verapamil for the suppression of idiopathic ventricular tachycardia of left bundle branch block-like...
TRANSCRIPT
Gill et al. November 1993
American Heart Journal
combinations of vagal and sympathetic stimulation that result in a constant spontaneous sinus cycle length. Circ Res 198’7; 60:942-51.
25. Lee RJ, Liem B, Cohen TJ, Franz MR. Relation between re- polarization and refractoriness in the human ventricle: cycle length dependence and effect of procainamide. J Am Co11 Cardiol 1992;19:614-8.
26. Thdinpson KA, Blair IA, Woosley RL, Roden DM. Compara- tive in vitro electrophysiology of quinidine, its major metab- olites and dihydroquinidine. J Pharmacol Exp Ther 1987; 241: 84-91.
27. Morady F, DiCarlo LA, Baerman JM, Krol RB. Rate-depen- dent effects of intravenous lidocaine, procainamide, and ami- odarone on intraventricular conduction. J Am Co11 Cardiol 198$:6:179-S.%
28. Dangman KH, Hoffman BF. In vivo and in vitro antiarrhyth- mic and arrhythmogenic effects of N-acetyl procainamide. J Pharmacol Exp Ther 1981;217:851-6.
29. Shechter JA, Caine R, Friehling T, Kowey PR, Engel TR. Ef- fect of procainamide on dispersion of ventricular refractori- ness. Am J Cardiol 1983;52:2’79-82.
30.
31.
32.
33.
34.
Watanabe T, Raut&arju PM, McDonald TF. Ventricular ac- tion potentials, ventricular extracellular potentials, and the ECG of guinea pig. Circ Res 1985;57:362-9. Franz MR, Bargheer K, Rafflenbeul W, Haverich A, Lichtlen PR. Monophasic action potential mapping in human subjects with normal electrocardiograms: direct evidence for the gen- esis of the T wave. Circulation 1987;75:379-89. Kuo CS, Munakata K, Reddy CP, Surawicz B. Characteristics and possible mechanism of ventricular arrhythmia dependent on the dispersion of action potential duration. Circulation 1983; 67:1356-62. Kuo CS, Atarashi H, Reddy CP. Dispersion of ventricular re- polarization and arrhythmia: study of two consecutive ven- tricular premature complexes. Circulation 1985;72:370-6. Kowey PR, Friehling TD, O’Connor KM. The effect of bretylium and clofilium on dispersion of refractoriness and vulnerability to ventricular fibrillation in the ischemic feline heart. A~H~~~~J1985;110:363-70.
Ve~ra~pamil for the wppression of idilop,qthic ventriwlar tachycardia of left .bundle bra.nch block-Mice morphology
This study examines the efficacy of verapamil for the suppression of idiopathic ventricular tachycardia (VT) of left bundle branch blqck &BBB-like morphology. Forty-two patients (mean age 36.2 rt 12.1 years;,20 men and 22’women) with’VT and without shy underlying cardiac abnormality on clinical examination and noninvasive investigation were studied. The inducibility of clinical VT was examined by treadmili exercise testing and programmed ventricular stimulation (PVS). In 29 patients VT was inducible by exercise testing, in 24 by PVS, and in 23 there was evidence of VT on Holter monitoring. After baseline testing, patients were treated with verapamil 120 mg thrice daily for at least 5 half-lives for the drug to load before evaluation. With Holter monitoring, 74% of, patients with evidence of VT at baseline testing demonstrated a change of status from nonsustained VT to no VT or from sustained VT to nonsustained VT. Four patients had nonsustained VT during verapamil treatment but no VT at baseline. There was a significant reduction in the number of ventricular ectopic beatS over 24 hours (baseline: 15541 -t 17599 vs verapamil treatment: 6692 t 15582, p < 0.01). Exercise-induced VT was suppressed in 56% of patients with VT during baseline testing, but no effect of verapamil on the tachycardia was obsetied in 26%. The remiining patients demonstrated a partial response to verapamil; the rate of VT was unchanged, although the duration qf the runs was reduced. Sustained monomorphic VT was inducible in only 5 patients, of wliom 4 were rendered noninducible; 1 patient remained inducible. However, of the 13 patients with nonsustained VT inducible at baseline, 4 became sustain’ed, of which 2 were hemodynamically unstable. There was no obvious difference in the age or sex distribution of the patients, axis of VT, presence of abnormal cardiac histology, or late potentials among patients responding to verapamil during Holter monitoring or exercise testing. VT of iair inferior axis was more likely to respond to verapamil, whereas VT of a superior axis did not respond to verapamil during Hdlter monitoring. W& conclude that idiopathic VT of &5BB-like morphology can be suppressed in approximately two thirds of the patients by verapqmil. In patients with a partial response, the rate of VT is unaffected. Some patients exhibit exacerbation of the arrhythmia and verapamil should be avoided in these cases. (AM HEART J 1993;126:1126-33.)
Jaswinder S. Gill, MD, Krzysztof Blaszyk, MD, David E. Ward, MD, and A. John Camm, MD London, United Kingdom
From the Department of Cardiological Sciences, St. George’s Hospital Medical School. Received for publication Feb. 16, 1993; accepted April 1, 1993.
1126
Reprint requests: J. S. Gill, MD, Cardiological Sciences, St. George’s Hos- pita1 Medical School, Cranmer Terrace, London SW17 ORE, UK.
