ventricular remodeling during long-term right ventricular pacing following his bundle ablation
TRANSCRIPT

Tlwiciithp
Dpfisopcp
Iec
z
0d
Ventricular Remodeling During Long-Term Right Ventricular Pacing FollowingHis Bundle Ablation
Kevin Vernooy, MDa,b,*, Barbara Dijkman, MD, PhDa, Emile C. Cheriex, MD, PhDa,Frits W. Prinzen, PhDb, and Harry J.G.M. Crijns, MD, PhDa
To investigate ventricular remodeling during long-term right ventricular (RV) pacingafter His bundle ablation (HBA) in patients with atrial arrhythmias, a retrospectiveanalysis was performed on echocardiographic data from 45 patients (mean age 57 �11 years) with atrial arrhythmias who underwent HBA and pacemaker implantation(HBA-PI) to control ventricular rate. Echocardiography was performed 1 year beforeHBA-PI, and up to 7 � 2 years of follow-up was conducted. An inverse linear relationwas found between the relative increase of left ventricular (LV) end-diastolic diam-eter (EDD) during long-term RV pacing and LVEDD before HBA-PI (r � �0.61,p <0.001). Patients were divided into 2 groups: those with LVEDDs smaller than themean LVEDD of 50 mm (group I, 46 � 2 mm, n � 28) and those with LVEDDs >50mm (group II, 56 � 4 mm, n � 17). Before HBA-PI, patients in group I hadsignificantly smaller LV weights (167 � 44 vs 238 � 56 g) and LV end-systolicdiameters (30 � 2 vs 42 � 7 mm) and higher LV ejection fractions (64 � 5% vs 49 �12%) than those in group II. In group I, long-term RV pacing increased LVEDD, LVend-systolic diameter, LV weight, and left atrial diameter; increased mitral regurgi-tation; and decreased the LV ejection fraction and LV fractional shortening. Nosignificant changes were observed during long-term RV pacing in group II. Inconclusion, long-term RV pacing after HBA adversely affects LV structure andfunction in patients with initially normal LV dimensions and function. © 2006
Elsevier Inc. All rights reserved. (Am J Cardiol 2006;97:1223–1227)rrtddLmcr
ptt1�
seedtvfptc
he aim of the present study was to investigate changes ineft ventricular (LV) dimensions and function in patientsho experience permanent right ventricular (RV) apex pac-
ng. For this purpose, we performed a retrospective echo-ardiographic analysis in patients during long-term RV pac-ng after His bundle ablation (HBA). We sought to gainnsight into the balance between the adverse effects of long-erm RV pacing and the beneficial hemodynamic effects ofeart rate regularization by HBA and tried to identify thoseatients who deteriorated as a consequence of RV pacing.
• • •uring the past decade, 60 patients underwent HBA andacemaker implantation (HBA-PI) at our institute. Forty-ve patients had undergone echocardiographic studieshortly before as well as after HBA-PI and were included inur analysis. Echocardiographic data were taken from ourrospective electronic echocardiographic database. Echo-ardiographic investigations were performed in the standardarasternal, apical, and subxiphoidal views according to the
Departments of aCardiology and bPhysiology, Cardiovascular Researchnstitute Maastricht, University Hospital Maastricht, Maastricht, The Neth-rlands. Manuscript received September 1, 2005; revised manuscript re-eived and accepted November 1, 2005.
Dr. Vernooy was supported by a grant from The Netherlands Organi-ation for Health Research and Development, Den Haag, The Netherlands.
* Corresponding author: Tel: 31-43-3881200; fax: 31-43-3884166.
lE-mail address: [email protected] (K. Vernooy).002-9149/06/$ – see front matter © 2006 Elsevier Inc. All rights reserved.oi:10.1016/j.amjcard.2005.11.044
ecommendations of the American Society of Echocardiog-aphy. To investigate global and regional LV remodeling,he following dimensions were measured: LV end-diastoliciameter (EDD) and end-systolic diameter and the end-iastolic thickness of the septum and LV posterior wall. TheV ejection fraction and LV fractional shortening wereeasured to study LV pump function. LV weight was cal-
ulated from LVEDD and regional wall thickness. Mitralegurgitation was analyzed by Doppler echocardiography.
