vivus investor luncheon ada 2008 scientific meeting...
TRANSCRIPT

VIVUS Investor LuncheonVIVUS Investor LuncheonADA 2008 Scientific MeetingADA 2008 Scientific MeetingOBOB--202 Results202 Results
June 10, 2008June 10, 2008San Francisco, CASan Francisco, CA

2
Leland WilsonLeland WilsonPresident and CEO, VIVUS Inc.President and CEO, VIVUS Inc.
33
NASDAQ: VVUSNASDAQ: VVUS
This presentation contains forward-looking statements about future products, future financial results and other events that have not yet occurred. Investors should be aware that actual results may differ materially from our expressed expectations because of risks and uncertainties about the future. Pharmaceutical development inherently includes significant risks in development, regulatory approval and commercialization of products. There are no guarantees that future results will meet the Company’s expectations. All Vivus products discussed herein have not been approved by the FDA and should only be used by physicians in clinical trials. Except as previously disclosed, no head to head clinical trials with approved therapies have been performed and data provided for approved therapies is from published sources which we believe are reliable. Data for other approved therapies is provided for information only. Please refer to the Company’s filings with the SEC, including its Form 10K-Annual Report and Forms 10Q-Quarterly Reports, which identify these and other risks and uncertainties that may cause actual results or events to differ materially from those presented.

4
AgendaAgendaOpening Leland Wilson, CEO
Treatment of Diabetes Nancy Bohannon, M.D.
OB-202 Results Barbara Troupin, M.D. M.B.A.
FDA Diabetes Guidelines David Orloff, M.D.
Expert Panel Timothy Garvey, M.D.
Nancy Bohannon, M.D.
Thomas Najarian, M.D.

5
Vivus ManagementVivus Management
Peter Tam– Sr. Vice President Product and Corporate Development
Dr. Wesley Day– Vice President Clinical Development
Dr. Barbara Troupin– Sr. Director Clinical Development
Dr. Charles Bowden– Director Clinical Development
Craig Peterson– Sr. Director Clinical Research

6
Panel of ExpertsPanel of Experts
W. Timothy Garvey, M.D.– University of Alabama, Birmingham
Nancy Bohannon, M.D.– St Luke’s Hospital, San Francisco
David G. Orloff, M.D.– Executive Medical Director Medpace, Inc.– Former Director of the Division of Metabolism and
Endocrinology Products at F.D.A
Thomas Najarian, M.D.– Inventor Qnexa
Dr. Nancy Bohannon, FACP, FACEDr. Nancy Bohannon, FACP, FACE
Director of Clinical Research at the Cardiovascular Risk Reduction Program
at St. Luke’s Hospital San Francisco
Treatment of DiabetesTreatment of Diabetes
Can you treat diabetes through weight loss?

9
Prevalence of CVD Risk Factors in Prevalence of CVD Risk Factors in Adults: US, 1961Adults: US, 1961--20012001
Reproduced with permission from National Institutes of Health, National Heart, Lung, and Blood Institute. Fact Book Fiscal Year 2005. 2005:52.
50
40
30
20
10
0
Percent o
f Pop
ulation
Year1960 1965 1970 1975 1980 1985 1990 1995
OverweightHypertensionSmokingHigh cholesterol
2000
60
70
2005

10

11
Link Between Obesity and Type 2 Link Between Obesity and Type 2 Diabetes: NursesDiabetes: Nurses’’ Health StudyHealth Study
Colditz GA, et al. Ann Intern Med. 1995;122:481-486.
0
20
40
60
80
100
120
< 22 22-22.9
23-23.8
24-24.9
25-26.9
27-28.9
29-30.9
31-32.9
33-34.9
> 35
BMI (kg/m2)
Age
-Adj
uste
d Re
lativ
e Ri
sk

12

13
Adipose Tissue Is an Endocrine OrganAdipose Tissue Is an Endocrine Organ
TNF=tumor necrosis factor; PAI-1=plasminogen activator inhibitor-1
Fat is a secretory/endocrine organEmerging View
LiverPancreas
Muscle
Vasculature
Leptin, fatty acids,adiponectin, TNF-α,PAI-1, cytokines
Fat is an inert storage depotTraditional View
Fatty acids Glycerol
Fatty acids Glucose
Kershaw EE, et al. J Clin Endocrinol Metab. 2004;89:2548-2556.

