vs. - maryland patient safety center · health management coaching and medication management...
TRANSCRIPT
Collaborative Activation of Resourcesand Empowerment Services
Building Programs to Fit Patients vs.Bending Patients to Fit Programs

Calvert Memorial Hospital is a 94 bedindependent, not-for-profit, community hospital.
Located in beautiful Prince Frederick, MD,CMH provides general medical / surgical,
psychiatric and post-acute skilled & rehab care.
Founded in 1919, CMH has been taking care of Southern Maryland families for almost 98 years.

• In FY 2016:– 41,928 patients visited our emergency room
– We had 5,092 inpatient admissions and 3,449 observation stays
– Our physicians performed 1,017 inpatient and 8,074 outpatientsurgeries
• There are 228 active and consulting physicians representingover 40 different specialties
• Approximately 1,200 dedicated employees help CMH providethe very best for our patients, with more than 200 volunteershelping to add those "special touches"
• In addition to our main hospital campus, 4 satellite medicaloffice buildings ensure that quality care is no more than 15minutes from anywhere in Calvert County


Discharge Planning Model• Case Managers:
– Inpatient Units: Telemetry, MedSurg, ICU, OB– Emergency Department– Psychiatric Unit
• RN role vs SW role• Weekdays, weekends, evenings• Patient-centered vs Unit-based• Multi-disciplinary rounds• Palliative Care Program• EMA and MDICS – Physician Champions• Curaspan Discharge Central / Ride Central• Bridging transition from acute to post-acute
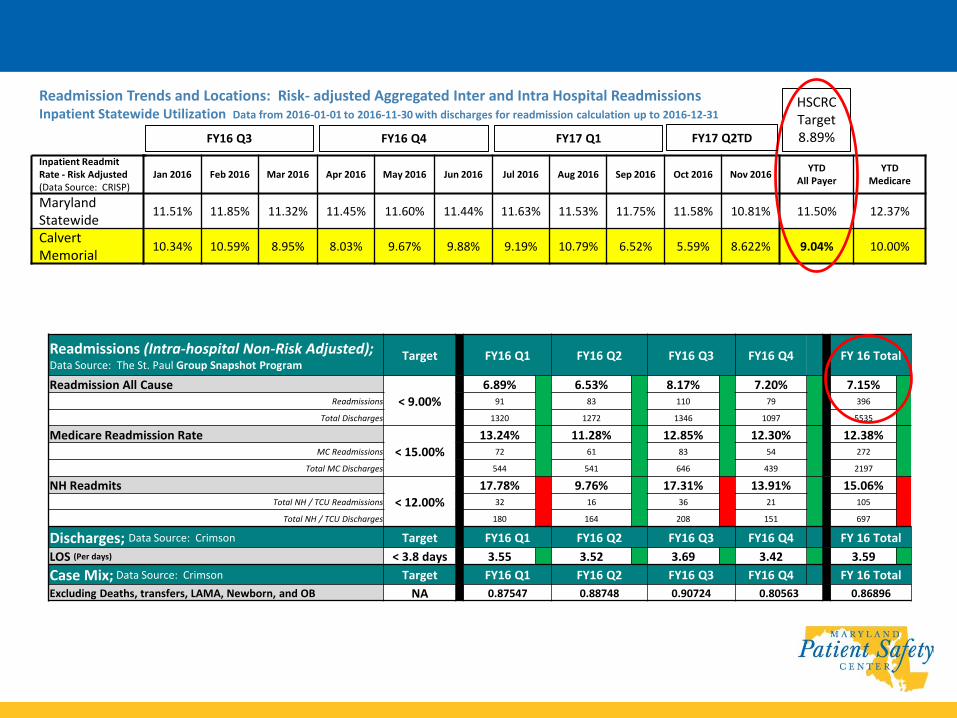
Readmissions (Intra-hospital Non-Risk Adjusted); Data Source: The St. Paul Group Snapshot Program
Target FY16 Q1 FY16 Q2 FY16 Q3 FY16 Q4 FY 16 Total
Readmission All Cause
< 9.00%
6.89% 6.53% 8.17% 7.20% 7.15%Readmissions 91 83 110 79 396
Total Discharges 1320 1272 1346 1097 5535
Medicare Readmission Rate
< 15.00%
13.24% 11.28% 12.85% 12.30% 12.38%MC Readmissions 72 61 83 54 272
Total MC Discharges 544 541 646 439 2197
NH Readmits
< 12.00%
17.78% 9.76% 17.31% 13.91% 15.06%Total NH / TCU Readmissions 32 16 36 21 105
Total NH / TCU Discharges 180 164 208 151 697
Discharges; Data Source: Crimson Target FY16 Q1 FY16 Q2 FY16 Q3 FY16 Q4 FY 16 Total
LOS (Per days) < 3.8 days 3.55 3.52 3.69 3.42 3.59
Case Mix; Data Source: Crimson Target FY16 Q1 FY16 Q2 FY16 Q3 FY16 Q4 FY 16 Total
Excluding Deaths, transfers, LAMA, Newborn, and OB NA 0.87547 0.88748 0.90724 0.80563 0.86896
Readmission Trends and Locations: Risk- adjusted Aggregated Inter and Intra Hospital ReadmissionsInpatient Statewide Utilization Data from 2016-01-01 to 2016-11-30 with discharges for readmission calculation up to 2016-12-31
Inpatient Readmit Rate - Risk Adjusted (Data Source: CRISP)
Jan 2016 Feb 2016 Mar 2016 Apr 2016 May 2016 Jun 2016 Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016YTD
All PayerYTD
Medicare
Maryland Statewide
11.51% 11.85% 11.32% 11.45% 11.60% 11.44% 11.63% 11.53% 11.75% 11.58% 10.81% 11.50% 12.37%
Calvert Memorial
10.34% 10.59% 8.95% 8.03% 9.67% 9.88% 9.19% 10.79% 6.52% 5.59% 8.622% 9.04% 10.00%
FY17 Q1FY16 Q4FY16 Q3
HSCRC Target8.89%FY17 Q2TD

