vapor rub, petrolatum, and no treatment for …...vapor rub, petrolatum, and no treatment for...
TRANSCRIPT
Vapor Rub, Petrolatum, and No Treatment forChildren With Nocturnal Cough and Cold Symptoms
WHAT’S KNOWN ON THIS SUBJECT: There are few evidence-based therapies for children with cold symptoms. Topicalaromatic compounds are widely used to treat cold symptomswithout contemporary evidence to support this practice.
WHAT THIS STUDY ADDS: A vapor rub combination of camphor,menthol, and eucalyptus oils provided nocturnal symptom relieffor children with cold symptoms. Children treated with vapor rubhad improved sleep, as did their parents, when compared withchildren given placebo or no treatment.
abstractOBJECTIVE: To determine if a single application of a vapor rub (VR) orpetrolatum is superior to no treatment for nocturnal cough, conges-tion, and sleep difficulty caused by upper respiratory tract infection.
METHODS: Surveys were administered to parents on 2 consecutivedays—on the day of presentation when no medication had been giventhe previous evening, and the next day when VR ointment, petrolatumointment, or no treatment had been applied to their child’s chest andneck before bedtime according to a partially double-blinded random-ization scheme.
RESULTS: There were 138 children aged 2 to 11 years who completedthe trial. Within each study group, symptoms were improved on thesecond night. Between treatment groups, significant differences inimprovement were detected for outcomes related to cough, conges-tion, and sleep difficulty; VR consistently scored the best, and no treat-ment scored the worst. Pairwise comparisons demonstrated the supe-riority of VR over no treatment for all outcomes except rhinorrhea andover petrolatum for cough severity, child and parent sleep difficulty,and combined symptom score. Petrolatum was not significantly betterthan no treatment for any outcome. Irritant adverse effects were morecommon among VR-treated participants.
CONCLUSIONS: In a comparison of VR, petrolatum, and no treatment,parents rated VR most favorably for symptomatic relief of their child’snocturnal cough, congestion, and sleep difficulty caused by upper re-spiratory tract infection. Despite mild irritant adverse effects, VR pro-vided symptomatic relief for children and allowed them and their par-ents to have a more restful night than those in the other study groups.Pediatrics 2010;126:1092–1099
AUTHORS: Ian M. Paul, MD, MSc,a,b Jessica S. Beiler,MPH,a Tonya S. King, PhD,b Edelveis R. Clapp, DO,a JulieVallati, LPN,a and Cheston M. Berlin Jr, MDa
Departments of aPediatrics and bPublic Health Sciences, PennState College of Medicine, Hershey, Pennsylvania
KEY WORDScough, congestion, rhinorrhea, camphor, menthol, eucalyptus,placebo, upper respiratory infection
ABBREVIATIONSURI—upper respiratory infectionOTC—over-the-counterVR—vapor rub
This trial has been registered at www.clinicaltrials.gov(identifier NCT00743990).
www.pediatrics.org/cgi/doi/10.1542/peds.2010-1601
doi:10.1542/peds.2010-1601
Accepted for publication Aug 13, 2010
Address correspondence to Ian M. Paul, MD, MSc, Department ofPediatrics, Penn State College of Medicine, HS83, 500 UniversityDrive, Hershey, PA 17033-0850. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2010 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: Dr Paul has been a paid consultant forthe Consumer Products Healthcare Association, McNeilConsumer Health Inc, the Procter and Gamble Company, ReckittBenckiser Healthcare International Ltd, and Novartis ConsumerHealth Inc; the other authors have indicated they have nofinancial relationships relevant to this article to disclose.
Funded by the National Institutes of Health (NIH).
1092 PAUL et al by guest on February 1, 2020www.aappublications.org/newsDownloaded from

Upper respiratory infections (URIs)are the most common acute illnessesin the world,1 and symptoms caused bythese infections are disruptive for chil-dren. The characteristic features ofURIs are often adversely affected sleepfor both ill children and their parentswith an effect on subsequent daytimeactivities. In addition to attempting toimprove their comfort, giving medica-tions to children before bed is often anattempt by parents to improve theirown sleep and functioning during thesubsequent day.
Recent studies2,3 and guidelines4–7
have questioned the efficacy of manyoral over-the-counter (OTC) treat-ments for URI symptoms. Cliniciansand parents have been left with limitedtherapeutic options to administer tochildren with these disruptive symp-toms. Alternatives to oral medicationsare popular topical preparations thatcontain menthol, camphor, and euca-lyptus oils and have been used inadults and children for more than acentury.8–12
Commenting on camphor-containingproducts, in 1994 the American Acad-emy of Pediatrics Committee on Drugswrote, “Since alternative agents existfor all indications for camphor ther-apy, other therapeutic agents that donot contain camphor should be consid-ered.”13 The “alternative agent” forcough and cold symptoms cited by theCommittee in 1994, dextromethor-phan, was subsequently not recom-mended by that committee 3 yearslater in a policy statement on dextro-methorphan use.4 Dextromethorphancontinues not to be recommended,14 andtherefore the question of whether clini-cians can recommend topical prepara-tions containing camphor, menthol, andeucalyptus oil for URI symptoms in chil-dren requires reevaluation.
With no contemporary evidence thatsupports or refutes the efficacy in chil-dren with URIs, this study sought to de-
termine if a single application of a va-por rub (VR) or petrolatum is superiorto no treatment for nocturnal cough,congestion, and sleep difficulty causedby URIs. We hypothesized that VR orpetrolatum would be superior to notreatment for relief of nocturnal symp-toms and that VR would be superior topetrolatum.
