 12 (24) 0.18†
(81) 42 (86)(19) 7 (14) 0.75†
(19) 30 (61)(81) 19 (39) �0.001†
(15) 30 (61)(85) 19 (39) �0.001†
(16–25) 16.0 (12.2–19.8) 0.049†
(46) 25 (51)(54) 24 (49) 0.76†
(13)(2)
(27)(10)(48)
Figure 2. Kaplan-Meier curves for CSS between pT4a and SSI
S
71.0 (63
2721
399
939
74120.5
2226
61
135
23
(HR 0.28, 95% CI 0.14–0.55, p �0.001).

SUBEPITHELIAL PROSTATIC STROMAL INVASION VERSUS TRANSMURAL BLADDER DISEASE56
due to aggressive tumor biology in transmural andextravesical stromal invasion. In contrast, patientswith SSI have organ confined disease, and theoret-ically should have lower positive margin rates andLN positive disease. This is supported by our resultsas LN positive disease was found in 17% of patientswith SSI vs 61% of patients with true locally ad-vanced disease (pT4a). Previous reports from large,single institution studies have demonstrated similarrates of LN positive disease for bladder pT2 (organconfined disease) compared to pT4a (locally ad-vanced disease).4,12 Our findings support SSI as anentity different from pT4a disease biologically andpathologically.
Secondary invasion of UC that originates withinthe prostatic urethra into the surrounding stroma isnot uncommon, and has an estimated frequency ofoccurrence in 12% to 48% of patients with bladdercancer.8,9 Risk factors for prostatic UC include non-invasive or invasive carcinoma in the region of thetrigone and bladder neck, or a history of high risknoninvasive bladder cancer with repeat transure-thral resection and BCG therapy.6,7,13 In one of thelargest series of its kind, Herr and Donat followed186 patients for a minimum of 15 years with highrisk noninvasive bladder cancer who received BCGtherapy and underwent repeat transurethral resec-tions.7 Overall, 39% of patients had relapse of UCthat involved the prostate during followup, whichdid not appear to impact CSS at a 15-year minimumfollowup. However, when the authors stratified themechanism of prostatic stromal invasion in 27 pa-tients, they found that the 15-year survival rate forSSI was significantly higher when compared withtransmural/extravesical stromal invasion (75% vs9%, p �0.001).
Pagano et al also demonstrated a difference insurvival based on the invasion pathways of the pros-tate in patients with UC.14 In their study of 72
Figure 3. Kaplan-Meier curves for OS between pT4a and SSI(HR 0.33, 95% CI 0.19–0.57, p �0.0001).
patients with pT4 disease, 8 (11%) had SSI and 44
(61%) had transmural or extravesical prostatic in-vasion, with a 5-year survival of 40% vs 7%, respec-tively. However, this study was limited by the low
Figure 4. CSS for patients with SSI stratified by bladder pT2stage and less than pT2 stage (p � 0.95) (A), LN involvement
(p � 0.87) (B) and SM (p � 0.85) (C).
SUBEPITHELIAL PROSTATIC STROMAL INVASION VERSUS TRANSMURAL BLADDER DISEASE 57
number of patients with SSI. Esrig et al conducted astudy in 143 patients with UC involving the pros-tate.11 The 5-year recurrence-free survival and OSin 58 (41%) patients with SSI was 48% and 36%,respectively, compared to 19 (13%) patients withtransmural invasion who had recurrence-free sur-vival and OS of 25% and 21%. However, almost halfof the patients in the SSI cohort also had pT3 dis-ease, which limits stratification of the subgroupsand may have negatively influenced the outcome ofthe SSI group. Based on their findings, the authorsof these studies recommended a change in the stag-ing classification of prostatic stromal invasion basedon the mechanism of invasion.
