vit b12
TRANSCRIPT

VITAMIN B12

Vitamin B12 (Cobalamin)
• Vitamin B12 is generic name for group of compounds called corrinoids
– corrin nucleus
– atom of cobalt in center
– attached are one of following
• CN = cyanocobalamin (CNCbl)
• OH=hydroxocobalamin (OHCbl)
• 5’-adenosyl=adenosylcobalamin*(AdoCbl)
• -CH3=methylcobalamin* (MeCbl)

Vitamin B12
P
H2N
N
N O
NH2
NH2
O
NH2
O
HO H
O
OH
N
H
O
OO
N
Co
N
O
O O-
O
C
NH
H2N
H2N
N
N

Sources• Seldom found in foods from plants
• Synthesis is limited to bacteria. Rumen microbial synthesis depend on the supply of cobalt in the diet
• Animal products
– Derive their cobalamin from micro-organisms
– Meat, poultry, fish, shellfish, eggs, milk, milk products
– Liver is a good source
• Supplements
– Cyanocobalamin and hydroxycobalamin

Sources of Vitamin B12 in Foods
Food Vitamin B12
(µg/100g)
Food Vitamin B12
(µg/100g)
Meats
Beef 1.94-3.64
Beef brain 7.83
Beef kidney 38.3
Beef liver 69-122
Chicken 0.32
Chicken liver 24.1
Ham 0.8
Pork 0.55
Turkey 0.379
Dairy products
Milk 0.36
Cheeses 0.36-1.71
Yoghurt 0.06-0.62
Fish and sea food
Herring 4.3
Salmon 3.2
Trout 7.8
Tuna 2.8
Clams 19.1
Oysters 21.2
Lobster 1.28
Shrimp 1.9
Other
Eggs, whole 1.26
Eggs white 0.09
Eggs yolk 9.26
Vegetables,grains,fruits none contain vitamin
B12

Digestion/Absorption• Ingested cobalamins must be released from food
matrix – Attached to polypeptides in foods– Release occurs via action of pepsin
• Functions at low pH • Requires adequate HCl production
• Released cobalamin interacts with:– R-binders (R-protein), Transcobalamin (TCI),
Haptocorrin (Hc)• R protein (found in saliva and gastric juice)• Non-specific• Complex moves from stomach into SI• In duodenum, R protein is hydrolyzed by proteases
– Inhibited by pancreatic insufficiency

Absorption
• Cobalamins bind to IF in proximal intestine– Cobalamin-IF complex travel to ileum
– Binds to receptors and is slowly absorbed into enterocyte
• Can occur by passive diffusion when pharmacologic amounts are given– Used for people not producing IF
• Malabsorption occurs– Achlorydia
– Lack of IF
– Pancreatic insufficiency
• Absorption rate decreases with increased intake (80% to 3%)

In Circulation• Cobalamins bound to one of three proteins called
transcobalamins
– TCI = binds 90% of vitamin B12 and may function as circulating storage form (hoptocorrin)
– TCII = carries newly absorbed cobalamin to tissues and helps with uptake of cobalamin• Receptors on cells for TCII
– TCIII = delivers cobalamin from periphery back to liver
– Methylcobalamin and adenosylcobalamin found primarily in blood
• Stored in liver (adenosylcobalamin)

