vcd and asthma: slp perspectivegetasthmahelp.org/documents/searl-vcd_slp-perspective.pdf · vcd and...
TRANSCRIPT
VCD and Asthma: SLP PerspectiveJeff Searl, Ph.D., CCC-SLPDepartment of Communicative Sciences & DisordersMichigan State University
The Name Issue• 1983 – Vocal Cord Dysfunction (VCD) coined by Christopher et al
(much earlier descriptions of the condition back to 1842 – usually associated with “hysterical patients”)
• Since – at least 40 different labels have been association
• Common nomenclature task force -2015 –
• Inducible Laryngeal Obstruction (ILO)• American College of Chest Physicians; European Respiratory Society;
European Laryngological Society• But not catching on as a universal term
The Name Issue from the SLP Perspective• Generally – use VCD to facilitate communication among
the care team and with patients
• But in our hearts – term is…
• Non-specific to the condition
• Overlaps with a large swath of others who demonstrate various types of vocal cord dysfunction with whom we work
• Preference for Paradoxical Vocal Cord Motion (PVCM) Disorder
Clinical Presentation - broadly• For years thought to be
“psychological”
• Not so now – broad patient base
• 65% > 19 years old• Median ages
• Adults = 36 years• Peds = 14 years
• Does seem to be female > male
• Sx: chronic in 85%, acute in 15%
Wide range of patient report Air hunger, chest tightness, tension in
throat, choking, trouble swallowing, throat clear, aphonia or dysphonia, cough, etc.
Fear, anxiety, panic – worsening of other Sx
Triggers/associated conditions: exercise, URI, reflux, sinus drainage, stress, odors == laryngeal hypersensitivity
‘Refractory asthma’ often part of the clinical picture [42% of those wihVCD misdx as asthma for average of 9 years; probis 33% with VCD have concomitant asthma (Traister et al 2013)]
For SLPS, Clinical Presentation is such that…
• SLP is NOT usually the first person that they go to
• General practitioners, Asthma and Allergy specialists, sometimes Ear, Nose, Throat docs
SLPs often asked to contribute to diagnostic process
Ruling in/out other possibilities
Directly confirming the laryngeal behavior consistent with VCD
Assessing stimulability for behavioral change
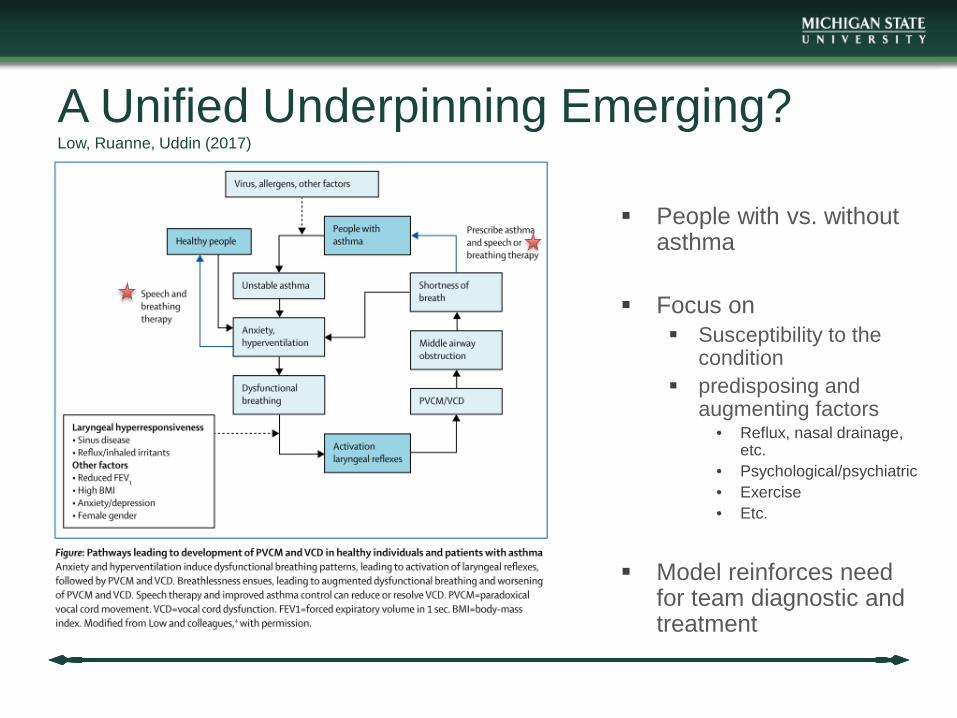
A Unified Underpinning Emerging?Low, Ruanne, Uddin (2017)
People with vs. without asthma
Focus on Susceptibility to the
condition predisposing and
augmenting factors• Reflux, nasal drainage,
etc.• Psychological/psychiatric• Exercise• Etc.