However, based on prior reports that claimed thatstromal invasion was an ominous prognostic factor,there remains nonconsensus among pathologistsand urologists.15,16 For example, numerous studieshave demonstrated no difference in survival whencomparing SSI to transmural pT4a disease, al-though study size and inclusion of pT3 bladder dis-ease limit some of the conclusions from these stud-ies. Njinou Ngninkeu et al found similar 5-yearoverall and recurrence-free survival for patientswith SSI and transmural prostate invasion (29%and 35%, vs 22% and 28%, respectively) in a smallseries of patients.17 Barocas et al conducted apathological review of 59 patients with prostaticstromal invasion, and found no difference in sur-vival between SSI and transmural prostatic inva-sion (3-year overall survival 17% vs 7%, p � 0.619).18
Ayyathurai et al examined 47 patients with pros-tatic invasion of UC.19 Although SSI was not di-rectly compared to transmural invasion, 5-yearOS for SSI was 26% vs 6% for transmural stromalinvasion (no p value reported). Shen et al demon-strated a 5-year survival probability of 32% forprostatic stromal invasion in 27 patients, but SSIand transmural invasion were not differenti-ated.20 Given that numerous previous studieshave suggested that bladder stage influences sur-vival to a greater extent than prostatic stromalinvasion alone, the results for survival in patientswith SSI would be negatively affected when in-cluding pT3 patients in the cohort.7,11,14 Despitethe limitations of study design and smaller co-horts, these studies support the controversy over
the AJCC reclassification of SSI.REFERENCES
Although the AJCC excluded SSI from the pT4astaging status, there are no guidelines as to howsubepithelial prostatic invasion should be staged.10
The staging of secondary prostatic UC could poten-tially follow the staging guidelines of primary pros-tatic UC, ie SSI would be classified as pT2 disease.10
Furthermore, prostatic involvement in a patientwith concurrent bladder cancer could be reported asa secondary stage in the final pathology report. Ex-amining true staging assignment and differences intumor biology should be the goals of future multi-institutional efforts.
Recent studies have attempted to evaluate out-comes based on the amount of extramural prostaticstromal invasion. Oliva et al found no difference inmedian OS when comparing focal vs extensive ex-tramural prostatic invasion in 35 patients (17.4 vs16.3 months).21 These findings support the theorythat tumor biology of transmural/extramural pros-tatic invasion, whether focal or extensive, may bemore aggressive than SSI.
Limitations of our study include its retrospec-tive nature and accompanying treatment biases,as well as a relatively small cohort of patients.However, the updated AJCC classification re-quires validation, and this retrospective effort willbe followed with prospective studies of subepithe-lial prostatic stromal invasion of UC. Other limi-tations may include the elimination of bladder pT3disease from the SSI cohort. This was planned apriori to keep the study sample pure and to prop-erly study the newly reclassified SSI vs pT4a dis-ease. In addition, 6 (13%) patients in our SSIcohort had bladder pT0 disease but had viableurothelial carcinoma in the prostatic stroma. Weincluded these cases in the study as they wereonce considered pT4a disease, but based on ourresults may have different tumor biology and out-comes. Stratification based on bladder stage foroutcomes and proper staging classification of SSIwill be the goals of future efforts.
CONCLUSIONS
In a retrospective, multi-institutional cohort wedemonstrated that SSI from bladder UC has morefavorable pathological and clinical outcomes com-pared to transmural pT4a disease at cystectomy.Our results support the exclusion of SSI from pT4a
staging classification for bladder cancer.1. Siegel R, Naishadham D and Jemal A:Cancer statistics, 2012. CA Cancer J Clin2012; 62: 10.
2. Howlader N, Noone AM, Krapcho M et al: SEERCancer Statistics Review, 1975–2009 (Vintage 2009Populations), National Cancer Institute. Bethesda, MD,
http://seer.cancer.gov/csr/1975_2009_pops09/,based on November 2011 SEER data submission,posted to the SEER web site, April 2012.

