value-based insurance design in the medicare...
TRANSCRIPT

Value-Based Insurance Design in the Medicare Prescription Drug Benefit /An Analysis of Policy OptionsLisa Murphy / Jenny Carloss / Ruth E. Brown / Erika Heaton / Tanisha Carino, PhD / Avalere Health
A. Mark Fendrick, MD / Michael Chernew, PhD / Allison B. Rosen, MD, ScD / Center for Value-Based Insurance Design, University of Michigan

Takeda Pharmaceuticals North America, Inc., provided funding for this research. Avalere and the Univer-sity of Michigan Center for Value-Based Insurance Design maintained editorial control and the conclusions expressed herein are solely those of the authors.
March 2009 © Avalere Health LLC
Acknowledgements
The authors would like to thank Jan Berger of Health Intelligence Partners for helpful comments on the draft. We would also like to recognize Jenifer Martin, Bonnie Washington, Khoa Nguyen, and Margaret Nowak for their valuable contributions to the study.

TableofContents
2 ExecutiveSummary
5 Introduction
8 Methodology
10 ExploringVBIDintheMedicarePartDProgram •WhyIsVBIDNotaCommonOptionforMedicarePartDBeneficiariesToday?
15 OptionsforImplementingVBIDinMedicarePartD
17 AnalysisofOptions •PotentialSizeoftheMedicarePartDPopulationAffected
•CMSAuthoritytoChangePolicy
•AbilitytoImplementOptions
•PoliticalSupport
27 Conclusion
29 DiscussionandImplications
31 References
34 Appendix

va
lue
-ba
se
d in
su
ra
nc
e d
es
ign
in t
he
me
dic
ar
e P
re
sc
riP
tio
n b
en
ef
it
2
ExecutiveSummary
Value-basedinsurancedesign(VBID)hasemergedasapotentiallyviableapproachtopromote
healthcarevalue.VBIDabandonsthetraditionalapproachofuniformlyapplyingcostsharingto
healthservicesregardlessoftheireffectonapatient’shealth.Instead,VBIDtailorscostsharing
tothevaluethattheserviceprovidesthebeneficiaryintermsofhealthgainedperdollarspent.
Themoreclinicallybeneficialtheserviceistoapatient,thelowerthatindividual’scostsharing
fortheservice.
GiventhegrowingneedtoincreasethevalueofcaredeliveredintheMedicareprogramand
theexistingevidencesuggestingthatVBIDcangeneratecostsavingsandimprovehealthoutcomes,
there are clear opportunities to explore how to implement VBID within the Medicare program.
ThisanalysispresentsoptionsforadvancingaVBIDapproachwithinMedicare’sprescriptiondrug
benefit(PartD),andspecificallyfocusesondifferentialcostsharingforchronicallyillbeneficiaries
andhigh-valuemedicationsthattargetchronicconditions.
OuranalysisofthecurrentstructureoftheMedicarePartDprogramidentifiedfiveoptions
forimplementingVBIDinthePartDprogram:
Option 1: Reducecostsharingforspecificdrugsordrugclasses
Option 2: Exemptspecificdrugsordrugclassesfrom100percentcostsharinginthe
coveragegap
Option 3: Reducecostsharingforenrolleeswithchronicconditions
Option 4: Reducecostsharingforenrolleesparticipatinginmedicationtherapy
managementprograms(MTMPs)
Option 5: Reducecostsharingforchronicconditionspecialneedsplans(CC-SNPs)
Weevaluatedthefeasibilityofeachofthesepolicyoptionsbasedonfourcriteria:
1)potentialsizeoftheMedicarePartDpopulationaffected(usingdiabetestoestimatetherelative
sizeoftheaffectedpopulationforoptionsthattargetspecificchronicconditions,andhypoglycemics
andinsulinforoptionsthattargetparticulardrugs);2)theCentersforMedicare&Medicaid
Services’(CMS)authoritytochangepolicywithinexistingstatuteandregulation;3)requirements
forimplementation;and4)politicalsupport.
Based on our evaluation, it appears that several options could be successful vehicles
forVBIDinMedicarePartD.Inparticular,Option 1targetingspecificdrugsordrugclassesisan
optionthatCMScanimplementundercurrentlaw,andhasthepotentialtoaffectapproximately
6millionPartDenrolleeswithdiabetes.Infact,atleastonePartDplan,UnitedHealthcare’sSenior
Dimensions,beganexercisingthisoptionin2008.Option 2isalsopresentlyavailabletoplansand,
whileaffectingfewerbeneficiaries,ittargetsthosepatientswithhighannualdrugspendingwho
maybenefitmostfromthistypeofintervention.However,in2009onlythreedrug-onlyprescription
drugplans(PDPs)offergapcoverageforanybrand-namemedications.Asmoreevidenceofthe
benefits of VBID becomes available, policymakers may wish to pursue legislative changes that
wouldcreatenewincentivestoencouragemorePartDplanstoadoptthistypeofbenefit.
Option 5 is also feasible in the current policy environment. However, targeting VBID
toenrolleesinCC-SNPswillhavealimitedimpactontheMedicarepopulation–currentlyabout
268,000beneficiaries,only1percentofPartDenrollment.Duetothesmallscaleofthisoption’s
ex
ec
ut
ive
su
mm
ar
y
3
impact,Option 5maybeanidealfirststepinimplementingVBIDintheMedicarePartDprogram.
CMSandpolicymakerscouldencourageCC-SNPstoincorporateVBIDintotheirbenefitdesignsand
tocollectdataonadherenceandoutcomesfortheirenrollees.AsCC-SNPsgatherevidenceonthe
valueofVBIDinthispopulation,policymakerscouldconsideradditionalmethodsforincorporating
VBIDintotheMedicarePartDprogrammorebroadly.
Whilenotthehighest-rankedalternative,Option 4presentsaninterestingopportunity
todemonstratethevalueofVBID,despitepotentiallegislativechallengesinauthorizingsuchan
option.Sincethisoptionwouldrequiredifferencesinbenefitdesignforbeneficiarieswithinthe
sameplan,regulatoryorlegislativechangesmaybenecessarytoexemptVBIDfromexisting
PartDrequirementsthatplansmaynotdiscriminateagainstcertaingroupsofbeneficiariesand
thatallenrolleesinaplanmustbesubjecttoauniformbenefitdesign, includingcostsharing.
WhileMTMPspresentlyattractonlyasmallnumberofPartDenrollees—8percentofbeneficiaries
in2007—linkingVBIDtoMTMPparticipationcouldboostMTMPenrollment.Themovecouldalso
positivelyreinforceMTMPeffortstoimprovebeneficiaries’medicationadherencebyloweringor
removingfinancialbarriersforthoseservicesrecommendedbytheprogram.Policymakersmaybe
interestedinexaminingthisoptionfurthertodeterminetheimpactonhealthoutcomesandoverall
costsorsavings.
Finally,whileOption 3hasthepotentialtoreachalargenumberofPartDbeneficiariesand
couldbeacost-effectiveapproachtoimplementingVBID,thepotentiallegislativeandregulatory
changesrequiredappeartobebarrierstoitsimplementation,makingthisalessattractiveoption.
Over the course of the past two years, a diverse group of stakeholders across the
healthcareenterprisehasexpressedsupportforVBID.Becausethepercentageofhealthservices
withunequivocalclinicalevidencetosupporttheiruseunderVBIDprogramsissmallinrelation
to aggregate medical expenditures, even groups that might typically oppose such efforts as
“paternalistic”havebeenreceptivetothisidea.
Overall,politicalsupportforVBIDappearstobestrong,bipartisan,bicameral,andgrowing.
Thepolicychangesidentifiedinthispaperprovidearoadmapforseveralscenariosthatwilladvance
VBIDprinciplesineffortstoimprovehealthandcontaincosts.
Inbrief,thispaperillustratesthatCongress,CMS,andothershaveseveralviableoptions
for the Medicare program to implement VBID in Part D. Each of these options have their own
strengthsandweaknessesbasedonhowmanyMedicarebeneficiariesmaybenefitandhoweasily
theparticularVBIDapproachcouldbeimplementedbyCongress,CMS,andhealthplans.Eachof
thesefactors,moreover,isdynamicandourevaluationoftheseoptionsissensitivetochangesin
theMedicarePartDmarket.
AstheObamaAdministrationandmembersofCongressexplorehealthreformoptions,
itisimportantthattheynotonlyexamineoptionstoincreasecoveragefortheuninsured,butalso
optionstoimprovequalityandcontaincosts.VBIDsimultaneouslyaddressestheobjectivesofcost
containmentandqualityimprovementinthedeliveryofcarebypromoting“fiscallyresponsible,
clinicallysensitive”costsharinginordertomitigatethewell-documentedadverseclinicaloutcomes
associatedwiththecurrent,one-size-fits-allmedicalsystem.Medicareisanidealplacetoimplement
VBIDbecausebeneficiariesareatamuchhigherriskofadverseeventsduetonon-adherencethan
youngerpatientpopulationsandensuringaccesstonecessarycareisafundamentaltenetofthe
Medicareprogram.VBIDisavitaltoolthathasthepotentialtotransformMedicareintoamore
prudentpurchaserofhealthcareservicesthatmeetpatientneeds.

va
lue
-ba
se
d in
su
ra
nc
e d
es
ign
in t
he
me
dic
ar
e P
re
sc
riP
tio
n b
en
ef
it
4
VBIDisnotamechanismthatwillsolveourhealthcarecrisis.Technologicaladvanceswill
continuetogenerateupwardpressureoncostsandincreasinglystraintheabilityofindividualsand
theiremployerstoaffordsuchcoverage.Thatsaid,comparedtothestatusquoofescalatingcosts
andsuboptimalqualityofcare,theimplementationofVBIDprincipleswouldencouragetheuseof
high-valuecareandultimatelyproducebetterhealthatanylevelofhealthcareexpenditure.

int
ro
du
ct
ion
5
Introduction
TheUnitedStatesisonaquestforbettervalueinthehealthcaresystem.Researchdemonstrating
widevariationinhealthspendingandthequalityofcarepatientsreceivehasfueledpurchasersof
healthcaretoseekreformoptionsthatgenerateamorefavorablereturnoninvestment(i.e.,more
healthbenefit)fortheirhealthcaredollar.1 Infact,manypolicymakersviewhealthreformefforts
toexpandinsurancecoveragetoAmerica’sunder-oruninsuredwithoutpromotingamorevalue-
drivenhealthcaresystemasshortsightedandunsustainable.
Traditionally, when faced with rising healthcare costs, payers have turned to raising
patients’ share of costs for healthcare services. However, a growing body of evidence suggests
thatdoingsoreducespatientutilizationofbothunnecessaryandnecessaryhealthcareservices,
especiallyforpatientswithchronicconditionswhoalreadyfacehighout-of-pocketcosts.2Studies
havelinkedincreasesincostsharingwithloweruseofessentialclinicalservices,suchasprescription
druguseandvaluablepreventivescreening.3Asaresult,adversehealthoutcomesmayrequirecostly
emergencyroomvisitsandhospitalizations.4Consequently,employers,patients,andpolicymakers
seeksolutionstoreducethegrowthinhealthspendingwithoutsacrificingpatienthealth.
Thesearchforvalueandtheneedtoidentifycostcontainmentoptionsthatdonotresult
inpoorerhealthoutcomesforpatientsismostacuteintheMedicareprogram.Anestimated83
percentofMedicarebeneficiarieshaveatleastoneofthefollowingchronicconditions:diabetes,
arthritis,hypertension,asthma,orheartdisease.5Additionally,the23percentofbeneficiarieswith
5ormorechronicconditionsaccountfor68percentoftheprogram’sspending.6
Value-based insurance design (VBID) has emerged as a potentially viable approach to
promote healthcare value. VBID abandons the traditional approach of uniformly applying cost
sharingtohealthservicesregardlessoftheireffectonapatient’shealth.Instead,VBIDtailorscost
sharingtothevaluethattheserviceprovidesthepatientintermsofhealthgainedperdollarspent.7
Themoreclinicallybeneficialtheserviceistoapatient,thelowerthatindividual’scostsharingfor
theservice.
This innovativebenefitdesignaligns incentivesbyofferingadvantages tobothpayers
andpatients.Byreducingfinancialbarrierstoessentialclinicalservices,patientsaremorelikely
toadheretotheirprescribedtreatmentregimensandappropriatelymanagetheirhealth.Inreturn,
payers may reduce healthcare costs in the long run by helping enrollees prevent costly health
emergencies.8Todate,themajorityofVBIDeffortsthathavegeneratedpositiveresultshavefocused
onreducingcostsharingforprescriptiondrugsusedtotreatchronicconditions,mainlydiabetesand
1 FisherE,etal.“RegionalVariationsinHealthCareIntensityandPhysicianPerceptionsofQualityofCare.”Ann Intern Med144, no.9(2006):641-649.2 Braithwaite,etal.“LinkingCostSharingtoValue:AnUnrivaledYetUnrealizedPublicHealthOpportunity.”Ann Intern Med146 (2007):602-605.3 Newhouse,Joseph,InsuranceExperimentGroup.FreeforAll?LessonsfromtheRANDHealthInsuranceExperiment.Cambridge, MA:HarvardUniversityPress;1993.4 Thomas,CP.“HowPrescriptionDrugUseAffectsHealthCareUtilizationandSpendingbyOlderAmericans:AReviewofthe Literature.”AARPPublicPolicyInstitute(April2008).5 NeumannP,etal.“MedicarePrescriptionDrugBenefitProgressReport:Findingsfroma2006NationalSurveyofSeniors.”Health AffairsWebExclusive26.5(August21,2007):w630-w643.6 Anderson,Gerard.“MedicareandChronicConditions.”NEJM353,no.3(2005):305-309.7 ChernewME,etal.“Value-BasedInsuranceDesign:ByAbandoningtheArchaicPrinciplethatAllServicesMustCosttheSamefor AllPatients,WeCanMovetoaHigh-ValueHealthSystem.”Health Affairs26,no.2(2007):w195-w203.8 FendrickAM,etal.“Value-BasedInsuranceDesign:FiscallyResponsible,ClinicallySensitiveApproachtoMakingTheMostOf HealthDollars.”AJMC13.(June2007):325-327.