METHODS
From October 2008 through February2010, patients were recruited from auniversity-affiliated pediatric practicein Hershey, Pennsylvania. Eligible pa-tients were aged 2 to 11 years withsymptoms attributed to URIs charac-terized by cough, congestion, and rhi-norrhea that lasted 7 days or longer.Patients were excluded for signs orsymptoms of a more treatable disease(eg, asthma, pneumonia, laryngotra-cheobronchitis, sinusitis, allergic rhi-nitis). They were also ineligible with ahistory of asthma, chronic lung dis-ease, or a seizure disorder. Childrenwith seizure disorders were excludedbecause of the reported association ofcamphor with seizures, particularly af-ter ingestions of toxic amounts.13 Fi-nally, subjects were excluded if on thenight before enrollment they used OTCor prescription medication that con-tained VR components, pseudoephed-rine, phenylephrine, dextromethor-phan, guaifenesin, diphenhydramine,brompheniramine, chlorpheniramine,or honey.
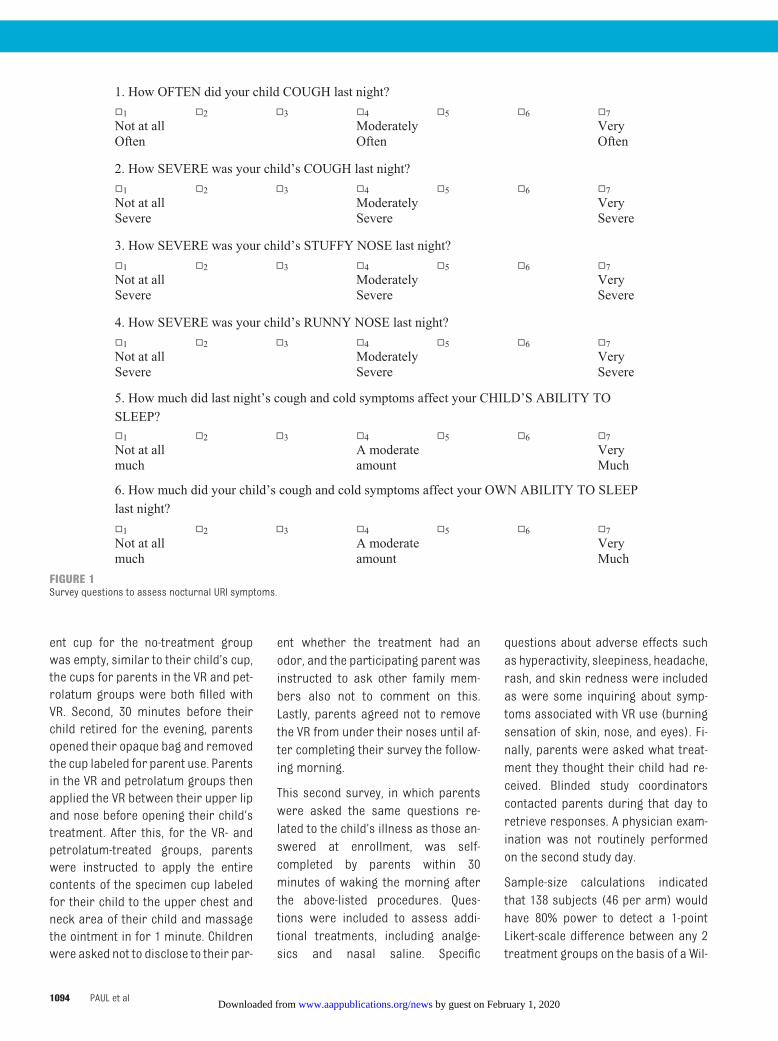
Subjective parental assessments oftheir child’s symptoms on the previousnight were assessed after informedconsent was obtained through a mod-ified version of our previously usedand validated questions15 by using a7-point Likert scale (Fig 1). Trainedstudy coordinators were responsiblefor survey administration, and surveyresponses ranged from most severesymptoms (7 points) to no symptoms(1 point). Minimum symptom-severity
criteria for enrollment were estab-lished. Only parents who answered atleast “moderately often” for cough fre-quency and “moderately severe” forstuffy nose (both equivalent to 4 pointson the scale) on the basis of the previ-ous night’s symptoms were eligible.
After stratification for age (2–5 and6–11 years), each child was randomlyassigned in a partially double-blindedfashion to 1 of 3 treatment groups: VRointment (Vicks VapoRub, which con-tains camphor [4.8%], menthol [2.6%],and eucalyptus oil [1.2%] [Procter andGamble, Cincinnati, OH]); petrolatumointment (Equate 100% pure white pe-troleum jelly [Wal-Mart Inc, Benton-ville, AR]); and no treatment. For the 2groups that received an ointment, thedose volume distributed was stratifiedaccording to age: 5 mL (2–5 years) and10mL (6–11 years). The randomizationsequence was constructed by a statis-tician not affiliated with the study andwas used to assign treatment groups.All study parents were instructed onroutine care for children with URI, in-cluding hydration measures, salinenose spray use, and use of acetamino-phen or ibuprofen as needed for com-fort. Because nasal saline could affectsome outcome measures, parentswere asked to not use it within 1 hourof bedtime or throughout the night.They were instructed not to administerexcluded OTC medications listed aboveto their child at any time after enroll-ment and to avoid giving them caffein-ated beverages within 4 hours ofbedtime.
To maintain investigator blinding, allstudy groups received an opaque pa-per bag that contained a glass speci-men cup filled with either ointment orno treatment. Given the aromatic andcharacteristic smell of VR, a series ofsteps was required to maintain paren-tal blinding. First, a second glass spec-imen cup labeled for parents wasplaced in each bag. Although the par-
ARTICLES
PEDIATRICS Volume 126, Number 6, December 2010 1093 by guest on February 1, 2020www.aappublications.org/newsDownloaded from
ent cup for the no-treatment groupwas empty, similar to their child’s cup,the cups for parents in the VR and pet-rolatum groups were both filled withVR. Second, 30 minutes before theirchild retired for the evening, parentsopened their opaque bag and removedthe cup labeled for parent use. Parentsin the VR and petrolatum groups thenapplied the VR between their upper lipand nose before opening their child’streatment. After this, for the VR- andpetrolatum-treated groups, parentswere instructed to apply the entirecontents of the specimen cup labeledfor their child to the upper chest andneck area of their child and massagethe ointment in for 1 minute. Childrenwere asked not to disclose to their par-
ent whether the treatment had anodor, and the participating parent wasinstructed to ask other family mem-bers also not to comment on this.Lastly, parents agreed not to removethe VR from under their noses until af-ter completing their survey the follow-ing morning.