Copyright @ 1993 by Mosby-Year Book, Inc. 0002.8703/93/$1.00+.10 4/l/48885

Volume 126, Number 5 American Heart Journal Gill et al. 1127
The majority of istudies examining the treatment of ventricular tachycardia (VT) caused. by ischemic heart disease or cardiomyopathy with calcium an- tagonists have reported disappointing results.1-3 There is some evidence that administration of these agents before induction of myocardial ischemia may reduce the incidence of VT and fibrillation,4 partic- ularly on reperfusion.5 There have been some case reports demonstrating suppression of VT when VT is associated with a clinically normal heart, also termed idiopathic VT. In particular, patients with fascicular tachycardia33 6 and right ventricular outflow tract (RVOT) VT7 appear to respond to calcium antago- nist drugs. The contrasting pharmacologic responses of these forms of VT from that experienced with ischemic VT has led to the suggestion that the mech- anism of arrhythmia may be triggered activity in contrast to the more common reentrant VT associ- ated withischemic heart disease.8 Most of the data on the treatment of right ventricul,ar tachycardia with calcium antagonists consist of case reports or series of <5 patients. 7,8 Currently there is no large pro- spective study of the efficacy of calcium antagonist drugs for the treatment of ventricular tachycardia associated with a clinically normal heart. This study examines the efficacy of verapamil for the suppres- sion of VT of left bundle branch block (LBBB)- like morphology associated with a clinically normal heart in a large group of patients in a prospective manner.
METHODS Patients. Patients were recruited for the study from
a group with VT associated with a clinically normal heart seen at our institution over a 3-year period. No patient had a history of cardiac #disease, and all had had VT documented on multiple ECG ieads on at least one occasion. The clinical examination, car- diothoracic ratio on chest x-ray film (<50 % ), and resting electrocardiogram (ECG) were normal in all patients (apart from minor T-wave abnormalities present on the ECGs of some patients). No patient had angiographic evidence of coronary artery disease, reduced ejection fraction of the left ventricle, or re- gional wall motion abnormality during left ventricu- lar cineangiography and routine echocardiography as assessed by two1 independent observers. Patients gave informed consent to the protocol for drug test- ing.
The morphology of the VT was defined from lead Vi, predominantly negative being LBBB-like and predominantly positive being right bundle branch block (RBBB)-like. The mean frontal plane axis of the clinical tachycardia was classified from the limb leads as leftward (<-300), rightward (>+90’) or normal (-30° to +90°) from the vector perpendicu-
lar to the bipolar lead,with the most isoelectric QRS - complexes. The axis was also analyzed as inferior or superior. Inferior axes were those between 0’ to 180°, whereas superior axes were those between <O” and -180”. Veptricular tachycardia was defined as ~5 consecutive ventricular ectopic depolarizations oc- curring at >lOO beatslmin. The episodes of tachy- cardia were defined as sustained if VT lasted >30 seconds or required termination because of hemody- namic compromise and nonsustained if VT lasted z-5 beats to <30 seconds and terminated spontaneously. Despite the nonsustained nature of the arrhythmia in many patients, all were severely symptomatic and merited treatmen.t on this basis.
Drug therapy. Some of the, patients had previously received treatment for their tachycardia but, in all, therapy was stopped at least 5 days before admission and evaluation of the patient so that the patient would be in a drug-free state. No patient was receiv- ing other concomittant drug therapy or had received amiodarone. After the baseline evaluation, patients received verapamil (360 mg daily in three divided doses) for a minimum of 5 half-lives to allow stable levels to be achieved before evaluation of efficacy.
Therapeutic evbluation. Patients were evaluated with exercise testing, programmed ventricular stim- ulation (PVS), H:olter monitoring at baseline (with the patient in a drug-free state), and after treatment with verapamil. Irurther PVS was not performed if the VT was not inducible at baseline or if a nonspe- cific response (polymorphic VT or ventricular fibril- lation) was obtained. Exercise tests and PVS were performed 2 to 4 hours after the last dose of the drug.
Exercise testin$. Treadmill exercise testing was performed with the Bruce protocollo on a treadmill (Marquette case 1.2, Marquette Electronics, Milwau- kee, Wis.). Patients exercised until their maximal predicted heart rate was achieved, they became lim- ited by dyspnea and fatigue, or they had sustained VT. .At least three simultaneous ECG leads were monitored during the test and for a minimum of 10 minutes after exercise or until the cardiac rhythm returned to the baseline sinus rate. ST-segment changes were monitored throughout. the test, but no patient had any changes that suggested ischemia.
Programmed vgntricular stimulation. Programmed ventricular stimulation was performed after an over- night fast. Multipolar electrode catheters were in- serted via the subclavian vein into the atria1 append- age and right ventricular apex. Intracardiac elec- trograms and the surface ECG were displayed simultaneously on a multichannel oscilloscope and recorded on a multichannel ink-jet recorder (Sie- mens Mingograph, Solna, Sweden) at a paper speed of 25 to 100 mm/set. Ventricular stimulation was performed with a programmable stimulator (Med-
November 1993
1128 Gill et al. American Heart Journal
Table I. Characteristics of patients, ventricular tachycardia (VT), and results of investigations of group studied
Demographics Age (yr; mean & SD) Men/Women
Clinical history Exercise-induced palpitations/ Palpitations unrelated to exercise Syncope/No syncope SustainedlNonsustained VT
Clinical VT Axis VT
Normal Right Left
Cycle length VT (msec; mean f SD) Investigations
End-systolic LV dimensions (mm; mean k SD)
End-diastolic LV dimensions (mm; mean f SD)
Abnormal/Normal cardiac biopsy
LV, Left ventricular.
