wednesday, august 21, 2013 1 virtual session #1 track 2: the human side of change by robert lloyd,...
TRANSCRIPT

Wednesday, August 21, 2013
1
Virtual Session #1 Track 2:The Human Side of Change
By Robert Lloyd, PhD & Dave Williams, PhDInstitute for Healthcare Improvement
Kim Werkmeister, RN, Cynosure

Robert Lloyd
Robert Lloyd, PhD is Executive Director of Performance Improvement for the Institute for Healthcare Improvement (IHI). Dr. Lloyd provides leadership in the areas of performance improvement strategies, statistical process control methods, development of strategic dashboards and building capacity and capability for quality improvement. He also serves as lead faculty for various IHI initiatives and demonstration projects in the US, the UK, Sweden, Denmark, New Zealand and Africa. Before joining the IHI, Dr. Lloyd served as the Corporate Director of Quality Resource Services for Advocate Health Care (Oak Brook, IL). He also served as Senior Director of Quality Measurement for Lutheran General Health System (Park Ridge, IL), directed the American Hospital Association's Quality Measurement and Management Project (QMMP) and served in various leadership roles at the Hospital Association of Pennsylvania. The Pennsylvania State University awarded all three of Dr. Lloyd’s degrees. His doctorate is in agricultural economics and rural sociology. Dr. Lloyd has written many articles and chapters in books. He is also the co-author of the internationally acclaimed book, Measuring Quality Improvement in Healthcare: A Guide to Statistical Process Control Applications (American Society for Quality Press, 2001, 5th printing) and the author of Quality Health Care: A Guide to Developing and Using Indicators, 2004 by Jones and Bartlett (Sudbury, MA).

Dave Williams
David M. Williams, PhD, Improvement Advisor, truesimple Consulting, is also on the teaching faculty of The George Washington University School of Medicine and Health Sciences. He is also a Six Sigma Black Belt and serves as faculty and an Improvement Advisor (IA) for the Institute for Healthcare Improvement, supporting teams through leading system changes using the Model for Improvement. Dr. Williams started his career as an urban street paramedic. For the last decade, he has acted as an internal and external IA to governmental agencies, hospitals, and for-profit and not-for-profit organizations. He works with clients to improve their organizations by enabling appreciation of systems, understanding of data and variation, testing changes, and recognizing the influence of psychology. He has published nearly 100 articles, led intensive workshops, presented at major conferences to thousands of attendees, and writes a popular blog.

Kim Werkmeister
4
Kim Werkmeister, RN, BA, CPHQ is a National Improvement Advisor working with the American Hospital Association / Health Research Educational Trust Hospital Engagement Network (HEN). As an Improvement Advisor, she is responsible for working directly with State Hospital Associations to drive improvement in hospital acquired conditions and patient harm in hospitals across the country. In addition, she is the lead Improvement Advisor for the Hospital Engagement Network for the Perinatal Harm initiative, the VTE Reduction initiative and the Psychiatric Affinity Group initiative.
Prior to this, Ms. Werkmeister worked with hospitals across California to improve patient outcomes, implement best practices, set up Quality/Risk programs, and prepare for and respond to licensing and accreditation activities. She served as an improvement advisor for both the California Public Hospital Improvement Collaborative and the California Partnership for Health/Patient Safety First Collaborative. She also served as the lead improvement advisor for the ICU Mortality Reduction Collaborative, a project focusing on reduction of mortality and morbidity in ICU care across the state of California.
Ms. Werkmeister is a Registered Nurse and graduated with a Bachelor of Arts degree from California State University Fullerton.

Where are you today?
5

Discussion Topics
• The critical role of Human Behavior in improvement
• Everett Roger’s adoption & diffusion journey
• Kurt Lewin’s unfreezing to refreezing journey
• Personality profiles & communication
Note that the material addressed in this session draws heavily upon the IHI Open School pre-work assignments. If you have not completed QI 105 Lessons 1 & 2
please take time to do so after this session.