To facilitate the combination of the data from all 45atients, echocardiographic follow-up was clustered in 4ime frames: before HBA-PI (�0.4 � 0.9 years; 45 pa-ients), �1 year after HBA-PI (0.6 � 0.4 years; 22 patients),to 5 years after HBA-PI (2.7 � 1.0 years; 26 patients), and5 years after HBA-PI (7.7 � 2.4 years; 33 patients).All values are given as mean values with their corre-
ponding SDs. Wilcoxon’s test was used to analyze differ-nces between baseline and long-term RV pacing withinach group. The Mann-Whitney test was used to analyzeifferences between the groups. Changes in LVEDD overime were evaluated using repeated-measures analysis ofariance. If analysis of variance indicated a significant dif-erence between time points, Bonferroni’s post hoc test waserformed to compare selected pairs of time points. In allests, a p value of �0.05 (2 sided) was considered statisti-ally significant.
HBA was performed to achieve complete atrioventricu-
ar block and was followed by the implantation of either awww.AJConline.org
Dar
wbdPRi0
vagm(mGaw
gcyndpattabLgt
(dc
sgtcrb
RdtGd
wpfio
T
Ftp
FRsioca
1224 The American Journal of Cardiology (www.AJConline.org)
DD or a VVI pacemaker, for paroxysmal or chronic atrialrrhythmia, respectively. The ventricular pacing lead wasoutinely placed in the RV apex.
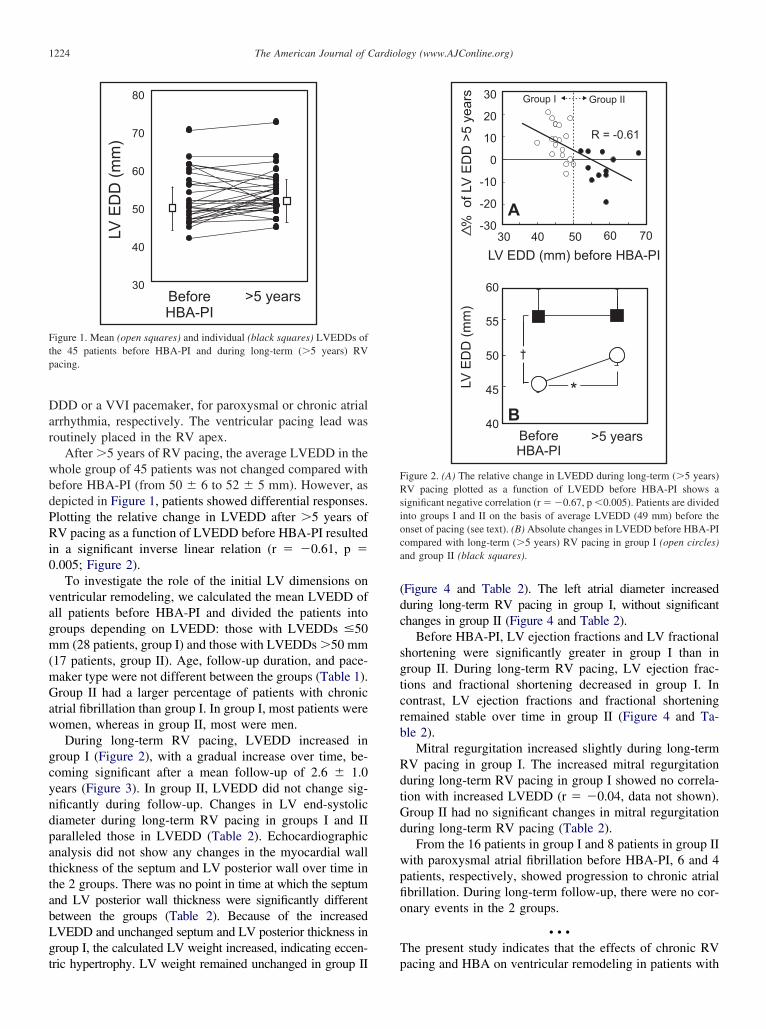
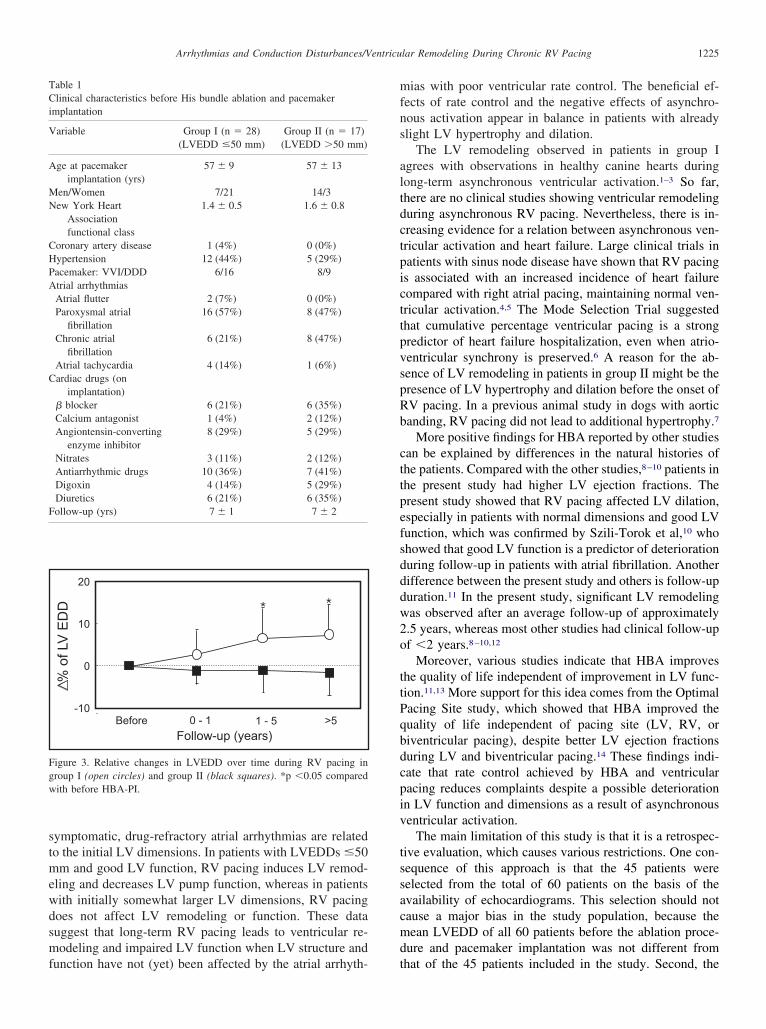
After �5 years of RV pacing, the average LVEDD in thehole group of 45 patients was not changed compared withefore HBA-PI (from 50 � 6 to 52 � 5 mm). However, asepicted in Figure 1, patients showed differential responses.lotting the relative change in LVEDD after �5 years ofV pacing as a function of LVEDD before HBA-PI resulted
