vol. 4 - the society of physicians of hong kongsophysicianshk.org/journal/2012_03.pdf · journal of...
TRANSCRIPT

March 2012 • Vol. 4 • No. 2
Journal of the Society of PhySicianS of hong Kong
ISSN 2072-4209
executive committee
PRESIDENT
Dr Lam tat chung, Paul 林達聰醫生
VIcE PRESIDENT
Dr tsang Wah tak, Kenneth曾華德醫生
HoN. SEcRETaRy
Dr Shiu cho tak, Wesely邵祖德醫生
HoN. TREaSuRER
Dr Lam how mo, ignatius 林孝武醫生
cHIEF EDIToR
Dr Lau chu Pak 劉柱柏醫生
eDitoRS
Dr chan hin Lee, henry 陳衍里醫生
Dr chan Kwok Wing, fredriech 陳國榮醫生
Dr chan Pui yiu, nicola 陳珮瑤醫生
Dr chan tak hin 陳德顯醫生
Dr chen yi tin 陳以天醫生
Dr Kung Wai chee, annie龔慧慈醫生
Dr Lam tat chung, Paul 林達聰醫生
Dr Lam cheung cheung, Barbara藍章翔醫生
Professor Leung Wai Keung 梁偉強教授
Dr ng fook hong 吳福康醫生
Dr Shiu cho tak ,Wesely 邵祖德醫生
Dr tsang Wah tak, Kenneth 曾華德醫生
Dr Wong chun yu, Benjamin 王振宇醫生
CONTENTS
16 Respiratory Syncytial virus Bronchiolitis in young infants – update on management and Prevention
Dr Lam Cheung Cheung, Barbara, JP (藍章翔醫生、太平紳士)
20 Rheumatoid arthritis: advances in therapeutics
Dr Cheung Tak Cheong (張德昌醫生)
22 the challenge and essence of the management of Psoriasis
Dr Hui Shiu Kee (許紹基醫生)
25 Role of chemotherapy in Soft tissue Sarcoma Dr Loh Kai Tsu, Kevin (陸凱祖醫生)
www.sophysicianshk.orgVisit the web site for our monthly cME programmes for doctors
香港內科學會THE SOCIETY OF PHYSICIANS OF HONG KONG


InthisissuewearepleasedtopresentarticlesbyDrBarbaraLam,DrCheungTakCheong,DrHuiShiuKeiandDrKevinLoh.
Allareseniorclinicianswithalottoshareintheirrespectivespe-cialties.Iamsureyouwillderivemuchbenefitfromtheseinformativeyeteasytoreadarticles.
With3yearsofexperiencebehindusinrunningthisJournal,weareconfidenttobeabletoimprovethestandardofthepublication.Wewillcontinuetobringtoyoucutting-edgeinformationindifferentaresinInternalMedicine.WehopeyouwillalsofindtheJournalusefulinyourdailypractice.
Dr lau chu Pak劉柱柏醫生FRCP, MD, FHKAM (Medicine)Chief Editor
Dr lam Tat chung, Paul林達聰醫生FRCP, FHKAM (Medicine), FHKAM (Psychiatry)President
editorial
Pictorial Medical history (1)
Dr lam Tat chung, Paul (林達聰醫生)FRCP, FHKAM (Medicine), FHKAM (Psychiatry)
Specialist in Psychiatry, Private Practice Honorary Clinical Assistant Professor, University of Hong Kong
Traditionallythedoctor’semblemcontainsasnakeandroddesign.Thereissomeconfusionabouttheoriginofthesign.SomeattributedittothebrazensnakecreatedbyMoses.AccordingtotheBook of Numbers,MosesledtheJewsoutofEgyptandwonderedinthedesertfor40yearsbeforeenteringthePromisedLand.Duringthejourney,hisfollowersencountereddrought,plagueandwerebittenbysnakes.TheLordinstructedMosestomakeasnakeofbronze,andtomountitonastick.Thoseinflictedbysnakebitewouldbehealedwhentheylookedatit.
However,Moses,thoughagreatprophet,hadlittleconnectionwithMedicine.ThesnakeofMoseswasnottheoriginofthedoctor’semblem.(NotethatthetopoftherodisintheformofaT.)
editorial office:UBM Medica 27th Floor, OTB Building, 160 Gloucester Road, Wan Chai, Hong KongT +852 2559 5888 F +852 2559 6910
advertising enquiries:Ms Chloe WongT +852 2155 8557e-mail: [email protected]
© 2012 The Society of Physicians of Hong Kong. All rights reserved. No part of this publication may be reproduced in any language, stored in or introduced into a retrieval system, or transmitted, in any form or by any means (electronic, mechanical, photocopying, recording or otherwise), without the written consent of the copyright owner. Permission to reprint must be obtained from the publisher. Advertisements are subject to editorial acceptance and have no influence on editorial content or presentation. The Society of Physicians of Hong Kong does not guarantee, directly or indirectly, the quality or efficacy of any product or service described in the advertisements or other material which is commercial in nature.
the Brazen Snake by french painter Sebastian Bourdon (1653)
Museo del Prado, Madrid, Spain

C
M
Y
CM
MY
CY
CMY
K
PressAd_NAN HA_Print_206x276_OP.pdf 2012/2/6 2:15:09 PM

Journal of The Society of Physicians of Hong Kong 16
Introduction
Respiratory syncytial virus (RSV)isasingle-strandedRNAvirusofthepara-myxoviridaefamily.RSVcauses respiratory tract disease
suchas infectionsof theairways, lungsand middle ear. RSV is transmissibleby sneezing and coughing or physicalcontacts such as kissing, touching orshakinghands.Unlikeothercoldviruses,RSV can survive up to 6-7 hours onobjects and surfaces. Viral sheddingpersists for about 8 days, but can besignificantly prolonged in immunocom-promisedindividuals.RSVinfectiondoesnot convey persistent immunity againstfuture infections, even in the presenceof significant antibody titres; however,highertitresmayattenuatethecourseofthedisease.RSVspreadsveryquicklyincrowdedhouseholdsanddaycarecentresandisthemostcommoncauseof lowerrespiratory tract diseases among infants;virtually all children have been infectedwith RSV by 2 years of age, with nearlyhalf having experienced two infections.The World Health Organization recentlyestimated that RSV accounts for morethan80%ofacutelowerrespiratorytractinfectionsininfantsbelow12monthsold.1
Most people with RSV suffermoderatetoseverecold-likesymptoms,butRSVinfectionscanbemoreseriousin high-risk infants. For example, RSVfrequently leads to hospitalization orserious lung infections in babies bornprematurelyorwithaheartorlungcon-dition. RSV infection provokes an ex-tremelycomplexinflammatoryresponsethat involves the release of multiplecytokines and chemokines from theepithelium and immunocytes, as wellas mast cell degradations that releaseleucotrienes. RSV bronchiolitis may be
