victimization, trauma, and suicidality among adolescents presenting for substance abuse treatment...
TRANSCRIPT
Victimization, Trauma, and Suicidality Among Adolescents Presenting for Substance Abuse Treatment
Michael Dennis, Ph.D. Chestnut Health Systems, Bloomington, IL
Part of the continuing education workshop, “Advancing the Field of Adolescent Substance Abuse Treatment”, Hamden, CT, April 22, 2005. Sponsored by the Department of Children and Families Substance Abuse Division. The content of this presentations are based on treatment & research funded by the Center for Substance Abuse Treatment (CSAT), Substance Abuse and Mental Health Services Administration (SAMHSA) under contract 270-2003-00006 using data provided by the following grantees: (TI11320, TI11324, TI11317, TI11321, TI11323, TI11874, TI11424, TI11894, TI11871, TI11433, TI11423, TI11432, TI11422, TI11892, TI11888, TI013313, TI013309, TI013344, TI013354, TI013356, TI013305, TI013340, TI130022, TI03345, TI012208, TI013323, TI14376, TI14261, TI14189,TI14252, TI14315, TI14283, TI14267, TI14188, TI14103, TI14272, TI14090, TI14271, TI14355, TI14196, TI14214, TI14254, TI14311, TI15678, TI15670, TI15486, TI15511, TI15433, TI15479, TI15682, TI15483, TI15674, TI15467, TI15686, TI15481, TI15461, TI15475, TI15413, TI15562, TI15514, TI15672, TI15478, TI15447, TI15545, TI15671)). several individual grants. The opinions are those of the author and do not reflect official positions of the consortium or government. Available on line at www.chestnut.org/LI/Posters or by contacting Joan Unsicker at 720 West Chestnut, Bloomington, IL 61701, phone: (309) 827-6026, fax: (309) 829-4661, e-Mail: [email protected]
Demonstrate the feasibility and desirability of measuring victimization at intake with the GAIN’s General Victimization Scale (GVS)
Show that victimization is common and varies in severity
Examine the how the severity of victimization (measured with GVS) is correlated with with level of care, demographic characteristics, substance use severity, relapse potential, HIV risk, mental health, and crime/violence
Examine the implications of traumatic victimization for treatment outcome and matching
Goals of this Presentation
Victimization (including physical, sexual, and emotional abuse) are the norm for adolescents presenting to substance abuse treatment.
Yet staff often express concerns that they do not have the tools for screening; that screening might disrupt rapport (leading to early drop out or mandated reporting); and that they lack the resources to do anything about victimization.
This is at odds with expert recommendations (CSAT, 1993, 1999, 2000; Dennis & Stevens, 2003; Dennis, 2004) that have consistently encouraged early systematic screening and intervention among adolescents entering substance abuse treatment.
