vascular access for haemodialysis · 2018-08-06 · • when patients enter ckd stage 4 ... •...
TRANSCRIPT

Vascular Access for Haemodialysis
Mike Stephens

Overview
• Learning Objectives
• History and development of vascular access
• Standards in vascular access surgery
• Types of vascular access
• Complications

Objectives of the Session
• Understand the different types of vascular access available for
haemodialysis patients
• Know how to assess a patient for vascular access surgery
• Know how to consent a patient for vascular access procedures

Development of Vascular Access Surgery
1657 Sir Christopher Wren invented an instrument for IV injections
1665 Lower reported the first transfusion between dogs
1667 Jean Denys performed the first successful transfusion into humans
1818 James Blundell performed the first trabsfusion of human blood
1901 Karl Landsteiner discovered ABO blood groups
1914 Richard Lewisohn introduced sodium citrate as anticoagulant
1937 Landsteiner and Weiner discovered the Rh factor
1913 Abel, Rowntree and Turner created an artificial kidney
1943 Kolff developed the first practical model for humans
1955 Kolff revised model (including 7 beer cans and a fruit juice can)
1960 Scribner, Dillard, Quinton devised a Teflon-Silastic AV shunt
1966 Brescia, Cimino, Appel and Hurwich described a subcutaneous AVF
1973 Indwelling right atrial catheter developed for TPN
1979 Hickman and colleagues reported their modification
1984 Bothe and colleagues described their Port-a-Cath

“…promptly jumped down from the table, and
apparently oblivious of its hurts, soon began to
fondle its master…..”
Lower, 1665
Development of Vascular Access Surgery
1657 Sir Christopher Wren invented an instrument for IV injections
1665 Lower reported the first transfusion between dogs
1667 Jean Denys performed the first successful transfusion into humans
1818 James Blundell performed the first trabsfusion of human blood
1901 Karl Landsteiner discovered ABO blood groups
1914 Richard Lewisohn introduced sodium citrate as anticoagulant
1937 Landsteiner and Weiner discovered the Rh factor
1913 Abel, Rowntree and Turner created an artificial kidney
1943 Kolff developed the first practical model for humans
1955 Kolff revised model (including 7 beer cans and a fruit juice can)
1960 Scribner, Dillard, Quinton devised a Teflon-Silastic AV shunt
1966 Brescia, Cimino, Appel and Hurwich described a subcutaneous AVF
1973 Indwelling right atrial catheter developed for TPN
1979 Hickman and colleagues reported their modification
1984 Bothe and colleagues described their Port-a-Cath


Development of Vascular Access Surgery
1657 Sir Christopher Wren invented an instrument for IV injections
1665 Lower reported the first transfusion between dogs
1667 Jean Denys performed the first successful transfusion into humans
1818 James Blundell performed the first trabsfusion of human blood
1901 Karl Landsteiner discovered ABO blood groups
1914 Richard Lewisohn introduced sodium citrate as anticoagulant
1937 Landsteiner and Weiner discovered the Rh factor
1913 Abel, Rowntree and Turner created an artificial kidney
1943 Kolff developed the first practical model for humans
1955 Kolff revised model (including 7 beer cans and a fruit juice can)
1960 Scribner, Dillard, Quinton devised a Teflon-Silastic AV shunt
1966 Brescia, Cimino, Appel and Hurwich described a subcutaneous AVF
1973 Indwelling right atrial catheter developed for TPN
1979 Hickman and colleagues reported their modification
1984 Bothe and colleagues described their Port-a-Cath

The Ideal Vascular Access
• Provide safe and effective therapy by enabling the
removal and return of blood via an extracorporeal circuit
• Easy to use
• Reliable
• Minimal risk to the individual

