visit us at drsarma
DESCRIPTION
Visit us at www.drsarma.in. Dr. R.V.S.N.Sarma., M.D., M.Sc., Consultant Physician & Chest Specialist E mail: [email protected] 3760 9226 or 2766 0593 93805 21221 or 98940 60593. Pulmonary Function Tests Ventilatory Function – Spirometry. Clinical Applications. LUNG FUNCTION TESTS. - PowerPoint PPT PresentationTRANSCRIPT

www.drsarma.in
Visit us at Visit us at www.drsarma.inwww.drsarma.in
Dr. R.V.S.N.Sarma.,Dr. R.V.S.N.Sarma., M.D., M.Sc., M.D., M.Sc.,
Consultant Physician & Chest SpecialistConsultant Physician & Chest Specialist
E mail: E mail: [email protected]@gmail.com
3760 9226 or 2766 05933760 9226 or 2766 0593
93805 21221 or 98940 6059393805 21221 or 98940 60593

www.drsarma.in
Pulmonary Function TestsPulmonary Function Tests
Ventilatory Function – Ventilatory Function – Spirometry Spirometry
ClinicalClinical ApplicationsApplications

www.drsarma.in
LUNG FUNCTION TESTSLUNG FUNCTION TESTS
Tests of VentilationTests of VentilationTests of DiffusionTests of DiffusionTests of PerfusionTests of PerfusionTests for V-P Tests for V-P
MismatchMismatch

www.drsarma.in
LUNG FUNCTION TESTSLUNG FUNCTION TESTS
Tests of VentilationTests of VentilationTests of DiffusionTests of DiffusionTests of PerfusionTests of PerfusionTests for V-P Tests for V-P
MismatchMismatch

www.drsarma.in
Function of VentilationFunction of Ventilation
Air ExitAir Exit – Airways, Bronchomotor tone, – Airways, Bronchomotor tone, Secretions, Thoracic muscles etcSecretions, Thoracic muscles etc
Air EntryAir Entry – Expansion of lungs – – Expansion of lungs – Functioning lung volume, its elastic Functioning lung volume, its elastic nature, Lung compliancenature, Lung compliance
‘‘Air Out’ ProblemAir Out’ Problem – Obstructive – Obstructive DiseasesDiseases
‘‘Air In’ problemAir In’ problem – Restrictive Diseases – Restrictive DiseasesBothBoth Air Out and In - Combined Air Out and In - Combined
www.drsarma.in
Objectives Objectives To detect Obstructive Airway Diseases To detect Obstructive Airway Diseases To quantify the severity of obstruction. To quantify the severity of obstruction. To assess response to IBD. To assess response to IBD. To identify Restrictive Lung Diseases.To identify Restrictive Lung Diseases. To identify flow-volume loop patternsTo identify flow-volume loop patterns To understand the clinical relevance. To understand the clinical relevance.
Spirometry Spirometry
www.drsarma.in
PEAK FLOW METERPEAK FLOW METER
Diagnosis of ASTHMA or COPD can beDiagnosis of ASTHMA or COPD can beconfirmed by demonstrating the confirmed by demonstrating the
presencepresenceof airway obstruction using of airway obstruction using Spirometry.Spirometry.

www.drsarma.in
PEFR - Pros and ConsPEFR - Pros and Cons
AdvantagesAdvantagesWith in 1 to 2 minutes,With in 1 to 2 minutes,Inexpensive (meter costs less than Rs.1000)Inexpensive (meter costs less than Rs.1000)Simple, useful for frequent follow up useSimple, useful for frequent follow up use
DisadvantagesDisadvantagesVery much effort dependentVery much effort dependentInsensitive to small changesInsensitive to small changesSmall airways cannot be assessedSmall airways cannot be assessedLarge inter & intra subject Large inter & intra subject
variation;variation;↓accurate↓accurate

www.drsarma.in
SPIROMETRYSPIROMETRY

www.drsarma.in
SPIROMETRYSPIROMETRY

www.drsarma.in
SPIROMETRYSPIROMETRY

www.drsarma.in
SPIROMETRYSPIROMETRY

www.drsarma.in
Spirometry - Pros and ConsSpirometry - Pros and ConsAdvantagesAdvantages
Evaluates smaller as well as larger airwaysEvaluates smaller as well as larger airwaysRelatively easy to use and maintainRelatively easy to use and maintainReversibility can be tested with IBD and steroidsReversibility can be tested with IBD and steroidsDiagnostic as well as management assessmentsDiagnostic as well as management assessments
DisadvantagesDisadvantagesCosts about 50,000 + computer and printerCosts about 50,000 + computer and printerTakes time to perform – 10 to 15 minutesTakes time to perform – 10 to 15 minutesRequires training – at least one day courseRequires training – at least one day course