va
lue
-ba
se
d in
su
ra
nc
e d
es
ign
in t
he
me
dic
ar
e P
re
sc
riP
tio
n b
en
ef
it
6
hypertension.Thereductionsinout-of-pocketpaymentsforthesepatientshaveledtoimproved
medicationadherence,betterclinicaloutcomes,anddecreasedhealthcarecoststhroughaverted
hospitalizationsandemergencyroomvisits.15,16TheAppendixprovidesasummaryofrecentVBID
studiesondifferentialcostsharingfordrugsusedtotreatcertainchronicconditions.
GiventhegrowingneedtoincreasethevalueofcaredeliveredintheMedicareprogram
andtheexistingevidencesuggestingthatVBIDcanreducehealthcarecostsandimprovehealth
outcomes, there are clear opportunities to implement VBID within the Medicare program. This
analysiswillpresentoptionsforadvancingaVBIDapproachwithinMedicare’sprescriptiondrug
benefit(PartD),andspecificallyfocusesondifferentialcostsharingforchronicallyillbeneficiaries
andhigh-valuemedicationsthattargetchronicconditions.Asafollow-uptothisstudy,Avalere
HealthandtheUniversityofMichiganVBIDCenterarecollaboratingonasecondpaperthatwill
examinetheimpactofimplementingaVBIDapproachintheMedicarePartDprogram.
AlthoughthisanalysisfocusesontheapplicationofVBIDtochronicconditionmedications
coveredunderMedicarePartD,itisimportanttorecognizethatVBIDhasamuchbroaderapplication
VBIDinPracticeInpractice,therearetwogeneralapproachestoVBID.Thefirstapproachtargetsclinically
valuable treatments, tests, or procedures, such as chronic condition maintenance
medicationsorpreventivemammography,forreducedcostsharingforallenrollees.The
secondVBIDapproachtargetspatientswithspecificclinicaldiagnoses,suchasdiabetes,
andlowerscostsharingforthehigh-valueservicesnecessarytomanagetheseconditions,
suchasinsulinoreyecare.9AlthoughtheapplicationofbothapproachestoVBIDispossible
foranymedicalservice,todatemosteffortshavefocusedonreducingcostsharingfor
prescriptiondrugsusedtotreatchronicconditions,mainlydiabetesandhypertension,
withtheintentofimprovingadherenceanddiseasemanagement.
Employers,includingPitneyBowes,Marriott,andtheUniversityofMichigan,have
championedVBIDinitiativesthatreducecostsharingforchronicconditionmedications
to encourage high-risk patients to manage their disease better 10,11,12,13 Pitney Bowes, for
example, reduced cost sharing for drugs commonly prescribed for diabetes, asthma,
andhypertensionandreportedfavorableresults. In2009,UnitedHealthcarelauncheda
VBID-typehealthplanwithcopaymentreliefspecificallyforbeneficiarieswithdiabetes
mellitus.Foremployeeswithdiabetes,thereductionsincostsharingincreasedmedication
adherence by 20 percent and decreased diabetes-related medical costs by 6 percent.14
GiventhepositiveoutcomesVBIDhasgeneratedfortheseemployersandothers,many
advocatesbelievethebroaderuseofVBIDwouldbenefitthehealthcaresystem.
9 Chernew,Health Affairs.10 CranorC.W.,etal.“TheAshevilleProject:Long-TermClinicalandEconomicOutcomesofaCommunityPharmacyDiabetesCare Program,” JAPA43,no.2(2003):173-184.11 Berger,J.“EconomicandClinicalImpactofInnovativePharmacyBenefitDesignsintheManagementofDiabetesPharmacotherapy.” AJMC13,no.2(2007):S55-58.12 SokolMC,etal.“ImpactofMedicationAdherenceonHospitalizationRiskandHealthcareCost.”Med Care 43,no.6(2005):521-530.13 ResultsfromM-Healthy:FocusonDiabetestwo-yearpilotprogram(unpublishedstudydatareportedinDrug Benefit News) December12,2008.14 Berger,AJMC.15 Sokol,Med Care.16 Berger,AJMC.

thandifferentialcostsharing.TheconceptofVBIDispartofthelargerparadigmshifttovalue-based
purchasing,whichseekstoalignincentiveswithevidence-basedhealthcaredelivery.
ThepotentialpromiseofVBIDintheMedicarePartDprogramissignificant.Onaverage,
thispopulationtakesatleastfiveprescriptiondrugsaday.17However,despitethecentralrolethat
prescriptiondrugsplayinmanagingchronicconditions,lackofadherencetomedicationregimens
isaseriousproblemamongtheMedicarepopulation.18Forexample,anationalsurveyofMedicare
beneficiariesfoundthatnearly20percentofPartDenrolleeseitherdidnotfillaprescriptionor
delayed filling a prescription because of cost.19 Poorly controlled chronic conditions are also
associatedwithhighmedicalcosts.Researchershavefoundthatimprovingmedicationadherence
cancutmedicalcostsinhalfforpatientswithdiabetesandhighcholesterol.20Studiesthathave
examinedthe impactof loweringoreliminatingcostsharingforoutpatientdrugsforMedicare
beneficiaries with chronic conditions report cost savings and improved health outcomes.21 For
example,onestudyfoundthatprovidingfullcoverageofACEinhibitorsforMedicarebeneficiaries
withdiabetescouldgeneratesavingsof$1,606perbeneficiaryperyear.22
PoliticalsupportforbroaderapplicationofVBIDisgainingmomentum.Atthefederallevel,
CongressandsupportagenciessuchastheMedicarePaymentAdvisoryCommission(MedPAC)are
exploringhowtoincorporateVBIDintofederalprograms.Sen.MaxBaucus(D-MT)supportedthe
conceptinhis“CalltoAction”whitepaperonhealthcarereform;23andSen.DebbieStabenow(D-MI)
andRep.JohnDingell(D-MI)hostedaFebruary2009congressionalbriefingonVBID.In2007,MedPAC
discussedimplementingVBIDwithinMedicare.24Mostrecently,abipartisangroupofU.S.Senators
isdraftinglegislationtoadvanceVBIDintheDepartmentofVeteransAffairs(VA).Thispopulationis
particularlywell-suitedtoVBIDbecausetheVA’suseofanelectronichealthrecordssystemprovides
thestructurenecessaryforefficientimplementation;theimpactofreducingcopaymentscanbe
easilytrackedandlinkedtoapatient’smedicaldiagnosis.Stategovernmentsarealsobeginning
toincorporateVBIDprinciplesintotheirbenefitdesignsasawaytopromotehealthybehavior.For
example,MichiganisworkingtointegrateVBIDprinciplesintoitsMedicaidprogrambywaiving
copaymentsoncertainmaintenancedrugsforchronicdiseases.25
int
ro
du
ct
ion
7
17 WilsonI,etal.“Physician-PatientCommunicationAboutPrescriptionMedicationNonadherence:A50-StateStudyofAmerica’s Seniors.” J of Gen Intern Med22,no.1(2007):6-12.18 Thomas,AARP Public Policy Institute.19 Neumann,Health Affairs.20 Sokol,Med Carep.525.21 Thomas,AARP Public Policy Institute.22 RosenAB,etal.”Cost-effectivenessofFullMedicareCoverageofAngiotensin-ConvertingEnzymeInhibitorsforBeneficiarieswith Diabetes.”Ann Intern Med143(2005):89-99.23 Baucus,Sen.Max.“CalltoAction:HealthReform2009.”(November12,2008)http://finance.senate.gov/healthreform2009/home. html(accessedJanuary5,2009).24 MedPACMeeting.October3,2007.http://www.medpac.gov/transcripts/1003-04medpac.final.pdf(accessedJanuary5,2009).25 “PublicProgramsareUsingIncentivestoPromoteHealthyBehavior.”TheCommonwealthFund.(October11,2007).http://www. commonwealthfund.org/innovations/innovations_show.htm?doc_id=676105

va
lue
-ba
se
d in
su
ra
nc
e d
es
ign
in t
he
me
dic
ar
e P
re
sc
riP
tio
n b
en
ef
it
8
Methodology
AvalereHealthandtheUniversityofMichiganVBIDCenterconductedthisanalysisfromDecember
2008 through February 2009. We examined published studies on VBID, policy documents, and
otherpubliclyavailablematerialstoinformthedevelopmentofoptionsandtheanalysis.Wethen
identifiedpolicyoptionsforincorporatingVBIDintotheMedicarePartDbenefitbasedonexamples
of employer-sponsored VBID programs, policy options considered for implementation in the
MedicarePartDprogram,andourcollectiveunderstandingofVBIDandMedicarepolicies.
Foreachpolicyoptionidentified,weassessedthesizeoftheMedicarepopulationaffected;
determinedtheCentersforMedicare&MedicaidServices’(CMS)authoritytoauthorizetheoption
withinexistingstatutesandregulations,andwhetherlegislativeorregulatoryactionisrequired;
requirementsforimplementation;andpoliticalsupport.Wethenrankedeachoption’simpactand
feasibilityaccordingtothescaledescribedinTable1.
Table 1. rating scale for options analysis
0 greatest Potential most feasible
Gmoderate Potential moderate feasibility
@ lowest Potential least feasible
PotentialtoImproveMedicare
SizeofMedicarePopulationAffected
Largestpopulationrelativetootheroptionsconsidered
Mid-sizepopulationrelativetootheroptionsconsidered
Smallestpopulationrelativetootheroptionsconsidered
Feasibility
CMSAuthoritytoChangePolicy
Maybeauthorizedundercurrentlawandregulation
MayrequirechangeinCMSregulationsorsub-regulatoryguidance
Mayrequirelegislativechangetoauthorizeoption
AbilitytoImplementPolicy
RequiresminorchangestoCMSandplanoperations
RequiresmoderatechangestoCMSandplanoperations
RequiresmajorchangestoCMSandplanoperations
PoliticalSupport
Highlikelihoodofpoliticalsupport;significantadvantagestopolicychange
Moderatelikelihoodofpoliticalsupport;someadvantagesandob-staclestopolicychange
Lowlikelihoodofpoliticalsupport;significantobstaclestopolicychange
However, it is important to note that this analysis does not seek to assess the value
of medications or distinguish between low- and high-value treatments. These are important
considerationswhenimplementingVBID,butbeyondthescopeofthispaper.Rather,ourgoalis
toidentifypotentialVBIDpolicyoptionswithintheMedicareprogram;evaluateeachoption;and
determinethemostfeasibleoptionswiththegreatestpotentialforimpact.
Wedescribeeachofouroptionsastargetingchronicconditions,butdonotattemptto
definewhichconditionsorclassesofdrugsshouldbethefocusofaVBIDapproachinMedicare.
However,weusediabetesthroughoutthepaperasanexampleofhowanoption’simplementation
mightlook.WeselecteddiabetesduetoitsappearanceintheVBIDliteratureasoneofthemost
commonlystudiedconditions,aswellasthepotentialforpayersandbeneficiariestoseeshort-term
positiveoutcomesandpossiblesavingsforVBIDtargetingdiabetescomparedtootherconditions.
DiabetesisoneofthemostcommonchronicconditionsamongMedicarebeneficiariesandone

me
th
od
olo
gy
9
of the most costly, accounting for $11,800 in annual program costs for the average beneficiary
with diabetes.26 Additionally, policymakers have highlighted diabetes as a priority condition for
theMedicareprogramthroughrecentchangesaddingcoverageofdiabetesscreeningtestsand
specifyingdiabetesasoneofalimitednumberofchronicconditionsspecialneedsplans(SNPs)may
target.27,28Donotinterpretouruseofdiabetesthroughoutthispaperassinglingoutthediseaseas
theonlyconditionorclassofdrugsthatVBIDcouldtarget.
Atthesametime,becauseweusediabetesasanexampleinaprimarilyqualitativeanalysis,
wehavenotdefinedthespecificmedicationsthatplanscouldseekoutinaVBIDapproachdesigned
arounddiabetes.Forexample,aplanimplementingVBIDforenrolleeswithdiabetescouldtakea
narrowapproachbyreducingcostsharingfororalhypoglycemicmedicationsandinsulinonly,while
abroaderapproachcouldincludecardiacmedications,antidepressants,orothermedicationsoften
utilizedbydiabetics.Forthepurposesofouranalysis,wehaveusedthenarrowerdefinition,but
PartDplansorpolicymakersinterestedindefiningVBIDmustdecidehownarrowlyorbroadlyto
approachtheissue.
Finally,while thispaper focuseson theVBIDmodelof reducedcostsharing, thereare
manyotherapproachespossibletoimprovebeneficiaries’adherenceandhealthoutcomesinPart
D.Pairingprogramsthatoffercounselingwithpharmacistsorotherchronicdiseasemanagement
initiativeswithVBID’slowercostsharingcouldhaveanevengreaterimpactonbeneficiaryhealth.
26 Tan,Ronnie.“CharacteristicsofMedicareBeneficiarieswithChronicConditions.”Presentationat2007AcademyHealth,June4, 2007.http://www.academyhealth.org/2007/monday/asia1/tanr.pdf27 CMS,“DiabetesScreening:Overview.”http://www.cms.hhs.gov/DiabetesScreening/28 CMS,SpecialNeedsPlanChronicConditionPanel,FinalReport.November12,2008.http://www.cms.hhs.gov/specialneedsplans/

va
lue
-ba
se
d in
su
ra
nc
e d
es
ign
in t
he
me
dic
ar
e P
re
sc
riP
tio
n b
en
ef
it
10
ExploringVBIDintheMedicarePartDProgram
Medicare’s prescription drug benefit provides coverage of most outpatient drugs for Medicare
beneficiaries.UnlikeotherpartsofMedicare,PartDdrugcoverageisonlyavailablethroughprivate
insuranceplans.EveryonecoveredbyMedicare isentitledto receiveprescriptiondrugcoverage,
althoughenrollmentisvoluntary.
BeneficiarieswhochoosetoobtainPartDcoveragehavetwooptions—enrollinastandalone
prescription drug plan (PDP) that offers drug-only coverage or select a Medicare Advantage
prescriptiondrugplan(MA-PDplan),providingcoverageofbothmedicalanddrugbenefits.Asof
January2009,morebeneficiarieswereenrolledinPDPsthaninMA-PDplans—17.4millionversus8.8
million(Figure1).29
Figure 1.MedicarePartDEnrollment,2009
Mostbeneficiarieshaveaccess toa largeselectionofPartDplans thatvarywidely in
coverage,premiums,andcostsharing,butallplansapprovedbyMedicaremustoffer,ataminimum,
astandardlevelofcoverage(Figure2).Establishmentofthecoverageisdoneonanannualbasis
andincludesaninitiallevelofprescriptiondrugcoverageaswellasprotectionforenrolleeswith
extraordinarily high drug costs, also known as “catastrophic coverage.” In between the initial
coverageperiodandcatastrophiccoverage,enrolleesmayexperienceagapincoveragewherethey
arerequiredtopayfortheentirecostoftheirprescriptiondrugsoutofpocket.Thisisknownasthe
coveragegapor“doughnuthole.”
TotalEnrolledinPartD=26.2million
MA-PD Plans
PDPs
PDPs67%
MA-PDPlans33%
Source:AvalereHealthanalysisofCMSdatafromJanuary2009.
29 AvalereHealthanalysisofCMSdatafromJanuary2009.