This second survey, in which parentswere asked the same questions re-lated to the child’s illness as those an-swered at enrollment, was self-completed by parents within 30minutes of waking the morning afterthe above-listed procedures. Ques-tions were included to assess addi-tional treatments, including analge-sics and nasal saline. Specific
questions about adverse effects suchas hyperactivity, sleepiness, headache,rash, and skin redness were includedas were some inquiring about symp-toms associated with VR use (burningsensation of skin, nose, and eyes). Fi-nally, parents were asked what treat-ment they thought their child had re-ceived. Blinded study coordinatorscontacted parents during that day toretrieve responses. A physician exam-ination was not routinely performedon the second study day.
Sample-size calculations indicatedthat 138 subjects (46 per arm) wouldhave 80% power to detect a 1-pointLikert-scale difference between any 2treatment groups on the basis of a Wil-
1. How OFTEN did your child COUGH last night? □□1 □□2 □□3 □□4 □□5 □□6 □□7 Not at all Moderately Very Often Often Often
2. How SEVERE was your child’s COUGH last night? □□1 □□2 □□3 □□4 □□5 □□6 □□7 Not at all Moderately Very Severe Severe Severe
3. How SEVERE was your child’s STUFFY NOSE last night? □□1 □□2 □□3 □□4 □□5 □□6 □□7 Not at all Moderately Very Severe Severe Severe
4. How SEVERE was your child’s RUNNY NOSE last night? □□1 □□2 □□3 □□4 □□5 □□6 □□7 Not at all Moderately Very Severe Severe Severe
5. How much did last night’s cough and cold symptoms affect your CHILD’S ABILITY TO SLEEP? □□1 □□2 □□3 □□4 □□5 □□6 □□7 Not at all A moderate Very much amount Much
6. How much did your child’s cough and cold symptoms affect your OWN ABILITY TO SLEEP last night? □□1 □□2 □□3 □□4 □□5 □□6 □□7 Not at all A moderate Very much amount Much
FIGURE 1Survey questions to assess nocturnal URI symptoms.
1094 PAUL et al by guest on February 1, 2020www.aappublications.org/newsDownloaded from
coxon rank-sum test with Bonferroni-corrected� � .0167 to allow for 3 pair-wise comparisons for outcomesrelated to cough, congestion, rhinor-rhea, and sleep difficulty.
Between-study-group baseline and de-mographic features were comparedby using a �2 and Fisher’s exact testwhere appropriate for gender andrace and Fisher’s exact tests forweight and age. Within-treatment-group comparisons for the 2 nightswere conducted using paired t tests.Treatment group comparisons wereconducted by analysis of covariance,which was deemed appropriate afterassessment outcome variable distri-bution. For the primary analysis oftreatment effect, the outcome ofbetween-night change included base-line scores as a covariate. Fisher’sexact tests were used to compareadverse reaction rates betweentreatments.
The study was approved by Penn StateCollege of Medicine’s Human SubjectsProtection Office andwas registered atwww.clinicaltrials.gov before the firstsubject’s enrollment. Informed con-sent was obtained from participatingparents, and verbal assent was ob-tained from children older than 7years.
RESULTS
There were 144 children with URIs en-rolled, and 138 (95.8%) completed thesingle-night study. The mean age of thechildren completing the study was5.8� 2.8 years (Table 1). Of these par-ticipants, 51.4% were female, and85.5% were described by their parentsas white and non-Hispanic. The cohorthad been coughing on average 4.3 �1.5 days and congested 4.2� 1.5 daysbefore enrollment. Of the children whocompleted the study, 44 were ran-domly assigned to the VR study group,and 47 participants were randomly as-signed to each of the other study
groups. There were no demographicor baseline symptom-severity differ-ences between groups.
The baseline symptom scores that de-scribed the night before enrollmentwhen no participants received treat-ment were compared with scoresfrom the subsequent night when VR,petrolatum, or no treatment was givenbefore bed. Within each treatmentgroup, all outcomes were signifi-cantly improved on the subsequentnight (P � .05 for all). When sepa-rated by treatment group, with theexception of rhinorrhea severity, sig-nificant differences were detected inthe amount of improvement re-ported for all of the study outcomesin the planned 3-way comparison(Fig 2). Again, with the exception of rhi-norrhea, all of the outcomes found VRto yield the greatest improvement, fol-lowed by petrolatum, whereas notreatment consistently showed theleast amount of improvement (P� .05for all).
Because differences existed for all out-comes except rhinorrhea, pairwisecomparisons were then performed.
For both cough severity and cough fre-quency, VR was significantly betterthan no treatment (P � .01), but onlymarginally better than petrolatum forfrequency (P� .07) and severity (P�.06). Petrolatum was marginally betterthan no treatment for cough frequency(P� .09), but not better than no treat-ment for cough severity. For nasal con-gestion, the only significant pairwisecomparison was VR versus no treat-ment (P� .01); other comparisons be-tween individual treatments were notsignificant.
The most profound effects in pairwisecomparisons were for the outcomesrelated to sleep. As rated by parents,children treated with VR were signifi-cantly more able to sleep than werechildren randomized to receive petro-latum (P� .006) or no treatment (P�.001). No significant difference was de-tected between petrolatum and notreatment. Similarly, parents of chil-dren treated with VR rated their ownability to sleep as significantly betterthan did parents of children random-ized to petrolatum (P � .008) or notreatment (P� .001).