Diagnosis Specific (Intra-hospital Non-Risk Adjusted); Data Source: : The St. Paul Group Snapshot Program
FY16 Q1 FY16 Q2 FY16 Q3 FY16 Q4 FY 16 Total
Congestive Heart FailureReadmissions SAME Diagnosis
Percentage10.20% 2.17% 4.26% 6.00% 5.73%
Readmissions SAME Diagnosis 5 1 2 3 11
Total Discharges 49 46 47 50 192
Readmissions DIFFERENT DiagnosisPercentage
4.08% 4.35% 14.89% 6.00% 7.29%
Readmissions DIFFERENT Diagnosis 2 2 7 3 14
Total Discharges 49 46 47 50 192
Chronic Obstructive Pulmonary Disease
Readmissions SAME DiagnosisPercentage
7.50% 0.00% 9.68% 8.11% 6.52%
Readmissions SAME Diagnosis 3 0 6 3 12
Total Discharges 40 45 62 37 184
Readmissions DIFFERENT DiagnosisPercentage
7.50% 2.22% 4.84% 0.00% 3.80%
Readmissions DIFFERENT Diagnosis 3 1 3 0 7
Total Discharges 40 45 62 37 184
Pneumonia
Readmissions SAME DiagnosisPercentage
2.22% 3.03% 0.00% 0.00% 1.36%
Readmissions SAME Diagnosis 1 1 0 0 2
Total Discharges 45 33 49 20 147
Readmissions DIFFERENT DiagnosisPercentage
2.22% 6.06% 4.08% 20.00% 6.12%
Readmissions DIFFERENT Diagnosis 1 2 2 4 9
Total Discharges 45 33 49 20 147

How are we doing it?Through patient,
caregiver, community and team collaboration.
Calvert CARES!!
Collaborative Activation of Resources and Empowerment Services


Partners in Accountable Care
Collaboration and Transitions(PACCT)
• community coalition of over 30 local agencies and health care providers
• focused on optimizing patient outcomes through improved care
coordination, collaboration and communication
• targeted improvement of transitions between the hospital and home
(medical home, skilled nursing, or retirement community)
Since October 2013, PACCT members have created a forum for sharing
best practices, increasing awareness of housing options for seniors, and
creating solutions to improve patient outcomes and patient experience.

