visual diagnosis -...
TRANSCRIPT
Dr. Rafah F. SayyedPEC - Al Sadd, Doha
Q-PEM: Jan 2017
Visual Diagnosis

DISCLOSURE
I do not have any relevant financial
relationship with commercial interest to
disclose.

• Speed and Accuracy of Diagnosis is the key to saving lives in
emergency and critical care medicine.
• Careful Visual Inspection of the Patient, and Related Clues
help providers choose the right diagnosis and ultimately the
best treatment.
Introduction
Objectives
123
4
Clarify the Visual Clues and their
Clinical Significance
Recognize Common Pediatric
Dermatologic Conditions
Learn to Recognize Common Pediatric
Rashes
Learn to Recognize Emergent Rashes

2-yrs old boy previously healthy presented with:
Diffuse rash over bilateral LL for the past 2 days
that is progressing to his trunk and UL
He is otherwise playful and well with no fever
His parents deny new creams, or drug exposures
His parents report mild URTI 1 week ago
Case Presentation 1
Picture Title

Physical Exam:
Multiple diffuse lesions with central clearing
The lesions on palms and soles but are
most prominent on his bilateral LL
No conjunctival injection ,no sores in or
around his mouth or genitalia
Case Presentation 1 – Continued
Picture Title

What is the next most appropriate
management strategy at this time?
A: Obtain complete blood count (CBC) and blood culture, administer
ceftriaxone, and admit for observation
B: Obtain CBC and blood culture, but do not treat with antibiotics
C: Discharge to home with diphenlhydramine as needed for itching
D: Consult dermatology emergently
E: Administer subcutaneous epinephrine immediately
Question:
Picture Title

Answer: “C”Erythema multiform (minor)
EM Hypersensitivity reaction
Lesions - symmetric, palms and soles,
extensor surfaces of the UL&LL
macular, urticarial, or vesicobullous
Prototypical lesion: target lesion with a
dusky center
The rash lasts 1 week - 6 weeks
Patients are asymptomatic, sometimes
itching or involvement of the oral mucosa
Carder KR. Hypersensitivity reactions in neonates and infants. Dermatol Ther 2005;18(2):160–75.

Erythema multiform (minor)
EM The causes of EM: infectious causes, HSV
The DD of EM: pemphigus, urticaria, or other viral exanthema
Treatment: supportive (antihistamines, NSAIDS, steroids)
Evaluate mucosal surfaces to differentiate EM minor or major
EM minor: involves the skin and only one mucosal surface
EM Major (Stevens–Johnson): involves the eye, oral cavity,
genital mucosa, upper airway, or esophagus.
Carder KR. Hypersensitivity reactions in neonates and infants. Dermatol Ther 2005;18(2):160–75.

Case Presentation 2 :
8-years old boy presents to PEC with
Rash for 2 days and an inability to ambulate
due to bilateral ankle pain
Rash began on his legs and is now more
generalized, It is not painful nor pruritic.

Case Presentation 2 :
On Exam:
The child is well with normal vital signs
Lesions are palpable and do not blanch with pressure
The ankles are warm and have minimal periarticular
swelling
The right wrist is painful and warm and swelling.
The rest of the exam is normal
Laboratory tests: Normal CBC, Coag. studies, elect,
and UA, Blood culture is pending.