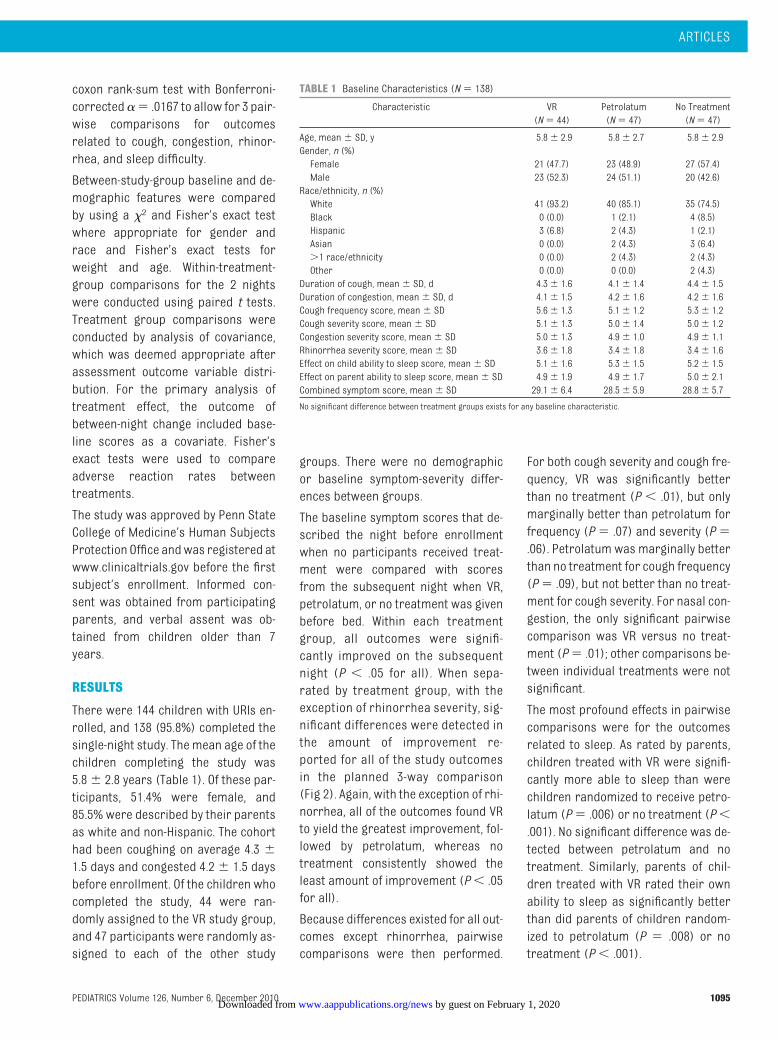
TABLE 1 Baseline Characteristics (N� 138)
Characteristic VR(N� 44)
Petrolatum(N� 47)
No Treatment(N� 47)
Age, mean� SD, y 5.8� 2.9 5.8� 2.7 5.8� 2.9Gender, n (%)Female 21 (47.7) 23 (48.9) 27 (57.4)Male 23 (52.3) 24 (51.1) 20 (42.6)Race/ethnicity, n (%)White 41 (93.2) 40 (85.1) 35 (74.5)Black 0 (0.0) 1 (2.1) 4 (8.5)Hispanic 3 (6.8) 2 (4.3) 1 (2.1)Asian 0 (0.0) 2 (4.3) 3 (6.4)�1 race/ethnicity 0 (0.0) 2 (4.3) 2 (4.3)Other 0 (0.0) 0 (0.0) 2 (4.3)Duration of cough, mean� SD, d 4.3� 1.6 4.1� 1.4 4.4� 1.5Duration of congestion, mean� SD, d 4.1� 1.5 4.2� 1.6 4.2� 1.6Cough frequency score, mean� SD 5.6� 1.3 5.1� 1.2 5.3� 1.2Cough severity score, mean� SD 5.1� 1.3 5.0� 1.4 5.0� 1.2Congestion severity score, mean� SD 5.0� 1.3 4.9� 1.0 4.9� 1.1Rhinorrhea severity score, mean� SD 3.6� 1.8 3.4� 1.8 3.4� 1.6Effect on child ability to sleep score, mean� SD 5.1� 1.6 5.3� 1.5 5.2� 1.5Effect on parent ability to sleep score, mean� SD 4.9� 1.9 4.9� 1.7 5.0� 2.1Combined symptom score, mean� SD 29.1� 6.4 28.5� 5.9 28.8� 5.7
No significant difference between treatment groups exists for any baseline characteristic.