www.drsarma.in
Spirometry ManeuverSpirometry Maneuver
In single breath testIn single breath testA few normal tidal respirationsA few normal tidal respirationsThen deeeeep inspirationThen deeeeep inspirationMomentary breath holdingMomentary breath holdingVery forced and fast expirationVery forced and fast expiration
As hard and as fast as he/she can blow As hard and as fast as he/she can blow outout
Then deep, quick and full inspirationThen deep, quick and full inspirationRepeat Repeat at least 3at least 3 times – take times – take the bestthe best

www.drsarma.in
Reproducibility of SpirometryReproducibility of Spirometry
Adequate explanation to the patientAdequate explanation to the patientDemonstrating the steps one by oneDemonstrating the steps one by oneEncouraging the patient to give best effortEncouraging the patient to give best effortTaking at least 3 and usually 5 attemptsTaking at least 3 and usually 5 attemptsSelecting the best effortSelecting the best effortCough and severe dyspnoea may interfereCough and severe dyspnoea may interfereNot like ECG – Not like ECG – Results depend on effortResults depend on effort

www.drsarma.in
Spirometry ResultsSpirometry ResultsFVC FVC Forced Vital CapacityForced Vital CapacityFEVFEV11 Forced Expiratory Forced Expiratory
Volume Volume in the first second in the first second FEVFEV11/FVC /FVC Ratio of the above twoRatio of the above two
PEFRPEFR Peak Expiratory Flow Peak Expiratory Flow RateRate
FETFET Forced Expiratory TimeForced Expiratory Time

www.drsarma.in
Normal
Flow-Volume
Volume-Time
Test Values

www.drsarma.in
Spirometry ResultsSpirometry ResultsFVC FVC Forced Vital CapacityForced Vital CapacityFEVFEV11 Forced Expiratory Forced Expiratory
Volume Volume in the first second in the first second FEVFEV11/FVC /FVC Ratio of the above twoRatio of the above two
PEFRPEFR Peak Expiratory Flow Peak Expiratory Flow RateRate
FETFET Forced Expiratory TimeForced Expiratory Time

www.drsarma.in
Spirometry Normal ValuesSpirometry Normal Values1.1. There are no fixed ‘Normal’ valuesThere are no fixed ‘Normal’ values
2.2. Dependent on age, sex, height, weight, ethnicityDependent on age, sex, height, weight, ethnicity
3.3. Observed value expressed as % of predicted Observed value expressed as % of predicted valuevalue
FVC FVC Normal if > 80% of predictedNormal if > 80% of predicted FEV1FEV1 Normal if > 80% of predictedNormal if > 80% of predicted FEV1/FVC FEV1/FVC At least 75%At least 75% PEFRPEFR Normal if > 80% of predictedNormal if > 80% of predicted FETFET Less than 4 secondsLess than 4 seconds

www.drsarma.in
The Four Square GameThe Four Square GameF
EV
1 N
OR
MA
LF
EV
1 <
80%
of
Pd
.
FVC NORMALFVC < 80% Pred.
80%
80%

www.drsarma.in
The Four Square GameThe Four Square Game
FVC NORMALFVC < 80% Pred.
80%
80%
Normal LungsFEV1÷FCV is N
FE
V1
NO
RM
AL
FE
V1 <
80%
of
Pd
.

www.drsarma.in
The Four Square GameThe Four Square Game
FVC NORMALFVC < 80% Pred.
80%
80%
FE
V1
NO
RM
AL
FE
V1 <
80%
of
Pd
.
Obstructive Disease
FEV1÷FCV is Low

www.drsarma.in
The Four Square GameThe Four Square Game
FVC NORMALFVC < 80% Pred.
80%
80%
FE
V1
NO
RM
AL
FE
V1 <
80%
of
Pd
.
Restrictive Disease
FEV1÷FCV is High

www.drsarma.in
The Four Square GameThe Four Square GameF
EV
1 N
OR
MA
LF
EV
1 <
80%
of
Pd
.
FVC NORMALFVC < 80% Pred.
80%
80%
Combined Obs+Res
FEV1÷FCV is N or L

www.drsarma.in
The Four Square GameThe Four Square GameF
EV
1 N
OR
MA
LF
EV
1 <
80%
of
Pd
.
FVC NORMALFVC < 80% Pred.
80%
80%
Normal LungsFEV1÷FCV is N
Obstructive Disease
FEV1÷FCV is Low
Restrictive Disease
FEV1÷FCV is High
Combined Obs+Res
FEV1÷FCV is N or L

www.drsarma.in
The Four Square GameThe Four Square GameF
EV
1 N
OR
MA
LF
EV
1 <
80%
of
Pd
.
FVC NORMALFVC < 80% Pred.
80%
80%
Normal AirEntry & Exit
Air Exit ProblemAirways choked
Air Entry ProblemLungs ↓
expansion
Both Air Entry &Air Exit Problem