36.2 t 12.1 Xl/22
15127
13129 29113
15 19 8
318.6 k 66.1
35 2k 1.1
49.9 + 6.4
26112
tronic 5326, Medtronic, Minneapolis, Minn.) by us- ing 1.8 msec rectangular pulses at twice diastolic threshold according to the Wellens protocol.ri In brief, 1, 2, or 3 premature ventricular stimuli were introduced in sinus rhythm or after every 8 paced or conducted ventricular QRS complexes beginning late in diastole and then at progressively closer coupling intervals until ventricular refractoriness was encoun- tered with the last introduced stimulus. The extras- timulus was moved 20 msec out of refractoriness and the next extrastimulus introduced. The process of diminishing coupling intervals was repeated for the last extrastimulus until three extrastimuli had been introduced. Paced drive cycle lengths of 600,500, and 400 msec were used. The test was considered positive if ventricular tachycardia of the same morphology and axis as the clinically documented tachycardia was induced. If other morphologies of tachycardia, polymorphic VT, or ventricular fibrillation were in- duced, the test was considered nonspecific and neg- ative.
Holter monitoring. Twenty-four-hour Holter record- ings were obtained by using the Reynolds Tracker (Reynolds Medical Ltd., Hertford, U.K.) or Marque- tte 8500 Holter recorders and anaIyzed on the Mar- quette XP Laser Holter system. The alogrithm detects normal beats, ventricular ectopic beats oc- curring as isolated ectopics, couplets, salvos (3 to 4 consecutive ventricular ectopic depolarizations), and runs of VT (25 consecutive ventricular ectopic
Table II. Numbers of patients with no ventricular tacby- cardia (VT), nonsustained (nonsust) VT, and sustained (sust) VT at Halter monitoring in baseline drug-free state and after treatment with verapamil, and Numbers of ven- tricular premature beats (VP&) at baseline and with ver- apamil treatment
Verapamil treatment
No VT Nonsust VT Sust VT Totals
Baseline No VT 8 4 0 12 Nonsust VT 11 5 0 16 Sust VT 2 1 0 3
TOTALS 21 10 0 31 Treatment NO. of VPBs per 24 hours (mean i SD)
Baseline 15,541 t 17,599 Verapamil 8,892 + 15,582 p < 0.01
depolarizations). Recordings were obtained at base- line and after treatment with verapamil.
Other investigations. Patients underwent a number of investigations that are pertinent to the results of this study but of which the methodology is not pre- sented in detail, including analysis of late potentials on signal-averaged ECG, endomyocardial biopsy, and detailed echocardiography, including right ven- tricular studies. The methods and results of these in- vestigations have been published previously.r2> i3
Statistical analysis. Treatment groups were com- pared by using t tests, nonparametric tests, and analysis of variance as appropriate.
RESULTS
Forty-two patients whose mean age was 36.2 + 12.1 years and who consisted of 20 men and 22 women were studied. The documented spontaneous arrhyth- mia was of LBBB-like morphology in all patients with a frontal plane axis that was rightward in 19 pa- tients, normal in 15, and leftward in 8. In 27 patients VT was inducible by exercise, 11 of these having sus- tained VT and the remaining 16 patients having nonsustained episodes. The arrhythmia could be in- duced by PVS in 20 patients, 7 of whom had sustained VT and 13 of whom had only nonsustained runs. In two patients PVS was not performed at baseline for clinical reasons. The other characteris- tics of the group are given in Table I. Typical exam- ples of VT in treated this study are presented in Figs. 1 and 2.