ex
Plo
rin
g v
bid
in t
he
me
dic
ar
e P
ar
t d
Pr
og
ra
m
11
30 CMS,PrescriptionDrugBenefitManual,Chapter6,Section30.2.7.http://www.cms.hhs.gov/PrescriptionDrugCovContra/Down loads/R2PDB.pdf31 ThisformularyrequirementisbasedonsimilarlanguageinthePartDstatute.SocialSecurityAct,Section1860D-11(e)(2)(D)(i).
Figure 2.MedicarePartDStandardBenefitDesign,2009
MostprivateinsurerswhoofferPartDplansusetheflexibilityallowedinthelawtodeviate
fromthestandardbenefitdesign,buteachplanmustmeettheminimumstandardsforPartD
coverageestablishedinlegislationandregulation.Onesuchrequirementstatesthatplanofferings
mustbe“actuariallyequivalent”to,orbetterthan,thestandardbenefitdesign.Mostplanschoose
tocreateanalternativebenefitdesignbyreducingthedeductible,creatingdifferentcost-sharing
tiersfordrugsontheplan’sformulary,orprovidingsupplementalcoverageforsomedrugsinthe
coverage gap. Because of the actuarial equivalence requirement, reducing cost sharing in one
partofthebenefitmayrequireplanstoincreasecostsinotherpartsofthebenefit.CMS,which
overseesPartDimplementation,reviewsplanbenefitdesignsannuallytoensurecompliancewith
allprogramstandards.OnlyplansthathavemetthesestandardsgainpermissiontoofferthePart
Dbenefit.
Similarly,whileprivateplanshavesomelatitudeindeterminingwhichdrugstocoveron
theirplan’sformularyandatwhatcost-sharinglevels,CMSreviewseachPartDplan’sformulary
coverageannually.CMS’formularyreviewprocessincludesanexaminationofthedrugsincluded
ontheplan’sformularyaswellasthecost-sharingtiersonwhichthedrugsareplacedandany
utilizationmanagementrequirements.Aspartofthisreview,CMSexaminestheformulary’scost-
sharingtiers“toensurethattheformularydoesnotsubstantiallydiscourageenrollmentofcertain
beneficiaries.”30,31Ifaplanfailsthistest,theplanmustreviseitsformularycoverageoritwillnotbe
approvedtoofferaPartDplan.
ThereareanumberofinitiativesinPartDfocusedonpromotingbettermedicationuse
forbeneficiarieswithchronicconditions,muchlikethegoalofVBID.Themostprominentinclude
medication therapymanagementprograms (MTMPs)andSNPs.TheMedicarePrescriptionDrug
ImprovementandModernizationAct(MMA)of2003establishedMTMPstooptimizetherapeutic
outcomesofPartDenrolleeswithmultiplechronicconditionsthroughmedicationmanagement.
■ BeneficiaryCostShare■Plan’sCoverage
CatastrophicCoverage
NoCoverage(“doughnuthole”)
PartialCoverage
Deductible
5%coinsurance
100%costsharing
$6,154*
$2,700
$295
*Equivalentto$4,350inout-of-pocketspending
25%coinsurance

va
lue
-ba
se
d in
su
ra
nc
e d
es
ign
in t
he
me
dic
ar
e P
re
sc
riP
tio
n b
en
ef
it
12
BothPDPsandmostMA-PDplansarerequiredtohaveanMTMPandmusttargethigh-riskpatients
whohavemultiplechronicconditions,takemultiplePartDdrugs,andarelikelytoincurmorethan
$4,000inannualdrugcosts.32Becauseplanshavewidelatitudeindefiningeligibilitycriteriaand
servicesoffered,currentMTMPservicesvarywidelybyplan.MTMPservicescouldincludemedication
reviewsandcounselingservicesthrougheducationalmailings,directphonecalls,and/orface-to-
faceinteractionswithpharmacists.
AlsoinstitutedbytheMMA,SNPsareatypeofMA-PDplandesignedtomeettheneedsof
Medicaresubpopulationsthatcouldbenefitfromspecializedcare.TheMMAgrantedSNPscertain
exceptionsrelativetootherMA-PDplanssuchastheabilityto limitenrollmenttobeneficiaries
whomeetoneofthreecriteria:“dualeligibles”(thosewhoqualifyforbothMedicareandMedicaid),
institutionalized beneficiaries, and those with severe or disabling chronic conditions. SNPs are
requiredtotailortheirmedicalanddrugbenefitstomeettheneedsofthetargetpopulation,ideally
improvingthequalityofcareforthoseenrolleesandloweringoverallcosts.SNPenrollmenthas
grownrapidlysincethebeginningoftheprogram,from603,000enrolleesin200633toalmost1.3
millionin2008.34
WhyIsVBIDNotaCommonOptionforMedicarePartDBeneficiariesToday?WhilePartDplanshavetheflexibilitytodesigntheirbenefitsandformularycoveragetolowercost
sharingforcertainhigh-valuedrugs,fewappeartodoso.However,thereareearlyindicationsthat
plansmaybe interested inVBID.SeniorDimensions,anMA-PDplanoffered inNevadathrough
a subsidiary of UnitedHealthcare, announced in late 2008 that it was reducing copayments for
selectedmaintenancemedicationsfordiabetes,chronicobstructivepulmonarydisease,asthma,
highbloodpressure,andseizures.35Prescriptionsforselectedbrand-namedrugsthatpreviouslycost
$20to$30sawcopaymentsreducedto$3to$5,similartochargesforgenericdrugs.Additionally,
somechronicconditionSNPs(CC-SNPs)maybecharginglowercostsharingfordrugstotreatthe
conditionstheytarget.
Despitetheseexamples,VBIDisnotyetprevalentinthePartDprogram.Inthissection,
wediscussseveralreasonswhymoreplansarenotimplementingVBIDandsuggestoptionsfor
mitigatinganyconcerns.Overall,planconcernsarelikelytofocusontheeffectsofVBIDonplan
enrollmentandthepotentialreturnoninvestment.Theseissuesare interrelated,astherelative
healthofaplan’senrolleescanaffecttheplan’scosts.
First,incorporatingVBIDinthePartDmarketwhereplanscompeteforenrolleesmayraise
concernsaboutadverseselection.36Amoregenerousbenefitdesign,suchasonethateliminatesor
reducescostsharingfortargetedbeneficiariesorselecteddrugs,islikelytoattractnewbeneficiaries
withthetargetedchronicconditionorwhotakethetargeteddrug.Attractingsickerbeneficiaries
mayincreaseaplan’scostsandultimatelyresultinhigherpremiumsforalltheplan’senrollees.
(SNPsmaybelessconcernedaboutadverseselectionthanotherMA-PDplansorPDPs,duetotheir
32 InJanuary2009,CMSreleasedguidanceproposingchangestoMTMPeligibilitycriteriaandrequiredMTMservices,beginning inplanyear2010.However,theagencyhassincewithdrawnthatdocumentforfurtherreview.Itisunclearatthistimehow MTMPeligibility,enrollment,andservicesmightchangeinfutureyears.CMS,“MedicarePartDMedicationTherapyManagement Programs:2008FactSheet.”March19,2008.http://www.cms.hhs.gov/PrescriptionDrugCovContra/Downloads/MTMFactSheet.pdf33 CMS,“2006SpecialNeedsPlan(SNP)EnrollmentReportbySNPType.”http://www.cms.hhs.gov/SpecialNeedsPlans/Downloads/ 06SNP_Enrollment_by_Type11-9-06.pdf34 CMS,MonthlySNPReports,September2008.35 “SeniorDimensionsLowersPrescriptionDrugCo-PaymentsonManyWidelyUsedBrand-NameMaintenanceDrugs.”Business Wire,September24,2008.36 Chernew,Health Affairs,w199-200.

ex
Plo
rin
g v
bid
in t
he
me
dic
ar
e P
ar
t d
Pr
og
ra
m
13
uniquestructurethatalreadytargetsspecific,high-riskpopulations.)Althoughtherelativehealth
statusofeachplan’senrolleesformpartofthebasisforPartDplanpayments,therisk-adjusted
paymentsdonotfullymitigatetheriskofadverseselection.EvenintheshorthistoryofthePart
Dprogram,severalplansponsorshaveeliminatedmoregenerousbenefitssuchasgapcoverage
becauseofadverseselection.Revisionstothecurrentrisk-adjustmentsystemoradditionalrisk-
adjustedpaymentsmayencouragemorewidespreadadoptionofVBIDinthePartDprogram.
AnotherwaytoreducetheriskofadverseselectionistorequirethatallPartDplansoffer
thesamecoverageforthetargetedbeneficiariesordrugs.Ifallplanscoveredthetargetedconditions
ordrugsequally,noindividualplanwouldbeatgreaterriskforattractinghigh-riskbeneficiaries
thananyotherplan.However, thisstandardizedapproachmayhaveunintendedconsequences,
andshouldbecarefullyconsidered.RequirementsthatstandardizePartDplans’coverageofcertain
drugs limitsplans’abilitytonegotiatewithpharmaceuticalmanufacturersfor lowerprices,and
couldincreaseoverallcoststothePartDprogram.Additionally,limitsonplanflexibilityinoffering
thebenefitcouldnegativelyaffectplans’interestinparticipatinginthePartDprogram.
Second,plansmaybeconcernedthatreducingcostsharingforsomebeneficiariesordrugs
mayrequireplanstoincreasecostsharingforotherdrugsorraisepremiumsinordertoremain
actuariallyequivalenttothestandardPartDbenefit.Plansmaybehesitantto raisepremiums,
however,andrisklosingenrollmentifmembersleavetheplanforother,lower-premiumoptions.
TheriskoflosingmarketshareinthecompetitivePartDmarketcouldbeadisincentiveforplansto
implementVBID.
Third, standalone PDPs, which offer drug benefits only, currently lack the financial
incentivestoincorporateVBIDintotheirbenefitdesigns.Reducingcostsharingfordrugswillnot
onlyincreasedrugcosts,asnotedabove,butprovidesnoreturnoninvestmentfortheseplans.While
MA-PDplans,whichcoverbothdrugsandmedicalservices,maygainsomereturnoninvestment
fromVBIDthroughreducedhospitalizationsoremergencycare,PDPsarenotabletorealizeoffsets
innon-drugspendingassociatedwithmoredrugadherence.ToencouragePDPstoadoptVBID,
significantincentiveswouldberequired.
MA-PDplansarelikelytohavefewerconcernsabouthigherdrugcoststhanPDPs,because
MA-PD plans could realize savings in the medical benefit if enrollees remain healthier because
of improved medication adherence. Though some studies have demonstrated that medication
adherence lowerstotalmedicalcosts,38 there is littleresearchspecificallymeasuringthe impact
ofVBIDonmedicationadherenceandoutcomesintheMedicarepopulation.Duetothislackof
researchinthePartDpopulation,MA-PDplansmaybereluctanttoadoptVBID,absentadditional
incentives.MA-PDplansconvincedofthepotentialforVBIDinthispopulationmaybeconcerned
thatanypotentialcostsavingsavailablefrombettermedicationadherencewouldaccruetoanother
planiftheenrolleechoosestoswitchplans,asPartDbeneficiariesareallowedtodoeachyear.39This
concernmaynotbeasgreatinPartDasinthecommercialmarket,becauseonlyasmallpercentage
ofPartDbeneficiariesswitchplanseachyear.40However,MA-PDplansmayneedtobereassured
37 “SierratoIncurLossonEnhancedMedicarePartDPrescriptionDrugProductOffering.”Business Wire.http://findarticles.com/p/ articles/mi_m0EIN/is_2007_Feb_27/ai_n2730698738 Thomas,AARPPublicPolicyInstitute.39CMSallowsdual-eligiblebeneficiariestochangeplansmonthly,andhasdesignatedspecialenrollmentperiodstoallowother subgroupsofbeneficiariestochangeplansthroughouttheyear.40About6percentofbeneficiarieschangedPartDplansin2008(excludinglow-incomebeneficiaries).CMSPressRelease,“Medicare PrescriptionDrugBenefit’sProjectedCostsContinuetoDrop.”January31,2008.

va
lue
-ba
se
d in
su
ra
nc
e d
es
ign
in t
he
me
dic
ar
e P
re
sc
riP
tio
n b
en
ef
it
14
thattheywillbenefitfromtheirinvestmentinVBID,potentiallythroughincentivessimilartothose
offeredtoPDPs.
Incentivestoplansfor incorporatingVBID intotheirbenefitdesignscouldtakeseveral
forms.FinancialincentiveswouldprovideadditionalpaymentstoplansthatincorporateVBID,
to offset the potential costs of reducing copays. Legislation may be required to offer financial
incentives,orCMScouldpursuethisapproachusingitsdemonstrationauthority.Additionalrisk-
adjustedpaymentsorfinancialincentivesforallPartDplansbasedonenrollees’adherencetodrug
regimenscouldencouragetheuseofVBIDintheirbenefitdesigns.
CMScouldalsooffernon-financial incentives toencouragegreaterVBIDadoption.For
example,CMScurrentlyusesastarratingsystemonitsMedicarePrescriptionDrugPlanFinderto
ratePartDplans’performanceonanumberofmeasures.CMScouldaddinformationtodenote
whichplansincludeVBIDintheirbenefitdesigns.CMScouldalsochangeitsPartDmarketingrules
tohighlighttheuseofVBID.NewmarketingrulesallowingplanstodiscusstheiruseofVBIDasa
differentiatorfromotherplans,orallowingpharmaciststoeducatebeneficiariesonplansusing
VBID, could provide plans a marketing advantage that may increase enrollment, encouraging
theuseofVBIDinPartDbenefits.However,marketingbasedonVBIDcouldexacerbateadverse
selectionconcerns.Thebestcourseistoconsiderbothissuesintandem.Finally,CMScouldoffer
plans additional flexibility on other Part D requirements, such as the six protected classes, in
exchangeforincorporatingVBIDintotheirbenefitdesigns.Inanyincentiveprogramofferedsolely
toplansincorporatingVBID,CongressorCMSwouldhavetoestablishclearstandardsdefiningVBID
approachesthatwouldqualifyfortheincentives.