www.drsarma.in
The Four Square GameThe Four Square GameF
EV
1 N
OR
MA
LF
EV
1 <
80%
of
Pd
.
FVC NORMALFVC < 80% Pred.
80%
80%
Normal LungsFEV1÷FCV is N
Obstructive Disease
FEV1÷FCV is Low
Restrictive Disease
FEV1÷FCV is High
Combined Obs+Res
FEV1÷FCV is N or L
www.drsarma.in
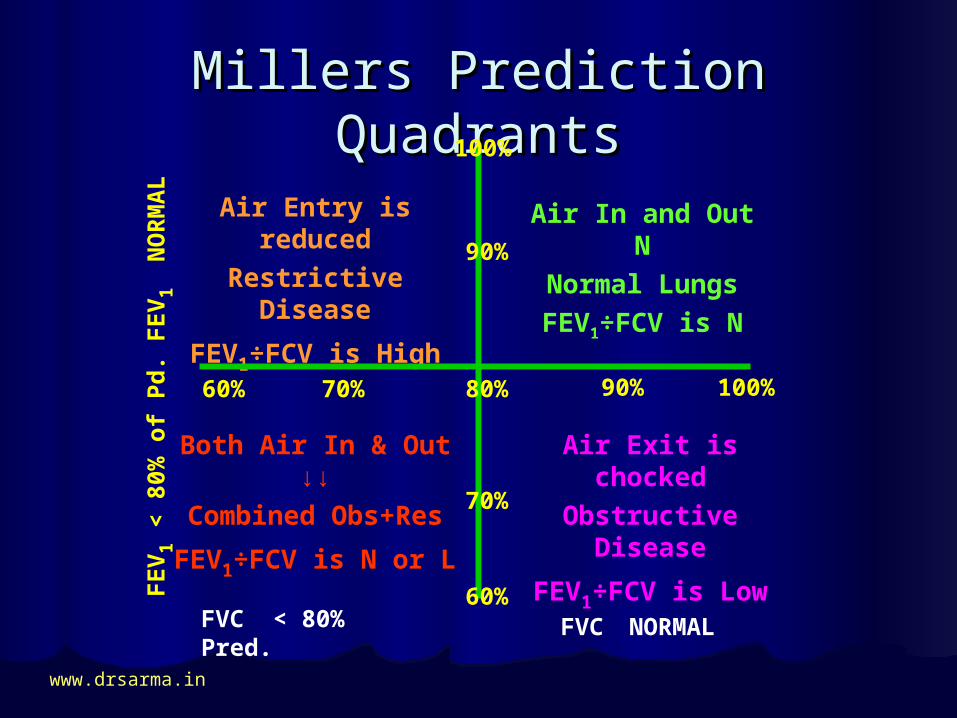
Millers Prediction QuadrantsMillers Prediction QuadrantsF
EV
1 N
OR
MA
LF
EV
1 <
80%
of
Pd
.
FVC NORMALFVC < 80% Pred.
Air In and Out NNormal LungsFEV1÷FCV is N
Air Exit is chockedObstructive
Disease
FEV1÷FCV is Low
Air Entry is reduced
Restrictive Disease
FEV1÷FCV is High
Both Air In & Out ↓↓
Combined Obs+Res
FEV1÷FCV is N or L
90% 100%70% 80%60%
90%
100%
70%
60%

www.drsarma.in
Algorithm for DiagnosisAlgorithm for Diagnosis
FVC
FVC > 80% FVC < 80%
FEV1 > 80% FEV1 < 80%
Normal PFT Obstructive
Reversible Irreversible Extra-pulmonary
FEV1 < 80%FEV1 > 80%
Restrictive Combined
Pulmonary
IBD

www.drsarma.in
Normal Airways and LungsNormal Airways and Lungs
FVC FVC > 80%> 80% FEVFEV11 > 80%> 80% FEVFEV11÷FCV÷FCV> 75%> 75%
PEFRPEFR > 80%> 80% FETFET <4 sec<4 sec
Air Entry NormalAir Entry Normal Air Exit Air Exit Normal Normal
FEV1 is LOW
FVC is Normal
FEV1 ÷ FVC is < 75%