Introduction
Prevalence Rates of Victimization It is estimated that 826,000 to 3,000,000 (3-12%)
adolescents (age 12 to 17) have been victimized (DHHS, 2001; Sedlack & Broadhurst, 1996).
Among adolescents presenting for substance abuse treatment, the rates ranged from 40 to 80% - varying by gender, timing, definition, and level of care (Dennis & Stevens, 2003) .
– 39% of male & 59% of females acknowledged a lifetime history of physical or sexual victimization when interviewed a few questions in DATOS-A a month after intake (Grella & Joshi, 2003).
– 48% of the males and 80% of the females acknowledged a lifetime history of physical, sexual, or emotional victimization when interviewed with the GAIN at intake (Titus, Dennis, White, Scott & Funk, 2003).
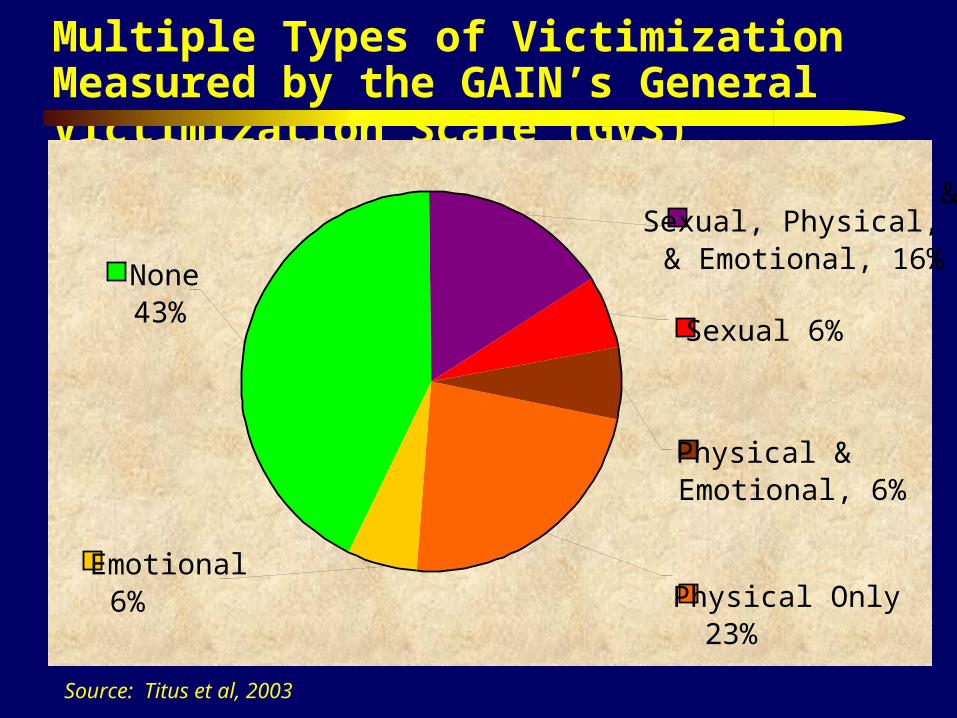
Multiple Types of Victimization Measured by the GAIN’s General Victimization Scale (GVS)
Source: Titus et al, 2003
Emotional6%
none43%
Physical Only23%
Sexual Physical, & Emotional16%Sexual6%
Physical & Emotional6%
Emotional6%
None43%
Physical Only23%
Sexual, Physical, && Emotional, 16%
Sexual 6%
Physical & Emotional, 6%
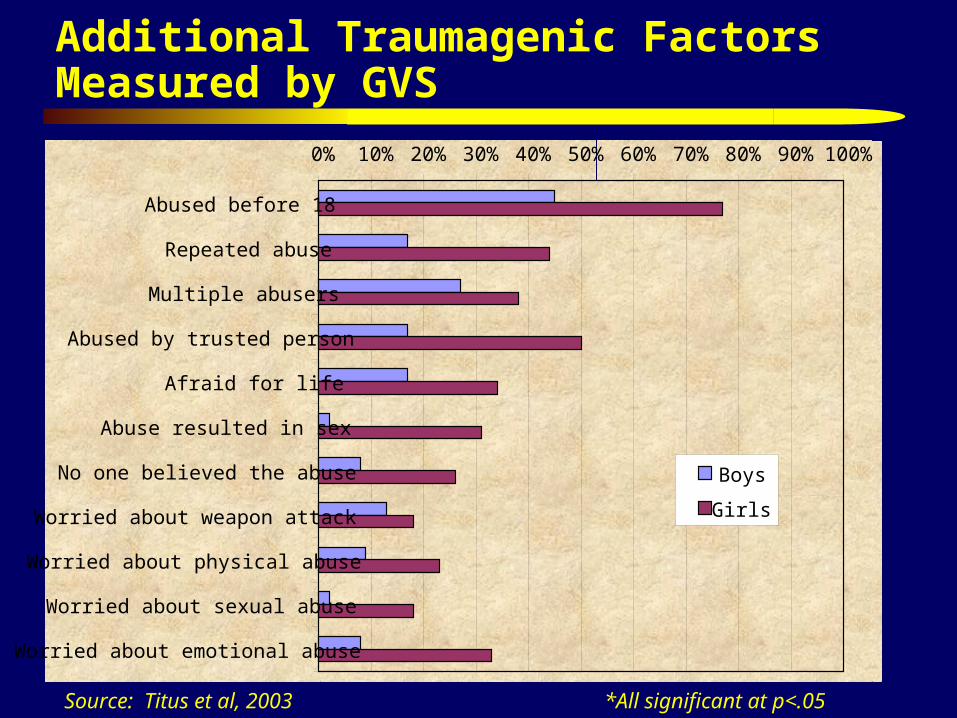
Additional Traumagenic Factors Measured by GVS
Source: Titus et al, 2003 *All significant at p<.05
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Abused before 18
Repeated abuse
Multiple abusers
Abused by trusted person
Afraid for life
Abuse resulted in sex
No one believed the abuse
Worried about weapon attack
Worried about physical abuse
Worried about sexual abuse
Worried about emotional abuse
Boys
Girls
CSAT Adolescent Treatment (AT) Programs Reordered by Level of Care and Severity
EAT: Effective Adolescent Treatment (2003-2007; n=975) replicating the CYT MET/CBT intervention in early intervention, school and outpatient settings(22 of 36 grants: Bradley, Brown, Clayton,Curry, Davis, Dillon, Dodge, Kressler, Kincaid, Levine, Levy, Locario, Mason, Moore, Rajaee-Moore, Paull, Payton, Rezende, Taylor, Tims, Turner, Vincent)
CYT: Cannabis Youth Treatment (1997-2001; n=600) Experiments with adolescent outpatient/intensive outpatient (5 grants: Babor, Dennis, Diamond, Godley, Tims)
TCE: Targeted Capacity Expansion (2002-2007; n=189) evaluation of intensive outpatient programs and some residential treatment (2 of 12 grants: Tims, Lloyd)
SCY: Strengthening Communities-Youth (2002-2007; n=1120) evaluations of early intervention, outpatient, intensive outpatient and some residential (11 of 12 grants: Beach, Bolland, Dahl, Gerstel, Godley, Hall, Hutchinson, Keehn, Murphy, Noonan, Panzarella)
