wa health clinical services - rph.health.wa.gov.au
TRANSCRIPT

WA Health Clinical ServicesFramework 2005 – 2015
Delivering a Healthy WA
Healthy Workforce ● Healthy Hospitals ● Healthy Partnerships ● Healthy Communities ● Healthy Resources ● Healthy Leadership
© Department of Health, 2005
HP
2978
SE
PT
’05
2064
3
September 2005

For further information please contact:
Health Policy and Clinical Reform
Department of Health
Phone: (08) 9222 4434
Fax: (08) 9222 2192
Email: [email protected]

Foreword
This WA Health Clinical Services Framework 2005 – 2015 is WA Health’s strategic overview forClinical Services, developed in response to recommendations made by the Health ReformCommittee in its Final Report of 2004 (the ‘Reid report’) and the Clinical Services Consultation.
The WA Health Clinical Services Framework has now been finalised following a period of intenseconsultation. WA Health is committed to the implementation of the recommendations of the Reidreport and to utilising all available resources for best outcomes and greatest benefit for thehealth of our community.
Significant elements of the WA Health Clinical Services Framework include:
● clear role delineation for each of our health services and care facilities
● a description of the bed numbers planned for the metropolitan area
● the location of the central tertiary hospital site at the QEII Medical Centre
● significant investment in our health service infrastructure including a new tertiary hospital forthe south metropolitan region to be developed as a collaborative initiative between FremantleHospital and Royal Perth Hospital
● building up our general hospitals
● investment in education and research
● a foreshadowing of work on models of care with a greater emphasis on prevention, primarycare and care in the most appropriate setting
● advancement of country health service role delineation in alignment with metropolitan plans.
This document should be read in conjunction with the Clinical Services Consultation 2005documents (http://www.health.wa.gov.au/HRIT/csc/index.cfm) which provide the backgrounddata, rationale for change and reform options which informed the decision-making process forthis framework. The consultation process engaged a large number of expert clinical stakeholders,staff and community in deliberation about the options and implications for implementation. I amgrateful to all who participated in this process for their interest, investment of time andcontribution of knowledge and expertise.
A number of critical factors will impact on the successful implementation of the framework.These factors include the development of a strategic workforce plan, clinical frameworks andservice models, infrastructure development plans, information, communication and technologyand Area Health Service development plans. These planning processes will provide opportunitiesfor the participation of all stakeholders (clinicians, staff, community, patients, consumers) andwill build on the existing strengths and the many initiatives already in progress.
i
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
clinicalframeworknew spread 21/9/05 3:14 PM Page 1

The way forward will present many challenges for the implementation of the WA Health ClinicalServices Framework, but we are investing significant effort to ensure we are fit for the journeyahead. This includes building on the wealth of talent, skills and experience of our people,developing our leaders through our Healthy Leadership strategies and organisational realignmentto ensure our Area Health Services have the support and resources needed to deliver appropriatestandards and quality of care.
The commitment of stakeholders to work together to implement the change required is vital andalready evident throughout many parts of our system. It is this commitment that will ensure thelong-term goals of the health reform program are achieved.
DR NEALE FONG
Director General Executive Chairman Health Reform Implementation Taskforce
September 2005
ii
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
clinicalframeworknew spread 21/9/05 3:14 PM Page 2

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
Content
Foreword i
Contents iii
1. Introduction 1
2. WA Health Clinical Services Framework 4
2.1 Model of Care 4
2.2 Clinical Services Role Delineation 7
2.2.1 Metropolitan Clinical Services Role Delineation 7
Metropolitan Clinical Services Framework Matrix 11a - 11d
2.2.2 Country and South West Area Clinical Services Role Delineation 13
2.3 Metropolitan Bed Strategy 13
2.4 Vision for Area Health Services 15
2.4.1 North Metropolitan Area Health Service 16
2.4.2 South Metropolitan Area Health Service 18
2.4.3 Women’s and Children’s Health Service 20
2.4.4 WA Country Health Service 22
2.4.5 South West Area Health Service 25
2.5 Education and Research 26
2.6 Pathology Services WA 27
2.7 Mental Health 27
3. Facilitating Change 29
3.1 Governance and Organisational Structure 29
3.2 Strategic Workforce Framework 30
3.3 Infrastructure Development Framework 33
3.4 Information and Communication Technology Framework 35
3.5 Recurrent Costing of the WA Health Clinical Services Framework 35
4. Health Service Development Timeframe 37
5. The Way Forward 38
Appendix 1 Clinical Services Role Delineation 39
Appendix 2 WA Country Health Service Clinical Services Delineation Matrix 63
iii
clinicalframeworknew spread 21/9/05 3:14 PM Page 3

iv
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
Delivering a Healthy WAWA Health Strategic Intent 2005-2010
WA Health Strategic Plan2005-2010
Healthy LeadershipImproving clinical and managerial leadership
Healthy ResourcesProviding sustainable resourcing
Managing budgetsAccountable for performance
Management of assets to deliver the best health benefit
Healthy WorkforceRecruit, develop and retain
Develop knowledge, skills and participationPromote a culture of professionalism, teamwork and accountability
Healthy PartnershipDeveloping strongerparticipation with:
Consumers NGOs
Health ProfessionalsFederal Government
Private Sector
Healthy HospitalsBuilding new
hospitalsUpgrating existing
hospital stockProviding efficient and
productive health system processes
Being innovative in delivery methodsNew generation
information technology
Healthy CommunitiesImproving lifestyle,
prevention and health promotion
Improving equitable andaccessible health services
clinicalframeworknew spread 21/9/05 3:14 PM Page 4

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
1. Introduction
The WA Health Clinical Services Framework (CSF) is a strategic planning framework for thedevelopment and provision of health care services throughout Western Australia over the next tento fifteen years and beyond.
Informed by the final recommendations of the Health Reform Committee in 2004 (the ‘Reidreport’), the CSF provides a guide for the Department of Health and Area Health Services for thedevelopment of a health care system that will contribute to the achievement of a number of longterm reform objectives, namely to:
● improve access to services
● reduce inequality in health status
● provide safe, high quality health care
● promote a patient centred continuum of care
● ensure value for money
● optimise public and private services
● improve the balance of preventative, primary and acute care
● be financially sustainable as an integrated system
● support a highly skilled and dedicated workforce.
The CSF should be viewed as a foundation from which more extensive and detailed planning willoccur. It is to be used in conjunction with other organisational planning documents such as theDelivering a Healthy WA Strategic Intent 2005-2010 which outlines key intentions for ensuring aHealthy Workforce, Healthy Partnerships, Healthy Hospitals, Healthy Communities, HealthyResources and Healthy Leadership.
The CSF has been developed as part of an extensive planning process encompassing the followingprojects and reviews:
● Health Reform Committee Final Report as endorsed by Governmenthttp://www.health.wa.gov.au/HRIT/publications/docs/Final_Report.pdf
● Health Reform Implementation Taskforce Workplanhttp://www.health.wa.gov.au/HRIT/publications/index.cfm
● WA Health Strategic Intent 2005-2010http://www.health.wa.gov.au/hrit/publications/docs/Strategic_Intent_2005-2010.pdf
● review of planning assumptions including impact of reform measures, impact of newtechnology, service demand modelling and population projections
1
clinicalframeworknew spread 21/9/05 3:14 PM Page 5

● Clinical Services Consultation 2005 http://www.health.wa.gov.au/HRIT/csc/index.cfm
● WA Country Health Services Review 2003http://www.wacountry.health.wa.gov.au/publications/docs/Country_Review.pdf
The Clinical Services Consultation was an important stage in the development of the CSF and theimmense wealth of information, recommendations and suggestions gathered was reviewed andused to inform the final decision-making. All submissions received during this process have beenregistered and will be used to inform the subsequent planning for implementation of the CSF andtransition arrangements.
The consultation process also validated a number of considerations which the health carecommunity of WA felt critical to the successful implementation of the CSF:
● the need for a greater focus on workforce planning
● the role of training and research
● the importance of participation from clinicians and staff in decision making and planningprocesses
● the need for greater integration of the health care system across the state
● the need for a more defined continuum of care across levels of care within many disciplines
● the need for work on appropriate models of care for specific clinical programs
● the importance of the private and non-government sector in health care provision.
The South West Area Health Services and WA Country Health Service have also embarked uponcomprehensive health service planning processes in consultation with their communities andregions. Whilst distinct from the metropolitan process due to the nature and timing of previoussystem reviews, this plan begins to incorporate all areas and health services as they align withthe overall vision for the health system.
The CSF is situated within an ongoing organisational planning framework that will ensure planningat all levels of the system is aligned and focused on the same strategic outcomes and thatstrategies are functioning within an accountable structure.
2
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
clinicalframeworknew spread 21/9/05 3:14 PM Page 6

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
Development of WA Health Strategic Plan 2005-2010
3
Clinical Services
Consultation
Along with● Workforce Planning● Recurrent Costing● Ambulatory Care
Projects● Infrastructure
Planning● Information and
CommunicationTechnology
WA HealthClinical Services
Framework
WACHS*Strategic
Plan
SWAHS**Services
Consultationand Planning
WA HealthStrategic
Plan
* WACHS – WA Country Health Service** SWAHS – South West Area Health Service
clinicalframeworknew spread 21/9/05 3:14 PM Page 7

2. WA Health Clinical Services Framework
2.1 Model of CareThe need for reform within the state’s public health system was well documented in the Reidreport. In particular, many recommendations were made regarding population health, primaryand community care and access to hospital services.
The report findings included:● fragmentation of the health system between primary care sector (GP, Pharmacist, Allied
Health Professional, Community Health Nurse) and the public hospital system● poor coordination and communication between primary care and acute care leading to
avoidable admissions, adverse events and poor patient outcomes● lack of focus on health promotion and early intervention● tertiary hospitals admitting 80% of patients for secondary care● concentration of hospital beds in large tertiary hospitals● barriers to patients accessing the system (cultural, geographical, socio-economic).
The Reid report recommended working towards a system that:● appears to the patient as a single unified health system, rather than comprising discrete
disconnected entities ● increasingly emphasises the importance of health promotion, early intervention and prevention
programs, and● provides care in the most appropriate setting, particularly through the development of both
general and specialist secondary care hospitals.
In essence, the vision offers a new direction forward for the model of care within the publichealth system, creating a system that invests more in keeping people well and at home andaccessing appropriate hospital services for the right reasons.
Of priority will be the implementation of appropriate strategies to reduce the inequality in healthstatus with a focus on Aboriginal health and the disadvantaged in areas of health promotion andearly intervention, fostering a patient centred approach to care services with strong consumerparticipation, the development of links with all sectors of health and broader community servicesand greater responsibility at local area health service level for service delivery.
Significant reconfiguration of health services is now required to deliver this vision. The CSF bringstogether those recommendations made in the Reid report designed to support this goal. The charton page 6 provides an example of how the principles of care as outlined in the Reid report willinform the way we organise our systems and health strategies with the goal of improving healthoutcomes and creating ‘Healthy communities’.
The model of care development will need to be supported by a range of other more specificclinical strategies and policies which complement the vision, a number of which are already well progressed. The Health Policy and Clinical Reform division within the Department of Health willtake a lead role in the development of statewide clinical networks to achieve this aim.
4
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
clinicalframeworknew spread 21/9/05 3:14 PM Page 8
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
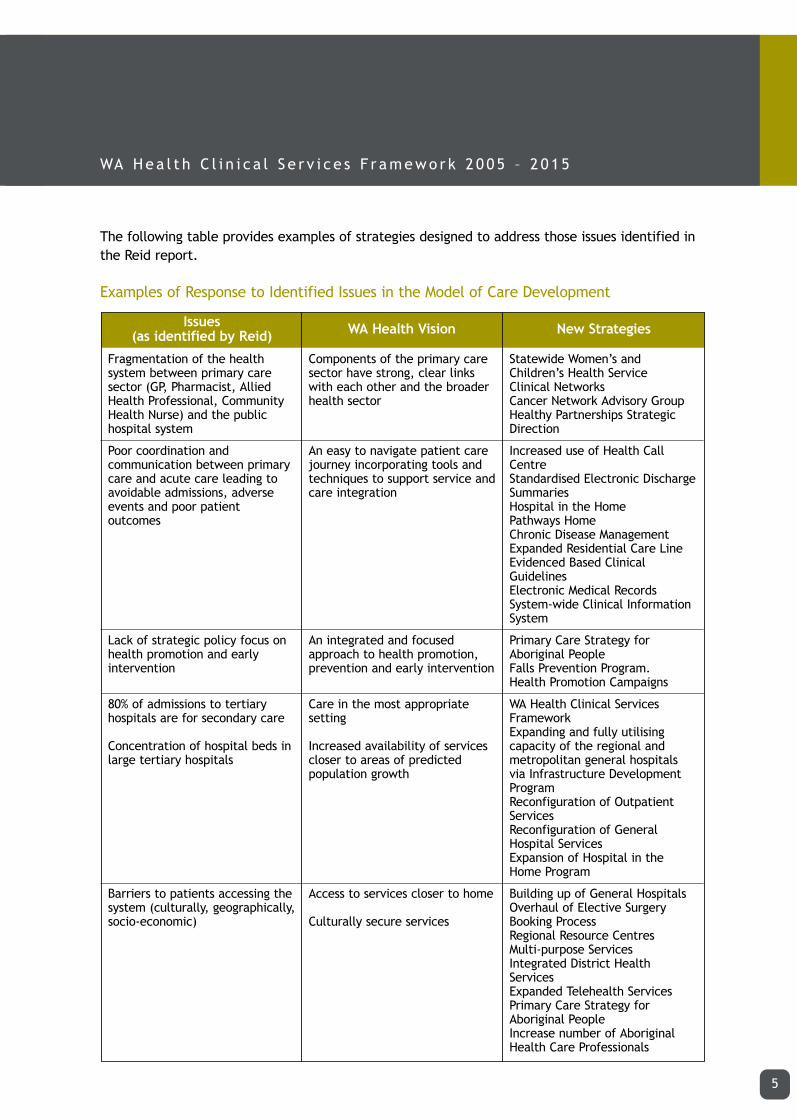
The following table provides examples of strategies designed to address those issues identified inthe Reid report.
Examples of Response to Identified Issues in the Model of Care Development
5
Fragmentation of the healthsystem between primary caresector (GP, Pharmacist, AlliedHealth Professional, CommunityHealth Nurse) and the publichospital system
Poor coordination andcommunication between primarycare and acute care leading toavoidable admissions, adverseevents and poor patientoutcomes
Lack of strategic policy focus onhealth promotion and earlyintervention
80% of admissions to tertiaryhospitals are for secondary care
Concentration of hospital beds inlarge tertiary hospitals
Barriers to patients accessing thesystem (culturally, geographically,socio-economic)
Components of the primary caresector have strong, clear linkswith each other and the broaderhealth sector
An easy to navigate patient carejourney incorporating tools andtechniques to support service andcare integration
An integrated and focusedapproach to health promotion,prevention and early intervention
Care in the most appropriatesetting
Increased availability of servicescloser to areas of predictedpopulation growth
Access to services closer to home
Culturally secure services
Statewide Women’s andChildren’s Health ServiceClinical Networks Cancer Network Advisory GroupHealthy Partnerships StrategicDirection
Increased use of Health CallCentreStandardised Electronic DischargeSummaries Hospital in the HomePathways HomeChronic Disease Management Expanded Residential Care LineEvidenced Based ClinicalGuidelinesElectronic Medical RecordsSystem-wide Clinical InformationSystem
Primary Care Strategy forAboriginal PeopleFalls Prevention Program.Health Promotion Campaigns
WA Health Clinical ServicesFrameworkExpanding and fully utilisingcapacity of the regional andmetropolitan general hospitalsvia Infrastructure DevelopmentProgramReconfiguration of OutpatientServicesReconfiguration of GeneralHospital ServicesExpansion of Hospital in theHome Program
Building up of General HospitalsOverhaul of Elective SurgeryBooking ProcessRegional Resource CentresMulti-purpose ServicesIntegrated District HealthServicesExpanded Telehealth ServicesPrimary Care Strategy forAboriginal PeopleIncrease number of AboriginalHealth Care Professionals
Issues (as identified by Reid) WA Health Vision New Strategies
clinicalframeworknew spread 21/9/05 3:14 PM Page 9

6
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
Prin
cipl
es:
Impr
ove
acce
ss t
o se
rvic
es
Redu
ce in
equa
lity
in h
ealt
hst
atus
;
Prov
ide
safe
, hi
gh q
ualit
yhe
alth
car
e;
Prom
ote
a pa
tien
t ce
nter
edco
ntin
uum
of
care
;
Ensu
re v
alue
for
mon
ey;
Opt
imiz
e pu
blic
and
pri
vate
serv
ices
;
Impr
ove
the
bala
nce
ofpr
even
tati
ve,
acut
e an
dpr
imar
y ca
re;
Be f
inan
cial
ly s
usta
inab
le a
s an
inte
grat
ed s
yste
m;
and
Supp
ort
a hi
ghly
ski
lled
and
dedi
cate
d w
orkf
orce
.
Clin
ical
Net
wor
ks
1.Ca
ncer
2.M
enta
l Hea
lth
3.Ca
rdio
vasc
ular
Dis
ease
4.Tr
aum
a, In
jury
and
Po
ison
ing
5.W
omen
’s H
ealt
h (L
ocat
ed
wit
hin
WCH
S)6.
Ch
ild a
nd Y
outh
Hea
lth
(Loc
ated
wit
hin
WCH
S)7.
M
obili
ty
8.
Resp
irat
ory
Hea
lth
9.
Gen
itou
rina
ry H
ealt
h10
. Di
gest
ive
and
Endo
crin
e H
ealt
h11
. In
fect
ious
Dis
ease
s an
d Se
lect
ed C
ondi
tion
s12
.N
euro
scie
nce
and
the
Sens
es
Popu
lati
on G
roup
s
Aged
Car
eAb
orig
inal
Hea
lth
Popu
lati
on H
ealt
h
Som
e ex
ampl
es
WA
Hea
lth
Clin
ical
Ser
vice
sFr
amew
ork
Hea
lthy
@H
ome
Chro
nic
Dise
ase
Fram
ewor
k
Men
tal H
ealt
h Fr
amew
ork
Aged
Car
e Fr
amew
ork
Prim
ary
Care
Str
ateg
y fo
rAb
orig
inal
Peo
ple
Falls
Pre
vent
ion
Prog
ram
Path
way
s H
ome
Hea
lth
Call
Cent
re
Resi
dent
ial C
are
Line
Evid
ence
Bas
ed C
linic
alG
uide
lines
Regi
onal
Res
ourc
e Ce
ntre
s
Mul
ti-p
urpo
se S
ervi
ces
Inte
grat
ed D
istr
ict
Hea
lth
Serv
ices
IMPR
OVE
D H
EALT
HO
UTC
OM
ES
HEA
LTH
Y CO
MM
UN
ITIE
S
PRIN
CIPL
ES O
F CA
RE
Deliv
erin
g a
Hea
lthy
WA
– St
rate
gic
Inte
ntH
ealt
hy W
orkf
orce
●H
ealt
hy P
artn
ersh
ips
●H
ealt
hy H
ospi
tals
●H
ealt
hy C
omm
unit
ies
●H
ealt
hy R
esou
rces
●H
ealt
hy L
eade
rshi
p
STRA
TEG
IES/
SERV
ICES
/FRA
MEW
ORK
SST
RUCT
URE
S
GU
IDE
ARTI
CULA
TECO
NTR
IBU
TE T
O
WA
Hea
lth
– M
odel
of
Care
clinicalframeworknew spread 21/9/05 3:14 PM Page 10

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
2.2 WA Health Clinical Services Role DelineationThe WA Health Clinical Services Framework (CSF) outlines the role of each metropolitan hospitalas well as the key clinical services to be provided at each hospital site, reflecting the principlesoutlined in the Reid report, the vision for the model of care and feedback gained throughconsultation. It is based on the principles of providing services closer to people’s homes and thereduction of duplication in services provided in the metropolitan area.
The CSF provides a strategic map of health care services and acts as a foundation for furtherplanning processes. The framework will continue to be developed and refined and used moreextensively throughout the state over time.
The CSF is essential to ensure that services are integrated, service directions are clearlyarticulated and can be planned for in a strategic manner. The CSF also allows for betterworkforce planning, informs financial and capital planning and clarifies clinical governance andmodels of evaluating care to ensure safety and quality while promoting economic efficiency in ourhealth system.
The CSF, including role delineation and service level definitions, has been developed incollaboration with clinical experts and is based upon similar approaches in other health caresystems. Important factors reviewed in the development of the CSF include:
● projected future demand for clinical services
● specialty specific patterns of services delivery including where patients receive servicescompared to where they live
● population growth and ageing
● scenario modelling designed to review detailed changes at clinical, age, region of residenceand hospital level including changes in demand, average length of stay and referral patterns
● impact of reform initiatives.
2.2.1 Metropolitan Clinical Services Role DelineationThe role delineation matrix provides a clear role statement for each metropolitan public hospitaland provides an outline of the type and level of clinical services to be provided at each of thesesites into the future.
The matrix shows planned movement in clinical services from site to site as well as the upgradingof clinical services at some sites and the establishment of clinical services at new sites.
The matrix is intended as a strategic role statement, focusing on key clinical groups. Roledelineation for more specific clinical specialties will be undertaken as part of the next planningstage.
7
clinicalframeworknew spread 21/9/05 3:14 PM Page 11

The role and service type outlined in the matrix for each hospital is based on the application ofsome underlying principles and data including:
● providing care closer to where people live
● ensuring accessibility across the metropolitan area and country regions
● developing networked clinical services across the metropolitan area, with rural links
● supporting the Area Health Service concept
● projected future demand for services
● projected future population growth and demographic trends.
Definitions used in the Clinical Services Role Delineation
Tertiary HospitalsCurrently (2004-05) tertiary hospitals include:
● Royal Perth Hospital
● Sir Charles Gairdner Hospital
● Fremantle Hospital
● Princess Margaret Hospital (tertiary paediatric facility)
● King Edward Memorial Hospital (tertiary women’s facility)
● Graylands Hospital (tertiary mental health facility)
● Royal Perth Hospital Shenton Park Campus (tertiary rehabilitation facility).
By 2011, tertiary hospitals will be:
● Sir Charles Gairdner Hospital (central tertiary hospital)
● Fiona Stanley Hospital (southern tertiary hospital)
● Princess Margaret Hospital (tertiary paediatric facility)
● King Edward Memorial Hospital (tertiary women’s facility)
● Graylands Hospital (tertiary mental health facility)
● Royal Perth Hospital Shenton Park Campus (tertiary rehabilitation facility)
Note that by at least 2015-16, it is planned that Joondalup Health Campus will also operate as afully-fledged tertiary facility (ie northern tertiary hospital). While this was originally not planneduntil after 2020, the demand for services as population growth in the north has resulted inbuilding up of Joondalup earlier than previously anticipated.
Also, by 2015–16, it is planned that tertiary rehabilitation services will be relocated from RoyalPerth Hospital Shenton Park Campus to the Fiona Stanley Hospital, with the Shenton Park campusclosing.
8
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
clinicalframeworknew spread 21/9/05 3:14 PM Page 12

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
Tertiary hospitals provide services requiring highly specialised skills, technology and support to allof Western Australia. Typically a tertiary hospital may include centres of excellence, research anddevelopment and will provide a leadership role of integrated clinical services.
As a general rule of thumb, a tertiary hospital provides services at a level 6 according to theclinical services definition.
General HospitalsBy 2011, general hospitals will be:
● Joondalup Health Campus (although this campus is planned to be a tertiary facility by 2015-16or sooner)
● Swan District Hospital
● Armadale Kelmscott Memorial Hospital
● Rockingham/Kwinana District Hospital.
The term general hospital highlights the community focus rather than a purely clinical focus. Ageneral hospital should provide for most of the health needs of its population. A general hospitalhas the following clinical services and facilities:
● emergency departments
● 24 hour anaesthetic cover
● high dependency units
● general surgery capacity (including day surgery)
● obstetric services
● general medical and geriatric services
● general paediatrics
● some rehabilitation and mental health services
● centre for diagnostics, treatment and ambulatory care.
In the main, a general hospital provides services at a level 4 according to the clinical servicedefinition. There are some exceptions, particularly with Joondalup Health Campus which will bebuilt up in the medium term as it positions itself to be a tertiary facility. A general hospital willhave resident general specialists, some visiting subspecialists and junior medical staff.
9
clinicalframeworknew spread 21/9/05 3:14 PM Page 13

Specialist HospitalsBy 2011, specialist hospitals will refer to Osborne Park, Bentley and Fremantle Hospitals whichwill be reconfigured to focus on mental health, aged care and rehabilitation services. None ofthese hospitals will have emergency departments (although Fremantle Hospital will have anurgent primary care service). All three hospitals will retain some same day/ambulatory medicaland surgical services. Some multiday elective surgical services will also be retained at Fremantlein the medium term. Osborne Park Hospital will retain some multiday elective surgery, becomingthe centre for elective surgery for the North Metropolitan Area Health Service.
Generally, specialist hospitals (Osborne Park, Bentley and Fremantle Hospitals) will provideservices at level 4/5 in their specialty according to the clinical services definition.
Other HospitalsOther hospitals by 2011 include:
● Kalamunda District Hospital
● Peel Health Campus.
Kalamunda hospital will provide varied services as per the Clinical Services Role Delineation. APeel Clinical Services Framework will be developed as part of a separate planning process.
The role delineation matrix which follows outlines the clinical services to be provided at eachmetropolitan hospital. For information regarding how to interpret the matrix, please refer toAppendix 1.
10
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
clinicalframeworknew spread 21/9/05 3:14 PM Page 14