www.drsarma.in
Normal Airways - PFTNormal Airways - PFT

www.drsarma.in
Normal PFT and CXRNormal PFT and CXR

www.drsarma.in
Bronchial Asthma – Reversible Airway Bronchial Asthma – Reversible Airway obs.obs.
Chronic bronchitis – Irreversible with IBDChronic bronchitis – Irreversible with IBDEmphysema – Irreversible with IBDEmphysema – Irreversible with IBDBronchiectasis – Airway rigidityBronchiectasis – Airway rigidityCystic FibrosisCystic FibrosisAllergic bronchopulmonary AspergillosisAllergic bronchopulmonary AspergillosisBronchiolitis Bronchiolitis
Obstructive Airways DiseaseObstructive Airways Disease
www.drsarma.in
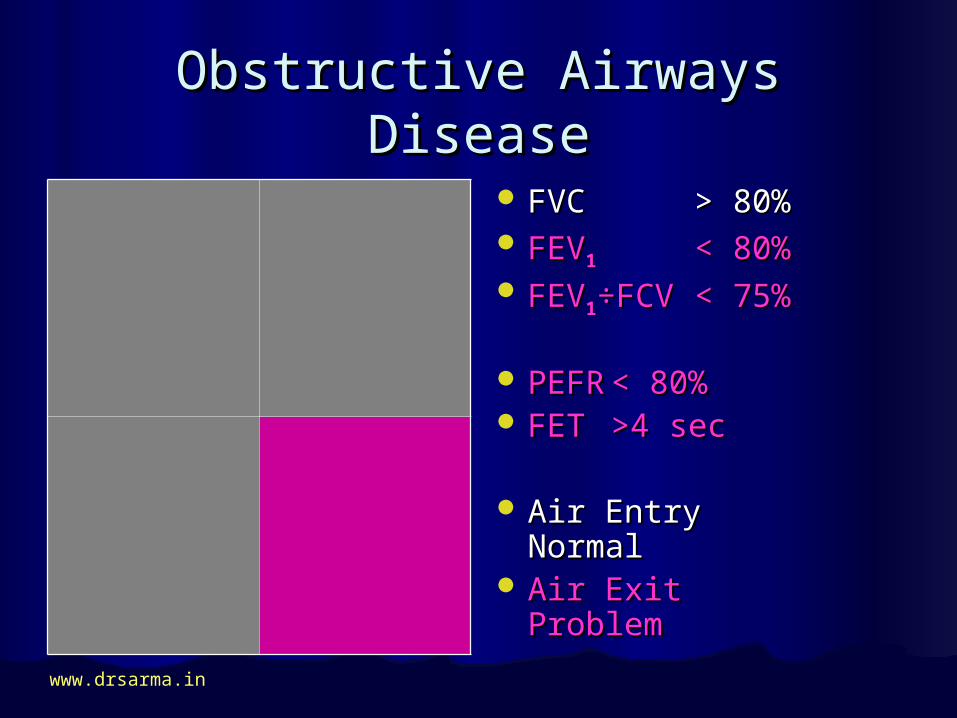
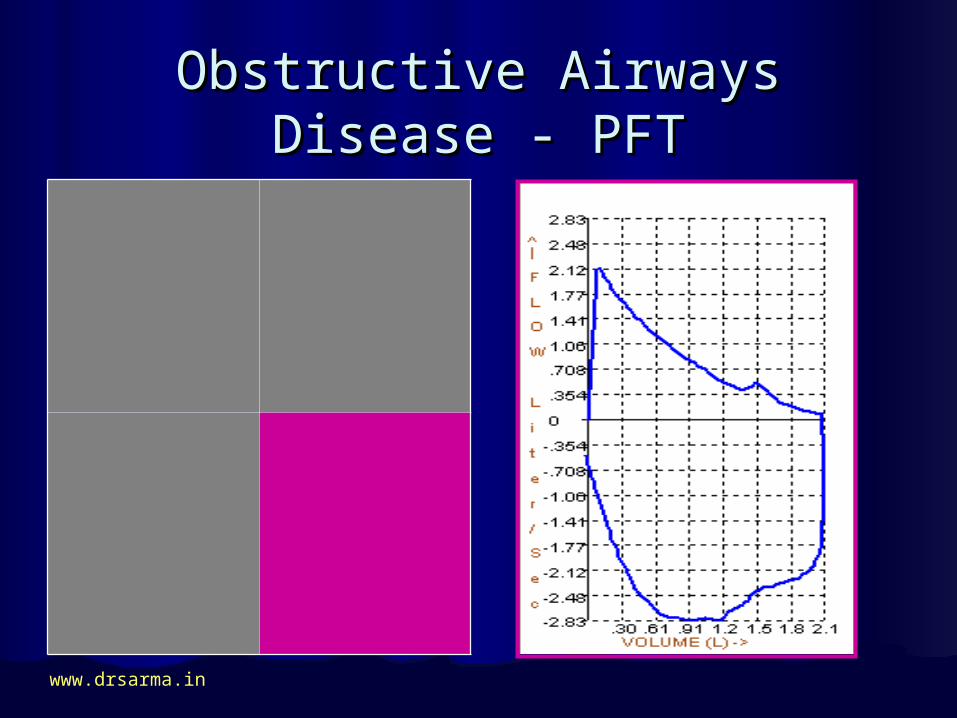
Obstructive Airways DiseaseObstructive Airways Disease
FVC FVC > 80%> 80% FEVFEV11 < 80%< 80% FEVFEV11÷FCV÷FCV< 75%< 75%
PEFRPEFR < 80%< 80% FETFET >4 sec>4 sec
Air Entry NormalAir Entry Normal Air Exit Air Exit Problem Problem
FEV1 is LOW
FVC is Normal
FEV1 ÷ FVC is < 75%
www.drsarma.in
Obstructive Airways Disease - Obstructive Airways Disease - PFTPFT
FEV1 is LOW
FVC is Normal
FEV1 ÷ FVC is < 75%