ATM: Adolescent Treatment Model (1998-2002; n=1468) evaluations of outpatient, short and long term residential (10 grants: Batttjes, Fishman, Godley, Liddle, Morral, Perry, Sabin, Shane, Stevens-2)
ART: Adolescent Residential Treatment (2003-2006; n=1179) evaluations of residential treatment enhancements and continuing care (17 grants: Beach, Fishman, Flores, Gay, Gnazzo, Hatch, Hurtig, Lane, Law, Manov, May, Miley, Nordquist, Snipes, Urquahart, Whitmore, Zammarelli)
CSAT AT Program Common Data Set The working CSAT adolescent treatment data set including data on 5,468
adolescents from 67 local evaluations (current through quarterly data submission cycle ending in December 2004)
All data collected with the Global Appraisal of Individual Needs (GAIN) using centrally trained and certified staff
Outcome data through 12 months available on over 90% of CYT and ATM clients and over 80% of others “due” in on-going programs
Programs include several standardized protocols based on both research and practice (ACC, ACRA, ATM, FFT, FSN, Matrix, MET/CBT, MDFT, MST)
Local evaluations include several experiments and quasi experiments Several workgroups working on common themes across programs (African
American, Co-morbidity, Family, Native American/Indian, Spanish translation/workforce)
Data being shared with several secondary analysis grantees and panel presentations for this week
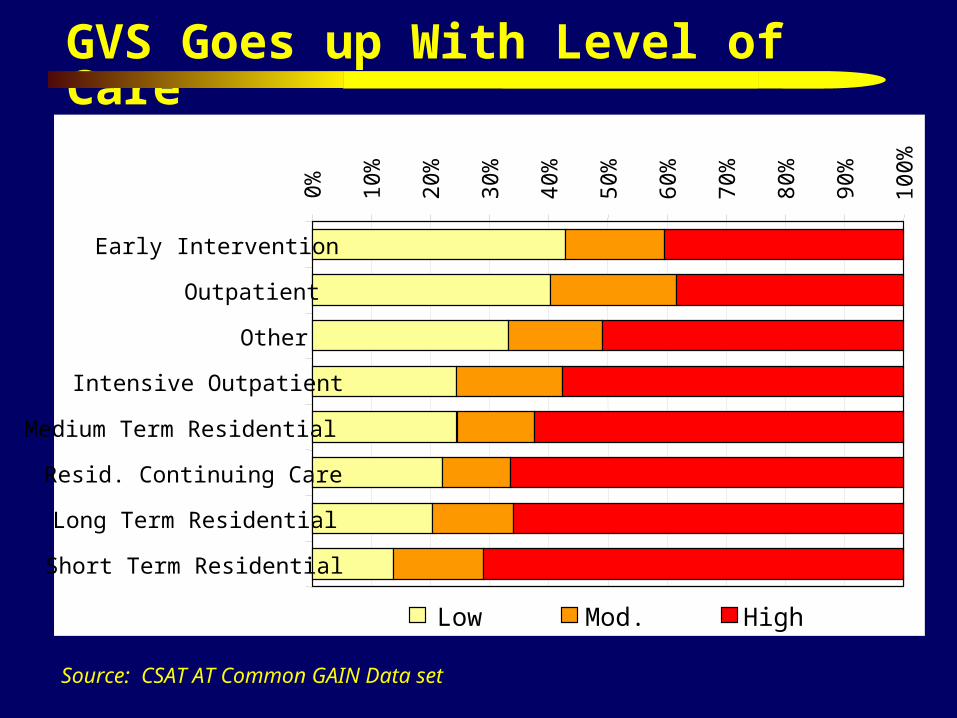
GVS Goes up With Level of Care
Source: CSAT AT Common GAIN Data set
0% 10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Early Intervention
Outpatient
Other
Intensive Outpatient
Medium Term Residential
Resid. Continuing Care
Long Term Residential
Short Term Residential
Low Mod. High
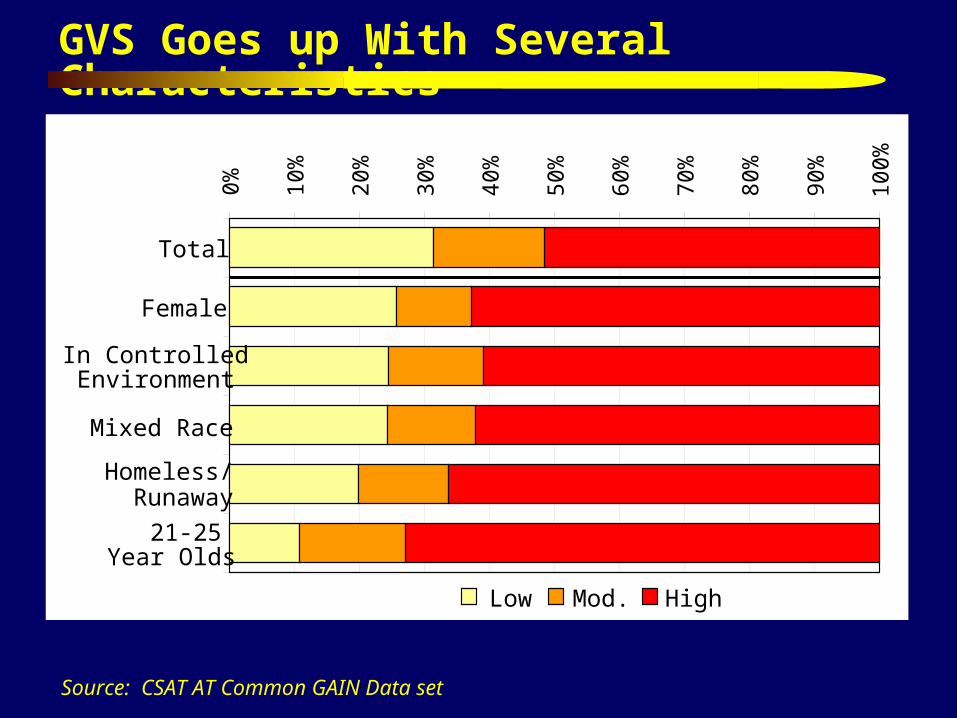
GVS Goes up With Several Characteristics
Source: CSAT AT Common GAIN Data set
0% 10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Total
Female
In ControlledEnvironment
Mixed Race
Homeless/Runaway
21-25 Year Olds
Low Mod. High
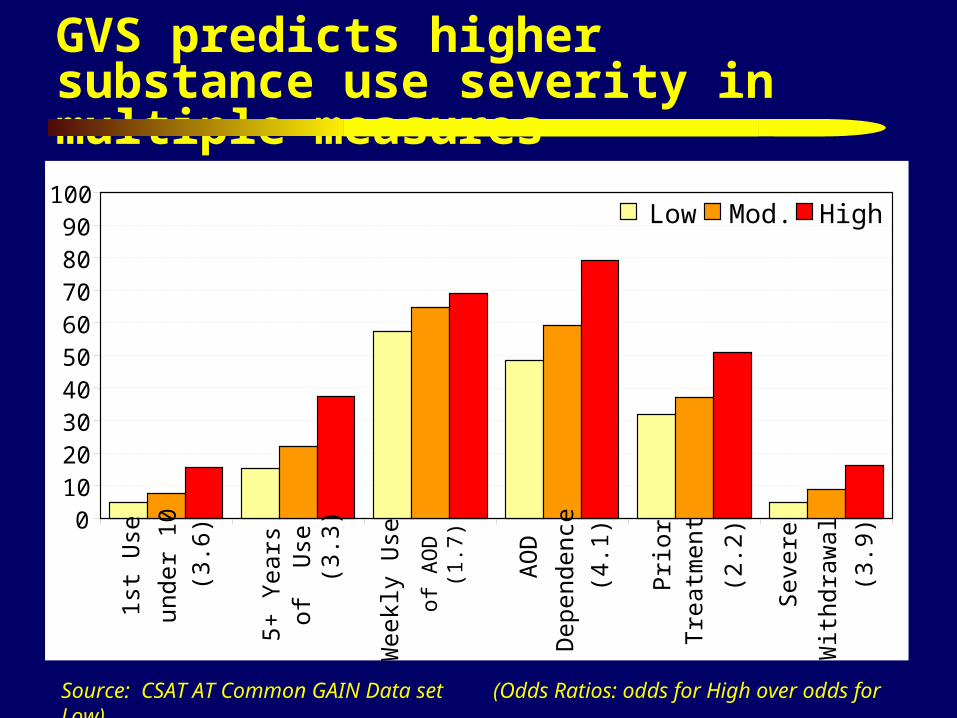
GVS predicts higher substance use severity in multiple measures
Source: CSAT AT Common GAIN Data set (Odds Ratios: odds for High over odds for Low)
0102030405060708090
100
1st U
se
unde
r 10
(3.6
)
5+ Y
ears
of
Use
(3
.3)
Wee
kly
Use
of A
OD
(1
.7)
AO
D
Dep
ende
nce
(4.1
)
Prio
rT
reat
men
t
(2.2
)
Seve
re
Wit
hdra
wal
(3.9
)
Low Mod. High
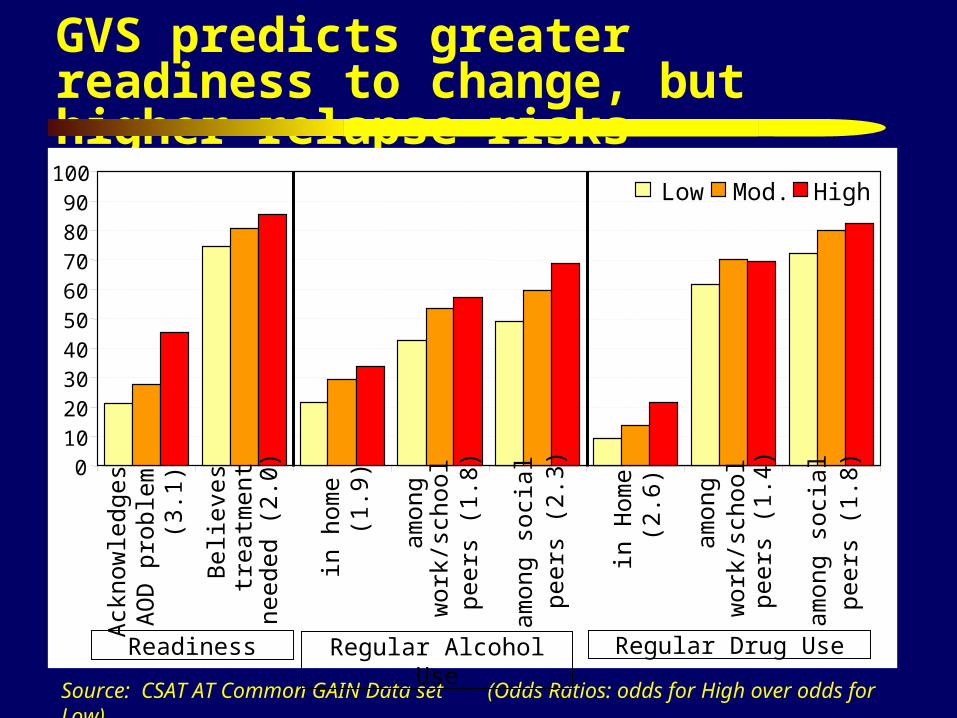
GVS predicts greater readiness to change, but higher relapse risks
Source: CSAT AT Common GAIN Data set (Odds Ratios: odds for High over odds for Low)
010
2030
4050
6070
8090
100
Ack
now
ledg
esA
OD
pro
blem
(3.1
)
Bel
ieve
str
eatm
ent
need
ed (
2.0)
in h
ome
(1.9
)
amon
gw
ork/
scho
olpe
ers
(1.8
)
amon
g so
cial
peer
s (2
.3)
in H
ome
(2.