Good quality Holter tapes at baseline and on ver- apamil treatment were available in 31 patients, In six
Volume 126, Number 5 American Heart Journal Gill et al. 1129
RVOT VT
sl 04.89
I I
IS
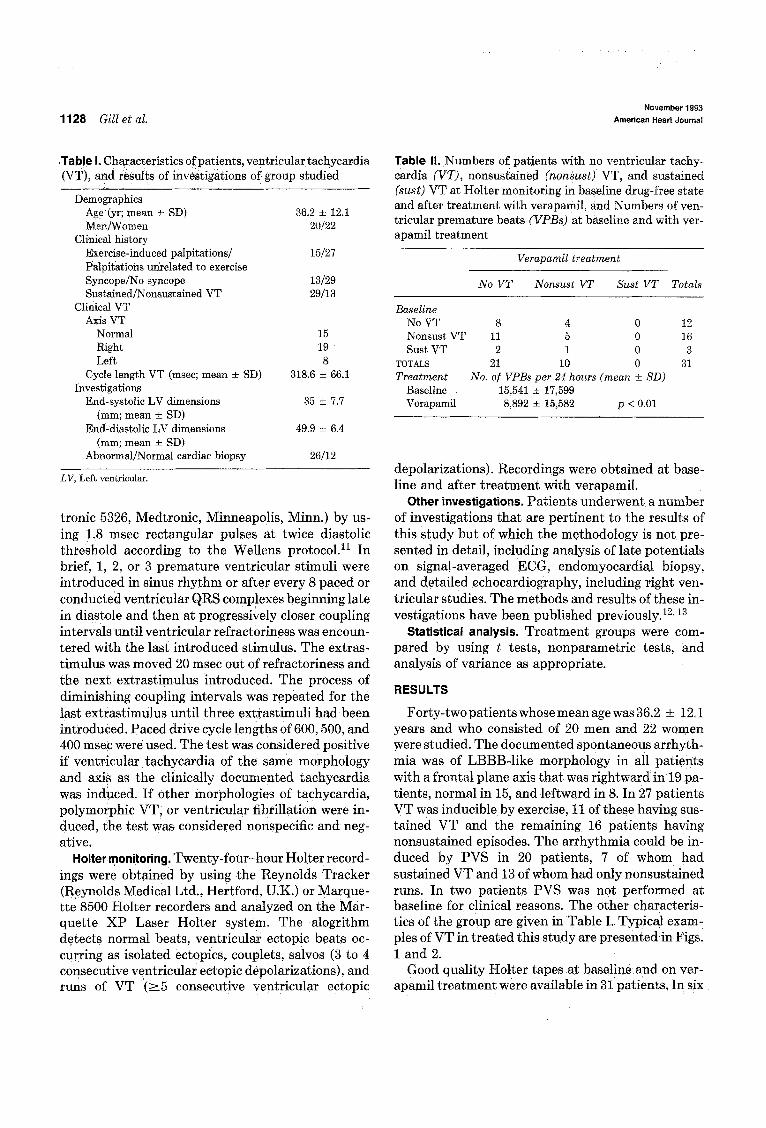
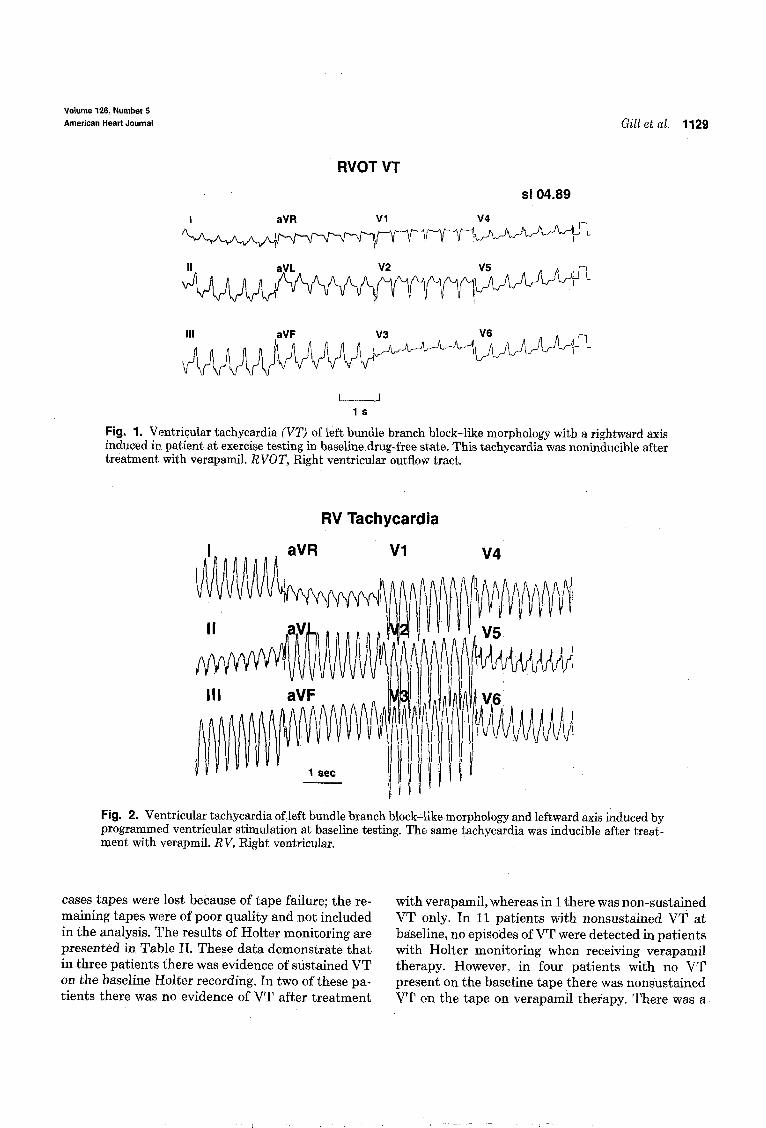
Fig. 1. Ventricular tachycardia (VT) of left bundle branch block-like morphology with a rightward axis induced in patient at exercise testing in baseline drug-free state. This tacbycardia was noninducible after treatment with verapamil. RVOT, Right ventricular outflow tract.