The Sequence of Improvement
Spreading a change to other
locations
Developing a change
Implementing a change (HTG)
Testing a change
Act Plan
Study Do
Theory and Prediction
Test under a variety of conditions
Make part of routine operations
Source: Robert Lloyd, IHI 2013

Spreading a change to other
locations
Developing a change
Implementing a change (HTG)
Testing a change
Act Plan
Study Do
Theory and Prediction
Test under a variety of conditions
Make part of routine operations
Source: Robert Lloyd, IHI 2013
The Sequence of Improvement requires an understanding of Human Behavior

Deming on the role of Psychology
“Psychology helps us to understand people,
interaction between people and
circumstance, interaction between
customer and supplier, interaction between
teacher and pupil, interaction between a
manager and his people and any system of
management.” W. Edwards Deming, The New Economics, 2000, page 107

Important Concepts fromPsychology and Change Management
Differences in people: Motivations Preferences Aspirations Learning styles Beliefs, Values & Culture
Most changes aimed at improvement will have to recognize the differences in people and account for them.
See Appendix A for details on these differences

Opening Dialogue onHuman Behavior
• So how have your interactions gone?
• Consider for a moment, the impact of human behavior on your HEN improvement efforts.
1. What has worked well?
2. What has not worked so well?
3. What will you do differently as you move forward?
• Type your reflections into the Chat Box.

Pursing Perfection for VTE
Jane Northcutt, RNChief Quality Officer
Hospital Overview
• Located in Birmingham, Alabama• One of 15 General Acute Care Hospital Providers
in the Birmingham MSA (4-County)• Licensed Beds - 534
– 17 Rehabilitation Beds– 64 Psychiatric Beds
• Employees - 1,686• Physicians & Allied Health on Staff: 698 • Population for Primary Service Area - 437,957• Population for Secondary Service Area - 608,771

VTE - HEN Specific Run Charts

Aim?: By December 2013, 100% of patients will receive VTE prophylaxis by defined protocols, patient assessments or have documentation of contraindications.
Important? VTE is the #1 preventable cause of death in hospitalized patients.
Aim Statement
Changes Being Tested, Implemented or
Spread
Recommendations and Next Steps
Lessons Learned
Run Charts
•Assessment of patients for VTE prophylaxis is completed for Inpatients and ICU patients.
•Protocols are implemented timely.•VTE Discharge Instructions are completed.
•Patients requiring overlap therapy are identified with measures implemented.
•Surgery patients are assessed for appropriate prophylaxis.
•Build in discharge documentation tools in electronic system to populate on all patients.
• Identify patients from radiological studies for identification of needed overlap therapy and have PharmD review for appropriate coverage.
•Set required timeline actions before the timeline actually ends.
•Order set with physician to design with physician driven education to medical staff.
•Use PI Referral Form for staff involved to document why variance occurred and lesson learned.
Project Title: Reducing VTE by Improved compliance with VTE Measures Date: 8/10/2013
Hospital Name: Trinity Medical Center State: Alabama
© 2012 Institute for Healthcare Improvement
Team Members
Self Assessment Score = _5__
•Re-assess protocols and current actions with identified variances.
•Evaluate effect of new electronic clinical documentation on compliance.
CQOCore Measure AnalystPharmDPhysician Liaison Director of Surgical ServicesCNOICU Nursing DirectorMed-Surge Nursing Director
Medical VTE Prophylaxis