ARTICLES
PEDIATRICS Volume 126, Number 6, December 2010 1095 by guest on February 1, 2020www.aappublications.org/newsDownloaded from
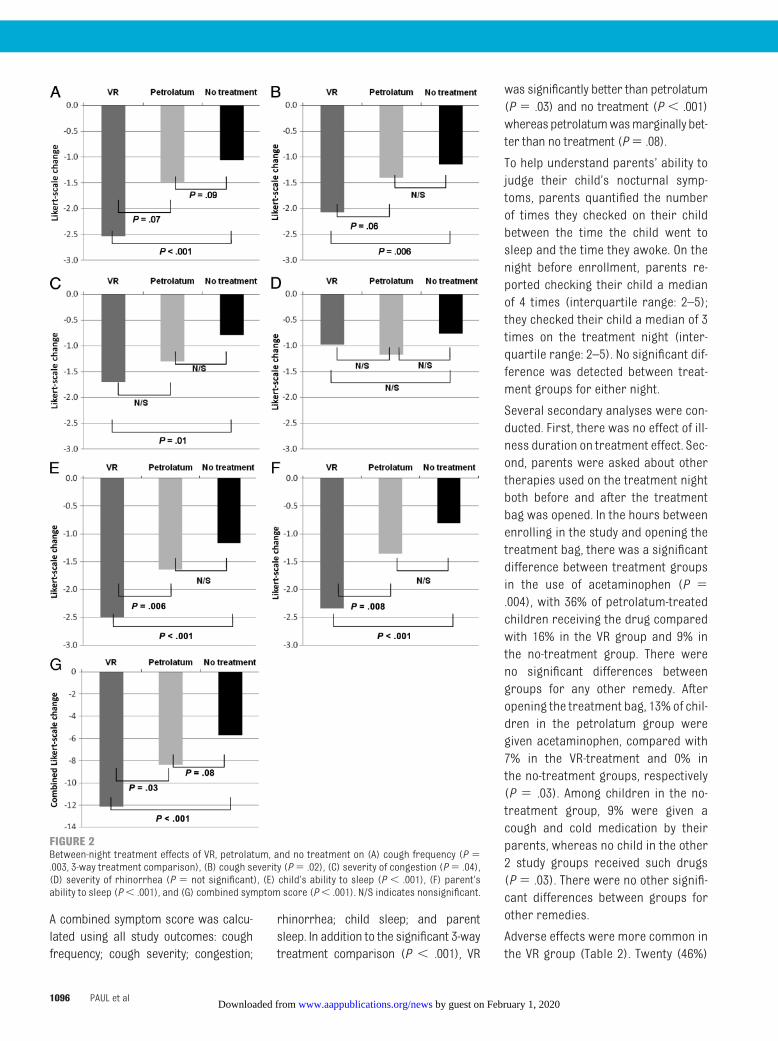
A combined symptom score was calcu-lated using all study outcomes: coughfrequency; cough severity; congestion;
rhinorrhea; child sleep; and parentsleep. In addition to the significant 3-waytreatment comparison (P � .001), VR
was significantly better than petrolatum(P � .03) and no treatment (P � .001)whereaspetrolatumwasmarginally bet-ter than no treatment (P� .08).
To help understand parents’ ability tojudge their child’s nocturnal symp-toms, parents quantified the numberof times they checked on their childbetween the time the child went tosleep and the time they awoke. On thenight before enrollment, parents re-ported checking their child a medianof 4 times (interquartile range: 2–5);they checked their child a median of 3times on the treatment night (inter-quartile range: 2–5). No significant dif-ference was detected between treat-ment groups for either night.
Several secondary analyses were con-ducted. First, there was no effect of ill-ness duration on treatment effect. Sec-ond, parents were asked about othertherapies used on the treatment nightboth before and after the treatmentbag was opened. In the hours betweenenrolling in the study and opening thetreatment bag, there was a significantdifference between treatment groupsin the use of acetaminophen (P �.004), with 36% of petrolatum-treatedchildren receiving the drug comparedwith 16% in the VR group and 9% inthe no-treatment group. There wereno significant differences betweengroups for any other remedy. Afteropening the treatment bag, 13% of chil-dren in the petrolatum group weregiven acetaminophen, compared with7% in the VR-treatment and 0% inthe no-treatment groups, respectively(P � .03). Among children in the no-treatment group, 9% were given acough and cold medication by theirparents, whereas no child in the other2 study groups received such drugs(P� .03). There were no other signifi-cant differences between groups forother remedies.
Adverse effects were more common inthe VR group (Table 2). Twenty (46%)
FIGURE 2Between-night treatment effects of VR, petrolatum, and no treatment on (A) cough frequency (P �.003, 3-way treatment comparison), (B) cough severity (P� .02), (C) severity of congestion (P� .04),(D) severity of rhinorrhea (P � not significant), (E) child’s ability to sleep (P � .001), (F) parent’sability to sleep (P� .001), and (G) combined symptom score (P� .001). N/S indicates nonsignificant.
1096 PAUL et al by guest on February 1, 2020www.aappublications.org/newsDownloaded from
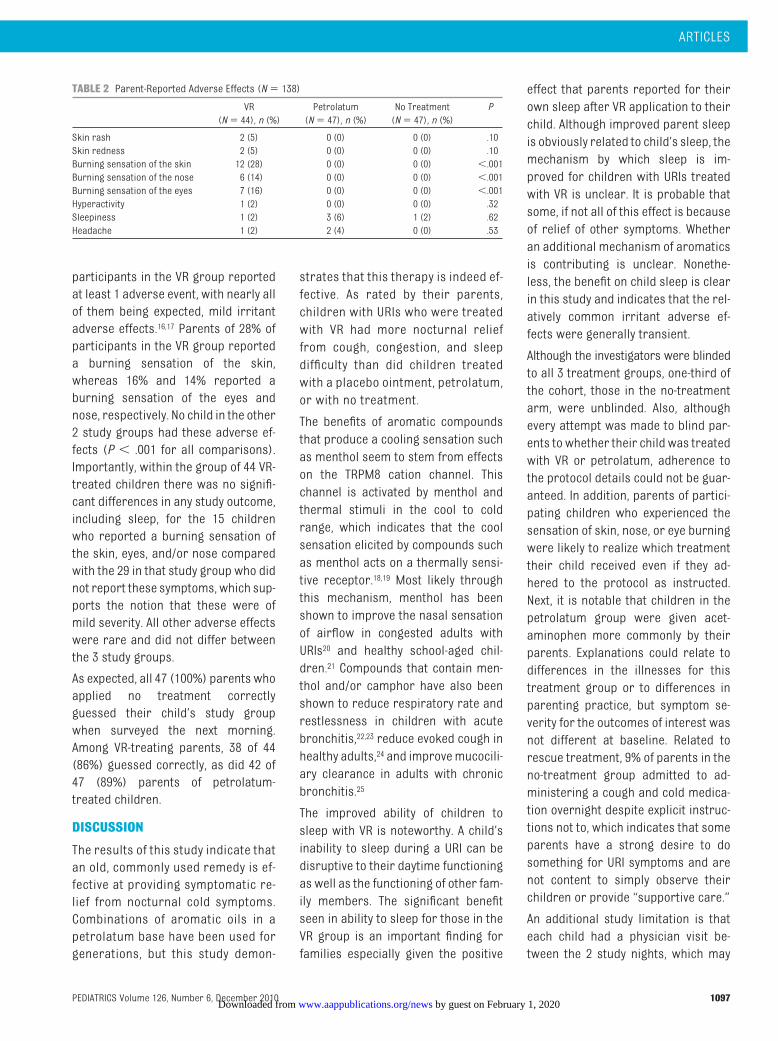
participants in the VR group reportedat least 1 adverse event, with nearly allof them being expected, mild irritantadverse effects.16,17 Parents of 28% ofparticipants in the VR group reporteda burning sensation of the skin,whereas 16% and 14% reported aburning sensation of the eyes andnose, respectively. No child in the other2 study groups had these adverse ef-fects (P � .001 for all comparisons).Importantly, within the group of 44 VR-treated children there was no signifi-cant differences in any study outcome,including sleep, for the 15 childrenwho reported a burning sensation ofthe skin, eyes, and/or nose comparedwith the 29 in that study group who didnot report these symptoms, which sup-ports the notion that these were ofmild severity. All other adverse effectswere rare and did not differ betweenthe 3 study groups.