Case Presentation 2 :
Question:
What would be the next step in managing this patient?
A - Discharge home with close follow-up by the primary
care doctor and anti-inflammatory medications for the
joint pain
B - Admit for observation
C - Admit for intravenous antibiotic therapy
D - Consult orthopedics for an ankle arthrocentesis
E - Administer subcutaneous epinephrine
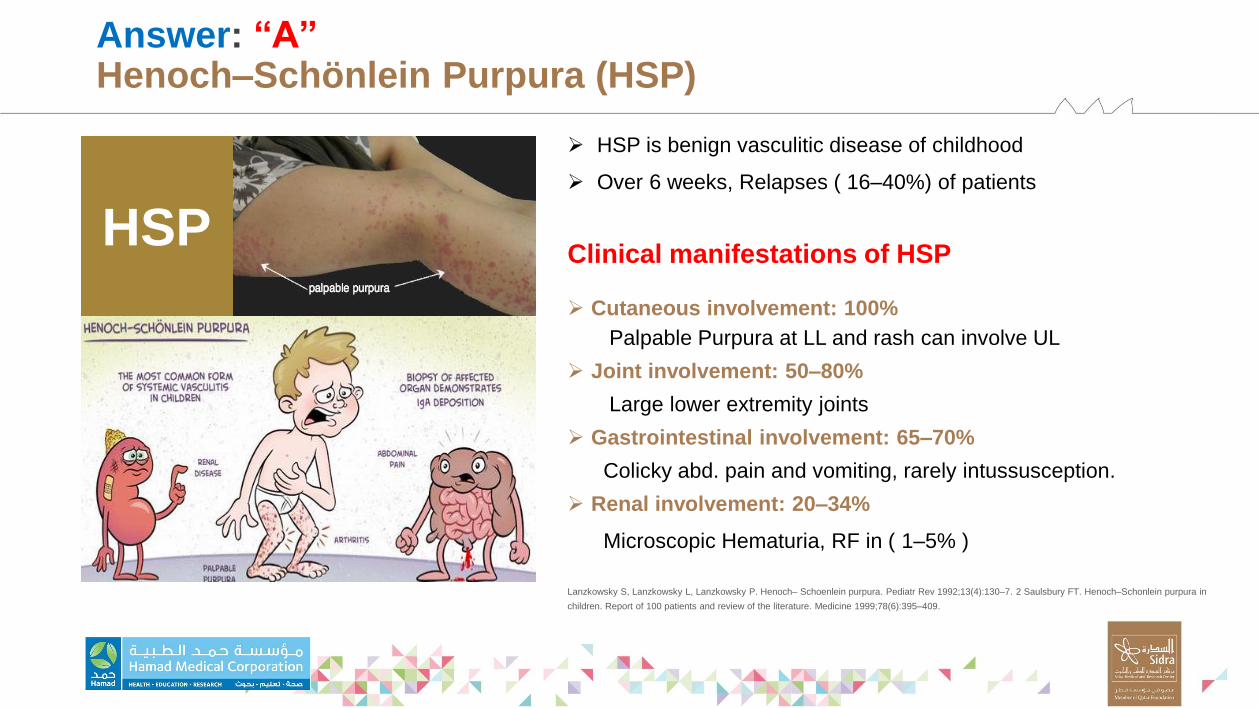
Answer: “A”Henoch–Schönlein Purpura (HSP)
HSP is benign vasculitic disease of childhood
Over 6 weeks, Relapses ( 16–40%) of patients
Clinical manifestations of HSP
Cutaneous involvement: 100%
Palpable Purpura at LL and rash can involve UL
Joint involvement: 50–80%
Large lower extremity joints
Gastrointestinal involvement: 65–70%
Colicky abd. pain and vomiting, rarely intussusception.
Renal involvement: 20–34%
Microscopic Hematuria, RF in ( 1–5% )
Lanzkowsky S, Lanzkowsky L, Lanzkowsky P. Henoch– Schoenlein purpura. Pediatr Rev 1992;13(4):130–7. 2 Saulsbury FT. Henoch–Schonlein purpura in
children. Report of 100 patients and review of the literature. Medicine 1999;78(6):395–409.
HSP