14
Relationship Between Relationship Between IntraIntra--abdominal Adiposity and abdominal Adiposity and
Cardiometabolic RiskCardiometabolic Risk

15
No Diabetes Type 2 Diabetes
Courtesy of Wilfred Y. Fujimoto, MD.
Extent of Visceral Fat DistributionExtent of Visceral Fat Distributionin Type 2 Diabetesin Type 2 Diabetes

16
Each 1Each 1--cm reduction in waist cm reduction in waist circumference reduces the circumference reduces the
risk of cardiovascular disease risk of cardiovascular disease by 2% to 6% in both men by 2% to 6% in both men
and womenand women

17

18
Behavioral interventionsBehavioral interventions
Several studies has shown that diet and physical activity reduced the incidence of Type 2 diabetes.
Example: The Swedish Malmo study showed that diet and exercise for 5 years in men with IGT reduced the incidence of Type 2 diabetes by 50%.
Eriksson et al, Diabetologia 1991; 34: 891-8

19
Surgically Induced Weight Loss:Surgically Induced Weight Loss:An effective therapy for diabetesAn effective therapy for diabetes

20
Scopinaro et al.: Results 10 years after Scopinaro et al.: Results 10 years after Biliopancreatic diversion (BPD)Biliopancreatic diversion (BPD)
Weight loss 49 kg (135 kg to 86 kg)
Glucose lowered to 89 mg/dl (reduction of 89 mg/dl from 178 mg/dl)
Tricylcerides lowered by 138% to 82 mg/dl from 220 mg/dl
Cholesterol lowered by 109 mg/dl to 113 mg/dl from 222 mg/dl
Scopinaro et al. Diabetes Care, 28:10, October 2005

21
Adjustable Gastric Banding and Adjustable Gastric Banding and Conventional Therapy for Type 2 Conventional Therapy for Type 2 DiabeticsDiabetics
Study: 60 patients, unblinded, randomized controlled trial to determine if surgically induced weight loss results in better glycemic control than conventional approaches
Study period: 2 years
Baseline:Study Conventional
– Weight (kg) 105 105– HbA1c 7.8 % 7.6%– TG (mg/dl) 190 189– SBP (mm Hg) 136 135– DBP (mm Hg) 87 86
Dixon, J. B. et al. JAMA 2008;299:316-323

22
Adjustable Gastric Banding and Adjustable Gastric Banding and Conventional Therapy for Type 2 Conventional Therapy for Type 2 Diabetics: ResultsDiabetics: Results
Net Change from Baseline:Study Conventional
– Weight (kg) -21 -1.5– Weight (%) -20.7% -1.7%– HbA1c -1.8 % -0.4%– TG (mg/dl) -72 -2
Remission of type 2 diabetesStudy Conventional
– Patients 73% 13%
Remission was related to weight loss and lower baseline HbA1c
Dixon, J. B. et al. JAMA 2008;299:316-323

23
SummarySummary
Obesity directly related to type 2 diabetes
Behavior modifications are helpful but often difficult for patients to achieve and maintain
Surgically induced weight loss of 20% can lead to remission of diabetes
Role of pharmacotherapy induced weight loss in type 2 diabetes….awaiting results.

Effect of Qnexa (phentermine and Effect of Qnexa (phentermine and topiramate) in Type 2 Diabetestopiramate) in Type 2 Diabetes
VIVUS Study OBVIVUS Study OB--202202
WT Garvey , B Troupin‡, P Tam‡, T Najarian‡,
C Peterson‡, WW Day‡
ADA 2008 – San Francisco*University of Alabama, Birmingham
‡ VIVUS, Inc. Mountain View, CA

25
OBOB--202 Background:202 Background:Obesity and Cardiovascular Disease SpectrumObesity and Cardiovascular Disease Spectrum
Increased Weight
Insulin Resistance
Cardiovascular Morbidity & Mortality
DiabetesDyslipidemiaHypertension Vascular Inflammation