As expected, all 47 (100%) parents whoapplied no treatment correctlyguessed their child’s study groupwhen surveyed the next morning.Among VR-treating parents, 38 of 44(86%) guessed correctly, as did 42 of47 (89%) parents of petrolatum-treated children.
DISCUSSION
The results of this study indicate thatan old, commonly used remedy is ef-fective at providing symptomatic re-lief from nocturnal cold symptoms.Combinations of aromatic oils in apetrolatum base have been used forgenerations, but this study demon-
strates that this therapy is indeed ef-fective. As rated by their parents,children with URIs who were treatedwith VR had more nocturnal relieffrom cough, congestion, and sleepdifficulty than did children treatedwith a placebo ointment, petrolatum,or with no treatment.
The benefits of aromatic compoundsthat produce a cooling sensation suchas menthol seem to stem from effectson the TRPM8 cation channel. Thischannel is activated by menthol andthermal stimuli in the cool to coldrange, which indicates that the coolsensation elicited by compounds suchas menthol acts on a thermally sensi-tive receptor.18,19 Most likely throughthis mechanism, menthol has beenshown to improve the nasal sensationof airflow in congested adults withURIs20 and healthy school-aged chil-dren.21 Compounds that contain men-thol and/or camphor have also beenshown to reduce respiratory rate andrestlessness in children with acutebronchitis,22,23 reduce evoked cough inhealthy adults,24 and improvemucocili-ary clearance in adults with chronicbronchitis.25
The improved ability of children tosleep with VR is noteworthy. A child’sinability to sleep during a URI can bedisruptive to their daytime functioningas well as the functioning of other fam-ily members. The significant benefitseen in ability to sleep for those in theVR group is an important finding forfamilies especially given the positive
effect that parents reported for theirown sleep after VR application to theirchild. Although improved parent sleepis obviously related to child’s sleep, themechanism by which sleep is im-proved for children with URIs treatedwith VR is unclear. It is probable thatsome, if not all of this effect is becauseof relief of other symptoms. Whetheran additional mechanism of aromaticsis contributing is unclear. Nonethe-less, the benefit on child sleep is clearin this study and indicates that the rel-atively common irritant adverse ef-fects were generally transient.
Although the investigators were blindedto all 3 treatment groups, one-third ofthe cohort, those in the no-treatmentarm, were unblinded. Also, althoughevery attempt was made to blind par-ents to whether their child was treatedwith VR or petrolatum, adherence tothe protocol details could not be guar-anteed. In addition, parents of partici-pating children who experienced thesensation of skin, nose, or eye burningwere likely to realize which treatmenttheir child received even if they ad-hered to the protocol as instructed.Next, it is notable that children in thepetrolatum group were given acet-aminophen more commonly by theirparents. Explanations could relate todifferences in the illnesses for thistreatment group or to differences inparenting practice, but symptom se-verity for the outcomes of interest wasnot different at baseline. Related torescue treatment, 9% of parents in theno-treatment group admitted to ad-ministering a cough and cold medica-tion overnight despite explicit instruc-tions not to, which indicates that someparents have a strong desire to dosomething for URI symptoms and arenot content to simply observe theirchildren or provide “supportive care.”