n a significant inverse linear relation (r � �0.61, p �.005; Figure 2).
To investigate the role of the initial LV dimensions onentricular remodeling, we calculated the mean LVEDD ofll patients before HBA-PI and divided the patients intoroups depending on LVEDD: those with LVEDDs �50m (28 patients, group I) and those with LVEDDs �50 mm
17 patients, group II). Age, follow-up duration, and pace-aker type were not different between the groups (Table 1).roup II had a larger percentage of patients with chronic
trial fibrillation than group I. In group I, most patients wereomen, whereas in group II, most were men.During long-term RV pacing, LVEDD increased in
roup I (Figure 2), with a gradual increase over time, be-oming significant after a mean follow-up of 2.6 � 1.0ears (Figure 3). In group II, LVEDD did not change sig-ificantly during follow-up. Changes in LV end-systoliciameter during long-term RV pacing in groups I and IIaralleled those in LVEDD (Table 2). Echocardiographicnalysis did not show any changes in the myocardial wallhickness of the septum and LV posterior wall over time inhe 2 groups. There was no point in time at which the septumnd LV posterior wall thickness were significantly differentetween the groups (Table 2). Because of the increasedVEDD and unchanged septum and LV posterior thickness inroup I, the calculated LV weight increased, indicating eccen-
igure 1. Mean (open squares) and individual (black squares) LVEDDs ofhe 45 patients before HBA-PI and during long-term (�5 years) RVacing.
ric hypertrophy. LV weight remained unchanged in group II p
Figure 4 and Table 2). The left atrial diameter increaseduring long-term RV pacing in group I, without significanthanges in group II (Figure 4 and Table 2).