26
The The ““OptimalOptimal”” Diabetes TherapyDiabetes Therapy
Achieves and maintains glucose lowering to guidelines– ADA < 7.0 %, IDF/WHO < 6.5%
Has a beneficial effect on other related comorbidities and ultimately cardiovascular mortality– Weight loss– Lipids– Blood pressure– Inflammation
Well tolerated and convenient (oral)
Demonstrated long term safety for chronic use

27
OBOB--202 Background: Qnexa202 Background: Qnexa
Proprietary, low dose, oral combination of two FDA approved drugs
– Phentermine, 15 mg
– Topiramate, 100 mg
Synergistic efficacy in weight loss*
* Gadde K et al, NAASO abstract 55-OR (2006); Najarian T ADA abstract 2733-PO (2007)
28
OBOB--202: Study Objective and Endpoints202: Study Objective and Endpoints
Primary: – Glycemic control (HbA1c at week 28)
Secondary: – Fasting Glucose – Blood Pressure– Lipids– Weight loss– Waist circumference

29
Placebo (N=104)
Qnexa (N=102)
Screening(2 weeks)
Titration(4 Weeks)
Treatment (24 weeks)
Week -2 Week 0 2 4 8 16 2012 24 28
OBOB--202: Study Design202: Study Design
N=206(10 Centers)
30
OBOB--202: Study Inclusion Criteria202: Study Inclusion Criteria
Subjects with type 2 diabetes
Inadequately treated with diet and exercise, oral diabetes medication
18-70 years
HbA1c 7-12%
BMI = 27-45 kg/m²
31
OBOB--202: Study Exclusion Criteria202: Study Exclusion Criteria
Use of insulin or incretins
Blood pressure greater than 150/95; triglycerides > 400 mg/dL
History of nephrolithiasis, glaucoma
Inadequately controlled depression
Unstable cardiac, pulmonary, renal, or hepatic disease
Previous bariatric surgery

32
OBOB--202: Baseline Demographics202: Baseline Demographics
PlaceboN=104
QnexaN=102
Female (%) 62 75
Mean Age (years) 48.5 50.2
Hispanic/Latino 50% 64%
Black/African American 12% 10%
Weight (kg) 98.1 94.7
BMI (kg/m2) 35.1 35.3
33
OBOB--202: Study Population202: Study Population
At study entry– Wide range of duration and severity of
disease– On a variety of oral diabetes medications
During study– Intervention with oral diabetes medications
permitted at any time during treatment

34
OBOB--202202: : Baseline Medical HistoryBaseline Medical History
PlaceboN=104
QnexaN=102
Cardiovascular 71% 65%
Central Nervous System 46% 53%
Metabolic (ex-DM2) 48% 50%
Gastrointestinal 57% 56%
Psychiatric 14% 18%

