viral hepatitis related antigens in 'autoimmune' hepatic disorders
TRANSCRIPT

1971 INTERNATIONAL SYMPOSIUM ON VIRAL HEPATITIS
Viral hepatitis related antigens in 'autoimmune'
hepatic disordersDeborah Doniach, Salvatore Del Prete, David S. Dane, and John H. Walsh,London, England
It appears likely that viruses are involved in triggeringautoimmune reactions. This has been demonstrated inseveral experimental mpdels and applies tb humandiseases such as virus pneumonia. However, to producethe intense and permanent autoiirimunization seen in so-called "primary autoimmune diseases" such as thy-roiditis or gastritis, an additional genetic defect of theimmune responses must be present. There is as yet nbgood evidence of an autoimmune hepatitis, in the sensethat liver-specific antibodies are rarely detected.1 Despitethis, a limited number of chronic hepatic syndromes ap¬pear to be associated with the constant presence of hightitre tissue antibodies.23
Autoimmune markersThe most reliable marker has proved to be the mito-chondrial antibody detected by immunofluorescence.This reaction is positive in over 90% of patients withprimary biliary cirrhosis47 and in a variable but smallproportion of cases in which the clinical diagnosis hasbeen cryptogenic cirrhosis or active chronic hepatitis(ACH). Primary biliary cirrhosis (PBC) is a well-definedcondition in its classical form and the patients constitutea homogeneous group.8 The other two syndromes ciearlyinclude diseases of varied etiological background. Theclinical distinction between "lupoid" hepatitis in itsbroader sense, and prolonged viral infection is difficultunless the patient has systemic manifestations suggestiveof a collagen disease such as butterfly rash, arthralgia,or an associated autoimmune disorder, for instancethyrotoxicosis or thyroiditis. Now that Australia antigenhas been demonstrated in the immune complexes in a fewcases of polyarteritis9 and in the renal deposits of a caseof nephrosis10 even extrahepatic involvement is no
longer a reliable index of autoimmunity as a putativeetiological agent in cases of prolonged or progressiveliver disease. Histologically it is impossible to distinguishlesions caused by direct virus action frorti those thatmight turn out to be mediated or perpetuated by auto¬immune factors. The same arguments apply to crypto¬
genic cirrhosis.1112Mitochondrial immunofluorescence has allowed the
segregation of a proportion of cases in these two cate¬gories which have many features in common with pri¬mary biliary disease in that the patients are mostlymiddle-aged women, many of whom have other evidenceof autoimmunity such as thyroiditis or collagen dis¬orders.13 Histologically also there are resemblances inthat portal zone infiltrates may contain germinal centresor small granulomas in those ca^ses of cryptogenic cirrho¬sis where mitochondrial antibodies are found in the se¬rum.14 A histological picture intermediate betweenaggressive hepatitis and biliary cirrhosis15 is also a com¬mon finding in patients having mitochondrial antibodiesindependent of their clinical mode of presentation. Theincidence of mitochondrial antibodies in cases with theclinical diagnosis of ACH or cryptogenic cirrhosis variesconsiderably according to the diagnostic criteria em¬
ployed and in different countries, being about 25% inpatients classified by Professor Sherlock in the UnitedKingdom,16 while it was less than 1% in Ugandan cirrho¬sis although alcoholic and nutritional causes were
apparently excluded.17Besides mitochondrial antibodies, two other autoim¬
mune markers have been of great help in the study ofchronic liver diseases. The LE-cell phenomenon typicallyfound in systemic lupus erythematosus and which reflectsthe presence of antinuclear antibodies (ANA), was thefirst criterion by which the concept of autoimmune hepa-
Dr. Deborah Doniach,Reader in Immunopathology,The Middlesex Hospital MedicalSchool, London, England
C.M.A. JOURNAL/FEBRUARY 26, 1972/VOL. 106, SPECIAL ISSUE 513
titis was put forward.18 This test is positive in no morethan 5% of chronic active hepatitis cases. The less specificand more sensitive fluorescent ANA test is positive in upto 80% of ACH cases, again depending on the clinicalselection. A serious disadvantage for the conceptualseparation of autoimmune liver cases is the widespreadoccurrence of these antibodies, not only in the collagendisorders but spontaneously with increasing age in fe¬males, in response to various drugs and to infections.Smooth muscle fluorescence19 has also been used suc-
cessfully to separate autoimmune from other variants ofchronic hepatitis.20 Low titres of these antibodies occuras a temporary phenomenon in 60 to 80% of infectivehepatitis cases21-22 and at first it was thought that hightitres were confined to autoimmune cases. However,there are now reports of titres up to 1:320 in uncompli-cated Australia-positive hepatitis,23 and comparabletitres are most unusual even in classical "lupoid" hepa¬titis with positive LE-cell tests.
