wc ebilling and hipaa claims - opcc.optum.com ebilling and hipaa claims 20080307.pdfebilling or...
TRANSCRIPT
WC eBilling and HIPAA Claims White Paper
Page 1 of 26
Workers’ Compensation eBilling
Compared to
HIPAA Claims
White paper on Similarities and Differences
March 7, 2008
Version 1
Revision 1
WC eBilling and HIPAA Claims White Paper
Page 2 of 26
Why This White Paper Over the last year there has been a surge of interest in the Workers’ Compensation community to take advantage of the electronic billing benefits that are starting to accrue to health care providers and group health payers as a result of implementing the HIPAA transactions. This interest seems to be spreading to multiple states and at this point it is starting to look like a serious trend among the different Workers Compensation jurisdictions.
Some of the excitement comes from the possibility to tap into the existing installed base of providers that can generate group health standard transactions using the HIPAA standards. At this point the CMS estimate is that more than 95% of the healthcare claims can be produced electronically, and there is already discussion about phasing out the paper claims altogether in favor of the HIPAA electronic transactions.
This white paper will attempt to discover the differences between some of the HIPAA standard transactions and the Workers’ Compensation requirements for electronic billing. It is not specific to any one jurisdiction, and it describes the differences and similarities in general terms. The general question that this paper is attempting to answer is: How can we use the HIPAA transactions to conduct Workers’ Compensation electronic billing? The focus is on the current HIPAA standards using the ASC X12 837 and 835. At this point the NCPDP standards are not addressed here yet.
The audience for this paper is a combination of the following:
• Providers and their practice management system vendors
• Payers and their system vendors, including TPAs, repricers, etc.
• Clearinghouses, electronic billing aggregators and similar EDI processors
• State workers’ compensation regulators contemplating the use of HIPAA transactions for electronic billing of workers’ compensation
At some point I may be discussing a particular way to do something. Please remember this is not an indication that the particular method is the only one feasible, or even the best. Since this is a purely educational paper, the exercise of finding the way to suit your particular needs is left up to you, the reader.
The presentation of the first part is in the form of a series of tables on different topics. This is an unusual presentation for a white paper, but it allows the easy location of the topic of interest. I hope that by breaking it into topics it will be easier to update later. The intent is to update this paper with feedback from all the industry participants, so we can all use it as a reference for migrating a provider or payer from the HIPAA world to the workers’ compensation world. Please, provide me with your feedback to improve this paper so we can all benefit from your knowledge and experience. You can send your comments to [email protected].

WC eBilling and HIPAA Claims White Paper
Page 3 of 26
Terminology
Term Difference Comments
Claim HIPAA: Each episode of care or encounter with a patient is billed as a separate claim using the 837.
WC: A claim is established when the employment-related injury or illness is reported under the WC policy and verification with the employer has occurred.
HIPAA: Services from multiple providers are generally billed as separate claims even if they are related to each other, such as the hospital charges, the surgeon charges and the anesthesiologist charges.
WC: A claim may remain open forever or at least for many years. In some states the claim never closes, and indemnity can continue with the injured employee’s dependents. Even if a claim “closes” it could re-open if there is additional billing activity. All the billing from the various providers is related to the claim.
The claim is normally set up regardless of compensability and compensability may not be determined until much after medical treatment has started.
eBilling or eBill HIPAA: This term is not used in group health. The term Claim in group health has the same meaning as eBill for WC.
WC: Each episode of care or encounter with an injured employee is billed as a separate eBill using the 837.
HIPAA: A group health payer may associate all the charges from several providers related to an episode of care, but this is transparent to the providers. Generally there is no persistence from one episode to the next and each one is treated independent of each other.
WC: Only eBills related to a compensable claim are reimbursed under WC. Since the same injured employee could have several open claims simultaneously, the specific claim number is generally required on the eBill.
Claim Number HIPAA: The payer assigns an Internal Control Number (ICN) or Document Control Number (DCN) to each received claim/eBill. This is reported back to the provider in the 277 and 835.
WC: The Claim Number is assigned by the Carrier or TPA or Self-Insured upon processing of the injury, which is normally initiated by the employer injury notification. The same claim number follows the claim regardless of
HIPAA: The provider does not know the ICN/DCN until after the claim/eBill has been filed. Knowing the ICN/DCN does not help the provider’s reimbursement.
WC: The provider should indicate the claim number on each eBill filed so the payer can associate the eBill with a particular claim. Failure to specify the claim number could result in the eBill being denied or rejected by the payer. However, sometimes the provider does not yet have the claim number or the claim has not been

WC eBilling and HIPAA Claims White Paper
Page 4 of 26
Term Difference Comments
how many eBills are filed. “established” when the provider sends the eBill. In some cases the initial eBill from the provider must be sent without the claim number as it is part of the payer process to initiate and establish a claim. In the absence of the claim number the payer should be able to match other data elements between the claim and the eBill.
Carrier HIPAA: Generally refers to Medicare Carriers for Medicare Part B.
WC: The insurance company that carries the insurance “risk” in workers’ compensation.
HIPAA: Other payers have other designations such as “Intermediary” or “DMERC” or simply “payer”.
WC: In many cases even though the risk is carried by an Insurance Company regulated by the State, the eBill processing is done by one or more bill administrators, TPAs, re-pricers or claim administrators.
Self-insured entities are not Carriers. Most self-insured entities rely on a re-insurance or stop-loss Carrier.
In some jurisdictions (e.g. Texas) the Certified Self-Insured entities receive a jurisdictional treatment as if they were Carriers.
Payer HIPAA: The entity that pays the claim.
WC: Generally not used term.
HIPAA and WC: For this white paper the Payer is the entity that receives the claim/eBill, processes it for adjudication, and produces the 835. It does not matter whether that entity is a Carrier, a TPA, Bill Reviewer or goes by another name. As far as the provider is concerned, the 837 eBill is sent to the “payer”, any issues with the eBill or payment are addressed by the “payer”, and the 835 payment comes from the “payer” even though the funds may be identified as coming from an employer or a Carrier. The term “payer” is related to being the entity that handles the eBill adjudication and payment as far as the provider is concerned. A clearinghouse or eBill agent is not a “payer” as they do not perform the adjudication of the eBill. When there are multiple entities involved in the adjudication like re-pricers and bill reviewers, the “payer” is the entity that receives the 837 eBill from the provider and sends the 835 back.