Before HBA-PI, LV ejection fractions and LV fractionalhortening were significantly greater in group I than inroup II. During long-term RV pacing, LV ejection frac-ions and fractional shortening decreased in group I. Inontrast, LV ejection fractions and fractional shorteningemained stable over time in group II (Figure 4 and Ta-le 2).
Mitral regurgitation increased slightly during long-termV pacing in group I. The increased mitral regurgitationuring long-term RV pacing in group I showed no correla-ion with increased LVEDD (r � �0.04, data not shown).roup II had no significant changes in mitral regurgitationuring long-term RV pacing (Table 2).
From the 16 patients in group I and 8 patients in group IIith paroxysmal atrial fibrillation before HBA-PI, 6 and 4atients, respectively, showed progression to chronic atrialbrillation. During long-term follow-up, there were no cor-nary events in the 2 groups.
• • •he present study indicates that the effects of chronic RV
igure 2. (A) The relative change in LVEDD during long-term (�5 years)V pacing plotted as a function of LVEDD before HBA-PI shows a
ignificant negative correlation (r � �0.67, p �0.005). Patients are dividednto groups I and II on the basis of average LVEDD (49 mm) before thenset of pacing (see text). (B) Absolute changes in LVEDD before HBA-PIompared with long-term (�5 years) RV pacing in group I (open circles)nd group II (black squares).
acing and HBA on ventricular remodeling in patients with
stmewdsmf
mfns
altdctpicttpvspRb
cttpefsdddw2o
ttPqbdcpiv
tssacmd
Fgw
TCi
V
A
MN
CHPA
C
F
1225Arrhythmias and Conduction Disturbances/Ventricular Remodeling During Chronic RV Pacing
ymptomatic, drug-refractory atrial arrhythmias are relatedo the initial LV dimensions. In patients with LVEDDs �50m and good LV function, RV pacing induces LV remod-
ling and decreases LV pump function, whereas in patientsith initially somewhat larger LV dimensions, RV pacingoes not affect LV remodeling or function. These datauggest that long-term RV pacing leads to ventricular re-odeling and impaired LV function when LV structure and
igure 3. Relative changes in LVEDD over time during RV pacing inroup I (open circles) and group II (black squares). *p �0.05 comparedith before HBA-PI.
able 1linical characteristics before His bundle ablation and pacemaker
mplantation
ariable Group I (n � 28) Group II (n � 17)(LVEDD �50 mm) (LVEDD �50 mm)
ge at pacemakerimplantation (yrs)
57 � 9 57 � 13
en/Women 7/21 14/3ew York Heart
Associationfunctional class
1.4 � 0.5 1.6 � 0.8
oronary artery disease 1 (4%) 0 (0%)ypertension 12 (44%) 5 (29%)acemaker: VVI/DDD 6/16 8/9trial arrhythmiasAtrial flutter 2 (7%) 0 (0%)Paroxysmal atrial
fibrillation16 (57%) 8 (47%)
Chronic atrialfibrillation
6 (21%) 8 (47%)
Atrial tachycardia 4 (14%) 1 (6%)ardiac drugs (on
implantation)� blocker 6 (21%) 6 (35%)Calcium antagonist 1 (4%) 2 (12%)Angiontensin-converting
enzyme inhibitor8 (29%) 5 (29%)
Nitrates 3 (11%) 2 (12%)Antiarrhythmic drugs 10 (36%) 7 (41%)Digoxin 4 (14%) 5 (29%)Diuretics 6 (21%) 6 (35%)ollow-up (yrs) 7 � 1 7 � 2
unction have not (yet) been affected by the atrial arrhyth- t
ias with poor ventricular rate control. The beneficial ef-ects of rate control and the negative effects of asynchro-ous activation appear in balance in patients with alreadylight LV hypertrophy and dilation.