Lesson 1: Overcoming Resistance to Change Course: QI 105: The Human Side of Quality Improvement
Many People Don’t Like Change Have you ever walked into your house or office and discovered that something is different? Maybe your roommate rearranged the furniture. Maybe your spouse repainted a wall. How did you feel? If you are like most people, you were probably a little bit annoyed, a little bit frustrated, and maybe even anxious to undo the change. Needless to say, you probably didn't jump right in and embrace it.
Change in health care is not perceived all that differently from change in any other context. When organizations make changes to care processes, procedures, and policies — even if those changes are improvements — the people involved with those processes, procedures, and policies are often a little bit annoyed, a little bit frustrated, and maybe even anxious to figure out a way to go back.
When we talk about change and improvement, we often focus on the numbers, the processes, and the graphs. And we sometimes forget the people. In this lesson, you will learn about barriers to change as well as different ways that people might respond to change in a social system. You’ll also be introduced to a basic model of change that includes unfreezing the old way we do things, moving to the new way, and then refreezing the way we want the future to be.

So what does change look like?
Add Text Subtitle• Add Text, Graph, Picture
Add Text Subtitle• Add Text, Graph, Picture

So what does change look like?
Add Text Subtitle• Add Text, Graph, Picture
Add Text Subtitle• Add Text, Graph, Picture

Lesson 1: Overcoming Resistance to Change Course: QI 105: The Human Side of Quality Improvement
Your Turn
Think back to a time when you were confronted with a new process in a familiar setting. Maybe you were asked to swipe a card, rather than insert cash or tokens, when boarding the bus or train. Or maybe your entire country switched off analog TV broadcasting, making it impossible to watch your favorite show without a digital converter box.
Once you’ve got a process in mind, write down your answers to the following questions:
1. What emotions did you experience when first presented with this change?
2. Did you resist embracing the change? If so, what were the reasons?
3. At what point did you accept the change, if ever? What factors helped you accept it?
Enter your response to each question into the Chat Box.

Source: IHI Open School, QI 105 Lesson 1

Reasons for Resistance to Washing Your Hands with Hand Sanitizer
Did your list include any of the following reasons? • “Hand washing is incredibly basic. I don’t see why I need a special policy to
tell me how to wash my hands.” • “What’s wrong with regular soap and water?” • “There’s no way I’ll remember to use the sanitizer. Things are just too busy
and this change is not a priority.” • “That alcohol-based stuff is going to dry out my hands.” • “With all I have to do, I just don’t have time to use the sanitizer before
every patient visit.” • “I bet the dispensers won’t be located in a convenient place.” • “This sanitizer stuff is just a marketing gimmick.” • “This is just another new policy that’s here today, gone tomorrow.”
Source: IHI Open School, QI 105 Lesson 1
Let’s consider two of these reasons for resistance
In his book The Limits of Organizational Change (Tuscaloosa: University of Alabama Press; 1971), Herbert Kaufman identified a number of barriers that can affect the implementation of significant change in health care, including the following:
The expected autonomy or independence of health care workers: Often, health care professionals perceive themselves as single providers working independently to provide patient care. If a health care provider feels a change may reduce or alter that autonomy, he or she may be reluctant to embrace a change.
Example: “Hand washing is incredibly basic. I don’t see why I need a special policy to tell me how to wash my hands.”
Stability that comes with routine: Routines such as standard operating procedures, certain recurring behaviors, or institutionalized ways of communicating create stability for people. This is reflected in the common statement, "We've always done it this way, and I’m comfortable with it, so why change now?"
Example: “What’s wrong with regular soap and water?”
Source: IHI Open School, QI 105 Lesson 1

Anticipating Barriers to Change
As a reminder, the following are some of the barriers we considered for adopting the new hand hygiene policy and potential responses to these barriers:
Barriers• “Hand washing is incredibly basic. I don’t see why I need a special policy
to tell me how to wash my hands.”
• “What’s wrong with regular soap and water?”
ResponseProvide education on the value of using hand sanitizer to reducing the possibility of infection. Include evidence grounded in good research and information on the growing numbers of hospitals relying on this new practice.