www.drsarma.in
Obstructive V/s NormalObstructive V/s Normal

www.drsarma.in
Obstructive Airways MildObstructive Airways Mild
Bronchial Asthma

www.drsarma.in
Bronchial Asthma
Reversible Obstruction (IBD)Reversible Obstruction (IBD)

www.drsarma.in
Bronchiectasis (Obstructive)Bronchiectasis (Obstructive)
BRONCHOGRAM - BIL UNILATERAL
www.drsarma.in
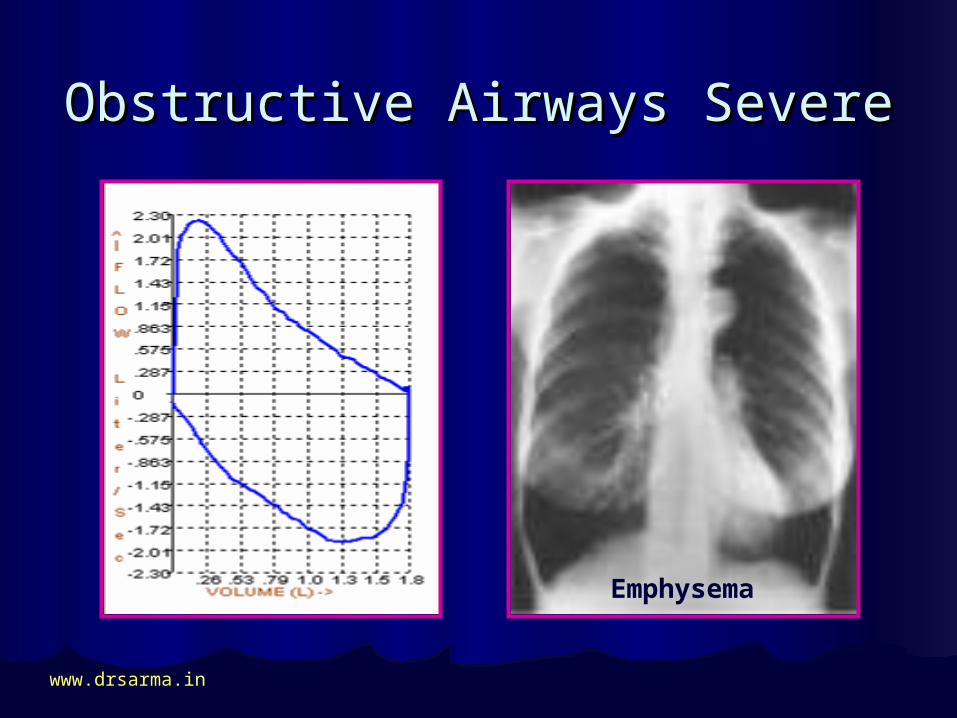
Obstructive Airways SevereObstructive Airways Severe
Emphysema

www.drsarma.in
Obstructive Airways Severe -Obstructive Airways Severe -IBDIBD
Emphysema