The LV remodeling observed in patients in group Igrees with observations in healthy canine hearts duringong-term asynchronous ventricular activation.1–3 So far,here are no clinical studies showing ventricular remodelinguring asynchronous RV pacing. Nevertheless, there is in-reasing evidence for a relation between asynchronous ven-ricular activation and heart failure. Large clinical trials inatients with sinus node disease have shown that RV pacings associated with an increased incidence of heart failureompared with right atrial pacing, maintaining normal ven-ricular activation.4,5 The Mode Selection Trial suggestedhat cumulative percentage ventricular pacing is a strongredictor of heart failure hospitalization, even when atrio-entricular synchrony is preserved.6 A reason for the ab-ence of LV remodeling in patients in group II might be theresence of LV hypertrophy and dilation before the onset ofV pacing. In a previous animal study in dogs with aorticanding, RV pacing did not lead to additional hypertrophy.7
More positive findings for HBA reported by other studiesan be explained by differences in the natural histories ofhe patients. Compared with the other studies,8–10 patients inhe present study had higher LV ejection fractions. Theresent study showed that RV pacing affected LV dilation,specially in patients with normal dimensions and good LVunction, which was confirmed by Szili-Torok et al,10 whohowed that good LV function is a predictor of deteriorationuring follow-up in patients with atrial fibrillation. Anotherifference between the present study and others is follow-upuration.11 In the present study, significant LV remodelingas observed after an average follow-up of approximately.5 years, whereas most other studies had clinical follow-upf �2 years.8–10,12
Moreover, various studies indicate that HBA improveshe quality of life independent of improvement in LV func-ion.11,13 More support for this idea comes from the Optimalacing Site study, which showed that HBA improved theuality of life independent of pacing site (LV, RV, oriventricular pacing), despite better LV ejection fractionsuring LV and biventricular pacing.14 These findings indi-ate that rate control achieved by HBA and ventricularacing reduces complaints despite a possible deteriorationn LV function and dimensions as a result of asynchronousentricular activation.
The main limitation of this study is that it is a retrospec-ive evaluation, which causes various restrictions. One con-equence of this approach is that the 45 patients wereelected from the total of 60 patients on the basis of thevailability of echocardiograms. This selection should notause a major bias in the study population, because theean LVEDD of all 60 patients before the ablation proce-