Committee
Purpose
1) Improve patient engagement: motivational interviewing & synchronization of education
2) Improve networking between community partners
3) Enhance information / strategy sharing
4) Take Transitions to Home and Patient Portal Programs "on the road" to community partners
5) Optimize engagement with / use of community resources
6) Optimize use of technology
7) Explore incentivization methods (what's in it for me?)
8) Brand our collaborative and publicize what we are doing / why / outcomes
1) Reduction in all cause readmission rate to < 8% (in Maryland intra and inter hospital rate)
2) Reduction in nursing home readmission rate to < 12%
3) Reduction in Medicaid readmission rate to < 12%
4) Reduction in Medicare patient readmission rate to < 12%
5) Reduction in avoidable hospital based utilization (PQI) < 4%Revised 9/15/16
Key Result
Measures:
Strategies:
3) Improve communication flow and patient centered care coordination between our community health
care partners, as evidenced by the development and implementation of post-acute pathways and
protocols.
Goals / Key
Result Areas:
9) Leverage our collective to increase our access to resources and capabilities and explore ways to share
risks and benefits ($)
PACCT's purpose is to facilitate and promote collaboration between our community health care partners,
with the goal of eliminating care fragmentation, while fostering an environment of collegiality,
networking and resource sharing focused on enhancing our efficiency and effectiveness in optimizing
patient outcomes.
1) Improve the patient centered experience by ensuring patient's receive the right care in the right
setting, as evidenced by the reduction of avoidable admissions, all cause readmissions, emergency
department visits and outpatient observations stays at Calvert Memorial Hospital.
2) Improve synergy (consistency, efficiency, and effectiveness) of patient centered disease specific care
planning, education and medication management provided by our community health care partners.
PACCT Charter
Partners in AccountableCare Collaboration and Transitions

• Initiative Calvert CARES is a free “community benefit” program which takes a
multi-faceted approach to meet the post-discharge needs of patients by assistingpatients at moderate to high risk for readmission or emergency department overuse.
• Team Physician, Nurse, Social Worker, Pharmacist
• Target Population Bridging the gap for patients who:
▪ Are unable to schedule a follow up physician appointment within 5 days post-discharge fromED, observation stay or inpatient admission
▪ Lack a primary care provider
▪ Can’t afford essential medications and/or those who need assistance managing multiplemedications
▪ Need assistance securing transportation to health care appointments
▪ Can benefit from access to an array of post-acute care resources
Interventions Phone calls, patient portal, community outreach, active listening withcoaching, home visits, CARES clinic, financial guidance and assistance
It’s all about the relationship…..
Consistency, Collaboration, Communication = TRUST12

Inputs Activities OutputShort Term Goals
Intermediate Goals
Long Term Goals
FundingCalvert CARES Program
Patient access to
care within 7 days post-
discharge
(Clinic)
Within 6 months
after patient is seen in
Clinic
Within 1 year after
Clinic opens1
Within 1 year after patient is seen in Clinic2
Within 2 years after
Clinic opens1
Within 2 years after patient is seen in Clinic2
Calvert CARES Program Logic Model
Staff
Clinic
Physician
Transitions
to Home
Team
- RN Case
Manager
- Pharmacist
- Social
Worker
Supplies
Clinic
supplies
Patient
self-
management
supplies
Services
Patient
assessment
Patient
education
Resource
referrals
Medication
Assistance
Program
(MAP)
Transportation
Assistance
Program
(TAP)
Patient
Activated
and
competent
in self-
managing
care
Participating
in goals of
care and
care
planning
PCP
collaboration
enhanced
Patient
New PCP ID’d
and has seen
them at least
once
All
prescriptions
filled
Medication
reconciliation
completed
and
communicated
to PCP
Received
Transitions to
Home
education,
including goals
of care
Targeted
population1
10%
reduction in
all-cause
readmissions
10%
reduction in
ED visits
10%
reduction in
observation
stays
Below
national
averages for
all-cause
readmissions
For program
patients2
25% will
have met
their goals of
care
Targeted
population1
10%
reduction in
all-cause
readmissions
10%
reduction in
ED visits
10%
reduction in
observation
stays
Below
national
averages for
all-cause
readmissions
For program
patients2
50% will
have met
their goals of
care
Assumptions:
Patients will use program / clinic
Community PCPs will support program / refer patients to it
Patient / community perception about access to care will improve
Contextual Factors:
Increasing hospital-based health care utilization is due to access to care challenges of under insured, uninsured
Calvert County has a greater than average growth in the population over age 65
Calvert Memorial Hospital is experiencing an increase in patient acuity, intensiveness and complexity
9