WC eBilling and HIPAA Claims White Paper
Page 5 of 26
Term Difference Comments
PPO or Re-pricer HIPAA: The term used is PPO.
WC: The term used is re-pricer.
HIPAA: The preferred provider organizations (PPO) re-price the claims based on the contracted fees. Generally the provider sends the claims to the PPO, as if the PPO was the payer, and the PPO forwards the re-priced claim to the payer that processes it for adjudication. In some cases the PPO discloses the contracted fees to the payer and the payer re-prices the claim during the adjudication process.
WC: Similar to HIPAA except that the term used is re-pricer. In WC it is more common to the re-pricing function to be invisible to the provider and the re-pricer interacts with the payer directly. Additionally, in some instances, the re-pricer is also the bill reviewer.
Bill Reviewer HIPAA: Not used.
WC: Entity that reviews a medical bill for accuracy as part of the adjudication process.
HIPAA: The review of medical services for accuracy of the billing is done by the Carrier, TPA or other payer. It is not a separate function.
WC: It is common for the review of medical services to be contracted out to a company that specializes in that area, especially when the Carrier or TPA does not have that particular expertise in house. Sometimes the provider is asked to send the bills directly to the bill reviewer and in other cases the provider sends the bills to the Carrier or TPA and the bill review process happens invisible to the provider. Additionally, in some instances, the bill reviewer is also the re-pricer.
Accident Indicator HIPAA: The presence of an Accident Indicator is an exceptional condition.
WC: Generally the WC claims are associated with an employment-related injury or illness. The presence of the Accident Indicator or employment-related indicator is the norm.
HIPAA: The Accident Indicator generally triggers coordination of benefits or subrogation activity to determine if the claim/eBill should be filed against a WC policy or an automobile policy or a liability policy.
WC: Without an employment related injury or illness there would not be a WC claim. Generally the “employment related” indicator is required in all WC eBills.

WC eBilling and HIPAA Claims White Paper
Page 6 of 26
Term Difference Comments
Appeals and Re-considerations
HIPAA: Generally after a claim is denied it can be filed again as a new claim.
WC: It is common to appeal eBills or to request a re-consideration especially if the eBill was filed before the Claim number was available.
HIPAA: Appeals and re-consideration requests are not as common as in WC.
WC: This is sometimes the easiest way to address the catch-22 situation of the need for the Claim number on the eBill, and the need for an eBill before a Claim can be opened.
WC eBill payment operates within clean claim timeframes that are strictly regulated, so the providers may not be able to re-file an eBill after the time window closes and therefore must request an appeal or re-consideration of a prior eBill that was filed within the appropriate filing time guidelines.
Jurisdiction HIPAA: Medicare has specific Federal rules and Medicaid has State-specific rules. Indian Health and Tricare also have some special requirements, but the vast majority of payers do not have jurisdictional authority.
WC: Each state has many specific Workers’ Compensation jurisdictional rules.
HIPAA: The Medicaid rules depend on the Medicaid payer receiving the claim. One per state.
WC: The jurisdiction that governs an eBill is independent of the payer that processes the eBill, and independent of the provider location or the place where the accident occurred. Generally the jurisdiction is the state where the particular Workers’ Compensation policy is written for the employer. The provider must be aware of the jurisdictional requirements applicable to each claim. The same provider and injured employee could be under different jurisdictions for two claims, depending on who the employer was at the time of the injury, and in what state the WC policy was written. Different jurisdictions have different rules and requirements.
Encounters HIPAA: In case of “managed care” a non-reimbursable medical service.
WC: Not applicable.
HIPAA: The encounters are reported for statistical purpose and to justify utilization, even if they are not reimbursable.
WC: Only electronic bills seeking reimbursement under a WC claim need to be submitted. The total charge amount must be greater than zero.

WC eBilling and HIPAA Claims White Paper
Page 7 of 26
Subscriber, Patient and Employer
Term Difference Comments
Subscriber HIPAA: Generally either the patient or a patient relative such as a parent or spouse.
WC: The Employer is the subscriber for purposes of electronic billing with the 837.
WC: The subscriber is never the injured employee. The employer information must be sent in the Subscriber loop of the 837 and the employer will be reflected as the subscriber in the 835.
Subscriber ID HIPAA: Required.
WC: Not used.
HIPAA: The Subscriber ID and Group Number are generally required. They are obtained from the Subscriber ID card.
WC: Since the Subscriber is the employer instead of a person, the 837 transaction does not require or even allow for the employer/subscriber ID. If the employer ID is known, it could be sent as the secondary Subscriber ID. Watch out for the HIPAA requirement that Employer IDs must be sent with a hyphen in the third position as in 99-9999999.
Subscriber’s Date of Birth
HIPAA: Required.
WC: Not used.
HIPAA: Important data element. It is used by the payer to validate and match the subscriber’s identity.
WC: Since the “subscriber” is the employer, there is no equivalent to the Subscriber’s DOB.
Subscriber Address HIPAA: Only required if the patient is the subscriber.
WC: Required.
HIPAA: If the patient is different from the subscriber, only the patient address is used and the subscriber address is not used.
WC: The employer address is required in all WC eBills, even though the injured employee will never be the same as the subscriber. Both injured employee address and subscriber/employer address are required.
Subscriber Name Type HIPAA: Person.
WC: Non-Person entity.
WC: Even when the employer is an individual, the subscriber name refers to the employer as an entity. So the 837 Subscriber Name must indicate a non-

WC eBilling and HIPAA Claims White Paper
Page 8 of 26
Term Difference Comments
person entity.
Policy or Group Number HIPAA: The actual number issued by the payer to this group of subscribers.
WC: Not used.
HIPAA: The provider obtains it from the insured’s ID card
WC: Generally not needed as there is a unique WC relationship between the employer and the payer. There is no equivalent of the insured’s ID card in WC.
Without the insured’s ID card or some equivalent method the provider has very little opportunity to immediately know who the payer is. Generally identifying the payer for a specific claim requires that the provider first call the employer. For this reason, routing, claim number identification and eligibility verification transactions recommended by HIPAA are difficult in WC.
Patient Information HIPAA: Required only if the patient is not the subscriber.
WC: Required.
HIPAA: The patient could be the same as the subscriber.
WC: The injured employee is never the same as the subscriber, as the subscriber is the injured employee’s employer.
Patient ID HIPAA: Proprietary number assigned by the payer to the subscriber or the patient.
WC: Social Security Number of the injured employee.
HIPAA: The use of SSN to identify patients has been practically phased out. The Patient ID is sometimes reflected on the insured’s ID card, in the form of a “person code” for each of the insured’s dependents
WC: The SSN is the common identifier, but in some rare cases the employer may use an employee ID number instead of the employee’s SSN. In these cases, unless the provider is certain that the payer will identify the employee by the employee ID, it may be necessary to send the employee’s SSN in the “Secondary ID” field in addition to sending the employee ID as the “Primary ID” field.
The requirement to use the SSN as the injured employee ID may be changing as states move away from SSNs for data privacy concerns.
Patient Relationship HIPAA: Self, Spouse, Other, etc. WC: The only valid relationship between the injured employee (patient) and the