RV Tachycardia
Fig. 2. Ventricular tachycardia of left bundle branch block-Eke morphology and leftward axis induced by programmed ventricular stimulation at baseline testing. The same tachycardia was inducible after treat- ment with verapmil. RV, Right ventricular.
cases tapes were lost because of tape failure; the re- with verapamil, whereas in 1 there was non-sustained maining tapes were of poor quality and not included VT only. In 11 patients with nonsustained VT at in the analysis. The results of Holter monitoring are presented in Table II. These data demonstrate that
baseline, no episodes of VT were detected in patients with Holter monitoring when receiving verapamil
in three patients there was evidence of sustained VT on the baseline Halter recording. In two of these pa- tients there was no evidence of VT after treatment
therapy. However, in four patients with no VT present on the baseline tape there was nonsustained VT on the tape on verapamil therapy. There was a
I
1130 Gill et al. November 18%
American Heart Journsl
Table III. Numbers of patients with noninducible ventric- ular tachycardia (VT), nonsustained VT, and sustained VT at exercise test in the baseline drug-free state and after treatment with verapamil; also presented are exercise tol- erance and cycle length of VT at baseline and with verap- amil treatment
Vei-apamil treatment
No VT Nonsust VT Sust VT Totals
Baseline No VT Nonsust VT Sust VT
TOTALS
Treatment
Baseline Verapamil
15 0 0 15 9 7 0 16 6 5 0 11
30 12 0 42 Exercise tolerance Cycle length VT (set; mean + SD) (msec; mean + SD)
593 z!z 238 355 * 72 655 k 196 338 + 61
A’S, Not significant.
statistically significant reduction (p < 0.01) in the number of ventricular ectopic beats after therapy with verapamil.
The results of verapamil treatment on exercise-in- duced VT are presented in Table III. Exercise toler- ence before and after verapamil therapy did not dif- fer significantly. Exercise-induced VT was sup- pressed in 56% of patients in tihom sustained or nonsustained VT was induced by exercise, whereas 18% demonstrated a partial response (i.e., sustained VT was rendered nonsustained); No response was observed in 26 % of patients, and no patient demon- strated an increase in the inducibility of VT on ver- apamil treatment. In patients with a partial response to verapamil, there was no change in the cycle length of the VT before and after verapamil treatment.
VT was inducible by programmed stimulation in 18 patients, of whom 13 had nonsustained runs of VT; sustained monomorphic VT was inducible in only 5 patients. The results of PVS are presented in Table IV. Of the patients with induction of sustained monomorphic VT, arrhythmia was made noninduc- ible in 4 patients by verapamil treatment, whereas 1 demonstrated no response and had the same VT in- ducible by PVS. In three patients who had nonsus- tained VT inducible at baseline, the arrhythmia was sustained with verapamil treatment. Two of these patients had hemodynamic compromise during the VT and required cardioversion. No patient had a longer duration’of VT 0; had hemodynamfc compro- mise while receiving verapamil in the small number of patie& with sustained m?nomorphic VT induc- ible by PVS.
Table IV. Results of programmed ventricular stimulation (PVS) at baseline and after verapamil treatment
Vei-apamil treatment
No VT Nonsust VT Sust VT Totals
Baseline No VT (VF) 17 (3) Nonsust VT 6 Sust VT 4
TOTALS 30
20 4 3 13 0 1 5 4 4 38
PVS with verapamil treatment was not performed if ventricular tachycar- dia (VT) similar to clinically documented arrhythmia was not induced at testing in drug-free state (2 patients with sustained VT inducible at base- line refused further PVS, and in 2 patients PVS was not pefformed at base- line or after verapamil treatment for clinical reasons. VI?, ventricular fibril- lation.
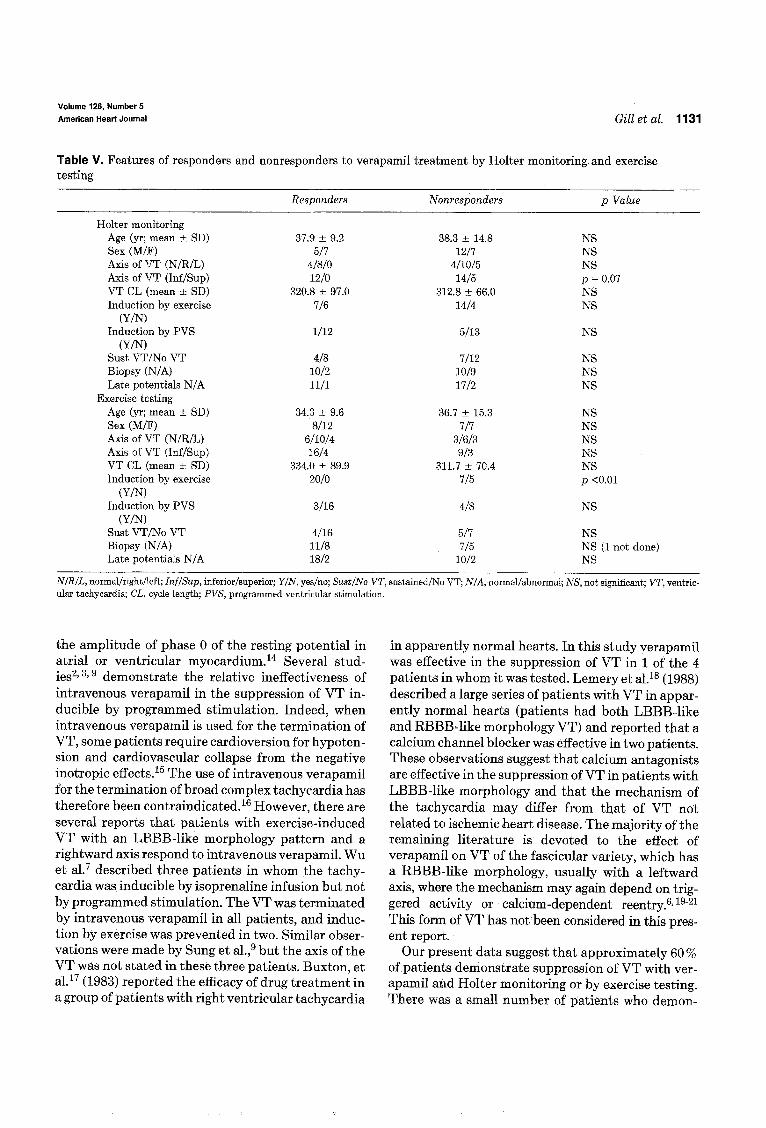
Patients were divided into two groups: those dem- onstrating a beneficial response to verapamil at Holter monitoring and at exercise testing. For Holter monitoring, responders were the patients who dem- onstrated the complete suppression of nonsustained VT or the conversion of sustained VT to nonsus- tained episodes only. For exercise testing, responders were considered patients who demonstrated nonsus- tained or sustained VT on baseline exercise tests that were rendered noninducible or rionsustained, respec- tively, on repeat testing during verapamil therapy. The numbers of patients with sustained monomor- phic VT by PVS were too small to permit this approach. The results of this analysis are presented in Table V. No patient with VT of a superior axis demonstrated a response to verapamil on Halter monitoring. There were no differences in age, sex distribution, occurrence of sustained or nonsustained VT, cycle length of VT, presence of abnormal cardiac biopsies, or the presence’of late potentials among the responders and nonresponderstoierapamil on Holter monitoring. There was no obvious difference in the patients demonstrating a response to verapwil com- pared with those not demonstrating a response by exercise testing for these variables.