associatedwithshort-termorlong-termcomplications that include recurrentwheezing, reactive airway disease, andpulmonary function abnormalities. IntheUSA,itisestimatedthatasmanyas126,000infantsperyear(24.2per1,000)are hospitalized due to acute bronchi-olitis, with 2–5 % requiring mechanicalventilation.2RSVinfectionskillupto400infantsannually–adeathrate10timeshigherthanthatofinfluenza.3
rSV Infections in Infants: Epidemiology and Disease Burden
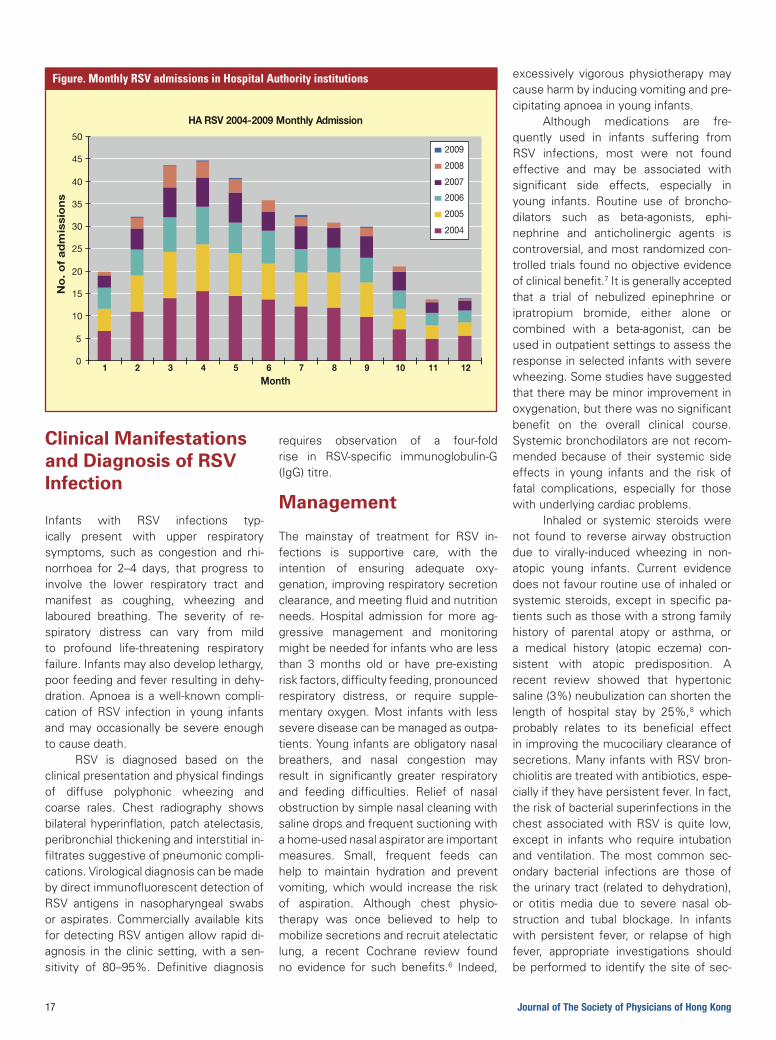
IntheUSAandthroughouttheNorthernHemisphere, annual RSV epidemicsusually begin in November, peak inJanuary or February and end in May.RSV seasonality in Hong Kong is lesspredictable, and the disease remainsactive fornearly10monthsof theyear.A local retrospectivestudyshowed thattheseasonusually starts inApril, peaksin July and August, and wanes in Sep-tember,withmonthly incidencestronglycorrelatingwithtemperatureandrelativehumidity.4 Based on Hospital AuthorityClinicalDischargeInformation,thistrendhasbecomeevenmoreunpredictableinrecent years, with outbreaks occurringeven during the “off peak” season likeNovember to January. (Figure) A localprospective population-based surveyconducted from 2003 to 2006 showedveryhigh ratesofRSVhospitalization ininfants less than 6 months old, with anincidenceof2.3–3.1per1,000.ThemeandurationofhospitalizationassociatedwithRSVinfectionwas4.04days,whichwassubstantiallyhigherthanthatofinfluenzaAandB,adenovirusandpara-influenza.5
Respiratory Syncytial virus Bronchiolitis in young infants – update on management and Prevention
Key words: Respiratory syncytial virus (呼吸道合胞病毒), bronchiolitis (細支氣管炎), management (治理), prevention (預防)
Dr lam cheung cheung, Barbara, JP (藍章翔醫生、太平紳士)
MBBS, MRCP(UK), FRCP(Edin., Lond.), FRCPCH(UK), FHKAM(HK), FHKCPaed
Honorary Consultant, Queen Mary Hospital, Hong Kong Sanatorium & Hospital
Honorary Clinical Associate Professor, Department of Paediatrics and Adolescent Medicine, University of Hong Kong
17 Journal of The Society of Physicians of Hong Kong
clinical Manifestations and Diagnosis of rSV Infection
Infants with RSV infections typ-ically present with upper respiratorysymptoms, such as congestion and rhi-norrhoea for 2–4 days, that progress toinvolve the lower respiratory tract andmanifest as coughing, wheezing andlaboured breathing. The severity of re-spiratory distress can vary from mildto profound life-threatening respiratoryfailure.Infantsmayalsodeveloplethargy,poorfeedingandfeverresultingindehy-dration.Apnoea isawell-knowncompli-cationofRSV infection in young infantsandmayoccasionallybesevereenoughtocausedeath.
RSV is diagnosed based on theclinicalpresentationandphysicalfindingsof diffuse polyphonic wheezing andcoarse rales. Chest radiography showsbilateralhyperinflation,patchatelectasis,peribronchialthickeningandinterstitialin-filtratessuggestiveofpneumoniccompli-cations.VirologicaldiagnosiscanbemadebydirectimmunofluorescentdetectionofRSV antigens in nasopharyngeal swabsor aspirates. Commercially available kitsfordetectingRSVantigenallowrapiddi-agnosis in theclinicsetting,withasen-sitivity of 80–95%. Definitive diagnosis
requires observation of a four-foldrise in RSV-specific immunoglobulin-G(IgG)titre.
Management
The mainstay of treatment for RSV in-fections is supportive care, with theintention of ensuring adequate oxy-genation,improvingrespiratorysecretionclearance,andmeetingfluidandnutritionneeds. Hospital admission for more ag-gressive management and monitoringmightbeneededforinfantswhoarelessthan 3 months old or have pre-existingriskfactors,difficultyfeeding,pronouncedrespiratory distress, or require supple-mentaryoxygen.Most infantswith lessseverediseasecanbemanagedasoutpa-tients.Younginfantsareobligatorynasalbreathers, and nasal congestion mayresult in significantly greater respiratoryand feeding difficulties. Relief of nasalobstructionbysimplenasalcleaningwithsalinedropsandfrequentsuctioningwithahome-usednasalaspiratorareimportantmeasures. Small, frequent feeds canhelp to maintain hydration and preventvomiting,whichwould increase the riskof aspiration. Although chest physio-therapy was once believed to help tomobilizesecretionsandrecruitatelectaticlung, a recent Cochrane review foundno evidence for such benefits.6 Indeed,
excessively vigorous physiotherapy maycauseharmbyinducingvomitingandpre-cipitatingapnoeainyounginfants.
Although medications are fre-quently used in infants suffering fromRSV infections, most were not foundeffective and may be associated withsignificant side effects, especially inyoung infants. Routine use of broncho-dilators such as beta-agonists, ephi-nephrine and anticholinergic agents iscontroversial,andmostrandomizedcon-trolledtrialsfoundnoobjectiveevidenceofclinicalbenefit.7Itisgenerallyacceptedthat a trial of nebulized epinephrine oripratropium bromide, either alone orcombined with a beta-agonist, can beusedinoutpatientsettingstoassesstheresponseinselectedinfantswithseverewheezing.Somestudieshavesuggestedthattheremaybeminorimprovementinoxygenation,buttherewasnosignificantbenefit on the overall clinical course.Systemicbronchodilatorsarenotrecom-mended because of their systemic sideeffects in young infants and the risk offatal complications, especially for thosewithunderlyingcardiacproblems.