Model reinforces need for team diagnostic and treatment
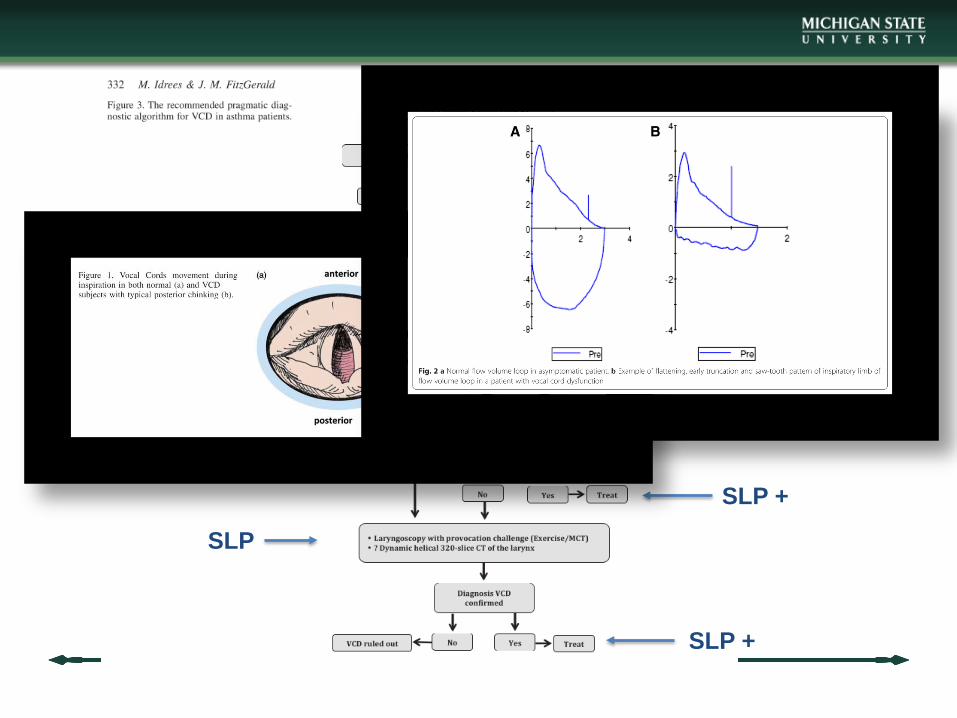
SLP
SLP +
SLP
SLP +
SLP +
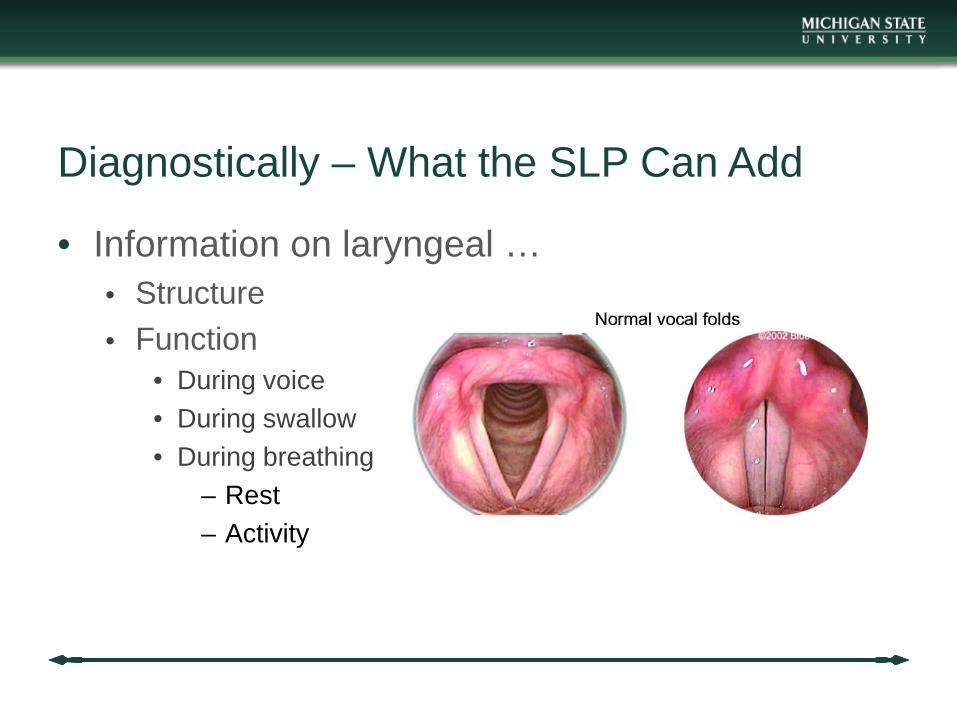
Diagnostically – What the SLP Can Add
• Information on laryngeal …• Structure• Function
• During voice• During swallow• During breathing
– Rest– Activity
Diagnostically – What the SLP Can Add
• Flexible laryngoscopy = visualization of the event itself• Gold-standard to date (but with limits)
• Generally with VCD• Vocal folds adduct anteriorly with glottal gap posteriorly• During inspiration, possibly expiration, possibly both
• But subjective; not always able to catch them during symptom occurrence (challenge tests – panting, exercise, methacholine, fast-extended talking)
flexendosc_exercise based PVCM_non exercise based
What are we [SLP] ruling out?
• Structural issues• Obstruction in larynx,