35
OBOB--202: Baseline Diabetes Therapy202: Baseline Diabetes Therapy
0
10
20
30
40
50
60
70
Per
cent
age
of S
ubje
cts
Placebo
Qnexa
Drug Naive
Metformin Monotherapy
>2 Diabetes Medications
More than 60% of subjects were on 2 or more diabetes medications
36
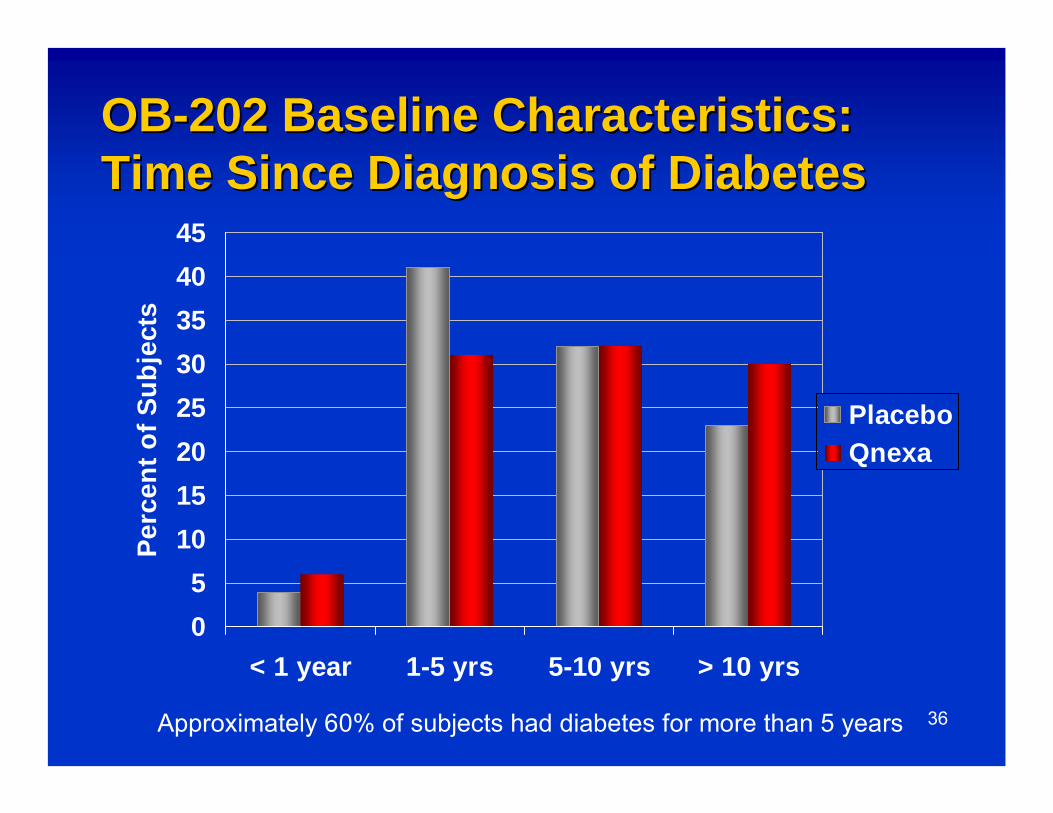
OBOB--202 Baseline Characteristics: 202 Baseline Characteristics: Time Since Diagnosis of DiabetesTime Since Diagnosis of Diabetes
05
1015202530354045
< 1 year 1-5 yrs 5-10 yrs > 10 yrs
Perc
ent o
f Sub
ject
s
PlaceboQnexa
Approximately 60% of subjects had diabetes for more than 5 years

37
OBOB--202: Demographics202: Demographics
Hispanic subjects in Qnexa group represented a majority compared to placebo (p=0.050)
62% of Qnexa subjects were on 2 or more oral diabetes medications– Most subjects were on medication at baseline for
other co-morbidities
60% had diabetes diagnosis greater than 5 years– 30% of Qnexa subjects had diabetes > 10 years

38
OBOB--202: Baseline Glycemic Parameters202: Baseline Glycemic ParametersPlacebo
N=104
Qnexa
N=102
Fasting Glucose (mg/dL) 174.0 174.7
Mean HbA1c 8.6% 8.7%
HbA1c 7-8 (% subjects) 38% 39%
HbA1c >8-12 (% subjects) 62% 61%

39
OBOB--202 Results: Change from 202 Results: Change from Baseline HbA1c (ITT, LOCF)Baseline HbA1c (ITT, LOCF)
p <0.001 at each time point
-1.4
-1.2
-1
-0.8
-0.6
-0.4
-0.2
0
Baseline Week 16 Week 28
Cha
nge
in H
bA1c
PlaceboQnexa

40
OBOB--202 Results: Change in Fasting 202 Results: Change in Fasting Glucose (ITT, LOCF)Glucose (ITT, LOCF)
135
145
155
165
175
Baseline Week 4 Week 16 Week 28
Fast
ing
Glu
cose
(mg/
dL)
QnexaPlacebo
p <0.001 at each time point

41
OBOB--202 Results: Change in Diabetic 202 Results: Change in Diabetic Medication During StudyMedication During Study
-20
-10
0
10
20
30
Net
cha
nge*
in M
eds
PlaceboQnexa
* Net change = number of medication additions (or dosage increases) minus number of medication subtractions (or dosage
Number of Meds Dosage of Meds

42
OBOB--202 Results:202 Results: % of Subjects Achieving % of Subjects Achieving ADA Glycemic GoalsADA Glycemic Goals
0%
10%
20%
30%
40%
HbA1c < 7.0% HbA1c < 6.5%*
Perc
ent o
f Tre
atm
ent G
roup Placebo
Qnexa
**
Baseline HbA1c: Placebo 8.6%, Qnexa 8.7%
*Incidence of hypoglycemia for Active and Placebo: 6% vs. 5% **p<0.01
**