Trigger Criteria:• mark all that apply
Risk Score =
☐ Readmitted w/in 30 days
☐ > 2 ED visits w/in 30 days
☐ Hospital LOS > 5 days
☐ Requires intensive case
management
☐ Un/Under insured
☐ Transferred to higher
level of care / where:
☐ Unable to schedule
provider visit w/in 5
days post-DC (or w/in
needed time frame)
☐ Transportation barrier
☐ Newly diagnosed or poorly
managed chronic health
condition
☐ Complex poly-pharmacy
☐ Cannot afford to pay for
medications
☐ Adherence barriers
Diagnosis(es): • mark all that apply
• circle main diagnosis triggering referral
☐ Diabetes
☐ Pneumonia
☐ CHF
☐ Other:
☐ COPD
☐ Other:
Special needs / challenges
which may impact patient’s
self-care management:
☐ Vision
☐ Cognitive Impairment
☐ Health Literacy
☐ Can’t read
☐ Can’t write
☐ Communication:
☐ Language
☐ Hearing
Preference:
☐ Physical Challenges
☐ Financial Challenges
☐ Computer Literacy/ Access
☐ Substance Abuse
☐ Other:
Calvert CARES Program Referrals

Calvert CARES Program Referral Follow-up
Nurse Pharmacist Physician Social Worker
☐ Self-care activation
☐ Patient education
☐ Communication with PCP
☐ Resource referral
☐
☐ Medication reconciliation
☐ Pillbox management
☐ Patient education
☐ Communication with PCP
☐ Resource Referral
☐
☐ Assessment
☐ Patient education
☐ Care planning
☐ Communication with PCP
☐ Resource Referral
☐
☐ Resource assessment
☐ Insurance issues
☐ Coping skills
☐ Social support
☐ Communication with PCP
☐ Resource Referral
☐
Plan: ☐ Transitions to Home Program ☐ Discharge CARES Clinic ☐ Phone Follow Up
• mark all that apply ☐ Medication Assistance Program ☐ Transportation Assistance Program ☐ None ☐ Referral Reviewed (who/when): ☐ Referral Source Follow Up (who/when):
☐ Note in Computer (when): ☐ Previous Referral (who/when):
☐ D/C call (who/when): ☐ 1° Care Manager assigned:
☐ MAP screening (who/when): ☐ TAP screening (who/when):
☐ Call to offer DCC (who/when): ☐ Call to schedule DCC (who/when):
☐ Pt. declined DCC. Alternate plan offered / pt. response:
☐ Call to inform PCP patient scheduled for DCC (who/when):

Calvert CARES Philosophy
• P atience
• E ngagement
• R espect
• K indness

Transitions to Home (T2H)Nurse, Social Worker, Pharmacist
▪ Initiated in 2012 with RN care managers, expanded in 2014 to include social worker andpharmacist
▪ Health management coaching and medication management guidance via phone calls andhome visits – Pharmacist home visits are a significant part of the program
▪ Target high utilizers with a focus on patients with heart failure, chronic obstructive pulmonarydisease, diabetes, pneumonia or multiple comorbidities
▪ Provides an average of 2,000 post-discharge calls to about 1,300 patients per quarter, inclusiveof assessment, coaching and follow-up
▪ Received 1,721 referrals for CARES clinic / MAP / TAP between March 2015 and January 2017
▪ Readmission RCA patient interviews and chart reviews
▪ Potentially avoidable admission RCA patient interviews and chart reviews

Project PhoenixBehavioral Health Case Manager
▪ Partnership between CMH and the Calvert County Health Department, launched August 2015
▪ Targets patients needing mental health and substance abuse services
▪ Provides care management coaching and medication management guidance via phone callsand in person coaching sessions with a social work case manager
▪ Readmission RCA patient interviews and chart reviews
▪ Funded by a Md. Community Health Resources Commission grant awarded to the CalvertCounty Health Department
▪ Received 504 referrals between August 2015 and January 2017
Medication Assistance Program (MAP)Transportation Assistance Program (TAP)
▪ Utilizes the financial assistance programs provided through CMH to help patients pay foressential medications, medical supplies or transportation to medical appointments whenfinancial resources and assistive programs do not meet their needs
Discharge CARES Clinic (DCC)▪ Care management coaching, health status assessment, goals building, intervention
planning, medication therapy management, psycho-social support and resource access
▪ Structured to allow patients extended time with the care team
▪ Facilitate information processing and dialogue between the patient and the careprovider
▪ Patients surveyed on service provision to gain real-time feedback, to address needs as theyarise, and to identify gaps in services which can be served by using the network ofpartners in Calvert CARES