Inhaled or systemic steroids werenot found to reverse airway obstructiondue to virally-induced wheezing in non-atopic young infants. Current evidencedoesnotfavourroutineuseofinhaledorsystemicsteroids,except inspecificpa-tientssuchasthosewithastrongfamilyhistory of parental atopy or asthma, ora medical history (atopic eczema) con-sistent with atopic predisposition. Arecent review showed that hypertonicsaline(3%)neubulizationcanshortenthelength of hospital stay by 25%,8 whichprobably relates to its beneficial effectinimprovingthemucociliaryclearanceofsecretions.ManyinfantswithRSVbron-chiolitisaretreatedwithantibiotics,espe-ciallyiftheyhavepersistentfever.Infact,theriskofbacterialsuperinfectionsinthechest associatedwithRSV is quite low,except in infantswho require intubationand ventilation. The most common sec-ondary bacterial infections are those oftheurinarytract(relatedtodehydration),or otitis media due to severe nasal ob-struction and tubal blockage. In infantswith persistent fever, or relapse of highfever, appropriate investigations shouldbeperformedtoidentifythesiteofsec-
HA RSV 2004-2009 Monthly Admission
0
5
10
15
20
25
30
35
40
45
50
1 2 3 4 5 6 7 8 9 10 11 12Month
No
. o
f a
dm
issi
on
s
2009
2008
2007
2006
2005
2004
figure. monthly RSv admissions in hospital authority institutions

Journal of The Society of Physicians of Hong Kong 18
ondary infection; antibiotics should beusedtotreatthesesecondaryinfectionsaccordingly.Ribavirin istheonlyantiviralagent licensed to treat RSV; however,its routine use is limited due to incon-clusive clinical benefits. Moreover, it isexpensive, troublesome to administer,andispotentiallyteratogenictoexposedpersonnel. For these reasons, ribavirinshouldberestrictedto treatingselectedimmunocompromised patients, and isusually combined with anti-RSV anti-bodiestolimitcontinuedviralshedding.9
Immunoprophylaxis
Palivizumab is a humanized monoclonalIgG1antibody produced by recombinantDNA technology. It has advantagesover RSV-IVIg hyperimmune polyclonalglobulinintermsofminimalimmunosup-pressiveeffectandnoriskoftransmittingblood-borne infection. Palivizumab canbe easily administered by intramuscularinjection in an outpatient setting.The American Academy of Pediatrics(AAP) recommends RSV prophylaxiswith monthly intramuscular injectionsof palivizumab (15 mg/kg) during theRSV season for the following high-riskinfants10:1. Infants and children younger than 24
monthsoldwithchronic lungdiseaseof prematurity who are receivingmedical therapy within 6 monthsbeforethenextRSVseasonbegins.
2. Infantsbornbefore32weeksofges-tation,eveniftheydonothavechroniclungdisease.
3. Infantsbornbetween32weeksto34weeks and 6 days of gestation, withat leastoneof the following tworiskfactors:• Theinfantattendschildcare,or• Hasat leastonesiblingoranother
childyoungerthan5yearsoldwhopermanently resides in the samehousehold.
4. Infants lessthan1yearoldwithcon-genitalabnormalitiesoftheairway,orneuromusculardisease.
5. Infantsandchildrenup to24monthsoldwithhaemodynamicallysignificantcongenitalheartdisease.
6. Infants with severe immunocom-promise.
Palivizumab for rSV Prophylaxis for at-risk Infants – local Perspective Despite its clinically proven benefits,palivizumab is not widely used in HongKong due to its prohibitively high cost.ThelackofclearRSVseasonalityinHongKongalsomakesitmorecomplicatedtoadoptrecommendationssimilartothoseof the AAP for local high-risk infants.Due to lackof localepidemiological andpharmacoeconomic data supporting itscost-effectiveness, public hospitals donot offer palivizumab to eligible at-riskinfants. Very few private paediatricianssystematically provide information onRSV immunoprophylaxis to parents ofat-riskinfants.BasedonAAPrecommen-dations, the author has been providingcounselling and information leafletson RSV prevention and prophylaxis toparents of at-risk infants shortly dis-charged from hospital. During the past3 years (2009–2011), 24 eligible infantswere treated with palivizumab immuno-prophylaxis.Allbut twowereextremelyprematurebabiesbornfrom24weeksto32weeksgestation(mean,28.1weeks)who had chronic lung disease, and fivewere oxygen-dependent at hospital dis-charge. One of the other two infantssuffered from congenital heart diseasewith congestive heart failure, and theotherhadararesyndromaldisorder,withoxygen-dependent chronic lung diseaseand severe upper airway obstruction.Most of these infants received onecourseof three tosixdosesatmonthlyintervals during the first 3–6 monthspost discharge from hospital, coincidingwiththepeakRSVseasoninHongKong(mostly March to August). The numberof doses given was titrated based onthe prevalence of RSV and the severityoftheunderlyinglungcondition,inorderto maximize the cost-effectiveness oftreatment. Two infants (a 25-week pre-maturebabyandtheonewithsyndromaldisorder, who both remained oxygen-dependent in the second RSV season)received two courses of five doses ofpalivizumab in two consecutive peakRSVseasons.Noneofthetreatedinfantsrequired hospitalization for respiratorytract infection during the treatmentperiod,andonlyonesufferedfromanRSVinfection; this infant recoveredpromptly
with conservative management. Thissmall series suggests that palivizumabis effective in preventing and reducingthe morbidity of RSV infection in at-riskinfants.
Recently, The Hong Kong Societyof Paediatric Respirology convened apanel of leading Hong Kong paedia-tricians, neonatologists, microbiologistsandrespiratologiststodiscusstheimpactofRSV infectionand itsmanagement inthelocalpaediatricpopulation.Thepanelsuggested that in the absence of localepidemiological and pharmacoeconomicdataandgiven limitedexperience intheuse of palivizumab locally, recommen-dationsonimmunoprophylaxisshouldbelimited to the highest-risk individuals toensureitscost-effectiveness.Whilegov-ernmentfundingisnotcurrentlyavailabletoprovidesupportforitsuse,parentsofat-risk infantsshouldbegivenadequateinformation so that they are in a betterpositiontobalancethebenefitandafford-ability. Local recommendations shouldhelppaediatricianstoidentifypatientsatrisk, and insuchcases theyareobligedto inform the parents of the option ofimmunoprophylaxis. It is important forphysicians to endeavour to maximizethetreatmentbenefitsaccordingtotheirpatients’abilitytopay.
references1. Shay DK, Holman RC, Newman RD, Liu LL, Stout JW, Anderson LJ. Bron-
chiolitis-associated hospitalizations among US children, 1980–1996. JAMA 1999;282:1440-1446.
2. Leader S, Kohlhase K. Respiratory syncytial virus-coded pediatric hospi-talizations, 1997 to 1999. Pediatr Infect Dis J 2002;21:629-632.
3. Thompson WW, Shay DK, Weintraub E, et al. Mortality associated with influenza and respiratory syncytial virus in the United States. JAMA 2003;289:179-186.
4. Chan PK, Sung RY, Fung KS, et al. Epidemiology of respiratory syncytial virus infection among paediatric patients in Hong Kong: Seasonality and disease impact. Epidemiol Infect 1999;123:257-262.
5. Chiu SS, Chan K-H, Chen H, et al. Virologically confirmed population-based burden of hospitalization caused by respiratory syncytial virus, adenovirus, and parainfluenza viruses in children in Hong Kong. Pediatr Infect Dis J 2010;29:1088-1092.
