varicocele mark rosemary
TRANSCRIPT
VARICOCELEVARICOCELE
Presented by: Mark Rosemary
Ml 6082015
INTRODUCTIONINTRODUCTION• A varicocele is a dilatation of the pampiniform
venous plexus and the internal spermatic vein. • Varicocele is a well-recognized cause of decreased
testicular function and occurs in approximately 15-20% of all males and in 40% of infertile males.
• Represents the most common cause of primary & secondary infertility in the male.
• Varicoceles are present in 15% of normal males, 19% to 41% in men with primary infertility,& up to 81% of men with secondary infertility.
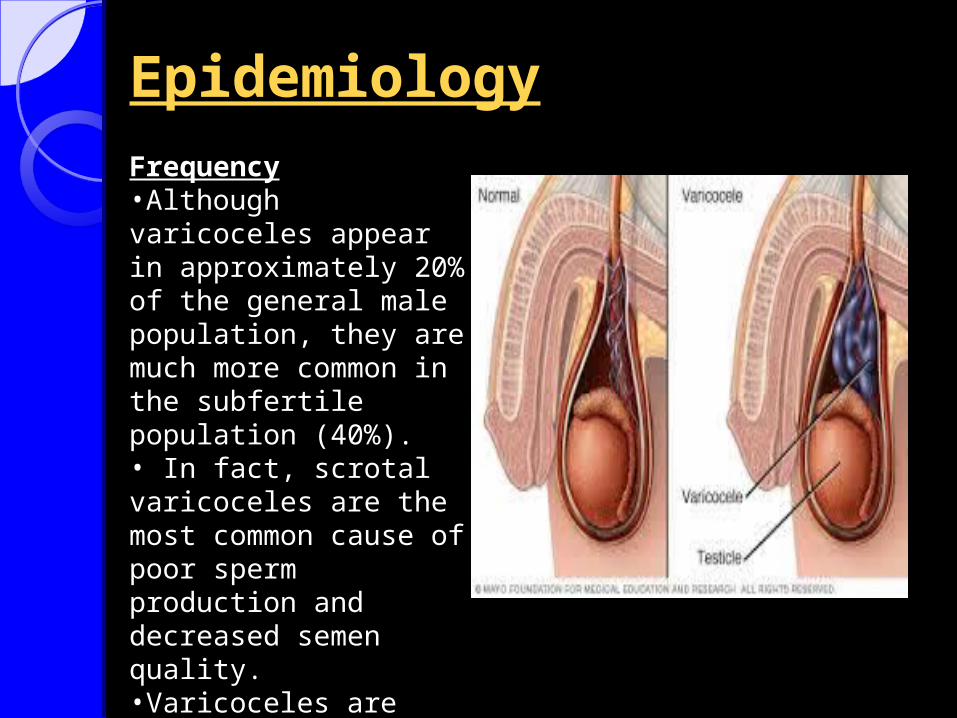
EpidemiologyEpidemiologyFrequency•Although varicoceles appear in approximately 20% of the general male population, they are much more common in the subfertile population (40%).• In fact, scrotal varicoceles are the most common cause of poor sperm production and decreased semen quality. •Varicoceles are easy to identify and to surgically correct.