How Can We Foster the Adoption of Successful Change Ideas?
The traditional approaches
MemoDate: February 2012
To: All Staff
From: Management
Starting next Monday, all staff will be
expected to implement the new
procedure we just tested in the 3 West
med/surg unit.
It worked there so in order to save time,
everyone will now start doing the new
procedure like 3 West.
Thank you for your
cooperation.

Adoption is a SOCIAL thing!
A better idea…
…communicated through a social network…
…over time

Diffusion of Innovations (1st edition1962)
A theory for understanding how people respond to innovation…
… and how to use those responses to drive needed
change

Diffusion of Innovations (1962)
An innovation, according to Rogers, is “an idea, practice, or object that is perceived as new by an individual or other unit of adoption.”
By this definition, the hand sanitizer example in this Open Scholl Lesson is an innovation, regardless of how long hand sanitizer has been on the market.
“If the idea seems new to the individual,” Rogers wrote, “it is an innovation.” And for many, washing their hands according to defined practice with sanitizer is innovative, even though it is not a new idea.
Source: IHI Open School, QI 105 Lesson 1

How Adopters
Adopt1.Awareness2.Persuasion3.Decision4.Implementation5.Confirmation
E. Roger’s Stages of Adoption

Adopter Categories See (see page 8 of QI 105 Lesson 1 for descriptions of the categories)
Rogers, E. M. (2003). Diffusion of innovations. New York, Free Press.

How Can We Foster Adoption of Successful Change Ideas?
A somewhat more sophisticated approach…

An Early Adopter

An Early Adopter
Falls
Bundle

Adopter Exercise 1
• Change 1: All primary care physicians should be required to provide on-line consultation to their patients.
• Lets see where each of us would place our self
in the adopter curve:– Innovators, early adopter, early majority, late
majority or laggard

Adopter Exercise 2
• Change 2: Each person in our country should have a: “medical information” chip inserted into their arm so they literally ‘carry their medical history with them.”
• Lets see where each of us would place our self in the adopter curve:– Innovator, early adopter, early majority, late
majority or laggard

The “Tipping Point”
“The name given to that one dramatic moment in an epidemic when everything can change all at once.”
- M. Gladwell
“The part of the diffusion curve from about 10 percent to 20 percent adoption is the heart of the diffusion process. After that point, it is often impossible to stop the further diffusion of a new idea, even if one wished to do so.”
- E. Rogers
Spread of Chronic Care Model Across Clinics
0
10
20
30
40
50
60
70
80
90
100
Sep-98
Oct Nov Dec Jan-99
Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan-00
Feb
Perc
ent o
f clin
ics
impl
emen
ting
CCM
Total of 80 Clinics in Organization
Tipping point

Valley Regional Hospital
Michael Lessard, RPh, MBADirector of Pharmacy

About Us
Critical Access Hospital 7 Physician practices General and Ortho
surgeries Infusion Center Home Health division JC Accredited Serving about 24,000
residents 37