Henoch–Schönlein Purpura (HSP)
Management:
Supportive care
Weekly BP, U/A throughout the course of disease
2/3 of patients resolve their symptoms within 1mo
No evidence supports use of glucocorticoids for
treatment of abdominal pain.
DD:
meningococcemia, ITP, SBE, HUS.
Lanzkowsky S, Lanzkowsky L, Lanzkowsky P. Henoch– Schoenlein purpura. Pediatr Rev 1992;13(4):130–7. 2 Saulsbury FT. Henoch–Schonlein
purpura in children. Report of 100 patients and review of the literature. Medicine 1999;78(6):395–409.
HSP
Case Presentation-3
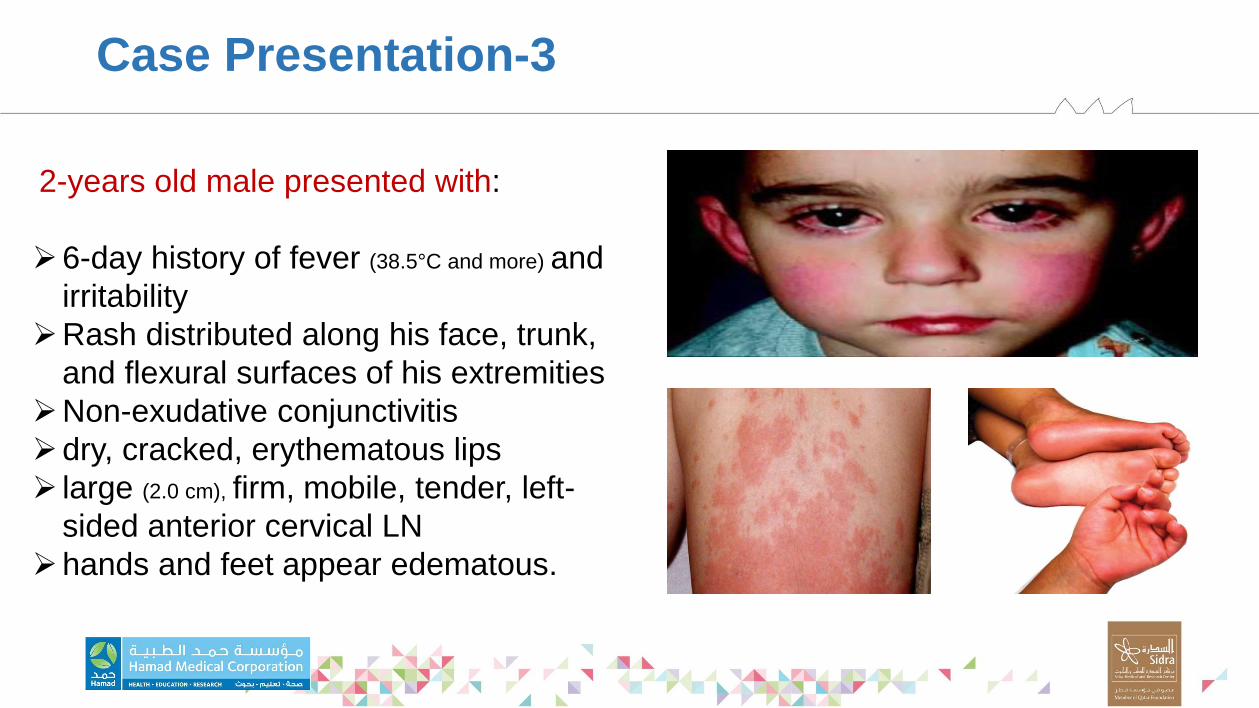
2-years old male presented with:
6-day history of fever (38.5°C and more) and
irritability
Rash distributed along his face, trunk,
and flexural surfaces of his extremities
Non-exudative conjunctivitis
dry, cracked, erythematous lips
large (2.0 cm), firm, mobile, tender, left-
sided anterior cervical LN
hands and feet appear edematous.