6)
amon
gw
ork/
scho
olpe
ers
(1.4
)
amon
g so
cial
peer
s (1
.8)
Low Mod. High
Regular Alcohol Use Regular Drug UseReadiness
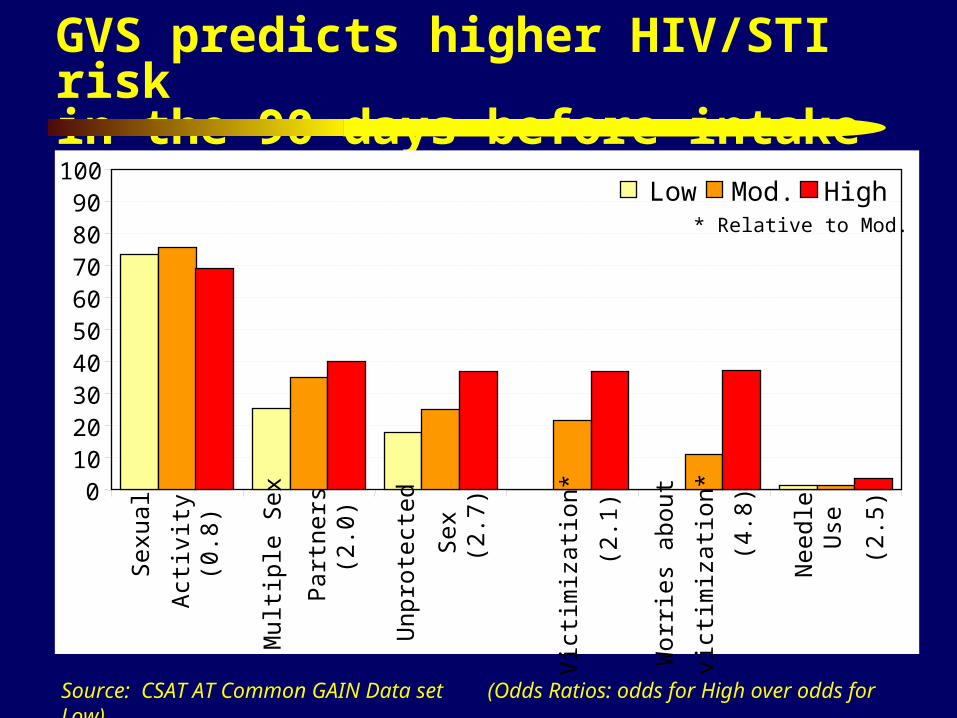
GVS predicts higher HIV/STI risk in the 90 days before intake
Source: CSAT AT Common GAIN Data set (Odds Ratios: odds for High over odds for Low)
0102030405060708090
100Se
xual
Act
ivit
y (0
.8)
Mul
tipl
e Se
x
Part
ners
(2.
0)
Unp
rote
cted
Sex
(2.7
)
Vic
tim
izat
ion*
(2.1
)
Wor
ries
abo
ut
vict
imiz
atio
n*
(4.8
)
Nee
dle
Use
(2.5
)
Low Mod. High* Relative to Mod.
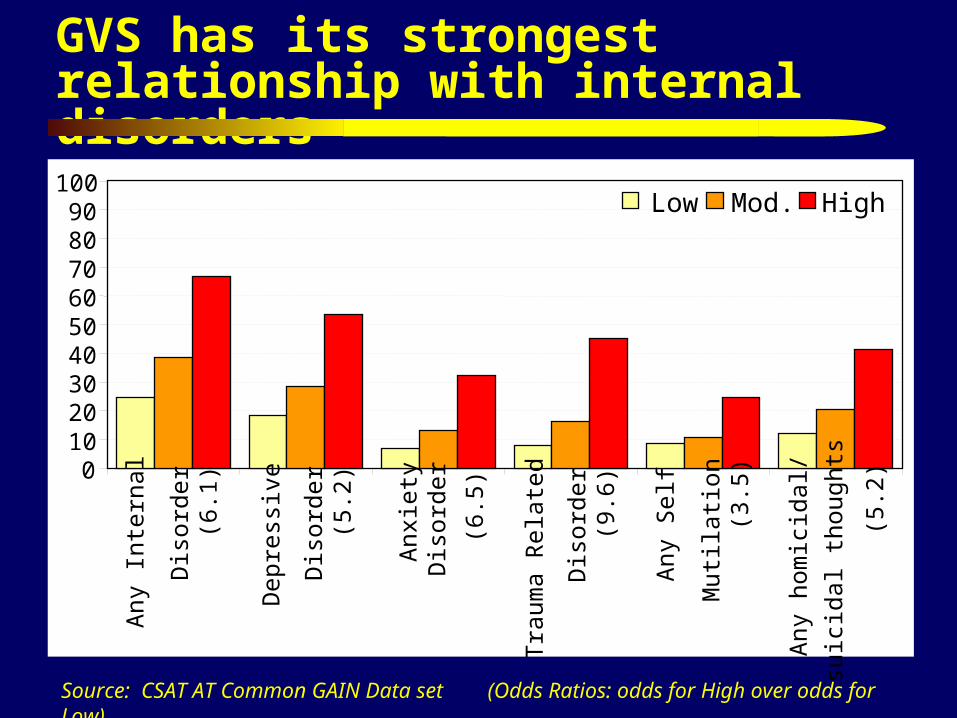
GVS has its strongest relationship with internal disorders
Source: CSAT AT Common GAIN Data set (Odds Ratios: odds for High over odds for Low)
0102030405060708090
100
Any
Int
erna
l
Dis
orde
r(6
.1)
Dep
ress
ive
Dis
orde
r (
5.2)
Anx
iety
Dis
orde
r
(6.5
)
Tra
uma
Rel
ated
Dis
orde
r (
9.6)
Any
Sel
f
Mut
ilat
ion
(3.
