week 7 – arterial and venous thrombolysis
DESCRIPTION
Week 7 – Arterial and Venous Thrombolysis. Week 7 Objectives. Week 7 – Arterial and Venous Thrombolysis Discuss CVA and TIA Identify different types of Stroke Know Signs and Symptoms of a Stroke Know indications and contraindications for Stroke Discuss basic set-up for Stroke Intervention - PowerPoint PPT PresentationTRANSCRIPT
Week 7 – Arterial Week 7 – Arterial and Venous and Venous
ThrombolysisThrombolysis
Week 7 ObjectivesWeek 7 Objectives
Week 7 – Arterial and Venous Week 7 – Arterial and Venous ThrombolysisThrombolysis
Discuss CVA and TIADiscuss CVA and TIA Identify different types of StrokeIdentify different types of Stroke Know Signs and Symptoms of a StrokeKnow Signs and Symptoms of a Stroke Know indications and contraindications for Know indications and contraindications for
StrokeStroke Discuss basic set-up for Stroke InterventionDiscuss basic set-up for Stroke Intervention Discuss Thrombolytic DrugsDiscuss Thrombolytic Drugs Identify other methods of Intervention for Identify other methods of Intervention for
StrokesStrokes Discuss thrombolysis for dural sinus thrombosisDiscuss thrombolysis for dural sinus thrombosis
Thrombolysis DefinedThrombolysis Defined
Thrombolysis is a defined as “the Thrombolysis is a defined as “the process of breaking up and process of breaking up and dissolving blood clots.”dissolving blood clots.”
We will begin with the arterial We will begin with the arterial thrombolysis and the treatment of thrombolysis and the treatment of patients that have suffered from a patients that have suffered from a stroke.stroke.
Neuroradiology: Neuroradiology: Stroke Stroke
InterventionsInterventions “ “Time is Brain!”Time is Brain!”
Stroke InterventionsStroke Interventions
You will often hear the phrase “Time You will often hear the phrase “Time is brain!”is brain!”
Once a vessel is occluded by either a Once a vessel is occluded by either a clot or other debris, brain ischemia clot or other debris, brain ischemia begins immediately.begins immediately.
Time is brain and the clock is ticking.Time is brain and the clock is ticking.
Stroke InterventionsStroke Interventions
What is a StrokeWhat is a Stroke? ? “Stroke is a “Stroke is a cardiovascular disease. It affects cardiovascular disease. It affects the arteries leading to and within the arteries leading to and within the brain. A stroke occurs when a the brain. A stroke occurs when a blood vessel that brings oxygen blood vessel that brings oxygen and nutrients to the brain bursts or and nutrients to the brain bursts or is clogged by a blood clot or some is clogged by a blood clot or some other particle.”other particle.”
Terminology of StrokesTerminology of Strokes
CVA –Cerebrovascular AccidentCVA –Cerebrovascular Accident Brain AttackBrain Attack TIA- Transient Ischemic AttackTIA- Transient Ischemic Attack SAH-Subarachnoid HemorrhageSAH-Subarachnoid Hemorrhage ICH- Intracranial HemorrhageICH- Intracranial Hemorrhage InfarctInfarct
Every 45 seconds, someone in America has a Every 45 seconds, someone in America has a stroke. About 700,000 Americans will have a stroke. About 700,000 Americans will have a stroke this year. Stroke is our nation's No. 3 killer stroke this year. Stroke is our nation's No. 3 killer and a leading cause of severe, long-term and a leading cause of severe, long-term disability. disability.
Stroke kills nearly 273,000 people/yearStroke kills nearly 273,000 people/year In 2006, the estimated direct and indirect cost of In 2006, the estimated direct and indirect cost of
stroke is $57.9 billion.stroke is $57.9 billion. 50 percent had one-sided paralysis 50 percent had one-sided paralysis 30 percent were unable to walk without some 30 percent were unable to walk without some
assistance assistance
Stroke/Infarction StatisticsStroke/Infarction Statistics
Stroke/Infarction StatisticsStroke/Infarction Statistics (continued)(continued)
26 percent were dependent in activities of daily 26 percent were dependent in activities of daily living (grooming, eating, bathing, etc.) living (grooming, eating, bathing, etc.)