6. Perrotta C, Ortiz Z, Roque M. Chest physiotherapy for acute bronchiolitis in paediatric patients between 0 and 24 months old. Cochrane Database Syst Rev 2007;(1):CD004873.
7. Gadomski AM, Bhasale AL. Bronchodilators for bronchiolitis. Cochrane Database Syst Rev 2006;(3): CD001266.
8. Zhang L, Mendoza-Sassi RA, Wainwright C, Klassen TP. Nebulized hypertonic saline solution for acute bronchiolitis in infants. Cochrane Database Syst Rev 2008;(4):CD006458.
9. Wright M, Piedimonte G. Respiratory syncytial virus prevention and therapy: Past, present, and future. Pediatric Pulmonology 2011;46:324-347.
10. American Academy of Pediatrics. Respiratory syncytial virus. In: Pickering LK, Baker CJ, Kimberlin DW, Long SS, ed. Red Book: 2009 Report of the Committee on Infectious Diseases. 28th edition. Elk Grove Village, IL, USA: American Academy of Pediatrics; 2009:560-569.

Journal of The Society of Physicians of Hong Kong 20
Introduction
undertreatedrheumatoidarthritis(RA) can cause functional im-pairment, deformity and earlydeath. However, through early
and aggressive intervention, it is nowpossible to halt and prevent the accu-mulation of permanent joint damage.Greater understanding of the patho-genesis of RA has resulted in recentadvances in its treatment. This articlereviews experience in the managementofRAgainedwithtumournecrosisfactor(TNF)inhibitorsandalsodiscussesnewerbiologicalagentsandothertargetedsmallmoleculesthatactonsignallingpathways.AllofthesemodalitiesareexpandingourknowledgeofRAandprovidingmoreef-fectiveandefficienttreatmentoptions.
First-generation Biologics: TNF Inhibitors
Efficacy in raThedevelopmentofbiologicagentsthatselectively block cytokines has beena major advance in the treatment ofRA. TNF is a proinflammatory cytokineabundantinpatientswithRA.1Currently,three TNF-targeting agents dominatethebiologicalmanagementofRA:Etan-ercept,adimericfusionprotein,consistsoftheextracellularportionofhumanp75TNF receptor linked to the Fc region ofhuman immunoglobulin-G1. Infliximabis a chimeric human/mouse monoclonalantibodycomprisingthehumanconstantandmurinevariableregions.Adalimumabisa recombinanthumanmonoclonalan-tibodyspecifictoTNF.Allthreeanti-TNFtherapies have well-demonstrated ef-ficacyinRA.
AnyoftheseTNFinhibitorsmaybegiven concomitantly with methotrexate(MTX) therapy; randomized controlled
trials showed that combinations withMTX are significantly more effectivethanMTXalone in achievingdisease re-mission, reducing signs and symptomsof RA, slowing or stopping radiographicprogression of disease and improvingphysicalfunction.AlthoughTNFinhibitorsare currently the recommendedfirst-linebiological agents for patients with RA,there are several unanswered questionsabouthowtoderivethemaximumbenefitfrom such agents. Convincing data in-dicate that using biologics early in thecourseofRAcanbehighlyefficaciousandmay induce clinical remission.2-6 Familyphysicians and other healthcare profes-sionalsmustbeeducatedabouttheearlysymptoms of RA, with an emphasis onthe importance of early referral to rheu-matologistsfordiagnosisandtreatment.
Potential for Effectiveness of TNF antagonists in Early raThe PREMIER study compared the ef-ficacyofearlyinterventionwithcombinedadalimumabandMTXvseitheragentasmonotherapy in patients with early, ag-gressive RA.3 The primary endpoints inthis2-year,double-blind,controlledstudywerethepercentageofpatientsinwhoman American College of Rheumatology50% (ACR50) response was achievedandthemeanchangefrombaselineinthemodifiedTotalSharpScore (TSS),whichassesses bone erosion and joint spacenarrowing on radiographs. Adalimumaband MTX combination therapy was su-perior to monotherapy for all outcomesmeasured. At 1 year, patients treatedwith combination therapy had a meanincrease in TSS of 1.3 units comparedwith 3.0 units in those receiving onlyadalimumab and 5.7 units in the MTXmonotherapy arm. At 2 years, patientsreceivingcombinationtherapycontinuedto have significantly less radiographicprogression(meanchange1.9TSSunits)comparedwiththosetreatedwitheitheradalimumab(5.5units)orMTX(10.4units)
Rheumatoid arthritis: advances in therapeutics
Key words: Biologics (生物製劑), rheumatoid arthritis (類風濕關節炎), treatment (治療)
Dr cheung Tak cheong (張德昌醫生)
MBBS, MRCP, PDipID, FHKCP, FHKAM, FRCPE
Specialist in Rheumatology
Private Practice

21 Journal of The Society of Physicians of Hong Kong
monotherapy. Although ACR responseswere comparable in the two mono-therapyarms,therewassignificantlylessprogressionintheadalimumabarmthantheMTXarmat6months(2.1vs3.5),1year(3.0vs5.7)and2years(5.5vs10.4).These results suggest that combinationtherapyinearlyRAisbeneficial.
Furthermore, drug-free remissionmaybea realisticgoal insomepatientswith early RA. In the BeSt study, 19%ofpatientswho received infliximabplusMTX inaDiseaseActivityStatus (DAS)-steered, tightly controlled manner werein drug-free remission at 5 years, for amean duration of 22 months. Infliximabwas successfully discontinued in 58%of patients, while 18% were still re-ceiving combination therapy. Moreover,compared with other treatmentstrategies, initial temporary treatmentwith infliximabplusMTXresultedinsig-nificantly better functional ability over 5years.7 This study raises the possibilitythat if aggressive treatment to induceremission is instituted very early in thecourse of RA, more conservative man-agementstrategiesmaybesufficient tomaintainthatremission.
SafetyBacterial infections,includingsepsisandpneumonia, invasive fungal infections,and other opportunistic infections haveallbeenassociatedwiththeuseofTNFinhibitors. Reactivation of latent tuber-culosis following treatment has led totheintroductionofpreinitiationscreeningprocedures, which have successfullyreducedthenumberofreportedcases.8,9Theriskofreactivatinglatenttuberculosisdepends on the incidence of latent in-fectionandisassociatedwithallTNFin-hibitors.Physiciansshouldremainalerttothedevelopmentofsymptomsrelatedtotuberculosisorotherinfections.Patientswith congestive heart failure should becloselymonitored.Other rarely reportedconditionsthatarepossiblyrelatedtouse
of TNF inhibitors include demyelinatingdiseases, seizures, aplastic anaemia,pancytopaenia, and drug-induced lupus.Physiciansshouldremainvigilantforthedevelopmentofsuchconditions.
advances in Biological Therapy
The pathogenesis of RA is a highlycomplex interplay of numerous inflam-matory pathways.10 Many biologicalagentsthatinterveneinvariouspathwayshavepotential,orarebeingdeveloped,totreatRA.
rituximabRituximab is a chimeric anti-CD20monoclonal antibody that was thefirst B-cell agent approved for treatingRA.11 Rituximab inhibits progression ofstructuraldamageinRAover2years,andlong-term treatment continues to inhibitjoint damage.12,13 A prospective cohortstudy found that patients who wereswitchedtorituximabduetoTNFinhibitorineffectiveness had significantly betterdiseaseimprovementthanthosetreatedwith an alternative TNF inhibitor.14 Pro-gressivemultifocal leukoencephalopathyorhepatitisBreactivationbothoccurveryrarelyduringrituximabtreatment.
abataceptAbataceptisaT-cellco-stimulationmod-ulator that is believed to prevent theactivation of T lymphocytes, includingnaïve T cells. Because abatacept wasthe first therapy targeting the inhibitionofco-stimulatorysignalstopreventT-cellactivation, its use in early disease andinbiologic-naïvepatientswith activeRAhas generated particular interest andresearch.15,16 Abatacept has also beenshown toprovideclinicalbenefits inpa-tients with RA who failed earlier TNFinhibitor treatment, regardless of whichTNFinhibitorswereusedorthereasonsfor treatment failure.17 This findingsuggests that switching to abataceptmaybeausefuloptionforpatientswhofailTNFinhibitortreatment.