DISCUSSION
Most of the currently available evidence suggests that verapamil and other calcium antagonists have little effect on recurrent VT related to ischemic heart disease.lW3 This theory is consistent with ‘the obser- vation that the effective refkactory period of ventric- ular myocardium is not lengthened by calcium chan- nel blockade and that the majority of these arrhyth- mias have a mechanism based on reentry. At clinically achievable concentrations qerapamil reduces the pla- teau height of the action potential but does not affect
Volume 126, Number 5
American Heart Journal Gill et al. 1131
Table V. Features of responders and nonresponders to verapamil treatment by Holter monitoring and exercise testing
Responders Nonresponders p Value
Holter monitoring Age (yr; mean + SD) 37.9 f 9.2 38.3 * 14.8 NS Sex (M/F) 517 1217 NS Axis of VT (N/R/L) 4/8/O 4flOl5 NS Axis of VT (Inf/Sup) 12/o 14/5 p = 0.07 VT CL (mean * SD) 320.8 k 97.0 312.8 + 66.0 NS Induction by exercise 716 1414 NS
W/N Induction by PVS l/l2 5113 NS
cm) Sust VT/No VT 418 7112 NS Biopsy (N/A) 1012 10/9 NS Late potentials N/A 11/l 1712 NS
Exercise testing Age (yr; mean + SD) 34.3 * 9.6 36.7 X!I 15.3 NS Sex (M/F) 8112 717 NS Axis of VT (N/R/L) 6/10/4 31613 NS Axis of VT &f/Sup) 16/4 9f3 NS VT CL (mean k SD) 334.0 f 89.9 311.7 * 70.4 NS Induction by exercise 20/O 715 p <O.Ol
(Y/N) Induction by PVS 3116 418 NS
nm) Sust VT/No VT 4116 517 NS Biopsy (N/A) 11/a 715 NS (1 not done) Late potentials N/A 1812 10/2 NS
NIRIL, normal/right/left; InffSup, inferior/superior; YIN, yes/no; SustlNo VT, sustained/No VT; N/A, normal/abnormal; NS, not significant; VT, vent+ ular tachycardia; CL, cycle length; PVS, programmed ventricular stimulation.
the amplitude of phase 0 of the resting potential in atria1 or ventri.cular myocardium.14 Several stud- ies? 3, g demonstrate the relative ineffectiveness of intravenous verapamil in the suppression of VT in- ducible by programmed stimulation. Indeed, when intravenous verapamil is used for the termination of VT, some patients require cardioversion for hypoten- sion and cardiovascular collapse from the negative inotropic effects. I5 The use of intravenous verapamil for the termination of broad complex tachycardia has therefore been contraindicated.i6 However, there are several reports that patients with exercise-induced VT with an LBBB-like morphology pattern and a rightward axis respond to intravenous verapamil. Wu et a1.7 described three patients in whom the tachy- cardia was inducible by isoprenaline infusion but not by programmed stimulation. The VT was terminated by intravenous verapamil in all patients, and induc- tion by exercise was prevented in two. Similar obser- vations were made by Sung et al.,g but the axis of the VT was not stated in these three patients. Buxton, et all7 (1983) reported the efficacy of drug treatment in a group of patients with right ventricular tachycardia
in apparently normal hearts. In this study verapamil was effective in the suppression of VT in 1 of the 4 patients in whom it was tested. Lemery et a1.18 (1988) described a large series of patients with VT in appar- ently normal hearts (patients had both LBBB-like and RBBB-like morphology VT) and reported that a calcium channel blocker was effective in two patients. These observations suggest that calcium antagonists are effective in the suppression of VT in patients with LBBB-like morphology and that the mechanism of the tachycardia may differ from that of VT not related to ischemic heart disease. The majority of the remaining literature is devoted to the effect of verapamil on VT of the fascicular variety, which has a RBBB-like morphology, usually with a leftward axis, where the mechanism may again depend on trig- gered activity or calcium-dependent reentry.6> 1g-21 This form of VT has not been considered in this pres- ent report.