supraglottic region• Cysts, papilloma,
malignancy• Stenosis• Laryngeal web• Swellings
– Epiglottis– Ingestion or
inhalation trauma• ETC.!
Functional issues Inspiratory phonation Vocal fold paralysis Psychogenic
(somatoform, conversion, malingering)
attempting to
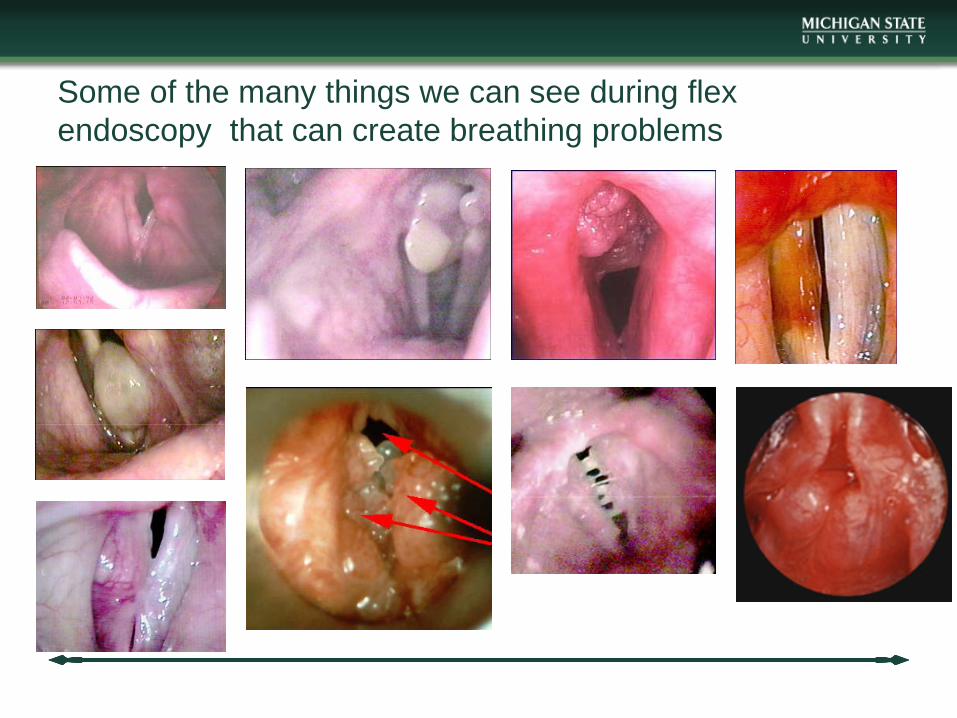
Some of the many things we can see during flex endoscopy that can create breathing problems
Multidisciplinary Team for Dx – SLP has a part
• Pulmonology, Asthma, Allergy specialists• ENT• Psychology/Psychiatry• GI• Neurology• Endocrinology• Infectious Disease• Athletic trainer, physical therapist
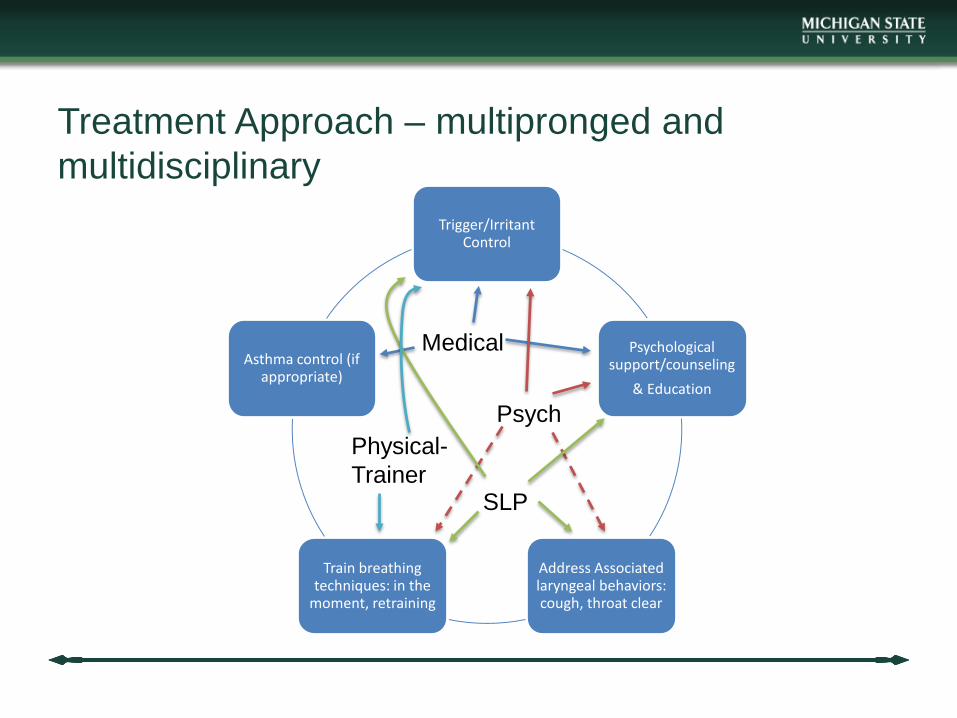
Treatment Approach – multipronged and multidisciplinary
Trigger/Irritant Control
Psychological support/counseling
& Education
Address Associated laryngeal behaviors: cough, throat clear