43
OBOB--202 Results: Percent Change in 202 Results: Percent Change in Body Weight (ITT, LOCF)Body Weight (ITT, LOCF)
-10
-8
-6
-4
-2
0
0 2 4 8 12 16 20 24 28
Cha
nge
from
Bas
elin
e (%
Wei
ght L
oss)
QnexaPlacebo
p <0.0001 at each time point
-1.2%
-8.0%
Weeks

44
OBOB--202 Results: Changes in CV 202 Results: Changes in CV Risk FactorsRisk Factors
Placebo Qnexa p-value
Systolic Blood Pressure (mmHg) ↑ ↓ <0.01
Diastolic Blood Pressure (mmHg) ↑ ↓ <0.05
Triglycerides (mg/dL) ↑ ↓ ↓ <0.05
Total chol/HDL ↑ ↔ <0.05
Waist Circumference (cm) ↓ ↓ ↓ <0.0001
Patients at study entry were well managed for lipids and BP

45
OBOB--202 Results: Adverse Events 202 Results: Adverse Events (% subjects)(% subjects)
Placebo Qnexa
Nausea 5% 18%
Paresthesia 0% 17%
Constipation 2% 10%
Insomnia 4% 9%
Dry Mouth 1% 8%

46
OBOB--202 Cognitive Adverse Events202 Cognitive Adverse Events
Cognitive events related to memory and attention, were mild to moderate, and manageable (7 Qnexa, 1 Placebo)
No discontinuations due to cognitive events
6 of 7 Qnexa subjects with cognitive events completed study
Note: Bray reported 23% of subjects had difficulty with memory and 9% had attention/concentration difficulty on the 96 mg topiramate alone dose in a 6 mo weight loss study.
Bray et al, Obesity Research 11:6 (2003)

47
OBOB--202 Results: Depression/Mood 202 Results: Depression/Mood ObservationsObservations
Depression/Mood cases were mostly mild, brief and manageable (5 Qnexa, 1 placebo)
3 cases were considered related, 3 unrelated
All Qnexa subjects completed the trial on treatment
No discontinuations due to depression/mood for Qnexa

48
OBOB--202: Patient Health 202: Patient Health Questionnaire (PHQQuestionnaire (PHQ--9)9)
PHQ-9: a validated, nine-item tool used to screen for depression at baseline and during the study

49
OBOB--202: Mean PHQ202: Mean PHQ--9 Scores (9 Scores (±±SE)SE)
Baseline Week 28
Placebo 2.8 (± 0.24 ) 2.1 (± 0.25 )
Qnexa 3.0 (± 0.31 ) 1.6 (± 0.29 )*
*P<0.05 vs. baseline

50
OBOB--202 Results: Retention and 202 Results: Retention and TolerabilityTolerability
Placebo Qnexa
Study Completion 72% 85%
Discontinuation due to AEs 4% 3%
Note: Bray reported 23% dropouts due to AEs for the 96 mg topiramate alone dose in a 6 mo weight loss study.
Bray et al, Obesity Research 11:6 (2003)

51
OBOB--202 Results: Safety Summary202 Results: Safety Summary
Discontinuations due to AEs – 3 in Qnexa: colon ca, nausea/vomiting, intermittent
disorientation– 4 in Placebo: colon ca, viral infection, eye
pain/vision change, dry mouth/forgetfulness
No drug related SAEs
Total SAEs– 5 in Qnexa: colon ca, anemia, gallbladder, viral
infection, osteoarthritis– 6 in Placebo: colon ca, cardiac (3), stroke, non-
cardiac chest pain

52
0
2
4
6
8
10
12
14
Physicalfunction
Self esteem Publicdistress
Total score
Domains
Cha
nge
from
Bas
elin
e in
QoL
Placebo
Qnexa
*
**
*
* p< 0.05** p< 0.01
OBOB--202: Impact of Weight Loss on 202: Impact of Weight Loss on Quality of LifeQuality of Life
*