5)
Any
hom
icid
al/
suic
idal
thou
ghts
(5.
2)
Low Mod. High
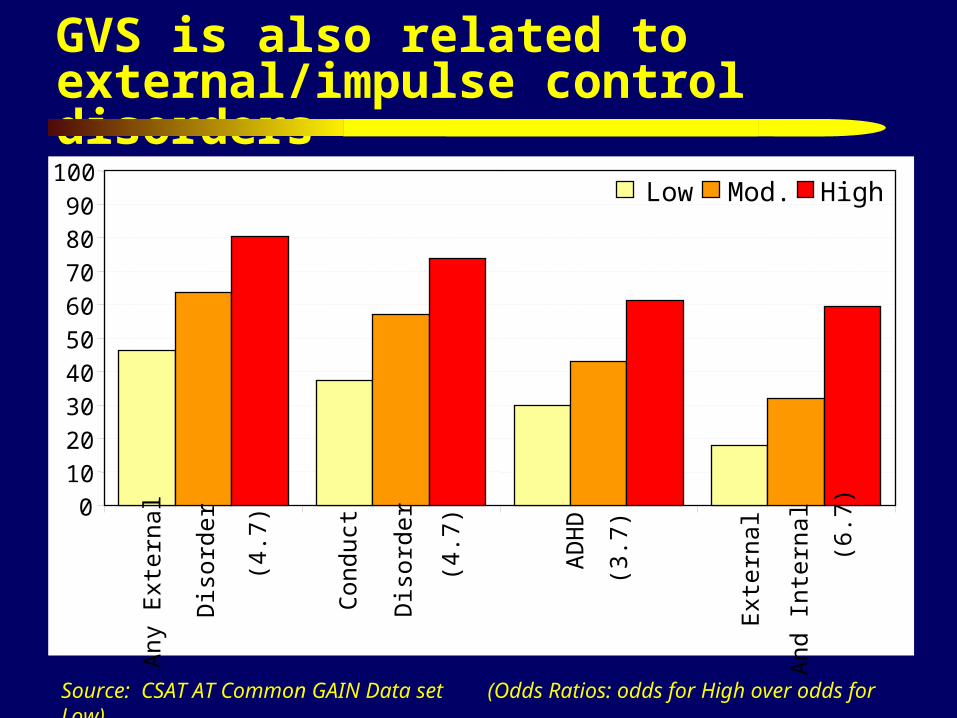
GVS is also related to external/impulse control disorders
Source: CSAT AT Common GAIN Data set (Odds Ratios: odds for High over odds for Low)
0
10
20
30
40
50
60
70
80
90
100A
ny E
xter
nal
Dis
orde
r
(4.7
)
Con
duct
Dis
orde
r
(4.7
)
AD
HD
(3.
7)
Ext
erna
l
And
Int
erna
l
(6.7
)
Low Mod. High
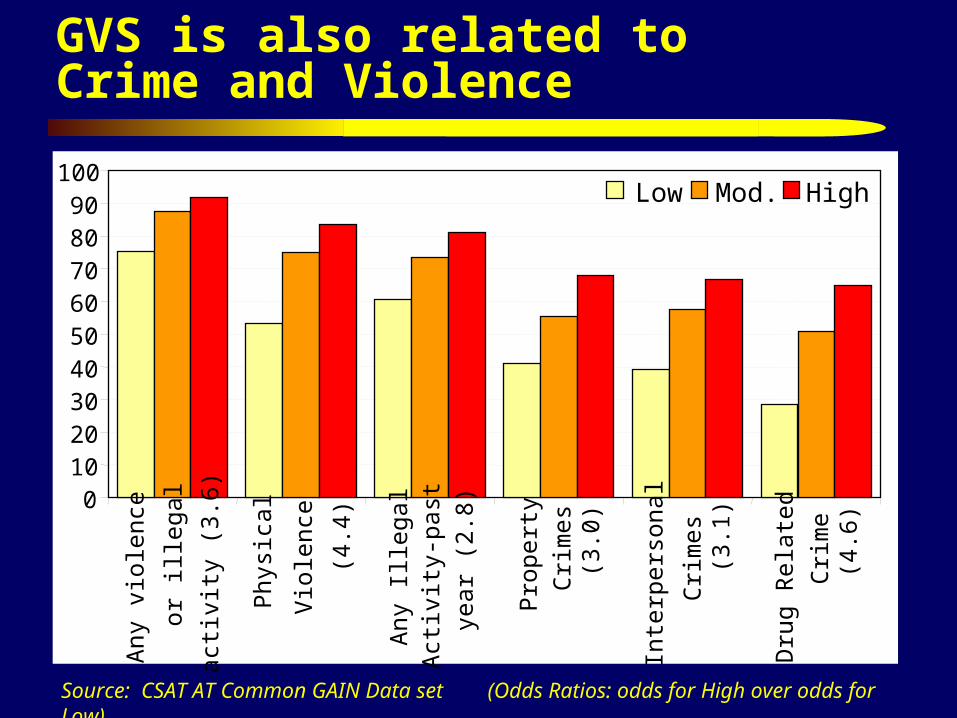
GVS is also related to Crime and Violence
Source: CSAT AT Common GAIN Data set (Odds Ratios: odds for High over odds for Low)
0102030405060708090
100
Any
vio
lenc
e
or il
lega
l
acti
vity
(3.
6)
Phys
ical
Vio
lenc
e
(4.4
)
Any
Ill
egal
Act
ivit
y-pa
st
year
(2.
8)
Prop
erty
Cri
mes
(3.