19 percent had aphasia (trouble speaking or 19 percent had aphasia (trouble speaking or understanding the speech of others) understanding the speech of others)
35 percent had depressive symptoms 35 percent had depressive symptoms 26 percent were institutionalized in a nursing 26 percent were institutionalized in a nursing
homehome from the American Stroke Association a division of from the American Stroke Association a division of
the American Heart Associationthe American Heart Association
Causes of Stroke:Causes of Stroke:
Complications of several disordersComplications of several disorders
Atherosclerosis – most common.Atherosclerosis – most common. Hypertension, smoking, diabetes.Hypertension, smoking, diabetes. Heart disease – Atrial fibrillation.Heart disease – Atrial fibrillation. Other: Other:
Trauma – fat embolismTrauma – fat embolism Tumor, InfectionTumor, Infection Caissons disease – The Bends (ex: Scuba Caissons disease – The Bends (ex: Scuba
Divers can suffer from Decompression Divers can suffer from Decompression sickness)sickness)
Types of StrokesTypes of Strokes
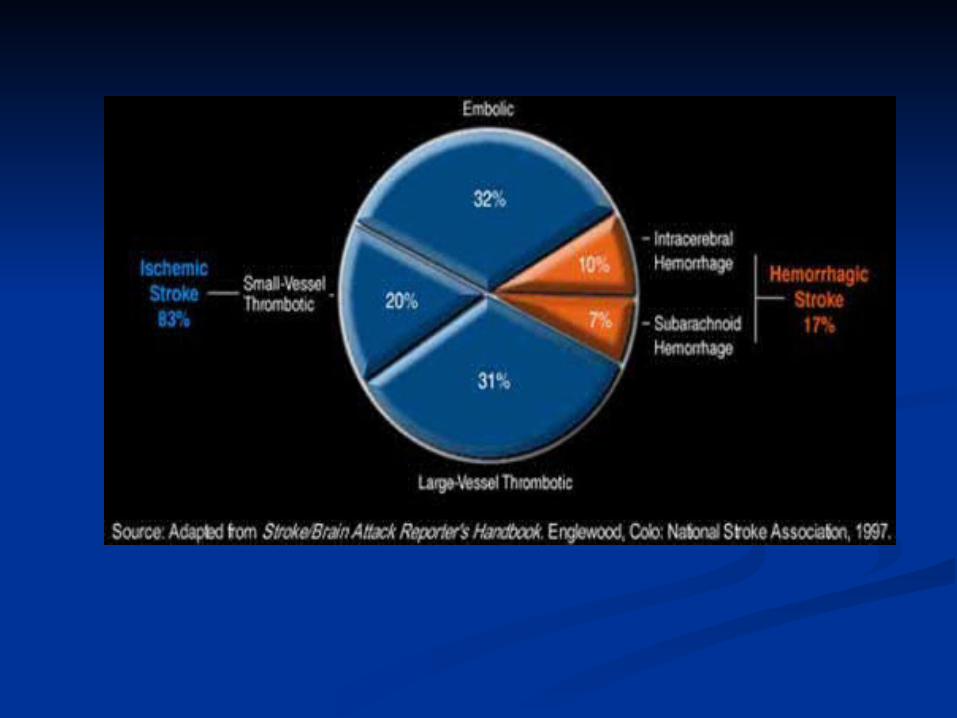
Ischemic- vessel clogs within Ischemic- vessel clogs within (accounts for 83% of all cases)(accounts for 83% of all cases)
Hemorrhagic- vessel ruptures causing Hemorrhagic- vessel ruptures causing blood to leak into the brain (17% of all blood to leak into the brain (17% of all cases)cases)