TocilizumabTocilizumab is a humanized anti-
interleukin-6 (IL-6) receptor monoclonalantibodythatinhibitssignalsthroughbothmembrane and soluble IL-6 receptors.Datafromfourrandomized,double-blind,controlled, phase III trials of tocilizumabindifferentpopulationssupportitsuseinRA, includingpatientsrefractorytoMTXorotherdisease-modifyinganti-rheumaticdrugs (DMARDs) (OPTION, TOWARD,LITHE),18-20 and MTX-naïve patients(AMBITION).21 Compared with placeboin these trials, tocilizumab significantlyimproved ACR 20% response (ACR20),physical function, fatigue, and physicalandmentalhealthscoresover24weeks.Inthe3-yearextensionoftheSAMURAIstudy, radiographic progression wasstronglysuppressedinpatientswithearlyRAwhoweretreatedwithtocilizumab.22Furthermore, radiographic progressionwas more effectively suppressed in pa-tients who received initial treatmentwith tocilizumab compared with con-ventional DMARDs. Early introductionof tocilizumab treatment may thereforebe more effective in preventing jointdamage. Tocilizumab has a well-char-acterized safety profile, with infectionsbeingthemostcommonadverseevent.Physicians should also check for de-creasedneutrophilcountsandincreasedlipidor liverenzymelevels,andmanagetheseappropriately.
Kinase Targets in DevelopmentKinases such as Janus kinase (JAK)are intracellular molecules that play apivotal role in signal transduction of in-terleukins. Tofacitinib is a pan-JAK in-hibitor that inhibits JAK1 and JAK3 toa greater extent than JAK2, and is ef-fective in patients who respond inad-equately to DMARDs. In a phase IIItrial, patients treated with tofacitinib10 mg twice-daily had a significantlybetter ACR20 response than placebo(65.7%vs26.7%).23
Alsoof interest aredata indicatingthatspleentyrosinekinasecouldserveasanewandpromising target for immuneintervention in rheumatic diseases. In aphase II study of RA patients refractorytoMTX,moreofthosetreatedwithfosta-matinib,whichisapotentspleentyrosinekinaseinhibitor,thanintheplacebogroupattainedanACR20responseatweek12(67%vs35%).24
“Drug-free remission may be a realistic goal
in some patients with early RA”

Journal of The Society of Physicians of Hong Kong 22
conclusion
Biological therapies have revolutionizedthe treatment of RA and allowed usto further curb its progression. Devel-opment of the first biologics, TNF in-hibitors,expandedourknowledgeofthepathogenesisofinflammatoryconditions.A largebodyofsafetyandefficacydataonTNFinhibitorshasaccumulatedduringmorethanadecadethattheyhavebeenavailable to rheumatologists. More re-cently, biologics with distinct mech-anisms of action (rituximab, abatacept,tocilizumab) have been approved. Nu-merous other targets within the inflam-matorycascadecontinuetobeidentified,and biologic and nonbiologic agents tomodulate/inhibittheassociatedpathwayshave already been developed, or are inthepipeline.
references1. Feldmann M, Brennan FM, Maini RN. Rheumatoid arthritis. Cell
1996;85:307-310.2. Emery P, Breedveld FC, Hall S. Comparison of methotrexate mono-
therapy with a combination of methotrexate and etanercept in active, early, moderate to severe rheumatoid arthritis (COMET): A randomised, double-blind, parallel treatment trial. Lancet 2008;372:375-382.
3. Breedveld FC, Weisman MH, Kavanaugh AF. The PREMIER study: A multi-center, randomized, double-blind clinical trial of combination therapy with adalimumab plus methotrexate versus methotrexate alone or adalimumab alone in patients with early aggressive rheumatoid arthritis who had not had previous methotrexate treatment. Arthritis Rheum 2006;54:26-37.
4. Tak PP, Rigby WF, Rubbert-Roth A. Inhibition of joint damage and improved clinical outcomes with rituximab plus methotrexate in early active rheu-matoid arthritis: The IMAGE trial. Ann Rheum Dis 2011;70:39-46.
5. van der Heijde D, Klareskog L, Rodriguez-Valverde V; TEMPO Study Investigators. Comparison of etanercept and methotrexate, alone and combined, in the treatment of rheumatoid arthritis: Two-year clinical and radiographic results from the TEMPO study, a double-blind, randomized trial. Arthritis Rheum 2006;54:1063-1074.
6. van Vollenhoven RF, Ernestam S, Geborek P. Addition of infliximab compared with addition of sulfasalazine and hydroxychloroquine to methotrexate in patients with early rheumatoid arthritis (Swefot trial): 1-year results of a randomized trial. Lancet 2009;374:459-466.
7. Klarenbeek NB, Guler-Yuksel M, van der Kooij SM. Clinical outcomes of four different treatment strategies in patients with recent-onset rheu-matoid arthritis: 5-years results of the BeSt study [abstract]. Ann Rheum Dis 2008;67(suppl II):187.
8. Hochberg MC, Lebwohl MG, Plevy SE. The benefit/risk profile of TNF-blocking agents: Findings of a consensus panel. Semin Arthritis Rheum 2005;34:819-836.
9. Schiff MH, Burmester GR, Kent JD. Safety analysis of adalimumab (HUMIRA*) in global clinical trials and US postmarketing surveillance of patients with rheumatoid arthritis. Ann Rheum Dis 2006;65:889-894
10. Voulgari PV. Emerging drugs for rheumatoid arthritis. Expert Opin Emerging Drugs 2008;13:175-196.
11. Cohen SB, Emery P, Greenwald MW; REFLEX Trial Group. Rituximab for rheumatoid arthritis refractory to anti-tumor necrosis factor therapy: Results of a multicenter, randomized, double-blind, placebo-controlled, phase III trial evaluating primary efficacy and safety at twenty-four weeks. Arthritis Rheum 2006;54:2793-2806.
12. Keystone E, Emery P, Peterfy CG. Rituximab inhibits structural joint damage in patients with rheumatoid arthritis with an inadequate response to tumour necrosis factor inhibitor therapies. Ann Rheum Dis 2009;68:216-221
13. Finckh A, Ciurea A, Brulhart L, et al. Which subgroup of patients with rheumatoid arthritis benefits from switching to rituximab versus alter-
native anti-tumour necrosis factor (TNF) agents after previous failure of an anti-TNF agent? Ann Rheum Dis 2010;69:387-393.
14. Schiff M, Bessette L. Evaluation of abatacept in biologic-naïve patients with active rheumatoid arthritis [includes some 2-year data from ATTEST trial]. Clin Rheumatol 2010;29:583-591.
15. Genant HK, Peterfy CG, Westhovens R. Abatacept inhibits progression of structural damage in rheumatoid arthritis: Results from the long-term extension of the AIM trial. Ann Rheum Dis 2008;67:1084-1089.