0)
Inte
rper
sona
l
Cri
mes
(3
.1)
Dru
g R
elat
ed
Cri
me
(4.6
)
Low Mod. High
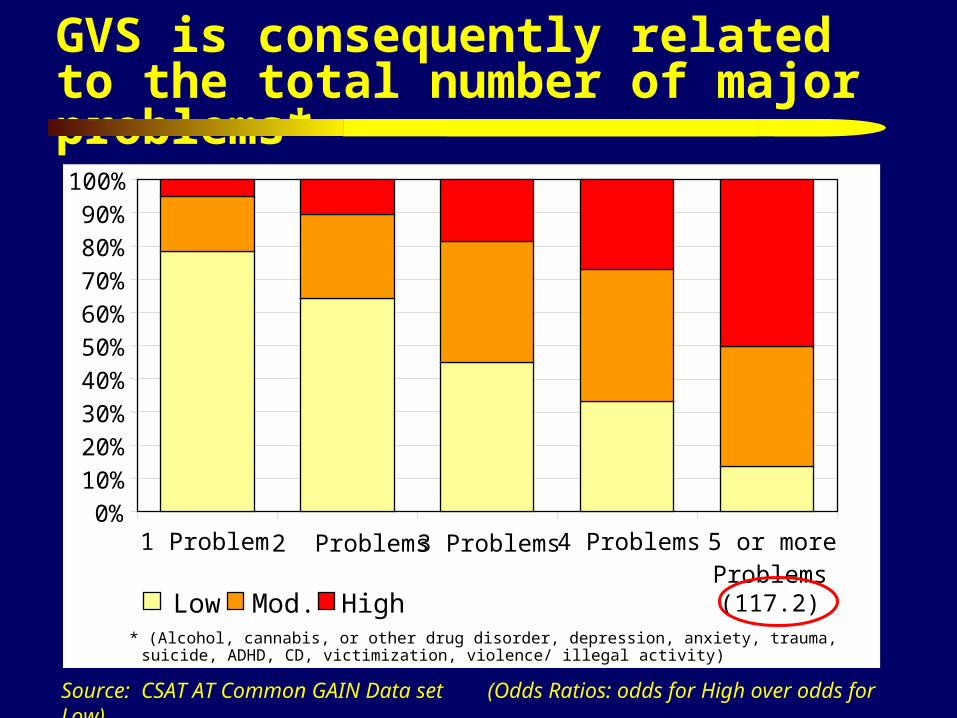
GVS is consequently related to the total number of major problems*
Source: CSAT AT Common GAIN Data set (Odds Ratios: odds for High over odds for Low)
0%
10%
20%30%
40%
50%60%
70%
80%90%
100%
1 Problem 2 Problems 3 Problems 4 Problems 5 or moreProblems(117.2)Low Mod. High
* (Alcohol, cannabis, or other drug disorder, depression, anxiety, trauma, suicide, ADHD, CD, victimization, violence/ illegal activity)
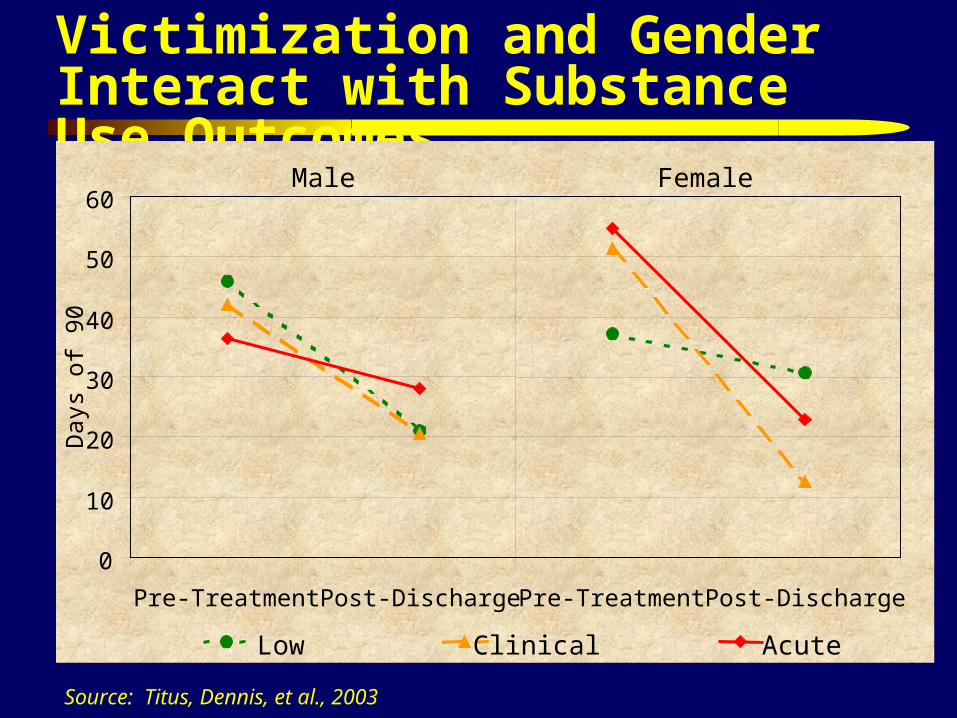
Victimization and Gender Interact with Substance Use Outcomes
Source: Titus, Dennis, et al., 2003
0
10
20
30
40
50
60
Pre-Treatment Post-Discharge Pre-Treatment Post-Discharge
Day
s of
90
Low Clinical Acute
Male Female
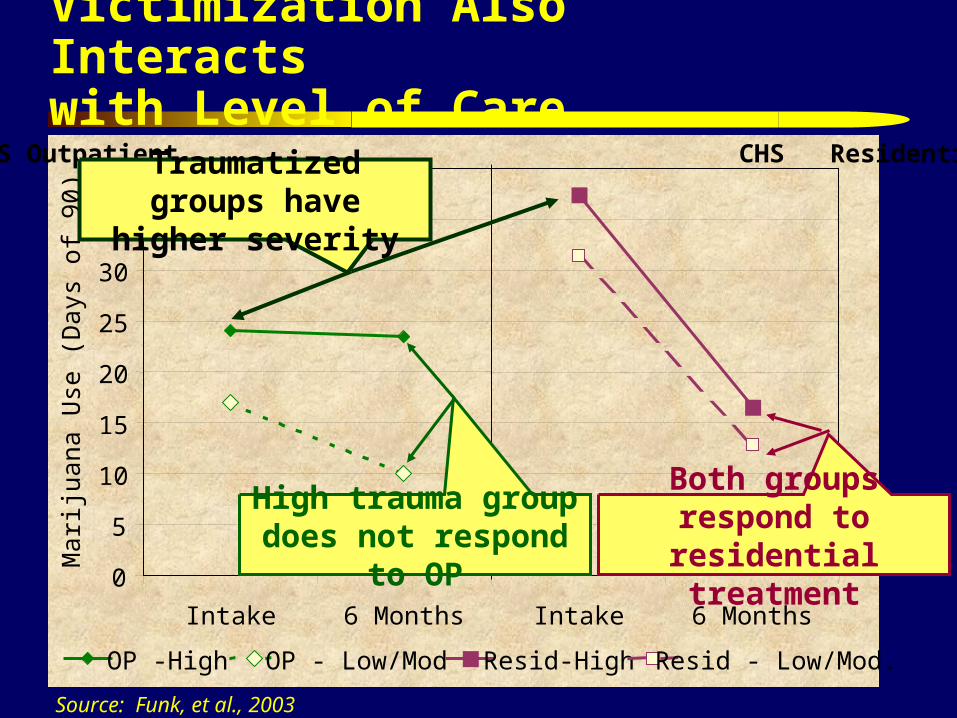
Victimization Also Interacts with Level of Care
Source: Funk, et al., 2003
0
5
10
15
20
25
30
35
40
Intake 6 Months Intake 6 Months
Mar
ijua
na U
se (
Day
s of
90)
OP -High OP - Low/Mod Resid-High Resid - Low/Mod.