WC eBilling and HIPAA Claims White Paper
Page 9 of 26
Term Difference Comments
WC: Employer. subscriber is that of “Employee”.
Claim Number HIPAA: Not used.
WC: Required (if the claim number is available.)
WC: Once the WC Claim has been established as compensable under the WC policy, the Claim Number should be submitted in all the eBills. If some eBills were filed before the Claim Number was issued, they may have to be submitted initially without the Claim Number and later submitted for re-consideration or appealed after the Claim Number is established.
Since WC claims could remain active/open for many years, it is possible that the same employee has several claim numbers. The claim number is essential for the correct adjudication of the eBill.
Responsible Party HIPAA: Used in cases where the responsible party is the patient’s estate.
WC: Not used.
WC: The employer information is sent in the subscriber loop and there is no other responsible party.
Other Subscriber HIPAA: Required for Coordination of Benefits.
WC: Not used.
HIPAA: If there is potential coverage by another policy or another subscriber, the information must be sent.
WC: There is no coordination of benefits. Worker’s compensation is always the primary payer responsible for all benefits associated with a work related injury. For workers’ compensation purposes the subscriber is the employer, and even if the injured employee has a group health policy, the group health policy generally does not coordinate benefits with the WC policy.
Providers
Term Difference Comments
Billing Provider ID HIPAA: Requires NPI.
WC: Requires NPI and sometimes other ID numbers.
HIPAA: Only the NPI is used and other provider IDs must not be sent.
WC: In addition to the NPI, other provider IDs may be required, such as the State

WC eBilling and HIPAA Claims White Paper
Page 10 of 26
Term Difference Comments
License Number. If the provider is eligible for an NPI then the provider must obtain an NPI and use it as the primary provider ID. Some WC jurisdictions have statutory requirements for the State License Number to be reported on every eBill even for providers that have an NPI. Some providers may not be eligible for NPI, for example foreign providers, in which case they are generally identified by their State License Number or Tax ID number.
Billing Provider Secondary ID
HIPAA and WC: The FEIN is required when the NPI is used as the primary ID.
HIPAA and WC: The requirement for the FEIN as the secondary provider ID is a requirement resulting from the Billing Provider NPI being sent as the primary ID. In addition to the NPI, the Billing Provider FEIN (Tax ID) is now required.
WC: In addition to the FEIN, some jurisdictions also require the billing provider State License Number. Not all providers have a State License with the state of jurisdiction. Some providers have a state license with another state. For historic and statutory reasons the State License Number may need to be sent with each eBill. Since the State License Number can easily be obtained from NPPES, the hope is that the requirement will change over time to require just the NPI on the eBill.
Billing Provider Contact Information
HIPAA and WC: Required if it is different from the Submitter Contact Information.
HIPAA and WC: When using a clearinghouse it is important to enter the Billing Provider Contact information even if it is identical to the Submitter Contact. As the clearinghouse combines transactions from multiple billing providers into one stream for the payer, the Submitter becomes the clearinghouse itself and the Billing Provider Contact becomes required. Providers using clearinghouses should send their contact information in the Billing Provider loop.
Billing Provider Taxonomy Code
HIPAA: Required if it impacts adjudication.
WC: Required by some jurisdictions.
HIPAA: Only required if the provider knows that the adjudication is impacted by the Taxonomy code.
WC: The Taxonomy Code may be required by some WC jurisdictions.
Deleted: ¶

WC eBilling and HIPAA Claims White Paper
Page 11 of 26
Term Difference Comments
Rendering or Attending Provider Information
HIPAA and WC: Required if different from Billing Provider.
HIPAA and WC: When the Billing Provider is not the same as the Rendering or Attending Provider, the information about the Rendering or Attending Provider is required. In this case the Identity code (NPI and State License Number) and possibly even the Taxonomy Code are required.
Because the Rendering or Attending providers are the sources of the services being billed, the requirement to identify them is the same as the requirement to identify the Billing Provider: The Identity code (NPI and State License Number) and possibly even the Taxonomy Code are required.
Referring and other providers
HIPAA and WC: Required if there were Referring or other providers.
HIPAA and WC: In this case the NPI or the provider’s Taxonomy code may not be known, so the requirement is not as strict as the requirement for the billing or rendering providers. Generally the name is sufficient, but if the NPI is available, it should also be entered.
Pay-To Provider Name and ID
HIPAA and WC: Should not be used. HIPAA and WC: This functionality will disappear in the next version of the HIPAA transactions, so it would be best to not use it and certainly to not rely on it. Only the ability to send an alternative Pay-To address will remain in 5010. In any case, most payers will ignore it, in order to avoid a hole for fraud, and will only send the payment to the billing provider in their files, regardless of what the Pay-To provider says.

WC eBilling and HIPAA Claims White Paper
Page 12 of 26
Payers
Term Difference Comments
Payer ID HIPAA: Well established lists of Payer IDs created by each clearinghouse.
WC: Active attempt to create a national list of Payer IDs common to the entire industry.
HIPAA: Generally based on the NAIC co-code, but each clearinghouse has proprietary IDs that cause problems when transferring transactions among clearinghouses or during COB.
WC: Use the SeBIN Payer ID as the primary ID, and the FEIN, if available, as the secondary identifier. See the Payer ID and Routing section of this paper for more details.
Secondary Payer Information
HIPAA: Required for Coordination of Benefits.
WC: Not used.
WC: There is no coordination of benefits in WC since the financial responsibility lies on the policy written for the employer. Worker’s compensation is always the primary payer responsible for all benefits associated with a work related injury.
In some cases there is a “stop loss” or “re-insurance” policy that covers high value claims, but this information is generally not important to the provider and is not represented on the eBill.
In WC jurisdictions which allow “high deductible” policies the eBill could be filed with the employer until the deductible is met, and then, once the deductible is met, the eBill could be filed with a different payer. This is still not Coordination of Benefits but only a change of payer as soon as the deductible is met. In any case, the rules for self-insured and high deductible WC coverage vary from jurisdiction to jurisdiction.
Some jurisdiction may require the FEIN of the payer, in addition to the Payer ID, due to some statutory requirement. This could be problematic as one Payer ID could correspond to multiple payer FEINs and one payer FEIN could correspond to multiple Payer IDs.

WC eBilling and HIPAA Claims White Paper
Page 13 of 26
Term Difference Comments
Other Payer HIPAA: Required for Coordination of Benefits.
WC: Not used.
HIPAA: If there is potential coverage by another policy or another subscriber, the information must be sent.
WC: There is no coordination of benefits. For workers’ compensation purposes the only payer is the WC payer, and even if the injured employee has a group health policy, the group health policy generally does not coordinate benefits with the WC policy.
Payer Responsibility Sequence Code
HIPAA: Primary, Secondary, Tertiary.
WC: Primary.
HIPAA: There could be multiple payers that need to coordinate benefits.
WC: Worker’s compensation is always the primary payer responsible for all benefits associated with a work related injury and there is no coordination of benefits with other payers. Even in case of “stop loss” or “re-insurance” the coordination happens behind the scene and the provider files the eBill to the primary payer.