Case Presentation-3
Question:
Which of the following is associated
with this clinical syndrome?
A: Hemorrhagic gastritis
B: Acute renal failure
C: Intracranial abscess
D: Coronary artery aneurysms
E: Pancytopenia

Answer: “D”Kawasaki disease (KD)
Small and medium vessel vasculitis before age 5.
Common cause of acquired heart disease in children (15–25%)
Etiology remains unknown
Classic diagnosis of KD: ”Warm CREAM”
Need:
Warm: Fever > 5 days
Plus 4 of 5 :
1: Conjunctivitis (bilateral, non purulent)
2: Rash (erythematous and maculopapular)
3: Erythema palms and soles (swelling and peeling)
4: Adenopathy (cervical, unilateral node)
5: Mucous Membrane (dry, cracked, red lips and strawberry tongue)
Further reading 1 Royle J, Burgner D, Curtis N. The diagnosis and management of Kawasaki disease. J Paediatr Child
Health 2005;41(3):87–93. 2 Newburger JW, Fulton DR. Kawasaki disease. Curr Opin Pediatr
KDKD

Kawasaki disease (KD)
Don’t Forget: “A-Typical” KD
Prolonged fever (with < 4 of the above symptoms,
infants)
laboratory findings:
ESR , UA (sterile pyuria), Platelet
Echo (coronary artery abnormalities)
Treatment: IVIG, Aspirin
Further reading 1 Royle J, Burgner D, Curtis N. The diagnosis and management of Kawasaki disease. J Paediatr Child
Health 2005;41(3):87–93. 2 Newburger JW, Fulton DR. Kawasaki disease. Curr Opin Pediatr
KDKD

Approach to:
Patient with Rash
History:
1
2
3
4
What does patient think is causing rash?
Where did the lesions originate?
When did the lesion first develop? What has been the progression of rash?
Was there any prodromal to the lesions? Qu
es
tio
ns
5 What are the associated symptoms?

History:
1
2
3
4
Does it itch , hurt?
What treatment was applied if any?
Is there h/o atopy in family?
What medication do they take regularly or intermittently?
Qu
es
tio
ns
What kind of exposure do they have? 5

Physical Exam:
1
2
3
4
Examine in well-lit area
Careful inspection of the skin,
Examine the entire skin surface
Description of rash Ph
ys
ica
l E
xa
m

Description of rash
1
2
3
4
Morphology
Color
Configuration
Distribution
RA
SH

Morphology:
Primary lesions
secondary
lesions
uncomplicated abnormalities which
represent initial pathologic change
reflect progression of disease such as
excoriation , infection, or keratinization

Primary Lesions-1
Macule
Papule
Patch
circumscribed flat
discoloration
-circumscribed
--superficial solid
-elevated lesion
circumscribed flat
discoloration
(gathering of Macule)
elevated flat top
superficial lesion
(gathering of Papule)
< 1cm in diameter
< 1cm in diameter
> 1cm in diameter
> 1cm in diameter
ash-leaf spots, flat
nevi and freckle
warts, elevated nevi
insect bites
Molluscum contagiosum.
vitiligo,
tinea versicolor
Psoriasis
pityriasis rosea. Plaque

Primary Lesions - 2
Pustule
Nodule
Bulla
fluid filled lesion
vesicle with purulent
exudates
circumscribed solid
elevated lesion with
depth
fluid filled lesion
<1cm in diameter
< 1cm in diameter
< 1cm in diameter
> 1cm in diameter
herpes simplex
varicella
acne , folliculitis
secondary / tertiary
syphilis
SSSS and bullous
impetigo
Vesicle

Primary lesions-3
Purpura
Ecchymosis
Wheal
pinpoint flat red spots
under the skin surface
visible collection blood
visible collection blood
transient edematous
papule or plaque with
pale center and pink
margin
<2mm in diameter
>2mm- 1cm in
diameter
> 1cm in diameter
> 1cm in diameter
ITP/HSP
ITP
Blood disease,
vessels
hives and insect bites
Urticaria
Petechiae

Secondary Lesions:
1234
Scale
s
Crust
Excoriation
Fissure
Dry and greasy masses of keratin (fine – coarse);
pathologic process in epidermis
Dried exudates ( pus or blood)
Linear abrasion caused by scratching
Linear crack or cleavage on skin with sharply defined margins
56
Ulcer
Scar
Depressed lesion with epidermal & dermal loss
Permanent lesion result from process of repair
by replacing connective tissue