ETIOLOGYETIOLOGY
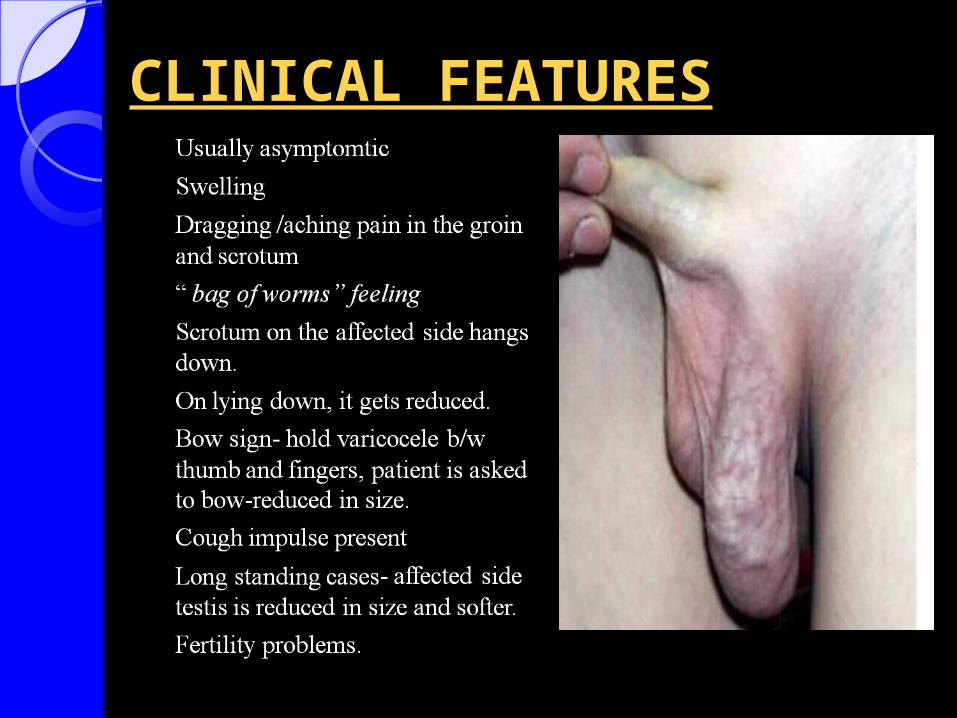
CLINICAL FEATURESCLINICAL FEATURES
GRADINGGRADING
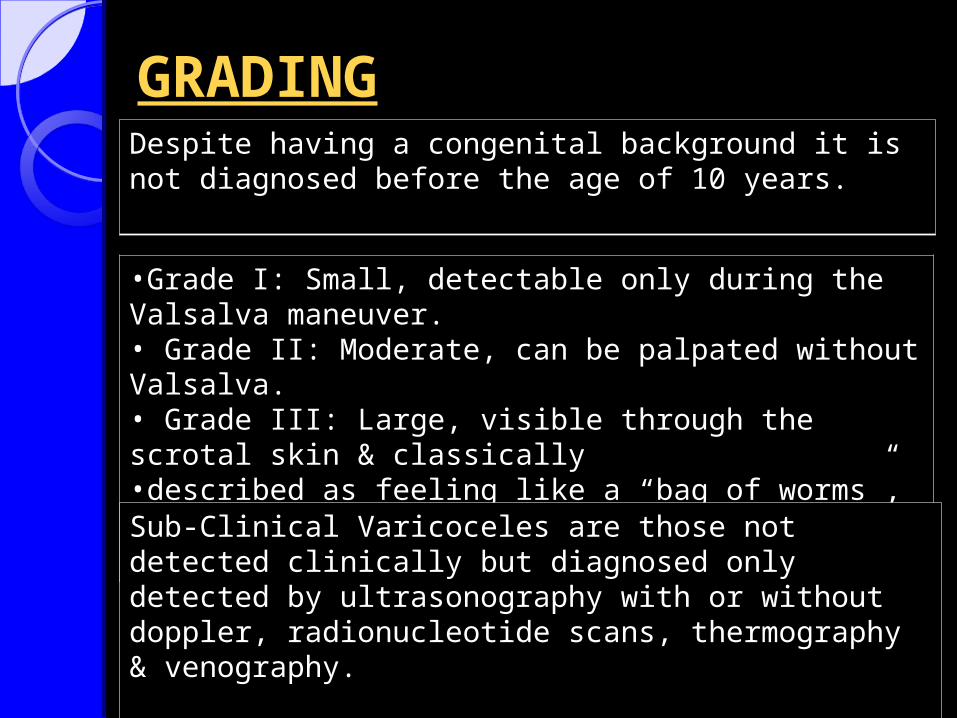
•Grade I: Small, detectable only during the Valsalva maneuver.• Grade II: Moderate, can be palpated without Valsalva.• Grade III: Large, visible through the scrotal skin & classically•described as feeling like a “bag of worms”, & decompresses in supine position.
Sub-Clinical Varicoceles are those not detected clinically but diagnosed only detected by ultrasonography with or without doppler, radionucleotide scans, thermography & venography.
Despite having a congenital background it is not diagnosed before the age of 10 years.