General
Cardiology
Endocrinology
Geriatric
Neurology
Renal - general- dialysis
Oncology
Radiation oncologyRespiratory
Palliative care
Gastroenterology
Other
General
ENT
Gynaecology
Ophthalmology
Orthopaedics
Urology
Cardiothoracic
Vascular surgery
Neurosurgery
Plastics
Burns
EDUrgent primary care
METROPOLITAN CLINICAL SERVICES FRAMEWORK
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
6
6
6
6
6
66
6
6
6
6
6
6
6
6
5
6
6
6
6
6
5/6
6
6
6
6
6
6
6
6
66
6
6
6
6
6
6
6
6
5
6
6
6
6
6
5/6
6
6
6
5/6
6
6
6
4
66
6
nil
6
6
6
6
6
6
4
6
6
6
6
6
4
5
4
6
3
nil
nil
5
nil
34
nil
nil
nil
nil
nil
nil
4
4
nil
4
nil
nil
nil
nil
nil
nil
nil
nil3
3
nil
nil
5
nil
34
nil
nil
nil
nil
nil
nil
4
4
nil
4
nil
nil
nil
nil
nil
nil
nil
nil3
4
3
3
4
3
nilnil
nil
nil
3
2
2/3
3/4
4
4
4
4
4
4
nil
3
nil
3
2
4
5
4
4
5
4
44
4
nil
4
4
4
4
5
4
4
4
4
4
nil
4
nil
4
2
5
5
4
4
5
4
44
4
nil
4
4
4
4
5
4
4
4
4
4
nil
4
nil
4
2
5
3
nil
3
5
2
22
nil
nil
3
2
3
3
3
4
3
3
3
3
nil
nil
nil
2/3
nil
nil
3
nil
3
5
nil
44
nil
nil
nil
nil
3
nil
4
4
nil
4
nil
4
nil
nil
nil
nil
nil
nil
3
nil
3
5
nil
44
nil
nil
nil
nil
3
nil
4
4
nil
4
nil
4
nil
nil
nil
nil
nil
nil
4
3
3
5
3
34
3
nil
4
2
3
4
4
4
4
4
4
4
nil
3
nil
3
2
4/5
5
4
4
5
4
45
4
nil
4
4
4
4
5
4
4
4
4
4
nil
4
nil
4
2
5
5
4
4
5
4
45
4
nil
4
4
4
4
5
4
4
4
4
4
nil
4
nil
4
2
5
6
6
6
6
6
66
6
6
6
6
6
6
6
6
nil
6
6
6
6
6
6
6
4
6
6
6
6
6
6
66
6
6
6
6
6
6
6
6
nil
6
6
6
6
6
6
6
4
6
6
6
6
6
6
66
6
6
6
6
6
6
6
6
nil
6
6
6
6
6
6
6
4
6
6
6
6
6
6
66
6
6
6
6
6
6
6
6
nil
6
6
6
6
6
6
6
6
6
nil
nil
nil
nil
nil
nil4
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil3
nil
nil
nil
nil
nil
nil4
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil3
nil
nil
nil
nil
nil
nil4
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
5
4
nil
nil
nil
4
nil
nil
nil
nil
nil
nil
nil
nilnil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nilnil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
4
3
3
5
4
34
nil
nil
4
2
4
4
4
4
4
3
4
4
nil
4
nil
3
2
4/5
5
4
4
5
4
44
4
nil
4
4
4
4
5
4
4
4
4
4
nil
4
nil
4
2
5
5
4
4
5
4
44
4
nil
4
4
4
4
5
4
4
4
4
4
nil
4
nil
4
2
5
3
nil
4
5
nil
nilnil
nil
nil
nil
2
5
4
4
4
4
4
4
4
nil
4
nil
4
nil
nil
3
nil
3
5
nil
44
nil
nil
nil
nil
4
nil
4
4
nil
4
4
4
nil
nil
nil
4
nil
nil
3
nil
3
5
nil
44
nil
nil
nil
nil
4
nil
4
4
nil
4
4
4
nil
nil
nil
4
nil
nil
3
nil
3
3
nil
nilnil
nil
nil
2
nil
3
3
3
4
3
3
3
3
nil
nil
nil
nil
nil
nil
3
nil
nil
3
nil
nilnil
nil
nil
nil
nil
nil
nil
3
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
3
nil
nil
3
nil
nilnil
nil
nil
nil
nil
nil
nil
3
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
4
3
4
5
4
34
3
nil
4
2
3
4
5
4
4
4
4
4
nil
4
4
4
3
5
5
4
4
5
4
45
4
nil
4
4
4
4
6
5
5
5
5
5
4
5
4
5
3
5
5
5
5
5
5
55
5
5
5
5
5
5
6
5/6
5
5/6
5/6
5/6
4
5/6
4
5
4
5/6
nil
nil
nil
nil
nil
nilnil
nil
nil
nil
nil
nil
nil
5
nil
6
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nilnil
nil
nil
nil
nil
nil
nil
5
nil
6
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nilnil
nil
nil
nil
nil
nil
nil
5
nil
6
nil
nil
nil
nil
nil
nil
nil
nil
nil
6
6
6
nil
6
66
6
nil
6
5
6
6
6
6
nil
6
6
6
6
6
6
6
6
6
6
6
6
nil
6
66
6
nil
6
6
6
6
6
6
nil
6
6
6
6
6
6
6
6
6
6
6
6
nil
6
66
6
nil
6
6
6
6
6
6
nil
6
6
6
6
6
6
6
6
6
nil
nil
nil
nil
nil
nilnil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nilnil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nilnil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil4
nil
nil
nil
4/5
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
South Metropolitan North Metropolitan Statewide
incl sleep unit incl sleep unit incl sleep unit
sameday
Fiona StanleyHospital Fremantle Rockingham Bentley Armadale SCGH RPH
RPH ShentonPark Campus Swan Osborne Park Kalamunda Joondalup KEMH PMH Graylands
Fiona Stanley Hospital includes Murdoch Hospice. SCGH includes Cottage and Hollywood Hospice publicly contracted beds
Current year: dialysis services at Fremantle Hospitalincludes Melville Satellite Centre and Swan Hospital includes Midland Satellite CentreFuture years: dialysis services at Fiona Stanley Hospital includes Melville Satellite Centre, Bentley Hospital includes Cannington Satellite Centre, Osborne Park Hospital includes Stirling Satellite Centre, and Swan Hospital includes Midland Satellite Centre
Medical Services
Surgical Services
Emergency/Trauma Services
Currently nil emergency medicine consultant on duty 24 hours per day
heart Tx
sameday
sameday
kidney Tx
thoracicheart, lung Tx
kidney Txkidney, liver Tx
sameday
samedaykidney Tx
heart, lung Tx
sameday
sameday
sameday
11a

METROPOLITAN CLINICAL SERVICES FRAMEWORK
Fiona StanleyHospital Fremantle Rockingham Bentley Armadale SCGH RPH
RPH ShentonPark Campus Swan Osborne Park Kalamunda Joondalup KEMH PMH Graylands
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
Obstetrics
Paediatrics
Neonatology
Rehabilitation
Community assessment
Environmental HealthCommunicable Disease Control Child and Community Health Aboriginal HealthHealthPromotionBreastscreen
Cervical
Genomics
GP based communitynursing
Surgical
Medical
Rehabilitation
Continuing care
Paediatrics
Obstetrics
5
4/5
5
6
5
55
5
5
3
5
3
3
3
6
4/5
6
6
5/6
5
5
5
5
4/5
5
6
5
55
5
5
3
5
3
3
3
6
4/5
6
6
5/6
5
5
5
4
4
3
6
5
45
4
5
2
5
3
3
3
4
4
nil
nil
nil
5
5
nil1
1
4
3
3
3
3
3
5
nil4
4
5
6
nil
nil
nil
nil
nil
5
5
nil1
1
4
3
3
3
3
3
5
3
4
4
5
6
nil
nil
4
3
3
3
5
41
1
4
2
3
3
3
3
4
4
4
3
5
5
41
1
4
2
3
3
3
3
5
2
5
5
4/5
5
4
4
4
4
3
5
5
45
4
1
1
4
2
3
3
3
3
3
5
5
5
5
4/5
5
4
4
4
2
3
5
5
31
1
4
2
3
3
3
3
nil4
nil
nil
nil
5
5
nil1
1
4
2
3
3
3
3
4
nil
nil
4
5
6
nil
nil
nil
nil
nil
5
5
nil1
1
4
2
3
3
3
3
5
nil
4
5
6
nil
nil
4
3
3
5
5
41
1
4
2
3
2
3
3
4
3
4
4
3
5
5
41
2
4
3
3
2
3
3
4
4
5
5
4/5
5
4
4
4
4
3
5
5
441
2
4
3
3
2
3
3
45
4
35
5
4/5
5
4
4
nil
nil
nil
6
5
nil5
4
5
5
5
5
5
3
5
nil
nil
nil
nil
6
5
nil5
5
5
5
5
5
5
3
5
6
6
6
5
nil
nil
nil
nil
nil
6
5
nil5
5
5
5
5
5
5
3
6
nil
6
6
6
5
nil
nil
nil
nil
nil
6
5
nil5
4
5
5
5
5
5
3
5
nil
nil
nil
nil
nil
nil
nilnil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
5
nil
nil
nil
nil
nil
nil
nil
nil
nilnil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
6
nil
nilnil
nil
nil
nil
nil
nil
nil
nil
nil
5
nil
5
nil
nil
nil
nil
nil
nil
6
nil
nilnil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
5
nil
nil
nil
nil
nil
nil
nil
nil
nilnil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
4
3
3
5
5
41
1
4
2
3
3
3
3
4
4
4
4
5
5
41
1
4
2
3
3
3
3
5
5
5
4/5
5
4
4
4
4
4
5
5
41
1
4
2
3
3
3
3
55
45
5
4/5
5
4
4
4/5
3
3
5
5
45
4
4
2
5
3
3
3
nil4
4/5
nil
nil
nil
5
5
nil1
1
4
2
3
3
3
3
5
4
4
5
6
nil
nil
nil
nil
nil
5
5
nil1
1
4
2
3
3
3
3
5
4
4
5
6
nil
nil
3
1
3
3
5
31
1
4
2
3
3
3
3
nil3
3
nil
nil
nil
3
5
nil1
1
4
2
3
3
3
3
nil3
nil3
3
1
2
nil
nil
nil
nil
nil
3
5
nil1
1
4
2
3
3
3
3
3
3
3
1
2
nil
nil
4
4
4
5
4
41
1
4
2
3
3
3
3
4
5
4/5
5
5
4
51
1
4
3
3
3
3
3
5
5
5
4/5
5
4/5
5
5
4/5
5
5/6
4
51
1
4
3
3
3
3
3
5/65
55/6
5/6
5
5
4/5
5
6
nil
6
nil
1
61
1
4
2
3
nil
3
3
n/a
6
nil
6
nil
1
61
1
4
3
3
nil
3
3
n/a
nil
5
5
nil
nil
nil
6
6
nil
6
nil
1
61
1
4
3
3
nil
3
3
n/a
5
5
nil
nil
nil
6
nil
6
6
5
1
nil1
1
4
2
3
nil
nil
3
n/a
nil
6
6
5
1
nil1
1
4
3
3
nil
nil
3
n/a
6
6
6
nil
6
nil
nil
6
6
5
1
nil1
1
4
3
3
nil
nil
3
n/a
6
6
6
nil
6
nil
nil
nil
nil
1
1
nil1
nil
nil
2
nil
nil
3
3
niln/a
nil
nil
nil
nil
1
nil1
1
nil
nil
3
nil
nil
3
3
n/a
nil
nil
nil
nil
nil
nil
nil
nil
nil
1
1
nil1
nil
nil
3
nil
nil
3
3
n/a
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
5
nil1
nil
nil
2
nil
nil
3
3
5
Primary Care Services
Ambulatory Care Services
Prevention and Promotion Services
Rehabilitation Services
North Metropolitan StatewideSouth Metropolitan
Defined as outpatient services and community based and home care provided within the catchment area of each facility.
Current year Ambulatory Care Services are undefined. Mental Health Ambulatory Care Services are covered under Mental Health Services
State Rehab Centre
Obstetrics Services
Paediatrics Services
KEMH & PMH deliver a combined neonatal service
Level 1 SCNL1 SCNLevel 1 SCNL1 SCNLevel 2B SCN
3 Nursery
Level 3 SCNLevel 3 SCNLevel 2B SCNL1 SCNL1 SCNL1 SCN
Continuing Care Services
11b

METROPOLITAN CLINICAL SERVICES FRAMEWORK
Fiona StanleyHospital Fremantle Rockingham Bentley Armadale SCGH RPH
RPH ShentonPark Campus Swan Osborne Park Kalamunda Joondalup KEMH PMH Graylands
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
Mental health promotion andillness preventionEmergency services(hospital based) Inpatient servicesCommunity clinical based servicesDay therapy services(hospital based) Community non clinical support programsIntermediate care
Mental health promotion and illness preventionEmergency services (hospital based) Inpatient servicesCommunity clinical based servicesDay therapyservices(hospital based)Community non clinical support programsIntermediate care
Mental health promotion andillness preventionEmergency services(hospital based) Inpatient servicesCommunity clinical based servicesDay therapy services(hospital based) Community non clinical support programsIntermediate care
Forensic
Maternal
Neurological
Alcohol and DrugOther- Eating disorders
6
6
nil
nil
nil
3
nil
36
6
6
5
6
nil
4
6
6
5
5
6
nil
nil
3
nil
nil
nil
nil
nil
6
6
nil
nil
nil
3
nil
3
6
6
6
5
6
nil
4
6
6
5
5
6
nil
nil
3
nil
nil
nil
nil
nil
3
5
nil
5
nil
2
nil
55
5
5
5
5
5
nil
nil
3
5
5
5
nil
4
5
nil
nil
nil
nil
nil
6
6
nil
6
nil
4
nil
46
5
5
5
5
5
4
6
5
5
5
5
5
4
4
nil
nil
nil
nil
nil
6
6
nil
6
nil
4
nil
46
5
5
5
5
5
4
6
5
5
5
5
5
4
46nil
nil
nil
nil
nil
nil
3
nil
5
nil
2
nil
3
5
3
nil
5
nil
3
nil
nil
3
nil
5
nil
nil
4
3
5nil
nil
nil
nil
nil
6
5
nil
5
nil
3
nil
3
6
5
5
5
5
6
4
6
5
5
5
5
5
5
3
6nil
nil
nil
nil
nil
56
5
nil
5
nil
3
nil
3
6
5
5
5
5
6
4
6
5
5
5
5
5
5
3
6nil
nil
nil
nil
nil
5
nil
6
6
6
2
6
35
5
5
5
5
3
nil
nil
3
5
5
6
nil
4
35nil
nil
nil
nil
nil
6
nil
6
6
6
3
6
3
6
5
5
5
5
6
6
6
5
5
5
6
5
6
3
6nil
nil
nil
nil
nil
6
nil
6
6
6
3
6
3
6
5
5
5
5
6
6
6
5
5
5
6
5
6
6nil
nil
nil
nil
nil
nil
nil
3
nil
5
nil
2
nil
3
5
4
5
5
5
3
nil
nil
3
5
5
5
nil
4
3
5nil
nil
nil
nil
nil
6
nil
nil
5
nil
3
4
3
6
5
5
5
5
5
5
6
5
5
5
5
5
4
3
6nil
nil
nil
nil
nil
6
nil
nil
5
nil
3
4
2
6
5
5
5
5
5
5
6
5
5
5
5
5
4
2
6nil
nil
nil
nil
nil
nil
5
nil
5
nil
2
nil
5
5
5
5
5
5
5
nil
nil
3
nil
5
nil
nil
nil
5
5nil
nil
nil
nil
6
6
6
nil
nil
nil
3
nil
5
6
6
6
5
6
6
4
6
6
6
5
6
5
nil
5
6nil
nil
6
6
6
6
6
nil
nil
nil
3
nil
56
6
6
5
6
6
4
6
6
6
5
6
5
nil
56nil
nil
6
6
6
nil
5
nil
5
nil
2
nil
55
5
5
5
5
5
nil
nil
3
nil
5
nil
nil
nil
55nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nilnil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nilnil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nilnil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nilnil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nilnil
nil
nil
nil
nil
3
3
nil
5
nil
2
nil
5
4
5
5
5
5
nil
nil
3
5
5
5
nil
4
5nil
nil
nil
nil
nil
6
5
nil
5
nil
3
nil
36
5
5
5
5
6
4
6
5
5
5
5
5
4
36nil
nil
nil
nil
nil
6
5
nil
5
nil
3
nil
3
6
5
5
5
5
6
4
6
5
5
5
5
5
4
3
6nil
nil
nil
nil
nil
5
nil
nil
5
nil
2
nil
5
nil
nil
5
nil
3
nil
nil
3
5
5
5
nil
4
5nil
nil
nil
nil
nil
6
nil
nil
5
nil
3
nil
3
6
5
5
5
5
6
5
6
5
5
5
5
5
6
3
6nil
nil
nil
nil
nil
6
nil
nil
5
nil
3
nil
3
6
5
5
5
5
6
5
6
5
5
5
5
5
6
3
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
2
nil
3nil
nil
nil
2
nil
3
nil
nil
3
nil
2
nil
nil
3
3nilnil
nil
nil
nil
nil
6
nil
nil
nil
nil
3
nil
3
6
nil
nil
2
nil
4
3
6
3
nil
2
nil
5
3
3
6nil
nil
nil
nil
nil
6
nil
nil
nil
nil
3
nil
3
6
nil
nil
2
nil
4
3
6
3
nil
2
nil
5
3
3
6nil
nil
nil
nil
nil
nil
5
nil
5
nil
2
nil
3
5
4
5
5
5
3
nil
nil
3
nil
5
nil
nil
4
3
5nil
nil
nil
nil
nil
6
6
6
6
5
3
6
3
6
6
5
5
5
6
6
6
6
5
5
5
5
4
3
6nil
nil
nil
nil
nil
6
6
6
6
5
3
6
3
6
6
5
5
5
6
6
6
6
5
5
5
5
4
3
nil
nil
nil
nil
nil
nil
3
nil
nil
nil
nil
nil
3
5
4
5
nil
5
nil
nil
nil
nil
nil
nil
nil
nil
nil
3
5nil
5
nil
nil
nil
6
3
nil
nil
nil
nil
nil
nil6
5
6
4
6
nil
4
nil
nil
nil
nil
nil
nil
nil
nil6nil
6
nil
nil
nil
6
3
nil
nil
nil
nil
nil
nil6
5
6
4
6
nil
4
nil
nil
nil
nil
nil
nil
nil
nil6nil
6
nil
nil
nil
5
4
6
4
5
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
6
6
5
6
6
6
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
6
6
5
6
6
6
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
6
nil
nil
nil
nil
nil
nil
nil
nil
6
6
nil
6
nil
nil
nil
nil
6
6
5
nil
4
nil
6
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
6
6
6
nil
6
nil
6
6
nil
6
6
6
nil
4
nil
6
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
6
6
6
nil
6
nil
6
6
nil
6
6
6
nil
4
nil
6
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
nil
5
nil
nil
nil
nil
nil
nil
nil
nil
Adult Mental Health Services
Child and Adolescents Mental Health Services
North Metropolitan StatewideSouth Metropolitan
Prevention promotion levels can not be considered as a continuum. Eg. Level 6 designation does not assume level 1- 5 are included in the level 6 coding.
Statewide Mental Health Services
Older Persons Mental Health Services
11c

METROPOLITAN CLINICAL SERVICES FRAMEWORK
Fiona StanleyHospital Fremantle Rockingham Bentley Armadale SCGH RPH
RPH ShentonPark Campus Swan Osborne Park Kalamunda Joondalup KEMH PMH Graylands
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
2004
/05
2010
/11
2015
/16
Pathology
Radiology
Pharmacy
ICU/HDU
Paediatric ICU
CCU
Anaesthetics
Operating theatresTraining and research
Geographical Catchment Population
- Medical/Surgical
- Obstetrics
- Paediatrics
- Same Day
- HDU/CCU/ICU
- ESSU
- Rehabilitation
- Mental Health
- Other
Total
6
6
6
6
nil
6
6
6
6
3352518355012424845610
6
6
6
6
nil
6
6
6
6
ni
57427187080161475670
1058
3
3
4
nil
nil
nil
3
4
4
950020100386623
252
3
3
4
nil
nil
nil
3
4
4
60003000386623217
3
4
4
nil
nil
nil
3
3
3
85
4
5
4
4
nil
4
4
4/5
4
10020821106244010239
54
5
4
4
nil
4
4
4/5
4
11520931158405018306
3
3/4
4
nil
nil
nil
4
4
4
235
3
3
4
nil
nil
nil
1
2
4
00010006311112196
3
3
4
nil
nil
nil
1
2
4
00010006311116200
3
5
4
nil
nil
nil
3
4
4
207
4
5
4
4
nil
4
4
4/5
4
94231031108404315274
4
5
4
4
nil
4
4
4/5
4
94231033108404315276
6
6
6
6
nil
6
6
6
6
645
6
6
6
6
nil
6
6
6
6
70500877020303638986
6
6
6
6
nil
6
6
6
6
70500877020309242
1046
6
6
6
6
nil
6
6
6
6
708
nil
nil
nil
nil
nil
nil
nil
nil
nil
00000024122864
nil
nil
nil
nil
nil
nil
nil
nil
nil
00000024123672
4
5
4
4
nil
nil
4
5
5
236
nil
nil
nil
nil
nil
nil
nil
nil
nil
000050
105012122
nil
nil
nil
nil
nil
nil
nil
nil
nil
0000000000
4
4/5
4
nil
nil
nil
3
4
4
206
4
5
4
4
nil
4
4
4/5
4
120251025158485124326
4
5
4
4
nil
4
4
4/5
4
120251025158485132334
3
3/4
4
nil
nil
nil
4
4
4
209
3
3/4
4
nil
nil
nil
4
4
4
60002400892516214
3
3/4
4
nil
nil
nil
4
4
4
60003000897420273
3
3
3
nil
nil
nil
3
3
3
71
2
2/3
3
nil
nil
nil
3
3
3
3300170000050
2
2/3
3
nil
nil
nil
3
3
3
3300170000050
4
5
4
4
nil
4
4
4
4
235
4
5
5
4
nil
4
4
4
4
2403019402510405634494
5/6
5/6
5/6
5/6
nil
5/6
5/6
5/6
5/6
3003019553016646247623
6
5
5
3
nil
nil
6
5
5
276
6
5
5
3
nil
nil
6
5
5
2092212500890229
6
5
5
3
nil
nil
6
5
5
2075212500890212
6
6
6
nil
6
6
6
6
6
256
6
6
6
nil
6
6
6
6
6
00
176291070826256
6
6
6
nil
6
6
6
6
6
00
11220660826178
2
nil
6
nil
nil
nil
nil
nil
4
263
2
nil
6
nil
nil
nil
nil
nil
4
0000000
2100
210
2
nil
6
nil
nil
nil
nil
nil
4
0000000
1360
136
6
nil
nil
nil
nil
nil
nil
nil
nil
11
6
6
6
6
nil
6
6
6
6
541
Clinical Support Services
North Metropolitan StatewideSouth Metropolitan
Population
Bed Capacity
2299
07
2479
87
2698
32
5037
7
5266
5
5368
9
1157
39
1406
12
1634
09
1135
10
1191
66
1246
55
1031
06
1141
22
1341
69
2225
35
2276
47
2338
23
1811
92
2176
33
2469
73
2220
19
2288
30
2377
42
4171
8
4194
1
4522
9
2050
31
2527
92
3069
95
NOTE: Bed numbers outlined in this document are indicative numbers only and will be subject to review as the implementation of the framework progresses. Bed numbers indicate hospital capacity.SCGH/RPH includes 12 public mental health beds and 24 public restorative beds provided under contract by Mercy Hospital as well as 18 public palliative care beds provided under contract by Cottage Hospice (14) and Hollywood Hospital (4). The FSH bed numbers include 11 public palliative care beds provide under contract by Murdoch Hospice. Fremantle Hospital beds include 11 public dialysis chairs provided at the Melville Dialysis Unit.Swan District bed numbers include the 12 dialysis chairs at the Midland dialysis unit. In future years, Osborne Park and Bentley catchment areas will provide dialysis services, however, these will not be located on the hospital sites. 'Other' bed numbers refers to dialysis, neonatal and palliative care.
11d

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
2.2.2 Country and South West Area Clinical Services Role DelineationClinical services within the WA Country Health Service and the South West Area Health Serviceswill be guided by the CSF and configured according to the Area Health Service plans as outlined in2.4 of this framework.
As per the Reid report, more formal links will be developed between country and metropolitanArea Health Services which will ensure regional patients have timely access to tertiary healthcare and up to date professional expertise. Such links, along with other strategies such asworkforce, education/training and information management and communication technology willbenefit metropolitan and country health systems and patients.
2.3 Metropolitan Bed StrategyThe complex demand modelling information, which underpins the CSF, has provided a vital dataplatform that will be used to inform the distribution, capacity and provision of health careservices over time, including the number of inpatient and same day beds required within thehealth care system.
Demand modelling is a dynamic process used in a progressive manner in response to changeswithin the system—including the impact of health care reforms within the Reid reportrecommendations, new technology, actual population growth and service activity trends—toensure health planning and decision making is based on the most advanced information.
Using the data provided by the demand modeling exercise, a comprehensive plan was developedfor the transition from the current metropolitan hospital configuration (including number of bedsand infrastructure capacity) to the long-term requirements. This information will be used toinform the Infrastructure Development Plan (see 3.3).
The following table provides an overview of the current and projected bed capacity required tomeet future health care needs as defined through this process. The numbers provided are inreference to the provision of physical beds and hospital capacity. Please note this is a relativelydynamic model. Future detailed facility design and planning may alter the final size of thedevelopments.
13
clinicalframeworknew spread 21/9/05 3:14 PM Page 15

* Palliative care beds provided under contract by Murdoch Hospice beds
It is important to note that opportunity for revision of bed distribution within Area HealthServices will be structured into the implementation process as information is updated, refinedand the effects of the reform process are evidenced. In addition each key component of the CSFwill require detailed and comprehensive business case development and approval. This mayresult in alteration to the scale and scope of some aspects of the associated capital worksprogram.
It is not possible at this stage of planning to specify the exact numbers of beds required by sub-specialties such as cardiology or orthopaedics. This work will be undertaken in the planning forspecific sites, the ongoing work on models of care and the pragmatic approach which facilitydesign and costing will require. An overview of major groups is included in the Role DelineationMatrix.
More specific information regarding bed configuration beyond the major specialty groups will bedefined during the implementation of the CSF.
14
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
Metropolitan HospitalsCurrent(April) 2010/2011 2015/2016
Fiona Stanley Fremantle (incl Woodside)Rockingham Bentley ArmadaleCentral Tertiary(SCGH/RPH) Shenton ParkSwan DistrictOsborne ParkKalamundaJoondalupKEMHPMHGraylands
TOTAL
11*54185
235207
135323620620971
235276256263
4,184
610252239196274
1,05012232621450
494229256210
4,522
1,058217306200276
1,1180
33427350
623212178136
4,981
Projected Hospital Capacity
clinicalframeworknew spread 21/9/05 3:14 PM Page 16

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
2.4 Vision for Area Health Services● The health system now operates within an Area health model divided to reflect the growth in
population and expansion of services and infrastructure:
● North Metropolitan Area Health Service (NMAHS)
● South Metropolitan Area Health Service (SMAHS)
● Women’s and Children’s Health Service (WCHS)
● WA Country Health Service (WACHS)
● South West Area Health Service (SWAHS)
A continuum of care is offered within each Area Health Service from the primary care sector,where the first point of contact for many is a local general practitioner, pharmacist or communityhealth nurse, through to the secondary level care, provided by a local general or regionalhospital, and then, for some, specialty clinical services, provided by a tertiary care hospital. Thehealth system aims to provide the most appropriate and safe health care to the community in themost appropriate setting and in many cases this is not inside a hospital.
15
North
South
TERTIARY HOSPITALS
SPECIALIST HOSPITALS
GENERAL HOSPITALS
OTHER HOSPITALS
NMAHS & SMAHS Configuration
Bentley
Joondalup Health Campus
Swan DistrictsOsborne Park
Kalamunda
Armadale-Kelmscott District
Rockingham-KwinanaDistrict
Peel Health Campus
Murray District
GraylandsSCGH
Fiona Stanley HospitalFremantle
clinicalframeworknew spread 21/9/05 3:14 PM Page 17

2.4.1 North Metropolitan Area Health ServiceThe population residing north of the Swan River is now part of the North Metropolitan Area HealthService (NMAHS).
The NMAHS will consolidate its service delivery and be able to dedicate resources to thepopulation in the northern corridor following considerable development of services planned forthe south metropolitan area. Those in communities residing in the very far north of themetropolitan area have had to travel significant distances to access many health services. Thereconfiguration of the NMAHS will improve access and reduce the distance travelled for services.
Outside of the public hospital facilities across the NMAHS are a range of health care services thatsupport and complement a continuum of care for patients, such as population health preventionand promotion programs, and ambulatory care services as part of Healthy@Home. Improvementsand expansion in service delivery in order to reduce the pressures on the tertiary hospital systemand allow patients to receive the best possible care in the most appropriate setting close to theircommunity is underway. Underpinning this will be the strengthening of prevention and promotionactivities to reduce trends of chronic disease and reduce the numbers of people entering thehospital system.
The reconfiguration and planning of health services in the NMAHS is based on the projectedburden of disease for the future. Mental health, aged care and rehabilitation services will bestrengthened as specialised services in response to predicted increased need.
The roles and functions of each of the major public health care centres in the NMAHS will changeto ensure an appropriate range of clinical services is provided to the population within this Area.This is shown in the following table.
16
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
clinicalframeworknew spread 21/9/05 3:14 PM Page 18