Vitamin B12 Absorption in Ileum
Pernicious Anemia Toh, B-H et al. NEJM 337:1441,1991
End stage of type A chronic atrophic (autoimmune) gastritis
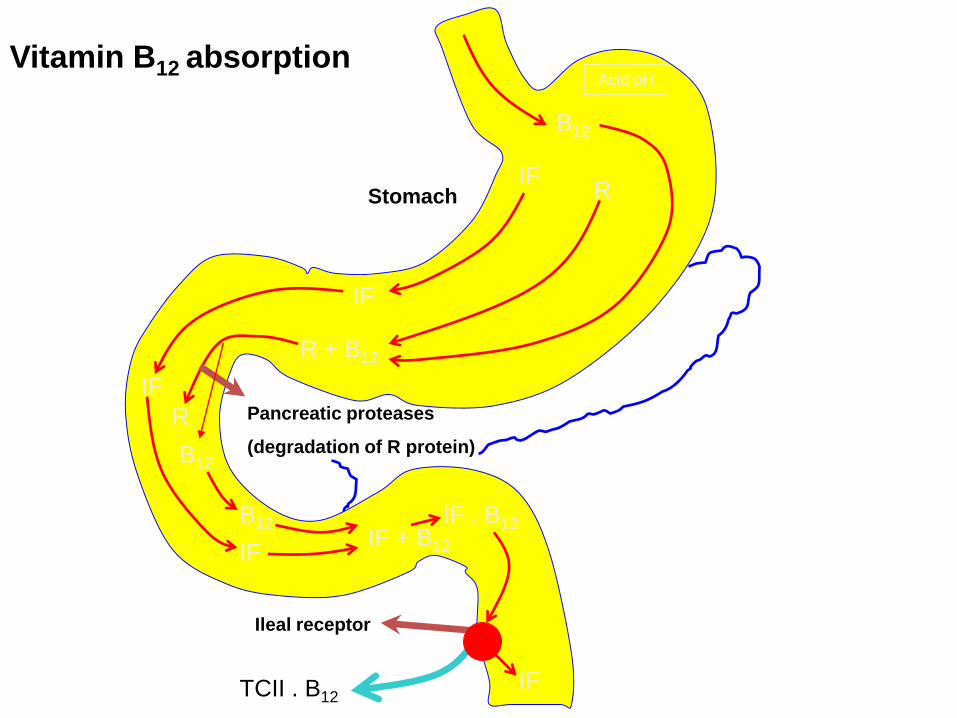
B12
R + B12
B12
B12IF + B12
IF . B12
TCII . B12
IF
IF
IF
IF
IF
R
R
Pancreatic proteases
(degradation of R protein)
Acid pH
Ileal receptor
Stomach
Vitamin B12 absorption

Transport
• TC receptors are degraded upon cellular uptake to release B12.
• All vitamin within cell is bound to protein:
– Methionine synthetase (cytosol) and methymalonyl-CoA mutase (mitochondria)
• Distribution in tissues
– Total body store 2-5mg
– Liver (60%)
– Long biological half life: 350-400 days in human.
– Low reserve in infant: about 25 μg.
– Plasma: methylcobalamin (60-80% of total)

Vitamin B12
• Metabolism
– Whole-body turnover ~ 0.1% / day
– Turnover rate is about 2.5 μg/day
– Loss of vitamin mainly due to fecal loss
• Excretion: 0.1-0.2% of total body reserve

Metabolic Roles of Vitamin B12 in Animals
Enzyme Metabolic function
Adenosylcobalamin
Methylmalonyl-CoA mutase Conversion of methylmalonyl-CoA to succinyl-CoA in
the degradation of propionate.
L-α-Leucine mutase Conversion of L-α-Leucine to aminoisocapronate as
the first step in the synthesis/degradation of the
amino acid
Methylcobalamin
Methionine synthetase Methylation of homocysteine to produce methionine,
serving as the methyl group carrier between the
donor 5-methyl-FH4 and the acceptor homocysteine

Functions
• Three known enzymatic reactions require Vitamin B12– Methylcobalamin required for methionine
synthesis from Hcy (cytosol)• Nitrous oxide inhibits MS
• Oxidizes cobalt from 1+ to 3+ state
• Must be in +1 state to function as coenzyme
– Adenosylcobalamin• Required for two reactions
• Both are mutases and function in mitochondria

Possible role of vitamin B12 in choline and methioninesynthesis
Serine Methionine
Vitamin B6 CH3-cobalamin S-adenosyl
CO2 transmethylase homocysteine
CH3-cobalamin
Ethanolamine Choline