CHS Outpatient CHS Residential Traumatized groups have higher severity
High trauma group does not respond to OP
Both groups respond to residential treatment
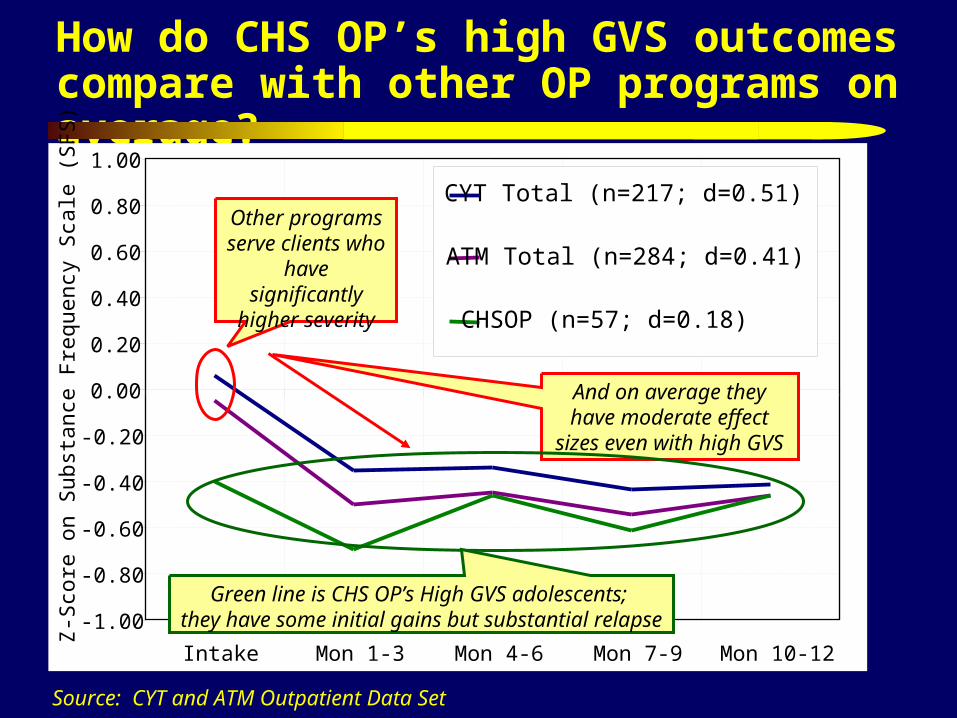
How do CHS OP’s high GVS outcomes compare with other OP programs on average?
Source: CYT and ATM Outpatient Data Set
-1.00
-0.80
-0.60
-0.40
-0.20
0.00
0.20
0.40
0.60
0.80
1.00
Intake Mon 1-3 Mon 4-6 Mon 7-9 Mon 10-12
Z-S
core
on
Sub
stan
ce F
requ
ency
Sca
le (
SF
S) CYT Total (n=217; d=0.51)
ATM Total (n=284; d=0.41)
CHSOP (n=57; d=0.18)
Other programs serve clients who have significantly
higher severity
And on average they have moderate effect sizes even
with high GVS
Green line is CHS OP’s High GVS adolescents; they have some initial gains but substantial relapse
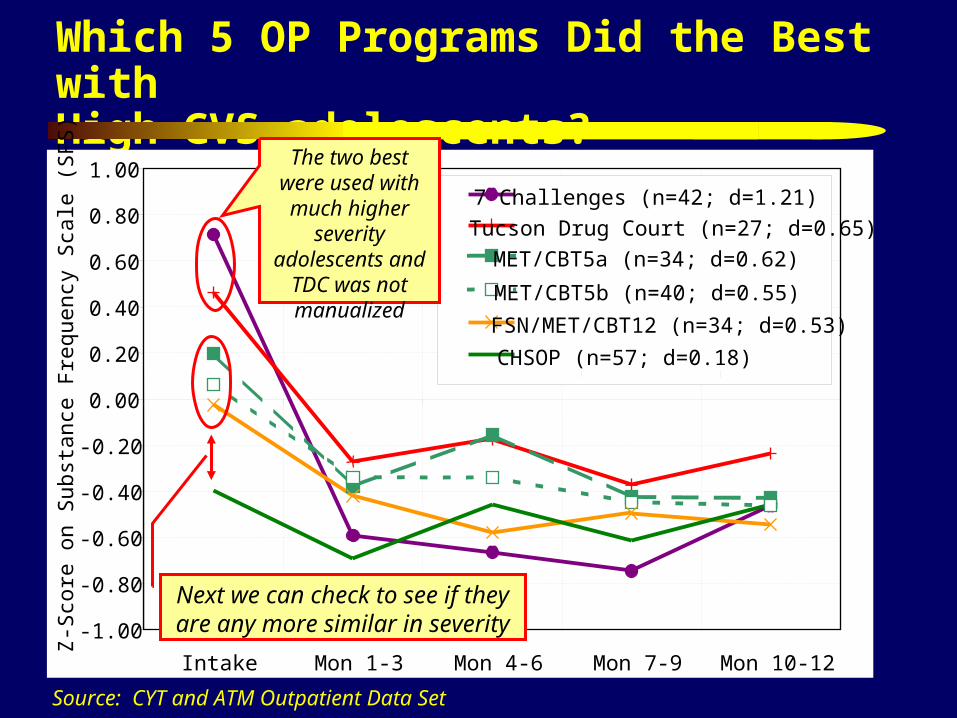
Which 5 OP Programs Did the Best with High GVS adolescents?