Our present data suggest that approximately 60 % of patients demonstrate suppression of VT with ver- apamil and Holter monitoring or by exercise testing. There was a small number of patients who demon-

1132 Gill et al. November 1993
American Heart Journal
strated no VT on the baseline Holter.recording and had nonsustained VT with verapamil treatment, al- though an increase in the inducibility or duration of arrhythmia was not observed at exercise testing. The numbers of patients with sustained monomorphic VT induced by PVS were too small to examine ade- quately. Nevertheless, four of five patients in whom sustained monomorphic VT could be induced by PVS in the drug-free state were noninducible with verapamil therapy. However, three patients who had nonsustained VT at baseline testing by PVS had sustained VT with verapamil treatment. This may have been the result of the inherent variability of the inducibility of VT by PVS or may constitute a gen- uine proarrhythmic effect. Therefore a small group of patients may demonstrate exacerbation of their VT when treated with verapamil, both with Holter mon- itoring and with PVS. The vasodilator effect of cal- cium antagonists on the peripheral vasculature can result in catecholamine activation.22 The antiar- rhythmic effects of drugs can be antagonized and re- versed by catecholamines,23 and this would be par- ticularly likely in forms of VT that are catecholamine sensitive. It is therefore likely that exacerbation of the arrhythmia would be seen in some patients with this form of VT. In some patients the inducibility if the VT was partially suppressed by verapamil. In this group, although the duration of the VT was affected (sustained forms being converted to nonsustained), the rate of VT remained unaltered. This is consistent with the observations that verapamil does not affect ventricular refractoriness or conduction within ven- tricular myocardium.24 Unfortunately, no dose-rang- ing was conducted in this study, and it is possible that patients demonstrating a partial response may have been rendered noninducible by a higher dose of ver- apamil. This study does not include a long-term fol- low-up of these patients, but many have remained on verapamil with good control of their symptoms.
Considerable evidence suggests that the mecha- nism of VT in patients with exercise-induced LBBB- like morphology VT with a rightward axis may be triggered activity. Lerman et al8 used adenosine, an endogenous nucleoside, as a probe to differentiate triggered activity from reentry. In ventricular tissue the major effect of adenosine is antiadrenergic, de- creasing catecholamine-mediated production of cy- clic adenosine monophosphate (cAMP).~~ Adenosine decreases the amplitude of after-depolarizations and terminates CAMP-medicated triggered activity. In his study patients with sustained RVOT variety of VT were terminated by adenosine and had features consistent with a triggered activity mechanism in-
cluding termination with.verapamil, more P-blocking drugs and vagal maneuvers. In cellular preparations, triggered activity generally occurs in situations of excess intracellular free calcium. Elevated intracel- lular calcium levels induce an inward current carried by sodium through t channels. This current leads to oscillations in the membrane potential, which may lead to triggered activity if the threshold potential is attained.26> 27 Agents preventing cellular calcium en- try may therefore prevent the initiation of triggered rhythms.
The results of our study suggest that the response of LBBB-like VT to verapamil is not limited to the forms that are induced by exercise, which are likely to be catecholamine sensitive, as some patients with VT that is not inducible by exercise do appear to demonstrate a response. Furthermore, there is no obvious difference in response to verapamil treat- ment in those demonstrating evidence of late poten- tials or of structural cardiac abnormality by biopsy. This may merely reflect the relative insensitivity of cardiac biopsy for revealing cardiac abnormalities when biopsy is usually limited to the interventricu- lar septum; the finding of abnormal cardiac histology in these patients is much more common when biopsy is directed to the likely site of VT in the right ventricular outflow tract.28 These results suggest that verapamil should be considered for the treatment of all forms of right ventricular tachycardia with an in- ferior axis because this variety appears to demon- strate a more consistent response to calcium antag- onist drugs.
We conclude that verapamil can suppress VT in patients with LBBB-like morphology VT associated with a clinically normal heart. In patients exhibiting partial responses there is no effect on the rate, although the duration of the arrhythmia is reduced. A small number of patients demonstrate exacerba- tion of the arrhythmia. Ventricular tachycardia of right ventricular origin with an inferior axis is more likely to respond to verapamil, but the agent should be considered for all forms of VT of right ventricular origin associated with a clinically normal heart.
REFERENCES
1. Belhassen B, Horowitz LN. Role of intravenous verapamil for ventricular tachycardia. Am J Cardiol1984;54:1131-3.
2. Wellens HJJ, Bar FW, Lie KI, Duren DR, Dohmen HJ. Effects of procainamide, propanolol and verapamil on mechanism of tachycardias in patients with chronic recurrent ventricular tachycardia. Am-J Cardiol 1977;40:579-85.
3. Mason JW. Swerdlow CD. Mitchell LB. Efficacv of veranamil in chronic,’ recurrent ventricular tabhycardia. “Am J Cardiol 1983;51:1614-7.