AUSTRALIA ANTIGEN IN CHRONICLIVER DISEASE ASSOCIATED WITHAUTOIMMUNITYActive chronic hepatitis andcryptogenic cirrhosisThe Australia antigen has been found in 0 to 60% of pa¬tients with the clinical diagnosis of ACH or the histologi¬cal diagnosis of aggressive hepatitis20-2426 which againsuggests that diagnostic criteria vary in different centres.In addition it is now clear that the incidence of infectionwith hepatitis viruses is much higher in some countriesthan in others.12 On the whole most workers find thatpatients with high titres of autoimmune markers tend tobe negative for Australia antigen. However, even takingthe strictest criterion for what is considered an auto¬immune case, i.e. the presence of LE-cells, several au¬thors have now described isolated patients having Aus¬tralia antigen in the serum.20-27
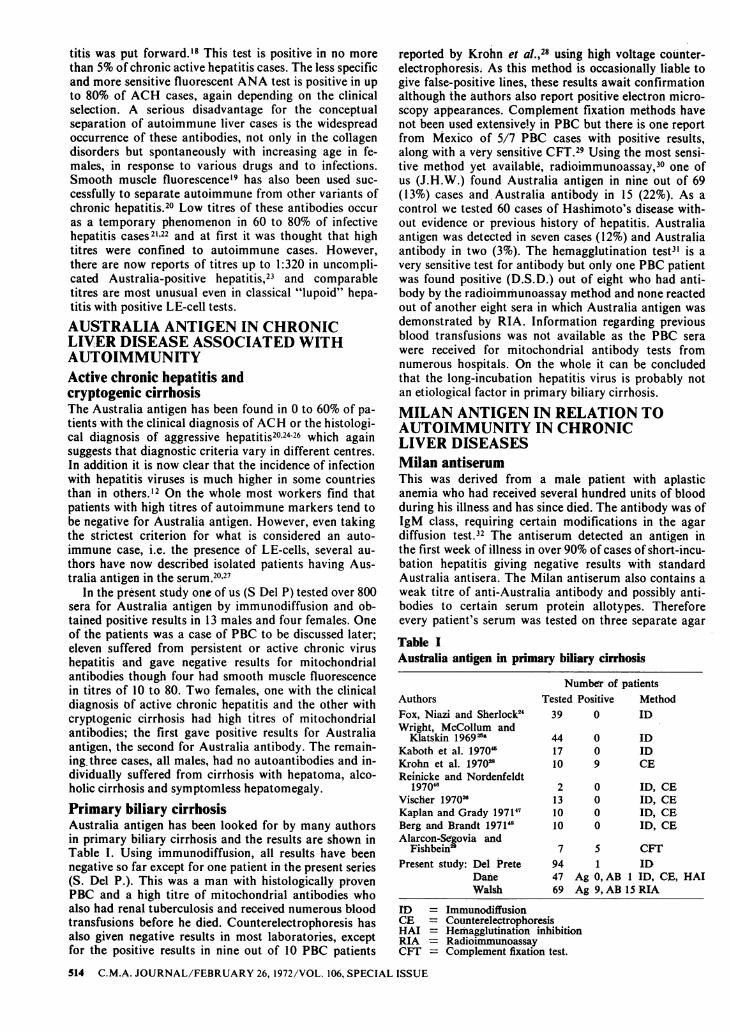
In the present study one of us (S Del P) tested over 800sera for Australia antigen by immunodiffusion and ob¬tained positive results in 13 males and four females. Oneof the patients was a case of PBC to be discussed later;eleven suffered from persistent or active chronic virushepatitis and gave negative results for mitochondrialantibodies though four had smooth muscle fluorescencein titres of 10 to 80. Two females, one with the clinicaldiagnosis of active chronic hepatitis and the other withcryptogenic cirrhosis had high titres of mitochondrialantibodies; the first gave positive results for Australiaantigen, the second for Australia antibody. The remain-ing three cases, all males, had no autoantibodies and in-dividually suffered from cirrhosis with hepatoma, alco¬holic cirrhosis and symptomless hepatomegaly.Primary biliary cirrhosisAustralia antigen has been looked for by many authorsin primary biliary cirrhosis and the results are shown inTable I. Using immunodiffusion, all results have beennegative so far except for one patient in the present series(S. Del P.). This was a man with histologically pfovenPBC and a high titre of mitochondrial antibodies whoalso had renal tuberculosis and received numerous bloodtransfusions before he died. Counterelectrophoresis hasalso given negative results in most laboratories, exceptfor the positive results in nine out of 10 PBC patients
reported by Krohn et a/.,28 using high voltage counter¬electrophoresis; As this method is occasionally liable togive false-positive lines, these results await confirmationalthough the authors also report positive electron micro¬scopy appearances. Complement fixation methods havenot been used extensively in PBC but there is one reportfrom Mexico of 5/7 PBC cases with positive results,along with a very sensitive CFT.29 Using the most sensi¬tive method yet available, radioimmunoassay,30 one ofus (J.H.W.) found Australia antigen in nine out of 69(13%) cases and Australia antibody in 15 (22%). As acontrol we tested 60 cases of Hashimoto's disease with¬out evidence or previous history of hepatitis. Australiaantigen was detected in seven cases (12%) and Australiaantibody in two (3%). The hemagglutination test31 is a
very sensitive test for antibody but only one PBC patientwas found positive (D.S.D.) out of eight who had anti¬body by the radioimmunoassay method and none reactedout of another eight sera in which Australia antigen wasdemonstrated by RIA. Information regarding previousblood transfusions was not available as the PBC serawere received for mitochondrial antibody tests fromnumerous hospitals. On the whole it can be concludedthat the long-incubation hepatitis virus is probably notan etiological factor in primary biliary cirrhosis.