53
OB 202: Patient SatisfactionOB 202: Patient Satisfaction
“How has the study treatment affected your ability to lose weight and maintain weight loss?”
"Greatly Improved"
0%
10%
20%
30%
40%
50%
60%
70%
Treatment Groups
% o
f Sub
ject
s R
epor
ting
PlaceboQnexa

54
OBOB--202 Results: Efficacy Summary202 Results: Efficacy Summary
1.2% reduction in HbA1c from baseline (ITT)
8.0% reduction in weight from baseline (ITT)
Significant improvements seen in:• Systolic and diastolic blood pressure• Triglycerides• Waist circumference• Quality of life (IWQoL)

55
VIVUS OBVIVUS OB--202: Conclusion202: Conclusion
Qnexa provided HbA1c reductions comparable to currently available oral diabetic medications, with the additional benefit of significant weight loss and importantly, significant improvement in cardiovascular risk factors
Qnexa was well tolerated

Dr. David OrloffDr. David Orloff
Executive Director of Medical and Regulatory Affairs, Medpace

57
U.S. RegulatoryU.S. RegulatoryPerspective on Diabetes Drug Perspective on Diabetes Drug DevelopmentDevelopment
David G. Orloff M.D.Executive Director, Regulatory Affairs
Medpace, Inc.

58
FDAFDA’’s guiding principles of drug s guiding principles of drug regulationregulation
Clinical risk vs. benefit calculus
Upside: public health value
Downside: public health risk dictates required level of assurance of safety

59
FDAFDA’’s benefits benefit--risk Equation: chronic risk Equation: chronic preventive therapiespreventive therapies
Risk of condition (thus potential benefit of therapy)– Continuum from mild morbidity to mortality– Short-term vs. long-term disease natural history
Benefit of drug:– Meaningful benefits experienced by small or large fraction of treated
patientsDrug tolerability/compliance also factors
– Ancillary “beneficial’ effects– Evidence of risk reduction (biomarkers vs. endpoints)
Risk of drug:– Reversible vs. irreversible– Severity, frequency– Temporal relationship to start of tx, dosing– Monitorability– Manageability: predictability, preventability
60
FDA value judgment for a new FDA value judgment for a new drug: public health needdrug: public health need
Risk-benefit evaluations are made in the context of the current armamentarium
Does a new drug address an unmet need?
Does it represent a therapeutic advance?
Can we meet or exceed the effects of the new drug with single or combination approved txs?

61
Height of Height of ““barbar”” varies directly with varies directly with size of target populationsize of target population
Expanding the indication increases number potentially to harm, requiring…
Greater assurance of safety, requiring…
Larger numbers of patients studied,
Longer periods of follow up, and
More intensive on-study monitoring

62
Risk Management issues for FDARisk Management issues for FDARisk mitigation can never be 100%
– Acceptability of risk relies on nature of risk, both relative and absolute risks, and significance of benefits
– Can entry into the market be moderated?
Can individuals at risk be prospectively identified?
Is monitoring for emergent adverse effects available to permit pre-emptive action?
If adverse effects do arise, are they reversible?
What is the scope of the risk management problem?
Are there built-in risk mitigators (tolerability, route of administration, cost)?
Is it possible to educate around risks?
63
Treatment of Diabetes with Obesity Treatment of Diabetes with Obesity Drugs Drugs
2008: a path but no precedents
Standard of evidence of benefit
Safety exposures
Presumptions about labeling
Necessary studies

64
Obesity Drugs for DiabetesObesity Drugs for Diabetes
2008: the door has been opened– Weight loss independent effects no longer
needed
Surrogate-based approval: HbA1c– Additionally: reduction in insulin
requirements, reduction in OADs– Need for M&M outcomes conditional on
safety concerns
65
Open door: Weight loss with Open door: Weight loss with improvement in glycemia is enoughimprovement in glycemia is enough
No precedents dictating specific clinical development path– Diabetes guidance recommends 2500 total,
1500 for one yr, 500 for 18 months– Presume build on obesity program for safety
FDA may be concerned about overall increased medical risk in DM population compared to non-diabetic obese
Presume MOA-driven CDP