Options

Options
• Arteriovenous fistula
• Arteriovenous graft
• Tunnelled venous catheter
• Non-tunnelled venous catheter
UK Renal Association Guidelines
• 65% of incident HD patients should commence dialysis
with an AV fistula
• 85% of prevalent HD patients should receive dialysis via
a functioning fistula
Clinical Practice Guidelines 2011
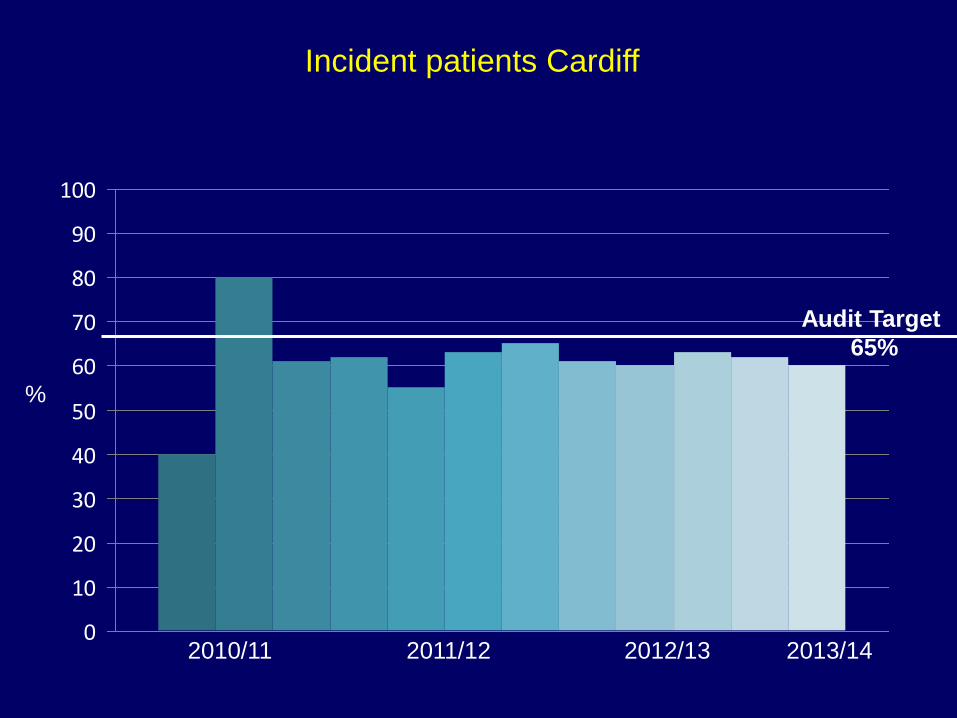
Incident patients Cardiff
%
2010/11 2011/120
10
20
30
40
50
60
70
80
90
100
Audit Target
65%
2012/13 2013/14

Prevalent patients Cardiff
%
2010/11 2011/120
10
20
30
40
50
60
70
80
90
100
2012/13 2013/14
Audit Target
85%

When to start planning for Vascular Access

When to start planning for Vascular Access
• When patients enter CKD stage 4
• Exact timing of placement will depend on rate of decline,
co-morbidities, transplant options and type of access
planned

Fistulogram
Transplant assessment required
Transplant assessment not required
Double OPA with prior duplex Date for surgery Pre-op assessment
One stop access clinic Date for surgery Pre-op assessment
Surgery 1 week post-op OPD review
Prevalent dialysis patient
with fistula problem
4 weeks post-op Doppler USS
Mature
Needle fistula
Discharge
Not Maturing
Review by access
surgeon
Fistulogram Re-do
surgery
Referral to Access Co-
ordinator
CKD patient with declining eGFR<20 (<25 with DM) or likely to require dialysis in
the next 6 months
‘Crash
Lander’

Vascular Access Clinic
Vascular Access Clinic
• General Health (DM/CVD/PVD)
• Medication history (anticoagulants/antiplatelets)
• Occupation
• Dominant Arm
• Superficial veins
• Allen’s test
• Doppler Ultrasound Scan
• Date for Surgery
• Pre-operative Assessment

Options for AV fistulae

Options for AV fistulae
• Snuff-box fistula
• Radiocephalic fistula (wrist or forearm)
• Brachiocubital fistula
• Brachiocephalic fistula
• Brachiobasilic fistula
• Saphenous vein fistula






AV graft options
• Forearm straight graft
• Forearm loop graft
• Brachio-axillary graft
• Femoro-saphenous loop graft
• Femero-femoral loop graft
• Axillo-axillary graft

Assessing maturation
• Clinical
• Doppler Ultrasound
Flow >600ml/min
Cannulation segment >10cm long or two 4cm segments
Outflow vein diameter >6mm
Cannulation segment <6mm from skin surface

Complications of Vascular Access

Thrombosis
• 1 year patency AVFs approx. 65%
• Many factors
small vessels
dehydration
hypotension
venous outflow obstruction
• Primary patency at 2 years:-
AVF 43% AVG 31%
• Secondary patency at 2 years:-
AVF 64% AVG 60%

High Output Heart Failure
• Rapid flow changes immediately after construction
RC AVF 250ml/min
BC AVF 600ml/min
• Heart Failure relatively uncommon (surprisingly)
• Probably need 25%-50% cardiac output through fistula
to result in failure
• Revision possible

Venous Hypertension
• Rapid if central stenosis
• May be due to retrograde flow
• Treatment depends on exact cause
May get better
May need to ligate fistula
Consider venogram

Aneurysms
• Pseudo-aneurysms
Needling sites
Infection
• True aneurysms
If skin threatened may bleed
Management depends on size/symptoms/skin

Ischaemic Steal Syndrome
• Prevalence 10-20% (symptomatic), 4% requiring intervention
• More likely and more rapid with AVG
• Diagnosis clinical plus Doppler assessment
• Difficult to predict
• Operative treatments:-
Ligation
Banding
DRIL
RUDI

Neuropathy
• Carpal tunnel syndrome-like symptoms
• Ischaemic Monomelic Neuropathy (Vascular Access
Neuropathic Syndrome)

Summary
• Vascular Access takes careful planning
• High failure rates but successful outcomes achievable
• Complications are common but usually manageable