www.drsarma.in
Obstructive Lung DiseasesObstructive Lung Diseases
ABPA CYSTIC FIBROSIS
www.drsarma.in
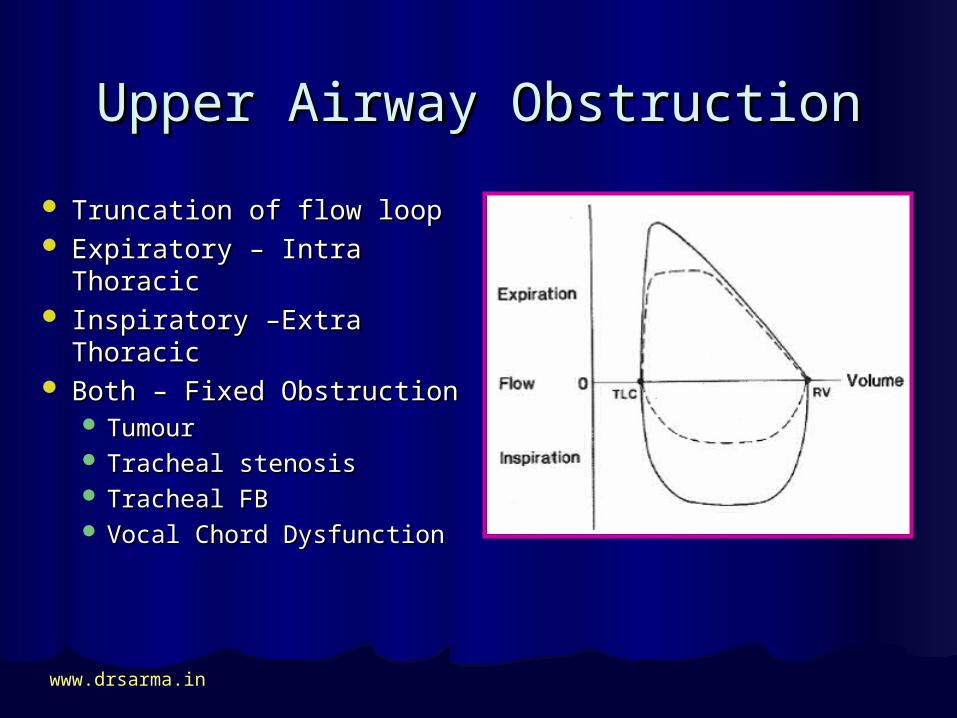
Upper Airway ObstructionUpper Airway Obstruction
Truncation of flow loop Truncation of flow loop Expiratory – Intra ThoracicExpiratory – Intra Thoracic Inspiratory –Extra Inspiratory –Extra
ThoracicThoracic Both – Fixed ObstructionBoth – Fixed Obstruction
TumourTumour Tracheal stenosisTracheal stenosis Tracheal FBTracheal FB Vocal Chord DysfunctionVocal Chord Dysfunction

www.drsarma.in
Restrictive Lung DiseasesRestrictive Lung Diseases
SarcoidosisSarcoidosisTuberculosis – (Fibrocaseous)Tuberculosis – (Fibrocaseous) Interstitial Lung Disease - ILD Interstitial Lung Disease - ILD Idiopathic pulmonary fibrosis - IPFIdiopathic pulmonary fibrosis - IPFPneumoconiosisPneumoconiosisDrug- or radiation-induced lung Drug- or radiation-induced lung
diseasediseasePneumonectomyPneumonectomy

www.drsarma.in
Extrinsic Restrictive DiseasesExtrinsic Restrictive Diseases
Kyphosis, ScoliosisKyphosis, ScoliosisAnkylosing SpondylitisAnkylosing SpondylitisMassive Pleural effusionMassive Pleural effusionPregnancy, Obesity, AscitesPregnancy, Obesity, AscitesRib fracturesRib fracturesNeuromuscular disordersNeuromuscular disorders

www.drsarma.in
Restrictive Lung DiseaseRestrictive Lung Disease
FVC FVC < 80%< 80% FEVFEV11 > 80%> 80% FEVFEV11÷FCV÷FCV> 75%> 75%
PEFRPEFR > 80%> 80% FETFET <4 sec<4 sec
Air Entry ProblemAir Entry Problem Air Exit Air Exit Normal Normal
FEV1 is LOW
FVC is Normal
FEV1 ÷ FVC is < 75%

www.drsarma.in
Restrictive Lung Disease - PFTRestrictive Lung Disease - PFT
FEV1 is LOW
FVC is Normal
FEV1 ÷ FVC is < 75%
ILD or IPF

www.drsarma.in
Restrictive V/s NormalRestrictive V/s Normal
ILD or IPF

www.drsarma.in
ILD or IPF
Restrictive Lung Disease - ILDRestrictive Lung Disease - ILD

www.drsarma.in
Restrictive Lung Disease - ILDRestrictive Lung Disease - ILD
HEPATIOD APPEARANCE

www.drsarma.in
Restrictive Lung Disease - ILDRestrictive Lung Disease - ILD
RETICULAR PERIPHERIES

www.drsarma.in
Restrictive Lung Disease - ILDRestrictive Lung Disease - ILD
HRCT Chest X-RAY CHEST - ILD

www.drsarma.in
Restrictive Lung DiseasesRestrictive Lung Diseases
SARCOIDOSIS RETICULO-NODULAR

www.drsarma.in
Combined Obstructive + Combined Obstructive + RestrictiveRestrictive
FVC FVC < 80%< 80% FEVFEV11 < 80%< 80% FEVFEV11÷FCV÷FCV< 75%< 75%
PEFRPEFR < 80%< 80% FETFET >4 sec>4 sec
Air Entry ProblemAir Entry Problem Air Exit Air Exit Problem Problem
FEV1 is LOW
FVC is Normal
FEV1 ÷ FVC is < 75%