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
Note: For detailed information regarding role and provision of clinical services please refer to theMetropolitan Clinical Services Role Delineation Framework at 2.2.1.
Overall, bed capacity itself will remain at a relatively constant level compared with currentfigures. In the long term there will be a slight increase in bed capacity to reflect growth inpopulation in the northern suburbs. The increase in bed capacity will not be as dramatic as thatplanned for the SMAHS. Historically, there has been a bed shortage in the south, with the northbridging the gap in services.
17
Health CareFacility
Current Role2005
Future Role2010-2015
Sir CharlesGairdnerHospital
Royal PerthHospital
JoondalupHealth Campus
KalamundaHospital
Osborne ParkHospital
Swan DistrictHospital
GraylandsHospital
RPH ShentonPark Campus
Tertiary Care
Tertiary Care
Secondary Care
Secondary Care
Secondary Care
Secondary Care
Specialist Care
RehabilitationCentre
Central tertiary hospital with significant growth and developmentplanned. Service directions to include development of the State CancerCentre, State Neurosciences Centre.
Tertiary and some secondary services to be relocated to FSH by2011. Some services will move to SCGH and northern generalhospitals. Princess Margaret Hospital to be relocated to the North Block,Wellington Street by 2015.
Significant development to become one of four metropolitangeneral hospitals. Medium term plan for Joondalup to become a second tertiaryhospital for the NMAHS and the development of a major privatehospital including mental health.
Role to change with focus on primary care, aged care and subacute care. Maternity services will be relocated whenappropriate facilities are available at general hospitals.
Role to change to a specialist hospital with focus on aged care,mental health and rehabilitation, planned overnight and samedaysurgery.
Significant development to become one of four metropolitangeneral hospitals providing increased capacity and servicecomplexity, increasing access to health care services in theeastern metropolitan region.
Continued role as specialist hospital, providing tertiary levelacute mental health services for the State.
Campus will close by 2016 with services relocated as alternativecare is available at appropriate sites. Tertiary rehabilitationservices will be relocated to a State Rehabilitation Centre atMurdoch.
clinicalframeworknew spread 21/9/05 3:14 PM Page 19

With the increased capacity in the south, the north will now be able to provide dedicatedservices to the NMAHS, thus increases will be moderate. Services outside of hospital facilities suchas hospital in the home and other ambulatory care programs will be strengthened to improveaccess and the range of health services offered to the community in the northern corridor anddecrease demand on inpatient care.
On the Joondalup Campus it is planned to have a private hospital facility guild by the privateoperator to complement the existing services (approximately 150-200 beds).
* Includes palliative care beds provided under contract by Hollywood and Cottage Hospices. Also includesrestorative and mental health beds provided under contract by Mercy Hospital.
2.4.2 South Metropolitan Area Health ServiceThe population residing south of the Swan River is now part of the South Metropolitan Area HealthService (SMAHS).
Significant development of health services will occur in the SMAHS in response to the needs of thepopulation and will include the commissioning of a new public tertiary hospital at Murdoch.
Planning for this exciting new development will commence in the short term and will beconducted as a collaborative initiative between the tertiary hospitals of Fremantle and RoyalPerth. The planning process will seek the contribution and participation of all stakeholders toensure the establishment of a new health care service of the highest quality.
As in the north, a range of health care services that support and complement a continuum of carefor patients will be enhanced outside of hospital-based services such as population healthprevention and promotion programs and ambulatory care services. Mental health, aged care andrehabilitation services will be strengthened as specialised facilities in response to the predictedincrease in demand.
18
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
2015/162010/112005Facility
Bed Provision Strategy
Central Tertiary Hospital (SCGH & RPH) Royal Perth Rehabilitation Hospital (Shenton Park) Joondalup HospitalKalamunda HospitalSwan District HospitalOsborne Park HospitalGraylands Hospital
Total
135323623571
206209263
2573
105012249450
326214210
2466
11180
62350
334273136
2534
clinicalframeworknew spread 21/9/05 3:14 PM Page 20

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
The roles and functions of facilities located in the SMAHS will be reconfigured as follows:
Note: For detailed information regarding role and provision of clinical services please refer to theMetropolitan Clinical Services Role Delineation Framework at 2.2.1.
Overall, bed capacity will increase in the SMAHS as some services are relocated and capacity isincreased. Existing secondary hospitals in the southern corridor such as Rockingham/KwinanaDistrict Hospital and Armadale/Kelmscott Memorial Hospital will have their capacity increasedand become two of the four General Hospitals in the metropolitan area.
Expressions of interest have been called for a potential private hospital collocation on theRockingham site.
19
Health CareFacility
Current Role2005
Future Role2010-2015
Fiona StanleyHospital
FremantleHospital(includingKaleeyaHospital)
WoodsideHospital
RockinghamKwinanaHospital
Bentley Hospital
Peel HealthCampus
ArmadaleKelmscottHospital
Tertiary Care
Tertiary Care
Maternity Care
Secondary Care
Secondary Care
Secondary Care
Secondary Care
New tertiary hospital to be developed at Murdoch by 2011.Service directions will include a State Trauma and Burns Centre,State Rehabilitation Centre, Heart/Lung Transplantation Services,Comprehensive Cancer Centre.
Role to change to specialist hospital with focus on rehabilitation,aged care and mental health services. All tertiary services to berelocated to the Fiona Stanley Hospital by 2011. Someambulatory/elective surgical services will be retained.
To be closed when appropriate alternative services are availablewithin the SMAHS.
Significant development to become one of four metropolitangeneral hospitals providing comprehensive range of core clinicalservices to its catchment in the SMAHS.
Role to change to become a specialist hospital with focus onaged care, rehabilitation and mental health services. Same dayelective surgery be maintained and ambulatory care services willbe enhanced.
Whilst not included in the metropolitan clinical servicesframework, Peel Health Campus will continue its role within theSMAHS in providing health care services appropriate to the localcatchment area. A separate Peel Clinical Services Framework isbeing developed.
Significant development to become one of four metropolitanGeneral Hospitals providing comprehensive range of core clinicalservices to its catchment in the SMAHS.

* Palliative care beds provided under contract by Murdoch Hospice beds
2.4.3 Women’s and Children’s Health ServiceThe Women’s and Children’s Health Service is a statewide service. Major services assigned toWCHS include:
● Princess Margaret Hospital (PMH)
● King Edward Memorial Hospital (KEMH)
● Child and Youth Health Clinical Network
● Women’s Health Clinical Network including maternal health.
The role and function of KEMH and PMH will continue at a tertiary level. Reconfiguration ofservices in the NMAHS and SMAHS will support and complement these existing statewide servicesby increasing the provision of women’s and children’s services in general hospitals closer to wherethe community lives.
A range of health care services support and complement the continuum of care for women andchildren, such as population health prevention and promotion programs and ambulatory careservices. Improvements and expansion in service delivery in order to reduce the pressures on thetertiary hospital system and allow patients to receive the best possible care in the mostappropriate setting close to their community is underway.
20
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
2015/162010/112005Facility
Bed Provision Strategy
Fiona Stanley HospitalFremantle HospitalWoodside Maternity Hospital Rockingham/Kwinana District HospitalBentley HospitalArmadale Kelmscott Memorial Hospital
Total
11*5043785
235207
1079
610252
0239196274
1571
1058217
0306200276
2057
2015/162010/112005(April)Facility
Bed Provision Strategy
Princess Margaret Hospital
King Edward Memorial Hospital
256
276
256
229
178
212
clinicalframeworknew spread 21/9/05 3:14 PM Page 22

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
Significant resources and effort have gone into re-establishing the reputation and physicalfacilities at King Edward Memorial Hospital. In the past 2 years over $25m has been spent on arange of capital works including the development of a Maternal Foetal Monitoring Centre and anupgrade of the delivery suite, emergency department and acute high dependency unit.
Long-term solutions are required for a range of issues identified at the KEMH and PMH facilitieswhich impact upon their effectiveness and efficiency.
Some of the issues identified are:
● constrained sites
● continuity of care
● isolation of some gynaecological services from other adult services
● ability to maintain high levels of clinical care, equipment, services and infrastructure onisolated sites
● difficulty in alignment of clinical quality and governance processes across distinct sites
● ability to maintain adequate maternity service provision on large number of sites given thelong-term issue of attraction and retention of suitably experienced workforce.
It is acknowledged that co-location of the hospitals within the Women’s and Children’s HealthServices at a tertiary adult site would be the preferred solution to address the issues identified.However, after extensive consultation and deliberation it has been concluded that:
● PMH should be relocated to the vacated Wellington Street Campus (North Block) when RPHservices are relocated. Many of the difficulties of the current PMH site will be addressed bythe more modern infrastructure of the north block and the proximity to public transport andparking.
● The Institute for Child Health Research should be relocated to the RPH site in close proximityto the Paediatric Hospital.
● King Edward Memorial Hospital should be relocated to a new site. Three options will bemaintained at the FSH, SCGH and a site to the west of the existing North Block at RPH, with afinal decision to be made closer to a move date. A ‘footprint’ for KEMH will be included inplanning for the development of all sites, retaining an option for the most appropriaterelocation when required.
● It is recognised that having diagnostic and adult high level support services co-located with thewomen’s tertiary service is a preferred option. If KEMH was to eventually locate at the RPHsite, it is possible that a private health provider might wish to collocate at this site, thusproviding adult tertiary support services and access to clinicians.
21
clinicalframeworknew spread 21/9/05 3:14 PM Page 23

Supporting the VisionThe WCHS will facilitate the enhanced coordination and support of women’s and children’s healthservice delivery to the state.
An important priority will be the articulation of a Maternal Services Framework, building uponsuccessful models of care already in place in WA, to help inform the planning of new andenhanced services within the metropolitan and country area health services. This will be donewith an aim to support and promote the practice of all members of the maternal care teamincluding obstetricians, GP obstetricians and midwives, ensuring that the community continues tohave choice in their preferred model of care.
Western Australia experiences a number of unique challenges in the provision of obstetric andmaternal care services due to our vast geography, population distribution and cultural diversity.As recommended in the Western Australian Statewide Obstetric Services Review 2002, laterendorsed by the Health Reform Committee in 2004 and as outlined in the Perinatal and InfantMortality Report 2001-02, a Statewide Obstetric Support Unit (SOSU) has been established underthe direction of the Women’s and Children’s Health Service.
The aim of the SOSU is to ensure the highest standard of maternity care is provided to thecommunity of Western Australia. To achieve this aim, the service will work collaboratively withina network of metropolitan and country maternity services to provide support and direction inareas such as development of policy and standards, clinical quality and safety activities,workforce support and professional advice.
2.4.4 WA Country Health ServiceThe WA Country Health Service has embarked upon the implementation of the recommendationsof the Country Health Services Review of 2003 (endorsed as part of the Reid report) that willguide the development of clinical services in regional areas.
The WA Country Health Service manages over 200 facilities, including 57 hospitals, 22 nursingposts and over 100 health centres, child, community and mental health facilities.
Regional Resource Centres, Integrated District Health Services and health services in smallertowns and communities form a regional network of health services across each region based on a‘hub and spoke’ concept.
The aim of building a regional network model across the WA Country Health Service is to:
● provide a guaranteed level of patient care in each hospital
● improve the patient care available within the region
● increase patient access to clinical services.
22
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
clinicalframeworknew spread 21/9/05 3:14 PM Page 24

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
Details on the level of service to be provided in each country hospital are included in Appendix 2.
Regional Resource CentresRegional Resource Centres will deliver as much acute care within regions as possible, limiting theneed for travel to Perth other than for services only available at major metropolitan hospitals.Regional Resource Centres will also provide patient services and other non-clinical supportservices to smaller health services within the region.
Regional Resource Centres are located in:
● Broome
● Port Hedland
● Geraldton
● Kalgoorlie
● Albany
● Bunbury
In the Wheatbelt, the dispersed population and close proximity to Perth suggest the developmentof four Integrated District Health Services rather than a single Regional Resource Centre. Adetailed plan for the unique hospital and health service system in the Wheatbelt region will beundertaken in 2005.
Integrated District Health Services Integrated District Health Services will provide a range of designated inpatient and primary careservices for the town and surrounding communities, supported by outreach services from theRegional Resource Centre. Services will include 24 hour emergency cover, the planned delivery oflow-risk births, and some low complexity surgery as well as diagnostic and primary healthservices.
Integrated District Health Servcies are located in:Esperance Katanning Moora NarroginMerredin Northam Carnarvon NewmanNickol Bay Derby Kununurra
Health Services in Small TownsHospital and health services in small towns will be flexible to accommodate changing healthneeds. The emphasis is on continued provision of 24 hour emergency treatment services, thecapacity for low level acute inpatient care, aged care and appropriate community-based services.
23
clinicalframeworknew spread 21/9/05 3:14 PM Page 25

Towns with such services include:Fitzroy Crossing, Halls Creek, Wyndham, Exmouth, Onslow, Paraburdoo, Wickham, Roebourne,Tom Price, Dongara, Kalbarri, Meekatharra, Morawa, Mullewa, North Midlands, Northampton,Laverton, Leonora, Norseman, Ravensthorpe, Beverley, Boddington, Bruce Rock, Corrigin,Cunderdin, Dalwallinu, Dumbleyung, Goomalling, Kellerberrin, Kondinin, Kununoppin, Lake Grace,Narembeen, Pingelly, Quairading, Southern Cross, Wagin, Wongan Hills, Wyalkatchem, York,Denmark, Gnowangerup, Kojonup, Plantagenet.
Health Services for small communities/settlementsSome small communities have difficulty in supporting resident general practitioner services.Where GPs cannot be attracted, the primary care needs of these small communities may be metthrough services staffed by resident nurse practitioners and supported by visiting generalpractitioners, community nurses and allied health staff.
Partner Metropolitan Health ServicesPartnerships between the country regions and metropolitan health services will provide supportfor country services including:
● visiting specialists/locum specialists/specialist rotations
● telehealth clinical consultations and support
● assistance with recruitment of specialists, doctors, nurses, allied health clinicians and jointappointments
● graduate medical, nursing and allied health rotations
● inservice education and training
● clinical advice and audit support.
Capital and InfrastructureA capital and infrastructure plan has been articulated to develop the capacity of our RegionalResource Centres and Integrated District Health Services, replace or upgrade small health serviceswhere necessary, improve staff and patient accommodation and medical transport services.
Priorities 2005-2010The priorities for the next five years are:
● establishing formal metro-country links
● building the clinical workforce in Regional Resource Centres
● developing the physical infrastructure and systems for regional health networks
● staff attraction and retention initiatives, especially improved staff housing
● better coordinated patient transport systems
● greater focus on aged care services.
24
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
clinicalframeworknew spread 21/9/05 3:14 PM Page 26

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
2.4.5 South West Area Health ServiceThe South West Area Health Services (SWAHS) has embarked on a strategic service planningprocess to ensure the systematic improvement of health care services in the region over time inalignment with the State Strategic Health Plan.
The SWAHS service planning will embody clinical services planning and includes a scope of analysisand planning which is broader than just clinical services. This approach by SWAHS seeks toachieve both the requirements of a clinical services plan with its focus on service settings and theten condition-based consumer centric programs that are the focus of service delivery in the SouthWest.
The South West Health Campus at Bunbury will be maintained as the key central hub for servicesin the south-west. This private-public collocation has been extremely successful.
25
Kimberley
Pilbara Gascoyne
Goldfields South East
MidwestMurchison
Wheatbelt
Great Southern
SouthWest
WA Country Health Service and South West Area Health Service Configuration
clinicalframeworknew spread 21/9/05 3:14 PM Page 27

2.5 Education and ResearchThe Western Australian health system has a distinguished role in undertaking cutting-edgeresearch which has benefited local, national and international patients. Similarly, there is astrong emphasis and long tradition in clinical education and training within our health caresystem.
The Department of Health is committed to the position of research within the system and tostrengthening opportunities for clinical research across all health settings, including hospital,community and ambulatory care. The newly established State Health Research Advisory Council(SHRAC) will have a pivotal role in providing leadership for the further development of health andmedical research, ensuring a coordinated approach to the planning, conduct of research andtranslation of research into policy and practice.
SHRAC will also provide advice on planning for development of facilities within current andproposed infrastructure developments, including Sir Charles Gairdner Hospital and the new FionaStanley Hospital and the expansion of research to be undertaken at the four general hospitals.Significant additional new research facilities will be established simultaneously with buildingdevelopment at FSH, SCGH and the newly located PMH.
The expanding role of health and medical research as outlined in the CSF is not confined to majorteaching hospitals – it goes beyond to general and specialist hospitals, where patients will havethe ability to participate in clinical research in hospitals that are closer to home and still benefitfrom the translation of research outcomes into policy and practice.
Teaching and training for medical, nursing and allied health students has traditionally beenthrough an apprenticeship model primarily based at our large metropolitan tertiary hospitals.After considering the medical workforce and the influx of additional medical graduates from2009, the Reid report recommended that new ways of undertaking medical training are needed.
Work has progressed to develop and implement new approaches to undergraduate andpostgraduate medical training, including:
● greater exposure to private and secondary hospitals where junior doctors have the opportunityto experience training in a variety of medical and surgical conditions
● increased training within the ambulatory care setting
● greater training in community settings.
Key stakeholders will be engaged, including clinicians, colleges and universities to discusssustainability of medical training into the future. A steering committee has been established toidentify strategies and to monitor risks, quality and timeliness of strategies for medical training.Issues already raised include the need to incorporate appropriate teaching facilities within thereconfiguration of our health system.
26
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
clinicalframeworknew spread 21/9/05 3:14 PM Page 28

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
There are a number of advantages to the ongoing commitment to research and training, includingthe improved quality of life and wellbeing for patients and the attraction and retention of staffinvolved in research and training.
2.6 Pathology Services WAAs recommended in the Reid report, a single pathology service has been established in WA withthe aim to providing service quality and economic benefits over time which will support theimplementation of the CSF.
Expected benefits include:
● improved demand management
● service rationalisation (adopting a system level approach to reducing costs by better matchingcapacity and demand, eliminating inappropriate duplication, and managing the developmentof specialist services)
● economies of scale in purchasing and procurement
● support for and expansion of teaching and research.
Further work will be done on the optimal facility deployment (eg centralised specialist laboratoryservices) in order to provide a comprehensive and world-class pathology service.
2.7 Mental Health The State’s mental health system has been under significant pressure for many years, andimproving mental health services for patients and health system staff is now a top priority.
$173.4 million in additional funding over the next three years has been allocated to enable theimplementation of comprehensive mental health reform initiatives.
This funding of a range of new initiatives and the expansion of existing mental health services willhave significant benefits to many individuals, carers and families in Western Australia who needsupport.
The Mental Health Strategy 2004-2007 (available at www.mental.health.wa.gov.au) outlines keyreforms needed to address the most pressing areas of need within the current mental healthsystem.
Specifically, the Mental Health Strategy 2004-2007 addresses the main areas of the health systemwhere targeted interventions have the capacity to immediately and significantly increase accessto mental health services and reduce demand on acute beds. The key areas are:
27
clinicalframeworknew spread 21/9/05 3:14 PM Page 29

1. Mental health emergency services
2. Adult inpatient services
3. Community mental health services (adult and young people)
4. Supported community accommodation
5. Workforce and safety initiatives
6. Promotion, prevention and early intervention
7. Specialist mental health services
8. Non-government mental health services
9. Improving mental health services
10. Primary mental health care
11. Increasing consumer and carer participation
The development of these individual strategies is the culmination of a significant amount ofconsultation involving consumers, carers, mental health professionals, governments and non-government mental health bodies and peak industry organisations.The Mental Health Advisory Group, made up of mental health specialists, is overseeing theimplementation of the Mental Health Strategy 2004-2007 and plays an integral role in thedevelopment and monitoring of activities.
In addition the Mental Health Action Plan 2005-2010 has been commenced to move improvementin mental health services including preventative strategies, forward as part of the StrategicHealth Plan (www.mental.health.wa.gov.au).
28
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
clinicalframeworknew spread 21/9/05 3:14 PM Page 30

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
3. Facilitating Change
A number of key support functions are critical to the successful implementation of the CSF, suchas governance and organisation structures, workforce, infrastructure, finance, informationmanagement and communication technology. Development of these support functions will takeplace over a long-term period. However, an overview of the direction for each function isincluded here.
3.1 Governance and Organisational StructureA number of key organisational changes as recommended by the HRC will serve to support theimplementation of the CSF and ensure accountability for the successful achievement of keyreform outcomes. The changes include:
● continuing the focus on reform though the Health Reform Implementation Taskforce in closeconnection with the Office of the Director General
● strengthening the Area Health Services Model
● refocussing the Department of Health’s functions towards a clearer role in supporting healthservices and reporting and evaluating health system performance for the Government
● strengthening the focus on health outcomes through the implementation of a policy frameworkfor health in Western Australia - the Health Policy and Clinical Reform Division will beresponsible for establishing statewide clinical networks within programs pertaining to long-established groups of conditions. This Division will bring together stakeholders in the public,private, non-government and academic sectors as well as consumers and carers to oversee thedevelopment of priorities that are underpinned by epidemiology, policy and protocols,planning, and performance targets for their respective clinical program areas
● establishment of the State Women’s and Children’s Health Service combining the formerWomen’s and Children’s Health and the Child and Community Health Directorate of theDepartment of Health
● Development and implementation of an improved Statewide Clinical Governance frameworkbuilt on the four pillars of clinical audit, clinical risk, consumer values and professionaldevelopment and management led by the Office of Safety and Quality in Health Care.
29
clinicalframeworknew spread 21/9/05 3:14 PM Page 31

30
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
HEALTH POLICY &CLINICAL REFORM*
INFRASTRUCTURE*
SYSTEM EFFICIENCY*
HEALTH SYSTEMSUPPORT
STATUTORYOFFICERS
SOUTHMETROPOLITANAREA HEALTH
SERVICE
NORTHMETROPOLITANAREA HEALTH
SERVICE
WA COUNTRYHEALTH SERVICE
SOUTH WEST AREAHEALTH SERVICE
WOMEN’S ANDCHILDREN’S HEALTH
SERVICE
INTERNALAUDIT/CORPORATE
GOVERNANCE*
OFFICE OF THEDIRECTOR GENERAL*
Public Relations & MarketingFederal AffairsMinisterial & Parliamentary LiasonSystem Policy
HEALTH FINANCE
DIRECTOR GENERAL*
HEALTH OPERATIONSHEALTH SYSTEM SUPPORT
HEALTH REFORM
Health Corporate NetworkPathologyDentalClinical Technology (Biomedical Eng)Drug & Alcohol Office
WA Organisational Chart
* Includes members of the Health Reform Implementation Taskforce
3.2 Strategic Workforce FrameworkThe changes planned within the health system will have significant implications for ourworkforce. Long term strategic planning is required to ensure we have the capacity to deliver theservices that will be required to meet the health care needs of our population into the future.
A forecast of the nature and scale of future health workforce defined by the CSF across each ofthe metropolitan health sites and clinical specialties has been developed.
Projections have been made based on quantitative and qualitative knowledge of health workforcepatterns and trends along with demand elements such as projected bed capacities, servicethroughputs, and service capability level data.
Detailed information is being developed to assist in workforce planning for the followingcategories of staff:
● nursing
● medical services including interns, registrars and specialist medical practitioners
● medical support including radiology, radiotherapy, pathology, dieticians, podiatry, chaplaincy,health promotion, other medical, pharmacy, technical, speech pathology, other ancillaryservices and allied health professionals
● site services including engineering, garden and security based occupations
● hotel services including catering, cleaning, stores/supply, laundry and transport occupations
● administration and clerical.
clinicalframeworknew spread 21/9/05 3:14 PM Page 32

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
31
The following work in progress will impact on the CSF workforce projections:
● the increase in training posts across the health system e.g. interns, junior doctors andsupervisory positions
● the third National Mental Health Plan
● privately contracted services, such as radiology
● an assessment of ‘replacement demand’ identifying demographic changes to the healthworkforce, including participation, retirement and migration trends.
Workforce InitiativesWorkforce reform and development strategies will centre on the new health workforce requiredto meet increasing demand. In particular the current scope of practice of the various healthoccupations requires examination and change in order to optimise workforce efficiency.
Major areas of workforce development include:
● better use of available professional workforce with delegation of tasks to other groups - forexample, providing administration and clerical support to medical staff, better utilising theirtime, particularly as ‘safe hours’ pressures reduce current average working time
● expansion of scope of practice - for example, providing more Nurse Practitioners withprescribing rights in various clinical settings
● development of new, multi-skilled health workers to meet specific needs - for example,developing rural health workers able to provide services currently provided by a range ofhealth workers in rural and remote settings
● review of current education and training regimes - for example, identifying where time intraining can be reduced to address critical supply shortages.
Increasing Workforce SupplyStrategies are being developed to increase health workforce supply to meet predicted growth indemand for services.
Medical training will increase significantly in WA, with the number of medical student completingtraining doubling over the next five years.
The WA Health medical workforce is being mapped to identify specialist training priorities andoptimise training capacity. Recently the Department completed an analysis of the surgicalworkforce, identifying training needs which will provide an adequate supply of surgeons to meetthe future demand. As part of this process existing and potential training posts have beenmapped and a business case developed to implement the required changes. This process willprovide the template for future work as the other medical specialties are mapped.
clinicalframeworknew spread 21/9/05 3:14 PM Page 33

32
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
The number of nurses in training and in the Nursing Register has also increased in recent years,and WA Health has developed retraining packages and supported training in key areas ofshortages, including mental health.
WA Health is developing new models of training, such as the new podiatry training program, andthe provision of scholarships for our staff to study in other states where there are no localtraining opportunities (e.g. radiation therapy and nuclear medicine).
Improved access to overseas labour is a key initiative to meet demand pressures in the shortterm. This is being achieved through the development of labour agreements and streamlinedimmigration processes with the Department of Immigration and Multicultural and IndigenousAffairs (DIMIA).
Attraction and RetentionWA Health is developing attraction and retention initiatives that are responsive to staff needs. Inaddition to negotiations to improve pay and working conditions, the Department is exploring:
● family friendly initiatives
● flexible working arrangements
● improving the quality of working life, by putting in place strategies such as targeting violencein the workplace.
Related Systems and Reporting Development The workforce aspect of the CSF links to a number of initiatives currently being undertaken byWorkforce Planning and Supply Branch of the Department of Health to improve human resourceanalysis and reporting capacity, including:
● enhancement of reporting capacity through an improved systems-based reporting framework,which provides a single aggregated source of human resource payroll data
● changes to core source data systems to improve the completeness and quality of workforcedata through a revision of record keeping standards and identification of health-specificminimum data requirements
● developing alternative views of financial measures, including productive and non-productiveworkforce profiles
● developing baseline establishment profiles that will facilitate improved reporting of actualstaff numbers, organisational structures and identification of vacancy rates, thereby deliveringimproved workforce planning capacity
● developing alternative service-related performance reporting and workforce profiling that ismore closely aligned with the operational requirements of health service units
● forging data links with other core Department of Health systems, including finance and activitysystems.
clinicalframeworknew spread 21/9/05 3:14 PM Page 34

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
33
Participation In National Health Workforce InitiativesWA Health actively participates in national workforce bodies and various national initiatives as ameans of ensuring that the state is represented at the highest level of national policydevelopment, and to ensure a coordinated approach to workforce concerns across all jurisdictions
The National Health Workforce Strategic Framework, which was endorsed by Australian HealthMinisters in April 2004, is focused on continuing to expand the supply of the medical, nursing,allied health and dental workforce. Priorities identified by the Australian Health WorkforceOfficials Committee (AHWOC) in December 2004 are:
● extending health workforce participation
● health workforce education and training including a new model of clinical education,alternative approaches to specialist education, and greater interaction with the highereducation sector, and
● minimising barriers, workforce reform, redesign and new workforce models.
Work undertaken by jurisdictions in collaboration with the Australian Government includes:
● review of the Royal Australasian College of Surgeons and other Colleges arising from theAustralian Competition and Consumer Commission (ACCC) determination
● review and reworking of national workforce projections undertaken by the Australian MedicalWorkforce Officials Committee (AMWAC), and review of national workforce data collections
● minimising barriers, workforce reform, redesign and new workforce models
● National reviews of workforce including the Surgical, General Practice, Radiation Oncology,Dental and Pathology workforces
● examining the interface between the health and education sectors
● developing nationally consistent medical registration and drafting instructions for medicalregistration legislation and for an intergovernmental agreement/memorandum ofunderstanding for endorsement by State and Territory Health Ministers
● The Productivity Commission has been asked to undertake a study examining issues such as:institutional, regulatory and other factors across the health and education sectors that affectthe supply of health workforce professionals; the structure and distribution of the healthworkforce; and factors affecting the demand for services to be completed by February 2006.
3.3 Infrastructure Development FrameworkIn order to maintain and improve existing health facility infrastructure and develop the newfacilities articulated in the CSF, significant investment in health care infrastructure is required.
The Health Infrastructure Steering Group (HISG), the peak decision-making body at a whole ofhealth level, will have responsibility for developing, managing and monitoring the overall healthinfrastructure program as agreed with Government. This will involve:
clinicalframeworknew spread 21/9/05 3:14 PM Page 35