4. Clusin WT, Bristow MR, Bairn DS, Schroeder JS, Jaillon P,
Volume 126, Number 5
American Heart Journal Gill et al. 7 733
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
Brett P, Harrison DC. The effects of diltiazem and reduced serum ionized calcium on ischemic ventricular fibrillation in the dog. Circ Res 1982;50:518-26. Kinoshita K, Mitani A, Hearse DJ, Eraimbridge MV, Manning AS. Reperfusion-induced arrhythmias in the conscious rat: a comparative study with three calcium antagonists. J Surg Res 1989;47:166-72. Ward DE, Nathan AW, Camm AJ. Fascicular tachycardia sensitive to calcium antagonists. Eur Heart J 1984;5:896-905. Wu D, Kou HC, Hung JS. Exercise-triggered paroxysmal ven- tricular tachycardia. A repetitive rhythmic activity possibly related to after depolarization. Ann Intern Med 1981;95:410-4. Lerman BB, Belardinelli L, West A, Berne RM, DiMarco JP. Adenosine sensitive ventricular tachycardia: evidence sug- gesting cyclic AMP-mediated triggered activity. Circulation 1986;74:270-325. Sung RJ, Shapiro EN, Shen EN, Morady E. Effect of verap- amil on ventricular tachycardias possibly caused by reentry, automaticity and triggered activity. J Clin Invest 1982;72:360- 70. Bruce RA, Hornsten TR. Exercise stress testing in evaluation of patients with ischemic heart disease. Prog Cardiovasc Dis 1969;11:317-90. Wellens HJJ, Brugada P, Stevenson WG. Programmed elec- trical stimulation of the heart in patients with life-threaten- ins arrhvthmias. What is the sienificance of the induced arrhythmias and what is the correct stimulation protocol. Cir- culation 1985;72:1-7. Metha D. McKenna WJ. Ward DE. Davies MJ. Camm AJ. Significance of signal-averaged electrocardiography in rela- tion to endomyocardial biopsy and ventricular stimulation studies in patients with ventricular tachycsrdia without clin- icallv annarent heart disease. J Am Co11 Cardiol1989:14:372-9.
1 - -
Mehta D, Odawara H, Ward DE, McKenna WJ, Davies MJ, Camm AJ. Echocardiographic and histologic evaluation of the right ventricle in ventricular tachycardias of left bundle branch block morphology without overt cardiac abnormahty. Am J Cardiol 1989;63:939-44. Zipes DP, Bailey DC, Elharrar V. The slow inward current and cardiac arrhyth:mias. The Hague: Martinus Nijhoff Publish- ing, 1980. Akhtar M, Shenasa M, Jazayeri M, Caceres J, Tchou P. Wide QRS complex tachycardia: reappraisal of a common clinical problem. Ann Intern Med 1988;109:905-12. Stewart RB, Bardy GH, Greene HL. Wide complex tachycar-
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
dia: reappraisal of a common clinical problem. Ann Intern Med 1986;104:766-71. Buxton AE, Waxman HL, Marchlinski FE, Simson MB, Cas- sidy D, Josephson ME. Right ventricular tachycsrdia: clinical and electrophysiological characteristics. Circulation 1983; 68:917-27. Lemery R, Brugada P, Bella PD, Dugernier T, van den Do01 A. Wellens HJJ. Non-ischemic ventricular tachvcardia. Clin- ical course and long-term follow-up in patientswithout clin- ically overt disease. Circulation 1989;79:990-9. Lin FC, Finley CD, Rahimtoola SH, Wu D. Idiopathic parox- vsmal ventricular tachvcardia with a wide QRS pattern of - - right bundle branch block and left axis deviation. A unique clinical entity with speci6c properties. Am J Cardiol 1983; 52:95-100. Zipes DP, Foster PR, Troup PJ, Pederson DH. Atria1 induc- tion of ventricular tachycardia. Reentry versus triggered au- tomaticity. Am J Cardiol 1979;44:1-8. Ohe T, Shimomura K, Aihara N, Kamakura S, Matsuhisa M, Sato I, Nakagawa H, Shimizu A. Idiopathic sustained left ventricular tachycardia: clinical and electrophysiological char- acteristics. Circulation 1988;77:560-8. Kiowski W, Erne P, Bertel 0, Bolli P, Buhler F. Acute and chronic sympathetic reflex activation and antihypertensive response to nifedipine. J Am Co11 Cardiol 1986;7:344-8. Morady F, Kou WH, Kadish AH, Nelson SD, Toivonen LK, Kushner JA, Schmaltz S, DeBuitleir M. Antagonism of quini- dine’s electrophysiologic effects by epinephrine in patients with ventricular tachycardia. J Am Colt Cardiol1988;12:388- 94. Opie LH, ed. Calcium channel antagonists in clinical use of calcium channel antagonist drugs. Dordrecht: Kluwer Aca- demic Publishers, 1990. Isenberg G, Belardinelli L. Ionic basis for antagonism between adenosine and isoproteronol on isolated mammalian ventric- ular myocytes. Circ Res 1984;55:309-25. Tsien RW, Kass RS, Weingart R. Cellular and subcellular mechanisms of cardiac pacemaker oscillations. J Exp Biol 1979;81:205-12. Kass RS, Tsien RW, Weingart R. Ionic basis of transient in- ward current induced by stropanthidin in cardiac Purkinje fi- bres. J Phvsiol (Land) 1978;281:209-26. Crijns H, Tuininga Y,‘Schoots C, Dijk RV, Wiesfeld A, Lie K. Value of target-directed endomyocardial biopsy in idiopathic right ventricular tachycardia. J Am Co11 Cardiol 1990;17:97A.