www.drsarma.in
Combined Obstructive + Combined Obstructive + RestrictiveRestrictive
FEV1 is LOW
FVC is Normal
FEV1 ÷ FVC is < 75%

www.drsarma.in
Combined Obstructive + Combined Obstructive + RestrictiveRestrictive
KOCHS + EMPHYSEMA

www.drsarma.in
Other PatternsOther Patterns
FIXED OBSTRUCTION

www.drsarma.in
Other PatternsOther Patterns
EXTRA THORACIC
COUGH

www.drsarma.in
Case 1Case 1
TestTest Pred.Pred. MeasMeas..
%%
FVCFVC 5.5 L5.5 L 4.5 L4.5 L 82%82%
FEV1FEV1 4.9 L4.9 L 3.0 L3.0 L 61%61%
RatioRatio 89%89% 66%66% --
Man, aged 28, 172cm, 71kg
Non smoker, Cough 3 M

www.drsarma.in
Case 1Case 1
Man, aged 28, 172cm, 71kg
Non smoker, Cough 3 M
Dx : Bron Asthma - Rev
IBD Good Response
TestTest Pred.Pred. MeasMeas..
%%
FVCFVC 5.5 L5.5 L 4.5 L4.5 L 82%82%
FEV1FEV1 4.9 L4.9 L 3.0 L3.0 L 61%61%
RatioRatio 89%89% 66%66% --

www.drsarma.in
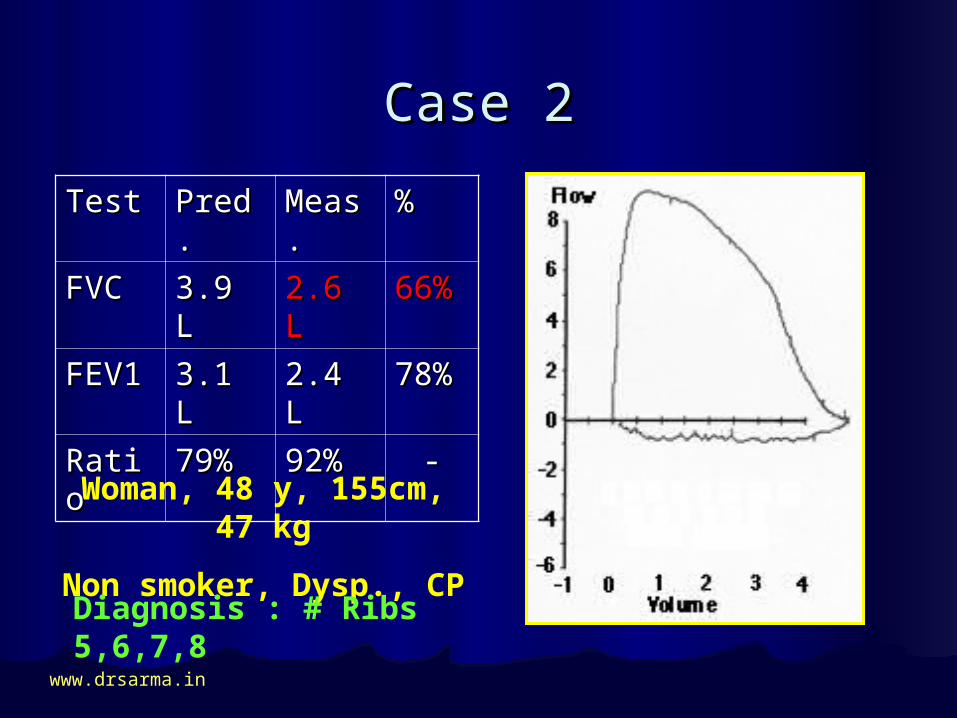
Case 2Case 2
Woman, 48 y, 155cm, 47 kg
Non smoker, Dysp., CP
TestTest Pred.Pred. MeasMeas..
%%
FVCFVC 3.9 L3.9 L 2.6 L2.6 L 66%66%
FEV1FEV1 3.1 L3.1 L 2.4 L2.4 L 78%78%
RatioRatio 79%79% 92%92% --
www.drsarma.in
Case 2Case 2
Woman, 48 y, 155cm, 47 kg
Non smoker, Dysp., CP
Diagnosis : # Ribs 5,6,7,8
TestTest Pred.Pred. MeasMeas..
%%
FVCFVC 3.9 L3.9 L 2.6 L2.6 L 66%66%
FEV1FEV1 3.1 L3.1 L 2.4 L2.4 L 78%78%
RatioRatio 79%79% 92%92% --

www.drsarma.in
Case 3Case 3
TestTest Pred.Pred. MeasMeas..
%%
FVCFVC 6.0 L6.0 L 5.0 L5.0 L 83%83%
FEV1FEV1 4.8 L4.8 L 4.1 L4.1 L 85%85%
RatioRatio 80%80% 82%82% --
Man 35, 175cm, 75kg, MC
Non smoker, Clinical N