ure and pacemaker implantation was not different from
hat of the 45 patients included in the study. Second, the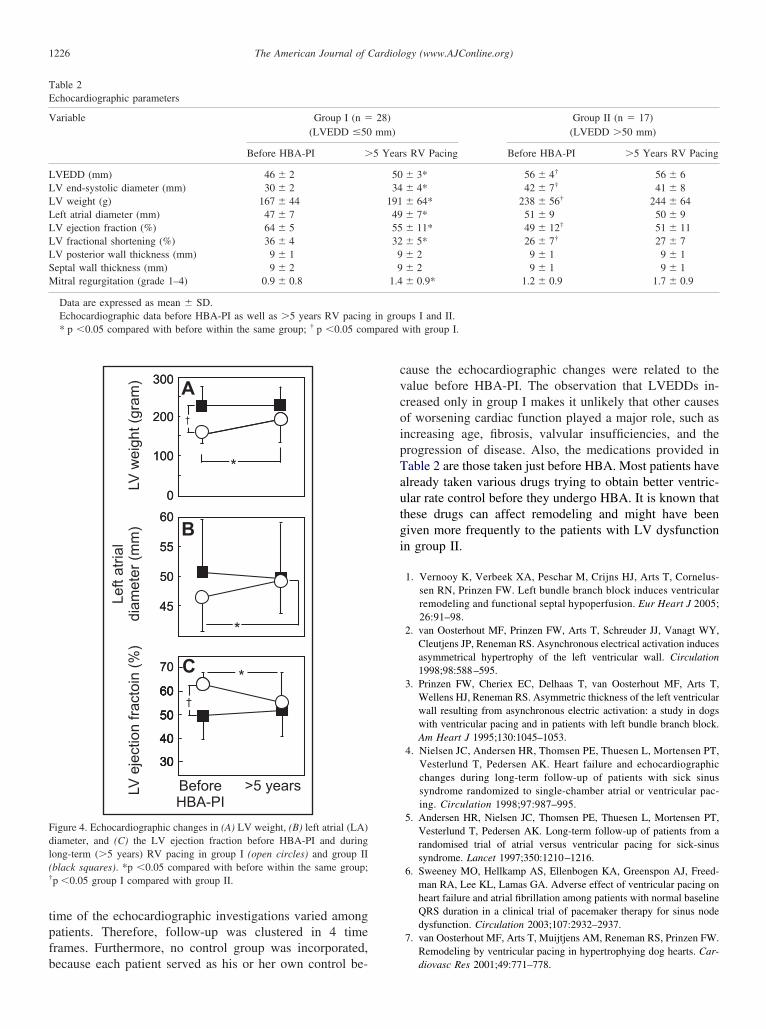
tpfb
cvcoipTautgi
Fdl(†
TE
V
LLLLLLLSM
pared
1226 The American Journal of Cardiology (www.AJConline.org)
ime of the echocardiographic investigations varied amongatients. Therefore, follow-up was clustered in 4 timerames. Furthermore, no control group was incorporated,
igure 4. Echocardiographic changes in (A) LV weight, (B) left atrial (LA)iameter, and (C) the LV ejection fraction before HBA-PI and duringong-term (�5 years) RV pacing in group I (open circles) and group IIblack squares). *p �0.05 compared with before within the same group;p �0.05 group I compared with group II.
able 2chocardiographic parameters
ariable Group I (n �
(LVEDD �50
Before HBA-PI �
VEDD (mm) 46 � 2V end-systolic diameter (mm) 30 � 2V weight (g) 167 � 44eft atrial diameter (mm) 47 � 7V ejection fraction (%) 64 � 5V fractional shortening (%) 36 � 4V posterior wall thickness (mm) 9 � 1eptal wall thickness (mm) 9 � 2itral regurgitation (grade 1–4) 0.9 � 0.8
Data are expressed as mean � SD.Echocardiographic data before HBA-PI as well as �5 years RV pacing* p �0.05 compared with before within the same group; † p �0.05 com
ecause each patient served as his or her own control be-
ause the echocardiographic changes were related to thealue before HBA-PI. The observation that LVEDDs in-reased only in group I makes it unlikely that other causesf worsening cardiac function played a major role, such asncreasing age, fibrosis, valvular insufficiencies, and therogression of disease. Also, the medications provided inable 2 are those taken just before HBA. Most patients havelready taken various drugs trying to obtain better ventric-lar rate control before they undergo HBA. It is known thathese drugs can affect remodeling and might have beeniven more frequently to the patients with LV dysfunctionn group II.
1. Vernooy K, Verbeek XA, Peschar M, Crijns HJ, Arts T, Cornelus-sen RN, Prinzen FW. Left bundle branch block induces ventricularremodeling and functional septal hypoperfusion. Eur Heart J 2005;26:91–98.
2. van Oosterhout MF, Prinzen FW, Arts T, Schreuder JJ, Vanagt WY,Cleutjens JP, Reneman RS. Asynchronous electrical activation inducesasymmetrical hypertrophy of the left ventricular wall. Circulation1998;98:588–595.
3. Prinzen FW, Cheriex EC, Delhaas T, van Oosterhout MF, Arts T,Wellens HJ, Reneman RS. Asymmetric thickness of the left ventricularwall resulting from asynchronous electric activation: a study in dogswith ventricular pacing and in patients with left bundle branch block.Am Heart J 1995;130:1045–1053.