Configuration:
1
2
3
Grouped papule in Molluscum contagiosum
Shape annular plaque of Tinea corporis
Grouped vesicles-Herpes simplex
Gen
era
l sh
ap
e o
r th
e p
att
ern
in
wh
ich
th
e le
sio
n a
re a
rra
ng
ed

Distribution:

RASH:
YES Infection/Dermatological Disease
NO Purpura/Petechie=Blood/vessel Disease
Blanching?
Feverish
Texture
Nikolskys sign
YES mostly Systemic infection
NO mostly local dermatological disease
sandpaper texture in scarlet fever
Epithelial shearing caused by lateral pressure to un-
blistered skin
Algorithmic Approach
for
Rash

Algorithmic Approach I:
Maculo-papular Rash
Central Distribution Peripheral Distribution
Lesion DistributionTarget lesions
Extensor
PsoriasisE
cz
e
m
a
MeningiococcemiaSJS
EMViral
Exanthem Pityriasis
Febrile, illY
E
S
N
O YESN
O
Y
E
S
N
O Flexor

Algorithmic Approach II:
Vesiculobullous Rash
Diffuse
DistributionLocalized
Distribution
SJS
EM
Febrile Afebrile
Varicella
Purpura fulminans
Bollous Pemphigoid
Pemphigus vulgaris
Contact Dermatitis
Herpes Zoster
Necrotizing fascitis
HFM-disease

Algorithmic Approach III
Petechial/Purpuric Rash
Palpable
Febrile ,toxic Afebrile ,nonetoxic
ITP
Meningiococcemia
HSP
TTP
DIC
Autoimmune Vasculitis

Emergent Rashes in Pediatrics
Toxic Epidermal Necrolysis (TEN)
Stevens Johnson Syndrome (SJS)
Staphylococcal Scalded Skin Syndrome (SSSS)
Toxic Shock Syndrome (TSS)
Kawasaki Disease (KD)
Anaphylaxis
Purpura Fulminans

Toxic Epidermal Necrolysis (TEN)
Sudden onset, generalization in 24 – 48 hrs
Sever form of EM
Confluent erythema ,skin tenderness
Absence of target lesion , blister formation
Nikolskys sign positive
Fever, inflammation of eyelid, conjunctivae, mouth precedes skin lesion
Complicated by dehydration shock, electrolyte imbalance septicemia

Stevens - Johnson Syndrome (SJS):
Erythema , edema of lips , buccal mucosa
Then develops bullae ulceration hemorrhagic crusting
Skin lesions are bullae denuded skin
More widespread than EM
Skin tenderness is minimal to absent
Mucosal ulceration is painful
Systemic involvement present

Staphylococcal Scalded Skin Syndrome (SSSS)
Caused by Staphylococci
Common in infant and young children's
Localized bullous impetigo -to- generalized
Begins as erythema then desquamation after 5 days
Diffuse sterile flaccid blisters
Intact bullae are sterile unlike in bullous impetigo
Absence of inflammatory infiltrate is characteristics
Treated with ABC( beta - lactamase resistant)

Meningococcemia:
Fever
Rash typically petechiae & purpura
Hypotension, Adrenal failure
Multi-organ failure
Meningitis feature
Mortality rate 40%
CAUTION!!Fever + Purperic Rash (non blanching) =
Meningococcemiauntil proved otherwise

Anaphylaxis:
Life Threatening Allergic Reaction
Face - Urticaria, Swelling, angioedema
Airway- Wheezing, dyspnea
Stomach-abdominal pain, vomiting
Total body –anxiety, dizziness, hypotension
All these in few seconds to minutes
think FAST
then ACTEpinephrine
IVF

Common Rashes in Pediatrics:
MEASLES
Roseola Infantum (6th Disease)
Scarlet Fever
Kawasaki disease (KD)
Herpes Simplex
Chickenpox