SUBEPITHELIAL PROSTATIC STROMAL INVASION VERSUS TRANSMURAL BLADDER DISEASE58
3. Ferlay J, Shin HR, Bray F et al: Estimates ofworldwide burden of cancer in 2008: GLOBOCAN2008. Int J Cancer 2010; 127: 2893.
4. Stein JP, Lieskovsky G, Cote R et al: Radicalcystectomy in the treatment of invasive bladdercancer: long-term results in 1,054 patients. J ClinOncol 2001; 19: 666.
5. Palou J, Baniel J, Klotz L et al: Urothelial carci-noma of the prostate. Urology 2007; 69: 50.
6. Wood DP Jr, Montie JE, Pontes JE et al: Tran-sitional cell carcinoma of the prostate in cysto-prostatectomy specimens removed for bladdercancer. J Urol 1989; 141: 346.
7. Herr HW and Donat SM: Prostatic tumor relapsein patients with superficial bladder tumors: 15-year outcome. J Urol 1999; 161: 1854.
8. Lerner SP and Shen S: Pathologic assessmentand clinical significance of prostatic involvementby transitional cell carcinoma and prostate can-cer. Urol Oncol 2008; 26: 481.
9. Donat SM, Genega EM, Herr HW et al: Mecha-nisms of prostatic stromal invasion in patientswith bladder cancer: clinical significance. J Urol
2001; 165: 1117.10. Edge SB, Byrd DR, Compton CC et al: AJCCCancer Staging Manual, 7th ed. New York:Springer 2010.
11. Esrig D, Freeman JA, Elmajian DA et al: Transi-tional cell carcinoma involving the prostate witha proposed staging classification for stromal in-vasion. J Urol 1996; 156: 1071.
12. Tarin TV, Power NE, Ehdaie B et al: Lymph node-positive bladder cancer treated with radical cys-tectomy and lymphadenectomy: effect of thelevel of node positivity. Eur Urol 2012; 61: 1025.
13. Hardeman SW, Perry A and Soloway MS: Tran-sitional cell carcinoma of the prostate followingintravesical therapy for transitional cell carci-noma of the bladder. J Urol 1988; 140: 289.
14. Pagano F, Bassi P, Ferrante GL et al: Is stage pT4a(D1) reliable in assessing transitional cell carci-noma involvement of the prostate in patientswith a concurrent bladder cancer? A necessarydistinction for contiguous or noncontiguous in-volvement. J Urol 1996; 155: 244.
15. Cheville JC, Dundore PA, Bostwick DG et al:Transitional cell carcinoma of the prostate: clin-icopathologic study of 50 cases. Cancer 1998; 82:
703.16. Schellhammer PF, Bean MA and Whitmore WFJr: Prostatic involvement by transitional cell car-cinoma: pathogenesis, patterns and prognosis.J Urol 1977; 118: 399.
17. Njinou Ngninkeu B, Lorge F, Moulin P et al:Transitional cell carcinoma involving the prostate:a clinicopathological retrospective study of 76cases. J Urol 2003; 169: 149.
18. Barocas DA, Patel SG, Chang SS et al: Outcomesof patients undergoing radical cystoprostatec-tomy for bladder cancer with prostatic involve-ment on final pathology. BJU Int 2009; 104: 1091.
19. Ayyathurai R, Gomez P, Luongo T et al: Prostaticinvolvement by urothelial carcinoma of the blad-der: clinicopathological features and outcome af-ter radical cystectomy. BJU Int 2007; 100: 1021.
20. Shen SS, Lerner SP, Muezzinoglu B et al: Pros-tatic involvement by transitional cell carcinoma inpatients with bladder cancer and its prognosticsignificance. Hum Pathol 2006; 37: 726.
21. Oliva IV, Smith SL, Chen Z et al: Urothelial car-cinoma of the bladder with transmural and directprostatic stromal invasion: does extent of stromalinvasion significantly impact patient outcome?
Hum Pathol 2011; 42: 51.