WC eBilling and HIPAA Claims White Paper
Page 14 of 26
Claims and eBills
Term Difference Comments
Claim Filing Indicator Code
HIPAA: Should not be “WC”.
WC: Must be “WC”.
HIPAA and WC: This is the differentiator between a group health (HIPAA) “claim” and a Workers’ Compensation “eBill”.
Related Causes (or Condition Codes)
HIPAA: Should not be related to employment.
WC: Must indicate “employment related.”
HIPAA: If the indicator states the services are related to employment, the group health payer will most likely deny payment.
WC: If the indicator does not state it is related to employment, the WC payer will most likely deny payment.
This is a critical differentiator between WC and group health scenarios.
Diagnosis Code HIPAA: Generally required, except for cases where there is no diagnosis.
WC: Required for all professional and institutional bills.
HIPAA: Some transport services (e.g. taxi services) do not have a valid diagnosis code. With the new 5010 version it will become required for all professional and institutional bills.
WC: Required in all cases for professional and institutional bills since the claim itself was opened under a specific compensable diagnosis, injury or illness.
Accident Date HIPAA: Generally not used.
WC: Generally required.
HIPAA: Could be used in cases of automobile accident or other accident. If used it will most likely trigger a coordination of benefits or a denial, with instructions to file with the liability payer.
WC: The term used for WC is “Date of Injury”. Not all the WC claims are related to injuries. Chronic conditions (asbestosis) and repetitive stress injuries (carpal tunnel syndrome) are two examples of WC conditions that are not related to a specific date of injury. But, if the WC claim is related to an employment-related injury, the date of injury is required.
Patient Account Number HIPAA: Either the patient account or the invoice/claim number.
WC: A unique eBill identifier number.
HIPAA: Some systems use an account posting with balance carry-forward payment logic instead of assigning each claim a unique number.
WC: It is important to use a unique eBill
Deleted: ¶C
WC eBilling and HIPAA Claims White Paper
Page 15 of 26
Term Difference Comments
identifier, as some payer systems will reject eBills as duplicates if they contain the same number as a previous eBill in the Patient Account field.
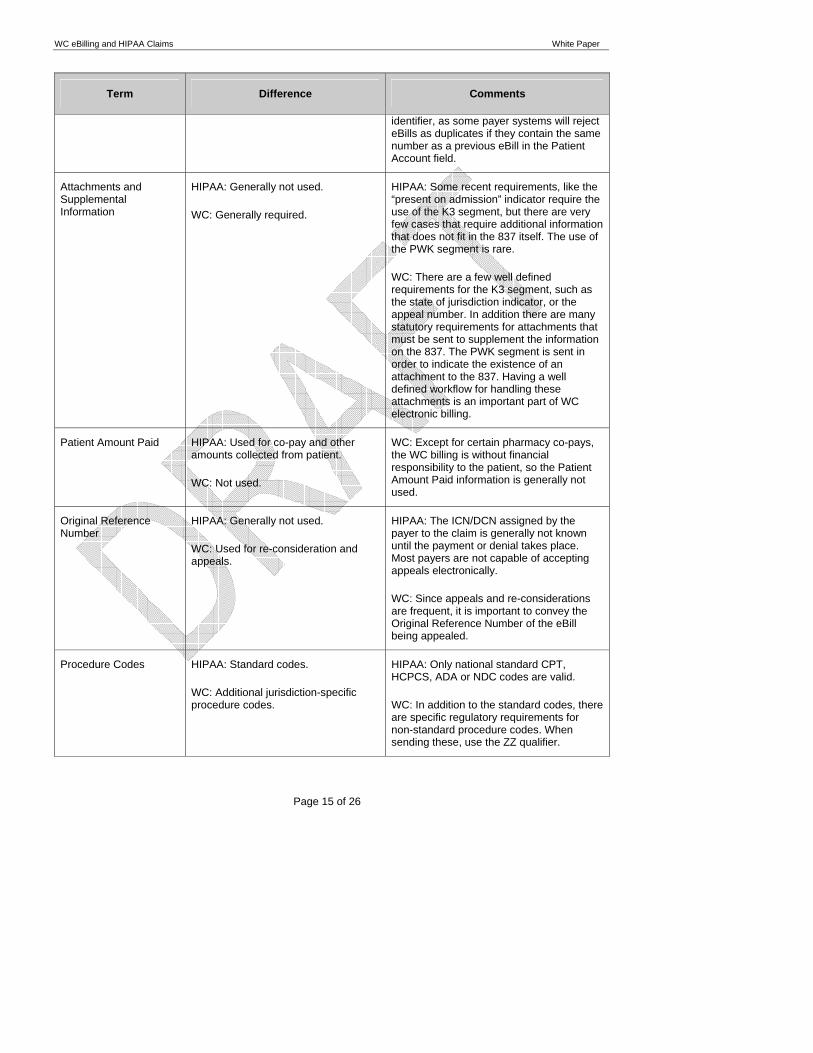
Attachments and Supplemental Information
HIPAA: Generally not used.
WC: Generally required.
HIPAA: Some recent requirements, like the “present on admission” indicator require the use of the K3 segment, but there are very few cases that require additional information that does not fit in the 837 itself. The use of the PWK segment is rare.
WC: There are a few well defined requirements for the K3 segment, such as the state of jurisdiction indicator, or the appeal number. In addition there are many statutory requirements for attachments that must be sent to supplement the information on the 837. The PWK segment is sent in order to indicate the existence of an attachment to the 837. Having a well defined workflow for handling these attachments is an important part of WC electronic billing.
Patient Amount Paid HIPAA: Used for co-pay and other amounts collected from patient.
WC: Not used.
WC: Except for certain pharmacy co-pays, the WC billing is without financial responsibility to the patient, so the Patient Amount Paid information is generally not used.
Original Reference Number
HIPAA: Generally not used.
WC: Used for re-consideration and appeals.
HIPAA: The ICN/DCN assigned by the payer to the claim is generally not known until the payment or denial takes place. Most payers are not capable of accepting appeals electronically.
WC: Since appeals and re-considerations are frequent, it is important to convey the Original Reference Number of the eBill being appealed.
Procedure Codes HIPAA: Standard codes.
WC: Additional jurisdiction-specific procedure codes.
HIPAA: Only national standard CPT, HCPCS, ADA or NDC codes are valid.
WC: In addition to the standard codes, there are specific regulatory requirements for non-standard procedure codes. When sending these, use the ZZ qualifier.