TIAs (Transient Ischemic Attacks)-TIAs (Transient Ischemic Attacks)-temporary minor or warning signs temporary minor or warning signs
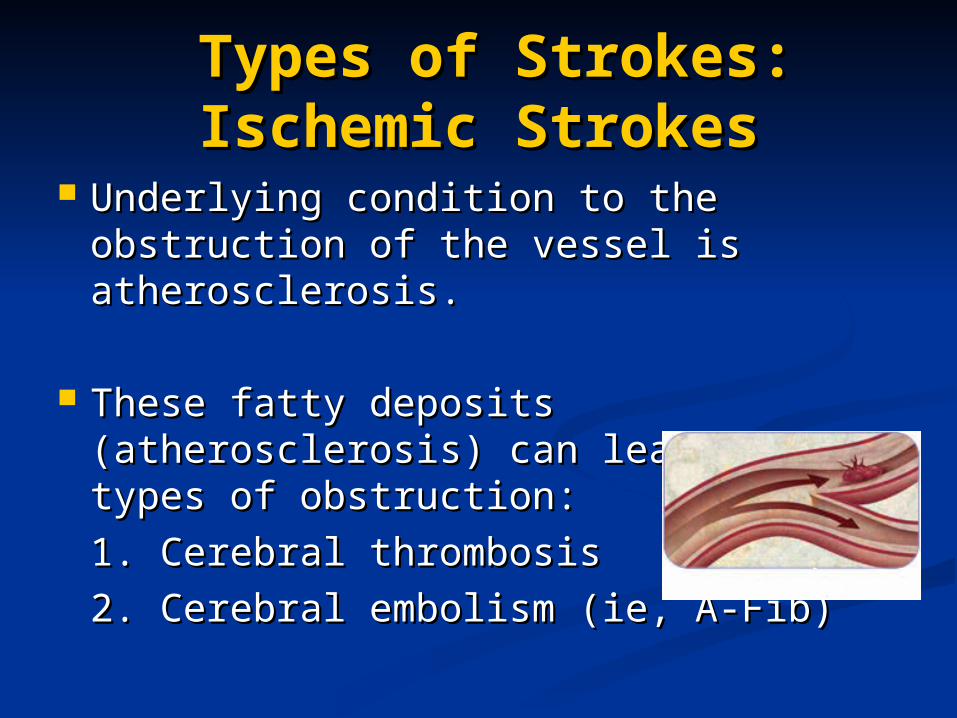
Types of Strokes: Types of Strokes: Ischemic StrokesIschemic Strokes
Underlying condition to the Underlying condition to the obstruction of the vessel is obstruction of the vessel is atherosclerosis.atherosclerosis.
These fatty deposits (atherosclerosis) These fatty deposits (atherosclerosis) can lead to two types of obstruction:can lead to two types of obstruction:
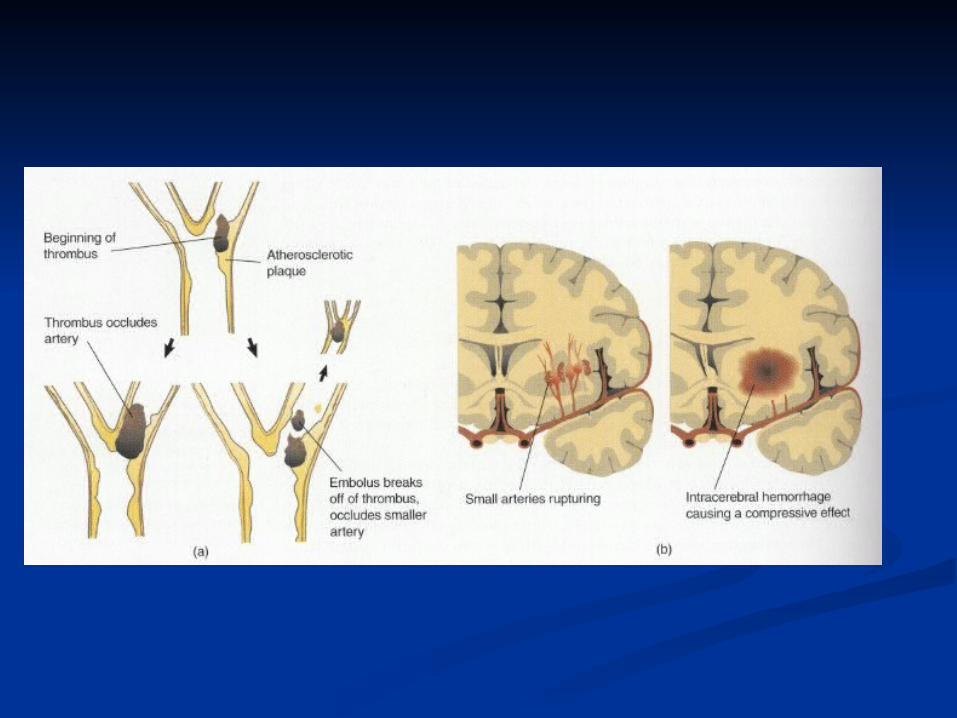