MEASLES
IP:1-2 weeks
Fever: high-40, 4 days then rash
Conjunctivitis + cough
Koplik spots: 2 days before rash
opposite 2nd molars
Rash: Cephalo - caudal
Maculo - papular
Infectious: from fever to 4 days after rash, Droplet
Investigation: measles IgM, IgG
ttt: supportive + IVF+ Vitamin A

Roseola Infantum (6th Disease)
High Fever 4 days suddenly disappears
Then Rash begins
Infant 6 -12 months
T- shirt distribution: trunk and extremities
ttt: supportive
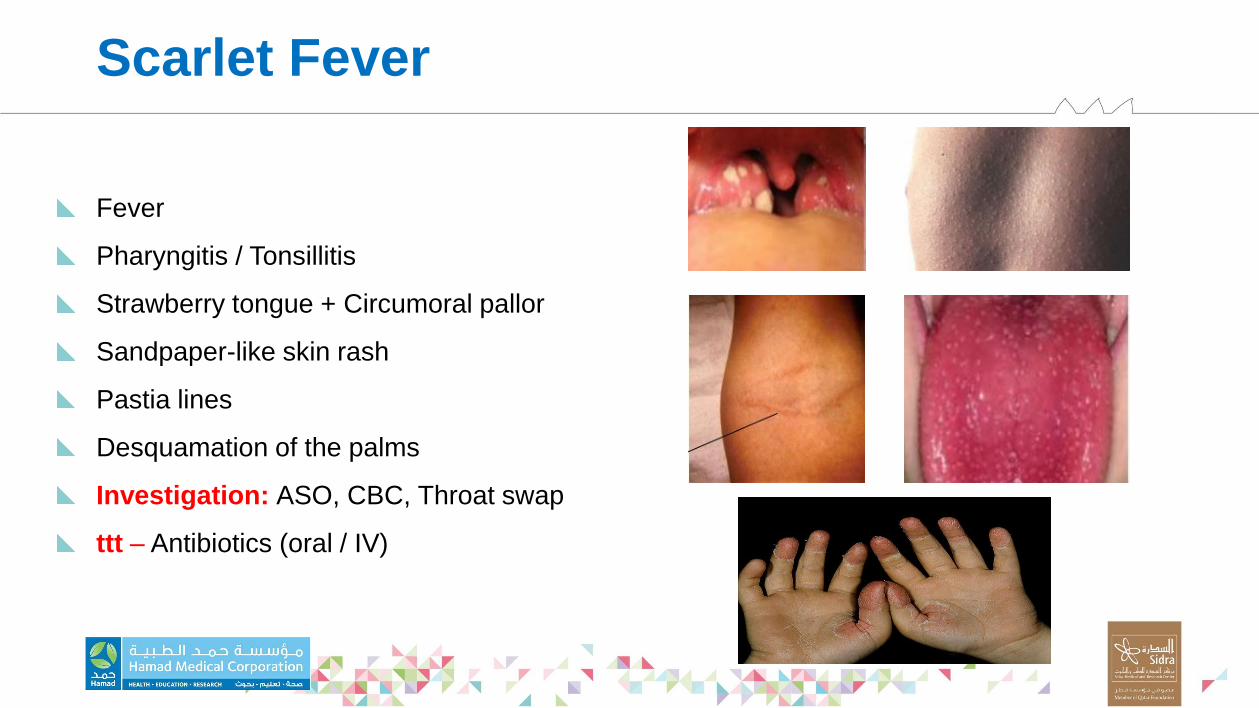
Scarlet Fever
Fever
Pharyngitis / Tonsillitis
Strawberry tongue + Circumoral pallor
Sandpaper-like skin rash
Pastia lines
Desquamation of the palms
Investigation: ASO, CBC, Throat swap
ttt – Antibiotics (oral / IV)
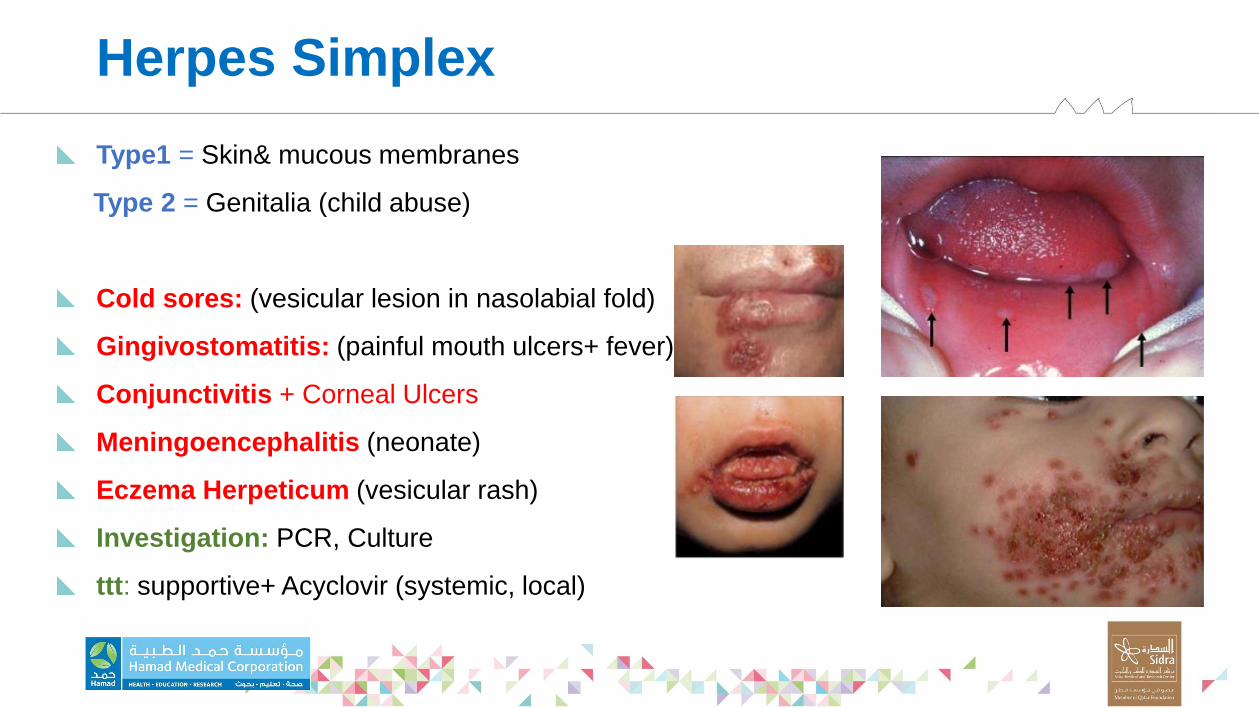
Herpes Simplex
Type1 = Skin& mucous membranes
Type 2 = Genitalia (child abuse)
Cold sores: (vesicular lesion in nasolabial fold)
Gingivostomatitis: (painful mouth ulcers+ fever)
Conjunctivitis + Corneal Ulcers
Meningoencephalitis (neonate)
Eczema Herpeticum (vesicular rash)
Investigation: PCR, Culture
ttt: supportive+ Acyclovir (systemic, local)

Chickenpox
Varicella - Zoster Virus
No Prodrom (usually)
Rash: Itchy
Vesicle + red base
( macule papule vesicle/crust
Scalp, face, trunk, proximal limbs, palms, soles, mm
Complication: 2ry bacterial infection (imptigo/cellulitis)
Spread of infection: chest, heart, CNS
Thrompocytopenia
ttt: supportive + Acyclovir (systemic, local)

Conclusion
Treating Pediatric Dermatology Patient in ED may appear
daunting, however, with a Systemic Approach one can more
readily and successfully diagnose and manage patient
effectively.

QUESTIONS?

THANK YOU!