WC eBilling and HIPAA Claims White Paper
Page 16 of 26
Data Flow The flow of data for workers’ compensation and for group health electronic billing is very similar. The terminology used to describe this flow, however, is somewhat different. In order to understand the data flow it is important to first understand the differences in terminology and the roles each player plays. The data flow can then be described in function of the roles and with less dependence on the particular terminology.
HIPAA Transactions Flow In the HIPAA “group health” environment, the transactions are sent from Providers to Payers either directly or through a clearinghouse. In general there are well defined data flows and the providers obtain from the subscriber’s ID card the information on where the transactions need to be sent, typically a Payer ID for electronic transactions and a P.O. Box or mailing address for paper billing.
© Ingenix, Inc. 3
HIPAA transactions flow
Insurance Carrier
(Carrier of Insurance Risk)
Repricer/PPO
Third Party
Administrator
Provider
There are three relevant scenarios, A) the claims are sent to the Insurance Carrier directly, B) the claims are sent to a PPO for repricing, or C) the claims are sent to a Third Party Administrator. These are all very common scenarios.
The role of the PPO as receiver of the claims from the provider varies depending on the particular arrangement with the health plan. In some cases the PPO receives the claim, re-prices it, and forwards the claim to the Carrier or the TPA. In other cases the claim is received by the Carrier or the TPA and, if it needs repricing, the Carrier or TPA gets the claim repriced according to the PPO fee schedule in a manner that is invisible to the provider.
In general, the role of the TPA, PPO or the Insurance Carrier is equivalent as far as the Provider is concerned. And all three of these entities can generally receive electronic HIPAA transactions.
The complexity of this data flow model stems from the provider having to establish a direct connect relationship with each one of the entities that will be receiving the transactions. This is generally not feasible for most providers.
HIPAA Clearinghouses The HIPAA Clearinghouses play an important role to simplify the process for both Providers and Payers. By sending their transactions to a clearinghouse the providers reduce their cost of administrating multiple connections and outsource the connectivity, data validation and even data formatting to their clearinghouse. In like manner, payers can receive their transactions aggregated by the clearinghouse and need only support a small number of trading partners.
Deleted: Page Break

WC eBilling and HIPAA Claims White Paper
Page 1 of 26
© Ingenix, Inc. 4
HIPAA clearinghouses
Insurance Carrier
(Carrier of Insurance Risk)
Repricer/PPO
Third Party
Administrator
Clearinghouse(s)
Provider
As providers and payers connect to clearinghouses, there are economies of scale that can be leveraged, especially for those connections that have low frequency or low volume.
Instead of one national clearinghouse there are a handful of competing national clearinghouses and dozens of smaller local or regional clearinghouses that specialize in different markets.
Some markets are geographical, other clearinghouses are associated with a particular practice management vendor, or with a particular payer or group of payers. Some specialize in Dental or Professional transactions.
The connectivity is achieved by most of the clearinghouses having data agreements with other clearinghouses, so practically any claim can be sent through the clearinghouse network, being routed among clearinghouses without provider intervention.
In some cases the payer will select a clearinghouse as their designated transaction connectivity gateway. In these cases, due to HIPAA regulations, the payer has to bear the cost of the transactions and offer the option to the provider to send transactions through the designated clearinghouse at no cost to the providers. These scenarios are generally referred to as “participating payers” in the clearinghouse payer directories.
In other cases the provider will choose a clearinghouse and route all of the transactions through the chosen clearinghouse. Even though these cases may present a higher per transaction fee to the provider, the convenience of outsourcing all the connectivity is generally worth the extra cost.
HIPAA Common Hybrid Flow However, most of the traffic of HIPAA transactions follows a hybrid flow pattern with the use of clearinghouses as well as direct connections.
© Ingenix, Inc. 5
HIPAA common hybrid flow
Insurance Carrier
(Carrier of Insurance Risk)
Repricer/PPO
Third Party
Administrator
Clearinghouse(s)
Provider
The providers generally prefer the lower cost option of sending transactions directly to payers, as long as they have enough transaction volume for the payer.
Generally the provider chooses to connect directly with the payers that represent their largest volume, such as Medicare, Medicaid, and perhaps the Blue Plan or commercial payer that represents most of their volume. The rest of the transactions are sent to a clearinghouse for distribution to payers that do not represent enough volume to justify a direct connection.
Similarly, the payers connect directly with their largest providers, such as clinical laboratories, and very large providers, and receive the rest of their transaction flow from clearinghouses.
This hybrid model satisfies the balance for lower cost per transaction and lower cost of administering multiple connections. Even in the case of Medicare, which does not pay for clearinghouse transactions, the largest submitters are clearinghouses acting on behalf of providers.
In this hybrid model the lines between a clearinghouse acting on behalf of a payer or a clearinghouse acting on behalf of a provider start to blur when the clearinghouses offer blended rates that are not directly correlated with transaction counts. Then many factors other than pricing impact the provider decision to either send transactions

WC eBilling and HIPAA Claims White Paper
Page 2 of 26
directly or through a clearinghouse, and the payer decision to either designate one clearinghouse as their only entry point or support multiple clearinghouses for HIPAA transactions.
Workers’ Compensation Data Flows The Workers’ Compensation industry has a data flow that is very similar, almost identical to the HIPAA data flow, but the terminology differences cause the flow to appear very different. In reality, the similarities are much greater than the small differences.
© Ingenix, Inc. 7
WC eBilling data flows
Insurance Carrier
(Carrier of Insurance Risk)
Repricer
Bill Review
Company
Third Party
Administrator
eBill Agent(s) or
Clearinghouse(s)
Provider
The role of the WC insurance Carriers, and third party administrators, as far as receiving EDI transactions for electronic billing, is practically identical to the corresponding role for the HIPAA transactions.
The role of the HIPAA PPO is identical to the role of the re-pricers in WC. In some cases the electronic bill has to be sent to the re-pricer first and in other cases the TPA, Carrier or bill review company takes care of the re-pricing part of the flow. The only difference is one of terminology, where under HIPAA they are called PPOs, under WC they are called re-pricers.
But in WC there is an entity referred to as “bill review” company, or a similar name, that generally does not exist in the HIPAA environment.
The Bill Reviewers play a role similar to the Carrier, TPA or Re-pricer as far as receiving the electronic billing is concerned. In some cases the provider needs to send the billing to the TPA, in other cases to the Bill reviewer, or to the Re-pricer or to the Carrier. Then the adjudication of the billing takes place behind the scenes and, unbeknownst to the provider, there are multiple communication paths among these entities in order to collaborate and reach the adjudication of the electronic billing. Adding the Bill Review entity does not significantly change the process, other than there is one more player than there is for the HIPAA transactions.
Another terminology difference is where the HIPAA Clearinghouses are called eBill Agents for WC transactions. Under HIPAA some clearinghouses act as the exclusive entry point for certain payers, in fact acting as the only EDI gateway to those payers. But even when the payers select a Clearinghouse as their exclusive EDI gateway, the clearinghouse still connects with other payers and providers. Under WC the eBill Agents play this role of exclusive entry point for a payer’s EDI transactions, being in the same role as the HIPAA Clearinghouses.
WC Direct Submission Some WC payers have chosen the direct submission method, where the providers are responsible for establishing the EDI connection to the payer and the payer acts as the hub for receiving transactions from multiple providers.