1. Cerebral thrombosis1. Cerebral thrombosis
2. Cerebral embolism (ie, A-Fib)2. Cerebral embolism (ie, A-Fib)
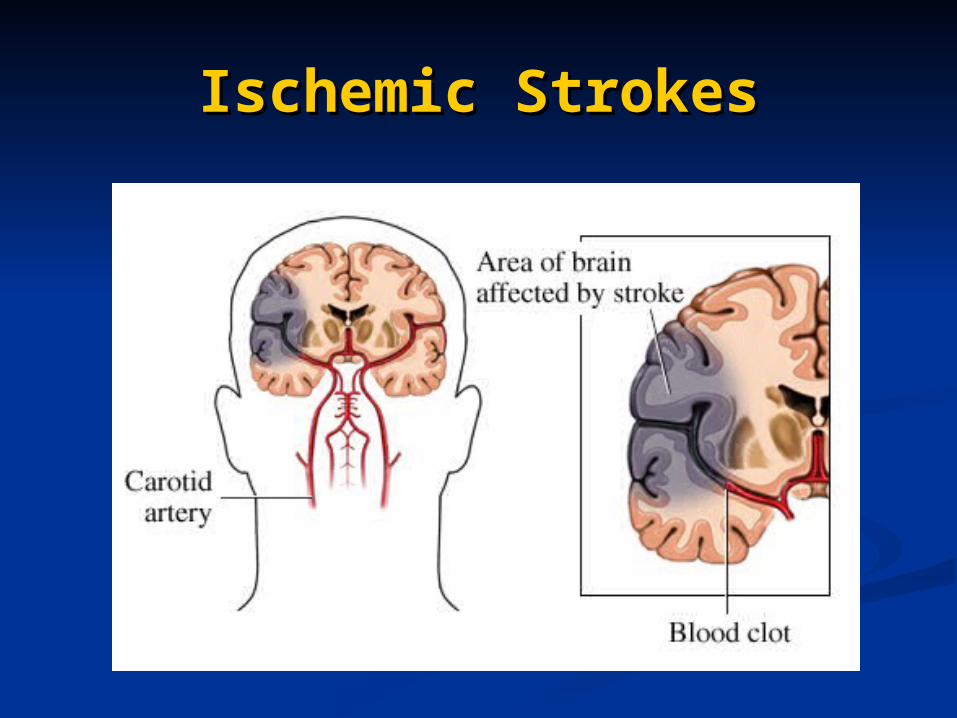
Ischemic StrokesIschemic Strokes
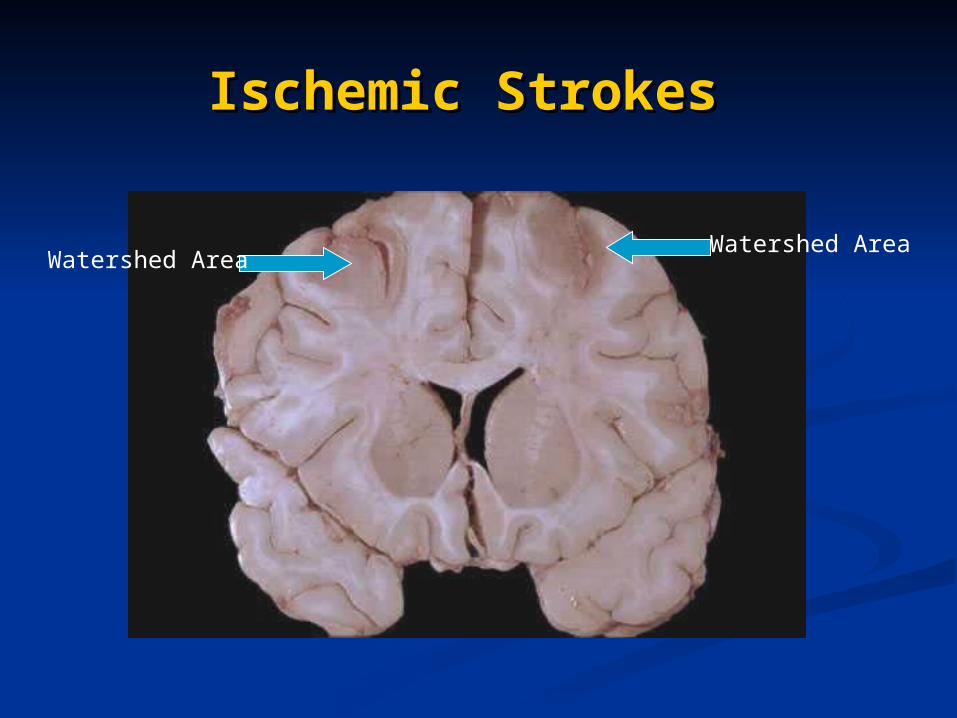
Ischemic Strokes Ischemic Strokes
Watershed AreaWatershed Area
Ischemic StrokesIschemic Strokes
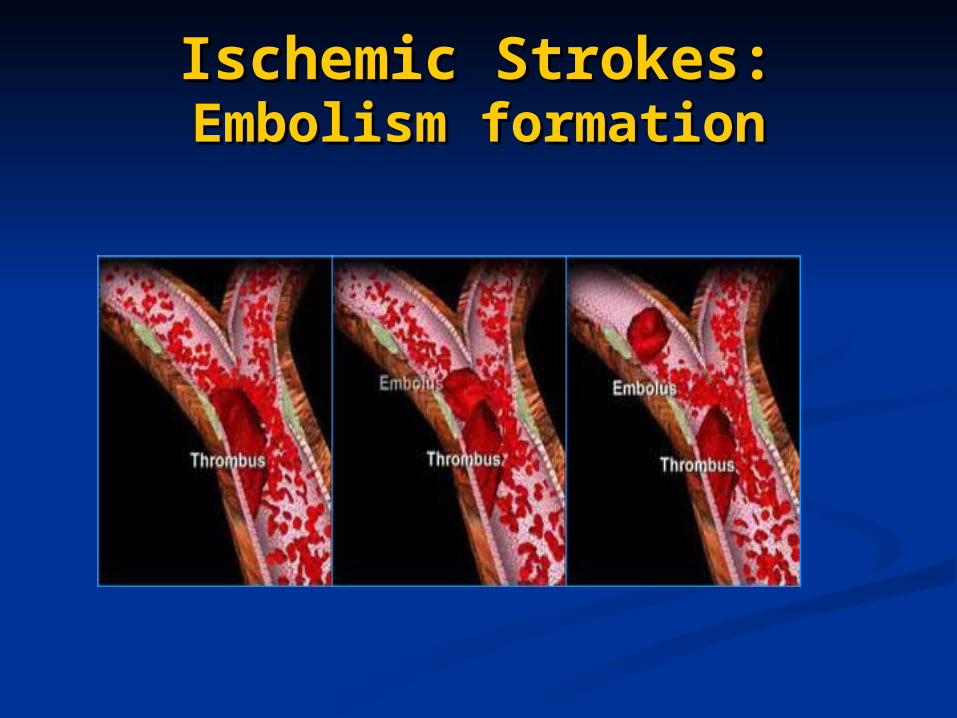
Embolism formationEmbolism formationIschemic Strokes:Ischemic Strokes:
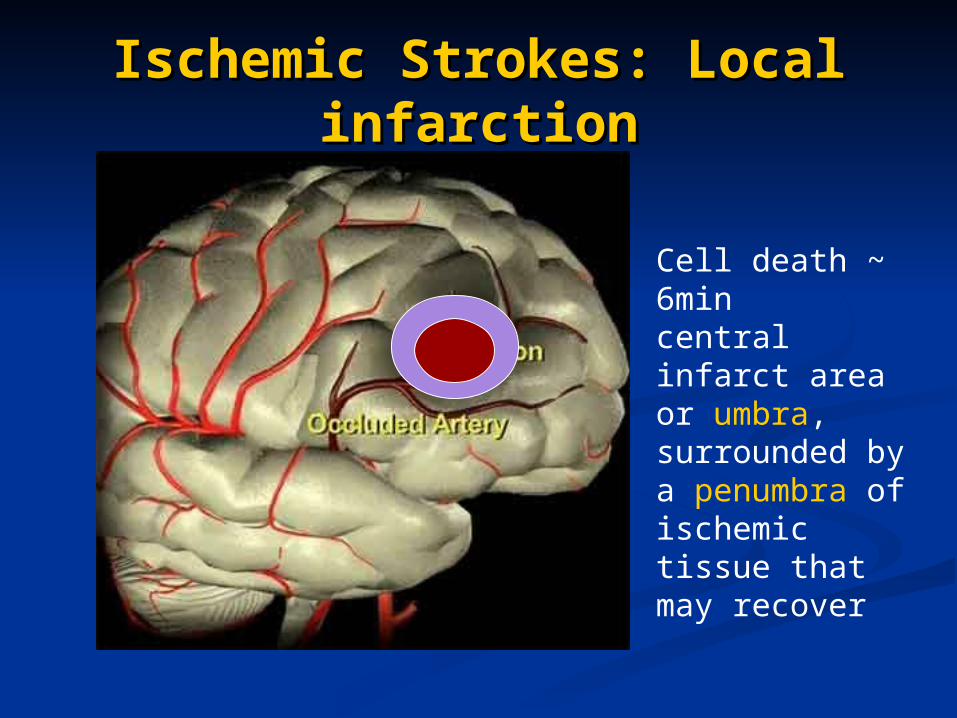
Ischemic Strokes: Local Ischemic Strokes: Local infarctioninfarction
Cell death ~ 6mincentral infarct area or umbra, surrounded by a penumbra of ischemic tissue that may recover
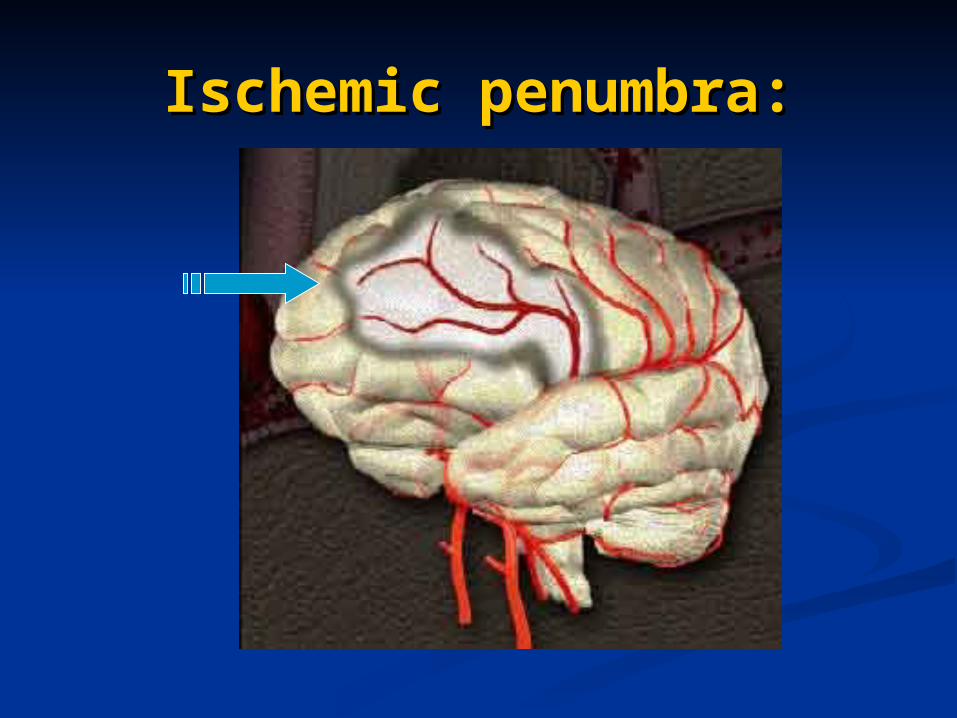