MILAN ANTIGEN IN RELATION TOAUTOIMMUNITY IN CHRONICLIVER DISEASESMilan antiserumThis was derived from a male patient with aplasticanemia who had received several hundred units of bloodduring his illness and has since died. The antibody was ofIgM class, requiring certain modifications in the agardiffusion test.32 The antiserum detected an antigen inthe first week of illness in over 90% of cases of short-incu-bation hepatitis giving negative results with standardAustralia antisera. The Milan antiserum also contains aweak titre of anti-Australia antibody and possibly anti¬bodies to certain serum protein allotypes. Thereforeevery patient's serum was tested on three separate agarTable IAustralia antigen in primary biliary cirrhosis
ID = ImmunodiffusionCE = CounterelectrophoresisHAI = Hemagglutination inhibitionRIA RadioimmunoassayCFT = Complement fixation test.
514 C.M.A. JOURNAL/FEBRUARY 26, 1972/VOL. 106, SPECIAL ISSUE

plates against: (1) Milan antiserum, (2) known Australiaantisera, and (3) pooled normal human serum. Serareacting in plates 1 and 3 were considered to give non-
specific lines. Those reacting in plates 1 and 2 were calledAustralia-positive and those reacting only in plate 1 wereconsidered to contain Milan antigen.Plan of studyThe present study was undertaken to assess the role ofthe short-incubation hepatitis virus in autoimmune liverdisorders. To demonstrate the separate nature of theMilan and Australia antigens, a number of sera positivefor Milan antigen were tested by radioimmunoassay andhemagglutination inhibition against known Australiaantisera. Sera received from various hospitals for auto-antibody tests were posted to Milan within one to 14days. Postal strikes in England and Italy delayed someof the Milan tests and increased the number of non-
specific lines. Since the Milan antigen is lipoprotein innature it does not keep well in storage and the positiveresults obtained probably represent a minimum inci¬dence. All sera were coded by numbers and tested with¬out knowledge ofthe clinical or immunological data. Anattempt was made to test Milan-positive cases on severaloccasions to see if the antigen persisted.Milan antigen in primary biliary cirrhosisNinety-four cases with the diagnosis of primary biliarycirrhosis (87 females, 7 males) were available for testing.Of these, 90 had mitochondrial antibodies (96%), 19 gavepositive ANA (20%) in titres of 10 to 640 and 46 patients(49%) had smooth muscle fluorescence in titres of 10 to320. Milan antigen was detected in 36 cases (38%), 45were negative (48%) and 13 gave non specific lines (TableII). Nineteen patients with PBC were tested on repeatedTable IIIncidence of Milan antigen in primary biliary cirrhosis,
occasions; 12 had positive tests between two and fivetimes at intervals of three to nine months and in sevencases the results varied. The most interesting instancewas a patient who showed persistent Milan antigenemiain five tests over seven months following liver traosplan-tation. A second liver transplant patient was pbsitivepreoperatively but had persistently negative tests follow¬ing operation. The results for Milan antigen in no waycorrelated with the degree of obstructive jaundice or withevidence of hepatic failure and this makes it unlikelythat this antigen is related to lipoprotein-X?3 or to theother abnormal lipoprotein described by Seidel in severeliver failure.