oP
tio
ns
fo
r im
Pl
em
en
tin
g v
bid
in m
ed
ica
re
Pa
rt
d
15
OptionsforImplementingVBIDinMedicarePartD
WhiledesigninganincentiveprogramtoencouragePartDplanstoadoptVBIDwillbeanimportant
task for policymakers, the first step toward more widespread VBID adoption is to identify how
planscouldintegrateaVBIDapproachintotheirbenefitdesigns.Ingeneral,planscanemployVBID
bytargetingcertainpopulationsor identifyingparticularmedications–thetwomostcommon
approaches for implementing VBID in the private sector. Our analysis of the Medicare Part D
program’sstructureidentifiedfiveoptionsdiscussedbelowandinTable2.
Table 2. summary of vbid Policy options in medicare Part d
PolicyOptions Description
1.ReduceCostSharingforSpecificDrugsorDrugClasses
Lowornocostsharingforhigh-valuedrugswouldencourageadherenceamongallenrolleeswhomaybenefitfromadrug,regardlessoftheirchronicconditiondiagnosis
2.ExemptSpecificDrugsorDrugClassesfrom100%CostSharingintheCoverageGap
Becauseadherencemaydeclineasenrolleesareexposedtohighcostsharing,thisoptionwouldofferprotectionwhencostsaregenerallythegreatest–duringthecoveragegap
3.ReduceCostSharingforEnrolleeswithChronicConditions
Targetingenrolleeswithaspecificchroniccondi-tionforlowercostsharing–foralldrugsorjustthosethattreattheparticularcondition–wouldlessentheout-of-pocketburdenassociatedwiththatchroniccondition
4.ReduceCostSharingforEnrolleesParticipatinginMTMPs
EnrolleesparticipatinginPartD’smedicationmanagementprogramwouldbenefitfromreducedcostsharingforspecificdrugs,inaddi-tiontootherpatientoutreachandcounselingonmedicationuse
5.ReduceCostSharingforCC-SNPEnrolleesBasedonthePlan’sTargetCondition
SNPstargetingparticularchronicconditionscouldreducecostsharingfordrugsthattreatthetargetconditionaspartofanoverallmodelofcareaimedatmanagingthechroniccondition
Option 1: reduce cost sharing for specific drugs or drug classes. PartDplans—bothPDPsand
MA-PDplans—couldlowercostsharingformedicationswithhighclinicalvaluerelativetoother
drugsontheformulary.Thisapproachwouldbenefitallenrolleeswhotakethetargeteddrugs,
regardlessofdiagnosis.Additionally,planscouldtargetanyhigh-valuedrugsordrugclassesand
wouldnotnecessarilychoosedrugstotreatasinglechroniccondition.Planscouldplacethesehigh-
valuedrugsonanexistingformularytierthatensuresminimalcostsharing—suchasalow-costtier
traditionallyreservedforgenericdrugs—orcreateaseparatetierthatwouldbelimitedtothehigh-
valuedrugsidentifiedbytheplan.

va
lue
-ba
se
d in
su
ra
nc
e d
es
ign
in t
he
me
dic
ar
e P
re
sc
riP
tio
n b
en
ef
it
16
Option 2: exempt specific drugs or drug classes from 100 percent cost sharing in the coverage gap.
Planscouldprovidecoverageforhigh-valuedrugsduringthecoveragegap.Thisoptioncouldsimply
extendcoverageofthesehigh-valuedrugsthroughthecoveragegaporworkincombinationwith
Option1toofferlowcostsharingforthetargeteddrugsthroughoutthebenefityear.
Option 3: reduce cost sharing for enrollees with chronic conditions.Planscouldtargetenrollees
diagnosedwithcertainchronicconditions,andlowercostsharingforhigh-valuedrugsthattreat
theparticularconditionforthoseenrollees.Avariationofthisoptionistolowercostsharingon
alldrugsforenrolleeswiththetargetedchronicconditions.Inordertodothis,planswouldhave
to implement processes for identifying qualified patients based on diagnosis. Unlike Option 1,
lowcostsharing—eitherforhigh-valuedrugsorforalldrugs—wouldbeavailableonlytopatients
diagnosedwithcertainconditionsidentifiedbyCMSortheplan.Thoughthisoptionmayaffect
fewerbeneficiariesthanOption1, itmayreduceimplementationcostsduetoitsmoretargeted
approach. Forexample, reducingcost sharing forACE inhibitors forpatientswithdiabetesmay
allow this population to control their chronic condition better than reduced cost sharing for
diabetesmedicationsalone,41andwouldbelesscostlyforplansthanreducingcostsharingforall
patientstakingACEinhibitors.TheabilitytomoreappropriatelytargetinterventionsusingthisVBID
approachmaybemorecost-effectiveandcouldleadtobetteroutcomesthanoptionsthattarget
specificdrugsordrugclasses.42
Option 4:reduce cost sharing for enrollees participating in MTMPs. Thisoptionisanalternative
totargetingenrolleesforVBIDbyinsteadidentifyingpatientswhoareparticipatinginanMTMP.
MTMPenrolleeswouldhaveaccesstolowercostsharingforhigh-valuemedicationstreatingtheir
chronic conditions, in addition to receiving MTMP-related services, a combination that has the
potentialtoimproveadherenceandoutcomessignificantly.
Option 5:reduce cost sharing for CC-SNP enrollees based on the CC-SNP’s target condition.
WhilethepreviousfourapproachestoVBIDcanworkinPDPsorMA-PDplans,CC-SNPs—aunique
typeofMA-PDplan—haveaparticularadvantageforusingVBID:CC-SNPsalreadytargetenrollment
toMedicarebeneficiarieswithparticularchronicconditions. InOption5,CC-SNPswouldreduce
oreliminatecostsharingforspecificdrugsordrugclassesthattreattheplan’stargetedchronic
conditions.
41 Rosen,AnnIntern Med.42 Chernew,Health Affairs.

an
aly
sis
of
oP
tio
ns
17
AnalysisofOptions
Weevaluatedthefeasibilityofeachofourfivepolicyoptionsbasedonfourcriteria:1)potential
sizeoftheMedicarePartDpopulationaffected;2)CMS’authoritytochangepolicywithinexisting
statuteandregulation;3)requirementsforimplementation;and4)politicalsupport.
PotentialSizeoftheMedicarePartDPopulationAffectedToassesseachoption’spotentialimpactontheMedicarePartDprogram,weestimatedthenumber
ofpeopleaffectedandthepotentialchangeinbeneficiaries’healthoutcomes.Forthepurposesof
thisanalysis,wemakecertainassumptionsbasedoncurrentliteratureandresearchonVBIDand
chronicconditions.Foroptionsthattargetspecificchronicconditions,weusediabetestoestimate
the relative size of the affected population. For options that target specific drugs, we use oral
hypoglycemicsandinsulinasexamples,becauseonlydiabeticsusetheseclassesofdrugs.However,
diabeticsmayuseotherclassesofdrugstomanagetheirconditionandcomorbidities,andplans
targetingspecificdrugsthroughVBIDarenot limitedtodrugsusedtotreatasinglecondition.
Whileallof theoptionscanapplytoamuchbroader rangeofchronicconditionsordrugs, the
selectionofasingleconditionconveysasenseofthemagnitudeoftheimpactanoptioncouldhave
ifapplieduniformlyinthePartDprogram.(Foradditionalinformationonwhywefocusondiabetes,
seeSectionII,Methodology.)
Additionally,toassessthefullpotentialofVBIDwithinMedicarePartD,weassumethat
allPartDplanstakeadvantageofthisopportunity.Finally,webaseourestimatesoncurrentPartD
marketandenrollmenttrends.Dramaticchangesinplanofferingsorbeneficiaryenrollmentcould
altercertainoutcomesofthisanalysis.Theseassumptionsallowforillustrationoftheimpactofa
VBIDapproachonbeneficiarieswithdiabetes,butmaynotreflecttheactualnumberofbeneficiaries
affectedifotherconditionsordrugsgainselectionforlowercostsharing.
ItisalsoimportanttonotethatreducedcostsharingthroughVBIDwillhavealimited
impactonbeneficiarieswhoqualifyforthelow-incomesubsidy(LIS).LIS-eligiblebeneficiariespaya
standardcopaymentamountforPartDdrugs,unlesstheirplan’scostsharingisbelowthatamount.
Forexample,LIS-eligiblebeneficiariesin2009areresponsibleforcostsharingofnogreaterthan
$2.40forgenericdrugsand$6forbrand-namemedications;43ifaplanchargeslowercopayments
thantheLISamount,thebeneficiarypaysthelowercopayment.44LIS-eligiblebeneficiariesenrolled
inplansimplementingVBIDbyeliminatingcostsharingorreducingitbelowtheLISamountswill
beabletobenefitfromVBID,butthoseenrolledinplanswhosereducedcostsharingisabovethe
LISamountswillnot.Duetothisuncertainty,ourestimatesinthissectionincludeallbeneficiaries,
regardlessofLISeligibility,unlessotherwisenoted.
Basedonouranalysisandtheavailableliterature,Options1and3,whichwouldimplement
VBIDthroughareductionofcostsharingforspecificdrugsorenrolleeswithchronicconditionsmay
reachthegreatestnumberofMedicarebeneficiaries(Table3).Amoredetaileddiscussionofhowwe
derivedtheseestimatesfollows.
43 CMS,PrescriptionDrugBenefitManual,Chapter13,AppendixA.http://www.cms.hhs.gov/PrescriptionDrugCovContra/Downloads/ R7PDB.pdf44 CMSFinalRule,CMS4131–FC.IssuedJanuary12,2009.http://edocket.access.gpo.gov/2009/E9-148.htm
va
lue
-ba
se
d in
su
ra
nc
e d
es
ign
in t
he
me
dic
ar
e P
re
sc
riP
tio
n b
en
ef
it
18
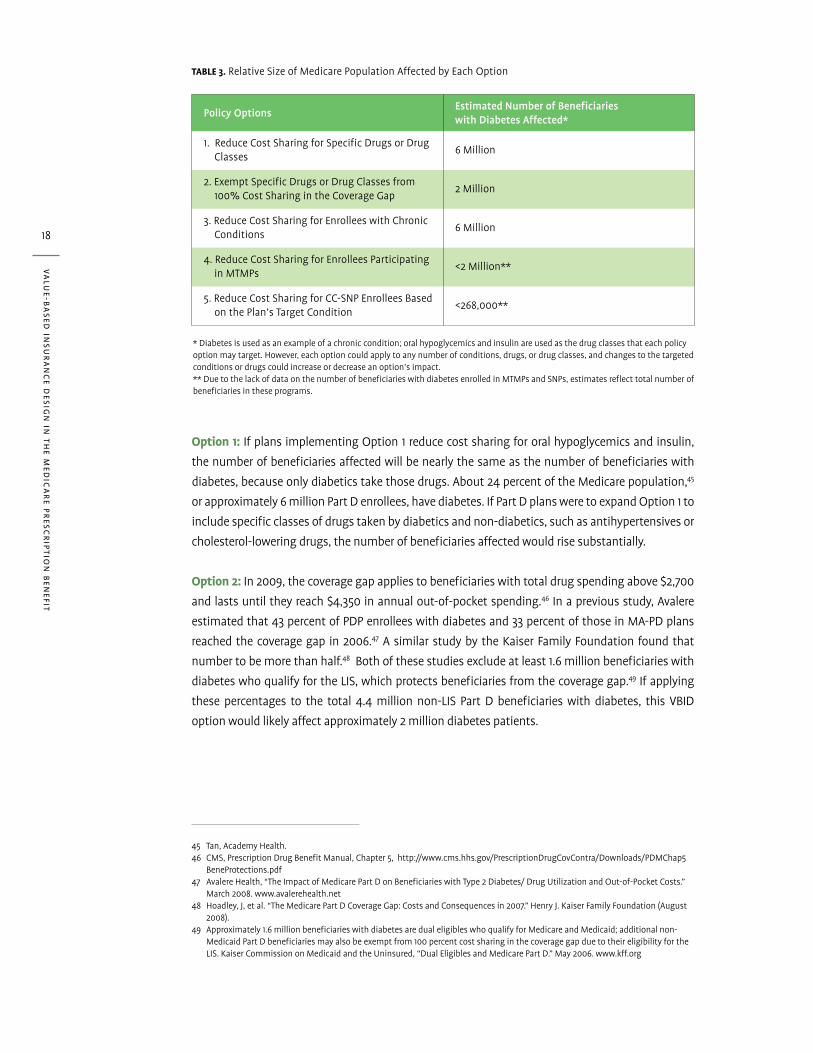
Table 3.RelativeSizeofMedicarePopulationAffectedbyEachOption
PolicyOptionsEstimatedNumberofBeneficiarieswithDiabetesAffected*
1.ReduceCostSharingforSpecificDrugsorDrugClasses
6Million
2.ExemptSpecificDrugsorDrugClassesfrom100%CostSharingintheCoverageGap
2Million
3.ReduceCostSharingforEnrolleeswithChronicConditions
6Million
4.ReduceCostSharingforEnrolleesParticipatinginMTMPs
<2Million**
5.ReduceCostSharingforCC-SNPEnrolleesBasedonthePlan’sTargetCondition
<268,000**
*Diabetesisusedasanexampleofachroniccondition;oralhypoglycemicsandinsulinareusedasthedrugclassesthateachpolicyoptionmaytarget.However,eachoptioncouldapplytoanynumberofconditions,drugs,ordrugclasses,andchangestothetargetedconditionsordrugscouldincreaseordecreaseanoption’simpact.**DuetothelackofdataonthenumberofbeneficiarieswithdiabetesenrolledinMTMPsandSNPs,estimatesreflecttotalnumberofbeneficiariesintheseprograms.
Option 1:IfplansimplementingOption1reducecostsharingfororalhypoglycemicsandinsulin,
thenumberofbeneficiariesaffectedwillbenearlythesameasthenumberofbeneficiarieswith
diabetes,becauseonlydiabeticstakethosedrugs.About24percentoftheMedicarepopulation,45
orapproximately6millionPartDenrollees,havediabetes.IfPartDplansweretoexpandOption1to
includespecificclassesofdrugstakenbydiabeticsandnon-diabetics,suchasantihypertensivesor
cholesterol-loweringdrugs,thenumberofbeneficiariesaffectedwouldrisesubstantially.
Option 2:In2009,thecoveragegapappliestobeneficiarieswithtotaldrugspendingabove$2,700
andlastsuntiltheyreach$4,350inannualout-of-pocketspending.46Inapreviousstudy,Avalere
estimatedthat43percentofPDPenrolleeswithdiabetesand33percentofthoseinMA-PDplans
reachedthecoveragegapin2006.47AsimilarstudybytheKaiserFamilyFoundationfoundthat
numbertobemorethanhalf.48Bothofthesestudiesexcludeatleast1.6millionbeneficiarieswith
diabeteswhoqualifyfortheLIS,whichprotectsbeneficiariesfromthecoveragegap.49Ifapplying
these percentages to the total 4.4 million non-LIS Part D beneficiaries with diabetes, this VBID
optionwouldlikelyaffectapproximately2milliondiabetespatients.
45 Tan,AcademyHealth.46 CMS,PrescriptionDrugBenefitManual,Chapter5,http://www.cms.hhs.gov/PrescriptionDrugCovContra/Downloads/PDMChap5 BeneProtections.pdf47 AvalereHealth,“TheImpactofMedicarePartDonBeneficiarieswithType2Diabetes/DrugUtilizationandOut-of-PocketCosts.” March2008.www.avalerehealth.net48 Hoadley,J,etal.“TheMedicarePartDCoverageGap:CostsandConsequencesin2007.”HenryJ.KaiserFamilyFoundation(August 2008).49 Approximately1.6millionbeneficiarieswithdiabetesaredualeligibleswhoqualifyforMedicareandMedicaid;additionalnon- MedicaidPartDbeneficiariesmayalsobeexemptfrom100percentcostsharinginthecoveragegapduetotheireligibilityforthe LIS.KaiserCommissiononMedicaidandtheUninsured,“DualEligiblesandMedicarePartD.”May2006.www.kff.org