Train breathing techniques: in the
moment, retraining
Asthma control (if appropriate)
Medical
Psych
SLP
Physical-Trainer
SLP Treatment
• Education• The condition – normal physiology vs. their situation
• What seems to trigger it for them; ways to control triggers
• Good vocal hygiene
• Supportive counseling• Reassurance• Benign nature, self-limited
SLP Treatment
• No studies comparing 1 vs another for superiority
• A few approaches – specific regimens vary
• Remove the focus on the larynx/neck during breathing• Abdominal breathing• Increased resistance at the lips/mouth (“sh,” “f,” “s”)• “ha” + sniff• pant
• Possibly use inspiratory muscle strength training – case studies suggesting success in athletes with VCD
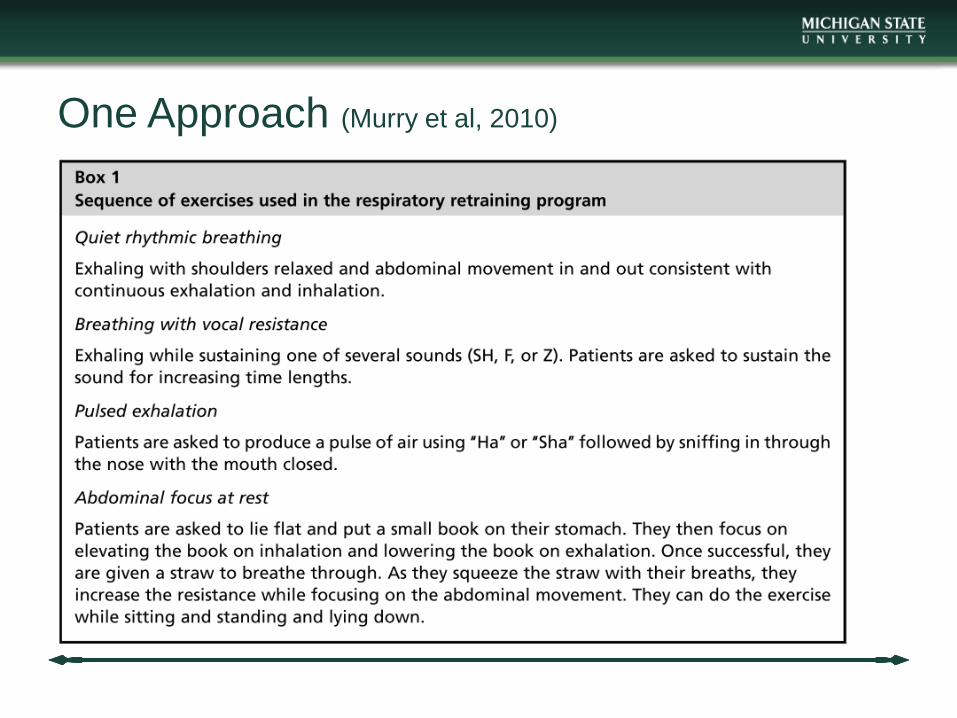
One Approach (Murry et al, 2010)
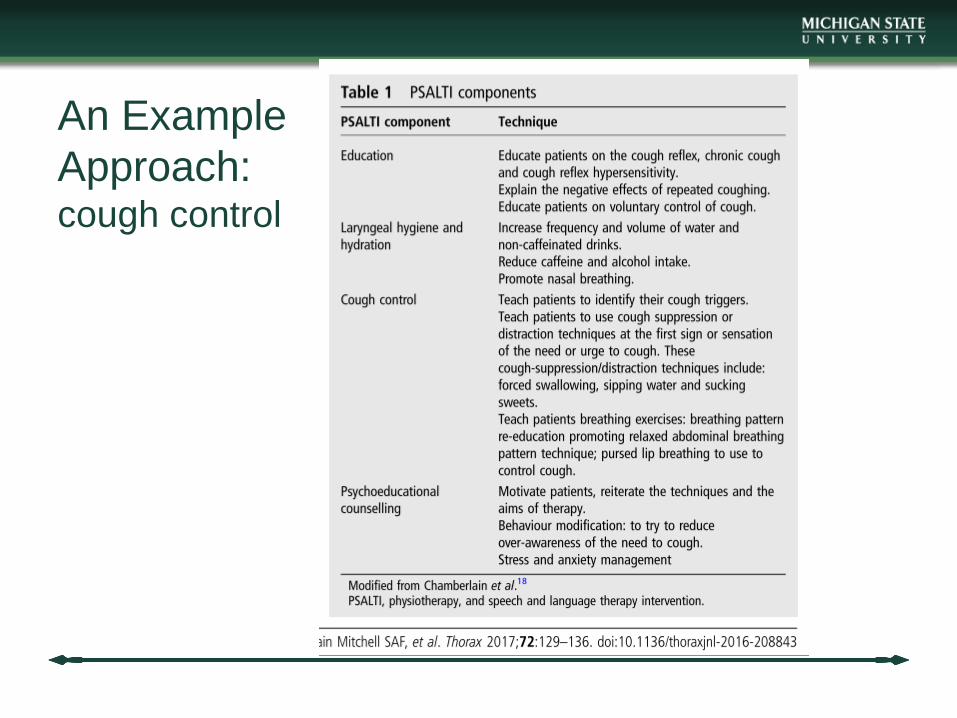
An Example Approach:cough control
Other foci of SLP Tx• Relaxation of oropharyngeal musculature (Christopher et al, 1983)
• Patient education that behavior can be controlled (cognitive-behavioral therapy; Campainha et al, 2012)
• Visualization re: “open throat breathing” (Pinhoe et al, 1997)
• Biofeedback re: breathing (Altman et al, 2000)
• Multimodality with medical/psychological Tx - many
Concluding Thoughts• Seems some combo of behavioral, cognitive, psychological, medical
intervention can help – assumes proper diagnosis
• Management of triggers is critical – some are medical/physiological, others are environmental, still others are behavioral and psychololgical
• SLP treatment research – seems we can be helpful; wanting more stringent assessment of protocols and comparison of approaches so we know what might work best for what patient.