Milan antigen in ACH and cryptogenic cirrhosisOne hundred and thirteen cases with the diagnosis ofactive chronic hepatitis were available for study and theoverall incidence of Milan antigen was 26% (Table II). Inthis group it was particularly difficult to assess thepresence of autoimmune factors since so many cases ofuncomplicated viral hepatitis have traces of smoothmuscle antibodies. However, the patients with autoanti-bodies had a higher incidence (30%) than those without(19%). In 53 cases of cryptogenic cirrhosis it was easier todistinguish patients with, from those without autoimmu¬nity since most cases have either negative tests or veryhigh titres in at least one of the three autoimmunemarkers. The total incidence of Milan antigen was 30%and cases without autoimmunity had this antigen almostas frequently as those with high titre autoantibodies.
Correlation of Milan antigenwith autoimmune markersIn order to correlate the importance of individual auto¬immune markers in relation to Milan antigen inde-
active chronic hepatitis and cryptogenic cirrhosis
Note: Patients giving non-specific lines in Milan test included in total number tested but not in positive or nega¬tive results. All these cases were Australia Ag-negative.
TableIII Table IVChronic liver disease with nuclear antibodies (ANA) . Chronic liver disease with smooth muscle antibody .titre 80 to1280 titre 80 to 640
Correlation with Milan antigen in 37 cases
Precipitin test for Milan antigenNumber of Non-specific
Correlation with Milan antigen in 29 cases
Precipitin test for Milan antigenNumber of Non-specific
C.M.A. JOURNAL/FEBRUARY 26, 1972/VOL. 106, SPECIAL ISSUE 515
pendently of the clinical diagnosis, patients with hightitres were selected. Thus, of 37 cases with a titre ofANAfrom 80 to 1280, 27% had Milan antigen (Table III); of29 cases with smooth muscle antibody titre from 80 to640, 31% had Milan antigen (Table IV) and of 139 pa¬tients with mitochondrial antibodies, 35% were positiveby the Milan test (Table V). It was not possible to sepa¬rate these markers from each other since all three are
frequently present in the same serum. The highest fre¬quency of Milan antigen was found in patients who hadall three antibodies in their serum.
Milan antigen in non-hepaticautoimmune disordersThree categories of autoimmune controls were tested forMilan antigen: (1) 60 patients (58 females, 2 males) withHashimoto's thyroiditis having no previous history ofhepatitis and no mitochondrial antibodies in the serum;(2) 14 individuals (11 females, 3 males) with positivemitochondrial antibody tests and no evidence of liverdisease (these were mostly symptomless Relatives ofpatients with hepatic disease or cases with autoimmunedisease not affecting the liver); (3) 16 cases of systemiclupus erythematosus with high titre ANA and negativemitochondrial reactions. All the patients with Hashi¬moto's disease gave negative results for Milan antigenas did all the "M"-positive subjects without overt liverdisease. There was one patient with SLE who had Milanantigen in the serum and one who gave a non-specificline.
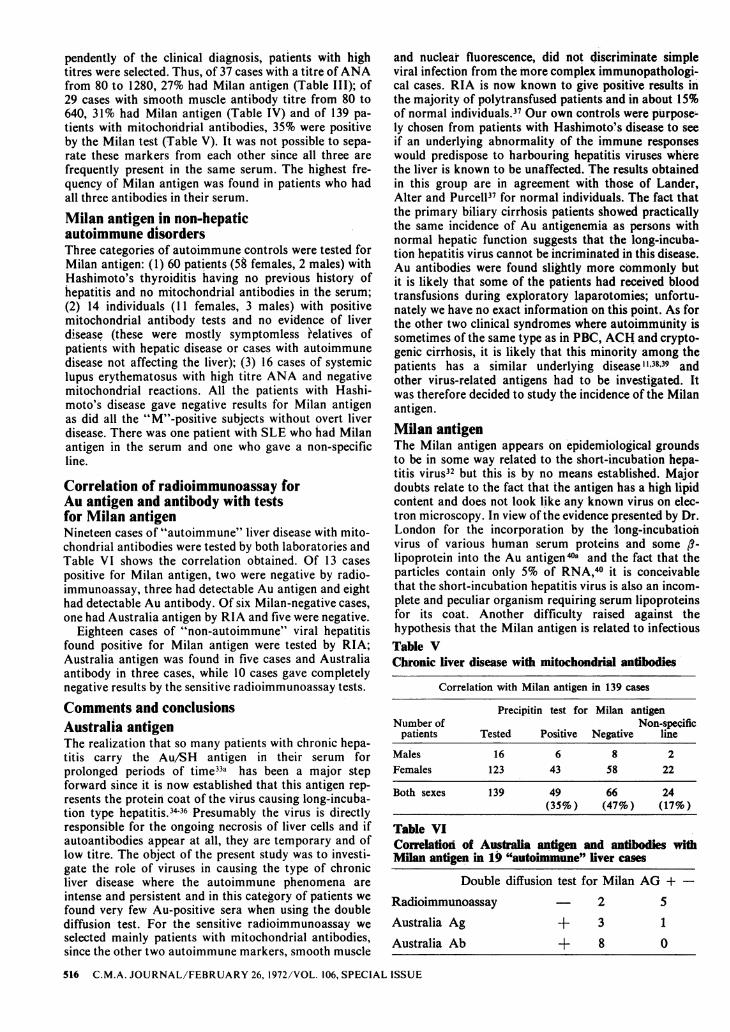
Correlation of radioimmunoassay forAu antigen and antibody with testsfor Milan antigenNineteen cases of "autoimmune" liver disease with mito¬chondrial antibodies were tested by both laboratories andTable VI shows the correlation obtained. Of 13 cases
positive for Milan antigen, two were negative by radio¬immunoassay, three had detectable Au antigen and eighthad detectable Au antibody. Of six Milan-negative cases,one had Australia antigen by RIA and Vwe were negative.
Eighteen cases of "non-autoimmune" viral hepatitisfound positive for Milan antigen were tested by RIA;Australia antigen was found in five cases and Australiaantibody in three cases, while 10 cases gave completelynegative results by the sensitive radioimmunoassay tests.