an
aly
sis
of
oP
tio
ns
19
Option 3:AllPartDenrolleeswiththetargetedchronicconditionwouldbenefitfromVBIDinthis
option.Fordiabetes,thisrepresentsapproximately6millionPartDenrollees.50
Option 4: CMS has reported that approximately 8 percent of beneficiaries, or 2 million people,
participatedinMTMPsin2007.51SinceMTMPsincludebeneficiarieswithotherchronicconditions,
thenumberofbeneficiarieswithdiabeteswouldbelowerthan2million.Inaddition,thisoption
wouldaffectrelativelyfewerbeneficiariesthantargetingallbeneficiarieswithdiabetes.However,
linkingVBIDtoMTMPparticipationcouldboostMTMPenrollment; in2007,7percentofeligible
beneficiaries did not participate in their MTMP.52 Additionally, efforts to increase the scope of
medication-related services provided through MTMPs, coupled with VBID, could have a greater
impactonbeneficiaryhealthcareutilizationandspending.
Option 5:In2009,almost268,000beneficiariesenrolledinCC-SNPs.53ManyCC-SNPsin2009target
diabetes;someincludediabetesandotherchronicconditions,andsomefocussolelyondiabetes.
However,beginningin2010,CMSwillrequirethatCC-SNPstargetonlyoneofaselectionofchronic
conditioncategories,includingdiabetes.54
CMSAuthoritytoChangePolicyWeanalyzedeachpolicyoptiontodetermineanyexistingstatutoryhurdlesthatCMSmayfaceand
the regulatory or legislative changes that would be necessary to implement the suggested VBID
approach.
Thenecessarychangesfallalongaspectrumfromoptionsrequiringnewlegislationto
optionsthatCMScanexecuteadministrativelyunderthecurrentlaw,andthosethatplanscando
todaywithoutanypolicychanges.Basedonouranalysis,PartDplanscanimplementOptions1,2,
and5inthecurrentpolicyenvironment,whileOptions3and4mayrequirelegislativechanges(Table
4).Amoredetaileddiscussionofthelegislativeandregulatoryhurdlesweuncoveredfollows.
50 Tan,AcademyHealth.51 CMS,“MedicarePartDMedicationTherapyManagementPrograms2008FactSheet.”http://www.cms.hhs.gov/PrescriptionDrug CovContra/Downloads/MTMFactSheet.pdf52 Ibid.53 AvalereHealthanalysisofCMS’SNPMonthlyEnrollmentFile,January2009.54 CMS,“SpecialNeedsPlanChronicConditionPanel2008FinalReport.”November12,2008.http://www.cms.hhs.gov/ specialneedsplans/

va
lue
-ba
se
d in
su
ra
nc
e d
es
ign
in t
he
me
dic
ar
e P
re
sc
riP
tio
n b
en
ef
it
20
Table 4. Policy changes required for implementation
PolicyOptions LikelyPolicyChangeNeeded
1.ReduceCostSharingforSpecificDrugsorDrugClasses
Nopolicychangenecessary,butadditionalincentivesmayberequiredtopromotegreateradoption
2. ExemptSpecificDrugsorDrugClassesfrom100%CostSharingintheCoverageGap
Nopolicychangenecessary,butadditionalincentivesmayberequiredtopromotemoregapcoverageoptionsthatcoverhigh-valuedrugs
3.ReduceCostSharingforEnrolleeswithChronicConditions
Examineapplicationofnon-discriminationclause;mayrequireexemptionthroughregulationorlegislation
ExemptVBIDfromuniformbenefitrequirementthroughregulationorlegislation
4.ReduceCostSharingforEnrolleesParticipatinginMTMPs
Examineapplicationofnon-discriminationclause;mayrequireexemptionthroughregulationorlegislation
ExemptVBIDfromuniformbenefitrequirementthroughregulationorlegislation
5.ReduceCostSharingforCC-SNPEnrolleesBasedonthePlan’sTargetCondition
Nopolicychangenecessary;someCC-SNPsmayalreadybedoingthis
Option 1: No policy change required, but incentives may be needed.PartDplanscurrentlyhave
theabilitytoplacecovereddrugsondifferentformularytierswithvariedcostsharingforeachtier.
Throughthisability,planscouldplacehigh-valuedrugsordrugclassesonlowercost-sharingtiers
toprovidebetteraccesstothosedrugsfortheirmembers.PlanscanimplementVBIDbyreducing
oreliminatingcostsharingforspecificdrugsaslongasaplan’sformularycontinuestomeetCMS’
formularyguidelines,rulesonactuarialequivalence,andotherapplicablePartDstandards.
Asnotedabove,atleastoneMA-PDplanbeganexercisingthisoptionin2008,butmost
PartDplansdonotappeartobeimplementingVBID.InordertoencouragemorePartDplansto
featureaVBIDapproachsimilartoOption1,CMSofficialscouldhighlightthistypeofbenefitdesign
asonethatisnotonlyacceptablebutcouldresultinimprovedhealthoutcomesforbeneficiaries.
CMScouldmakesuchastatementthroughitsregularcommunicationswithPartDplans,viapress
release,orinsubregulatoryguidancesuchastheannualCallLetterortheMedicarePrescription
Drug Benefit Manual. Additionally, to encourage plans, particularly PDPs, to adopt this option
supplementalpaymentsornon-financial incentives,suchasthosediscussed inSectionIII,may
havearole.
Option 2: No policy change required, but incentives may be needed.Similarly,Option2iscurrently
availabletoPartDplanswishingtocovercertaindrugsthroughthecoveragegap.Inordertodoso,
theplanmustofferanenhancedbenefitdesignincludinggapcoverage.Planscanchoosewhich
formularydrugsareeligibleforgapcoveragebytheplan,andcouldselecthigh-valuedrugsordrug
classesforthiscoverage.Beneficiariesintheseplanswouldpaythesamecost-sharingamountfor
theselecteddrugsintheinitialcoverageperioduntiltheyreachthecatastrophiclimit.
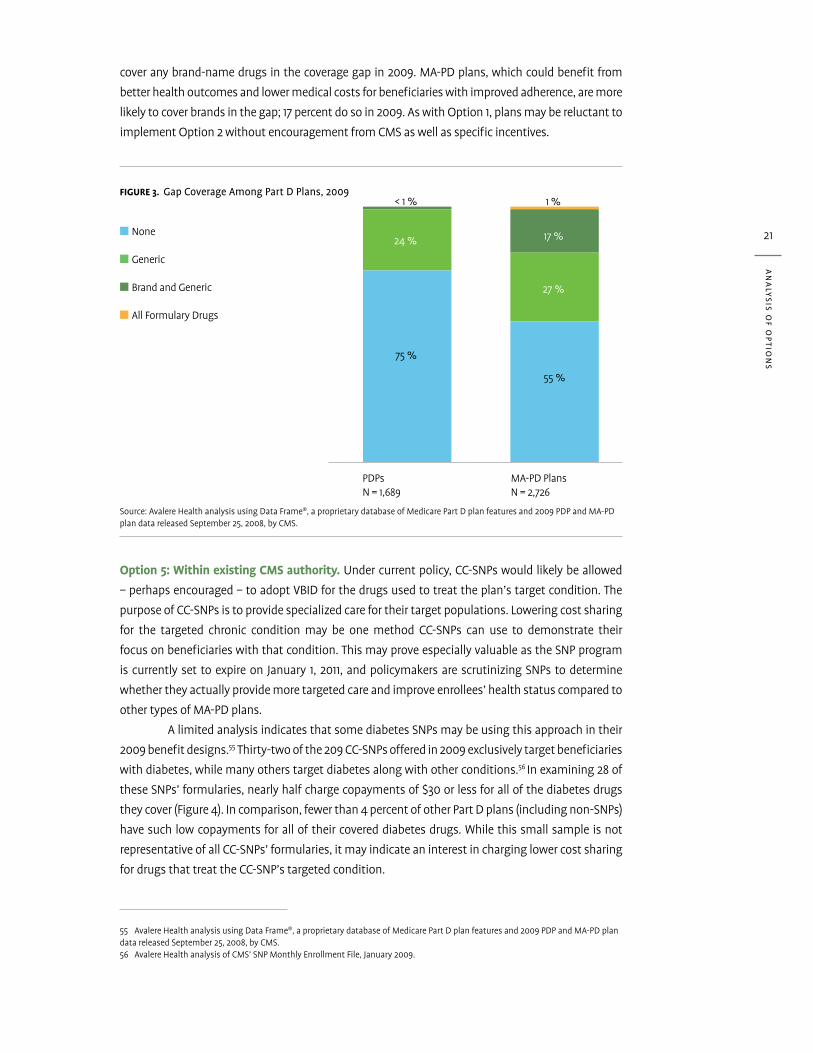
In2009,25percentofPDPsand44percentofMA-PDplansoffergapcoveragetobeneficiaries,
butmostofthesecoveronlygenericsinthegap(Figure3).AmongstandalonePDPs,onlythreeplans
an
aly
sis
of
oP
tio
ns
21
coveranybrand-namedrugsinthecoveragegapin2009.MA-PDplans,whichcouldbenefitfrom
betterhealthoutcomesandlowermedicalcostsforbeneficiarieswithimprovedadherence,aremore
likelytocoverbrandsinthegap;17percentdosoin2009.AswithOption1,plansmaybereluctantto
implementOption2withoutencouragementfromCMSaswellasspecificincentives.
Figure 3. gap coverage among Part d Plans, 2009
Option 5: Within existing CMS authority.Undercurrentpolicy,CC-SNPswouldlikelybeallowed
–perhapsencouraged–toadoptVBIDforthedrugsusedtotreattheplan’stargetcondition.The
purposeofCC-SNPsistoprovidespecializedcarefortheirtargetpopulations.Loweringcostsharing
for the targeted chronic condition may be one method CC-SNPs can use to demonstrate their
focusonbeneficiarieswiththatcondition.ThismayproveespeciallyvaluableastheSNPprogram
iscurrentlysettoexpireonJanuary1,2011,andpolicymakersarescrutinizingSNPstodetermine
whethertheyactuallyprovidemoretargetedcareandimproveenrollees’healthstatuscomparedto
othertypesofMA-PDplans.
AlimitedanalysisindicatesthatsomediabetesSNPsmaybeusingthisapproachintheir
2009benefitdesigns.55Thirty-twoofthe209CC-SNPsofferedin2009exclusivelytargetbeneficiaries
withdiabetes,whilemanyotherstargetdiabetesalongwithotherconditions.56Inexamining28of
theseSNPs’formularies,nearlyhalfchargecopaymentsof$30orlessforallofthediabetesdrugs
theycover(Figure4).Incomparison,fewerthan4percentofotherPartDplans(includingnon-SNPs)
havesuchlowcopaymentsforalloftheircovereddiabetesdrugs.Whilethissmallsampleisnot
representativeofallCC-SNPs’formularies,itmayindicateaninterestincharginglowercostsharing
fordrugsthattreattheCC-SNP’stargetedcondition.
55 AvalereHealthanalysisusingDataFrame®,aproprietarydatabaseofMedicarePartDplanfeaturesand2009PDPandMA-PDplandatareleasedSeptember25,2008,byCMS.56 AvalereHealthanalysisofCMS’SNPMonthlyEnrollmentFile,January2009.
Source:AvalereHealthanalysisusingDataFrame®,aproprietarydatabaseofMedicarePartDplanfeaturesand2009PDPandMA-PDplandatareleasedSeptember25,2008,byCMS.
■ None
■ Generic
■ BrandandGeneric
■ AllFormularyDrugs
0
20
40
60
80
100<1%
24%
75%
PDPsN=1,689
MA-PDPlansN=2,726
1%
17%
27%
55%