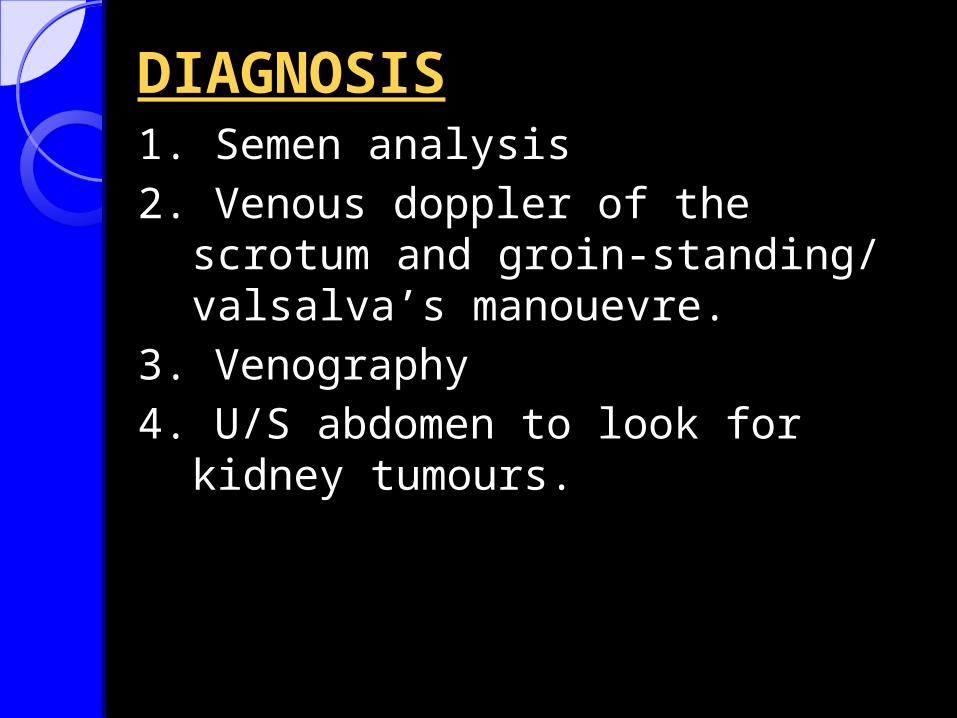
DIAGNOSIS1. Semen analysis
2. Venous doppler of the scrotum and groin-standing/ valsalva’s manouevre.
3. Venography
4. U/S abdomen to look for kidney tumours.
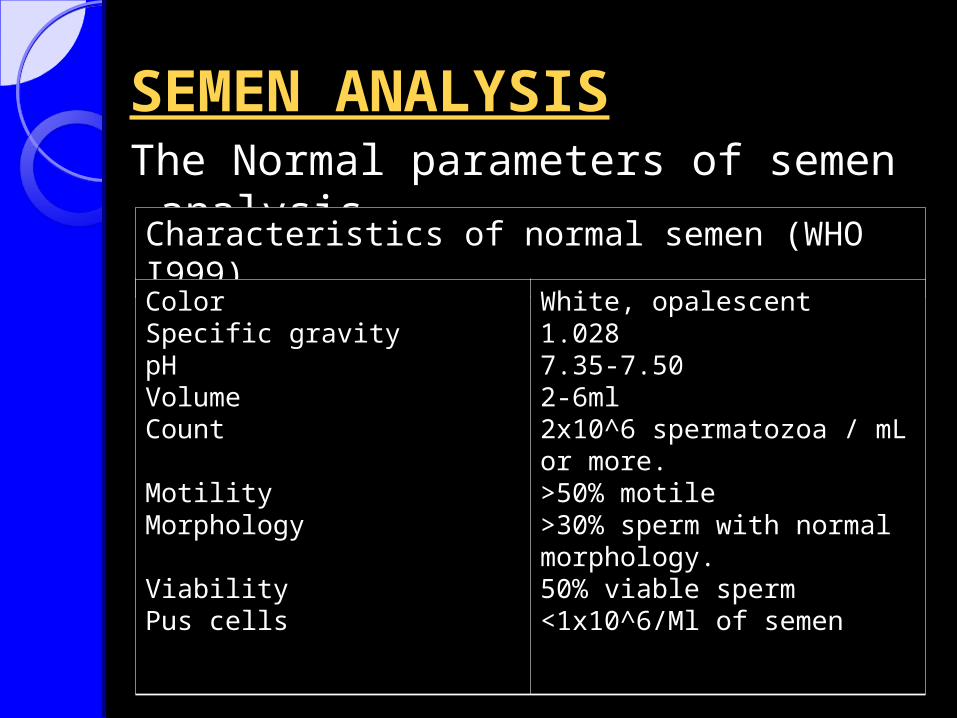
SEMEN ANALYSISSEMEN ANALYSISThe Normal parameters of semen analysis..