34
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
● providing direction on infrastructure development strategies and objectives
● developing and monitoring Health’s capital expenditure program and capital investment plan
● approving new project concepts and business cases
● monitoring the progress of all approved infrastructure projects.
The HISG will meet its responsibilities with support from corporate health functions, including theHealth Reform Implementation Taskforce (HRIT), Health Finance and the Licensing Unit. Thesegroups will provide input into the infrastructure development process at various stages and:
● provide support to further clinical service planning
● develop and monitor the capital expenditure plan and investment program
● assist in the preparation, review and evaluation of business cases
● liaise with Department of Treasury and Finance
● ensure operational and facility standards are met
● explore the opportunities for public-private partnerships in line with Government policy.
The HISG will also be supported by a number of Project Control Groups (PCG) that will be thepeak decision-making bodies for Area Health Service infrastructure projects and statewideprojects such as mental health, clinical equipment replacement, minor capital works andinformation and communication technology.
The PCGs will be chaired by Area Health Service Chief Executives who will be members of theHISG and will be responsible for reporting on their infrastructure program, including reporting onworks in progress and ensuring that new projects are bought to the HISG for approval. Asmembers of the HISG, Chief Executives will also contribute to infrastructure planning at a wholeof health level.
The Infrastructure Development Framework will be prepared with reference to the roledelineation matrix and demand modeling and use a process with key steps as follows:
● development of a bed numbers framework as a guide to requirements in 2010, 2015 and 2020
● development of a ‘bed strategy’ to ensure the required numbers of beds by category bycatchments can be available on a year by year basis to 2020
● development of a facility strategy that describes how the beds and associated infrastructurecan be delivered on a campus by campus basis and in stages to 2020
● estimated area requirement (m2) (based on national benchmarks) for functional componentsfrom the facility strategies then used to estimate costs to inform the overall developmentplan.
clinicalframeworknew spread 21/9/05 3:14 PM Page 36

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
35
Consideration will also be given to associated infrastructure development needs in partnershipwith other government agencies and non-government organisations needs, such asaccommodation for staff in country areas, accommodation for patients and families and publictransport plans to enable access to health services.
3.4 Information and Communication Technology FrameworkSupporting the CSF and a number of health reform projects is an Information and CommunicationTechnology (ICT) strategy.
The ICT program will deliver a system-wide integrated clinical information system that willincorporate the public and private hospitals, community health, primary care and mental healthsectors. This new system will be progressively implemented across the state and will includeelectronic patient records, single patient identifiers and provider identification.
The ICT program will engage stakeholders in the development of system requirements for allclinical modules. This process is now almost complete. After further discussions with stakeholdersand the completion of the regulatory processes, the Department of Health will proceed to atender process in the later part of this year.
3.5 Recurrent Costing of the WA Health Clinical Services Framework Recurrent costing of the WA Health Clinical Services Framework is progressing. As a first phase, arange of cost estimate scenarios covering metropolitan inpatient services and emergencydepartment services have been prepared.
These estimates will be used to assess the potential impact of the WA Health Clinical ServicesFramework on the State health budget over the medium and long term. The estimates will be animportant indicator of the further work that is required to place our State health system on amore sustainable footing that is in line with Government policy and priorities on the financing ofhealth services.
The costing results generated to this point will be fed into the next stages of demand, workforceand financial planning. The costing results will be used to engage partners and stakeholderswithin the system and outside, in productive discussions about health system financing andachieving better integration between service provision and budget management.
More reliable and robust costing scenarios will become available as further detailed planning isundertaken around health system infrastructure, demand and workforce, and as there is greaterclarity around the financial costs and benefits of health reforms being progressed in associationwith the WA Health Clinical Services Framework.
clinicalframeworknew spread 21/9/05 3:14 PM Page 37

36
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
More robust costing estimates will also be derived through the progressing of developmentprojects as mentioned earlier, which will provide the necessary business intelligence, tools andcapability for enhanced medium and long term financial forecasting, including:
● Inpatient Activity Demand Modelling (next phase of demand modelling beyond the WA HealthClinical Services Framework)
● Non-Inpatient Activity Demand Modelling (including emergency care, ambulatory care, out-patients)
● Development of a uniform costing manual for the system to ensure consistent policies andpractice, and enhance intelligence around cost structures and cost behaviours
● Medium to long term cost and financial modelling of health workforce
● Medium to long term cost and financial modelling of health services
● Medium to long term price modelling of health services
● Development of a population-output based resource allocation and incentive and penaltymodel
● Development of a financial and service delivery benchmarking framework.
These projects are being undertaken in a joint manner between the Office of the DirectorGeneral, Health Reform Implementation Taskforce, Health Finance, State Health Support Services,Health Policy and Clinical Reform and the Area Health Services.
The WA Health Clinical Services Framework is a crucial first phase of system planning that willfacilitate for more detailed planning around demand, infrastructure, workforces and finances intothe future. Optimising the efficiency and effectiveness of our limited and valuable systemresources, and achieving greater financial sustainability has been a key consideration during theshaping of the WA Health Clinical Services Framework and will continue to be a considerationthrough the next phases of planning.
clinicalframeworknew spread 21/9/05 3:14 PM Page 38

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
37
SOU
TH M
ETRO
POLI
TAN
2017201620152014201320122011201020092008200720062005
Fiona Stanley
Fremantle
Woodside
Rockingham
Bentley
Armadale
SCGH
RPH
Shenton Park
Joondalup
Kalamunda
Swan
Osborne Park
Graylands
KEMH
PMH
NO
RTH
MET
ROPO
LITA
NST
ATEW
IDE
Relocation
Hospital Operational
Development/Redevelopment
4. Health Service Development Timeframe
This chart provides an overview of the indicative Infrastructure Development timeframes whichwill guide implementation planning. Again, it is important to note that timeframes may beadjusted as the planning process unfolds and more explicit plans are detailed.
clinicalframeworknew spread 21/9/05 3:14 PM Page 39

38
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
5. The Way Forward
The WA Health Clinical Services Framework provides the strategic direction for the delivery ofclinical services throughout Western Australia. However it is only one aspect of the overallplanning process that will inform WA Health’s Strategic Intent for 2005-2010 and see theimplementation of the State Health Strategic Plan 2005-2010.
Successful implementation of the plan will realise a number of health reform objectivesincluding:
● improved access to services
● reduced inequality in health status
● provision of safe, high quality health care
● promotion of a patient-centred continuum of care
● optimisation of public and private services
● improvement in the balance of preventative, primary and acute care
● financial sustainability as an integrated system
● support for a highly skilled and dedicated workforce.
Implementation PlanImplementing the CSF will be the responsibility of the entire team with WA Health.
Naturally, there will be a need for more extensive and detailed planning in many areas, buildingupon work already commenced and incorporating the new directions articulated.
This will also include a comprehensive and timely plan for the support and transition of ourworkforce as the changes are implemented. It will be important to ensure that all staff haveopportunity to participate and contribute during the implementation, are well informed about thechange process and are supported through transition arrangements.
A great deal of valuable information was submitted during the Clinical Services Consultation 2005,and this will be used to inform the implementation and transition phase which now follows.
A detailed implementation guide will be made available in due course.
clinicalframeworknew spread 21/9/05 3:14 PM Page 40

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
39
Hospital Information
Service Information
Appendix 1 – Clinical Services Role Delineation
Reading The Clinical Services Role Delineation
Hospital InformationIf you are interested in a particular hospital scan horizontally along the row for the nominatedfacility, then scan down to view the service provided for the specialty of interest.
Service InformationIf you are interested in a particular service scan down the column for the nominated facility, thenscan across to view the service provided at the hospital of interest.
Bed NumbersIf you are interested in the number of beds for a particular specialty at a hospital, scan down thevertical column to the specialty and across to the hospital of interest.
Clinical Services Role Delineation Matrix
clinicalframeworknew spread 21/9/05 3:14 PM Page 41

Determining Level of ServiceOnce you have located the hospital and service of interest on the Clinical Services RoleDelineation Matrix, such as Cardiology Services at Rockingham/Kwinana District Hospital, you willview a number located in this box. Using this example, you will see this is shown as a Level 3 for2004/05. For an explanation of the level of service, refer to the Clinical Services Role DelineationDefinitions document.
40
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
Determining Level of Service
E.g. This box will indicate the levelof service for Cardiology Servicesat Rockingham/Kwinana DistrictHospital
Clinical Service Role Delineation Matrix
clinicalframeworknew spread 21/9/05 3:14 PM Page 42

41
CLIN
ICAL
SER
VICE
S RO
LE D
ELIN
EATI
ON
DEF
INIT
ION
S
MED
ICA
L
Gen
eral
ist
Type
I Su
bspe
cial
ties
Type
II S
ubsp
ecia
ltie
sG
ener
alis
tTy
pe I
Subs
peci
alti
esTy
pe II
Sub
spec
ialt
ies
SURG
ICA
L
■Ph
ysic
ian
■Ca
rdio
logy
■D
erm
atol
ogy
■En
docr
inol
ogy
■G
astr
oent
erol
ogy
■G
eria
tric
med
icin
e■
Neu
rolo
gy■
Rena
l M
edic
ine
■Rh
eum
atol
ogy
■Ve
nere
olog
y■
Paed
iatr
ics
■Re
spir
ator
y M
edic
ine
■Cl
inic
al H
aem
atol
ogy
■Cl
inic
al M
icro
biol
ogy
■Im
mun
olog
y■
Med
ical
Onc
olog
y■
Palli
ativ
e Ca
re■
Radi
othe
rape
utic
Onc
olog
y■
Gen
etic
s■
Clin
ical
Inf
ecti
ous
Dis
ease
s
■G
ener
al S
urge
on■
Ear,
Nos
e an
d Th
roat
■O
bste
tric
s an
dG
ynae
colo
gy■
Oph
thal
mol
ogy
■O
rtho
paed
ics
■U
rolo
gy
■Ca
rdio
thor
acic
■N
euro
surg
ery
■Pl
asti
c su
rger
y■
Tran
spla
nt S
urge
ry■
Vasc
ular
Sur
gery
■Bu
rns
LEVE
L O
F SE
RVIC
E –
INPA
TIEN
T SE
RVIC
ESN
ilN
o se
rvic
e av
aila
ble
1O
utpa
tien
t ca
re –
RN
and
vis
itin
g G
P.
In r
emot
e ar
eas
poss
ibly
sup
port
via
tel
epho
ne2
Out
pati
ent
and
inpa
tien
t ca
re –
plu
s 24
hou
r G
P co
ver
and
limit
ed v
isit
ing
gene
ral
spec
ialis
ts f
or o
utpa
tien
t se
rvic
es o
nly
3O
utpa
tien
t an
d in
pati
ent
care
– p
lus
visi
ting
gen
eral
spe
cial
ists
(lo
w r
isk
obst
etri
cs a
nd e
lect
ive
surg
ery)
4O
utpa
tien
t an
d in
pati
ent
care
– p
lus
resi
dent
gen
eral
spe
cial
ists
plu
s vi
siti
ng T
ype
I su
bspe
cial
ists
, pl
us s
ome
juni
or m
edic
al s
taff
5
Out
pati
ent
and
inpa
tien
t ca
re –
plu
s vi
siti
ng T
ype
II su
bspe
cial
ists
plu
s so
me
med
ical
sta
ffin
g pl
us H
DU
. M
ay i
nclu
de s
ome
rese
arch
and
tra
inin
g.6
Stat
ewid
e se
rvic
es,
incl
udin
g Ty
pe I
I su
bspe
cial
ists
and
res
earc
h/ed
ucat
ion/
trai
ning
LEVE
L O
F SE
RVIC
E –
AMBU
LATO
RY C
ARE
SERV
ICES
Nil
No
serv
ice
avai
labl
e1
GP
only
2G
P an
d ou
tpat
ient
clin
ic a
t di
scha
rge
hosp
ital
. Li
mit
ed a
cces
s to
gen
eral
ist
dom
icili
ary
nurs
ing
3Vi
siti
ng s
peci
alis
t. S
ome
hosp
ital
avo
idan
ce/h
ospi
tal
subs
titu
tion
. So
me
earl
y di
scha
rge
serv
ices
. Ac
cess
to
gene
ralis
t do
mic
iliar
y nu
rsin
g an
d so
me
allie
dhe
alth
4Li
nks
wit
h H
ACC.
Inc
reas
ing
rang
e an
d co
mpl
exit
y of
hos
pita
l av
oida
nce/
subs
titu
tion
/ear
ly d
isch
arge
. Ch
roni
c di
seas
e pr
ogra
ms.
Vis
itin
g m
edic
al s
peci
alis
t.G
ood
acce
ss t
o ge
nera
list
allie
d he
alth
/nur
sing
sta
ff5
Spec
ialis
t m
edic
al/n
ursi
ng/a
llied
hea
lth
staf
f.
Incr
ease
d ra
nge
and
com
plex
ity.
HAC
C in
tegr
atio
n. E
nhan
ced
diag
nost
ics.
Tea
chin
g an
d tr
aini
ng r
ole
6Re
sear
ch r
ole.
Ful
ly i
nteg
rate
d am
bula
tory
car
e se
rvic
es.
Fully
int
egra
ted
diag
nost
ics
NB:
Def
init
ions
are
als
o pr
ovid
ed f
or p
rim
ary
care
, pr
even
tion
and
pro
mot
ion,
and
dia
gnos
tic
and
supp
ort
serv
ices
. Pl
ease
ref
er t
o th
e re
leva
nt s
ecti
on i
n th
isdo
cum
ent
for
mor
e in
form
atio
n.
clinicalframeworknew spread 21/9/05 3:14 PM Page 43

42
TABL
E O
F CO
NTE
NTS
Serv
ice
Type
■M
edic
al S
ervi
ces
43
■Su
rgic
al S
ervi
ces
47
■Em
erge
ncy/
Trau
ma
Serv
ices
50
■O
bste
tric
s Se
rvic
es
51
■Pa
edia
tric
s Se
rvic
es
51
■Re
habi
litat
ion
Serv
ices
52
■Co
ntin
uing
Car
e Se
rvic
es
53
■Pr
even
tion
and
Pro
mot
ion
Serv
ices
53
■Pr
imar
y Ca
re S
ervi
ces
54
■Am
bula
tory
Car
e Se
rvic
es
54
■Ch
ild a
nd A
dole
scen
ts M
enta
l H
ealt
h, A
dult
Men
tal
Hea
lth,
Old
er P
erso
ns M
enta
l H
ealt
h Se
rvic
es
56
■St
atew
ide
Men
tal
Hea
lth
Serv
ices
58
■Cl
inic
al S
uppo
rt S
ervi
ces
59
Abb
revi
atio
ns
EDEm
erge
ncy
Dep
artm
ent
BBV
Bloo
d Bo
rne
Viru
ses
CCU
Coro
nary
Car
e U
nit
CDCo
mm
unic
able
Dis
ease
CDC
Child
Dev
elop
men
t Ce
ntre
CHN
Child
Hea
lth
Nur
seCO
PMI
Child
ren
of P
aren
ts w
ith
Men
tal
Illne
ssCT
Com
pute
rise
d Ax
ial
Tom
ogra
phy
DU
E’s
Dru
g U
sage
Eva
luat
ion
EEG
Elec
tro-
ence
phal
ogra
mEM
GEl
ectr
o-m
yleo
gram
ENT
Ear,
nos
e an
d th
roat
GEM
Ger
iatr
ic E
valu
atio
nM
anag
emen
tG
PG
ener
al P
ract
itio
ner
HAC
CH
ome
and
Com
mun
ity
HD
UH
igh
Dep
ende
ncy
Uni
t
ICU
Inte
nsiv
e Ca
re U
nit
LUCS
Low
er U
teri
ne C
aesa
rian
Sect
ion
MRI
Mag
neti
c Re
sona
nce
Imag
eO
&G
Obs
tetr
ics
and
Gyn
aeco
logy
OR
Ope
rati
ng R
oom
OT
Occ
upat
iona
l Th
erap
ist
PET
Posi
tron
Em
issi
on T
omog
raph
y PT
Phys
ioth
erap
ist
RMO
Regi
ster
ed M
edic
al O
ffic
erRM
Regi
ster
ed M
idw
ife
RNRe
gist
ered
Nur
seSP
Sp
eech
The
rapi
st
SRN
Seni
or R
egis
tere
d N
urse
STI
Sexu
ally
Tra
nsm
itte
dIn
fect
ion
Care
WAC
HS
WA
Coun
try
Hea
lth
Serv
ice
clinicalframeworknew spread 21/9/05 3:14 PM Page 44

43
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
Gen
eral
Card
iolo
gy
Endo
crin
olog
y
■Ca
re i
s ca
rrie
d ou
t by
GPs
(pot
enti
ally
vis
itin
g) w
ith
or w
itho
ut t
he a
ssis
tanc
eof
RN
s de
pend
ing
on t
hety
pe o
f pa
tien
t ca
rene
eded
■Ca
re i
s ca
rrie
d ou
t by
GPs
(pot
enti
ally
vis
itin
g) w
ith
or w
itho
ut t
he a
ssis
tanc
eof
RN
s de
pend
ing
on t
hety
pe o
f pa
tien
t ca
rene
eded
■Ca
re i
s ca
rrie
d ou
t by
GPs
(pot
enti
ally
vis
itin
g) w
ith
or w
itho
ut t
he a
ssis
tanc
eof
RN
s de
pend
ing
on t
hety
pe o
f pa
tien
t ca
rene
eded
As f
or l
evel
1 p
lus:
■In
pati
ent
and
outp
atie
ntca
re■
Visi
ting
GP
■24
hou
r co
ver
by R
N
As f
or l
evel
1 p
lus:
■In
pati
ent
and
outp
atie
ntca
re■
Visi
ting
GP
■24
hou
r co
ver
by R
N
As f
or l
evel
1 p
lus:
■In
pati
ent
and
outp
atie
ntca
re■
Visi
ting
GP
■24
hou
r co
ver
by R
N
As f
or l
evel
2 p
lus:
■G
P in
pati
ent
care
■24
hou
r co
ver
by R
N■
Out
pati
ent
care
by
visi
ting
gen
eral
phys
icia
n/ge
nera
l in
tern
alm
edic
ine
spec
ialis
t an
dm
aybe
som
e Ty
pe I
spec
ialis
ts
As f
or l
evel
2 p
lus:
■G
P in
pati
ent
care
■24
hou
r co
ver
by R
N■
Out
pati
ent
care
by
visi
ting
gen
eral
phy
sici
anan
d po
ssib
ly c
ardi
olog
ist
As f
or l
evel
2 p
lus:
■G
P in
pati
ent
care
■24
hou
r co
ver
by R
N■
Out
pati
ent
care
by
visi
ting
gen
eral
phy
sici
an
As f
or l
evel
3 p
lus:
■In
pati
ent
care
by
resi
dent
gene
ral
phys
icia
n an
d G
Ps■
Out
pati
ent
cons
ulta
tion
by v
isit
ing
Type
I s
ub-
spec
ialis
ts■
Spec
ialis
t RN
As f
or l
evel
3 p
lus:
■In
pati
ent
care
by
resi
dent
gene
ral
phys
icia
n ■
Out
pati
ent
cons
ulta
tion
by v
isit
ing
card
iolo
gist
■Sp
ecia
list
RN
As f
or l
evel
3 p
lus:
■In
pati
ent
care
by
resi
dent
gene
ral
phys
icia
n ■
Out
pati
ent
cons
ulta
tion
by v
isit
ing
endo
crin
olog
ist
■D
iabe
tes
educ
atio
nse
rvic
e an
d in
tegr
ated
hosp
ital
/com
mun
ity
diab
etes
man
agem
ent
serv
ice
■Sp
ecia
list
RN
As f
or l
evel
4 p
lus:
■In
pati
ent
care
by
resi
dent
gene
ral
phys
icia
n an
d G
Psan
d so
me/
all
Type
I s
ub-
spec
ialis
ts■
Visi
ting
Typ
e II
sub-
spec
ialis
ts■
Regi
stra
r/RM
O/I
nter
n■
CCU
/HD
U■
Regi
onal
ref
erra
l ro
le■
Som
e un
derg
radu
ate
teac
hing
■Em
erge
ncy
serv
ices
avai
labl
e by
on
call
spec
ialis
t
As f
or l
evel
4 p
lus:
■In
pati
ent
care
by
resi
dent
card
iolo
gist
■Re
gist
rar/
RMO
/Int
ern
■CC
U/H
DU
■In
clud
es C
ath
Labs
■Re
gion
al r
efer
ral
role
■
Acce
ss s
peci
alis
t SR
N■
Som
e un
derg
radu
ate
teac
hing
and
pos
sibl
yso
me
rese
arch
rol
e■
Link
s w
ith
leve
l 5
reha
bilit
atio
n se
rvic
e■
Emer
genc
y se
rvic
esav
aila
ble
by o
n ca
llca
rdio
logi
sts
As f
or l
evel
4 p
lus:
■In
pati
ent
care
by
resi
dent
endo
crin
olog
ist
■Re
gist
rar/
RMO
■Re
gion
al r
efer
ral
role
■Ac
cess
to
spec
ialis
t SR
N■
Dia
bete
s ed
ucat
ion
serv
ice
and
inte
grat
edho
spit
al/c
omm
unit
ydi
abet
es m
anag
emen
tse
rvic
e■
Som
e un
derg
radu
ate
teac
hing
and
pos
sibl
yre
sear
ch r
ole
■Li
nks
to l
evel
5re
habi
litat
ion
serv
ice
■Em
erge
ncy
care
ava
ilabl
efr
om o
n ca
ll sp
ecia
list
As f
or l
evel
5 p
lus:
■Fu
ll ra
nge
of m
edic
al s
ub-
spec
ialis
ts T
ype
I an
d II
and
emer
genc
y m
edic
alse
rvic
es■
Stat
ewid
e re
ferr
al r
ole
ince
rtai
n su
bspe
cial
ties
■U
nder
grad
uate
and
post
grad
uate
tea
chin
gro
le
As f
or l
evel
5 p
lus:
■Fu
ll ra
nge
card
iac
serv
ices
inc
ludi
ng c
ardi
acsu
b-sp
ecia
ltie
s an
dem
erge
ncy
serv
ices
■CC
U/H
DU
■St
atew
ide
refe
rral
rol
e■
Und
ergr
adua
te a
ndpo
stgr
adua
te t
each
ing
role
■Re
sear
ch r
ole
As f
or l
evel
5 p
lus:
■Fu
ll ra
nge
ofen
docr
inol
ogy
serv
ices
,w
ith
endo
crin
olog
yde
part
men
t an
dem
erge
ncy
care
■St
atew
ide
refe
rral
rol
e■
Und
ergr
adua
te a
ndpo
stgr
adua
te t
each
ing
role
■Re
sear
ch r
ole
Med
ical
Ser
vice
s
clinicalframeworknew spread 21/9/05 3:14 PM Page 45

44
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
Ger
iatr
ic
Neu
rolo
gy
Rena
l –
gene
ral
■Ca
re i
s ca
rrie
d ou
t by
GPs
(pot
enti
ally
vis
itin
g) w
ith
or w
itho
ut t
he a
ssis
tanc
eof
RN
s de
pend
ing
on t
hety
pe o
f pa
tien
t ca
rene
eded
■Ca
re i
s ca
rrie
d ou
t by
GPs
(pot
enti
ally
vis
itin
g)
wit
hor
wit
hout
the
ass
ista
nce
of R
Ns
depe
ndin
g on
the
type
of
pati
ent
care
need
ed
■Ca
re i
s ca
rrie
d ou
t by
GPs
(pot
enti
ally
vis
itin
g) w
ith
or w
itho
ut t
he a
ssis
tanc
eof
RN
s de
pend
ing
on t
hety
pe o
f pa
tien
t ca
rene
eded
As f
or l
evel
1 p
lus:
■In
pati
ent
and
outp
atie
ntca
re■
Visi
ting
GP
and
poss
ibly
visi
ting
gen
eral
phy
sici
an■
24 h
our
cove
r by
RN
■Po
ssib
ly r
espi
te c
are
As f
or l
evel
1 p
lus:
■In
pati
ent
and
outp
atie
ntca
re■
Visi
ting
GP
■24
hou
r co
ver
by R
N
As f
or l
evel
1 p
lus:
■In
pati
ent
and
outp
atie
ntca
re■
Visi
ting
GP
■24
hou
r co
ver
by R
N
As f
or l
evel
2 p
lus:
■In
pati
ent
and
outp
atie
ntca
re■
Resi
dent
GP
and
visi
ting
gene
ral
phys
icia
n■
24 h
our
cove
r by
RN
and
by G
P■
Resp
ite
care
and
lim
ited
reha
bilit
atio
n se
rvic
es
As f
or l
evel
2 p
lus:
■G
P In
pati
ent
Care
■24
hou
r co
ver
by R
N■
Out
pati
ent
care
by
visi
ting
gen
eral
phy
sici
anan
d po
ssib
ly n
euro
logi
st
As f
or l
evel
2 p
lus:
■G
ener
al p
hysi
cian
(lik
ely
to b
e vi
siti
ng)
inpa
tien
tca
re■
GP
care
■24
hou
r co
ver
by R
N■
Out
pati
ent
care
by
visi
ting
gen
eral
phy
sici
anan
d po
ssib
ly r
enal
spec
ialis
t■
May
acc
omm
odat
e se
lfca
re d
ialy
sis
in-p
atie
nts
As f
or l
evel
3 p
lus:
■Ac
cess
to
cons
ulta
ntph
ysic
ian
spec
ialis
ing
inge
riat
ric
med
icin
e■
Acti
ve a
sses
smen
t an
dre
habi
litat
ion
serv
ices
for
inpa
tien
ts a
nd o
utpa
tien
ts
As f
or l
evel
3 p
lus:
■In
pati
ent
care
by
resi
dent
gene
ral
phys
icia
n ■
Out
pati
ent
cons
ulta
tion
by v
isit
ing
neur
olog
ist
■Li
nks
wit
h at
lea
st l
evel
4ge
riat
ric
and
reha
bilit
atio
n se
rvic
es■
Spec
ialis
t RN
As f
or l
evel
3 p
lus:
■In
pati
ent
care
by
resi
dent
gene
ral
phys
icia
n ■
Out
pati
ent
cons
ulta
tion
by v
isit
ing
rena
l sp
ecia
list
■Se
lf c
are
dial
ysis
uni
t w
ith
links
to
larg
er r
enal
uni
t■
Spec
ialis
t RN
As f
or l
evel
4 p
lus:
■In
pati
ent
care
by
resi
dent
spec
ialis
t■
Regi
stra
r/RM
O■
Link
wit
h in
pati
ent
reha
bilit
atio
n un
it■
Inpa
tien
t as
sess
men
t un
itan
d do
mic
iliar
y co
nsul
tant
serv
ices
■Ac
cess
to
spec
ialis
t SR
N■
Som
e un
derg
radu
ate
teac
hing
■
Link
s w
ith
geri
atri
cps
ychi
atry
ser
vice
s
As f
or l
evel
4 p
lus:
■In
pati
ent
care
by
resi
dent
neur
olog
ist
■Re
gist
rar/
RMO
■Re
gion
al r
efer
ral
role
■Ac
cess
to
spec
ialis
t SR
N■
Som
e un
derg
radu
ate
teac
hing
and
pos
sibl
yso
me
rese
arch
rol
e■
Neu
rosu
rger
y su
ppor
t,EM
G,
nerv
e co
nduc
tion
,ev
oked
res
pons
es a
nd E
EGon
sit
e■
Emer
genc
y se
rvic
espr
ovid
ed b
y on
cal
lne
urol
ogis
t
As f
or l
evel
4 p
lus:
■In
pati
ent
care
by
resi
dent
rena
l sp
ecia
lists
■Re
gist
rar/
RMO
■Em
erge
ncy
serv
ices
prov
ided
by
on c
all
spec
ialis
t■
Regi
onal
ref
erra
l ro
le■
Acce
ss t
o sp
ecia
list
SRN
■So
me
unde
rgra
duat
ete
achi
ng a
nd p
ossi
bly
som
e re
sear
ch r
ole
■Al
l ty
pes
of d
ialy
sis
avai
labl
e an
d re
nal
biop
sies
per
form
ed■
Prov
ides
a f
ull
rang
e of
dial
ysis
acc
ess
surg
ery
As f
or l
evel
5 p
lus:
■Re
side
nt g
eria
tric
ian
■U
nder
grad
uate
and
post
grad
uate
tea
chin
gro
le■
Rese
arch
rol
e■
Stat
ewid
e re
ferr
al r
ole
As f
or l
evel
5 p
lus:
■Fu
ll ra
nge
of n
euro
logy
serv
ices
, w
ith
neur
olog
yde
part
men
t an
dem
erge
ncy
care
■
Stat
ewid
e re
ferr
al r
ole
■U
nder
grad
uate
and
post
grad
uate
tea
chin
gro
le■
Acce
ss t
o CT
and
MRI
and
poss
ibly
PET
■Re
sear
ch r
ole
As f
or l
evel
5 p
lus:
■Fu
ll ra
nge
of r
enal
serv
ices
, w
ith
rena
lde
part
men
t an
dem
erge
ncy
care
ser
vice
s■
Rena
l tr
ansp
lant
atio
nav
aila
ble
■Co
ordi
nate
d by
ful
l ti
me
rena
l un
it m
anag
er
■St
atew
ide
refe
rral
rol
ean
d st
atew
ide
geog
raph
ical
are
a ba
sed
serv
ice
deliv
ery
role
■U
nder
grad
uate
and
post
grad
uate
tea
chin
gro
le■
Rese
arch
rol
e■
Prov
ides
a f
ull
rang
e of
dial
ysis
acc
ess
surg
ery
clinicalframeworknew spread 21/9/05 3:14 PM Page 46