www.drsarma.in
Case 3Case 3
TestTest Pred.Pred. MeasMeas..
%%
FVCFVC 6.0 L6.0 L 5.0 L5.0 L 83%83%
FEV1FEV1 4.8 L4.8 L 4.1 L4.1 L 85%85%
RatioRatio 80%80% 82%82% --
Man 35, 175cm, 75kg, MC
Non smoker, Clinical N
Diagnosis : Normal PFT

www.drsarma.in
Case 4Case 4
Child, 8 y, 128 cm, 19 kg
Stridor, Dysp G3, BS Decr.
TestTest Pred.Pred. MeasMeas..
%%
FVCFVC 1.9 L1.9 L 0.7 L0.7 L 36%36%
FEV1FEV1 1.6 L1.6 L 0.4 L0.4 L 25%25%
RatioRatio 84%84% 57%57% --

www.drsarma.in
Case 4Case 4
Child, 8 y, 128 cm, 19 kg
Stridor, Dysp G3, BS Decr.
TestTest Pred.Pred. MeasMeas..
%%
FVCFVC 1.9 L1.9 L 0.7 L0.7 L 36%36%
FEV1FEV1 1.6 L1.6 L 0.4 L0.4 L 25%25%
RatioRatio 84%84% 57%57% --
FB in the UAW

www.drsarma.in
Case 5Case 5
Woman, 29 y, 160cm, 41 kg
Had ATT, Dysp G3, Wheeze
TestTest Pred.Pred. MeasMeas..
%%
FVCFVC 3.5 L3.5 L 1.8 L1.8 L 51%51%
FEV1FEV1 2.8 L2.8 L 1.2 L1.2 L 43%43%
RatioRatio 80%80% 66%66% --

www.drsarma.in
Case 5Case 5
Diagnosis : TB + ABPA
TestTest Pred.Pred. MeasMeas..
%%
FVCFVC 3.5 L3.5 L 1.8 L1.8 L 51%51%
FEV1FEV1 2.8 L2.8 L 1.2 L1.2 L 43%43%
RatioRatio 80%80% 66%66% --
Woman, 29 y, 160cm, 41 kg
Had ATT, Dysp G3, Wheeze

www.drsarma.in
Case 6Case 6
Man, aged 58, 165cm, 51kg
Smoker 16yr, Severe Dysp.
TestTest Pred.Pred. MeasMeas..
%%
FVCFVC 4.5 L4.5 L 3.7 L3.7 L 82%82%
FEV1FEV1 3.6 L3.6 L 1.8 L1.8 L 50%50%
RatioRatio 80%80% 49%49% --

www.drsarma.in
Case 6Case 6
Man, aged 68, 165cm, 51kg
Smoker 16yr, Severe Dysp.
DX :COPD- Irreversible
TestTest Pred.Pred. MeasMeas..
%%
FVCFVC 4.5 L4.5 L 3.7 L3.7 L 82%82%
FEV1FEV1 3.6 L3.6 L 1.8 L1.8 L 50%50%
RatioRatio 80%80% 49%49% --
IBD NO Response

www.drsarma.in
The Four Square GameThe Four Square GameF
EV
1 N
OR
MA
LF
EV
1 <
80%
of
Pd
.
FVC NORMALFVC < 80% Pred.
80%
80%
Normal LungsFEV1÷FCV is N
Obstructive Disease
FEV1÷FCV is Low
Restrictive Disease
FEV1÷FCV is High
Combined Obs+Res
FEV1÷FCV is N or L

www.drsarma.in
Millers Prediction QuadrantsMillers Prediction QuadrantsF
EV
1 N
OR
MA
LF
EV
1 <
80%
of
Pd
.
FVC NORMALFVC < 80% Pred.
Air In and Out NNormal LungsFEV1÷FCV is N
Air Exit is chockedObstructive
Disease
FEV1÷FCV is Low
Air Entry is reduced
Restrictive Disease
FEV1÷FCV is High
Both Air In & Out ↓↓
Combined Obs+Res
FEV1÷FCV is N or L
90% 100%70% 80%60%
90%
100%
70%
60%

www.drsarma.in
Take Home PointsTake Home Points
All that wheezes All that wheezes is notis not Asthma only Asthma onlyAll Dyspnoea All Dyspnoea does notdoes not wheeze wheeze Do not over simplify dyspnoea to DeriphyllinDo not over simplify dyspnoea to DeriphyllinEtiology of Dyspnoea needs elucidationEtiology of Dyspnoea needs elucidationSpirometry tests but Ventilation function Spirometry tests but Ventilation function
onlyonlyNeed to test diffusion, Perfusion functions Need to test diffusion, Perfusion functions Cardiac, Hematologic and other causes

www.drsarma.in