Ischemic penumbra:Ischemic penumbra:
Ischemic Strokes:Ischemic Strokes: Infarct Infarct PathogenesisPathogenesis
Reduced blood supply – hypoxia/anoxia.Reduced blood supply – hypoxia/anoxia. Altered metabolism Altered metabolism Na/K pump Na/K pump
block. block. Glutamate receptor act. Glutamate receptor act. calcium calcium
influx.influx. 1-6 min – ischemic injury – vacuolation.1-6 min – ischemic injury – vacuolation. >6 min – cell death.>6 min – cell death.
Infarct Stages:Infarct Stages: Immediate – Immediate – 6 hours6 hours
No Change both gross & microNo Change both gross & micro Acute stage – Acute stage – 2 days2 days
Edema, loss of grey/white matter border.Edema, loss of grey/white matter border. Inflammation, Red neurons, neutrophilsInflammation, Red neurons, neutrophils
Intermediate stage – Intermediate stage – 2 weeks.2 weeks. Demarcation, soft friable tissue, cystsDemarcation, soft friable tissue, cysts Macrophages, liquifactive necrosisMacrophages, liquifactive necrosis
Late stage – After Late stage – After 4 weeks.4 weeks. Fluid filled cysts with dark grey margin (gliosis)Fluid filled cysts with dark grey margin (gliosis) Removal of tissue by macrophagesRemoval of tissue by macrophages Gliosis – proliferation of glia, loss of architecture. Gliosis – proliferation of glia, loss of architecture.