Adenosylcobalamin
• Methylmalonyl CoA mutase
– Converts L-methylmalonyl CoA generated from propionyl CoA to succinyl CoA
– Propionyl CoA generated from oxidation of • Odd chain fatty acids
• Valine,methionine, isoleucine, threonine
– In cobalamin deficiency• Methylmalonyl CoA and methylmalonic acid (MMA)
accumulate; see rise in blood and urine
• Have observed genetic defects in methylmalonyl CoA mutase and adenosylcobalamin synthesis

Vitamin B12-dependent isomerization of methylmalonyl CoA to succinyl CoA
Valine CO2 methylmalonyl
Isoleucine mutase
Methionine Propionyl CoA Methylmalonyl CoA Succinyl CoA krebs’
Threonine adenosyl Cycle
cobalamin

Adenosylcobalamin
• Leucine Aminomutase
– Requires adenosylcobalamin as co-enzyme
– B leucine generated from bacteria in gut may be converted to L-leucine in body
– Beta leucine may also be generated from L-leucine and undergo transamination and provide alternate route for leucine catabolism
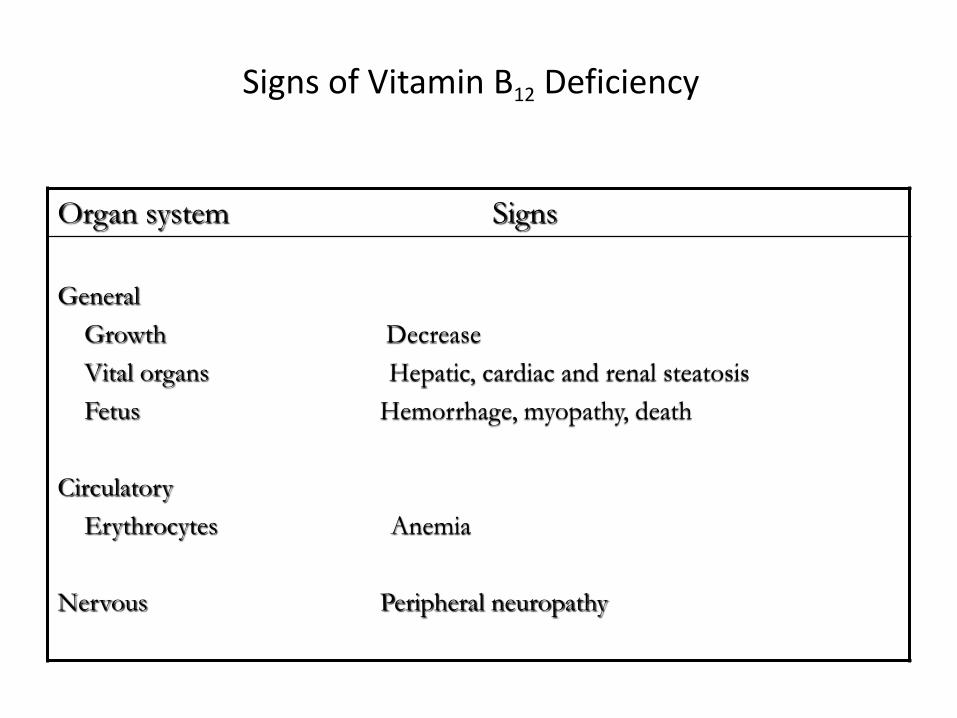
Signs of Vitamin B12 Deficiency
Organ system Signs
General
Growth Decrease
Vital organs Hepatic, cardiac and renal steatosis
Fetus Hemorrhage, myopathy, death
Circulatory
Erythrocytes Anemia
Nervous Peripheral neuropathy

Deficiency
• Definite association– Megaloblastic anemia
– Neuropathy
• Possible association– Atheroma
• Hcy
• Pernicous anemia : no increase
– NTDs• B12 association
– Hepatic steatosis• Ethanol inhibits methionine synthase
• Methionine and choline deficiency