Source: CYT and ATM Outpatient Data Set
-1.00
-0.80
-0.60
-0.40
-0.20
0.00
0.20
0.40
0.60
0.80
1.00
Intake Mon 1-3 Mon 4-6 Mon 7-9 Mon 10-12
Z-S
core
on
Sub
stan
ce F
requ
ency
Sca
le (
SF
S) 7 Challenges (n=42; d=1.21)
Tucson Drug Court (n=27; d=0.65)
MET/CBT5a (n=34; d=0.62)
MET/CBT5b (n=40; d=0.55)
FSN/MET/CBT12 (n=34; d=0.53)
CHSOP (n=57; d=0.18)
The two best were used with much higher severity adolescents and
TDC was not manualized
Next we can check to see if they are any more similar in severity
-1.00
-0.80
-0.60
-0.40
-0.20
0.00
0.20
0.40
0.60
0.80
1.00
Intake Mon 1-3 Mon 4-6 Mon 7-9 Mon 10-12
Z-S
core
on
Sub
stan
ce F
requ
ency
Sca
le (
SF
S)
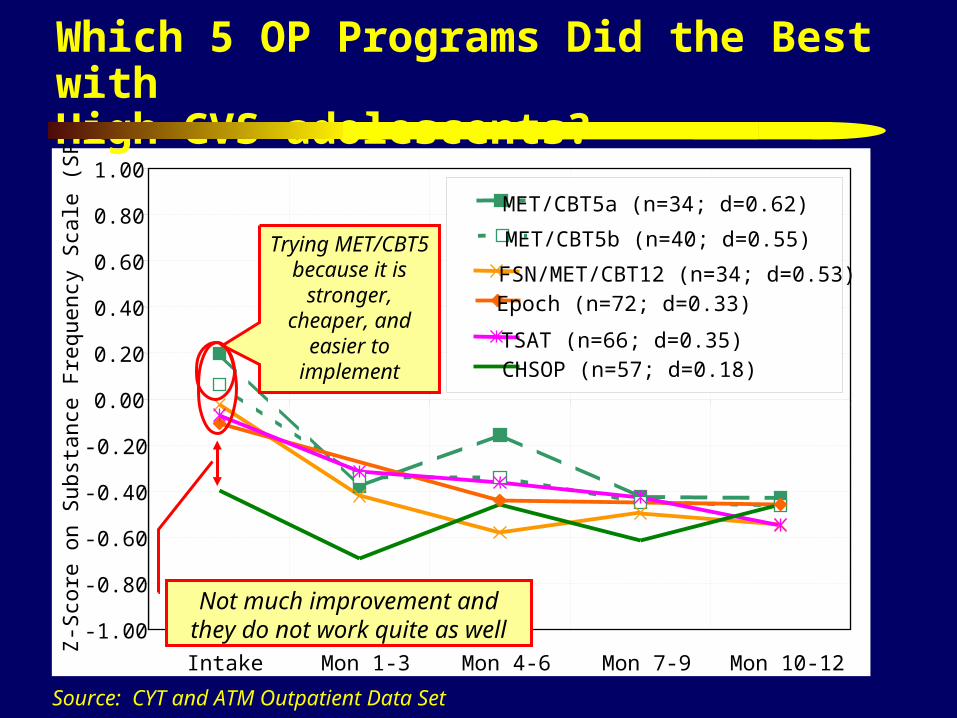
MET/CBT5a (n=34; d=0.62)
MET/CBT5b (n=40; d=0.55)
FSN/MET/CBT12 (n=34; d=0.53)Epoch (n=72; d=0.33)
TSAT (n=66; d=0.35)CHSOP (n=57; d=0.18)
Which 5 OP Programs Did the Best with High GVS adolescents?
Source: CYT and ATM Outpatient Data Set
Trying MET/CBT5 because it is
stronger, cheaper, and easier to
implement
Not much improvement and they do not work quite as well
Other approaches specifically targeting trauma Cognitive Behavioral Intervention for Trauma in Schools (CBITS)®
Manual (Lisa H. Jaycox Ph.D., 2004) www.sopriswest.com or [email protected]
Seeking Safety: A Treatment Manual for PTSD and Substance Abuse (Najavits, 2002) www.seekingsafety.org or from Guilford Press (800-365-7006)
Trauma Adaptive Recovery Group Education & Therapy Model for Adolescents (TARGET-A; Ford et al., 2000, Ford, Mahoney & Russo, 2004) from www.ptsdfreedom.org or [email protected]
Dialectical Behavior Therapy for Adolescents (DBT-A; Rathus, Miller, & Linehan, in press) from
School-Based Trauma/Grief Group Psychotherapy Program (SPARCS; Layne, Saltzman, Pynoos, et al., 2000) from [email protected]
Concluding Comments Victimization is the norm among adolescents presenting for
substance abuse treatment Victimization can and should be comprehensively assessed at intake The severity of traumatic victimization is highly correlated with a
wide range of substance use, HIV risk behaviors, mental health, and crime/violence problems.
Higher levels of victimization interact with treatment effectiveness Substance abuse treatment programs vary in their effectiveness at
dealing with trauma More interventions are need to specifically target victimization and
trauma It is Time to Stop Ignoring the Elephant in our Counseling Room
Resources and References Copy of these slides and handouts are at http://www.chestnut.org/LI/Posters/ , see also
www.mayatech
Information on the GAIN is at www.chestnut.org/li/gain
Information on the adolescent treatment manuals discussed are at www.chestnut.org/li/apss/csat/protocols
References cited:Dennis, M.L. (2004). Traumatic victimization among adolescents in substance abuse treatment: Time to stop ignoring
the elephant in our counseling rooms. Counselor, April, 36-40.Dennis, M. L., & Stevens, S. J., (Eds.). (2003). Maltreatment issues and outcomes of adolescents enrolled in substance
abuse treatment [special issue]. Journal of Child Maltreatment, 8(1): 3-6. See http://www.sagepub.com/journalIssue.aspx?pid=15&jiid=6072
Dennis, M. L., Titus, J. C., White, M., Unsicker, J., & Hodgkins, D. (2003). Global Appraisal of Individual Needs (GAIN) Administration guide for the GAIN and related measures. (Version 5 ed.). Bloomington, IL Chestnut Health Systems. Retrieve from http//www.chestnut.org/li/gain
Funk, R. R., McDermeit, M., Godley, S. H., & Adams, L. (2003). Maltreatment issues by level of adolescent substance abuse treatment The extent of the problem at intake and relationship to early outcomes. Journal of Child Maltreatment, 8, 36-45.
Grella, C. E., & Joshi, V. (2003). Treatment processes and outcomes among adolescents with a history of abuse who are in drug treatment. Journal of Child Maltreatment, 8(1): 7-18.
Jaycox, L.H., Stein, B., Kataoka, S., Wong, M., Fink, A., Escudera, P. & Zaragoza, C. (2002). Violence exposure, PTSD, and depressive symptoms among recent immigrant school children. Journal of the American Academy of Child and Adolescent Psychiatry, 41(9): 1104-1110.
References Continued
Kataoka, S., Stein, B. D., Jaycox, L. H., Wong, M., Escuerdo, P., Tu, W., Zaragosa, C., & Fink, A. (2003). A school-based mental health program for traumatized Latino immigrant children. Journal of the American Academy of Child and Adolescent Psychiatry, 42(3), 311-318.
Najavits, L. (2002). Seeking Safety: A Treatment Manual for PTSD and Substance Abuse. New York, NY: Guilford Press. Aavailalbe from www.seekingsafety.org or 800-365-7006.
Schwebel, R. (2004) The Seven Challenges® Manual. Available from www.sevenchallenges.com or [email protected]
Stein, B.D., Jaycox, L.H., Kataoka, S.H., Wong, M., Tu, W., Eliot, M.N., & Fink, A. (2003). A mental health intervention for school children exposed to violence: A randomized controlled trial. Journal of the American Medical Association, 290(5), 603-611.
Titus, J.C., Dennis, M.L., White, W.L., Scott, C.K., & Funk, R.R. (2003). Gender Differences in Victimization Severity and Outcomes Among Adolescents Treated for Substance Abuse. Journal of Child Maltreatment, 8(1), 19-35.
U.S. Department of Health and Human Services. (2001). Child Maltreatment 1999. Washington, DC: U.S. Government Printing Office.