Patient Portal ▪ Provides patients secure internet access to their hospital medical record and
services, such as reviewing lab results, scheduling appointments and paying hospital bills
▪ Exceeded Meaningful Use targets by 70%
CARES Grand Rounds▪ Community focused committee, serving in an advisory capacity to facilitate identification of
potential solutions to care challenges and gaps for high utilization group (HUG) patients
▪ Focus will be on:
- provision of safe, quality patient care in an optimal setting
- awareness, education and accessibility of Calvert Health System and community-basedprograms and resources
- community support and guidance in developing and implementing multi-faceted care plans

Discharge CARES Clinic: Setting Our Sights
This material was prepared by Health Quality Innovators (HQI), the Medicare Quality Innovation Network-Quality Improvement Organization for Maryland and Virginia, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. HQI|11SOW|20170125-164747
Discharge CARES Clinic
▪ Clinic visits are scheduled within 3 to 7 days post-discharge,dependent on patient needs and availability.
▪ Every attempt is made to schedule around other clinic visits / services tohelp the patient with care coordination and management.
▪ The duration of the patient engagement with the Clinic is a mutuallydefined goal between the Clinic and the patient.
▪ Patients may see up to 4 of the Clinic staff in one visit, and will bescheduled for up to a 1 hour block of time per staff person, based ontheir needs.

Discharge CARES Clinic Team
Medical Director / Clinic Physician
▪ Assessment, care planning collaboration / coordination / communicationwith Primary Care Provider (PCP), resource referrals
▪ Focused patient education and care planning in a communication conducivesetting to facilitate patient ability to ask questions, get answers, learn andretain information to allow them to self-manage their health
Transitions of Care RN Care Managers
▪ Self-care activation assessment, intervention, collaboration with PCP
▪ Facilitation of care coordination between CMH, the Clinic, PCP offices andother health care resources
▪ Provides patient teaching/coaching in disease management
▪ Refers to CMH / community services and resources
▪ Assists patient in defining goals and developing a To-Do list

Discharge CARES Clinic TeamTransitions of Care Pharmacist
▪ Medication Therapy Management and medication reconciliation incollaboration with PCP
▪ Provides support with medication changes and education
▪ Supplies pill boxes and guides patients in filling them
▪ Facilitates and fosters patient understanding of their medication plan
Transitions of Care Social Worker
▪ Identify and address social determinants, mental health co-morbidities and overridingsocial and family issues impacting patients ability to manage and coordinate their care
▪ Community resource assistance / counseling in collaboration with PCP
▪ Refer patients to social and health related programs available in their community.
▪ Network with outside agencies to help provide and coordinate these services

Discharge CARES Clinic TeamCoordinator / Liaison
▪ Scheduling, registration, portal enrollment, document management
▪ Face of the clinic - sets the tone for the patient – keeps the patient linked in andengaged between visits
Diabetes Educator
▪ Diabetes knowledge / self-care assessment and education, collaboration with PCP
▪ Review of home use of diabetes management medications, equipment and supplies
▪ Facilitate referral to diabetes related CMH / community services and resources
Coming soon! Respiratory Therapist
▪ Pulmonary assessment and interventions for Heart Failure and Chronic ObstructivePulmonary Disease patients ,with PCP collaboration
▪ Review of home use respiratory management medications, equipment and supplies
▪ Facilitate referral to cardio-pulmonary related CMH / community servicesand resources.
Medication Reconciliation andMedication Therapy Management (MTM)
What brings our patients into our hospitals?
• Medication-related problems: result in 5-10% of hospital admissions
….. 60% of these were avoidable!
• Adverse drug events: the 3rd leading preventable cause of death in the United States
• Medication errors: administration of and missed doses
• Non-adherence: due to cost, access, life style barriers
• Lack of or miscommunication: at admission, during care provision, patient education, transitions of care
26

Medication Therapy Management (MTM)
• Medical care provided by pharmacists
• Goal is to optimize drug therapy and improve therapeuticoutcomes for patients
• Includes:
- performing a comprehensive medication review
- formulating a medication treatment plan
- monitoring efficacy and safety of medication therapy
- enhancing medication adherence through patient empowerment and education
- documenting and communicating MTM services to prescribers in order to maintain comprehensive patient care