Characteristics of normal semen (WHO I999)
ColorSpecific gravitypHVolumeCount
MotilityMorphology
ViabilityPus cells
White, opalescent1.0287.35-7.502-6ml2x10^6 spermatozoa / mL or more.>50% motile>30% sperm with normal morphology.50% viable sperm<1x10^6/Ml of semen
Scrotal ultrasoundScrotal ultrasoundAlthough clinical varicoceles do not require
confirmation with ultrasound examination, color Doppler ultrasound may be required when the clinical examination is difficult.
Demonstration of reversal of venous blood flow with the Valsalva maneuver or spermatic vein diameters of 3 mm or greater support the diagnosis of varicocele.
Scrotal ultrasound is not recommended for screening for subclinical varicoceles as repair of these has not been demonstrated to be of clinical benefit.

TREATMENT
INDICATIONSINDICATIONS1.Palpable varicocele on physical examination.2. Large varicoceles producing clinical symptoms such as dull hemiscrotal discomfort or sense of heaviness.3. 5. Adolescent males with unilateral or bilateral clinical varicoceles & ipsilateral testicular hypotrophy (20% or 3ml volume decrement from the contralateral testis).
Patients with subclinical varicoceles are not candidates for varicocele treatment due to lack of demonstrated efficacy in this population.
The various methods of varicocele treatment all involve ligation or occlusion of dilated gonadal veins.
METHODS OF SURGICAL METHODS OF SURGICAL REPAIRREPAIR
1. Scrotal Approach
2. Retroperitoneal approaches (Open or Laparoscopic)
3. Inguinal Approach
4. Sub-Inguinal Approach
5. Radiographic Occlusion Techniques (Embolization)
SCROTAL APPROACHSCROTAL APPROACH- The very 1st approach for varicocele repair
employed in the early 1900s
- Involves mass ligation & Excision of the varicosed veins.
- Not preferred practically due to the high incidence of testicular artery injury with subsequent impairment of the testicular blood supply, testicular atrophy & more impaired spermatogenesis & fertility.
Retroperitoneal approachesRetroperitoneal approaches- Incision at the level of the internal ring near to the Anterior Superior Iliac Spine.
- Splitting of the External & Internal Oblique Muscles.
- Exposure of the Internal Spermatic Artery & Vein retroperitoneaelly near the ureter where only one or two large veins are present & the testicular artery is not yet branched & so easy to separate.
- High recurrence rate 15% due to preservation of the testicular artery & the peri-arterial venae comitatntes which communicates with the
larger internal spermatic veins causing recurrence.
- Recurrence is prevented by intentional artery ligation, However it may cause testicular atrophy & subsequent azoospermia.
Inguinal and sub-inguinal approachInguinal and sub-inguinal approach-Allows access to external spermatic and
gubernacular veins which causes recurrences if not ligated.
- Inguinal: The incision begins at the externalring and extended laterally 2 to 3.5 cm alongLanger lines.
- Sub-Inguinal:The incision is placed in theskin lines just below the external ring.
Radiographic occlusion techniquesDoes not prevent recurrence (4% to 11%) but allows visualization of all collaterals difficult to be seen with the 2D view.
• Drawbacks:1) Take 1-3 hours to perform compared with 25 to 45
minutesrequired for surgical repair.2) Femoral vein perforation or thrombosis3) Anaphylaxis to radiographic medium4) Recurrence with large varicoceles & with Failure to
cannulate small collaterals.5) Migration of the balloon or coil into the renal vein,
resulting in loss of a kidney, pulmonary embolization.
Operative complicationsOperative complications1. Hydrocele: The most common
complication with incidence 3 -33% (Average 7%).
2. Testicular artery injury: Injury or ligation of the testicular artery carries with it the risk of testicular atrophy and/or impaired spermatogenesis. (which is less likely to occur in children due to compensatory neovascularization).
ReccurenceReccurenceThe incidence of recurrence after varicocele
repair varies from 0.6% to 45%
Recurrence is mostly associated with:1. Pediatric Varicocele2. Non-Magnified Operations3. Retro-peritoneal approaches (that misses
the parallel inguinal collaterals).
THE END