45
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
Rena
l –
dial
ysis
Onc
olog
y
Radi
atio
n O
ncol
ogy
■Ca
re i
s ca
rrie
d ou
t by
GPs
(pot
enti
ally
vis
itin
g) w
ith
or w
itho
ut t
he a
ssis
tanc
eof
RN
s de
pend
ing
on t
hety
pe o
f pa
tien
t ca
rene
eded
■Se
rvic
es o
ffer
ed b
y a
gene
ral
heal
thse
rvic
e/cl
inic
■Ca
re u
nder
sup
ervi
sion
of
GP
wit
h or
wit
hout
RN
■Se
lf-c
arin
g st
able
pat
ient
s■
Out
reac
h su
ppor
t fo
rho
me
dial
ysis
, po
ssib
lyun
der
rem
ote
dire
ctio
nfr
om a
Lev
el 5
or
Leve
l 6
dial
ysis
fac
ility
As f
or l
evel
1 p
lus:
■In
pati
ent
and
outp
atie
ntca
re■
Visi
ting
GP
■24
hou
r co
ver
by R
N
As f
or l
evel
2 p
lus:
■Co
mm
unit
y-ba
sed
sate
llite
ser
vice
■Pr
edom
inat
ely
self
-car
ing
stab
le p
atie
nts
■Sp
ecia
list
RN■
Visi
ting
spe
cial
ist
for
mor
e co
mpl
icat
ed c
ases
■So
me
asse
ssm
ent
serv
ices
As f
or l
evel
2 p
lus:
■G
P in
pati
ent
care
■24
hou
r co
ver
by R
N■
Out
pati
ent
care
by
visi
ting
gen
eral
phy
sici
anan
d po
ssib
ly o
ncol
ogis
t
As f
or l
evel
3 p
lus:
■G
ener
al h
ospi
tal-
base
dsa
telli
te s
ervi
ce■
Visi
ting
spe
cial
ist
orge
nera
l ph
ysic
ian
wit
hne
phro
logy
ski
lls■
Mor
e co
mpl
icat
ed c
ases
■As
sess
men
t se
rvic
es■
Spec
ialis
t RN
■Ac
cess
to
on-s
ite
allie
dhe
alth
sup
port
(eg
;D
ieti
tian
s an
d So
cial
Wor
kers
)
As f
or l
evel
3 p
lus:
■In
pati
ent
care
by
resi
dent
gene
ral
phys
icia
n ■
Out
pati
ent
cons
ulta
tion
by v
isit
ing
onco
logi
st■
Link
s w
ith
radi
othe
rapy
,pa
lliat
ive
care
and
pai
nm
anag
emen
t se
rvic
es■
Spec
ialis
t RN
■Vi
siti
ng r
adia
tion
onco
logi
st w
orki
ng i
nco
njun
ctio
n w
ith
com
preh
ensi
ve c
ance
rse
rvic
e ■
No
trea
tmen
t fa
cilit
ies
As f
or l
evel
4 p
lus:
■Re
side
nt s
peci
alis
t■
Acce
ss t
o sp
ecia
list
SRN
■M
ore
com
plic
ated
cas
es■
Asse
ssm
ent
serv
ices
■Re
gion
al r
efer
ral
role
■Ac
cess
to
on-s
ite
allie
dhe
alth
sup
port
(eg
;D
ieti
tian
s an
d So
cial
Wor
kers
)
As f
or l
evel
4 p
lus:
■In
pati
ent
care
by
resi
dent
onco
logi
st■
Regi
stra
r/RM
O■
Regi
onal
ref
erra
l ro
le■
Acce
ss t
o sp
ecia
list
SNR
■So
me
unde
rgra
duat
ete
achi
ng a
nd p
ossi
bly
som
e re
sear
ch r
ole
■M
ulti
disc
iplin
ary
man
agem
ent
of p
atie
nts
incl
udin
g ca
seco
nfer
ence
s.■
Link
s w
ith
palli
ativ
e ca
rese
rvic
es a
nd m
ay h
ave
pain
man
agem
ent
clin
ic
■Em
erge
ncy
care
ava
ilabl
e■
Acce
ss t
o sp
ecia
list
SRN
As f
or l
evel
4 p
lus:
■Ba
sic
radi
atio
n on
colo
gyse
rvic
e w
ith
min
imum
equi
pmen
t -
poss
ibly
onl
yon
e m
achi
ne■
Has
acc
ess
to r
adia
tion
onco
logi
sts,
phy
sici
sts
and
radi
atio
n th
erap
ists
■Ac
cess
to
spec
ialis
t SR
N■
Link
s to
lev
el 5
pal
liati
veca
re s
ervi
ce
As f
or l
evel
5 p
lus:
■Re
side
nt s
peci
alis
t■
Mor
e co
mpl
icat
ed c
ases
■Pr
ovid
es a
cute
dia
lysi
sw
hen
nece
ssar
y■
Asse
ssm
ent
serv
ices
■U
nder
grad
uate
and
post
grad
uate
tea
chin
gro
le■
Stat
ewid
e ce
ntre
of
exce
llenc
e an
d re
ferr
alro
le■
Acce
ss t
o sp
ecia
list
SRN
■Ac
cess
to
on-s
ite
allie
dhe
alth
sup
port
(eg
;D
ieti
tian
s an
d So
cial
Wor
kers
)■
Com
plic
ated
ass
essm
ent
and
trea
tmen
t of
uns
tabl
eco
-mor
bidi
ties
As f
or l
evel
5 p
lus:
■Fu
ll ra
nge
of o
ncol
ogy
serv
ices
, w
ith
onco
logy
depa
rtm
ent
and
emer
genc
y se
rvic
es■
Stat
ewid
e re
ferr
al r
ole
■U
nder
grad
uate
and
post
grad
uate
tea
chin
gro
le■
Rese
arch
rol
e■
Acce
ss t
o sp
ecia
list
SNR
As f
or l
evel
5 p
lus:
■Fu
ll ra
nge
of r
adia
tion
onco
logy
ser
vice
s, l
ocat
edin
pri
ncip
le r
efer
ral
cent
re w
ith
acce
ss t
o al
lsu
bspe
cial
ties
■St
atew
ide
refe
rral
rol
e■
Und
ergr
adua
te a
ndpo
stgr
adua
te t
each
ing
role
■Re
sear
ch r
ole
■Fu
lly i
nteg
rate
dco
mpu
teri
sed
plan
ning
,tr
eatm
ent
and
veri
fica
tion
sys
tem
s■
Mec
hani
cal
and
biom
edic
al s
uppo
rtfa
cilit
ies
clinicalframeworknew spread 21/9/05 3:14 PM Page 47

46
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
Resp
irat
ory
Palli
ativ
e Ca
re
Gas
troe
nter
olog
y
■Ca
re i
s ca
rrie
d ou
t by
GPs
(pot
enti
ally
vis
itin
g) w
ith
or w
itho
ut t
he a
ssis
tanc
eof
RN
s de
pend
ing
on t
hety
pe o
f pa
tien
t ca
rene
eded
■Ca
re i
s ca
rrie
d ou
t by
GPs
(pot
enti
ally
vis
itin
g) w
ith
or w
itho
ut t
he a
ssis
tanc
eof
RN
s de
pend
ing
on t
hety
pe o
f pa
tien
t ca
rene
eded
■Ca
re i
s ca
rrie
d ou
t by
GPs
(pot
enti
ally
vis
itin
g) w
ith
or w
itho
ut t
he a
ssis
tanc
eof
RN
s de
pend
ing
on t
hety
pe o
f pa
tien
t ca
rene
eded
As f
or l
evel
1 p
lus:
■In
pati
ent
and
outp
atie
ntca
re■
Visi
ting
GP
■24
hou
r co
ver
by R
N
As f
or l
evel
1 p
lus:
■M
anag
emen
t by
GPs
and
gene
ralis
t nu
rses
■24
hou
r co
vera
ge■
Link
age
wit
h co
mm
unit
yba
sed
serv
ices
pro
vide
dby
Silv
er C
hain
Nur
sing
Asso
ciat
ion
As f
or l
evel
1 p
lus:
■In
pati
ent
and
outp
atie
ntca
re■
Visi
ting
GP
■24
hou
r co
ver
by R
N
As f
or l
evel
2 p
lus:
■G
P in
pati
ent
care
■24
hou
r co
ver
by R
N■
Out
pati
ent
care
by
visi
ting
gen
eral
phy
sici
anan
d po
ssib
ly r
espi
rato
rysp
ecia
list
As f
or l
evel
2 p
lus:
■In
pati
ent
care
by
accr
edit
ed G
P or
spec
ialis
t ph
ysic
ian
■24
hou
r co
ver
clin
ical
nurs
e w
ith
expe
rien
ce i
npa
lliat
ive
care
ser
vice
s■
Out
pati
ent
care
by
visi
ting
gen
eral
phy
sici
anan
d po
ssib
ly p
allia
tive
care
spe
cial
ist
As f
or l
evel
2 p
lus:
■G
P in
pati
ent
care
■24
hou
r co
ver
by R
N■
Out
pati
ent
care
by
visi
ting
gen
eral
phy
sici
anan
d po
ssib
lyga
stro
ente
rolo
gist
■
Poss
ibly
hav
e fi
bre
opti
cen
dosc
opy
by a
ccre
dite
dm
edic
al p
ract
itio
ner
As f
or l
evel
3 p
lus:
■In
pati
ent
care
by
resi
dent
gene
ral
phys
icia
n ■
Out
pati
ent
cons
ulta
tion
by v
isit
ing
resp
irat
ory
spec
ialis
t■
Spec
ialis
t RN
As f
or l
evel
3 p
lus:
■Pa
lliat
ive
care
inp
atie
ntbe
ds m
anag
ed b
y G
P or
med
ical
pra
ctit
ione
rsp
ecia
lisin
g in
pal
liati
veca
re■
Acce
ss t
o sp
ecia
list
SRN
■Se
amle
ss l
inka
ge t
o Si
lver
Chai
n N
ursi
ng A
ssoc
iati
onw
ho p
rovi
de c
omm
unit
yba
sed
palli
ativ
e ca
re
As f
or l
evel
3 p
lus:
■In
pati
ent
care
by
resi
dent
gene
ral
phys
icia
n ■
Out
pati
ent
cons
ulta
tion
by v
isit
ing
gast
roen
tero
logi
st■
Regu
lar
endo
scop
y se
rvic
ein
clud
ing
colo
nosc
opy
■Sp
ecia
list
RN■
Gas
troe
nter
olog
y se
rvic
espr
ovid
ed b
y in
tegr
ated
phys
icia
n an
d su
rgic
alse
rvic
es
As f
or l
evel
4 p
lus:
■In
pati
ent
care
by
resi
dent
resp
irat
ory
spec
ialis
t■
Regi
stra
r/RM
O■
Regi
onal
ref
erra
l ro
le■
Acce
ss t
o sp
ecia
list
SRN
■So
me
unde
rgra
duat
ete
achi
ng a
nd p
ossi
bly
som
e re
sear
ch r
ole
■Ac
cess
to
leve
l 5
card
iolo
gy a
ndca
rdio
thor
acic
sur
gery
■Em
erge
ncy
care
pro
vide
dby
on
call
spec
ialis
t
As f
or l
evel
4 p
lus:
■In
pati
ent
care
by
resi
dent
palli
ativ
e ca
re p
hysi
cian
■Re
gist
rar/
RMO
■Re
gion
al r
efer
ral
role
■Ac
cess
to
spec
ialis
t SR
N■
Und
ergr
adua
te t
each
ing
and
som
e re
sear
ch r
ole
■In
tegr
ated
com
mun
ity/
hosp
ice
cons
ulta
tive
ser
vice
und
erdi
rect
ion
of p
allia
tive
care
phy
sici
an■
Link
s w
ith
onco
logy
,ra
diot
hera
py,
anae
sthe
tics
, ps
ychi
atry
,pa
in c
linic
and
reha
bilit
atio
n
As f
or l
evel
4 p
lus:
■In
pati
ent
care
by
resi
dent
gast
roen
tero
logi
st■
Regi
stra
r/RM
O■
Regi
onal
ref
erra
l ro
le■
Acce
ss t
o sp
ecia
list
SRN
■So
me
unde
rgra
duat
ete
achi
ng a
nd p
ossi
bly
som
e re
sear
ch r
ole
■Fu
ll en
dosc
opy
serv
ice
■Em
erge
ncy
care
ava
ilabl
eby
on
call
spec
ialis
t
As f
or l
evel
5 p
lus:
■Fu
ll ra
nge
of r
espi
rato
ryse
rvic
es,
wit
h re
spir
ator
yde
part
men
t an
dem
erge
ncy
care
■St
atew
ide
refe
rral
rol
e■
Und
ergr
adua
te a
ndpo
stgr
adua
te t
each
ing
role
■
Rese
arch
rol
e■
Has
a r
espi
rato
ry f
unct
ion
labo
rato
ry■
Acce
ss t
o sp
ecia
list
SRN
As f
or l
evel
5 p
lus:
■Fu
ll ra
nge
of p
allia
tive
care
ser
vice
s w
ith
palli
ativ
e ca
re s
peci
alis
tpr
ovid
ing
cons
ulta
ncy
toot
her
unit
s re
ferr
alho
spit
als
■Em
erge
ncy
serv
ices
avai
labl
e ■
Stat
ewid
e re
ferr
al r
ole
■U
nder
grad
uate
and
post
grad
uate
tea
chin
gro
le
■H
as s
taff
wit
h co
njoi
ntap
poin
tmen
ts w
ith
hosp
ice
■Ac
cess
to
spec
ialis
t SR
N
As f
or l
evel
5 p
lus:
■Fu
ll ra
nge
ofga
stro
ente
rolo
gy s
ervi
ces,
wit
h ga
stro
ente
rolo
gyde
part
men
t an
dem
erge
ncy
care
■St
atew
ide
refe
rral
rol
e■
Und
ergr
adua
te a
ndpo
stgr
adua
te t
each
ing
role
■
Rese
arch
rol
e■
Acce
ss t
o sp
ecia
list
SRN
clinicalframeworknew spread 21/9/05 3:14 PM Page 48

47
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
Gen
eral
ENT
Gyn
aeco
logy
■Ca
re i
s ca
rrie
d ou
t by
GPs
(pot
enti
ally
vis
itin
g) w
ith
or w
itho
ut t
he a
ssis
tanc
eof
RN
s de
pend
ing
on t
hety
pe o
f pa
tien
t ca
rene
eded
As f
or l
evel
1 p
lus:
■M
inor
out
pati
ent
and
sam
e da
y pr
oced
ures
onl
yby
GP
or v
isit
ing
gene
ral
surg
eon
■In
pati
ent
care
fol
low
ing
surg
ery
else
whe
re
■M
inor
out
pati
ent
and
sam
e da
y pr
oced
ures
onl
yby
GP
or v
isit
ing
gene
ral
surg
eon
■In
pati
ent
care
fol
low
ing
surg
ery
else
whe
re
As f
or l
evel
2 p
lus:
■D
ay s
urge
ry t
ype
case
s,un
com
plic
ated
ele
ctiv
esu
rger
y an
d em
erge
ncy
surg
ery
■G
P an
d vi
siti
ng g
ener
alsu
rgic
al s
peci
alis
t■
Visi
ting
ana
esth
etis
t w
ith
visi
ting
sur
geon
■Th
eatr
e tr
aine
d RN
As f
or l
evel
2 p
lus:
■Co
mm
on a
ndin
term
edia
te p
roce
dure
son
low
or
mod
erat
e ri
skpa
tien
ts b
y vi
siti
ngge
nera
l su
rgeo
n
As f
or l
evel
3 p
lus:
■Su
rger
y by
GPs
, ge
nera
lsu
rgeo
ns a
nd v
isit
ing
Type
I su
b-sp
ecia
lists
■Br
oad
rang
e of
day
and
gene
ral
surg
ery
and
som
esp
ecia
lty
surg
ery
■Th
eatr
e tr
aine
d nu
rses
■M
ore
than
1 t
heat
re■
May
inc
lude
hig
h-de
pend
ency
nur
sing
uni
t
■Co
mm
on a
ndin
term
edia
te s
urge
ry d
one
on l
ow o
r m
oder
ate
risk
pati
ents
by
visi
ting
EN
Tsu
rgeo
n■
No
neur
o-op
tic
orin
trac
rani
al s
urge
ry
As f
or l
evel
3 p
lus:
■Co
mm
on,
inte
rmed
iate
and
som
e m
ajor
proc
edur
es o
n lo
w a
ndm
oder
ate
risk
pat
ient
spe
rfor
med
by
visi
ting
gyna
ecol
ogis
ts■
Link
s w
ith
onco
logy
,ra
diot
hera
py a
ndpa
lliat
ive
care
ser
vice
s
As f
or l
evel
4 p
lus:
■G
ener
al s
urge
ons
■So
me/
all
Type
I s
ub-
spec
ialis
ts■
Visi
ting
Typ
e II
sub-
spec
ialis
ts■
Regi
stra
r/RM
O■
ICU
■Re
gion
al r
efer
ral
role
■M
ay h
ave
som
e te
achi
ngan
d re
sear
ch r
ole
■U
nder
take
s m
ost
emer
genc
y su
rger
y■
May
inc
lude
kid
ney
tran
spla
ntat
ion
inse
lect
ed s
ites
As f
or l
evel
4 p
lus:
■D
iagn
osti
c se
rvic
es a
ndsu
rger
y on
low
, m
oder
ate
and
high
ris
k pa
tent
s by
on c
all
ENT
surg
eon
■Ac
cess
to
spec
ialis
t SR
N■
Regi
onal
ref
erra
l ro
le■
May
hav
e so
me
teac
hing
and
rese
arch
rol
e■
Link
s w
ith
onco
logy
,ra
diot
hera
py a
ndpa
lliat
ive
care
ser
vice
s■
Lim
ited
neu
ro-o
ptic
surg
ery
As f
or l
evel
4 p
lus:
■D
iagn
osti
c se
rvic
es a
ndsu
rger
y on
low
, m
oder
ate
and
high
ris
k pa
tien
ts b
yon
cal
l gy
naec
olog
ists
■Ac
cess
to
spec
ialis
t SR
N■
May
hav
e gy
naec
olog
yre
gist
rar/
RMO
■Re
gion
al r
efer
ral
role
■M
ay h
ave
som
e te
achi
ngan
d re
sear
ch r
ole
As f
or l
evel
5 p
lus:
■Fu
ll ra
nge
of s
urgi
cal
sub-
spec
ialis
ts T
ype
I an
d II
■St
atew
ide
refe
rral
rol
e■
Und
ergr
adua
te a
nd p
ost
grad
uate
tea
chin
g ro
le■
Rese
arch
rol
e■
Und
erta
kes
emer
genc
ysu
rger
y■
May
inc
lude
kid
ney
and
liver
tra
nspl
anta
tion
in
sele
cted
sit
es
As f
or l
evel
5 p
lus:
■Ab
ility
to
deal
wit
h al
lca
ses
incl
udin
g fu
ll ra
nge
of c
ompl
ex c
ases
in
asso
ciat
ion
wit
h ot
her
spec
ialis
ts i
nclu
ding
neur
o-op
tic
and
intr
acra
nial
pro
cedu
res,
as l
ong
as l
evel
6ne
uros
urge
ry a
vaila
ble
onsi
te■
Emer
genc
y se
rvic
esav
aila
ble
■St
atew
ide
refe
rral
rol
e■
Und
ergr
adua
te a
nd p
ost
grad
uate
tea
chin
g ro
le■
Rese
arch
rol
e■
ENT
regi
stra
r/RM
O
As f
or l
evel
5 p
lus:
■Ab
ility
to
deal
wit
h al
lca
ses
incl
udin
g fu
ll ra
nge
of c
ompl
ex c
ases
in
asso
ciat
ion
wit
h ot
her
spec
ialis
ts i
nclu
ding
repr
oduc
tive
endo
crin
olog
y, i
nfer
tilit
y,gy
naec
olog
ical
mal
igna
ncy
■Fu
ll em
erge
ncy
serv
ices
■St
atew
ide
refe
rral
rol
e■
Und
ergr
adua
te a
nd p
ost
grad
uate
tea
chin
g ro
le■
Rese
arch
rol
e■
Gyn
aeco
logy
regi
stra
r/RM
O a
ndpo
ssib
ly r
egis
trar
s in
subs
peci
alti
es
Surg
ical
Ser
vice
s
clinicalframeworknew spread 21/9/05 3:14 PM Page 49
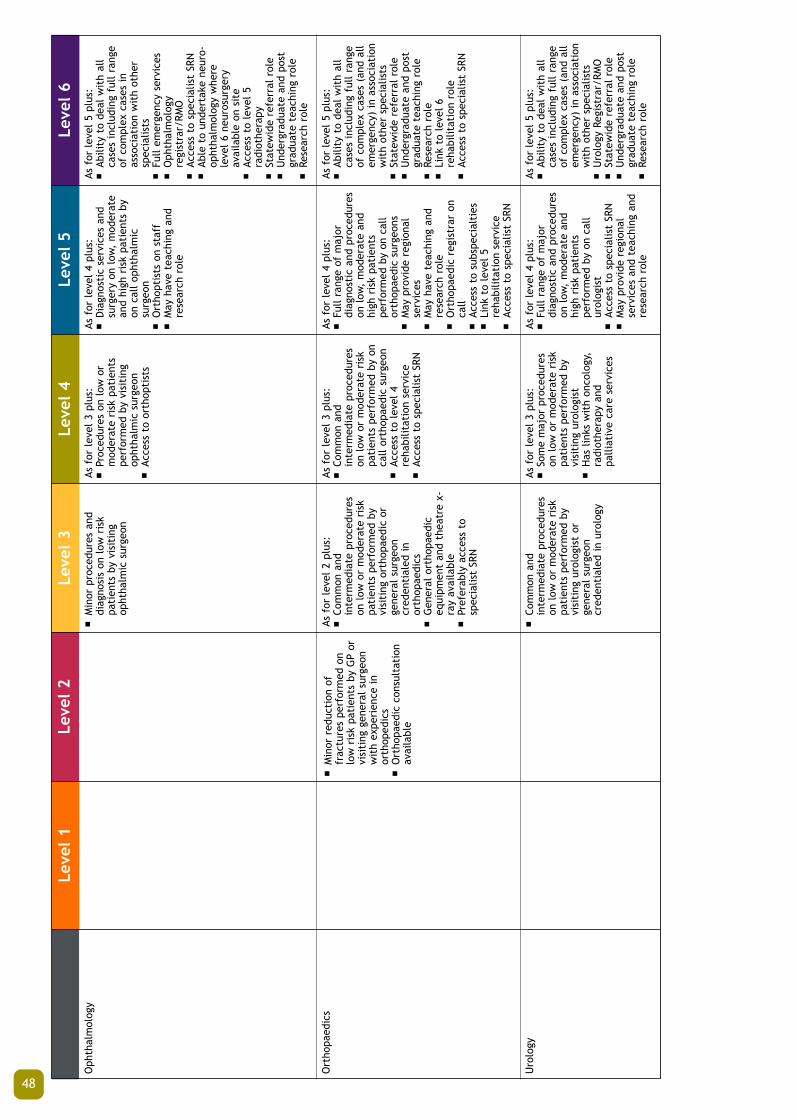
48
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
Oph
thal
mol
ogy
Ort
hopa
edic
s
Uro
logy
■M
inor
red
ucti
on o
ffr
actu
res
perf
orm
ed o
nlo
w r
isk
pati
ents
by
GP
orvi
siti
ng g
ener
al s
urge
onw
ith
expe
rien
ce i
nor
thop
edic
s■
Ort
hopa
edic
con
sult
atio
nav
aila
ble
■M
inor
pro
cedu
res
and
diag
nosi
s on
low
ris
kpa
tien
ts b
y vi
siti
ngop
htha
lmic
sur
geon
As f
or l
evel
2 p
lus:
■Co
mm
on a
ndin
term
edia
te p
roce
dure
son
low
or
mod
erat
e ri
skpa
tien
ts p
erfo
rmed
by
visi
ting
ort
hopa
edic
or
gene
ral
surg
eon
cred
enti
aled
in
orth
opae
dics
■G
ener
al o
rtho
paed
iceq
uipm
ent
and
thea
tre
x-ra
y av
aila
ble
■Pr
efer
ably
acc
ess
tosp
ecia
list
SRN
■Co
mm
on a
ndin
term
edia
te p
roce
dure
son
low
or
mod
erat
e ri
skpa
tien
ts p
erfo
rmed
by
visi
ting
uro
logi
st o
rge
nera
l su
rgeo
ncr
eden
tial
ed i
n ur
olog
y
As f
or l
evel
3 p
lus:
■Pr
oced
ures
on
low
or
mod
erat
e ri
sk p
atie
nts
perf
orm
ed b
y vi
siti
ngop
htha
lmic
sur
geon
■Ac
cess
to
orth
opti
sts
As f
or l
evel
3 p
lus:
■Co
mm
on a
ndin
term
edia
te p
roce
dure
son
low
or
mod
erat
e ri
skpa
tien
ts p
erfo
rmed
by
onca
ll or
thop
aedi
c su
rgeo
n■
Acce
ss t
o le
vel
4re
habi
litat
ion
serv
ice
■Ac
cess
to
spec
ialis
t SR
N
As f
or l
evel
3 p
lus:
■So
me
maj
or p
roce
dure
son
low
or
mod
erat
e ri
skpa
tien
ts p
erfo
rmed
by
visi
ting
uro
logi
st■
Has
lin
ks w
ith
onco
logy
,ra
diot
hera
py a
ndpa
lliat
ive
care
ser
vice
s
As f
or l
evel
4 p
lus:
■D
iagn
osti
c se
rvic
es a
ndsu
rger
y on
low
, m
oder
ate
and
high
ris
k pa
tien
ts b
yon
cal
l op
htha
lmic
surg
eon
■O
rtho
ptis
ts o
n st
aff
■M
ay h
ave
teac
hing
and
rese
arch
rol
e
As f
or l
evel
4 p
lus:
■Fu
ll ra
nge
of m
ajor
diag
nost
ic a
nd p
roce
dure
son
low
, m
oder
ate
and
high
ris
k pa
tien
tspe
rfor
med
by
on c
all
orth
opae
dic
surg
eons
■M
ay p
rovi
de r
egio
nal
serv
ices
■M
ay h
ave
teac
hing
and
rese
arch
rol
e■
Ort
hopa
edic
reg
istr
ar o
nca
ll ■
Acce
ss t
o su
bspe
cial
ties
■Li
nk t
o le
vel
5re
habi
litat
ion
serv
ice
■Ac
cess
to
spec
ialis
t SR
N
As f
or l
evel
4 p
lus:
■Fu
ll ra
nge
of m
ajor
diag
nost
ic a
nd p
roce
dure
son
low
, m
oder
ate
and
high
ris
k pa
tien
tspe
rfor
med
by
on c
all
urol
ogis
t■
Acce
ss t
o sp
ecia
list
SRN
■M
ay p
rovi
de r
egio
nal
serv
ices
and
tea
chin
g an
dre
sear
ch r
ole
As f
or l
evel
5 p
lus:
■Ab
ility
to
deal
wit
h al
lca
ses
incl
udin
g fu
ll ra
nge
of c
ompl
ex c
ases
in
asso
ciat
ion
wit
h ot
her
spec
ialis
ts■
Full
emer
genc
y se
rvic
es■
Oph
thal
mol
ogy
regi
stra
r/RM
O■
Acce
ss t
o sp
ecia
list
SRN
■Ab
le t
o un
dert
ake
neur
o-op
htha
lmol
ogy
whe
rele
vel
6 ne
uros
urge
ryav
aila
ble
on s
ite
■Ac
cess
to
leve
l 5
radi
othe
rapy
■St
atew
ide
refe
rral
rol
e■
Und
ergr
adua
te a
nd p
ost
grad
uate
tea
chin
g ro
le■
Rese
arch
rol
e
As f
or l
evel
5 p
lus:
■Ab
ility
to
deal
wit
h al
lca
ses
incl
udin
g fu
ll ra
nge
of c
ompl
ex c
ases
(an
d al
lem
erge
ncy)
in
asso
ciat
ion
wit
h ot
her
spec
ialis
ts■
Stat
ewid
e re
ferr
al r
ole
■U
nder
grad
uate
and
pos
tgr
adua
te t
each
ing
role
■Re
sear
ch r
ole
■Li
nk t
o le
vel
6re
habi
litat
ion
role
■Ac
cess
to
spec
ialis
t SR
N
As f
or l
evel
5 p
lus:
■Ab
ility
to
deal
wit
h al
lca
ses
incl
udin
g fu
ll ra
nge
of c
ompl
ex c
ases
(an
d al
lem
erge
ncy)
in
asso
ciat
ion
wit
h ot
her
spec
ialis
ts■
Uro
logy
Reg
istr
ar/R
MO
■St
atew
ide
refe
rral
rol
e■
Und
ergr
adua
te a
nd p
ost
grad
uate
tea
chin
g ro
le■
Rese
arch
rol
e
clinicalframeworknew spread 21/9/05 3:14 PM Page 50