Comments and conclusionsAustralia antigenThe realization that so many patients with chronic hepa¬titis carry the Au/SH antigen in their serum forprolonged periods of time33a has been a major stepforward since it is now established that this antigen rep¬resents the protein coat of the virus causing long-incuba-tion type hepatitis.3436 Presumably the virus is directlyresponsible for the ongoing necrosis of liver cells and ifautoantibodies appear at all, they are temporary and oflow titre. The object of the present study was to investi-gate the role of viruses in causing the type of chronicliver disease where the autoimmune phenomena areintense and persistent and in this category of patients wefound very few Au-positive sera when using the doublediffusion test. For the sensitive radioimmunoassay weselected mainly patients with mitochondrial antibodies,since the other two autoimmune markers, smooth muscle
and nuclear fluorescence, did not discriminate simpleviral infection from the more complex immunopathologi-cal cases. RIA is now known to give positive results inthe majority of polytransfused patients and in about 15%of normal individuals.37 Our own controls were purpose-ly chosen from patients with Hashimoto's disease to seeif an underlying abnormality of the immune responseswould predispose to harbouring hepatitis viruses wherethe liver is known to be unaffected. The results obtainedin this group are in agreement with those of Lander,Alter and Purcell37 for normal individuals. The fact thatthe primary biliary cirrhosis patients showed practicallythe same incidence of Au antigenemia as persons withnormal hepatic function suggests that the long-incuba-tion hepatitis virus cannot be incriminated in this disease.Au antibodies were found slightly more commonly butit is likely that some ofthe patients had received bloodtransfusions during exploratory laparotomies; unfortu¬nately we have no exact information on this point. As forthe other two clinical syndromes where autoimmunity issometimes ofthe same type as in PBC, ACH and crypto¬genic cirrhosis, it is likely that this minority among thepatients has a similar underlying disease11'3839 andother virus-related antigens had to be investigated. Itwas therefore decided to study the incidence ofthe Milanantigen.Milan antigenThe Milan antigen appears on epidemiological groundsto be in some way related to the short-incubation hepa¬titis virus32 but this is by no means established. Majordoubts relate to the fact that the antigen has a high lipidcontent and does not look like any known virus on elec¬tron microscopy. In view ofthe evidence presented by Dr.London for the incorporation by the long-incubatiohvirus of various human serum proteins and some /?-lipoprotein into the Au antigen403 and the fact that theparticles contain only 5% of RNA,40 it is conceivablethat the short-incubation hepatitis virus is also an incom-plete and peculiar organism requiring serum lipoproteinsfor its coat. Another difficulty raised against thehypothesis that the Milan antigen is related to infectiousTable VChronic liver disease with mitochondrial antibodies
Table VICorrelation of Australia antigen and antibodies withMilan antigen in 19 "autoimmune" liver cases
Double diffusion test for Milan AG H-
Radioimmunoassay . 25Australia Ag +31Australia Ab +80
516 C.M.A. JOURNAL/FEBRUARY 26, 1972/VOL. 106, SPECIAL ISSUE

hepatitis virus is the fact that after prolonged search onlyone or two polytransfused sera have been found to con-tain Milan antibody, yet it is known that normal r-globulin protects against this disease. It is possible thatminute amounts of antibody are sufficient for protectionand that a radioimmunoassy is necessary to detect suchsmall traces of active immunoglobulin. As the precipitintest used for the detection of the labile Milan antigen isinsensitive and in view of the relatively long intervals oftime between collection of blood and performance of theMilan tests in our cases, it is perhaps significant that atleast 35% of patients with mitochondrial antibodies andchronic liver disease gave positive results. On electronmicroscopy the Milan antigen resembled lipoprotein-X4'which is an abnormal serum component connected withcholestasis of whatever cause. It is