WC eBilling and HIPAA Claims White Paper
Page 1 of 26
© Ingenix, Inc. 8
WC eBilling direct submission
Insurance Carrier
(Carrier of Insurance Risk)
Repricer
Bill Review
Company
Third Party
Administrator
eBill Agent(s) or
Clearinghouse(s)
Provider
While this method of submission is adequate for connections between providers and payers that have substantial volume of transactions, it is expensive, with the common technology used today, for providers and payers that have a low volume of transactions.
Providers and payers that have low volume are better served by Clearinghouses that can aggregate the volume and deliver economies of scale in managing those EDI connections.
There are four relevant scenarios, A) the eBills are sent to the Insurance Carrier directly, B) the Ebills are sent to a Bill Review entity, C) the eBills are sent to a repricer, or D) the eBills are sent to a Third Party Administrator. These are all very common scenarios.
The role of the different receivers of the eBills from the provider varies depending on the particular arrangement with the health plan. The interconnections between these entities happen in the background unbeknownst to the provider. In general, the role of the TPA, Bill Reviewer, Re-pricer or the Insurance Carrier is equivalent as far as the Provider is concerned. And all four of these entities can generally receive electronic WC transactions.
The complexity of this data flow model stems from the provider having to establish a direct connect relationship with each one of the entities that will be receiving the transactions. This is generally not feasible for most providers, and it is equally expensive for a WC payer to establish connectivity with many providers that send low volumes of transactions. For this reason both payers and providers tend to gravitate to eBill Agents or Clearinghouses that can leverage the economies of scale.
WC Clearinghouses or eBill Agents The WC Clearinghouses, or eBill Agents, play an important role to simplify the process for both Providers and Payers. By sending their transactions to a clearinghouse the providers reduce their cost of administrating multiple connections and outsource the connectivity, data validation and even data formatting to their clearinghouse. In like manner, payers can receive their transactions aggregated by the clearinghouse and need only support a small number of trading partners.
© Ingenix, Inc. 9
WC eBilling Clearinghouse (eBill Agent)
Insurance Carrier
(Carrier of Insurance Risk)
Repricer
Bill Review
Company
Third Party
Administrator
eBill Agent(s) or
Clearinghouse(s)
Provider
As providers and payers connect to clearinghouses, there are economies of scale that can be leveraged, especially for those connections that have low frequency or low volume.
Instead of one national clearinghouse there are a handful of competing clearinghouses that specialize in the WC market. In general these clearinghouses are small and only connect to a few WC payers.
The connectivity will eventually be achieved by most of the clearinghouses having data agreements with other clearinghouses, so practically any eBill can be sent through the clearinghouse network, being routed among clearinghouses without provider intervention.
In some cases the WC payer will select a clearinghouse as their designated transaction connectivity gateway. In these cases, the selected clearinghouse is designated as the payer’s “eBill Agent” and the payer has to bear the cost of the transactions and offer the option to the provider to send transactions through the designated clearinghouse at no cost to the providers. These eBill Agents may be listed in the jurisdictional payer directories.

WC eBilling and HIPAA Claims White Paper
Page 2 of 26
In other cases the provider will choose a clearinghouse and route all of the transactions through the chosen clearinghouse. Even though these cases may present a higher per transaction fee to the provider, the convenience of outsourcing all the connectivity is generally worth the extra cost.
Whereas the HIPAA clearinghouses are regulated as HIPAA “Covered Entities”, under WC the clearinghouses escape the regulatory authority as they are neither payers nor providers. The designation of a clearinghouse as an eBill Agent of a payer could start bringing the clearinghouses under the regulatory authority in some jurisdictions.
WC eBilling Common Hybrid Flow Once electronic WC billing becomes more prevalent and the WC clearinghouse networks acquire the necessary interconnectivity, most of the traffic of WC transactions will follow a hybrid flow pattern with the use of clearinghouses as well as direct connections, similar to the HIPAA data traffic.
© Ingenix, Inc. 10
WC eBilling common hybrid flow
Insurance Carrier
(Carrier of Insurance Risk)
Repricer
Bill Review
Company
Third Party
Administrator
eBill Agent(s) or
Clearinghouse(s)
Provider
The providers will generally prefer the lower cost option of sending transactions directly to payers, as long as they have enough transaction volume for the payer.
Generally the provider will choose to connect directly with only a handful of payers, the payers that represent their largest volume. The rest of the transactions will be sent to a clearinghouse for distribution to payers that do not represent enough volume to justify a direct connection.
Similarly, the payers will connect directly with their largest providers, such as clinical laboratories, and very large providers, and receive the rest of their transaction flow from clearinghouses.
This hybrid model, as in the case of HIPAA transactions, will satisfy the balance for lower cost per transaction and lower cost of administering multiple connections. In this hybrid model the lines between a clearinghouse acting on behalf of a payer or a clearinghouse acting on behalf of a provider will start to blur when the clearinghouse serves both providers and payers.
In addition, the clearinghouses are developing the capability to handle electronic attachments in order to make the attachment data flow follow the same path as the eBills. Handling of attachments is a problem particularly important in Workers’ Compensation, and one that is not yet fully resolved.