Huddles, Hand-offs and Supplies, Oh My!
▪ Weekly Team Planning Meetings
▪ Briefing and Debriefing Huddles
▪ Warm Hand-offs
▪ Supplies

Mr. X and the Blueberries• 49 year old male with history of high blood pressure, chronic alcohol abuse with liver
impact, reflux, Barrett’s esophagus, obesity, medication non-compliance, depression
• Challenges - hadn’t seen Primary Care Provider (PCP) in > 1yr. due to financial issues
- not following medication regime
- unemployed due to severe joint pain and swelling
• Referred to Discharge CARES Clinic post-inpatient discharge
• Saw nurse / physician / pharmacist / social worker at 4 weekly visits over 1 month(12+ hrs. of intervention, including follow-up phone calls) March through April 2015
• Opportunities - high blood pressure and reflux, not taking meds correctly
- Ibuprofen and alcohol overuse due to pain
- Financial management, needs insurance
- Prior elevated uric acid level obtained from remote lab (gout)

Patient Primary Goal: Return to work as a mason
• Plan - Modify medication regime, adding gout medication, replacing Ibuprofen with Acetaminophen, and changed prescriptions so that all medications are now once a day in the AM with breakfast (went from 7 to 11 meds, but patient’s cost actually less)
- Use MAP to help patient pay for medications until he returns to work / gets MA
- Coach on medication compliance improvement and alcohol use reduction
- Add B-complex vitamin and ½ cup of blueberries daily (anti-oxidants)
- Complete paperwork for Hospital Presumptive Eligibility (temporary MA)
- Start simple exercise program, begin with walking
• 3rd Visit - Blood pressure improved from180/100 to 130/85
- Alcohol use self-reported as occasional
- Joint pain improved to degree Mr. X worked several days the previous week
- Clinic MD contacted PCP who agreed to see patient
- Mr. X reports he is feeling better and his family has been supportive of changes
needed. “It is easy to manage these new medications since they are all once a day.
The bad news is I have to fight my family for my blueberries!”

Surprise visit! Mr. X popped into the Clinic about 1 month later, after walking therefrom home (about 2 miles), to thank everyone for their help and toshare his continued success with them.
Outcomes by the numbers
• 3 ED visits and 1 observation stay in the 3 months before being seen in the clinic
• 2 ED visits in the 5 months prior to that
• 0 ED visits / hospital stays during his time attending the clinic
• 0 ED visits / hospital stays in the 10 months after he was transitioned from the clinic
• Patient is compliant with seeing his PCP
• In the 1 year and 10 months since he was last seen in the clinic, he has had 2 ED visits(February 2016 / January 2017) and 2 hospital stays (November 2016 / January 2017)
• Due to his recent hospitalization and ED visit, we are again offering him the CARES Program
31
Sustaining the Win
Discharge CARES Clinicby the Numbers – CY 2016
▪ 165 of the patients referred to Calvert CARES were offered the clinic
▪ 136 of those patients attended at least 1 clinic visit (82.4%)
▪ 335 clinic visits completed (excludes no shows and reschedules)
▪ 45 patients saw the Diabetes Educator (33.1%)
▪ 122 patients utilized Financial Services (89.7%)
Discharge CARES Clinicby the Numbers – CY 2016
▪ Average number of clinic visits / patient = 2.5
▪ Average length of service / patient = 10 weeks
▪ January to June 2016 readmission rate = 3.74%
▪ July to December 2016 readmission rate = 3.60%
▪ CY 2016 readmission rate = 3.67%