therefore of impor-tance that many of the PBC patients in the present serieshad no clinical jaundice at the time of testing. Prelimi-nary results suggest that Milan-positive sera do notnecessarily react in the lipoprotein-X test but this aspectof the study is still in progress. The Milan antiserum doesnot react with purified lipoprotein-X so it is unlikely thatthis theory will be substantiated. However, there may beother unidentified lipoproteins in the serum of patientswith liver dysfunction. It is conceivable that the Milanantiserum contains antibodies against human tissuecomponents and that some PBC patients might havefree mitochondrial antigen in their serum. This wouldparallel the known presence of free DNA in patients withactive systemic lupus erythernatosus and would not con-flict with the electron-microscopic appearances of Milanantigen since the mitochondrial antibodies in PBC aredirected against a lipoprotein of the mitochondrial innermembranes.42 Against this theory is the finding of Milanantigen in children with subclinical infectious hepatitisand no evidence of mitochondrial antibodies.43
If the Milan antigen is indeed related to short-incubation hepatitis virus then this organism should beseriously considered as a possible triggering agent' thatmight initiate the train of events leading to the develop-ment of "'autoimmune" liver disease in genetically pre-disposed individuals. A genetic predisposition to auto-immunity in PBC is suggested by family studies.44
We would like to acknowledge the help received in these investigationsfrom Dr. D. Costantino and Dr. M. Doglia. We are most grateful to thenurperous physicians who allowed us to test the serum of their patients,particularly Dr. R. Williams.
Mr. G. Swana provided excellent technical assistance.Work in the Middlesex Hospital is supported by the Medical Re-
search Council, The Rheumatism Foundation and the World HealthOrganisation.
References1. MEYER Z, BUJSCHENFELDE KH, KOSSLING FK: Immu-
nology ofthe Liver. London, Heinemann, 1971, p 1692. SHERLOCK S: Immunology of Liver Disease. Am J Med 49:
693-706, 19703. DONIACH D: The concept of 'autoallergic' hepatitis. Proc Roy
Soc Med 63: 527-531, 19704. WALKER JG, DONIACH D, RoITT IM, et al: Serological tests
in diagnosis of primary biliary cirrhosis. Lancet i: 827-831, 19655. GoUDIE RB, MACSWEEN RNN, GOLDBERG DM: Serologi-
cal and histological diagnosis of primary biliary cirrhosis. J ClinPathol 19: 527-538, 1966
6. WHITTINGHAM S, IRWIN J, MACKAY IR, et al: Smoothmuscle autoantibody in "autoimmune" hepatitis. Gastroenterology51: 499-505, 1966
7. KANTOR FS, KLATSKIN G: Serological diagnosis of primarybiliary cirrhosis: a potential clue to pathogenesis. Trans AssocAm Physicians 80: 267-274, 1967
8. SHERLOCK S: Diseases of the liver and biliary system. 4th ed.Philadelphia, 1968
9. GOCKE DJ, Hsu K, MORGAN C, et al: Association betweenpolyarteritis and Australia antigen. Lancet ii: 1149, 1970
10. COMBES B, STASTNY P, SHOREY J, et al: Glomerulonephri-tis with deposition of Australia antigen-antibody complexes inglomerular basement membrane. Lancet ii: 234-237, 1970
11. ZEEGEN R, STANSFELD AG, DAWSON AM, et al: Bleedingoesophageal varices as the presenting feature in primary biliarycirrhosis. Lancet ii: 9-12, 1969
12. SHERLOCK S, Fox RA, NIAZI SP, et al: Chronic liver diseaseand primary liver-cell cancer with hepatitis-associated (Australia)antigen in serum. Lancet i: 1243-1247, 1970
13. REYNOLDS TB, DENISON EK, FRANKEL HD, et al: Primarybiliary cirrhosis with scleroderma, Raynaud's phenomenon andtelangiectasia. Am J Med 50: 302-312, 1971
14. Ross A, Fox RA, SCHEUER PJ, et al: In press, 197115. POULSEN H, CHRISTOFFERSEN P: Abnormal bile duct epi-
thelium in liver biopsies with histological signs of viral hepatitis.Acta Pathol microbiol Scand 76: 383-390, 1969
16. DONIACH D, ROITT IM, WALKER JG, et al: Tissue antibodiesin primary biliary cirrhosis, active chronic (lupoid) hepatitis, cryp-togenic cirrhosis and other liver diseases and their clinical implica-tions. Clin Exp Immunol 1: 237-262, 1966