49
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
Card
ioth
orac
ic
Vasc
ular
sur
gery
Neu
rosu
rger
y
■Co
mm
on m
inor
and
unco
mpl
icat
ed e
lect
ive
vasc
ular
sur
gery
■Pe
rfor
med
by
visi
ting
vasc
ular
or
gene
ral
surg
eons
■El
ecti
ve a
nd e
mer
genc
yth
orac
ic p
roce
dure
s by
visi
ting
/on
call
thor
acic
surg
eons
As f
or l
evel
3 p
lus:
■Co
mm
on,
inte
rmed
iate
and
som
e m
ajor
proc
edur
es o
n lo
w a
ndm
oder
ate
risk
pat
ient
spe
rfor
med
by
visi
ting
vasc
ular
sur
geon
s or
gene
ral
surg
eons
■
Pre-
oper
ativ
ere
habi
litat
ion
spec
ialis
tco
nsul
tant
ava
ilabl
e
■M
inor
hea
d in
juri
es d
ealt
wit
h by
gen
eral
sur
geon
■N
euro
surg
ical
con
sult
atio
nav
aila
ble
■O
pera
ting
equ
ipm
ent
adeq
uate
for
em
erge
ncy
neur
osur
gery
■Li
nk w
ith
leve
l 4
reha
bilit
atio
n se
rvic
es
As f
or l
evel
4 p
lus:
■El
ecti
ve a
nd e
mer
genc
yth
orac
ic a
nd e
lect
ive
card
ioth
orac
ic p
roce
dure
sby
vis
itin
g/on
cal
lca
rdio
thor
acic
sur
geon
s ■
Leve
l 5
reha
bilit
atio
nse
rvic
es a
vaila
ble
on s
ite
■Li
nk w
ith
palli
ativ
e ca
rean
d pa
in m
anag
emen
tse
rvic
es■
Acce
ss t
o sp
ecia
list
SRN
■So
me
regi
onal
ref
erra
lro
le■
ICU
/CCU
As f
or l
evel
4 p
lus:
■D
iagn
osti
c se
rvic
es a
ndsu
rger
y on
low
, m
oder
ate
and
high
ris
k pa
tien
ts b
yon
cal
l va
scul
ar o
r ge
nera
lsu
rgeo
n■
May
hav
e re
gion
al r
efer
ral
■M
ay h
ave
som
e te
achi
ngan
d tr
aini
ng a
nd r
esea
rch
role
■Li
nk w
ith
leve
l 5
reha
bilit
atio
n se
rvic
es
As f
or l
evel
4 p
lus:
■D
iagn
osti
c se
rvic
es a
ndsu
rger
y on
low
, m
oder
ate
and
high
ris
k pa
tent
s by
on c
all
neur
osur
geon
■D
esig
nate
d ne
uros
urgi
cal
beds
■Ac
cess
to
spec
ialis
t SR
N■
24 h
our
acce
ss t
o CT
■Li
nk w
ith
brai
n an
d sp
inal
inju
ry r
ehab
ilita
tion
■M
ay h
ave
som
e te
achi
ngan
d re
sear
ch r
ole
As f
or l
evel
5 p
lus:
■El
ecti
ve a
nd e
mer
genc
yth
orac
ic a
ndca
rdio
thor
acic
pro
cedu
res
by c
ardi
otho
raci
csu
rgeo
ns■
Able
to
deal
wit
h hi
ghly
com
plex
dia
gnos
is a
ndtr
eatm
ent
in a
ssoc
iati
onw
ith
othe
r sp
ecia
ltie
s■
Card
ioth
orac
icre
gist
rar/
RMO
■St
atew
ide
refe
rral
rol
e■
Und
ergr
adua
te a
nd p
ost
grad
uate
tea
chin
g ro
le■
Rese
arch
rol
e■
Leve
l 6
ICU
■To
inc
lude
hea
rt a
nd l
ung
tran
spla
ntat
ion
atse
lect
ed s
ites
As f
or l
evel
5 p
lus:
■Ab
ility
to
deal
wit
h al
lca
ses
incl
udin
g fu
ll ra
nge
of c
ompl
ex c
ases
in
asso
ciat
ion
wit
h ot
her
spec
ialis
ts■
Prov
ides
all
emer
genc
yse
rvic
es■
On
call
vasc
ular
sur
geon
■Ac
cess
to
spec
ialis
t SN
R■
Stat
ewid
e re
ferr
al r
ole
■U
nder
grad
uate
and
pos
tgr
adua
te t
each
ing
role
■Re
sear
ch r
ole
As f
or l
evel
5 p
lus:
■Ab
le t
o de
al w
ith
all
case
sin
clud
ing
all
emer
genc
yca
ses
■N
euro
surg
ical
war
d an
dne
uros
urgi
cal
high
depe
nden
cy/I
CU■
Neu
rosu
rger
yre
gist
rar/
RMO
■Li
nk w
ith
leve
l 5
reha
bilit
atio
n se
rvic
e■
Acce
ss t
o sp
ecia
list
SRN
■St
atew
ide
refe
rral
rol
e■
Und
ergr
adua
te a
nd p
ost
grad
uate
tea
chin
g ro
le■
Rese
arch
rol
e
clinicalframeworknew spread 21/9/05 3:14 PM Page 51

50
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
Plas
tics
Burn
s
Emer
genc
y D
epar
tmen
t
Urg
ent
Prim
ary
Care
■Ca
re i
s ca
rrie
d ou
t by
GPs
(pot
enti
ally
vis
itin
g) w
ith
or w
itho
ut t
he a
ssis
tanc
eof
RN
s de
pend
ing
on t
hety
pe o
f pa
tien
t ca
rene
eded
■Ba
sic
resu
scit
atio
neq
uipm
ent
and
drug
s
■M
inor
out
pati
ents
and
sam
e da
y pr
oced
ures
by
GP
■M
inor
out
pati
ent
and
sam
e da
y pr
oced
ures
onl
yby
GP
■Ab
le t
o pr
ovid
eem
erge
ncy
stab
ilisa
tion
serv
ice
for
burn
s
As f
or l
evel
1 p
lus:
■Li
mit
ed G
P co
ver
■Se
rvic
es b
y RN
■Re
susc
itat
ion
and
stab
ilisa
tion
cap
abili
ty
As f
or l
evel
2 p
lus:
■As
for
lev
el 2
but
proc
edur
es m
ay r
equi
revi
siti
ng p
last
ics
surg
eon
As f
or l
evel
2 p
lus:
■G
ener
al s
urge
on a
ble
topr
ovid
e se
rvic
es f
orm
inor
/mod
erat
e bu
rns
tosm
all
area
s of
bod
y
As f
or l
evel
2 p
lus:
■Lo
cal
GPs
ros
tere
d to
prov
ide
24 h
our
cove
rw
ith
serv
ice
by R
N■
Min
or p
roce
dure
capa
bilit
y■
Resu
scit
atio
n an
dst
abili
sati
on c
apab
ility
As f
or l
evel
3 p
lus:
■Se
lect
ed m
inor
proc
edur
es o
n lo
w a
ndm
oder
ate
risk
pat
ient
s by
visi
ting
pla
stic
sur
geon
s
As f
or l
evel
3 p
lus:
■G
ener
al s
urge
on p
rovi
ding
serv
ices
for
min
or/m
oder
ate
burn
s to
smal
l pa
rts
of b
ody
■Ac
cess
to
spec
ialis
t SN
R■
Link
s to
lev
el 4
reha
bilit
atio
n se
rvic
es
■Lo
cal
GPs
ros
tere
d to
prov
ide
24 h
our
cove
rw
ith
serv
ice
by R
N■
Emer
genc
y op
erat
ing
thea
tre
faci
litie
s■
Resu
scit
atio
n an
dst
abili
sati
on■
On-
call
gene
ralis
tsp
ecia
lists
■Ac
cess
to
spec
ialis
t SR
N
As f
or l
evel
4 p
lus:
■D
iagn
osti
c se
rvic
es a
ndsu
rger
y on
low
, m
oder
ate
and
high
ris
k pa
tent
s by
on c
all
plas
tic
surg
eons
■
Link
wit
h le
vel
5re
habi
litat
ion
serv
ices
■M
ay h
ave
som
e te
achi
ngan
d tr
aini
ng r
ole
■Vi
siti
ng b
urns
L6
spec
ialis
t
As f
or l
evel
4 p
lus:
■G
ener
al s
urge
on p
rovi
ding
serv
ices
for
min
or/m
oder
ate
burn
s to
smal
l pa
rts
of b
ody
■24
hou
r on
cal
l re
gist
rar
■Ac
cess
to
spec
ialis
t SR
N■
Link
s to
lev
el 5
reha
bilit
atio
n se
rvic
es
As f
or l
evel
4 p
lus:
■M
edic
ally
sta
ffed
24
hour
spe
r da
y■
Med
ical
and
sur
gica
l su
b-sp
ecia
lists
ava
ilabl
e on
-ca
ll■
Acce
pts
tran
sfer
s fr
omot
her
hosp
ital
s in
reg
ion
■Ac
cess
to
ICU
and
CCU
faci
litie
s ■
Acce
ss t
o sp
ecia
list
SRN
As f
or l
evel
5 p
lus:
■Ab
le t
o de
al w
ith
all
case
sin
clud
ing
all
emer
genc
yca
ses
■Pl
asti
cs r
egis
trar
/RM
O■
Acce
ss t
o sp
ecia
list
SRN
■St
atew
ide
refe
rral
rol
e■
Und
ergr
adua
te a
nd p
ost
grad
uate
tea
chin
g ro
le■
May
hav
e re
sear
ch r
ole
As f
or l
evel
5 p
lus:
■Fu
ll ra
nge
of b
urns
serv
ices
, w
ith
a sp
ecia
lbu
rns
unit
, in
clud
ing
all
emer
genc
y ca
ses
■24
hou
r on
cal
l co
ver
■St
atew
ide
refe
rral
rol
e■
Emer
genc
y ca
re s
ervi
ces
prov
ided
by
on c
all
spec
ialis
t■
Acce
ss t
o sp
ecia
list
SRN
■U
nder
grad
uate
and
pos
tgr
adua
te t
each
ing
role
■Re
sear
ch r
ole
As f
or l
evel
5 p
lus:
■Em
erge
ncy
med
icin
eco
nsul
tant
on
duty
24
hour
s pe
r da
y*■
Stat
ewid
e re
ferr
al r
ole
■Ac
cess
to
spec
ialis
t SR
N■
Back
up f
rom
ful
l ra
nge
ofm
edic
al a
nd s
urgi
cal
spec
ialis
ts a
nd d
iagn
osti
cse
rvic
es■
ICU
and
CCU
fac
iliti
es
Emer
genc
y/Tr
aum
a Se
rvic
es
* N
ot c
urre
ntly
ope
rati
ng i
n W
A
clinicalframeworknew spread 21/9/05 3:14 PM Page 52

51
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
Obs
tetr
ics
Paed
iatr
ics
■N
o pl
anne
d de
liver
ies
■An
tena
tal,
pos
t na
tal
care
is c
arri
ed o
ut b
y G
Ps(p
oten
tial
ly v
isit
ing)
wit
hor
wit
hout
the
ass
ista
nce
of R
N/R
M d
epen
ding
on
the
type
of
pati
ent
care
need
ed
■Ca
re i
s ca
rrie
d ou
t by
GPs
(pot
enti
ally
vis
itin
g) w
ith
or w
itho
ut t
he a
ssis
tanc
eof
RN
s de
pend
ing
on t
hety
pe o
f pa
tien
t ca
rene
eded
■St
abili
sati
on a
nd f
irst
aid
As f
or l
evel
1 p
lus:
■N
o pl
anne
d de
liver
ies
■In
pati
ent
care
fol
low
ing
deliv
ery
else
whe
re■
Ante
nata
l, p
ost
nata
l ca
reis
car
ried
out
by
GPs
wit
hor
wit
hout
the
ass
ista
nce
of R
N/R
M d
epen
ding
on
the
type
of
pati
ent
care
need
ed
As f
or l
evel
1 p
lus:
■Pa
edia
tric
med
ical
bed
s –
care
by
gene
ral
phys
icia
n■
On
call
paed
iatr
ic a
dvic
e■
No
surg
ery
As f
or l
evel
2 p
lus:
■Pl
anne
d de
liver
ies
of l
owri
sk m
othe
rs/b
abie
s■
Serv
ice
by G
Ps a
ndtr
aine
d m
id-w
ives
■LU
CS t
rans
ferr
edel
sew
here
but
mus
t be
wit
hin
safe
tim
efra
me
■Vi
siti
ng o
bste
tric
ian
■Ac
cess
to
Leve
l 1
Spec
ial
Care
Nur
sery
As f
or l
evel
2 p
lus:
■O
utpa
tien
t ca
re b
yvi
siti
ng p
aedi
atri
cian
■Li
mit
ed s
urge
ry b
y vi
siti
ngpa
edia
tric
sur
geon
or
surg
eon
wit
h pa
edia
tric
skill
s■
Day
sur
gery
,un
com
plic
ated
ele
ctiv
esu
rger
y an
d em
erge
ncy
surg
ery
■D
esig
nate
d pa
edia
tric
med
ical
war
d■
Inpa
tien
t m
edic
al c
are
byG
P or
gen
eral
phy
sici
an o
rpa
edia
tric
ian
As f
or l
evel
3 p
lus:
■Pl
anne
d de
liver
ies
of l
owan
d m
oder
ate
risk
mot
hers
/bab
ies
■Ac
cess
to
accr
edit
edob
stet
ric
and
paed
iatr
ictr
aine
d do
ctor
s■
Able
to
cope
wit
h su
dden
unex
pect
ed r
isks
■Ca
esar
ian
sect
ion
capa
bilit
y■
Acce
ss t
o Le
vel
2A S
peci
alCa
re N
urse
ry
As f
or l
evel
3 p
lus:
■O
utpa
tien
t ca
re b
yre
side
nt p
aedi
atri
cian
■Li
mit
ed s
urge
ry b
y vi
siti
ngpa
edia
tric
sur
geon
■D
ay s
urge
ry,
unco
mpl
icat
ed e
lect
ive
surg
ery
and
emer
genc
ysu
rger
y■
Des
igna
ted
med
ical
war
d■
Inpa
tien
t m
edic
al c
are
byvi
siti
ng p
aedi
atri
cian
■Ac
cess
to
spec
ialis
t SR
N■
Poss
ibly
Res
iden
t/RM
Oro
tati
ons
from
Lev
el 5
or
6 fa
cilit
y
As f
or l
evel
4 p
lus:
■D
eliv
erie
s of
low
,m
oder
ate
and
high
ris
km
othe
rs/b
abie
s■
Able
to
cope
wit
h m
ost
com
plic
atio
ns■
Serv
ice
prov
ided
by
spec
ialis
t ob
stet
rici
ans
and
paed
iatr
icia
ns t
o hi
ghri
sk p
atie
nts
■Re
gist
rar/
RMO
■Ac
cess
to
spec
ialis
tpa
edia
tric
ians
/obs
tetr
icia
ns a
nd t
rain
ed n
urse
s an
dal
lied
heal
th■
Regi
onal
ref
erra
l ro
le■
Acce
ss t
o Le
vel
2B S
peci
alCa
re N
urse
ry
As f
or l
evel
4 p
lus:
■In
pati
ent
and
outp
atie
ntca
re b
y re
side
ntpa
edia
tric
ian
■Re
gist
rar/
RMO
■Re
gion
al r
efer
ral
role
■So
me
unde
rgra
duat
ete
achi
ng■
Rang
e of
pae
diat
ric
surg
ery
■Re
side
nt p
aedi
atri
csu
rgeo
n■
24 h
our
on c
all
paed
iatr
ican
aest
heti
st■
Neo
nata
l IC
U
■Ac
cess
to
spec
ialis
t SR
N
As f
or l
evel
5 p
lus:
■Sp
ecia
list
obst
etri
c un
itfo
r st
ate
■O
bste
tric
reg
istr
ar a
ndm
idw
ives
tra
inin
g■
Acce
ss t
o sp
ecia
list
SRN
■24
hou
r co
ver
byob
stet
rici
ans
and
paed
iatr
icia
ns■
Acce
ss t
o Le
vel
3 Sp
ecia
lCa
re N
urse
ry
As f
or l
evel
5 p
lus:
■In
pati
ent
and
outp
atie
ntca
re b
y re
side
ntpa
edia
tric
ian
■Re
gist
rar/
RMO
■St
atew
ide
refe
rral
rol
e■
Und
ergr
adua
te a
ndpo
stgr
adua
te t
each
ing
role
■Fu
ll ra
nge
of p
aedi
atri
csu
rger
y■
Resi
dent
pae
diat
ric
surg
eon
■N
eona
tal
ICU
■O
pera
tes
in s
peci
alis
tfa
cilit
y■
Acce
ss t
o sp
ecia
list
SRN
Obs
tetr
ics
Serv
ices
Paed
iatr
ics
Serv
ices
clinicalframeworknew spread 21/9/05 3:14 PM Page 53

52
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
Neo
nato
logy
Reha
bilit
atio
n■
Visi
ting
con
sult
ativ
ese
rvic
es p
rovi
ded
onre
ques
t■
Care
is
carr
ied
out
by G
Ps(p
oten
tial
ly v
isit
ing)
wit
hor
wit
hout
the
ass
ista
nce
of R
Ns
depe
ndin
g on
the
type
of
pati
ent
care
need
ed
■O
bste
tric
ians
,pa
edia
tric
ians
and
anae
sthe
tist
s on
cal
l 24
hour
s■
Nor
mal
low
ris
kpr
egna
ncie
s an
dde
liver
ies
and
man
agem
ent
of n
ewbo
rns
> 36
wee
ks g
esta
tion
wit
hm
inim
al c
ompl
icat
ions
■Le
vel
1 Sp
ecia
l Ca
reN
urse
ry■
Basi
c lif
e su
ppor
t fo
rne
onat
es a
vaila
ble
wit
hac
cess
to
24 h
our
anae
sthe
tic
and
neon
atal
resu
scit
atio
n se
rvic
e
As f
or l
evel
1 p
lus:
■Re
gula
r vi
siti
ng s
ervi
ces
prov
ided
by
dist
rict
/reg
iona
l al
lied
heal
th s
taff
■Li
mit
ed l
evel
alli
ed h
ealt
hav
aila
bilit
y
As f
or l
evel
3 p
lus:
■O
bste
tric
ians
and
paed
iatr
icia
ns o
n ca
ll 24
hour
s■
Low
to
mod
erat
e ri
skpr
egna
ncie
s an
dde
liver
ies
and
man
agem
ent
of n
ewbo
rns
> 34
wee
ks g
esta
tion
wit
hm
inim
al c
ompl
icat
ions
■Le
vel
2A S
peci
al C
are
Nur
sery
wit
h lo
wde
pend
ency
pat
ient
s an
dlo
w-l
evel
Oxy
gen
ther
apy
and
airw
ay m
anag
emen
t■
Basi
c lif
e su
ppor
t fo
rne
onat
es a
vaila
ble
wit
hac
cess
to
24 h
ran
aest
heti
c an
d ne
onat
alre
susc
itat
ion
serv
ice
■Pr
ovid
es s
hort
-ter
mm
echa
nica
l ve
ntila
tion
(<6
hour
s) p
endi
ngtr
ansf
er
As f
or l
evel
3 p
lus:
■Fu
ll ti
me
sala
ried
phys
ioth
erap
y,oc
cupa
tion
al t
hera
py■
Spee
ch a
nd s
ocia
l w
ork
serv
ices
■D
istr
ict
refe
rral
rol
e■
Lim
ited
day
hos
pita
lpr
ogra
m
As f
or l
evel
4 p
lus:
■H
as a
cces
s to
clin
ical
and
diag
nost
ic p
aedi
atri
csu
bspe
cial
ties
■O
bste
tric
ians
and
paed
iatr
icia
ns o
n ca
ll 24
hour
s■
Med
ical
off
icer
(s)
on s
ite
24 h
ours
■M
oder
ate
to h
igh-
risk
preg
nanc
ies
and
deliv
erie
s an
dm
anag
emen
t of
new
born
s>
32 w
eeks
ges
tati
on w
ith
min
imal
com
plic
atio
ns■
Leve
l 2B
Spe
cial
Car
eN
urse
ry w
ith
high
depe
nden
cy p
atie
nts
and
prov
isio
n of
sho
rt t
erm
mec
hani
cal
vent
ilati
on (
<6
hour
s) p
endi
ng t
rans
fer
■Ac
cess
to
spec
ialis
t SR
N■
Mul
ti-d
isci
plin
ary
follo
wup
ser
vice
pro
vide
d■
Role
in
post
gra
duat
em
edic
al a
nd n
ursi
nged
ucat
ion
As f
or l
evel
4 p
lus:
■Re
hab
prog
ram
for
bot
hin
pati
ent
and
outp
atie
nt■
Link
ages
bet
wee
n re
gion
san
d de
sign
ated
met
ropo
litan
hos
pita
ls■
Hav
e a
day
hosp
ital
wit
h:■
Mem
ory
clin
ic■
Falls
Clin
ic■
Cont
inen
ce c
linic
■A
GEM
uni
t if
ED
ser
vice
sco
lloca
ted
■Pa
rt t
ime
serv
ices
of
Ger
iatr
icia
n1
■Re
hab
Spec
ialis
t w
ith
expe
rien
ced
RN/P
T/O
T/SP
/ D
ieti
tian
■Co
lloca
ted
wit
hps
ycho
geri
atri
c se
rvic
es
As f
or l
evel
5 p
lus:
■H
as a
cces
s to
clin
ical
and
diag
nost
ic p
aedi
atri
csu
bspe
cial
ties
■M
edic
al o
ffic
er(s
) on
sit
e24
hou
rs■
Hig
h-ri
sk,
high
depe
nden
cy p
regn
anci
esan
d de
liver
ies
■M
anag
emen
t of
new
born
s<
32 w
eeks
ges
tati
on■
Leve
l 3
Spec
ial
Care
Nur
sery
wit
h hi
ghde
pend
ency
pat
ient
s an
dpr
ovis
ion
of m
ediu
m -
long
term
mec
hani
cal
vent
ilati
on a
nd f
ull
life-
supp
ort
■U
nder
take
s ne
onat
alsu
rger
y an
d ca
re f
orco
mpl
ex c
onge
nita
l an
dm
etab
olic
dis
ease
s of
the
new
born
– n
ote
curr
entl
yat
PM
H■
Acce
ss t
o sp
ecia
list
SRN
■O
n-si
te m
ulti
-dis
cipl
inar
yse
rvic
es
■Ro
le i
n po
st g
radu
ate
med
ical
and
nur
sing
educ
atio
n■
Has
neo
nato
logy
res
earc
h
As f
or l
evel
5 p
lus:
■W
ill h
ave
GEM
uni
t■
Hav
e ac
cess
to
acut
e ca
re■
Full
tim
e re
hab
spec
ialis
t■
Full
tim
e ge
riat
rici
an a
spe
r fo
otno
te o
f le
vel
5■
Tert
iary
lev
el r
ehab
serv
ices
(St
atew
ide
Reha
bCe
ntre
) on
ly i
n on
e le
vel
6 ho
spit
al w
ith
a fu
ll ti
me
clin
ical
dir
ecto
r
Reha
bilit
atio
n Se
rvic
es
1G
eria
tric
ian
shou
ld i
deal
ly b
e fu
ll ti
me,
wit
h pa
rt t
ime
spen
t in
Lev
el 6
sup
port
ing
GEM
and
acu
te c
are,
and
par
t ti
me
in l
evel
5 s
uppo
rtin
g in
reh
abili
tati
on u
nit/
day
hosp
ital
and
GEM
uni
t.
clinicalframeworknew spread 21/9/05 3:14 PM Page 54