va
lue
-ba
se
d in
su
ra
nc
e d
es
ign
in t
he
me
dic
ar
e P
re
sc
riP
tio
n b
en
ef
it
22
57 CMS,InterimFinalRuleCMS4138-IFC,issuedSeptember15,2008.58 Ibid.59 CMShasprovidedadditionaldiscussiononthemodelofcarerequirementinsubregulatoryguidancedocuments,includingthe 2008and2009CallLetters.CMS,ContractYear2008CallLetter,April19,2007,andCMS,ContractYear2009CallLetter,March17, 2008.http://www.cms.hhs.gov/PrescriptionDrugCovContra/Downloads/CallLetter.pdf
Figure 4.HighestCopaymentsforCoveredDiabetesDrugs,2009
AsanadditionalincentiveforCC-SNPstoincorporateVBIDintheirbenefitdesigns,CMScoulddefine
Option5tohelpCC-SNPsmeettherequirementthattheydesignamodelofcare“tomeetthe
specializedneedsoftheSNPtargetpopulation.”57Themodelofcarerequirementwasestablished
bytheMedicareImprovementsforPatientsandProvidersActof2008(MIPPA),andCMSreleased
furtherguidanceinaninterimfinalrulethathasnotyetbeenfinalized.Inthisregulation,CMS
indicatedthatitwouldnot“endorseanyparticularsetofevidence-basedguidelinesorprotocols,”
butprovidesexamplesoftheelementseachSNPshouldincludeinitsmodelofcare,includingcare
coordinationservicesandanetworkofspecializedproviders.58,59CMScouldaddmoreexamplesof
elementsofaSNPmodelofcare,includingVBID,throughfurtherregulationorguidance.
Options 3 and 4: exceptions to ‘uniform benefit’ requirement may be required.Options3and
4eachproposetoimplementVBIDbyidentifyingasubgroupofPartDbeneficiariesandreducing
costsharingforonlythosebeneficiaries.Inbothofthesescenarios,enrolleesinaPartDplanwill
facedifferencesincostsharingforthesamedrugsbasedonwhethertheenrolleeisamemberof
thetargetpopulation.Allowingdifferencesinbenefitdesignforbeneficiarieswithinthesameplan
mayrequirelegislativeandregulatorychanges.LegislationspecificallydefiningthisVBIDapproach
andexemptingsuchbenefitstructuresfromtheantidiscriminationanduniformbenefitprovisions
wouldmostclearlyestablishtheauthorityofCMStoapproveplanbidsusingVBIDapproachesthat
targetasubsetofplanbeneficiaries.
Source:AvalereHealthanalysisusingDataFrame®,aproprietarydatabaseofMedicarePartDplanfeatures.DatafromNovember2008reflecting2009plans.Graphicsrepresentthecopaymentrangeforeachplan’shighestformularytiercontainingadrugusedtotreatdiabetes.*ChronicConditionSpecialNeedsPlansthatexclusivelytargetdiabetes.**Analysisexcludes1CC-SNPand721otherPartDplanswhosehighesttierfordiabetesdrugsrequirescoinsurance.
CC-SNPsTargetingDiabetes* AllOtherPartDPlans
N=27** N=3,330**
Over$5022%
$0-$1037%
$40-$5030%
Over$5078%
$10-$207%
$20-$304%
$40-$5012%
$ 0-$10: 1%$10-$20:<1%$20-$30: 2%$30-$40: 6%

an
aly
sis
of
oP
tio
ns
23
60 SocialSecurityAct,Section1860D-11(e)(2)(D)(i).61 CMS,FinalRule42CFR423.265(c)issuedOctober1,2007.http://edocket.access.gpo.gov/cfr_2007/octqtr/pdf/42cfr423.265.pdf62 CMS,FinalRule,CMS-4068-F,issuedJanuary28,2005.http://www.cms.hhs.gov/quarterlyproviderupdates/downloads/CMS4068F. PDF%2063 Beneficiarieswhoareeligibleforthelow-incomesubsidyorchargedalateenrollmentpenaltyarepermittedtohavedifferent premiumsand/orcostsharingthanotherenrollees.CMS,MMA1360D-13(a)(1)(F).
Thenondiscriminationclause,whichpreventsPartDplansfromdesigningabenefitthat
“substantiallydiscourage[s]enrollmentofcertainbeneficiaries,”60maybeseenasanobstacleto
VBID approaches that target a subset of plan enrollees. While the VBID design may encourage
enrollmentofsomebeneficiaries,itispossiblethataformularystructurethatreducescostsharing
forcertainbeneficiariesbutnotothersmaybeinterpretedasviolatingthisprovision.Forexample,a
planthatchargeslowercostsharingforbeneficiarieswithdiabetescouldbeviewedas“substantially
discouraging”theenrollmentofbeneficiarieswhodonothavediabetes.LegislationtoallowVBID
couldclarifytheparametersofabenefitdesignthattargetscertainbeneficiariesasanexceptionto
thisprovision.
Additionally,alegislativechangetoauthorizeOptions3or4shouldaddressthePartD
requirementthatplansprovideauniformbenefittoallenrollees.Infinalregulationsimplementing
thePartDprogram,CMSdescribesrequirementsforprospectivePartDplans,includingarequirement
thateachplan“mustreflectauniformbenefitpackage,includingpremium…andallapplicablecost
sharing,forallindividualsenrolledintheplan.”61Inthepreambletothisregulation,CMSexplains:
“ThismeansthatallenrolleesinagivenPDPorMA-PDplanwillbesubjecttothesamecostsharing
structureandwillbechargedthesamepremiumforbenefitsthePDPsponsororMAorganization
chosetooffer.”62CMSbasedthisregulationonaprovisionoftheMMAthatrequiresplanstocharge
allbeneficiariesauniformpremiumamount.63Whilethelegislativelanguageontheuniformbenefit
doesnotspecificallyrequireequivalentcostsharingforallenrollees,CMSwouldhavetoreviseits
regulatorylanguagetoallowVBIDtargetingcertainbeneficiaries.CMScouldalsoconsiderusingits
demonstrationauthoritytoallowtheseoptions.

va
lue
-ba
se
d in
su
ra
nc
e d
es
ign
in t
he
me
dic
ar
e P
re
sc
riP
tio
n b
en
ef
it
24
AbilitytoImplementOptionsGiventhehigh likelihood for the implementationofVBID inMedicarePartD,certainoperating
processesmayneedtobealtered.Thissectiondiscussessomeoftheoperationalchangesthat
mayberequired.Asummaryoftheimplementationissuesweidentifiedwitheachoptionappear
inTable5.
Table 5. operational changes required for implementation
PolicyOptions LikelyOperationalChangeNeeded
1.ReduceCostSharingforSpecificDrugsorDrugClasses
Plansmaycreatenewformularytierfortargeteddrugs
2.ExemptSpecificDrugsorDrugClassesfrom100%CostSharingintheCoverageGap
PlansmustoffergapcoveragefortargeteddrugsPlansmaycreatenewformularytierfortargeteddrugs
3.ReduceCostSharingforEnrolleeswithChronicConditions
Processtoidentifyenrolleeswithparticularchronicconditiondiagnosesandtoselectdrugseligibleforreducedcostsharing
4.ReduceCostSharingforEnrolleesParticipatinginMTMPs
AbilitytomonitorparticipationinMTMPs
5.ReduceCostSharingforCC-SNPEnrolleesBasedonthePlan’sTargetCondition
None
Each option identifies certain beneficiaries or drugs for reduced cost sharing. Identifying which
beneficiariesand/orwhichdrugs, ifnotspecifiedbyauthorizing legislation,maybe left toCMS
or another entity to determine, or could be left to individual plans to decide. In the event that
policymakerswishtoestablishastandardizedsetofdrugsorconditionstotargetwithVBID,legislation
orregulationscouldnameparticularconditions,drugs,ordrugclassesfortargeting.Alternatively,
policymakerscouldestablishaprocessfordeterminingthetargetedconditionsordrugs,similarto
theprocessCMSusedtodeterminethechronicconditionsforwhichplanscouldcreateCC-SNPs.
However,oncethatlevelofdetail isestablished,CMSmayneedtoprovideplanswithadditional
guidance,particularlyiftheVBIDapproachtargetsbeneficiarieswhomeetcertaincriteria.
Options1and2,whichfocusonspecificclassesofdrugs,mayhavefewimplementation
issuesoncetheidentificationoftargetedclassesofdrugsoccurs.InOption1,planscouldcreate
anewformularytierwithlowornocostsharingexclusivelyforthetargeteddrugs,orplacethose
drugsontheirexistinglowest-costtier.ToimplementOption2,aplanwouldhavetochangeits
offeringto includegapcoveragefor thetargeteddrugsordrugclassesbyaddinggapcoverage
wherenotofferedoraddinghigh-valuedrugstothelistofdrugsincludedinaplan’sgapcoverage.
Option3requiresplanstoidentifyenrolleeswithcertaindiagnoses.PartDplansalready
estimatetheirenrollees’particulardiagnosesandtheirseverityonanaggregatelevel,whichdetermines
therisk-adjustedpaymentsCMSmakestoeachplan.PlanscouldworkwithCMStoassigntheserisk
scoresatan individual levelanduse thosecodesasaproxy forbeneficiaries’ chronicconditions to
determineabeneficiary’seligibilityforreducedcostsharing.Alternatively,planscouldverifyeligibility
throughanotefromthepatient’sprovider,similartotheverificationprocessthatCC-SNPsemploy,
butthismethodwouldimposeahighadministrativeburdenonplansandbecostlytoimplement.

InOption4,planswouldberequiredtoidentifyenrolleeswhoareparticipatingintheir
MTMP.Thoughinitialidentificationmaybestraightforward,MTMPparticipantsmaydisenrollduring
thebenefityear,andplansmaywishtomonitorparticipationtolimitthenumberofenrolleeswho
benefitfromlowcostsharingbutnolongerparticipateintheirMTMP.IndividualPartDplansorCMS
couldestablishaprocessfordeterminingabeneficiary’sparticipationintheprogram,potentially
severaltimesduringtheyear,toensureheorshecontinuestoqualifyforlowcostsharing.
ForOptions3and4,CMSandplansmayneedtoovercomeoperationalchallengesin
determiningwhichcost-sharingamounteachenrolleemustpayforeachprescription.Underthe
currentsystem,allbeneficiarieswithinaplanpaythesameamountforagivendrugunlessthey
qualifyfortheLIS.UnderOptions3and4,plansmusttrackwhichbeneficiariesqualifyforlowercost
sharingandwhichdonot,andchargetheappropriatecostsharingforeachenrollee’sdrugs.Itmaybe
possibletodevelopaprocesssimilartotheoneusedtotrackLIScostsharingtomanagethistask.
Option5mayrequireCMStoidentifystandardsforVBIDnecessaryforfulfillingthe
modelofcarerequirement,andcompareCC-SNPformulariestothosestandardsintheformulary
reviewprocess.
PoliticalSupportTheVBIDapproachesdescribed in thispaperprovideexcitingopportunities forpolicymakers to
addresstherealitiesofspiralinghealthcarecostsandsuboptimalquality,issuesofgreatimportance
totheirmultipleconstituencies.Overthepasttwoyears,adiversegroupofstakeholdersacross
thehealthcareenterprisehasexpressedsupportforthisconcept.Becausethepercentageofhealth
serviceswithunequivocalclinicalevidencetosupporttheiruseunderVBIDprogramsissmallin
relationtoaggregatemedicalexpenditures,evengroupsthatmighttypicallyopposesuchefforts
as“paternalistic”havebeenreceptivetothisidea.
Patient advocacy groups representing individuals with chronic conditions who are
concerned about high cost sharing in Medicare Part D are likely to support VBID in general,
andthemore likelytheirmembersaretobenefitfromVBID,thestrongertheirsupportwillbe.
PharmaceuticalmanufacturersappeartosupportVBIDinconceptbuthaveparticularinterestin
howvalueisdetermined.HealthplanstendtoencouragePartDpoliciesthatprovideadditional
flexibilityinbenefitdesigns,andarelikelytoshowinterestinVBIDinMedicare,asanextensionof
theconcept’srapidlygrowingpresenceintheprivatesector.
PoliticalinterestinOption5islikelytobestrong,asdiscussedinprevioussections.Whileit
appearsthatsomeCC-SNPsmaybeusingaVBIDapproachintheircurrentbenefitdesigns,integrating
VBIDintomoreoftheseplansprovidesCC-SNPsanopportunitytooffermorespecializedbenefitsfor
theirtargetpopulation,demonstratesignificantdifferencesfromotherPartDplans,andpotentially
gatherdataontheimpactofVBIDonMedicarebeneficiaries’adherenceandhealthoutcomes.
Similarly,policymakersarelikelytoviewOptions1and2positively,sincePartDplans
canimplementbothoptionsinthecurrentprogram.Infact,CMSnotedinitsPartDregulations
thatplansshouldconsidertheimpactontotalmedicalcostswhendecidinghowtocoverdrugs
ontheirformularies:“Forexample,totheextentthataparticulardrughasbeenshowntobe
moreeffectiveinpreventingtheneedforhospitalcareorbetteratcontrollingacuteflare-ups
requiringtheuseofotherservices,weexpect[plans]totakethesethingsintoaccountintheir
determinationsofdrugefficacy.”64
an
aly
sis
of
oP
tio
ns
25
64 CMS,FinalRule,CMS-4069-F,issuedJanuary28,2005.

va
lue
-ba
se
d in
su
ra
nc
e d
es
ign
in t
he
me
dic
ar
e P
re
sc
riP
tio
n b
en
ef
it
26
While Options 3 and 4 may appear promising, they are likely to be less attractive to
policymakersdue to thepossiblechanges to legislativeand regulatorypolicies,particularly the
uniformbenefitprovision.Additionally,policymakersmaybereluctanttoadoptOption4dueto
potentialpolicychangesregardingMTMPparticipation.MTMPsarestillevolvinginPartD,andCMS
hasindicatedaninterestinchangingguidancerelatedtothestructureofandservicesprovidedby
theseprograms.
Overall,politicalsupportforVBIDappearstobestrong,bipartisan,bicameral,andgrowing.
Thepolicychangesidentifiedinthispaperprovidearoadmapforseveralscenariosthatwilladvance
VBIDprinciplesineffortstoimprovehealthandcontaincosts.