An additional study limitation is thateach child had a physician visit be-tween the 2 study nights, which may
TABLE 2 Parent-Reported Adverse Effects (N� 138)
VR(N� 44), n (%)
Petrolatum(N� 47), n (%)
No Treatment(N� 47), n (%)
P
Skin rash 2 (5) 0 (0) 0 (0) .10Skin redness 2 (5) 0 (0) 0 (0) .10Burning sensation of the skin 12 (28) 0 (0) 0 (0) �.001Burning sensation of the nose 6 (14) 0 (0) 0 (0) �.001Burning sensation of the eyes 7 (16) 0 (0) 0 (0) �.001Hyperactivity 1 (2) 0 (0) 0 (0) .32Sleepiness 1 (2) 3 (6) 1 (2) .62Headache 1 (2) 2 (4) 0 (0) .53
ARTICLES
PEDIATRICS Volume 126, Number 6, December 2010 1097 by guest on February 1, 2020www.aappublications.org/newsDownloaded from

provide some of the explanation forthe improvement in all of the groups,including the no-treatment group, be-cause parents may have been reas-sured that their child had a URI insteadof a more severe illness. Alternatively,some of the improvement in all groupscan also be attributed to the naturalhistory of URIs, which generally im-prove with time and supportive care.The subjective survey used for thisstudy may also be considered as alimitation, but clinicians and parentsoften make decisions on the basis ofsubjective assessment of symptomseverity, which has been arguedpreviously.3,26,27
Some clinicians may express cautionabout using a product that containscamphor because of the associationbetween toxic ingestions and adverseevents such as seizures.28–32 Historicalconcerns over the toxicity of camphorcentered on the ingestion of camphoras a liquid preparation, camphoratedoil,13,33 and a recent report of seizures
was associated with ingestion of ille-gally sold camphor.28 In contrast withoral ingestion, dermal exposure tocamphor, as occurs when followingthe directions for use of VR, results inlow systemic exposure.34 Serious ad-verse events such as seizures associ-ated with dermal exposure are gener-ally limited to young infants in whomVR use is not recommended.30,35 Mini-mizing safety concerns, the Food andDrug Administration approved cam-phor as an effective antitussive, butlimited the concentration in prepara-tions to 11%.36 The concentration in VRointment is 4.8%. Although recom-mended only for topical use, at thisconcentration it is estimated that aningestion of 20 mL of VR is required toproduce toxic effects and 40 mL to po-tentially cause a fatality in a childyounger than 6.29
CONCLUSIONS
Parents desire effective therapies fortheir children with cough and cold
symptoms, and clinicians want to offerevidence-based therapies. Althoughlimited data support many commonlyavailable and OTC remedies for coughcold symptoms, the current data indi-cate that VR helps to fill the therapeu-tic void. Despite mild irritant adverseeffects, VR provided symptomatic re-lief for children with URIs and allowedthem and their parents to have a morerestful night.
ACKNOWLEDGMENTSThis study was supported by an unre-stricted research grant from Procterand Gamble to Penn State Universityand by National Institutes of HealthGeneral Clinical Research Center grantM01RR10732 and GCRC constructiongrant C06RR016499 awarded to thePennsylvania State University Collegeof Medicine.
Dr King had full access to all the data inthe study and takes responsibility forthe integrity of the data and the accu-racy of the data analysis.
REFERENCES
1. Monto AS. Epidemiology of viral respiratoryinfections. Am J Med. 2002;112(suppl 6A):4S–12S
2. Paul IM, Yoder KE, Crowell KR, et al. Effect ofdextromethorphan, diphenhydramine, andplacebo on nocturnal cough and sleep qual-ity for coughing children and their parents.Pediatrics. 2004;114(1). Available at: www.pediatrics.org/cgi/content/full/114/1/e85
3. Paul IM, Beiler J, McMonagle A, Shaffer ML,Duda L, Berlin CM Jr. Effect of honey, dextro-methorphan, and no treatment on noctur-nal cough and sleep quality for coughingchildren and their parents. Arch PediatrAdolesc Med. 2007;161(12):1140–1146
4. Use of codeine- and dextromethorphan-containing cough remedies in children.American Academy of Pediatrics. Commit-tee on Drugs. Pediatrics. 1997;99(6):918–920
5. Department of Child and Adolescent Health.Cough and Cold Remedies for the Treat-ment of Acute Respiratory Infections inYoung Children. Geneva, Switzerland: WorldHealth Organization; 2001
6. Chang AB, Glomb WB. Guidelines for evalu-ating chronic cough in pediatrics: ACCP
evidence-based clinical practice guidelines.Chest. 2006;129(1 suppl):260S–283S
7. ShieldsMD, Bush A, EverardML, McKenzie S,Primhak R. BTS guidelines: recommenda-tions for the assessment and managementof cough in children. Thorax. 2008;63(suppl3):iii1–iii15
8. Todd GB. Notes on the eucalyptus oils pres-ently used in medicine with a short historyof the oils used during the last 10 years.Glasgow Med J. 1896;46:346
9. Rosenberg A. Menthol, a replacement forcocaine as a local anesthetic in the noseand pharynx [in German]. Berl KlinWchnschr. 1885;22:449
10. Fox N. Effect of camphor, eucalyptol, andmenthol on the vascular state of the mu-cous membrane. Arch Otolaryngol. 1927;6(2):112–122
11. Perrin M. A strong camphor ointmentintroduced in the nostrils of a young infantcan have the same disadvantages as men-thol [in French]. Province Méd. 1912;23:145
12. Dawson KP, Abbott GD, Allan J. Acute respi-ratory infection in childhood: a study of pa-rental prescribing patterns and advicesources. N Z Med J. 1983;96(734):481–482
13. Camphor revisited: focus on toxicity. Com-mittee on Drugs. American Academy of Pe-diatrics. Pediatrics. 1994;94(1):127–128
14. Letter to Joel Schiffenbauer, Food and DrugAdministration, September 6, 2007:325–328. Available at: www.fda.gov/ohrms/dockets/ac/07/briefing/2007-4323b1-02-FDA.pdf. Accessed October 11, 2010
15. Haver K, Hardy SC, Weber TM, Zurakowski D,Hartnick CJ. Validation of a pediatric coughquestionnaire. Presented at: AmericanThoracic Society 2006 InternationalConference; May 19–24, 2006; San Diego,CA. Abstract 374
16. Green BG. Sensory characteristics of cam-phor. J Invest Dermatol . 1990;94(5):662–666