66
Diabetes indications now Diabetes indications now ““standardizedstandardized”” with disclaimers as with disclaimers as applicableapplicable
[drug] is indicated as an adjunct to diet and exercise to improve glycemic control in [adults/children] with type 2 diabetes mellitus– Limitations on use: [drug] has not been
studied [as monotherapy or] in combination with [approved agent] nor studied extensively with [approved agent]

67
Standard diabetes programStandard diabetes program
Monotherapy: 6-month placebo controlled in naïve/washout patients
Add-on to max or near max doses of one or more OADs (met, SU, TZD, DPP-4i)– FDA believes this mimics SOC– FDA believes avoid issues related to
upward dose titration of background OADs
Add-on to insulin

68
Rationale for Unique Development Rationale for Unique Development ProgramProgram
Primary/dominant effect may weight loss-associated improvements in mediators of risk/risk factors
No tendency to directly cause hypoglycemia
Addresses critical/universal management issue in T2DM
Primary PD effect is monitorable, as are multiple secondary risk factor modifications
No clinical reason to “stage” intervention with weight loss agent

69
Opportunities in Prevention with Opportunities in Prevention with Effective Weight Loss and Effective Weight Loss and MaintenanceMaintenance
Cardiovascular: hypertension, Cardiovascular: hypertension, coronary artery disease, angina coronary artery disease, angina pectoris, congestive heart failurepectoris, congestive heart failure
Cerebrovascular: strokeCerebrovascular: stroke
HyperlipidemiaHyperlipidemia
Metabolic syndrome/type 2 DMMetabolic syndrome/type 2 DM
CholelithiasisCholelithiasis
Gout, uric acid nephrolithiasisGout, uric acid nephrolithiasis
OsteoarthritisOsteoarthritisObstructive sleep apnea, Obstructive sleep apnea, hypoventilationhypoventilationHyperandrogenism, hirsutism, Hyperandrogenism, hirsutism, irregular menses, complications irregular menses, complications of pregnancy, stress of pregnancy, stress incontinenceincontinenceMalignancies: breast, Malignancies: breast, endometrium, colon, prostateendometrium, colon, prostateIncreased surgical riskIncreased surgical riskPsychological disordersPsychological disorders

70
FDAFDA’’s Role in Diabetess Role in Diabetes--Obesity Obesity Drug DevelopmentDrug Development
The magnitude of the obesity epidemic, its contribution to chronic disease, its costs to individuals and society, and the absence of broadly effective therapeutics constitute a “call to action” by the collective medical community, including FDATo advance the field of diabetes-obesity therapeutics, FDA must provide guidance around resolution of issues related to real or perceived barriers to development The “quality” of the diabetes-obesity armamentarium ultimately should be on par with those in other areas of preventive medicine

71
Proposed Development PlanProposed Development Plan
Assume that trial scope, design, choice of background tx not fixed– Consider monotherapy vs. placebo in naives or
patients washed out of meds or combination with met as initial tx
– Consider add on to stable regimens “based” on commonly used medication classes
E.g., Metformin-based, TZD alone or in combo, insulin-based, incretin-based
– Consider small study in Type ½– Explore diabetes prevention in IGT

72
Leland WilsonLeland WilsonPresident and CEO, VIVUS Inc.President and CEO, VIVUS Inc.
73
Qnexa News Flow 2008Qnexa News Flow 2008
OB-202 ADA presentation Q2 2008
Top-line data from EQUATE (obesity) Q4 2008
Top-line data from DM-230 (diabetes) Q4 2008

74
Panel of ExpertsPanel of Experts
W. Timothy Garvey, M.D.,– University of Alabama, Birmingham
Nancy Bohannon, M.D.– St Luke’s Hospital, San Francisco
David G. Orloff, M.D.– Executive Medical Director Medpace, Inc.– Former Director of the Division of Metabolism and
Endocrinology Products at F.D.A
Thomas Najarian, M.D.– Inventor Qnexa

Questions and DiscussionsQuestions and Discussions

VIVUS Investor LuncheonVIVUS Investor LuncheonADA 2008 Scientific MeetingADA 2008 Scientific MeetingOBOB--202 Results202 Results
June 10, 2008June 10, 2008San Francisco, CASan Francisco, CA