16. Genovese MC, Schiff M, Luggen M. Efficacy and safety of the selective co-stimulation modulator abatacept following 2 years of treatment in patients with rheumatoid arthritis and an inadequate response to anti-tumour necrosis factor therapy. Ann Rheum Dis 2008;67:547-554.
17. Schiff M, Pritchard C, Huffstutter JE. The 6-month safety and efficacy of abatacept in patients with rheumatoid arthritis who underwent a washout after anti-tumour necrosis factor therapy or were directly switched to abatacept: The ARRIVE trial. Ann Rheum Dis 2009;68:1708-1714.
18. Smolen JS, Beaulieu A, Rubbert-Roth A; OPTION Investigators. Effect of interleukin-6 receptor inhibition with tocilizumab in patients with rheumatoid arthritis (OPTION study): A double-blind, placebo-controlled, randomised trial. Lancet 2008;371:987-997.
19. Kremer JL, Blanco R, Brzosko M. Tocilizumab inhibits structural joint damage in rheumatoid arthritis patients with inadequate responses to methotrexate at 1 year: The LITHE study. Arthritis Rheum 2011;63:609-621.
20. Genovese MC, McKay JD, Nasonov EL. Interleukin-6 receptor inhibition with tocilizumab reduces disease activity in rheumatoid arthritis in rheumatoid arthritis with inadequate response to disease-modifying antirheumatic drugs: The tocilizumab in combination with traditional disease-modifying antirheumatic drug therapy study. Arthritis Rheum 2008;58:2968-2980.
21. Jones G. The AMBITION trial: Tocilizumab monotherapy for rheumatoid arthritis. Expert Rev Clin Immunol 2010;6:189-195.
22. Nishimoto N, Hashimoto J, Miyasak N. Three-year extension of the SAMURAI study confirms tocilizumab to prevent joint destruction in patients with rheumatoid arthritis. Ann Rheum Dis 2008;67(suppl 2):335.
23. Kremer J, Li ZG, Hall S. Tofacitinib and oral JAK inhibitor, in combi-nation with traditional DMARDs: Phase 3 study in patients with active rheumatoid arthritis with inadequate response to DMARDs [abstract]. Presented at EULAR annual congress; May 25-28 2011, London, England. Abstract LB0005.
24. Weinblatt ME, Kavanaugh A, Genovese MC. An oral spleen tyrosine kinase (Syk) inhibitor for rheumatoid arthritis. N Engl J Med. 2010;363:1303-1312.
the challenge and essence of the management of Psoriasis
Dr hui Shiu Kee (許紹基醫生)
LMCHK, MRCP (UK), FHKCP, FHKAM (Medicine)
Specialist in Dermatology and Venereology, Private Practice
Psoriasis is a cutaneous andsystemic chronic inflammatorydisorderthatresultsfrombothin-ternal genetic factors (polygenic
abnormalities) and external environ-mental factors (trauma, infection andmedications). It is relatively common inWesterncountries,withaprevalenceof2%, while the prevalence ranges from0.3–1.1%inAsianandAfricancountries.1
Although the prevalence of pso-riasis is not as high as that of atopic
eczema, psoriasis has significantnegativeimpactontheeverydaylifeofapatient.Moreover,upto40%ofpatientswithpsoriasisregardthetreatmenttheyreceived as unsatisfactory. The man-agementofpsoriasisremainsachallengein routine clinical practice of generalphysicians and dermatologists alike.This article will discuss the essence ofmanagingthischallengingdiseaseunderfour headings: I) General management;II)specifictherapy;III)thechallengesforpatients;andIV)thechallengesfacedbyphysicians.Themanagementofspecifictypes of psoriasis such as palmoplantarpustulosis, pustular psoriasis and eryth-rodermic psoriasis are not discussed inthisarticle.
Key words: Psoriasis (牛皮癬), management (治理), biologics (生物製劑)

23 Journal of The Society of Physicians of Hong Kong
General Management of Psoriasis
While taking detailed medical history,some points are important and worthmentioningtothepatients.
The positive side of the nature ofthis illness should be stressed. It is im-portant topointout thatpsoriasis isnotcontagious,andthefamilyandfriendswillnotbe“infected”.It isalsoconstructiveto point out that up to 40% of patientsmay enjoy a period of remission thatmaylastforupto54years.2Duringthatperiod,patientswillbefreeofanysignsandsymptomsofpsoriasisevenwithoutany treatment. Finally, the fact that anincreasing number of effective agentssuch as biologics will become availableproposes a brighter future for psoriaticpatients.3 The confidence gained by pa-tientswilllargelyimprovetheirtreatmentcompliance, which in turn will improvetheeffectivenessoftreatment.
A realistic picture of the levelof control with different treatmentmeasures, and their potential long-termriskandimplications,especiallythelong-term side effects and financial expen-diture, should all be communicated topatientsfortheirthoroughconsideration.
Patients’ own perception of theillnessandtheirexpectationoftreatmentoutcomeshouldbeunderstoodbytheat-tendingphysicianbeforeaskingforcom-mitment to a long-term treatment plan.This approach will largely eliminate theunnecessaryiatrogenicdamagefromthe
physician and unrealistic expectationsfromthepatients.
General advice on lifestyle adjustmentSince psychological stress is a well-known predisposing factor of psoriasis,4simple general measures that enhancethesenseofwell-beingmighthelpenor-mouslyandshouldbeencouraged.Theseincludeapplyingmoisturizersproperly,ad-equaterest,abstinencefromsmokinganddrinking,5takinggoodwoundcareandre-frainingfromexcessivescratchingofskin,gradual arrangement for sun exposure,and participating in self-help supportgroupsandhealthtalksonpsoriasis.
Eliminating Infection Upper respiratory tract infections andurinary tract infections are consideredas predisposing factors for psoriasis.Patients should be encouraged to seekearlymedicaladviceiftheyhavewarningsymptoms.
MedicationsMedications known to exacerbate pso-riasis,suchaslithiumandbeta-blockers,shouldbediscontinued.6
Specific Therapy of Psoriasis
The selection of specific therapies forpatients with psoriasis should be basedon all the aforementioned factors, such
as patients’ general physical condition,social economic status, expectation oftreatment outcome, perception of theimpact of psoriasis, current disease ac-tivity and clinical variants of psoriasis.Four major therapeutic approaches canthen be considered, namely topicaltherapy, phototherapy, systemic therapyandbiologictherapy.
Theprosandconsofthesefourap-proachesaresummarizedintheTable.
Medications and treatment mo-dalitiescommonlyusedinHongKongarelistedbelow:
Topical TherapyVitamin D3 analogues (calcipotriol[Daivonex],calcitriol[Silkis])areeffectiveinlocalized psoriasis, but local irritation mayoccuronthefaceandintertriginousarea.
Topical corticosteroids are themainstayoftreatmentforsmalllesionsofpsoriasis(<5%bodysurfacearea).Tachy-phylaxiscanbereducedifthedurationofcontinuoustreatmentisrestrictedtolessthan2weeksandswitchedtoweekendapplicationonly.
Topical calcineurins (tacrolimus[Protopic], pimecrolimus [Elidel]) areusefulfortreatmentoffacialandflexuralpsoriasis,sincetheseareasarepronetocorticosteroid side effects and irritationfromvitaminDanalogues.