53
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
Com
mun
ity
asse
ssm
ent
Envi
ronm
enta
l H
ealt
h
Hea
lth
Prot
ecti
on i
nclu
ding
food
, ai
r, w
ater
, ra
diat
ion,
phar
mac
euti
cal,
pes
tici
des,
mos
quit
o bo
rne
dise
ases
.
Com
mun
icab
le D
isea
seCo
ntro
l
■In
clud
es f
ood
and
wat
erbo
rne
dise
ases
,va
ccin
atio
n pr
ogra
ms,
STI’s
, BB
V’s
and
arbo
vira
ldi
seas
es
Child
and
Com
mun
ity
Hea
lth
■Co
mm
unit
y H
ealt
hSe
rvic
es,
Scho
ol H
ealt
hSe
rvic
es,
Child
Hea
lth
Serv
ices
, Ch
ildD
evel
opm
ent
Serv
ices
Abor
igin
al H
ealt
h
Hea
lth
Prom
otio
n
■Pr
imar
y pr
even
tion
incl
udin
g lif
esty
ledi
seas
es a
nd i
njur
ypr
even
tion
■Vi
siti
ng s
ervi
ces
on a
sre
quir
ed b
asis
■Lo
cal
Gov
ernm
ent
resp
onsi
bilit
y w
ith
acce
ssto
DO
H s
tate
wid
e un
itw
hen
requ
ired
■Vi
siti
ng p
rim
ary
care
prov
ider
s, i
nclu
ding
GPs
and
Com
mun
ity
Hea
lth
Nur
ses
■Vi
siti
ng p
rim
ary
care
prov
ider
s, i
nclu
ding
GPs
and
Com
mun
ity
Hea
lth
Nur
ses
■Vi
siti
ng p
rim
ary
care
prov
ider
s
■Vi
siti
ng p
rim
ary
care
prov
ider
s w
ith
acce
ss t
oD
OH
sta
tew
ide
prog
ram
reso
urce
s. E
xpos
ure
tom
ass
med
ia c
ampa
igns
As f
or l
evel
1 p
lus:
■Re
side
nt p
rim
ary
care
prov
ider
sup
port
ing
stat
epr
ogra
ms
incl
udin
g G
Psan
d Co
mm
unit
y H
ealt
hN
urse
s
As f
or l
evel
1 p
lus:
■Re
side
nt p
rim
ary
care
prov
ider
s w
ith
acce
ss t
ost
atew
ide
prog
ram
init
iati
ves
As f
or l
evel
1 p
lus:
■M
ains
trea
m h
ealt
h se
rvic
epr
ovid
ers
(inc
ludi
ng G
Ps)
As f
or l
evel
1 p
lus:
■Re
gula
r vi
siti
ng s
ervi
cesu
ppor
ted
by l
imit
ed l
ocal
allie
d he
alth
As f
or l
evel
1 p
lus:
■As
sist
sta
tew
ide
serv
ices
inve
stig
atio
n of
loc
alin
cide
nts
As f
or l
evel
2 p
lus:
■M
ains
trea
m h
ealt
h se
rvic
epr
ovid
ers
As f
or l
evel
1 p
lus:
■Re
side
nt p
rim
ary
care
prov
ider
s w
ith
awar
enes
sof
sta
tew
ide
prog
ram
init
iati
ves
As f
or l
evel
3 p
lus:
■Vi
siti
ng s
ervi
ce s
uppo
rted
by l
ocal
alli
ed h
ealt
hpr
ofes
sion
als
■M
ost
disc
iplin
es a
vaila
ble
As f
or l
evel
3 p
lus:
■Co
ordi
nate
inv
esti
gati
ons
of l
ocal
inc
iden
tsAs
for
lev
el 2
plu
s:■
CDC
Nur
se i
n Po
pula
tion
Hea
lth
Uni
t
As f
or l
evel
2 p
lus:
■Co
mm
unit
y H
ealt
hCe
ntre
/Chi
ldD
evel
opm
ent
Cent
re
As f
or l
evel
3 p
lus:
■M
ains
trea
m p
rovi
ders
■Co
mm
unit
y co
ntro
lled
Abor
igin
al h
ealt
h se
rvic
e
As f
or l
evel
4 p
lus:
■H
ome
base
for
tea
m w
ith
regi
onal
/dis
tric
tre
spon
sibi
litie
s -
part
tim
e ge
riat
rici
an
As f
or l
evel
4 p
lus:
■Co
mpr
ehen
sive
mul
tidi
scip
linar
yPo
pula
tion
Hea
lth
Uni
t
As f
or l
evel
4 p
lus:
■Co
mpr
ehen
sive
mul
tidi
scip
linar
yPo
pula
tion
Hea
lth
Uni
tw
ith
dise
ase
cont
rol
doct
or a
nd c
apac
ity
to:
■In
vest
igat
e ca
ses/
outb
reak
s■
Perf
orm
con
tact
tra
cing
■Co
ordi
nate
reg
iona
lva
ccin
atio
n pr
ogra
ms
etc
As f
or l
evel
4 p
lus:
■Co
mpr
ehen
sive
mul
tidi
scip
linar
yPo
pula
tion
Hea
lth
Uni
tw
ith
com
mun
ity
heal
thst
aff
As f
or l
evel
4 p
lus:
■M
ains
trea
m p
rovi
ders
■
Com
mun
ity
cont
rolle
dAb
orig
inal
hea
lth
serv
ice
■In
tegr
ated
ser
vice
deliv
ery
As f
or l
evel
3 p
lus:
■Co
mpr
ehen
sive
mul
tidi
scip
linar
yPo
pula
tion
Hea
lth
Uni
tin
clud
ing
resi
dent
off
icer
sw
ith
heal
th p
rom
otio
ntr
aini
ng
As f
or l
evel
5 p
lus:
■St
atew
ide
prog
ram
,pl
anni
ng,
and
coor
dina
tion
rol
es■
Ded
icat
ed o
ffic
ers
wit
hst
atew
ide
resp
onsi
bilit
ies
and
legi
slat
ed s
ervi
cefu
ncti
ons
As f
or l
evel
5 p
lus:
■St
atew
ide
prog
ram
,pl
anni
ng,
and
coor
dina
tion
rol
es■
Ded
icat
ed o
ffic
ers
wit
hst
atew
ide
resp
onsi
bilit
ies
and
legi
slat
ed s
ervi
cefu
ncti
ons
As f
or l
evel
5 p
lus:
■St
atew
ide
Prog
ram
,pl
anni
ng,
and
coor
dina
tion
rol
es
As f
or l
evel
5 p
lus:
■St
atew
ide
prog
ram
,pl
anni
ng,
and
coor
dina
tion
rol
es■
Ded
icat
ed o
ffic
ers
wit
hst
atew
ide
resp
onsi
bilit
ies
As f
or l
evel
5 p
lus:
■St
atew
ide
prog
ram
,pl
anni
ng,
and
coor
dina
tion
rol
es■
Ded
icat
ed o
ffic
ers
wit
hst
atew
ide
resp
onsi
bilit
ies
Cont
inui
ng C
are
Serv
ices
Prev
enti
on a
nd P
rom
otio
n Se
rvic
es
clinicalframeworknew spread 21/9/05 3:14 PM Page 55

54
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
Brea
stsc
reen
■Sc
reen
ing
and
asse
ssm
ent
Cerv
ical
■H
ealt
h pr
omot
ion,
scre
enin
g aw
aren
ess,
mai
ntai
n ce
rvic
al c
ytol
ogy
regi
ster
Gen
omic
s
■Ed
ucat
ion,
res
earc
h
GP
base
d
Com
mun
ity
nurs
ing
Surg
ical
■Vi
siti
ng p
rim
ary
care
prov
ider
s
■Vi
siti
ng p
rim
ary
care
prov
ider
s w
ith
no s
peci
fic
prog
ram
■Vi
siti
ng G
P or
GP
byph
one
■So
me
visi
ting
alli
ed h
ealt
h■
Oth
er s
ervi
ces
such
as
child
hea
lth
and
post
nata
l ca
re b
y RN
■G
P on
ly
■Vi
siti
ng s
ervi
ce b
y m
obile
scre
enin
g un
it■
All
imag
es r
ead
bysp
ecia
list
radi
olog
ist
As f
or l
evel
1 p
lus:
■Vi
siti
ng p
rim
ary
care
prov
ider
s w
ith
acce
ss t
ost
atew
ide
educ
atio
n an
din
form
atio
n
As f
or l
evel
1 p
lus:
■G
P an
d sp
ecia
list
outp
atie
nt c
linic
at
disc
harg
e ho
spit
al■
Lim
ited
acc
ess
toge
nera
list
dom
icila
rynu
rsin
g
As f
or l
evel
2 p
lus:
■Fi
xed
site
scr
eeni
ng c
linic
As f
or l
evel
1 p
lus:
■Re
side
nt p
rim
ary
care
prov
ider
s, i
nclu
ding
GPs
As f
or l
evel
2 p
lus:
■Re
side
nt p
rim
ary
care
prov
ider
s w
ith
acce
ss t
ost
atew
ide
educ
atio
n an
din
form
atio
n
As f
or l
evel
1 p
lus:
■Re
side
nt G
Ps■
Som
e vi
siti
ng T
ype
Isp
ecia
lists
(ou
tpat
ient
s)■
Resi
dent
or
visi
ting
phys
ioth
erap
y■
Oth
er v
isit
ing
allie
dhe
alth
■O
ther
ser
vice
s by
RN
/CH
N(r
esid
ent)
As f
or l
evel
2 p
lus:
■Vi
siti
ng s
peci
alis
t■
Som
e ho
spit
alav
oida
nce/
hosp
ital
subs
titu
tion
■So
me
earl
y di
scha
rge
serv
ices
■Ac
cess
to
gene
ralis
tdo
mic
iliar
y nu
rsin
g an
dso
me
allie
d he
alth
As f
or l
evel
3 p
lus:
■Re
side
nt G
Ps■
Mos
t vi
siti
ng T
ype
I su
b-sp
ecia
lists
■M
ajor
ity
allie
d he
alth
avai
labl
e■
Resi
dent
com
mun
ity
nurs
ing
spec
ialis
t
As f
or l
evel
3 p
lus:
■Li
nks
wit
h H
ACC
■In
crea
sing
ran
ge a
ndco
mpl
exit
y of
hos
pita
lav
oida
nce/
subs
titu
tion
/ea
rly
disc
harg
e■
Chro
nic
dise
ase
prog
ram
s■
Visi
ting
med
ical
spe
cial
ist
■G
ood
acce
ss t
o ge
nera
list
allie
d he
alth
/nur
sing
sta
ff
As f
or l
evel
3 p
lus:
■As
sess
men
t by
an
expe
rien
ced
mul
tidi
scip
linar
y te
am o
fsc
reen
det
ecte
dab
norm
alit
ies
As f
or l
evel
3 p
lus:
■Pa
thol
ogy
labo
rato
ries
trai
ned
in t
he c
olla
tion
and
repo
rtin
g of
Cer
vica
lCy
tolo
gy R
egis
try
data
As f
or l
evel
4 p
lus:
■Re
side
nt G
Ps■
Resi
dent
som
e/al
l Ty
pe I
sub-
spec
ialis
ts■
Visi
ting
Typ
e II
sub-
spec
ialis
ts■
Full
rang
e of
alli
ed h
ealt
h■
Exte
nsiv
e co
mm
unit
y nu
rsin
g se
rvic
e
As f
or l
evel
4 p
lus:
■Sp
ecia
list
med
ical
/nur
sing
/ al
lied
heal
th s
taff
■In
crea
sed
rang
e an
dco
mpl
exit
y■
HAC
C in
tegr
atio
n■
Enha
nced
dia
gnos
tics
■Te
achi
ng a
nd t
rain
ing
role
As f
or l
evel
5 p
lus:
■St
atew
ide
prog
ram
,pl
anni
ng,
and
coor
dina
tion
rol
es■
Ded
icat
ed o
ffic
ers
wit
hst
atew
ide
resp
onsi
bilit
ies
As f
or l
evel
5 p
lus:
■St
atew
ide
Prog
ram
,pl
anni
ng,
and
coor
dina
tion
rol
es■
Ded
icat
ed o
ffic
ers
wit
hst
atew
ide
resp
onsi
bilit
ies
As f
or l
evel
5 p
lus:
■St
atew
ide
Prog
ram
,pl
anni
ng,
and
coor
dina
tion
rol
es■
Ded
icat
ed o
ffic
ers
wit
hst
atew
ide
resp
onsi
bilit
ies
As f
or l
evel
5 p
lus:
■Re
side
nt G
Ps■
Full
rang
e of
Typ
e I
and
IIsu
b-sp
ecia
lists
■Fu
ll ra
nge
of a
llied
hea
lth
■Ex
tens
ive
com
mun
ity
nurs
ing
serv
ice
■Re
sear
ch a
nd t
each
ing
role
As f
or l
evel
5 p
lus:
■Re
sear
ch r
ole
■Fu
lly i
nteg
rate
dam
bula
tory
car
e se
rvic
es■
Fully
int
egra
ted
diag
nost
ics
■In
clud
es r
egio
nal
suba
cute
cen
tre/
serv
ice
Prim
ary
Care
Ser
vice
s
Ambu
lato
ry C
are
Serv
ices
clinicalframeworknew spread 21/9/05 3:14 PM Page 56

55
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
Med
ical
Reha
bilit
atio
n
Cont
inui
ng C
are
Paed
iatr
ics
■G
P on
ly
■G
P on
ly
■G
P on
ly
■G
P on
ly
As f
or l
evel
1 p
lus:
■G
P an
d sp
ecia
list
outp
atie
nt c
linic
at
disc
harg
e ho
spit
al■
Lim
ited
acc
ess
toge
nera
list
dom
icila
rynu
rsin
g
As f
or l
evel
1 p
lus:
■G
P an
d sp
ecia
list
outp
atie
nt c
linic
at
disc
harg
e ho
spit
al■
Lim
ited
acc
ess
toge
nera
list
dom
icila
rynu
rsin
g
As f
or l
evel
1 p
lus:
■G
P an
d sp
ecia
list
outp
atie
nt c
linic
at
disc
harg
e ho
spit
al■
Lim
ited
acc
ess
toge
nera
list
dom
icila
rynu
rsin
g
As f
or l
evel
1 p
lus:
■G
P an
d sp
ecia
list
outp
atie
nt c
linic
at
disc
harg
e ho
spit
al■
Lim
ited
acc
ess
toge
nera
list
dom
icila
rynu
rsin
g
As f
or l
evel
2 p
lus:
■Vi
siti
ng s
peci
alis
t■
Som
e ho
spit
alav
oida
nce/
hosp
ital
subs
titu
tion
■So
me
earl
y di
scha
rge
serv
ices
■Ac
cess
to
gene
ralis
tdo
mic
iliar
y nu
rsin
g an
dso
me
allie
d he
alth
As f
or l
evel
2 p
lus:
■Vi
siti
ng s
peci
alis
t■
Som
e ho
spit
alav
oida
nce/
hosp
ital
subs
titu
tion
■So
me
earl
y di
scha
rge
serv
ices
■Ac
cess
to
gene
ralis
tdo
mic
iliar
y nu
rsin
g an
dso
me
allie
d he
alth
As f
or l
evel
2 p
lus:
■Vi
siti
ng s
peci
alis
t■
Som
e ho
spit
alav
oida
nce/
hosp
ital
subs
titu
tion
■So
me
earl
y di
scha
rge
serv
ices
■Ac
cess
to
gene
ralis
tdo
mic
iliar
y nu
rsin
g an
dso
me
allie
d he
alth
As f
or l
evel
2 p
lus:
■Vi
siti
ng s
peci
alis
t■
Som
e ho
spit
alav
oida
nce/
hosp
ital
subs
titu
tion
■So
me
earl
y di
scha
rge
serv
ices
■Ac
cess
to
gene
ralis
tdo
mic
iliar
y nu
rsin
g an
dso
me
allie
d he
alth
As f
or l
evel
3 p
lus:
■Li
nks
wit
h H
ACC
■In
crea
sing
ran
ge a
ndco
mpl
exit
y of
hos
pita
lav
oida
nce/
subs
titu
tion
/ea
rly
disc
harg
e■
Chro
nic
dise
ase
prog
ram
s■
Visi
ting
med
ical
spe
cial
ist
■G
ood
acce
ss t
o ge
nera
list
allie
d he
alth
/nur
sing
sta
ff
As f
or l
evel
3 p
lus:
■Li
nks
wit
h H
ACC
■In
crea
sing
ran
ge a
ndco
mpl
exit
y of
hos
pita
lav
oida
nce/
subs
titu
tion
/ea
rly
disc
harg
e■
Chro
nic
dise
ase
prog
ram
s■
Visi
ting
med
ical
spe
cial
ist
■G
ood
acce
ss t
o ge
nera
list
allie
d he
alth
/nur
sing
sta
ff
As f
or l
evel
3 p
lus:
■Li
nks
wit
h H
ACC
■In
crea
sing
ran
ge a
ndco
mpl
exit
y of
hos
pita
lav
oida
nce/
subs
titu
tion
/ea
rly
disc
harg
e■
Chro
nic
dise
ase
prog
ram
s■
Resi
dent
/vis
itin
g m
edic
alsp
ecia
list
■G
ood
acce
ss t
o ge
nera
list
allie
d he
alth
/nur
sing
sta
ff
As f
or l
evel
3 p
lus:
■In
crea
sing
ran
ge a
ndco
mpl
exit
y of
hos
pita
lav
oida
nce/
subs
titu
tion
/ea
rly
disc
harg
e■
Chro
nic
dise
ase
prog
ram
s■
Visi
ting
med
ical
spe
cial
ist
■G
ood
acce
ss t
o ge
nera
list
allie
d he
alth
/nur
sing
sta
ff
As f
or l
evel
4 p
lus:
■Sp
ecia
list
med
ical
/nu
rsin
g/ a
llied
hea
lth
staf
f■
Incr
ease
d ra
nge
and
com
plex
ity
■H
ACC
inte
grat
ion
■En
hanc
ed d
iagn
osti
cs■
Teac
hing
and
tra
inin
g ro
le
As f
or l
evel
4 p
lus:
■Sp
ecia
list
med
ical
/nu
rsin
g/al
lied
heal
th s
taff
■In
crea
sed
rang
e an
dco
mpl
exit
y■
HAC
C in
tegr
atio
n■
Enha
nced
dia
gnos
tics
■Te
achi
ng a
nd t
rain
ing
role
As f
or l
evel
4 p
lus:
■Sp
ecia
list
med
ical
/nur
sing
/ al
lied
heal
th s
taff
■In
crea
sed
rang
e an
dco
mpl
exit
y■
HAC
C in
tegr
atio
n■
Enha
nced
dia
gnos
tics
■Te
achi
ng a
nd t
rain
ing
role
As f
or l
evel
4 p
lus:
■Sp
ecia
list
med
ical
/nu
rsin
g/al
lied
heal
th s
taff
■In
crea
sed
rang
e an
dco
mpl
exit
y■
Enha
nced
dia
gnos
tics
■Te
achi
ng a
nd t
rain
ing
role
As f
or l
evel
5 p
lus:
■Re
sear
ch r
ole
■Fu
lly i
nteg
rate
dam
bula
tory
car
e se
rvic
es■
Fully
int
egra
ted
diag
nost
ics
■In
clud
es r
egio
nal
suba
cute
cen
tre/
serv
ice
As f
or l
evel
5 p
lus:
■Re
sear
ch r
ole
■Fu
lly i
nteg
rate
dam
bula
tory
car
e se
rvic
es■
Fully
int
egra
ted
diag
nost
ics
■In
clud
es r
egio
nal
suba
cute
cen
tre/
serv
ice
As f
or l
evel
5 p
lus:
■Re
sear
ch r
ole
■Fu
lly i
nteg
rate
dam
bula
tory
car
e se
rvic
es■
Fully
int
egra
ted
diag
nost
ics
■In
clud
es r
egio
nal
suba
cute
cen
tre/
serv
ice
As f
or l
evel
5 p
lus:
■Re
sear
ch r
ole
■Fu
lly i
nteg
rate
dam
bula
tory
car
e se
rvic
es■
Fully
int
egra
ted
diag
nost
ics
■In
clud
es r
egio
nal
suba
cute
cen
tre/
serv
ice
clinicalframeworknew spread 21/9/05 3:14 PM Page 57

56
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
Obs
tetr
ics
Men
tal
heal
th p
rom
otio
nan
d ill
ness
pre
vent
ion
Emer
genc
y se
rvic
es
(hos
pita
l ba
sed)
Inpa
tien
t se
rvic
es
■Co
mm
unit
y ba
sed
GP
wit
hor
wit
hout
com
mun
ity
nurs
ing
post
onl
y
■Pr
omot
ion
of m
enta
lhe
alth
in
the
com
mun
ity
■Eg
. Im
prov
ing
men
tal
heal
th l
iter
acy,
res
ourc
ece
ntre
s an
d st
igm
are
duct
ion
stra
tegi
es.
■Eg
. Ex
posu
re t
o m
ass
med
ia c
ampa
igns
As f
or l
evel
1 p
lus:
■N
o pl
anne
d de
liver
ies
■O
utpa
tien
t cl
inic
for
ante
nata
l an
d po
st n
atal
care
by
visi
ting
GP
obst
etri
cian
wit
h or
wit
hout
reg
iste
red
mid
wif
e ■
Lim
ited
acc
ess
toge
nera
list
dom
icili
ary
nurs
ing
care
As f
or l
evel
1 p
lus:
■U
nive
rsal
pre
vent
ion
■Id
enti
fica
tion
of
risk
fact
ors
for
men
tal
illne
ssan
d in
terv
enti
on a
t th
epo
pula
tion
lev
el b
efor
ein
itia
l on
set
of a
dis
orde
r■
Eg.
Prog
ram
s to
pre
vent
bully
ing
in s
choo
ls,
Auss
ieO
ptim
ism
. Tr
iple
P■
Eg.
Loca
l co
mm
unit
yac
tivi
ty t
hat
impr
oves
qual
ity
of l
ife
incl
udin
gM
enta
l H
ealt
h W
eek
As f
or l
evel
2 p
lus:
■G
P ob
stet
rici
an a
ndm
idw
ifer
y se
rvic
es■
Visi
ting
spe
cial
ist
obst
etri
cian
■
Out
pati
ent
clin
ic f
oran
tena
tal
and
post
nat
alca
re
■So
me
earl
y di
scha
rge
prog
ram
s■
Acce
ss t
o do
mic
iliar
ynu
rsin
g ca
re a
nd v
isit
ing
mid
wif
e■
Basi
c ul
tras
ound
and
path
olog
y se
rvic
es
As f
or l
evel
2 p
lus:
■Se
lect
ive
prev
enti
on■
Targ
etin
g po
pula
tion
grou
ps a
t ri
sk o
fde
velo
ping
a d
isor
der
topr
even
t it
s on
set
■Eg
. Su
ppor
t fo
r CO
PMI
■M
ains
trea
m p
rovi
ders
tele
phon
e su
ppor
t fr
omon
cal
l te
am m
embe
r/p
sych
iatr
ic e
mer
genc
yte
am
■G
ener
al h
ospi
tal
inpa
tien
tse
rvic
es w
itho
utde
sign
ated
men
tal
heal
thbe
ds,
prov
idin
g m
enta
lhe
alth
car
e fo
r vo
lunt
ary
pati
ents
adm
itte
d un
der
man
agem
ent
of G
P or
othe
r m
edic
al o
ffic
er
As f
or l
evel
3 p
lus:
■Sp
ecia
list
obst
etri
cian
■Ea
rly
disc
harg
e pr
ogra
ms
■H
ome
visi
ting
mid
wiv
es■
Dia
gnos
tic
ultr
asou
nd w
ith
spec
ialis
t ra
diol
ogis
tof
feri
ng a
nten
atal
scre
enin
g ■
Full
rang
e pa
thol
ogy
serv
ices
■Vi
siti
ng g
enet
ic s
ervi
ces
As f
or l
evel
3 p
lus:
■In
dica
ted
prev
enti
on■
Targ
etin
g hi
gh r
isk
indi
vidu
als
who
may
hav
ede
tect
able
sig
ns a
ndsy
mpt
oms
fore
shad
owin
gm
enta
l ill
ness
■Eg
. Su
icid
e pr
even
tion
stra
tegi
es
As f
or l
evel
3 p
lus:
■Li
mit
ed E
D m
enta
l he
alth
liais
on n
ursi
ng s
ervi
ce■
24 h
our
on c
all
liais
onps
ychi
atri
st m
edic
alse
rvic
e
As f
or l
evel
3 p
lus:
■Sp
ecia
l m
enta
l he
alth
care
sui
te w
ith
desi
gnat
edbe
ds■
Gen
eral
ly o
pera
ted
onde
man
d w
itho
utpe
rman
ent
staf
f (r
oom
ing
in s
ervi
ces)
■Fa
cilit
y is
una
utho
rise
d
As f
or l
evel
4 p
lus:
■Sp
ecia
list
obst
etri
cian
■Sp
ecia
lised
ant
enat
al a
ndpo
stna
tal
educ
atio
n an
dsu
ppor
t pr
ogra
ms
■Te
achi
ng a
nd t
rain
ing
role
■En
hanc
ed d
iagn
osti
cs
As f
or l
evel
4 p
lus:
■Ea
rly
inte
rven
tion
for
thos
e w
ith
earl
y si
gns
and
sym
ptom
s of
a m
enta
ldi
sord
er o
r a
firs
t ep
isod
eof
men
tal
illne
ss.
■Eg
. Ea
rly
epis
ode
psyc
hosi
s pr
ogra
ms
As f
or l
evel
4 p
lus:
■O
n du
ty E
D m
enta
l he
alth
liais
on n
ursi
ng s
ervi
ce■
On
duty
psy
chia
tris
tm
edic
al s
ervi
ce
As f
or l
evel
4 p
lus:
■D
edic
ated
acu
te m
enta
lhe
alth
hos
pita
l or
desi
gnat
ed m
enta
l he
alth
inpa
tien
t un
its
in a
cute
hosp
ital
s■
Psyc
hiat
rist
con
sult
atio
nav
aila
ble
and
on c
all
24ho
urs
■Co
mpr
ehen
sive
tea
m
As f
or l
evel
5 p
lus:
■Re
sear
ch r
ole
■St
ate
obst
etri
c su
ppor
tse
rvic
e/un
it (
SOSU
)■
Spec
ialis
t ob
stet
ric
serv
ices
inc
ludi
ngm
ater
nal
feta
l m
edic
ine
subs
peci
alty
, ob
stet
ric
med
icin
e, g
enet
icse
rvic
es■
Fully
int
egra
ted
ambu
lato
ry c
are
serv
ices
(soc
ial
wor
k,ps
ycho
logi
cal
med
icin
eet
c)■
Fully
int
egra
ted
diag
nost
ic s
ervi
ces
As f
or l
evel
5 p
lus:
■Re
laps
e pr
even
tion
for
thos
e id
enti
fied
wit
hm
enta
l ill
ness
■G
P(s)
and
loc
al m
enta
lhe
alth
tea
m m
embe
r(s)
wit
h vi
siti
ng p
sych
iatr
ist
■Eg
. Ch
ange
s (R
PH r
elap
sepr
even
tion
pro
gram
) an
dW
elln
ess
Reco
very
Act
ion
Plan
(W
RAP)
a c
onsu
mer
led
prog
ram
As f
or l
evel
5 p
lus:
■O
n du
ty E
D m
enta
l he
alth
liais
on n
ursi
ng s
ervi
ce■
On
duty
psy
chia
tris
tm
edic
al s
ervi
ce■
Acut
e ad
mis
sion
uni
tse
rvic
e
As f
or l
evel
5 p
lus:
■Sp
ecia
list
stat
ewid
ese
rvic
es p
rovi
ded
■A
stro
ng a
cade
mic
and
rese
arch
com
pone
nt i
nth
e se
rvic
e
Child
and
Ado
lesc
ents
Men
tal
Hea
lth,
Adu
lt M
enta
l H
ealt
h, O
lder
Per
sons
Men
tal
Hea
lth
Serv
ices
Men
tal
Hea
lth
Ambu
lato
ry C
are
Serv
ices
are
cov
ered
und
er M
enta
l H
ealt
h Se
rvic
es
clinicalframeworknew spread 21/9/05 3:14 PM Page 58