4. Nielsen JC, Andersen HR, Thomsen PE, Thuesen L, Mortensen PT,Vesterlund T, Pedersen AK. Heart failure and echocardiographicchanges during long-term follow-up of patients with sick sinussyndrome randomized to single-chamber atrial or ventricular pac-ing. Circulation 1998;97:987–995.
5. Andersen HR, Nielsen JC, Thomsen PE, Thuesen L, Mortensen PT,Vesterlund T, Pedersen AK. Long-term follow-up of patients from arandomised trial of atrial versus ventricular pacing for sick-sinussyndrome. Lancet 1997;350:1210–1216.
6. Sweeney MO, Hellkamp AS, Ellenbogen KA, Greenspon AJ, Freed-man RA, Lee KL, Lamas GA. Adverse effect of ventricular pacing onheart failure and atrial fibrillation among patients with normal baselineQRS duration in a clinical trial of pacemaker therapy for sinus nodedysfunction. Circulation 2003;107:2932–2937.
7. van Oosterhout MF, Arts T, Muijtjens AM, Reneman RS, Prinzen FW.Remodeling by ventricular pacing in hypertrophying dog hearts. Car-
Group II (n � 17)(LVEDD �50 mm)
s RV Pacing Before HBA-PI �5 Years RV Pacing
� 3* 56 � 4† 56 � 6� 4* 42 � 7† 41 � 8� 64* 238 � 56† 244 � 64� 7* 51 � 9 50 � 9� 11* 49 � 12† 51 � 11� 5* 26 � 7† 27 � 7� 2 9 � 1 9 � 1� 2 9 � 1 9 � 1� 0.9* 1.2 � 0.9 1.7 � 0.9
ups I and II.with group I.
28)mm)
5 Year
5034
19149553299
1.4
in gro
diovasc Res 2001;49:771–778.

1
1
1
1
1
1227Arrhythmias and Conduction Disturbances/Ventricular Remodeling During Chronic RV Pacing
8. Rodriguez LM, Smeets JL, Xie B, de Chillou C, Cheriex E, PietersF, Metzger J, den Dulk K, Wellens HJ. Improvement in left ven-tricular function by ablation of atrioventricular nodal conduction inselected patients with lone atrial fibrillation. Am J Cardiol 1993;72:1137–1141.
9. Edner M, Caidahl K, Bergfeldt L, Darpo B, Edvardsson N, RosenqvistM. Prospective study of left ventricular function after radiofrequencyablation of atrioventricular junction in patients with atrial fibrillation.Br Heart J 1995;74:261–267.
0. Szili-Torok T, Kimman GP, Theuns D, Poldermans D, Roelandt JR,Jordaens LJ. Deterioration of left ventricular function following atrio-ventricular node ablation and right ventricular apical pacing in patientswith permanent atrial fibrillation. Europace 2002;4:61–65.
1. Szili-Torok T, Bountioukos M, Muskens AJ, Theuns DA, Polder-mans D, Roelandt JR, Jordaens LJ. The presence of contractile
reserve has no predictive value for the evolution of left ventricularfunction following atrio-ventricular node ablation in patients withpermanent atrial fibrillation. Eur J Echocardiogr 2005;6:344 –350.
2. Weerasooriya R, Davis M, Powell A, Szili-Torok T, Shah C, WhalleyD, Kanagaratnam L, Heddle W, Leitch J, Perks A, et al. The AustralianIntervention Randomized Control of Rate in Atrial Fibrillation Trial(AIRCRAFT). J Am Coll Cardiol 2003;41:1697–1702.
3. Brignole M, Menozzi C, Gianfranchi L, Musso G, Mureddu R, BottoniN, Lolli G. Assessment of atrioventricular junction ablation and VVIRpacemaker versus pharmacological treatment in patients with heartfailure and chronic atrial fibrillation: a randomized, controlled study.Circulation 1998;98:953–960.
4. Brignole M, Gammage M, Puggioni E, Alboni P, Raviele A, SuttonR, Vardas P, Bongiorni MG, Bergfeldt L, Menozzi C, Musso G.Comparative assessment of right, left, and biventricular pacing inpatients with permanent atrial fibrillation. Eur Heart J 2005;26:
712–722.