Coaltariseffectivebutmessy.Sal-icylic acid is keratolytic and can removescaly plaques. It inactivates calcipotrioland blocks UVB, and should thereforebeavoidedinthepresenceoftheabovetherapies. Tararotene and anthralin have
table. Pros and cons of therapeutic approaches for psoriasisPros cons
topical therapy • Convenient, economic• Relatively free from systemic side effects• Predictable effect on patients with less than 5% body surface area
involvement• Self-administered
• Have no effect on reducing the occurrence of new lesions• Long-term usage should be under medical supervision; otherwise there
will be problems of tolerance and/or tachyphylaxis
Phototherapy • Relatively safe and free of systemic side effects• Good for widespread disease• May have prompt improvement after a few treatment sessions
• Time-consuming • Facility-dependent• Expenses may be a concern• Not suitable for physically compromised patients
Systemic therapy • Convenient• Suitable for widespread disease• Some with relatively prompt improvement
• Systemic side effects common after long-term usage• Regular laboratory monitoring needed in some patients• Many patients may have pre-existing medical conditions that are
relative or absolute contraindications
Biologic therapy • Good response• Relatively free of systemic side effects• Some are relatively convenient
• Very expensive• Relative short history of clinical usage, awaiting long-term established
safety profile• Some have potential risk of exacerbating infection

Journal of The Society of Physicians of Hong Kong 24
problems of skin irritation and are lesscommonlyused.
Phototherapy Narrow band ultraviolet B (nUVB) andphotochemotherapy with psoralen andultraviolet A (PUVA) are used relativelycommonly in Hong Kong. Targeted pho-totherapies with Excimer (308 nm) laseror lamp are more effective for localizedlesions,butonlyavailableinafewcentres.
Systemic TherapyMethotrexate, cyclosporineandacitretinarethethreemajorsystemicagentsusedinthemanagementofpsoriasis.
Methotrexateiseffective,economicandhasrelativelypromptdiseasecontrol.However, hepatotoxicity and marrowsuppression with idiosyncratic reactionareitsmajordrawbacks.
Cyclosporine is also effective andhaspromptdiseasecontrol.However, itisrelativelyexpensive,andnephrotoxicityand hypertension are its common sideeffects,limitingitsusetolessthan1to2years.Acitretinisrelativelysafeintermsoforgantoxicity,withreversiblemild-to-moderate alterations in liver enzymesand blood lipids. It takes approximately2 weeks to have noticeable effect ondiseaseprogress.
Biologic TherapyCurrentlyavailablebiologicsfortreatmentof psoriasis include the tumour ne-crosis factor (TNF) inhibitors infliximab(Remicade), etanercept (Enbrel) andadalimumab(Humira),theinterleukin-12/interleukin-23 inhibitor ustekinumab(Stelara),andtheT-cellinhibitoralefacept(Amevive). All of these new agents areexpensivebuteffectiveforthetreatmentof psoriasis. Approximately 60–70% ofpatients using these agents will have75%improvementofpsoriasis in2to3months.Themajorconcernwiththisap-proachmightbetreatmentcostandtheirunknownlong-termsafetyprofile.7-11
challenge for Patients With Psoriasis
Misconception of the PublicHistorically, patients with psoriasis had
suffered from unjustified discriminationfor centuries due to the visible lesionsofpsoriaticplaques.EventhoughRobertWilanandHebrarecognizedpsoriasisasadistinctentity from leprosy in thefirsthalf of the 19th century, public under-standing of the noncontagious natureof this illnessseemsfar fromadequate,making it a heavy psychological burdenforpsoriaticpatients.Propereducationofthepublicwillease thisburden,makinglifeeasierforpsoriaticpatients.
Unrealistic ExpectationsPatients may have unrealistic expec-tations of cure towards some newapproachesandnewlyencounteredphy-sicians. However, after a certain periodofremissionandrecurrence,confidenceand compliance deteriorate due to lesssatisfactory psoriasis control, and pa-tients become over-pessimistic towardsanyotherpotentiallyeffectivetherapeuticapproaches, resulting in further dete-rioration of psoriasis, even into erythro-dermicstage.
challenge for Physicians
Diagnostic ProblemsIt is not uncommon for an experienceddermatologist to make a definite di-agnosisofpsoriasisafteryearsoftreatingthe same patient labeled with chroniceczema. Vigilantly looking for well-circumscribedcutaneouslesions,scalinglesionsunderhair,pittingnailsandfamilyhistoryofunknowndermatosesmayhelp
reveal the real picture. Adequate con-sultation time with suitable sampling ofskinbiopsy indifficultcases isvaluable,since topicalandsystemicsteroidsmaydramatically alter the clinical as well ashistologicalpresentationoftheillness.
Patients’ compliancePatients’ compliance is the key togooddiseasecontrol.Patients’trustbuildsonrobustcommunicationwiththeattendingphysician. The more knowledgeablethe patients are on psoriasis, the morewillingwilltheybetoactaccordingtothetreatment plan, which should be tailor-madefortheirlong-termbettermentandshort-termneeds.
The expected time to have no-ticeable improvement of psoriasis fromdifferent therapies should be told be-forehand.Patientsshouldbeencouragedtoreportanyunwantedorunexpectedex-periencewithtreatmentandtheyshouldbepromptlyexplainedand/orresolved.
While patients accept the no-curereality of psoriasis, sensible andpragmatic approaches in controlling thesymptoms and signs of psoriasis wouldbeappealing.
references:1. Christophers E. Psoriasis-epidemiology and clinical spectrum. Clin Exp
Dermatol 2001;26:314-320.2. Farber EM, Mall ML. The natural history of 5600 patients. Dermatologica
1974;148:1-18.3. Menter A, Gottlieb A, Feldman SR, et al. Guidelines of care for the
management of psoriasis and psoriatic arthritis: Section 1. Overview of psoriasis and guidelines of care for the treatment of psoriasis with biologics. J Am Acad Dermatol 2008;58:826-850.
4. Gupta MA, Gupta AK, Kirkby S, et al. A psychocutaneous profile of psoriasis patients who are stress reactors. A study of 127 patients. Gen Hosp Psychiatry 1989;11:166-173.
5. Higgins E. Alcohol, smoking and psoriasis. Clin Exp Dermatol 2000;25:107-110.
6. Tsankov n angelova I, Kazandjieva R. Drug-induced psoriasis. Recog-nition and management. Am J Clin Dermatol 2000;1:159-65.
7. Menter A, Feldman SR, Weinstein GD, et al. A randomized comparison of continuous vs. intermittent infliximab maintenance regimens over 1 year in the treatment of moderate-to-severe plaque psoriasis. J Am Acad Dermatol 2007;56:31.e1-e15.
8. Paller AS, Siegfried EC, Langley RG, et al. Etanercept treatment for children and adolescents with plaque psoriasis. N Engl J Med 2008;358:241-251.
9. Menter A, Tyring SK, Gordon K, et al. Adalimumab therapy for moderate to severe psoriasis: A randomized, controlled phase III trial. Am Acad Dermatol 2008;58:106-115.
10. Papp KA, Langley RG, Lebwohl M, et al. Efficacy and safety of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with psoriasis: 52-week results from a randomised, double-blind, placebo-controlled trial (PHOENIX 2). Lancet 2008;371:1675-1684.
11. Lebwohl M, Christophers E, Langley R, et al. An international, ran-domized, double-blind, placebo-controlled phase 3 trial of intramuscular alefacept in patients with chronic plaque psoriasis. Arch Dermatol 2003;139:719-727.
“Look for well- circumscribed
cutaneous lesions, scaling lesions under hair, pitting nails and
family history of unknown dermatoses”

25 Journal of The Society of Physicians of Hong Kong
Sarcomas are a heterogeneousgroup of mesenchymal neo-plasmsthatcanbegroupedintotwo general categories: soft
tissuesarcomas(STS)andbonesarcoma.Bonesarcomas(osteogenicsarcomaandEwing’ssarcoma)areconsideredchemo-therapy sensitive, but STS are generallymore resistant to chemotherapy.1 ThisreviewsummarizestheemergingroleofsystemicchemotherapyinSTS.