Conclusion
Based on this analysis, it appears that several options could be successful vehicles for VBID in
MedicarePartDandimmediatelyimplemented(Table6).Inparticular,Option1targetingspecific
drugsordrugclassesisanoptionforplansinthecurrentpolicyenvironment,andhasthepotential
toreachalargenumberofPartDbeneficiaries.Option2isalsopresentlyavailabletoplansand,
whileaffectingfewerbeneficiaries,ittargetsthosepatientswithhighannualdrugspendingwho
maybenefitmostfromthistypeofintervention.AsmoreevidenceofthebenefitsofVBIDbecomes
available,policymakersmaywishtopursuelegislativechangesthatwouldcreatenewincentivesto
encouragemorePartDplanstoadoptthesetypesofbenefits.
Table 6. summary of analysis
PolicyOptions
Option 1: reduce cost sharing for specific drugs or drug classes
Option 2: exempt specificdrugs or drug classes from 100% cost sharing in the coverage gap
Option 3: reduce cost sharing for enrollees with chronic conditions
Option 4: reduce cost sharing for enrollees Participating in mtmPs
Option 5:ReduceCostSharingforCC-SNPEnrolleesBasedonthePlan’sTargetCondition
PotentialtoImproveMedicare
size of medicare Population affected
0 G 0 G @
Feasibility
cms author-ity to change Policy
0 0 @ @ 0
ability to implement Policy
0 0 @ G 0
Political support 0 0 G G 0
0GreatestPotential/MostFeasibleGModeratePotential/Feasibility@ LeastPotential/Feasible
Option5isalsofeasibleinthecurrentpolicyenvironment.However,targetingVBIDto
enrollees in CC-SNPs will have a limited impact on the Medicare population – currently about
268,000beneficiaries,only1percentofPartDenrollment.Duetothesmallscaleofthisoption’s
impact,Option5maybeanidealfirststepinimplementingVBIDintheMedicarePartDprogram.
CMSandpolicymakerscouldencourageCC-SNPstoincorporateVBIDintotheirbenefitdesignsand
tocollectdataonadherenceandoutcomesfortheirenrollees.AsCC-SNPsgatherevidenceonthe
valueofVBIDinthispopulation,policymakerscouldconsideradditionalmethodsforincorporating
VBIDintotheMedicarePartDprogrammorebroadly.
co
nc
lus
ion
27

va
lue
-ba
se
d in
su
ra
nc
e d
es
ign
in t
he
me
dic
ar
e P
re
sc
riP
tio
n b
en
ef
it
28
Option 4 also presents an interesting opportunity to demonstrate the value of VBID,
despitepotentiallegislativechallengesinauthorizingsuchanoption.ThepairingofMTMPs’services
focusedonappropriatemedicationusewithlowercostsharingthroughVBIDappearstohavehigh
potential to impactbeneficiaries’adherenceandoutcomes.Loweringor removingthefinancial
barrierstomedicationusewillenhancemedicationmanagement;conversely,MTMPservicessuch
ascounselingbypharmacistscouldgreatlyimproveVBID’ssuccessinimprovingadherenceand
outcomes.WhileasmallnumberofPartDenrolleestakepartinMTMPsatpresent,onecouldargue
thatMTMPparticipantsarethoseinthegreatestneedofaninterventionsuchasVBID.Policymakers
maybeinterestedinexaminingthisoptionfurthertodeterminetheimpactonhealthoutcomes
andoverallprogramspending.
Finally,whileOption3hasthepotentialtoreachalargenumberofPartDbeneficiariesand
couldbeacost-effectiveapproachtoimplementingVBID,thelegislativeandregulatorychanges
likelyrequiredmaybebarrierstoitsimplementation,makingthisalessattractiveoption.

65 TrivediA,etal.“EffectofCostSharingonScreeningMammographyinMedicareHealthPlans.”NEJM358,no4(2008):375-383.
DiscussionandImplications
ThispaperpresentsseveralviableoptionsfortheMedicareprogramtoimplementVBIDinPartD.
PolicymakershavebecomeincreasinglyinterestedinVBIDastheevidencebaseforthemeritofVBID
intheprivatesectorbecomesclearerandMedicarefacescontinuedpressuretogetmorevaluefrom
thefederaldollarsspent.Eachoftheseoptionshavetheirownstrengthsandweaknessesbasedon
howmanyMedicarebeneficiariesmaybenefitandhoweasilytheparticularVBIDapproachcouldbe
implementedbyCongress,CMS,andhealthplans.Eachofthesefactorsisdynamicandouroption
evaluationsaresensitivetochangesintheMedicarePartDmarket.
Thescopeandpurposeofthispaperresultinvariouslimitationsthatcouldbethefocusof
futureanalyses.First,thispaperdoesnotfocusontheincentivesPartDplansmayrequiretoadopt
VBID.Whilewediscusstheneedforsuchincentivesandofferseveralexamplesofincentivesthat
policymakerscouldoffer,thistopicrequiresfurtherresearch.DiscussionswithPartDplansabout
theirinterestandconcernsaboutVBID,andfeedbackontheincentivesthatmightbemostattractive
toplanswouldhelptofurtherinformpolicymakersinterestedinencouragingVBID.
Second, though this paper suggests VBID for high-value drugs and particular chronic
conditions,itdoesnotexplicitlyrecommendwhatthosedrugsorconditionsshouldbe.Whilewe
usediabetesasanillustrativeexampleofanappropriatecondition,othersmayalsobeviable.Itis
alsoimportanttonotethatwhilesomeoptionstargetbeneficiarieswithspecificchronicconditions,
doingsoisnotrequiredforVBIDimplementation.Options1and2,forexample,couldtargetany
drugsordrugclassesdeterminedtoprovidehighvalue.
Third,thispaperdoesnotattempttoprojectcostsorsavingsfromVBIDimplementation.
TodosowithanyaccuracywillrequiremorespecificanalysisofaparticularVBIDproposal.The
potential cost or savings of legislative proposals will play a substantial role in determining an
option’sfeasibility.Whileaquantitativeanalysisisnotincludedinthispaper,AvalereHealthand
theUniversityofMichiganVBIDCenterarecollaboratingonacompanionpiecethatestimatesthe
potentialimpactofVBIDinMedicarePartD.
In addition, this paper does not discuss the measurement or evaluation of VBID after
implementation.WhenincorporatingVBIDintoMedicarePartD,policymakersshouldalsoconsider
providingresourcesformeasuringimpact,allowingstakeholderstoevaluatesuccessesanddrawbacks.
AlthoughthisanalysisfocusedontheapplicationofVBIDtochronicconditionmedications
coveredunderMedicarePartD,thereispromiseforVBIDinotheraspectsofMedicare.Alternative
applicationsofVBIDwithinMedicarecouldincludelowercostsharingforhigh-valuehospitaland
providerservicescoveredunderMedicarePartsAandB.Forexample,exemptingfemalebeneficiaries
from cost sharing for mammography could encourage better adherence to the U.S. Preventive
ServicesTaskForcerecommendationthatwomenover40getregularscreeningmammography.65
AstheObamaAdministrationandmembersofCongressexplorehealthreformoptions,
it is important that theynotonlyexamineoptions to increasecoverage for theuninsured,but
alsooptionstoimprovequalityandcontaincosts.VBIDsimultaneouslyaddressestheobjectives
ofcostcontainmentandqualityimprovementinthedeliveryofcarebypromoting“fiscally
responsible, clinically sensitive” cost sharing in order to mitigate the well-documented adverse
dis
cu
ss
ion
an
d im
Pl
ica
tio
ns
29

va
lue
-ba
se
d in
su
ra
nc
e d
es
ign
in t
he
me
dic
ar
e P
re
sc
riP
tio
n b
en
ef
it
30
clinicaloutcomesassociatedwiththecurrent,one-size-fits-allmedicalsystem.66Medicare isan
idealplacetoimplementVBIDbecausebeneficiariesareatamuchhigherriskofadverseevents
thanyoungerpatientpopulationsandensuringaccesstonecessarycareisafundamentaltenetof
theMedicareprogram.VBIDisavitaltoolthathasthepotentialtotransformMedicareintoamore
prudentpurchaserofhealthcareservicesthatmeetpatientneeds.
VBIDisnotamechanismthatwillsolveourhealthcarecrisis.Technologicaladvances
will continue to generate upward pressure on costs and increasingly strain the ability of
individuals and their employers toaffordsuch coverage. That said, compared to the status
quoofescalatingcostsandsuboptimalqualityofcare,theimplementationofVBIDprinciples
wouldencouragetheuseofhigh-valuecareandultimatelyproducebetterhealthoutcomesat
anylevelofhealthcareexpenditure.
66 FendrickAM,etal.“Value-BasedInsuranceDesign;A‘ClinicallySensitive’ApproachtoPreserveQualityandContainCosts.”AJMC 1 (2006):18-20.

References
Aetna.“NewAetnaRx-SavingsSMProgramCutsCostForMedicationsUsedToTreatChronicHealthConditions.”(December,52007)Accessedathttp://www.aetna.com/news/2007/1205.htm.
Anderson,Gerard.“MedicareandChronicConditions.”NEJM353,no.3(2005):305-309.
AvalereHealthanalysisofCMS’SNPMonthlyEnrollmentFile,January2009.
AvalereHealth,“TheImpactofMedicarePartDonBeneficiarieswithType2Diabetes/DrugUtilizationandOut-of-PocketCosts,”March2008.www.avalerehealth.net
Baucus,Sen.Max.“CalltoAction:HealthReform2009.”(November12,2008)http://finance.senate.gov/healthre-form2009/home.html(accessedJanuary5,2009).
Berger,J.“EconomicandClinicalImpactofInnovativePharmacyBenefitDesignsintheManagementofDiabetesPharmacotherapy.”AJMC13,no.2(2007):S55-58.
Blustein,J.“DrugCoverageandDrugPurchasesbyMedicareBeneficiarieswithHypertension.”Health Aff19,no.2(2000):219-230.
Braithwaite,etal.“LinkingCostSharingtoValue:AnUnrivaledYetUnrealizedPublicHealthOpportunity.”Ann Intern Med,146(2007):602-605.
ChernewME,etal.“EffectsofIncreasedPatientCostSharingonSocioeconomicDisparitiesinHealthCare.”J Gen Intern Med23,no.8(2008):1131-1136.
ChernewME,etal.“ImpactofDecreasingCopaymentsonMedicationAdherencewithinaDiseaseManagementEnvironment.”Health Aff27,no.1(2008):103-112.
ChernewME,etal.“Value-BasedInsuranceDesign:ByAbandoningtheArchaicPrinciplethatAllServicesMustCosttheSameforAllPatients,WeCanMovetoaHigh-ValueHealthSystem.”Health Aff 26,no.2(2007):w195-197.
ChoudhryN,PatrickA,AntmanE,AvornJ,ShranW.“Cost-effectivenessofProvidingFullDrugCoveragetoIncreaseMedicationAdherenceinPostMyocardialInfarctionMedicareBeneficiaries.”Circ117(2008):1261-1268.
CMS,“BeneficiaryExperience.”PresentationatMedicarePrescriptionDrugBenefitSymposium,October30,2008.http://www.cms.hhs.gov/PrescriptionDrugCovGenIn/08_PartDData.asp
CMS,ContractYear2008CallLetter,April19,2007.
CMS,ContractYear2009CallLetter,March17,2008.http://www.cms.hhs.gov/PrescriptionDrugCovContra/Down-loads/CallLetter.pdf
CMS,MedicareAdvantage/PartDContractandEnrollmentData,January2009.http://www.cms.hhs.gov/MCRAdvPartDEnrolData/
CMS,“2006SpecialNeedsPlan(SNP)EnrollmentReportbySNPType.”http://www.cms.hhs.gov/SpecialNeed-sPlans/Downloads/06SNP_Enrollment_by_Type11-9-06.pdf
CMS,FinalRule42CFR423.265(c),issuedOctober1,2007.http://edocket.access.gpo.gov/cfr_2007/octqtr/pdf/42cfr423.265.pdf
CMS,FinalRuleCMS-4068-F,issuedJanuary28,2005.http://www.cms.hhs.gov/quarterlyproviderupdates/down-loads/CMS4068F.PDF%20
CMS,InterimFinalRuleCMS4138-IFC,issuedSeptember15,2008.http://edocket.access.gpo.gov/2008/pdf/E8-21686.pdf
re
fe
re
nc
es
31