WC eBilling and HIPAA Claims White Paper
Page 2 of 26
Attachments Many of the eBills need additional information, or attachments, before they can be adjudicated and paid. This supporting information is required in some cases for statutory reasons, and in other cases it is necessary to understand the clinical aspects of the case such as progress notes and treatment plans.
In the paper world, the additional information is attached to the paper bill with a staple or paper clip. In the electronic world there are no such staples or paper clips, but the “attachment” analogy prevails even for electronic documents. These attachments are a necessary part of the electronic billing and need to be considered when implementing an electronic billing solution for WC.
In the HIPAA world there is a proposed rule, still pending for HHS to publish the Final Rule, that requires the implementation of electronic attachments using the ASC X12 275 transaction, with implementation guides developed jointly by X12 and HL7 that define how the electronic attachments are to be sent.
One of the most important features of the HIPAA Attachments rule is that the provider should only send attachments with the claim in those cases where the payer has explicitly instructed the provider to send specific attachments up front, along with the claim, because they are always required. An example of these “unsolicited” attachments that are always required, are the patient’s signed consent forms for sterilization procedures. In all other cases the provider must not send attachments unless the payer requests the attachments (“solicited” attachments) during the adjudication process. To send attachments when they are not absolutely required, either because they are documented to be required in all cases, or because they were requested by the payer, will be considered to be a violation of the “minimum necessary” requirement under HIPAA.
The association between the electronic 837 and the attachment (both, paper or electronic attachment) happens through the PWK segment in the 837 transaction. A single claim/eBill can contain up to 10 repetitions of PWK segments, each one referring to a different type of attachment. Each of the PWK segments has a code indicating the type of attachment being sent (e.g., Discharge Summary, Prescription), another code indicating the method of transmission (e.g., US Mail, Fax) and an Attachment Control Number. The Attachment Control Number is a unique identification number, assigned by the provider, that is also present on the attachment itself, either stamped or written on paper attachments, or included as a REF segment for electronic attachments. The attachment Control Number is the linkage between the electronic claim/eBill and the attachment itself within the provider system. Since it is possible that two providers could, by chance, use the same Attachment Control Number (e.g., because the use the same version of practice management system) most payers create new document control numbers that are unique to the payer and serve to associate the electronic claim/eBill with the attachments in the payer’s document management system.
In the WC world, at least until the 275 Final Rule is published, there are several common ways to transmit the attachments.
Paper and Fax Attachments These are perhaps the most common methods of transmission of attachments for both HIPAA and WC situations. Either the claim/eBill is sent on paper with the attachments in the same envelope, or the claim/eBill is sent electronically with the attachments following in the mail or via fax.
In the case of electronic billing where there are paper or fax attachments, it is extremely important to clearly mark each page of the attachments with the Attachment Control Number that is in the PWK segment, so the attachments can be re-associated with the electronic claim or Bill.

WC eBilling and HIPAA Claims White Paper
Page 1 of 26
Generally the providers will send a cover page with the attachments, in order to include not only the Attachment Control Number, but a variety of data elements so the payer can associate the attachments to the correct electronic claims/eBills. In some cases a paper copy of the claim/eBill, stamped “COPY” takes the place of the cover page.
The cover page should contain enough information for the payer to match the attachment and the electronic claim/eBill, including demographic information about the patient, the provider, the payer, and the summary information about the electronic claim/eBill. In cases where the payer receives multiple electronic claims/eBills for one patient from the same provider, it is important that it be associated to the correct one.
Technically, the Attachment Control Number in the PWK segment is all that is absolutely necessary to include. However, as the matching between the paper attachments and the electronic claim/eBill is a manual operation, it is always best to include enough information on the cover page in order to ensure the matching to the correct electronic claim/eBill.
This same cover page is frequently used when sending the attachments via fax. Not all the payers receive attachments via fax, but, for those payers that do, it is generally a convenient way to send the attachments. In addition, some payers and clearinghouses offer a system for the provider to create bar-coded cover pages for attachments.
The benefit of a bar-coded cover page is that the payer’s document management system is capable of using the bar-code to automatically associate the attachment to the correct electronic claim/eBill without manual intervention or with minimal intervention. This speeds up the processing of the attachment and reduces the errors caused by associating an attachment to the incorrect claim/eBill.
In addition to the bar-code, some or all of the information on the cover page is pre-filled on the cover page. This allows the provider to match the bar-coded cover page to the correct attachment before transmitting it to the payer. And, if the fax resolution degrades the bar-code to the point that it is not usable for the automatic association of the attachment to the electronic claim/eBill, it provides an alternative mechanism that can be used for manually associating the attachment to the proper claim/eBill.
These paper attachments are generally sent by mail, courier, or fax. However, in the last two years and with the availability of low cost scanners and graphic terminals, more providers are sending their attachments by uploading scanned images to a web site. Either TIFF, JPEG or PDF files with a scan of the paper attachment are common now.

WC eBilling and HIPAA Claims White Paper
Page 1 of 26
When uploading scanned paper images to the payer, it is generally necessary to either include a cover page, just as for paper or fax attachments, or to enter on the web page, along with the uploaded images, enough information for the payer to associate the attachment to the correct claim/eBill.
Uploading these scanned paper images has the advantage of faster receipt by the payer, better image quality than faxes, and, in some cases, immediate association of the attachment to the corresponding electronic claim/eBill. However the process is generally manual, requiring the provider to use a web browser to upload each attachment file and to enter the information necessary to associate the file to the corresponding claim/eBill.
Electronic X12 Attachments The best way to automate the transmission of attachments is by using the ASC X12 275 transaction and the HL7 Additional Information Specifications (AIS), as described in the HIPAA proposed rule. Conceptually, the 275 and the HL7 act as the cover page for the attachments. Because of certain limitations of both the 275 and the HL7 AIS, the HIPAA proposed rule describes why it is necessary to send both data structures. The 275 transaction provides the linkage to the electronic claim/eBill and the HL7 AIS provides the description of the attachment being sent in clinical terms.
Electronic Attachment (Scanned)Submitter (Provider) Information (Name, ID)Receiver (Payer) Information (Name, ID)Patient Information (Name, ID)Claim Information (Date, type, reference, control number)Attachment typeQuestion that was asked by payer (LOINC)Response from provider (LOINC)
Scanned image (fax, pdf, rtf, html, or jpeg)
The HIPAA attachments implementation guides describe the flexibility in sending electronic attachments. The simplest type of attachment can be either scanned paper, or images of documents or clinically relevant pictures and radiographs.
A more advance type of attachment would be an HL7 Clinical Document Architecture (CDA) attachment generated directly by the electronic medical record system of the provider.
The CDA information can range from marked-up free form text to fully encoded CDA documents that can be automatically processed by a claim/eBill adjudication system without human intervention.
Probably one of the most useful functionalities of the combination of the X12 275 and the HL7 CDA attachment is that the information can be processed automatically by the adjudication system as well as rendered into a friendly human representation for those payers or bill reviewers that lack the system functionality for automated adjudication of the attachment.
Submitter (Provider) Information (Name, ID)Receiver (Payer) Information (Name, ID)Patient Information (Name, ID)Claim Information (Date, type, reference, control number)Attachment typeQuestion that was asked by payer (LOINC)Response from provider (LOINC)
Electronic Attachment (CDA-Codified)
HL7 CDA codified (HL7 v3 XML CDA mark-up)
<section><caption>EMS TRANSPORT, DESTINATION SITE INFORMATION
<caption_cd V="15512-7"/></caption><paragraph>
<caption>EMS TRANSPORT DESTINATION SITE NAME<caption_cd V="18582-7"/>
</caption><content>Alfred Newman Neurological Institute</content>
</paragraph><paragraph>
<caption>EMS TRANSPORT, DESTINATION SITE ADDRESS<caption_cd V="18583-5"/>
</caption><content>123 Main St; Anytown, UT 85912
<local_markup descriptor="AD"><local_attr name="LIT" value=“123 Main St"/><local_attr name="CTY" value=“Anytown"/><local_attr name="STA" value="UT"/><local_attr name="ZIP" value="85912"/>
</local_markup></content>
</paragraph></section>
One of the components of the HL7 attachments standard is a style sheet and transformation control file that converts the XML markup in the HL7 part of the attachment into a human readable template.
Using this XSLT transformation, the CDA-encoded document can be rendered, with a standard web browser, into a user friendly form. Thus the same attachment can be viewed by a bill reviewer today, or be automatically adjudicated by a sophisticated system in the future.
The 275 provides an envelope that can be routed through traditional EDI systems, acting as the equivalent of the cover page used when faxing or mailing attachments.
Inside the 275, the HL7 CDA provides the description of the attachment in clinical terms. The content of the attachment inside the HL7 CDA document can be either codified, marked up text, or a scanned image. In any case, it can be easily viewed by the bill reviewer, and, if it is codified CDA, it can also be processed automatically.