Discharge CARES Clinic
Patient Perception Post-visit
34
93%
5%StronglyAgree
Agree
Neutral
Disagree
StronglyDisagree
Felt I know when, how and why to take my
medication
92%
4%StronglyAgree
Agree
Neutral
Disagree
StronglyDisagree
Feel better prepared to follow my health care
plan
94%
4% StronglyAgree
Agree
Neutral
Disagree
StronglyDisagree
Know what I need to do between clinic visit and my next Drs.
appointment
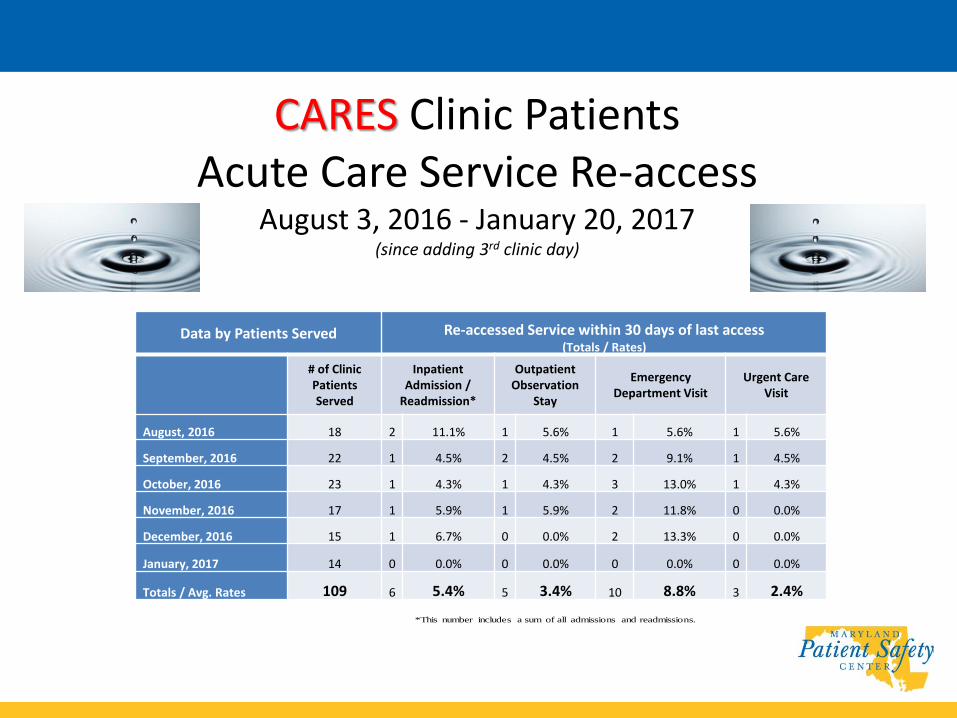
CARES Clinic PatientsAcute Care Service Re-access
August 3, 2016 - January 20, 2017(since adding 3rd clinic day)
Data by Patients Served Re-accessed Service within 30 days of last access(Totals / Rates)
# of Clinic Patients Served
Inpatient Admission /
Readmission*
Outpatient Observation
Stay
Emergency Department Visit
Urgent Care Visit
August, 2016 18 2 11.1% 1 5.6% 1 5.6% 1 5.6%
September, 2016 22 1 4.5% 2 4.5% 2 9.1% 1 4.5%
October, 2016 23 1 4.3% 1 4.3% 3 13.0% 1 4.3%
November, 2016 17 1 5.9% 1 5.9% 2 11.8% 0 0.0%
December, 2016 15 1 6.7% 0 0.0% 2 13.3% 0 0.0%
January, 2017 14 0 0.0% 0 0.0% 0 0.0% 0 0.0%
Totals / Avg. Rates 109 6 5.4% 5 3.4% 10 8.8% 3 2.4% *This number includes a sum of all admissions and readmissions.

CARES Grand Rounds Charter & CY'16 Plan
Committee Purpose:
Calvert Memorial Health System's CARES Grand Rounds (Collaborative Activation of Resources and Engagement Services), as a community focused committee, serves in an advisory capacity to facilitate identification of potential solutions to care challenges and gaps for high utilization group (HUG) patients. Committee focus will be on: ▪ provision of safe, quality patient care in the optimal setting ▪ awareness, education and accessibility of Calvert Health System and community-based programs and resources ▪ fostering an environment of collegiality and best practice sharing based upon open discussion and the ability to have crucialconversations ▪ community support and guidance in developing and implementing multi-faceted care plans
Goals / Key Result Areas:
1) Improve the patient centered experience by ensuring patient's receive the right care in the right setting, as evidenced by the reduction of inappropriate utilization of health care services in the community.
2) Improve synergy (consistency, efficiency, and effectiveness) of patient centered disease specific care planning, education and medication management provided by our community health care partners.
3) Improve communication flow and "breakdown the silos" between our community health care partners, as evidenced by the development and implementation of community-based care plans.
Strategies:
1) Improve patient engagement: motivational interviewing & synchronization of education2) Improve networking between community partners3) Enhance information / strategy sharing4) Optimize engagement with / use of community resources5) Optimize use of technology6) Leverage our collective to increase our access to resources and capabilities and explore ways to share risks and benefits ($)
Key Result Measures:
Patients reviewed at CARES Grand Rounds will:1) Have a care plan developed and implemented within 30 days post review, with a goal to avoid observation stays or inpatient admissions, for a minimum of 30 days post review2) Attain individualized goals developed for them by members of the CARES Grand Round Team, in collaboration with their community physician(s), in the projected time frames with measurable outcomes
Examples: - improved medication adherence - decreased emergency department visits - increased community resource utilization