At diagnosis, fewer than 50% ofpatientswithSTSwillbeprescribedcu-rativetreatmentwithsurgeryorradiationtherapy. However, 30–60% of patientswith clinically localized disease at pre-sentation will eventually develop localrecurrence or metastases, mostly inthe lungs.MetastaticSTS isusuallynotamenabletocurativetreatment,andpal-liationwithsystemictherapyremainsanurgentclinicalproblem.
chemotherapy in Metastatic STS
Appropriate use of chemotherapy maybeofsomebenefitintreatingmetastaticSTS. Experience shows that certain pa-tients tend to respondbetter tochemo-therapy,including:thosewhoareyoung;have good performance status; withoutliver involvement; and long disease-free interval between primary surgeryand relapse. Single-agent doxorubicin,ifosfamide or dacarbazine, or anthra-cycline-basedcombinationregimens(eg,doxorubicinorepirubicinwithifosfamideand/or dacarbazine) produce objectiveresponses in 13–33% of patients, butdo not usually improve overall survival.More recently, gemcitabine and taxanecombinationshavedemonstratedactivityin STS, especially in leiomyosarcoma.2
Role of chemotherapy in Soft tissue Sarcoma
Key words: chemotherapy (化療), soft tissue sarcoma (軟組織肉瘤), trabectedin
Dr loh Kai Tsu, Kevin (陸凱祖醫生)
FACP, FRCPC
Specialist in Medical Oncology, Private Practice
table. chemotherapy agents and regimens with activity in soft tissue sarcoma
Sarcoma type chemotherapy agents and regimens
General • Doxorubicin monotherapy• Doxorubicin, ifosfamide and mesna (AIM)• Doxorubicin and dacarbazine (AD)• Mesna, doxorubicin, ifosfamide and decarbazine (MAID)• Epirubicin, ifosfamide and mesna• Gemcitabine and docetaxel• Gemcitabine and vinorelbine
Leiomyosarcoma • Doxorubicin, gemcitabine, dacarbazine• Gemcitabine and docetaxel
Myxoid liposarcoma • Anthracyclines• Trabectedin• Ifosfamide
Synovial sarcoma • Anthracyclines• Trabectedin• Ifosfamide
Poorly-differentiated liposarcoma • Ifosfamide
Angiosarcoma • Paclitaxel or docetaxel• Liposomal dxoxorubicin• Sorafenib
Desmoid tumours (fibromatosis) • Doxorubicin-based regimens• Hormonal therapy (eg, tamoxifen ± sulindac)• Methotrexate and vinblastine
Adapted from reference 1.

Journal of The Society of Physicians of Hong Kong 26
ThE SocIETY oF PhYSIcIaNS oF hoNG KoNGCME FOR MEDICAL DOCTORS
SUNDAY SYMPOSIUM • MARCH 11, 2012
11:00 am – 12:00 pm Effective & efficient management of osteoporosis – Practical tips for physiciansDr. Cheung Tak Cheong (張德昌醫生) FRCP, Specialist in Rheumatology
12:00 pm – 1:00 pm Treating hba1c to target in T2DM: Putting trial results into perspective Dr. Yeung Chun Yip (楊俊業醫生)Specialist in Endocrinology, Diabetes and Metabolism
1:00 pm – 2:00 pm ※※※※※ lunch ※※※※※one snake or two snakes, the mystery of the medical insignia (1.30-2.00pm)Dr. Lam Tat Chung Paul 林達聰醫生FRCP, FHKAM (Medicine), FHKAM(Psychiatry), President, The Society of Physicians of Hong Kong
2:00 pm – 3:00 pm advances in the management of coPDDr. Ko Wai San, Fanny (古惠珊醫生)FRCP, MD, Specialist in Respiratory Medicine
3:00 pm – 4:00 pm Management update on allergic rhinitis & common sinonasal problems Dr. Wong Hon Wai, Simon (黃漢威醫生)FRCS, Specialist in Otolaryngology
Q&a
Place: The Langham Hotel, 8 Peking Road, TST, Kowloon
Enquiry: Tel 2526 2626 (no telephone registration) CME points under application Non-members please pay $50 on admission (Do not mail your cheque).
Fee: Free for Members and Associate Members. Merck Sharp & Dohme (Asia) Ltd.
Sponsors: Nycomed (Hong Kong) Limited – A Takeda Company
First come first serve basis. Pre-registration is required. No confirmation will be sent for registration. Unsuccessful applicants will be notified.
registration form: Fax to 2856 2728 attention: Ms. Sally Wong of Nycomed-a Takeda company Web registration and further details: www.SoPhYSIcIaNShK.org
I wish to attend Sunday Symposium on March 11, 2012 ($50)Name of Doctor (Surname first): Tel:
Free for Members and associate Members on presentation of valid membership cards of ThE SocIETY oF PhYSIcIaNS oF hoNG KoNG
CertainhistologicsubtypessuchasGIST,alveolar soft part sarcoma, clear cellsarcoma,well-differentiated liposarcomaareintrinsicallyresistanttochemotherapy.Incontrast,leiomyosarcoma,myxoidandpoorly-differentiated liposarcoma, angio-sarcomaandsynovialsarcomaaremoresensitive to chemotherapy. The Tableliststhechoiceofchemotherapyagentsforvarioussarcomahistologies.1
chemotherapy in the adjuvant Setting
Patientswithhighergrade,deepseatedand larger (>5 cm) STS are more prone(>50%) to local recurrence and me-tastases, despite surgery and local ra-diation therapy. The role of adjuvant
systemic chemotherapy in STS is un-proven. Although several meta-analyseshave shown that modern adjuvant che-motherapy can improve disease re-currence rate and increase disease freesurvival,3 there is usually no increase inlong-termoverall survival. Thechoiceofadjuvant chemotherapy should conformtothesameagentsthatperformbestinthemetastaticsetting.
Trabectedin – a New chemotherapy agent in STS
Trabectedin (ET-743),whichwasderivedfromamarinetunicate,isanewchemo-therapeutic agent that induces deoxy-ribonucleic acid double-strand breaks.
PreliminarytrialsshowedthattrabectedinhassubstantialactivityinSTS,particularlyamong leiomyosarcomas and myxoidliposarcomas, with response rates upto 51% and prolonged disease control.4Toxicity is limited to transient reversibleliver enzyme elevation and myelosup-pression. Trabectedin and anthracyclinecombinationsarenowbeingusedinSTSandovariancarcinoma.
references1. D’Adamo DR. Appraising the current role of chemotherapy for the
treatment of sarcoma. Semin Oncol 2011;5(Suppl 3):S19-S29.2. Hensley MI, Blessing JA, Mannel R, Rose PG. Fixed-dose rate gem-
citabine plus docetaxel as first-line therapy for metastatic uterine leiomyosarcoma: A Gynecologic Oncology Group phase II trial. Gynecol Oncol 2008;109:329-334.
3. O’Connor JM, Chacón M, Petracci FF, Chacón RD. Adjuvant chemo-therapy in soft tissue sarcoma (STS): A meta-analysis of published data. J Clin Oncol 2008;26(Suppl):abstract 10526.
4. Thornton KA. Trabectedin: The evidence for its place in therapy in the treatment of soft tissue sarcoma. Core Evid 2009;4:191-198.