Aim?: Reduce the incidence of harm due to high-alert medications by 50% by December 2013.
• Why is this project important?: Medications are the most common intervention in healthcare but are also most commonly associated with adverse events in hospitalized patients. At least 20% of all harm is associated with medication errors.
Aim Statement
Changes Being Tested, Implemented or
Spread
Recommendations and Next Steps
Lessons LearnedRun Charts
• Pharmacy dosing of warfarin in all Ortho/surgery patients
• Pharmacy dosing of warfarin as requested of any other in-patients
• Pharmacy monitoring of all warfarin patients
• Note in eMar when patient is receiving no dose of warfarin
• Set up order so pharmacy has daily printouts for warfarin patients
• Note daily INR and wafrarin doses in vital signs on emar so MD/nursing have running view of dosing
Project Title: Reducing ADEs by Pharmacy Warfarin Dosing Date: 6/10/2013Hospital Name: Valley Regional Hospital State: New Hampshire
© 2012 Institute for Healthcare Improvement
Team Members
Self Assessment Score = _5__
• Re-assess protocol for elderly
•Look at interaction evaluation process
Michael Lessard, RPhMichael Saracino, PharmDRichard Martin, RPh
Six Month TotalsDec-12 Jan-13 Feb-13 Mar-13 Apr-13 May-13 Totals
Over-Coagulated (INR>6)0 0 0 0 2 0 2
Patients Receiving Warfarin11 10 17 12 7 18 75
% INR > 6.0 0.00% 0.00% 0.00% 0.00% 28.57% 0.00% 2.67%
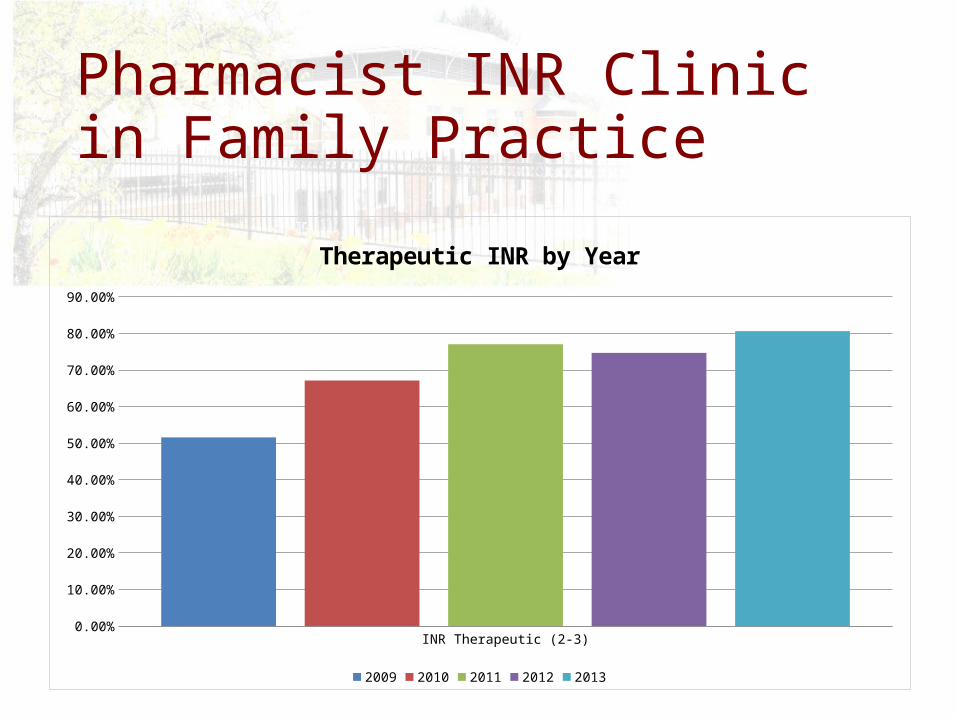
Pharmacist INR Clinic in Family Practice
INR Therapeutic (2-3)0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
Therapeutic INR by Year
2009 2010 2011 2012 2013

Basic Model for Understanding the Change Process
Kurt Lewin(1890-1947)
So far in this lesson, we have discussed some common barriers to change, and we have seen that not everyone adopts change at the same time or in the same way. Being conscious of this behavior can reduce your frustrations, and help you to work with the people involved in the change process.
So how can an organization help different types of people adjust to change?
Let’s take a look at one more model for understanding change in organizations. This mode, proposed by the psychologist Kurt Lewin, provides a simple way to understand the change process.