57
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
Com
mun
ity
clin
ical
bas
edse
rvic
es
Day
the
rapy
ser
vice
s(h
ospi
tal
base
d)
Com
mun
ity
non
clin
ical
supp
ort
prog
ram
s
Inte
rmed
iate
car
e
■Lo
cal
prim
ary
heal
thAs
for
lev
el 1
plu
s:■
Visi
ting
men
tal
heal
thpr
ofes
sion
al(s
)
■G
P an
d co
mm
unit
y he
alth
cent
re b
ased
scr
eeni
ngan
d ea
rly
dete
ctio
n of
men
tal
illne
ss■
Eg.
GPs
and
com
mun
ity
heal
th c
entr
es
As f
or l
evel
2 p
lus:
■Lo
cally
bas
ed m
enta
lhe
alth
tea
m■
Not
Mul
tidi
scip
linar
y
■So
me
limit
ed s
ervi
ces
As f
or l
evel
2 p
lus:
■N
on c
linic
al c
omm
unit
ysu
ppor
t (i
nclu
ding
psyc
hoso
cial
, di
sabi
lity,
recr
eati
onal
, an
d re
spit
eto
ind
ivid
uals
) in
the
irow
n ho
mes
and
the
com
mun
ity
up t
o 10
hou
rspe
r w
eek
■In
depe
nden
t liv
ing
prog
ram
(w
ith
supp
orti
vela
ndlo
rd)
■D
rop-
in c
entr
es a
ndfa
cilit
atin
g re
crea
tion
alac
tivi
ties
■
Care
r re
spit
e■
Care
r su
ppor
t an
ded
ucat
ion
■In
depe
nden
t liv
ing
skill
ssu
ppor
t■
They
do
not
all
rela
te t
ore
spit
e. T
his
is t
he r
ange
of c
omm
unit
y su
ppor
tse
rvic
es
■Cl
inic
ally
sup
ervi
sed
serv
ice
in p
erso
n’s
hom
e
As f
or l
evel
3 p
lus:
■Co
mm
unit
y m
enta
l he
alth
prog
ram
wit
hm
ulti
disc
iplin
ary
team
■Se
rvic
es g
ener
ally
prov
ided
dur
ing
core
busi
ness
hou
rs o
nly
■Li
mit
ed r
ange
ass
essm
ent
and
trea
tmen
t pr
ogra
ms
prov
ided
As f
or l
evel
3 p
lus:
■Li
mit
ed r
ange
of
day
ther
apy
serv
ices
As f
or l
evel
3 p
lus:
■N
on c
linic
al c
omm
unit
ysu
ppor
t up
to
30 h
ours
per
wee
k■
Psyc
hoso
cial
sup
port
■
Serv
ices
for
you
th a
t ri
skof
hom
eles
snes
s an
d lo
ngte
rm m
enta
l ill
ness
As f
or l
evel
3 p
lus:
■Cl
inic
ally
sup
ervi
sed
serv
ice
in a
fac
ility
or
pers
on’s
hom
e■
Sub
acut
e ca
re
As f
or l
evel
4 p
lus:
■Co
mm
unit
y m
enta
l he
alth
prog
ram
wit
hm
ulti
disc
iplin
ary
team
■7
day
a w
eek
cove
r ■
Exte
nsiv
e ra
nge
ofas
sess
men
t an
d tr
eatm
ent
prog
ram
s ■
Som
e lim
ited
aft
er h
ours
serv
ices
may
be
prov
ided
■Eg
. M
ulti
syst
emic
The
rapy
for
fam
ilies
■
Eg.
Inte
nsiv
e cl
inic
alre
habi
litat
ion
As f
or l
evel
4 p
lus:
■Ex
tens
ive
rang
e of
day
ther
apy
serv
ices
As f
or l
evel
4 p
lus:
■N
on c
linic
al c
omm
unit
ysu
ppor
t up
to
40 h
ours
per
wee
k■
Inte
nsiv
e di
sabi
lity
supp
ort
for
adul
ts a
t ri
skof
hom
eles
snes
s■
Cons
umer
res
pite
/cri
sis
care
■Su
ppor
ted
acco
mm
odat
ion
serv
ices
As f
or l
evel
4 p
lus:
■Cl
inic
ally
sta
ffed
24/
7■
Una
utho
rise
d fa
cilit
y■
Sub
acut
e ca
re
As f
or l
evel
5 p
lus:
■Co
mm
unit
y m
enta
l he
alth
prog
ram
wit
hm
ulti
disc
iplin
ary
team
prov
idin
g 24
hou
r/7
day
aw
eek
cove
r■
Spec
ialis
t st
atew
ide
derv
ices
pro
vide
d■
Eg.
Psyc
hiat
ric
emer
genc
yse
rvic
es■
Eg.
Spec
ialis
t re
side
ntia
lse
rvic
e■
Eg.
Fore
nsic
dis
char
gese
rvic
e
As f
or l
evel
5 p
lus:
■M
ulti
disc
iplin
ary
team
■St
atew
ide
or s
peci
alis
tre
ferr
al r
ole
As f
or l
evel
5 p
lus:
■N
on c
linic
al 2
4 ho
urm
enta
l he
alth
acco
mm
odat
ion
and
reha
bilit
atio
n in
resi
dent
ial
acco
mm
odat
ion
As f
or l
evel
5 p
lus:
■Cl
inic
ally
sta
ffed
24/
7■
Auth
oris
ed f
acili
ty■
Stat
ewid
e re
ferr
al r
ole
■Su
b ac
ute
care
clinicalframeworknew spread 21/9/05 3:14 PM Page 59

58
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
Fore
nsic
Mat
erna
l
Neu
rolo
gica
l
Alco
hol
and
Dru
g
Oth
er■
Eati
ng d
isor
der
■Sp
ecia
list
men
tal
heal
thpr
ogra
m w
ith
mul
tidi
scip
linar
y te
am■
Exte
nsiv
e ra
nge
ofas
sess
men
t an
d tr
eatm
ent
prog
ram
s in
clud
ing
fore
nsic
dis
char
ge a
ndac
com
mod
atio
n pr
ogra
m
■Sp
ecia
list
men
tal
heal
thpr
ogra
m w
ith
mul
tidi
scip
linar
y te
am■
Exte
nsiv
e ra
nge
ofas
sess
men
t an
d tr
eatm
ent
prog
ram
s
■Sp
ecia
list
men
tal
heal
thpr
ogra
m w
ith
mul
tidi
scip
linar
y te
am■
Exte
nsiv
e ra
nge
ofas
sess
men
t an
d tr
eatm
ent
prog
ram
s
■Sp
ecia
list
men
tal
heal
thpr
ogra
m w
ith
mul
tidi
scip
linar
y te
am■
Exte
nsiv
e ra
nge
ofas
sess
men
t an
d tr
eatm
ent
prog
ram
s
■Sp
ecia
list
men
tal
heal
thpr
ogra
m w
ith
mul
tidi
scip
linar
y te
am■
Exte
nsiv
e ra
nge
ofas
sess
men
t an
d tr
eatm
ent
prog
ram
s
As f
or l
evel
5 p
lus:
■Sp
ecia
list
stat
ewid
ein
pati
ent
serv
ices
prov
ided
■A
stro
ng a
cade
mic
and
rese
arch
com
pone
nt i
nth
e se
rvic
e
As f
or l
evel
5 p
lus:
■Sp
ecia
list
stat
ewid
ein
pati
ent
serv
ices
prov
ided
■A
stro
ng a
cade
mic
and
rese
arch
com
pone
nt i
nth
e se
rvic
e
As f
or l
evel
5 p
lus:
■Sp
ecia
list
stat
ewid
ein
pati
ent
serv
ices
prov
ided
■In
clud
es A
BI a
ndin
telle
ctua
l di
sabi
lity
■A
stro
ng a
cade
mic
and
rese
arch
com
pone
nt i
nth
e se
rvic
e
As f
or l
evel
5 p
lus:
■Sp
ecia
list
stat
ewid
ein
pati
ent
serv
ices
prov
ided
As f
or l
evel
5 p
lus:
■Sp
ecia
list
stat
ewid
ein
pati
ent
serv
ices
prov
ided
■A
stro
ng a
cade
mic
and
rese
arch
com
pone
nt i
nth
e se
rvic
e
Stat
ewid
e M
enta
l H
ealt
h Se
rvic
es
Spec
ialis
t de
sign
ed m
enta
l he
alth
ser
vice
s fo
r pe
ople
wit
h m
enta
l di
sord
ers
and
men
tal
heal
th p
robl
ems
whi
ch,
due
to a
ran
ge o
f fa
ctor
s in
clud
ing
tech
nica
l sp
ecia
lty,
hig
h co
st,
high
lev
el o
f cl
ient
nee
d an
d sm
all
clie
nt p
opul
atio
n, a
re p
rovi
ded
on a
sta
tew
ide
basi
s
clinicalframeworknew spread 21/9/05 3:14 PM Page 60

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
59
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
Path
olog
y
Radi
olog
y
Phar
mac
y
■Sp
ecim
en c
olle
ctio
n by
RN■
Spec
imen
s tr
ansm
itta
l to
refe
rral
lab
orat
ory
■Se
rvic
e ov
ersi
ght
byph
arm
acis
t lo
cate
del
sew
here
■D
rugs
sup
plie
d on
indi
vidu
al p
resc
ript
ion
from
com
mun
ity
phar
mac
y
As f
or l
evel
1 p
lus:
■Sp
ecim
en c
olle
ctio
n by
RN
■Sp
ecim
ens
tran
smit
tal
to r
efer
ral
labo
rato
ry
■M
obile
ser
vice
and
lim
ited
to x
-ray
of
extr
emit
ies,
ches
t, a
bdom
en■
Inte
rpre
ted
by o
nsit
edo
ctor
/hea
lth
prof
essi
onal
As f
or l
evel
1 p
lus:
■Vi
siti
ng p
harm
acis
t fr
omre
gion
al h
ospi
tal
■M
inim
al c
linic
al s
ervi
ce■
Staf
f ed
ucat
ion
■D
rugs
pro
vide
d by
regi
onal
hos
pita
l
As f
or l
evel
2 p
lus:
■Sp
ecim
en c
olle
ctio
n by
RN
for
tra
nsm
itta
l to
re
ferr
al l
abor
ator
y■
Able
to
perf
orm
a d
efin
edra
nge
urge
nt t
ests
As f
or l
evel
2 p
lus:
■As
lev
el 2
, pl
us h
as o
nsi
te d
esig
nate
d ro
om
■Ra
diog
raph
er i
nat
tend
ance
who
has
regu
lar
acce
ss t
ora
diol
ogic
al c
onsu
ltat
ion
■Si
mpl
e ul
tras
ound
capa
city
for
foe
tal
mon
itor
ing
■Te
lera
diol
ogy
faci
lity
avai
labl
e
As f
or l
evel
2 p
lus:
■At
lea
st o
ne p
harm
acis
tem
ploy
ed f
ull
tim
e■
Phar
mac
y dr
ug p
urch
asin
gan
d di
stri
buti
on t
oin
pati
ents
in
acco
rdan
cew
ith
stat
e dr
ug p
olic
ies
and
form
ular
y■
May
pro
vide
pha
rmac
yun
derg
radu
ate
and
post
grad
uate
tea
chin
gro
le■
May
hav
e re
gion
al r
ole
As f
or l
evel
3 p
lus:
■Pe
rfor
ms
rang
e of
bas
ic
test
s■
May
hav
e bl
ood
gas
anal
yser
■Bl
ood
bank
■Se
rvic
es s
urro
undi
ng
■Fu
ll ti
me
labo
rato
ryte
chno
logi
sts
As f
or l
evel
3 p
lus:
■As
lev
el 3
, w
ith
faci
litie
sfo
r ge
nera
l an
dfl
uoro
scop
y, i
n ad
diti
on t
om
obile
CD
for
war
ds,
OR
and
ED■
Auto
film
pro
cess
ing
capa
city
■M
obile
im
age
inte
nsif
ier
in O
R an
d/or
ICU
/CCU
■St
aff
radi
ogra
pher
on
call
24 h
ours
■Vi
siti
ng s
peci
alis
tra
diol
ogic
al a
ppoi
ntm
ent
■Al
way
s ha
s ul
tras
ound
■
May
hav
e CT
sca
nner
■Re
gist
ered
nur
se a
sre
quir
ed■
Tele
radi
olog
y fa
cilit
yav
aila
ble
As f
or l
evel
3 p
lus:
■M
ore
than
one
pha
rmac
ist
empl
oyed
■
Emer
genc
y af
ter
hour
son
-cal
l se
rvic
e■
Lim
ited
clin
ical
pha
rmac
yse
rvic
e to
inp
atie
nts
■Li
mit
ed o
utpa
tien
tsdi
spen
sing
■D
evel
ops
loca
l dr
ugpo
licie
s■
Part
icip
ates
in
hosp
ital
com
mit
tees
■M
ay p
rovi
de p
harm
acy
unde
rgra
duat
e an
dpo
stgr
adua
te t
each
ing
role
■M
ay h
ave
regi
onal
rol
e
As f
or l
evel
4 p
lus:
■24
hou
r on
sit
e se
rvic
e■
Path
olog
y de
part
men
t■
Full
tim
e pa
thol
ogis
t■
Mic
robi
olog
y an
dhi
stop
atho
logy
ava
ilabl
e■
Regi
onal
ref
erra
l ro
le
As f
or l
evel
4 p
lus:
■As
Lev
el 4
plu
ses
tabl
ishe
d D
epar
tmen
t■
Full
ultr
asou
nd■
Has
rad
iolo
gist
in
char
ge■
May
hav
e ra
diol
ogy
regi
stra
r■
Has
reg
iste
red
nurs
e 24
hour
on
site
ser
vice
for
urge
nt x
-ray
s■
CT s
cann
er o
n si
te o
rlo
cally
ava
ilabl
e■
PACs
ava
ilabl
e■
Poss
ible
MRI
As f
or l
evel
4 p
lus:
■6
day
serv
ice
and
on c
all
serv
ice
■In
pati
ent
and
outp
atie
ntse
rvic
es■
Dru
g in
form
atio
n■
Exte
nsiv
e cl
inic
alph
arm
acy
serv
ice
toin
pati
ents
■In
trav
enou
s ad
diti
vean
d/or
cyt
otox
ic d
rug
prep
arat
ion
■
Exte
mpo
rane
ous
disp
ensi
ng■
Supp
ort
for
clin
ical
tri
als
■U
nder
grad
uate
and
post
grad
uate
pha
rmac
yte
achi
ng r
ole
■M
ay h
ave
regi
onal
rol
e
As f
or l
evel
5 p
lus:
■St
atew
ide
refe
rral
rol
e■
Teac
hing
and
res
earc
hro
le■
Spec
ialis
t re
gist
rar
intr
aini
ng
As f
or l
evel
5 p
lus:
■As
lev
el 5
, pl
us s
peci
alro
oms
for
digi
tal
angi
ogra
phy,
neur
orad
iolo
gy e
tc■
CT s
can
and
full
ultr
asou
nd s
ervi
ceav
aila
ble
24 h
ours
■Al
way
s ha
s M
RI a
nd d
igit
alan
giog
raph
y■
Has
rad
iolo
gy r
egis
trar
and
post
gra
duat
e fe
llow
s■
Perf
orm
s in
vasi
vepr
oced
ures
■PA
Cs a
vaila
ble
As f
or l
evel
5 p
lus:
■7
day
serv
ice
■24
hou
r on
-cal
l se
rvic
e■
Spec
ialis
t ph
arm
acis
tpo
siti
ons
eg o
ncol
ogy,
card
iolo
gy,
paed
iatr
ics,
geri
atri
cs,
psyc
hiat
ry,
drug
inf
orm
atio
n ■
Invo
lved
in
rese
arch
,cl
inic
al t
rial
s, c
linic
alre
view
, D
UE’
s,
■Pr
ovid
e un
derg
radu
ate
and
post
grad
uate
teac
hing
rol
e■
Prod
uct
eval
uati
on w
ith
drug
use
/pol
icy
deve
lopm
ent
Clin
ical
Sup
port
Ser
vice
s
clinicalframeworknew spread 21/9/05 3:14 PM Page 61

60
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
ICU
/HD
U
Paed
iatr
ic I
CU
■H
igh
depe
nden
cy a
rea
for
gene
ral
war
d pa
tien
tsre
quir
ing
obse
rvat
ion
over
and
abov
e th
at a
vaila
ble
in g
ener
al w
ard
area
As f
or l
evel
3 p
lus:
■Pr
ovid
es b
asic
,m
ulti
syst
em l
ife
supp
ort
usua
lly f
or l
ess
than
a 2
4ho
ur p
erio
d■
Able
to
prov
ide
mec
hani
cal
vent
ilati
onan
d si
mpl
e ca
rdio
vasc
ular
mon
itor
ing
for
a pe
riod
of
at l
east
sev
eral
hou
rs,
orca
re o
f a
sim
ilar
natu
re■
Spec
ialis
t RN
■Ac
cess
to
spec
ialis
t SR
N
As f
or l
evel
4 p
lus:
■Pr
ovid
es c
ompl
ex,
mul
tisy
stem
lif
e su
ppor
t■
Able
to
prov
ide
mec
hani
cal
vent
ilati
on,
extr
acor
pore
al r
enal
supp
ort
serv
ices
and
inva
sive
car
diov
ascu
lar
mon
itor
ing
for
a pe
riod
of
at l
east
sev
eral
day
s, o
rfo
r lo
nger
per
iods
in
rem
ote
area
s or
car
e of
asi
mila
r na
ture
■Sp
ecia
list
RN■
Acce
ss t
o sp
ecia
list
SRN
As f
or l
evel
5 p
lus:
■Pr
ovid
es c
ompl
ex,
mul
tisy
stem
lif
e su
ppor
tfo
r an
ind
efin
ite
peri
od■
Tert
iary
ref
erra
l ce
ntre
for
pati
ents
in
need
of
inte
nsiv
e ca
re s
ervi
ces
■H
ave
exte
nsiv
e ba
ckup
labo
rato
ry a
nd c
linic
alse
rvic
e fa
cilit
ies
tosu
ppor
t th
e te
rtia
ryre
ferr
al r
ole
■Ab
le t
o pr
ovid
em
echa
nica
l ve
ntila
tion
,ex
trac
orpo
real
ren
alsu
ppor
t se
rvic
es a
ndin
vasi
ve c
ardi
ovas
cula
rm
onit
orin
g fo
r an
inde
fini
te p
erio
d, o
r ca
reof
a s
imila
r na
ture
■
Spec
ialis
t RN
■Ac
cess
to
spec
ialis
t SR
N
As f
or l
evel
5 p
lus:
■Pr
ovid
es c
ompl
ex,
mul
tisy
stem
lif
e su
ppor
tfo
r an
ind
efin
ite
peri
od■
Tert
iary
ref
erra
l ce
ntre
for
child
ren
need
ing
inte
nsiv
e ca
re■
Hav
e ex
tens
ive
back
upla
bora
tory
and
clin
ical
serv
ice
faci
litie
s to
supp
ort
this
ter
tiar
y ro
le■
Able
to
prov
ide
mec
hani
cal
vent
ilati
on,
extr
acor
pore
al r
enal
supp
ort
serv
ices
and
inva
sive
car
diov
ascu
lar
mon
itor
ing
for
anin
defi
nite
per
iod
toin
fant
s an
d ch
ildre
n le
ssth
an 1
6 ye
ars
of a
ge,
orca
re o
f a
sim
ilar
natu
re■
Spec
ialis
t RN
■Ac
cess
to
spec
ialis
t SR
N
clinicalframeworknew spread 21/9/05 3:14 PM Page 62

61
Leve
l 1
Leve
l 2
Leve
l 3
Leve
l 4
Leve
l 5
Leve
l 6
CCU
Anae
sthe
tics
Ope
rati
ng T
heat
res
Trai
ning
and
Res
earc
h
■An
alge
sia/
min
imal
seda
tion
ava
ilabl
e by
visi
ting
med
ical
off
icer
As f
or l
evel
1 p
lus:
■M
inor
pro
cedu
reca
pabi
lity
no e
mer
genc
yop
erat
ing
thea
tre
As f
or l
evel
1 p
lus:
■Li
mit
ed –
pos
sibl
e m
edic
alst
uden
t w
ith
visi
ting
GP
As f
or l
evel
2 p
lus:
■G
ener
al A
naes
thet
ics
onlo
w r
isk
pati
ents
giv
en G
Pan
aest
heti
sts
or g
ener
alan
aest
heti
st■
May
hav
e vi
siti
ngsp
ecia
list
anae
sthe
tist
As f
or l
evel
2 p
lus:
■Si
ngle
ope
rati
ng t
heat
refo
r m
inor
/sam
e da
ypr
oced
ures
■24
hou
r co
ver
for
caes
aria
n se
ctio
n if
perf
orm
ing
obst
etri
cs
As f
or l
evel
2 p
lus:
■So
me
med
ical
nur
sing
and
allie
d he
alth
tra
inin
g
As f
or l
evel
3 p
lus:
■Ab
le t
o su
pply
cri
tica
lca
re e
xper
tise
for
coro
nary
pat
ient
s■
Prov
ides
a l
evel
of
care
mor
e in
tens
ive
than
war
dba
sed
care
■D
iscr
ete
area
wit
hin
the
heal
th f
acili
ty (
may
be
com
bine
d w
ithi
n an
ICU
or H
DU
)■
Non
inv
asiv
e m
onit
orin
g■
Can
prov
ide
resu
scit
atio
nan
d st
abili
sati
on o
fem
erge
ncie
s un
til
tran
sfer
or r
etri
eval
to
a ba
ck u
pfa
cilit
y■
Spec
ialis
t RN
■Ac
cess
to
spec
ialis
t SR
N■
Form
al l
ink
wit
h pu
blic
or
priv
ate
heal
th f
acili
ty(s
)fo
r pa
tien
t re
ferr
al a
ndtr
ansf
er t
o/fr
om a
hig
her
leve
l of
ser
vice
, to
ens
ure
safe
ser
vice
pro
visi
on
As f
or l
evel
3 p
lus:
■G
ener
al a
naes
thet
ics
onlo
w r
isk
pati
ents
giv
en b
yac
cred
ited
med
ical
prac
titi
oner
■Sp
ecia
list
anae
sthe
tist
appo
inte
d fo
rco
nsul
tati
on a
nd t
opr
ovid
e se
rvic
e fo
rm
oder
ate
risk
pat
ient
s■
Spec
ific
ope
rati
ng r
oom
anae
sthe
tic
staf
f su
ppor
tav
aila
ble
As f
or l
evel
3 p
lus:
■M
ore
than
one
ope
rati
ngth
eatr
e/pr
oced
ure
room
■Se
para
te r
ecov
ery
■Ac
cred
ited
med
ical
prac
titi
oner
pro
vidi
ngan
aest
heti
c se
rvic
es■
Spec
ialis
t RN
■Ac
cess
to
spec
ialis
t SR
N
As f
or l
evel
3 p
lus:
■So
me
regi
star
and
resi
dent
tra
inin
g■
Som
e sp
ecia
list
nurs
ing
and
allie
d he
alth
tra
inin
g ■
Poss
ibly
col
labo
rati
vere
sear
ch
As f
or l
evel
4 p
lus:
■Ab
le t
o pr
ovid
e ad
diti
onal
mon
itor
ing
capa
city
(cen
tral
mon
itor
ing
atst
aff
stat
ion)
for
car
diac
pati
ents
and
inc
reas
edm
edic
al a
nd n
ursi
ngsu
ppor
t■
Spec
ialis
t RN
■Ac
cess
to
spec
ialis
t SR
N■
As f
or C
CU s
ervi
ce l
evel
4pl
us:
■Be
dsid
e an
d ce
ntra
lm
onit
orin
g ca
paci
ty(a
ble
to m
onit
orpa
tien
ts a
t th
e st
aff
stat
ion)
As f
or l
evel
4 p
lus:
■Sp
ecia
list
anae
sthe
tist
on
24 h
our
rost
er f
or l
ow,
mod
erat
e an
d hi
gh r
isk
pati
ents
■N
omin
ated
spe
cial
ist
dire
ctor
of
anae
sthe
tic
staf
f■
Anae
sthe
tic
regi
stra
r on
site
24
hour
s
As f
or l
evel
4 p
lus:
■Sp
ecia
list
anae
sthe
tist
on
24 h
our
rost
er f
or l
ow,
mod
erat
e an
d hi
gh r
isk
pati
ents
■M
edic
al o
ffic
er o
n si
te 2
4ho
urs
■Ac
cess
to
ICU
■Sp
ecia
list
RN■
Acce
ss t
o sp
ecia
list
SRN
As f
or l
evel
4 p
lus:
■Sm
all
rese
arch
uni
t ■
Spec
ialis
t tr
aini
ng f
ornu
rsin
g an
d al
lied
heal
th■
Som
e in
tern
, re
side
nt a
ndre
gist
ar t
rain
ing
As f
or l
evel
5 p
lus:
■Pr
ovid
es f
ull
rang
e of
card
iac
mon
itor
ing
(inc
ludi
ng i
nvas
ive
mon
itor
ing)
for
car
diac
pati
ents
■Fu
ll ca
rdio
logy
sup
port
incl
udin
g 24
hou
r on
cal
lec
hoca
rdio
grap
hy,
angi
ogra
phy,
ang
iopl
asty
and
perm
anen
tpa
cem
aker
ser
vice
s■
Spec
ialis
t RN
■Ac
cess
to
spec
ialis
t SR
N■
As f
or C
CU s
ervi
ce l
evel
5pl
us:
■In
vasi
ve c
ardi
ovas
cula
rm
onit
orin
g(i
ndef
init
ely)
■H
ighe
st l
evel
ref
erra
lce
ntre
for
CCU
pat
ient
sw
ith
acti
ve l
iais
on w
ith
low
er l
evel
cri
tica
l ca
rese
rvic
es f
or r
efer
rals
and
tran
sfer
of
pati
ents
to e
nsur
e sa
fe s
ervi
cepr
ovis
ion
As f
or l
evel
5 p
lus:
■24
spe
cial
ist
anae
sthe
tist
rost
er■
Sub
spec
ialis
ts,
rese
arch
and
teac
hing
of
grad
uate
san
d un
derg
radu
ates
■24
hou
r on
sit
ean
aest
heti
c re
gist
rar
■Te
achi
ng a
nd r
esea
rch
role
As f
or l
evel
5 p
lus:
■M
ulti
ple
oper
atin
gth
eatr
es a
nd p
roce
dure
room
s■
Maj
or a
nd c
ompl
expr
oced
ures
(car
diot
hora
cic
and
tran
spla
nt)
■Te
achi
ng a
nd r
esea
rch
role
■Sp
ecia
list
RN■
Acce
ss t
o sp
ecia
list
SRN
As f
or l
evel
5 p
lus:
■Ac
adem
ic U
nit
Rese
arch
Inst
itut
e■
Full
trai
ning
pro
gram
at
all
leve
ls■
Form
al t
rain
ing
links
wit
hth
e un
iver
siti
es
clinicalframeworknew spread 21/9/05 3:14 PM Page 63

62
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
clinicalframeworknew spread 21/9/05 3:14 PM Page 64

WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
63
Appendix 2 - WACHS Clinical Services Delineation Matrix
Regional Resource Centres (1)
Integrated District Health Services (2)
Hospitals in Small Towns (3)
Level* Level* Level*
Medical Services
Surgical Services
Emergency TraumaServices
Obstetric Services
Paediatric Services
Rehabilitation Services
Prevention andPromotion Services
Primary Care Services
Ambulatory CareServices
Mental Health Services
Clinical Support
4
4
4
4
3/4
4/5
5
4/5
4
3/4
3/4
2/3
2/3
2/3
2/3
2
3
3/4
3
2/3/4
2/3
2/3
1/2
1/2
1/2
1/2
1
1
1/2/3/4
1/3
1/2
1/2
1
■ This is an approximate guide to the services WACHS aims to provide at each hospital. The full range ofservices denoted by each level may not be available at all sites.
■ * the level of service is defined in the Clinical Services Consultation 2005 paper.
■ The key refers to the Centres, Services and Hospitals as per above table:
(1) Broome, Port Hedland, Geraldton, Kalgoorlie and Albany(2) Esperance, Katanning, Moora, Narrogin, Merredin, Northam, Carnarvon, Newman, Nickol Bay, Derby and
Kununurra(3) Fitzroy Crossing, Halls Creek, Wyndham, Exmouth, Onslow, Paraburdoo, Wickham, Roebourne, Tom
Price, Dongara, Kalbarri, Meekatharra, Morawa, Mullewa, North Midlands, Northampton, Laverton,Leonora, Norseman, Ravensthorpe, Beverley, Boddington, Bruce Rock, Corrigin, Cunderdin, Dalwallinu,Dumbleyung, Goomalling, Kellerberrin, Kondinin, Kununoppin, Lake Grace, Narembeen, Pingelly,Quairading, Southern Cross, Wagin, Wongan Hills, Wyalkatchem, York, Denmark, Gnowangerup, Kojonup,Plantagenet.
clinicalframeworknew spread 21/9/05 3:14 PM Page 65

62
WA H e a l t h C l i n i c a l S e r v i c e s F r a m e w o r k 2 0 0 5 – 2 0 1 5
clinicalframeworknew spread 21/9/05 3:14 PM Page 66

For further information please contact:
Health Policy and Clinical Reform
Department of Health
Phone: (08) 9222 4434
Fax: (08) 9222 2192
Email: [email protected]

WA Health Clinical ServicesFramework 2005 – 2015
Delivering a Healthy WA
Healthy Workforce ● Healthy Hospitals ● Healthy Partnerships ● Healthy Communities ● Healthy Resources ● Healthy Leadership
© Department of Health, 2005
HP
2978
SE
PT
’05
2064
3
September 2005