17. SADIKALI F, DONIACH D: Unpublished results18. MACKAY IR, WEIDEN S, HASKER J: Autoimmune hepatitis.
Ann NY Acad Sci 124: 767-780, 196519. JOHNSON GD, HOLBOROW EJ, GLYNN LE: Antibody to
smooth muscle in patients with liver disease. Lancet II: 878-879,1965
20. WRIGHT R: Immunology of the liver. London, Heinemann 1971,p 28
21. FARROW LJ, HOLBOROW EJ, JOHNSON GD, et al: Auto-antibodies and the hepatitis-associated antigen in acute infectivehepatitis. Br Med J ii: 693-695, 1970
22. WALKER JG, DONIACH D, WILLETTE M, et al: Virus anti-gen, immunoglobulins and autoantibodies in acute hepatitis. Gut11: 369, 1970
23. GROB PJ, JEMELKA H: Faecal S. H. (Australia) antigen in acutehepatitis. Lancet i: 206-208, 1971
24. Fox RA, NIAZI SP, SHERLOCK S: Hepatitis-associated anti-gen in chronic liver disease. Lancet ii: 609-612, 1969
24b. BULKLEY BH, HEIZER WD, GOLDFINGER SE, et al: Dis-tinctions in chronic active hepatitis based on circulating hepatitis-associated antigen. Lancet ii: 1323-1326, 1970
25a. WRIGHT R, MCCOLLUM RW, KLATSKIN G: Australia anti-gen in acute and chronic liver Oisease. Lancet ii: 117-121, 1969
25b. GITNICK GL, GLEICH GJ, SCHOENFIELD LJ, et al: Aus-tralia antigen in chronic active liver disease with cirrhosis. Lancetii: 285-288, 1969
26. VISCHER TL: Australia antigen and autoantibodies in chronichepatitis. Br Med J ii: 695-698, 1970
27. MATHEWS JD, KACKAY IR: Australia antigen in chronic hepa-titis in Australia. Br MedJ i: 259-261, 1970
28. KROHN K, FINLAYSON NDC, JOKELAINEN PT, et al: Elec-tron microscopical and immunological observations on the serum-hepatitis (S.H.) antigen in primary biliary cirrhosis. Lancet ii:379-383, 1970
29. ALARC6N-SEGOVIA D, FISHBEIN E: Australia antigen insystemic lupus. N Engl J Med 284: 448, 1971
30. WALSH JH, YALOW R, BERSON SA: Detection of Australiaantigen and antibody by means of radioimmunoassay techniques.J Infect Dis 121: 550-554, 1970
31. VYAS GN, SHULMAN NR: Hemagglutination assay for antigenand antibody associated with viral hepatitis. Science 170: 332-333,1970
32. DEL PRETE S, COSTANTINO D, DOGLIA M, et al: Detectionof a new serum-antigen in three epidemics of short-incubationhepatitis. Lancet ii: 579-581, 1970
33a. SEIDEL D, ALAUPOVIC P: An abnormal low-density lipopro-tein in obstructive jaundice. Ger Med Mon 15: 665-670, 1970
33b. CHALMERS TC, ALTER HJ: Management of the asymptoma-tic carrier of the hepatitis-associated (Australia) antigen. N EngiJMed 285: 613-617, 1971
34. DANE DS, CAMERON CH, BRIGGS M: Virus-like particles in'serum of patients with Australia-antigen-associated hepatitis.