Megaloblastic anemia
• Low B12 low methionine and THF high tHcy and 5-CH3-THF
• Low THF low 5,10-CH2-THF low conversion of dUMP to dTMP low DNA synthesis
• Low methionine and SAM: low methylene reductase– 5,10-CH2-THF 5-CH3-THF (irreversible)
– 5-CH3-THF: poor substrate for glutamate synthetase, poor incorporation into CH3-Cbl (folate deficiency)

Neuropathy• Undetected Vitamin B12 deficiency leads to
neuropathy (10+ years)
• Cause– Related to availability of methionine for SAM??
– SAM required for methylation reactions• Essential for myelin maintenance and thus neural function
• Neuropathy induced in animals by N2O inhalation
• Neuropathy associated with N2O inhalation in Humans
• Congenital deficiency

Congenital Disorders of Vitamin B12 Metabolism
Condition Missing/deficient factor Signs/symptoms
Methylmalonic aciduria
Lack of intrinsic factor
Imerslund-Gräsbeck syndrome
Lack of transcobalamins
Lack of R proteins
Methylmalonyl-CoA mutase
Intrinsic factor
IF receptors
Transcobalamins
R proteins
Methylmalonic aciduria,
homocysteinuria, lethargy, muscle
cramps, vomiting, mental
retardation
Signs consistent with vitamin
B12 deficiency
Specific malabsorption of vitamin
B12
Severe (fatal) megaloblastic
anemia appearing early in life
None

Disorders of Cbl absorption
• Malabsorption of food• Achlorydia: Corrected with synthetic source
• Pancreatic Insufficiency – Low pancreatic enzymes, bicarbonate, affect intestinal pH
• Pernicious anemia– Low If secretion, antibodies (blocking and binding)
• Gastrectomy and destruction of gastric mucosa» Treat with pharmacologic amounts of Vit B12
• Decreased absorptive surface– Ileal resection, celiac and tropical sprue, ileitis
• Parasitic Infections (Tape Worm)
• Infestation of the intestinal lumen: – Competition with bacteria
• AIDS: Low B12 (uptake of IF-B12 complex)

Vitamin B12 deficiency
• Disorders of transport– TCII deficiency (1st or 2nd month of life)
• Inherited disorders of Cbl metabolism– Disorders of AdoCbl (CblA and CblB) and
methylmalonyl CoA mutase• OHCbl to AdoCbl!!
• No megaloblastic anemia or neuropathy
• Defects in cellular CH3-Cbl and AdoCbl synthesis– Treatment with OH-Cbl: variable response
• Defects in CH3-Cbl syntheis– Failure to thrive, vomiting, anemia, neuropathy

Vitamin B12 (Cobalamin)
Common initial sign of
B12 deficiency:
The red sore tongue, with
atrophy of the papillae is often
present in pernicious anemia
and, in the case illustrated,
angular stomatitis is also
present.

Vitamin B12 (Cobalamin)
Pallor of pernicious anemia:
There is a pronounced lemon-
yellowish tint to the skin together with
faint icterus of the sclerae due to
hyperbilirubinanemia. The skin is
often velvety smooth, yet inelastic. It
is remarkable how frequently patients
have blonde or prematurely grey hair
and light-colored irises.

Potential Causes of Vitamin B12 Deficiency
Cause Example
Inadequate intake Plant-derived, unsupplemented diet
Impaired absorption Lack of IF
Pancreatic insufficiency
Intestinal parasitism
Drug treatment

Vitamin B12 Deficiency
• Inadequate absorption is primarily responsible
• Inadequate intake is more common among vegetarians
– Prevent with consumption of fortified cereals
• Occurs in stages
– Low serum concentrations
– Low cell concentrations
– Decreased DNA synthesis• High Hcy and MMA
– Megaloblastic Anemia

Assessment
– Serum B12
– MMA*
– Hcy
– Schilling test
• Used to determine problems with absorption
• Administer radioactive vitamin B12 and measure its urinary excretion