Mr. Z – It Takes a Village• 54 year old male with history of peripheral vascular disease with
ischemic left foot ulcer, complicated by cellulitis and abscess. Also has history of high blood pressure, hyperlipidemia, previous alcohol and tobacco use. 1 ED visit and 1 inpatient admission June 2016 – referred by Case Management.
• Challenges - hadn’t seen Primary Care Provider (PCP)in > 2yrs. due to financial issues
- not following medication regime
- no insurance / no photo ID
- homeless
• Referred to Discharge CARES Clinic + MAP for wound caresupplies and medications

Mr. Z – It Takes a Village• Saw CARES Team for 16 visits October 2016 thru January 2017
• Collaborators: Vascular Clinic, Southern Maryland Community Network, On Our Own of Calvert (socialization / transportation)
• Goals - obtain insurance within 1 month of 1st clinic visit (met)
- find housing within 1 week of 1st clinic visit (met)
- connect with mental health resources in community within 1 month of 1st clinic visit (met)
- assist with obtaining a photo ID within 3 months of 1st
clinic visit (met)
- assist with obtaining a PCP, once photo ID obtained and insurance coverage active (met)
• Outcomes - 1 inpatient admission December 2016,cellulitis left foot, continues in program

How Big is Our CARES Village?• 0.8 FTE Physician
• 2.5 FTE Nurse
• 0.9 FTE Pharmacist
• 1.6 FTE Social Worker
• 1.0 FTE Coordinator / Liaison
Total = 6.8 FTE (272 hours / week)
Supported by our PACCT membershipof 30+ organizations / agencies

Show Me the ▪ Initial FY15 program budget = $417K
▪ Due to program success, and the need to serve a larger number of patients, the budget was increased to $526K for FY16 and $577K for FY17
▪ We have performed ≈ 3% better to budget each year
Program ROI Due to Improvements in:▪ Health care spend per beneficiary
- through reduced utilization and readmissions
▪ Safer patient environment- through reduced exposure to hospital associated conditions due to reducedhospital utilization
▪ Overall patient health- through provision of services in the patient home, care coaching, referrals topartnering service providers and discharge CARES clinic services …..
Through state incentive programs and grant opportunities (HSCRC andRural Maryland Prosperity Investment Fund) Calvert Memorial Hospitalhas been awarded ≈ $1.2M over the past 3 years

CARES in Action


The Future
Maryland Care Redesign Programs
• Complex and Chronic Care Improvement Program (CCIP)
• Hospital Care Improvement Program (HCIP)
Physician Engagement Strategies
• Calvert CARES Program, with focus on Pharmacist & Social Worker support to key practices
• TLC-MD Coalition, with a focus on initiatives, information sharing, care planning, communication
CARES Take AwaysPut Patient at the Center and the Rest Will Follow
▪ Slow down the pace – give patients time to listen, process andformulate questions
▪ Identify the patient’s goal(s) and then build the plan upon them
▪ Rinse and repeat – the 3rd, 4th …. or 7th time may be the charm
▪ See the patient fresh each time….don’t give up – you never knowwhen they are ready / activated to make needed lifestyle changes
▪ Consider implementing Medication Therapy Management, a group ofservices provided by a trained pharmacist, to gain the bestmedication outcomes for your patients
45

Remember PERK
• Patience
• Engagement
• Respect
• Kindness
More CARES Take AwaysDesign Programs for Your Patients, Not Your Data
▪ Consider a patient-centered model when developing TransitionsTeams, Discharge Care Clinics, Chronic Care Clinics
▪ Remember - programs are tools. Make sure your tools fit yourpatients needs, not your needs or what you think patients need
▪ Decrease hand-offs and enhance the strength of the relationshipbetween the patient and your post-acute tools by crossing over staffbetween programs
Remember,It’s all about the relationship…..
Consistency, Collaboration, Communication = TRUST
47