WC eBilling and HIPAA Claims White Paper
Page 1 of 26
ST*275*0001~Submitter, Receiver, Patient, Claim, Etc.
BIN*8642*MIME headersMIME boundary –abcdefghijklmnopq
--abcdefghijklmnopqimage/jpeg name=“lab_results.jpg”
--abcdefghijklmnopq--~SE*43*0001~
<section><caption>EMS TRANSPORT, DESTINATION SITE INFORMATION
<caption_cd V="15512-7"/></caption><paragraph>
<caption>EMS TRANSPORT DESTINATION SITE NAME<caption_cd V="18582-7"/>
</caption><content>Alfred Newman Neurological Institute</content>
</paragraph><paragraph>
<caption>EMS TRANSPORT, DESTINATION SITE ADDRESS<caption_cd V="18583-5"/>
</caption><content>123 Main St; Anytown, UT 85912
<local_markup descriptor="AD"><local_attr name="LIT" value=“123 Main St"/><local_attr name="CTY" value=“Anytown"/><local_attr name="STA" value="UT"/><local_attr name="ZIP" value="85912"/>
</local_markup></content>
</paragraph></section>
VQQLEz13d3cudmVyaXNpZ24uY29tL3JlcG9zaXRvcnkvQ1BTIEluY29ycC4gYnkgUmVmLixMSUFCLkxURChjKTk2MSYwJAYDVQQLEx1EaWdpdGFsIElEIENsYXNzIDEgLSBOZXRzY2FwZTEWMBQGA1UEAxMNS2VwYSBadWJlbGRpYTErMCkGCSqGSIb3DQEJARYca2VwYS56dWJlbGRpYUBlbnZveS1uZWljLmNvbTBcMA0GCSqGSIb3DQEBAQUAA0sAMEgCQQDTpPphGGti96yriSSzajE8HQXv9yCxWDfzFKQsKAd8SRyClY7GjNJxbwQGddqNIUTy6NKbVAoDhhSvB4kaT+mPAgMBAAGjggcIMIIHBDAJBgNVHRMEAjAAMIICHwYDVR0DBIICFjCCAhIwggIOMIICCgYLYIZIAYb4RQEHAQEwggH5FoIBp1RoaXMgY2VydGlmaWNhdGUgaW5jb3Jwb3JhdGVzIGJ5IHJlZmVyZW5jZSwgYW5kIGl0cyB1c2UgaXMgc3RyaWN0bHkgc3ViamVjdCB0bywgdGhlIFZlcmlTaWduIENlcnRpZmljYXRpb24gUHJhY3RpY2UgU3RhdGVtZW50IChDUFMpLCBhdmFpbGFibGUgYXQ6IGh0dHBzOi8vd3d3LnZlcmlzaWduLmNvbS9DUFM7IGJ5IEUtbWFpbCBhdCBDUFMtcmVxdWVzdHNAdmVyaXNpZ24uY29tOyBvciBieSBtYWlsIGF0IFZlcmlTaWduLCBJbmMuLCAyNTkzIENvYXN0IEF2ZS4sIE1vdW50YWluIFZpZXcsIENBIDk0MDQzIFVTQSBUZWwuICsxICg0MTUpIDk2MS04ODMwIENvcHlyaWdodCAoYykgMTk5NiBWZXJpU2lnbiwgSW5jLiAgQWxsIFJpZ2h0cyBSZXNlcnZlZC4gQ0VSVEFJTiBXQVJSQU5USUVTIERJU0NMQUlNRUQgYW5kIExJQUJJTElUWSBMSU1JVEVELqAOBgxghkgBhvhFAQcBAQGhDgYMYIZIAYb4RQEHAQECMCwwKhYoaHR0cHM6Ly93d3cudmVyaXNpZ24uY29tL3JlcG9zaXRvcnkvQ1BTIDARBglghkgBhvhCAQEEBAMCB4AwNgYJYIZIAYb4QgEIBCkWJ2h0dHBzOi8vd3d3LnZlcmlzaWduLmNvbS9yZXBvc2l0b3J5L0NQUzCCBIcGCWCGSAGG+EIBDQSCBHgWggR0Q0FVVElPTjogVGhlIENvbW1vbiBOYW1lIGluIHRoaXMgQ2xhc3MgMSBEaWdpdGFsIApJRCBpcyBub3QgYXV0aGVudGljYXRlZCBieSBWZXJpU2lnbi4gSXQgbWF5
Imag
eH
L7 C
DA-
enco
ded
275 X12Envelope
HL7 CDA-encodedandimage
Electronic Attachment (Hybrid)
This powerful mechanism of sending attachments electronically with the 275 has several important advantages: a) the linkage between the attachment and the electronic claim/eBill is complete and does not have the possibility of mis-matching attachments and claims/eBills; b) it allows for the transmission of “unsolicited” attachments at the same time as the claims/eBills; c) it allows the submission of attachments as a response to a request for additional information from the payer; d) many attachments can automatically sent in one single submission without requiring human intervention; e) the transmission mechanism is the same mechanism used by other EDI transmissions such as the 837; and f) the payer can view the attachments with a web browser, without the need for special software, using the style sheet and XSLT provided by HL7 as part of the standard.
These electronic attachments will significantly reduce the complexity and expense of administering WC for everybody involved.

WC eBilling and HIPAA Claims White Paper
Page 2 of 26
Contributors:
Name Company Email
Zubeldia, Kepa Ingenix [email protected]
Guidry, Sandra Ingenix [email protected]
Nichols, Conny Ingenix [email protected]
Greene, Tina Ingenix [email protected]
Maloney, Shawn Red Oak E-Commerce Solutions, Inc. (ROES), an Ingenix Company
Miller, Brandon Ingenix [email protected]

WC eBilling and HIPAA Claims White Paper
Page 3 of 26
Document Revision History:
Date Changed
Page / Section Changed Change Description