Lewin proposed that organizational change occurs in the following three stages:
1. Unfreezing 2. Change or transition 3. Freezing (or re-freezing)
In other words, Lewin suggests that in order to effect long-lasting change, you have to recognize that people have to be loosened from their old way, transitioned, and then molded into their new way.
It’s a conscious process that involves preparing people for change, actually managing the change, and then working to ensure that the change stays in place.
Lewin’s Change Model(see page 10 of QI 105 Lesson 1 for descriptions of the stages)
Source: IHI Open School, QI 105 Lesson 2
• I know I am motivated when …• I know I am lacking motivation when …• I know people are motivated when I see…• I know people are not motivated when I see …• I know the organization has de-motivated people when I see…
Stephen Brookfield, Becoming a Critically Reflective Teacher
Lewin’s model requires and understanding of Motivation!
Type your responses into the Chat Box
Motivation Assumptions Inventory

Lesson 2: What Motivates People to Change QI 105: The Human Side of Quality Improvement
Using Assessment Tools to Understand Team DynamicsThere are many assessment instruments that can help the members of a team better understand their individual strengths and preferences. For instance:
• StrengthsFinder 2.0 • Myers-Briggs Type Indicator (MBTI)• Strength Deployment Inventory (SDI) • DiSC Profile • Riso-Hudson Enneagram Type Indicator (RHETI)
Each tool is different and the decision of which tool to use, if any, often relies on personal preference. Some tools require qualified professionals to administer and interpret. Each tool takes a different look at people, but they all offer a lens into understanding our diversity and openness to change.
Source: IHI Open School, QI 105 Lesson 2

44 Where we are!

45
Where we
want to be!
Where we are!

46
Where we
want to be!
Where we are!
How do you
bridge the
gap between
these two
conditions?

Q X A = E
Adapted from General Electric’s approach to Six Sigma quality improvement
An equation for achieving results…

Q X A = EQuality
of a Solution
X Acceptance of a Solution
= Effectiveness of a Solution
Adapted from General Electric’s approach to Six Sigma quality improvement
An equation for achieving results…

The Primary Drivers of Improvement
Will
Ideas Execution
Having the Will (desire) to change the current state to one that is better
Developing Ideas that will contribute to making processes and outcome better
Having the capacity to apply CQI theories, tools and techniques that enable the Execution of the ideas
QI

Key Components* Self-Assessment • Will (to change)• Ideas• Execution
• Low Medium High• Low Medium High• Low Medium High
*All three components MUST be viewed together. Focusing on one or even two of the components will guarantee sub optimized
performance. Systems thinking lies at the heart of CQI!
How prepared is your organization?
So, what forces are
driving you forward?
And what forces are
holding you back?

Driving Forces (+) Restraining Forces (-)
Actions to reduce the Restraining Forces:
• • •
Issue or Project: _______________________________________________
Force Field Analysis Worksheet

Deming on the role of Psychology
“Psychology helps us to understand
people, interaction between people
and circumstance, interaction between
customer and supplier, interaction
between teacher and pupil, interaction
between a manager and his people and
any system of management.” W. Edwards Deming, The New Economics, 2000, page 107

Appendix A:Key Points on Motivation
1. Differences in PeopleFact: We each have our own preferences, aspirations, motivations, learning styles.Fact of Life: Most changes aimed at improvement will have to recognize the differences in people and account for them.
2. Behavior is Driven By MotivationFact: Behavior does not often give us a clear window into what is motivating someone’s behavior.Fact of Life: Understanding what is motivating someone rather than relying on our interpretation of the behavior can help us take appropriate actions to build commitment to change.

Appendix A:Key Points on Motivation (continued)
3. Fundamental Attribution ErrorFact: We make this error when explaining or rationalizing our behavior in terms of the situation while holding others accountable for their own behavior.Fact of Life: It is often easier to blame people than to take a hard look at how the system affects behavior.
4. Intrinsic and Extrinsic MotivationFact: Commitment to an activity will decline as extrinsic motivators are reduced or eliminated.Fact of Life: When a change is proposed, leaders need to explain the why of the change in terms of the organization’s values.
Appendix A:Key Points on Motivation (continued)
5. Attracting People to ChangeFact: Building commitment to change requires leaders to understand that change involves more than just the tangible and technical aspects of an activity.Fact of Life: People will resist change if they do not feel included or understand the benefits of the change to the organization or to themselves.