17. Green BG. The sensory effects of l-mentholon human skin. Somatosens Mot Res. 1992;9(3):235–244
18. McKemy DD, Neuhausser WM, Julius D. Iden-tification of a cold receptor reveals a gen-eral role for TRP channels in thermosensa-tion. Nature. 2002;416(6876):52–58
19. Patel T, Ishiuji Y, Yosipovitch G. Menthol: arefreshing look at this ancient compound. JAm Acad Dermatol. 2007;57(5):873–878
1098 PAUL et al by guest on February 1, 2020www.aappublications.org/newsDownloaded from

20. Eccles R, Jawad MS, Morris S. The effects oforal administration of (�)-menthol on na-sal resistance to airflow and nasal sensa-tion of airflow in subjects suffering fromnasal congestion associated with the com-mon cold. J Pharm Pharmacol. 1990;42(9):652–654
21. Kenia P, Houghton T, Beardsmore C. Doesinhaling menthol affect nasal patency orcough? Pediatr Pulmonol. 2008;43(6):532–537
22. Berger H, Jarosch E, Madreiter H. Effect ofVaporub and petrolatum on frequency andamplitude of breathing in children withacute bronchitis. J Int Med Res. 1978;6(6):483–486
23. Berger H, Madreiter H, Jarosch E. Effect ofVaporub on the restlessness of childrenwith acute bronchitis. J Int Med Res. 1978;6(6):491–493
24. Morice AH, Marshall AE, Higgins KS, GrattanTJ. Effect of inhaled menthol on citric acid
induced cough in normal subjects. Thorax.1994;49(10):1024–1026
25. Hasani A, Pavia D, Toms N, Dilworth P, AgnewJE. Effect of aromatics on lung mucociliaryclearance in patients with chronic airwaysobstruction. J Altern Complement Med.2003;9(2):243–249
26. Taylor JA, Novack AH, Almquist JR, RogersJE. Efficacy of cough suppressants in chil-dren. J Pediatr. 1993;122(5 pt 1):799–802
27. Hutton N, Wilson MH, Mellits ED, et al. Effec-tiveness of an antihistamine-decongestantcombination for young children with thecommon cold: a randomized, controlledclinical trial. J Pediatr. 1991;118(1):125–130
28. KhineH,WeissD,GraberN,HoffmanRS,Esteban-Cruciani N, Avner JR. A cluster of children withseizures caused by camphor poisoning. Pediat-rics. 2009;123(5):1269–1272
29. Love JN, Sammon M, Smereck J. Are one ortwo dangerous? Camphor exposure in tod-dlers. J Emerg Med. 2004;27(1):49–54
30. Shannon M, McElroy EA, Liebelt EL. Toxic sei-zures in children: case scenarios and treat-ment strategies. Pediatr Emerg Care. 2003;19(3):206–210
31. Gibson DE, Moore GP, Pfaff JA. Camphor in-gestion. Am J Emerg Med. 1989;7(1):41–43
32. Siegel E, Wason S. Camphor toxicity. PediatrClin North Am. 1986;33(2):375–379
33. American Academy of Pediatrics, Commit-tee on Drugs. Camphor: who needs it? Pedi-atrics. 1978;62(3):404–406
34. Martin D, Valdez J, Boren J, Mayersohn M.Dermal absorption of camphor, menthol,and methyl salicylate in humans. J ClinPharmacol. 2004;44(10):1151–1157
35. Uc A, Bishop WP, Sanders KD. Camphor hep-atotoxicity. South Med J . 2000;93(6):596–598
36. Food and Drug Administration. Proposedrules: external analgesic drug products forover-the-counter human use; tentative finalmonograph. Federal Register. 1983;48
Exercise and the Brain: We all know that physical fitness has many beneficialeffects but can better physical fitness improve brain function? In an articlepublished in Science Daily (September 16, 2010) researchers showed that theanswer is yes. In 49 9- and 10-year-old children, physical fitness was determinedby measuring oxygen consumption while on a treadmill. The size of variousstructures of the brain was measured using magnetic resonance imaging. Itturns out that physical fitness directly correlated with hippocampal size. Thehippocampus is involved in learning and memory. Previous studies in animalshad shown that exercise can lead to increased hippocampal size and adult datahas suggested that larger hippocampal size correlated with better perfor-mance on spatial reasoning and other cognitive tasks. The hippocampus ofphysically fit children was approximately 12% larger relative to total brain size,than not fit children. The benefit to exercise was not just anatomic. Physically fitchildren outperformed not fit children on tests of relational memory, the abilityto remember and integrate information. While genetics and environment con-trol many aspects of cognitive function, here is an intervention that could po-tentially benefit all children. Here is yet another reason to recommend thatchildren put down the video controller, get off the couch, and run around out-side with their friends.
Noted by JFL, MD and WVR, MD
ARTICLES
PEDIATRICS Volume 126, Number 6, December 2010 1099 by guest on February 1, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2010-1601 originally published online November 8, 2010; 2010;126;1092Pediatrics
Cheston M. Berlin, JrIan M. Paul, Jessica S. Beiler, Tonya S. King, Edelveis R. Clapp, Julie Vallati and
and Cold SymptomsVapor Rub, Petrolatum, and No Treatment for Children With Nocturnal Cough
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/126/6/1092including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/126/6/1092#BIBLThis article cites 31 articles, 6 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/therapeutics_subTherapeuticshttp://www.aappublications.org/cgi/collection/pharmacology_subPharmacologyfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on February 1, 2020www.aappublications.org/newsDownloaded from
DOI: 10.1542/peds.2010-1601 originally published online November 8, 2010; 2010;126;1092Pediatrics
Cheston M. Berlin, JrIan M. Paul, Jessica S. Beiler, Tonya S. King, Edelveis R. Clapp, Julie Vallati and
and Cold SymptomsVapor Rub, Petrolatum, and No Treatment for Children With Nocturnal Cough
http://pediatrics.aappublications.org/content/126/6/1092located on the World Wide Web at:
The online version of this article, along with updated information and services, is
1073-0397. ISSN:60007. Copyright © 2010 by the American Academy of Pediatrics. All rights reserved. Print
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on February 1, 2020www.aappublications.org/newsDownloaded from