CMS,“MedicarePartDMedicationTherapyManagementPrograms:2008FactSheet.”March19,2008.http://www.cms.hhs.gov/PrescriptionDrugCovContra/Downloads/MTMFactSheet.pdf.
CMS,MedicarePrescriptionDrugImprovementandModernizationAct,Pub.L.108-173,Section1360D-13(a)(1)(F).
CMS,MonthlySNPReports,September2008.
CMS,PrescriptionDrugBenefitManual,Chapter5,http://www.cms.hhs.gov/PrescriptionDrugCovContra/Down-loads/PDMChap5BeneProtections.pdf
CMS,PrescriptionDrugBenefitManual,Chapter6,Section30.2.7.http://www.cms.hhs.gov/PrescriptionDrugCov-Contra/Downloads/R2PDB.pdf
CMSPressRelease,“MedicarePrescriptionDrugBenefit’sProjectedCostsContinuetoDrop,”January31,2008.
CMS,“SpecialNeedsPlanChronicConditionPanel2008FinalReport.”November12,2008.http://www.cms.hhs.gov/specialneedsplans/
Cole,etal.“DrugCopaymentandAdherenceinChronicHeartFailure:EffectonCostandOutcome.”Pharmaco-therapy26,no.8(2006):1157-1164.
CranorC.W.,etal.“TheAshevilleProject:Long-TermClinicalandEconomicOutcomesofaCommunityPharmacyDiabetesCareProgram,”JAPA43,no.2(2003):173-184.
EllisJJ.“SuboptimalStatinAdherenceandDiscontinuationinPrimaryandSecondaryPreventionPopulationsShouldWeTargetPatientswiththeMosttoGain?”J Gen Intern Med19(2004):639-646.
FendrickAM,etal.“Value-BasedInsuranceDesign:FiscallyResponsible,ClinicallySensitiveApproachToMakingTheMostOfHealthDollars.”AJMC13(June2007):325-327.
FisherE,etal.“RegionalVariationsinHealthCareIntensityandPhysicianPerceptionsofQualityofCare.”Ann Intern Med144,no.9(2006):641-649.
GibsonTB,etal.“TheEffectsofPrescriptionDrugCopaymentsonStatinAdherence.”AJMC12(2006):509-517.
GoldmanDP,etal.“PharmacyBenefitsandtheUseofDrugsbytheChronicallyIll.”JAMA291,no.19(2004):2344-50.
GoldmanDP,etal.“PrescriptionDrugCostSharing:AssociationswithMedicationandMedicalUtilizationandSpendingandHealth.”JAMA298,no.1(2007):61-69.
GoldmanDP,etal“VaryingPharmacyBenefitswithClinicalStatus:theCaseofCholesterol-LoweringTherapy.”AJMC12(2006):21-28.
GreeneFL.“ImpactofLoweringMember’sOut-of-PocketCosts.”AMCPPosterPresentation.March2007.
Hoadley,J,etal.“TheMedicarePartDCoverageGap:CostsandConsequencesin2007.”HenryJ.KaiserFamilyFoundation(August2008).
KaiserCommissiononMedicaidandtheUninsured,“DualEligiblesandMedicarePartD.”May2006.www.kff.org
Kamal-Bahl,S.andBriesacher,B.“HowdoIncentive-BasedFormulariesInfluenceDrugSelectionandSpendingforHypertension?”Health Aff23,no.1(2004):227-236.
Mahoney,JJ.“ReducingPatientDrugAcquisitionCostsCanLowerDiabetesHealthClaims,”AJMC11,no.5(2005):S170-S176.
MedPACMeeting.October3,2007.http://www.medpac.gov/transcripts/1003-04medpac.final.pdf(accessedJanuary5,2009).
va
lue
-ba
se
d in
su
ra
nc
e d
es
ign
in t
he
me
dic
ar
e P
re
sc
riP
tio
n b
en
ef
it
32

NeumannP,etal.“MedicarePrescriptionDrugBenefitProgressReport:Findingsfroma2006NationalSurveyofSeniors.”Health AffairsWebExclusive26.5(August21,2007):w630-w643.
Newhouse,Joseph,InsuranceExperimentGroup.FreeforAll?LessonsfromtheRANDHealthInsuranceExperiment.Cambridge,MA:HarvardUniversityPress;1993.
Nicholson,S.“TheEffectofCostSharingonEmployeeswithDiabetes.”AJMC12(2006):SP20-SP26.
Piette,J.D.,etal.“ProblemsPayingOut-of-PocketMedicationCostsAmongOlderAdultswithDiabetes.”Diabetes Care27(2004):384-391.
“PublicProgramsareUsingIncentivestoPromoteHealthyBehavior.”TheCommonwealthFund.(October11,2007).http://www.commonwealthfund.org/innovations/innovations_show.htm?doc_id=676105
ResultsfromM-Healthy:FocusonDiabetestwo-yearpilotprogram(unpublishedstudydatareportedinDrug Benefit News)December12,2008.
Roblin,D.W.etal.“EffectofIncreasedCost-SharingonOralHypoglycemicUseinFiveManagedCareOrganiza-tions:HowMuchisTooMuch?”Med Care43,no.10(2005):951-959.
RosenAB,etal.,“IndicationsforandUtilizationofACEInhibitorsinOlderIndividualswithDiabetes:FindingsfromtheNationalHealthandNutritionExaminationSurvey1999to2002,”J Gen Intern Med21,no.4(2006):315–319.
RosenAB,HamelMB,WeinsteinMC,CutlerDM,FendrickAM,VijanS.“Cost-effectivenessofFullMedicareCoverageofAngiotensin-ConvertingEnzymeInhibitorsforBeneficiarieswithDiabetes.”Ann Intern Med 143(2005):89-99.
“SeniorDimensionsLowersPrescriptionDrugCo-PaymentsonManyWidelyUsedBrand-NameMaintenanceDrugs.”Business Wire,September24,2008.
“SierratoIncurLossonEnhancedMedicarePartDPrescriptionDrugProductOffering.”Business Wire.http://findarticles.com/p/articles/mi_m0EIN/is_2007_Feb_27/ai_n27306987
SocialSecurityAct,Section1860D-11(e)(2)(D)(i).
SokolMC,etal.“ImpactofMedicationAdherenceonHospitalizationRiskandHealthcareCost.”Med Care43,no.6(2005):521-530.
Stockl,K,etal.“EffectofanInterventiontoIncreaseStatinUseinMedicareMembersWhoQualifiedforaMedica-tionTherapyManagementProgram.”JMCP.July/August2008.
Tan,Ronnie.“CharacteristicsofMedicareBeneficiarieswithChronicConditions.”Presentationat2007AcademyHealth,June4,2007.http://www.academyhealth.org/2007/monday/asia1/tanr.pdf
Thomas,CP.“HowPrescriptionDrugUseAffectsHealthCareUtilizationandSpendingbyOlderAmericans:AReviewoftheLiterature.”AARPPublicPolicyInstitute(April2008).
WilsonI,etal.“Physician-PatientCommunicationAboutPrescriptionMedicationNonadherence:A50-StateStudyofAmerica’sSeniors.”J of Gen Intern Med22,no.1(2007):6-12.
Wong,MitchellD,etal.“EffectsofCostSharingonCareSeekingandHealthStatus:ResultsFromtheMedicalOutcomesStudy.”AJPH91,no.11(2001).
re
fe
re
nc
es
33

Art
icle
(l
ead
aut
hor o
r Pu
blis
her,
year
)
Des
crip
tion
of
Inte
rven
tion
Cond
itio
nU
se
Med
icar
eD
ata
Out
com
esM
easu
red*
*
dia
bete
sh
yper
ten-
sion
oth
er*
adh
eren
ce
(+/-
)
emer
genc
y
med
ical
use
(+
/-)
cost
s (+
/-)
Incr
ease
dCo
stS
hari
ngfo
rCh
roni
cCo
ndit
ion
Dru
gs
Blus
tein
,200
0M
odel
ede
ffec
tofn
oth
avin
gdr
ugc
over
age
onra
tea
twhi
chb
ene-
fici
arie
sw
ith
hype
rten
sion
pur
chas
eda
ntih
yper
tens
ive
tabl
ets
✕✕
—
Cher
new
,200
8
J Gen
Inte
rn M
edM
odel
edw
heth
erd
oubl
ing
copa
ysfo
rmed
icat
ions
use
dto
tr
eat
diab
etes
and
chr
onic
hea
rtfa
ilure
dec
reas
eda
dher
ence
at
diff
eren
tra
tes
ford
iffe
rent
inco
me
leve
ls
✕✕
—
Cole
,200
6M
odel
edim
pact
ofa
$10
incr
ease
inc
opay
forb
eta-
bloc
kers
an
dAC
Esfo
rchr
onic
hea
rtfa
ilure
pat
ient
s✕
—
✕
Gib
son,
200
6M
odel
edim
pact
ofa
cros
sth
ebo
ard
copa
yin
crea
ses
ons
tati
nad
here
nce
forp
atie
nts
wit
hhy
pert
ensi
on
✕—
Gol
dman
,200
4M
odel
edim
pact
ofd
oubl
ing
copa
ysfo
reig
htt
hera
peut
ic
clas
ses
onp
resc
ript
ion
fill
rate
s✕
✕✕
✕—
✕
Piet
te,2
004
Mod
eled
impa
cto
finc
reas
edc
opay
sfo
rdia
bete
sm
edic
atio
ns
ona
dher
ence
rate
s✕
—
Robl
in,2
005
$10
incr
ease
inc
opay
sfo
rora
lhyp
ogly
cem
ics
✕—
dec
reas
ed c
ost
shar
ing
for c
hron
ic c
ondi
tion
dru
gs
Aet
na,2
007
Act
iveH
ealt
hM
anag
emen
tre
duce
dco
pays
by
$5fo
rsel
ect
gene
rics
and
by
50p
erce
ntfo
rsel
ect
bran
ds✕
✕✕
✕
—
Berg
er,2
007
Pitn
eyB
owes
mov
eda
llm
edic
atio
nfo
rast
hma,
dia
bete
s,a
nd
hype
rten
sion
to
tier
1✕
✕✕
✕
——
Cher
new
,200
8H
ealt
h Af
fA
ctiv
eHea
lth
Man
agem
ent
redu
ced
copa
ysb
y$5
fors
elec
tge
neri
csa
ndb
y50
per
cent
fors
elec
tbr
ands
✕✕
✕
✕
Chou
dhry
,200
8M
odel
edim
pact
ofw
aivi
ngc
opay
sfo
rasp
irin
,bet
a-bl
ocke
rs,
ACEs
and
ARB
s,a
nds
tati
nsa
fter
acu
tem
yoca
rdia
linf
arct
ion
✕✕
——
*O
ther
con
diti
ons
stud
ied
incl
ude
asth
ma,
rheu
mat
oid
arth
riti
s,c
hron
ich
eart
failu
re,p
ost-
acut
em
yoca
rdia
linf
arct
ion,
and
dep
ress
ion.
**
✕
=in
crea
se;
—
=de
crea
se
Not
e:T
his
tabl
eis
not
mea
ntt
obe
ac
ompr
ehen
sive
revi
ewo
fall
stud
ies
ond
iffe
rent
ialc
ost
shar
ing
forc
hron
icc
ondi
tion
dru
gs;r
athe
r,it
see
kst
opr
esen
tth
em
ore
rece
nts
tudi
eso
nth
ist
opic
.
app
end
ix
Rece
ntV
BID
Stu
dies
ofD
iffe
rent
ialC
ost
Shar
ing
forC
hron
icC
ondi
tion
Dru
gs
aP
Pe
nd
ix
34

Art
icle
(l
ead
aut
hor o
r Pu
blis
her,
year
)
Des
crip
tion
of
Inte
rven
tion
Cond
itio
nU
se
Med
icar
eD
ata
Out
com
esM
easu
red*
*
dia
bete
sh
yper
ten-
sion
oth
er*
adh
eren
ce
(+/-
)
emer
genc
y
med
ical
use
(+
/-)
cost
s (+
/-)
dec
reas
ed c
ost
shar
ing
for c
hron
ic c
ondi
tion
dru
gs
Cran
or,2
003
Ash
evill
ePr
ojec
t—em
ploy
ers
wai
ved
copa
ysfo
rdia
bete
s
med
icat
ions
✕
✕—
—
Dru
gBe
nefi
tN
ews,
200
8M
-Hea
lthy
—w
aive
dor
redu
ced
copa
yso
fsel
ecte
dm
edic
atio
ns
forU
nive
rsit
yof
Mic
higa
nfa
cult
y,s
taff
and
the
ird
epen
dent
sw
ith
diab
etes
✕
✕
Ellis
,200
4Ex
amin
ede
ffec
tof
redu
cing
cop
ays
ofs
tati
nso
nm
edic
atio
nad
here
nce
amon
gpa
tien
tsw
ith
high
risk
of
coro
nary
hea
rtd
isea
se✕
✕
Gol
dman
,200
6M
odel
edim
pact
ofw
aivi
ngc
opay
sfo
rcho
lest
erol
-low
erin
gth
erap
yfo
rpat
ient
sw
ith
high
cho
lest
erol
✕
✕
——
Gre
ene,
200
7La
rge
empl
oyer
wai
ved
copa
ysfo
rsta
tins
fora
llem
ploy
eess
✕
✕
—
Mah
oney
,200
5Pi
tney
Bow
esm
oved
all
med
icat
ion
fora
sthm
a,d
iabe
tes,
an
dhy
pert
ensi
ont
oti
er1
✕✕
✕
✕
Kam
al-B
ahl,
2004
Exam
ined
impa
cto
finc
enti
ve-b
ased
form
ular
ies
and
anti
-hy
pert
ensi
vea
dher
ence
rate
sam
ong
pati
ents
wit
hhy
pert
ensi
on✕
✕
Nic
hols
on,2
006
Sim
ulat
edt
hee
ffec
tofm
ovin
gal
ldia
bete
sm
edic
atio
nsto
tie
r1
✕
✕
—
Rose
n,2
005
Mod
eled
the
impa
cto
fwai
ving
cop
ays
forA
CEs
for
bene
fici
arie
sw
ith
diab
etes
✕✕
——
Soko
l,20
05Ex
amin
edt
hee
ffec
tof
MTM
Pfo
rpat
ient
sw
ith
diab
etes
and
co
rona
rya
rter
ydi
seas
e✕
✕✕
✕
✕
——
Won
g,2
001
Exam
ined
eff
ect
ofd
ecre
asin
gco
pays
of
sele
ctm
edic
atio
nsfo
rch
roni
cco
ndit
ion
pati
ents
✕
✕✕
✕
——
*O
ther
con
diti
ons
stud
ied
incl
ude
asth
ma,
rheu
mat
oid
arth
riti
s,c
hron
ich
eart
failu
re,p
ost-
acut
em
yoca
rdia
linf
arct
ion,
and
dep
ress
ion.
**
✕
=in
crea
se;
—
=de
crea
se
Not
e:T
his
tabl
eis
not
mea
ntt
obe
ac
ompr
ehen
sive
revi
ewo
fall
stud
ies
ond
iffe
rent
ialc
ost
shar
ing
forc
hron
icc
ondi
tion
dru
gs;r
athe
r,it
see
kst
opr
esen
tth
em
ore
rece
nts
tudi
eso
nth
ist
opic
.
(Con
tinu
ed)
aP
Pe
nd
ix
35



Avalere Health LLC1350 Connecticut Avenue, NWWashington, DC 20036202.207.1300www.avalerehealth.net
University of Michigan Center for Value-Based Insurance Design109 South ObservatoryAnn Arbor, MI 48109-2029734.615.7197www.vbidcenter.org