-Lancet i: 695-698. 1970
C.M.A. JOURNAL/FEBRUARY 26, 1972/VOL. 106, SPECIAL ISSUE 517

35. SHULMAN NR: Hepatitis-associated antigen. Am J Med 49:669-692, 1970
36. COSSART Y: Australia antigen and hepatitis: a review. J ClinPathol 24: 394-403, 1971
37. LANDER JL, ALTER HJ, PURCELL RH: Frequency of anti-body to hepatitis-associated antigen as measured by a new radio-immunoassay technique. J Immunol 106: 1166-1171, 1971
38. DONIACH D, WALKER JG: A unified concept of autoimmunehepatitis. Lancet i: 813-815, 1969
39. WALKER JG, DONIACH D, DONIACH 1: Mitochrodrial anti-bodies and subclinical liver disease. Q J Med 39: 31-48, 1970
40. JOZWIAK W, KOSCIELAK J, MADALINSKI K, -et al: RNAof Australia antigen. Nature New Biol 229: 92-94, 1971
40a. BLUMBERG BS, MILLMAN 1, SUTNICK Al, et al: The natureof Australia antigen and its relation to antigen-antibody complexformation. J Exp Med 134: 320-329 s, 1971
41. HAMILTON RL, HAVEL RJ, KANE JP, et al: Cholestasis: La-mellar structure of the-abnormal human serum lipoprotein. Science172: 475-478, 1971
42. BERG PA, ROITT IM, DONIACH D, et al: Mitochondrial anti-bodies in primary biliary cirrhosis. Characterization of the inner-membrane complement fixing antigen. Clin Exp Immunol 4: 511-525, 1969 t
43. AJDUKIEWICZ A, SHERLOCK S, DONIACH D: In prepara-tion, 1971
44. FEIZi T, NACARRATO R, SHERLOCK S, et al: In prepara-tion, 1971
45. KABOTH U, SCHOBER A, ARNDT HJ, et al: Australia (S.H.)-Antigen-Befunde bei Leberkranken and Blutspendern. Dtsch MedWchschr 95: 2157-2165, 1970
46. REINICKE V, NORDENFELT E: Hepatitis-associated antigenin chronic liver disease. Lancet i: 141-142, 1970
47. KAPLAN MM, GRADY G: Serum-hepatitis antigen in chronichepatitis and primary biliary cirrhosis. Lancet i: 159-161, 1971
48. J3ERG PA, BRANDT H: In preparation, 1971
DiscussionQUESTION: Primary biliary cirrhosis and chronicactive hepatitis, are fairly well defined conditions, al-though neither one of these conditions is necessarily theresult of a single etiological factor. The third group ofpatients you labelled with the term "cryptogenic cirrho-sis". The term means to me that these are patients inwhom careful' and detailed investigation failed to revealan etiological factor. I suppose that in this third groupyou have patients whose cirrhosis is due to as many dif-ferent etiological factors as the number of patients in
this group. I would like to make a plea that when suchterms as "cryptogenic cirrhosis" are used, they shouldcarry with them a definition as to what specific etiologi-cal factors were excluded. Secondly, in such a hetero-geneous group, what meaning can one attach to the find-ing of some sort of antibodies in, say, 30% of the group?DR. DONIACH: Primary biliary cirrhosis and activechronic hepatitis are fairly well-defined conditions andclinicians in different countries tend to agree on the diag-nosis. The term "cryptogenic cirrhosis" is not acceptedeverywhere and therefore, the diagnostic criteria must bedefined. Professor Sherlock has used this term to includepatients with an established cirrhosis who usually pre-sented with ascites or bleeding from esophageal varices.Some were discovered at laparotomy undertaken forattacks simulating gall stone colic. All known causes ofcirrhosis were carefully excluded, but even so "crypto-genic cirrhosis" is a blanket term covering a number ofunrelated etiologies. If patients having mitochondrialantibodies are selected from this mixed group, they arefound to be mostly middle-aged women, some of whomhave associated thyroid autoimmunity or connectivetissue disorders.
Hiistological features such as portal lymphoid cellinfiltrates, piecemeal necrosis and granulomata aresometimes seen and the serum IgM level may be elevatedas in primary biliary cirrhosis. In England, about 25 to30% of cryptogenic cirrhosis cases appear to be of theautoimmune type. But in countries with a high rate ofalcoholism where this cause cannot always be excluded,and in Africa where unknown nutritional and toxic fac-tors are operating, only about 2 to 5% of cryptogeniccases have detectable mitochondrial antibodies.DR. LONDON: How many of the 60 patients withprimary biliary cirrhosis that were tested by radioim-munoassay had been transfused?
DR. DONIACH: These sera were received from a num-ber of hospitals and the transfusional histories of thepatients are not known to me.
518 C.M.A. JOURNAL/FEBRUARY 26, 1972/VOL. 106, SPECIAL ISSUE