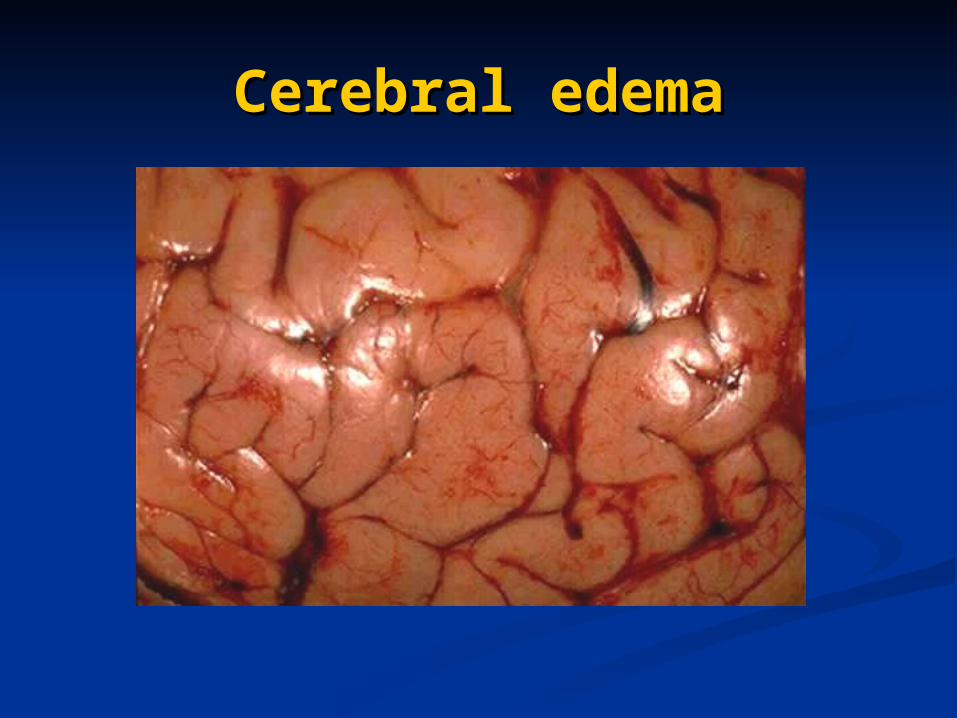
Cerebral edemaCerebral edema
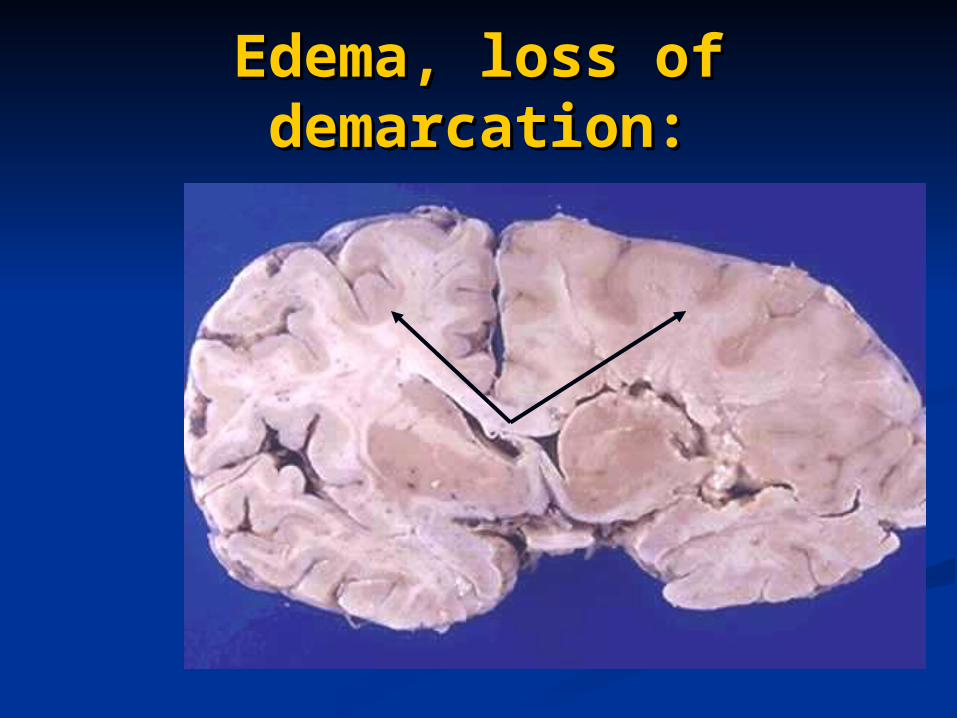
Edema, loss of Edema, loss of demarcation:demarcation:
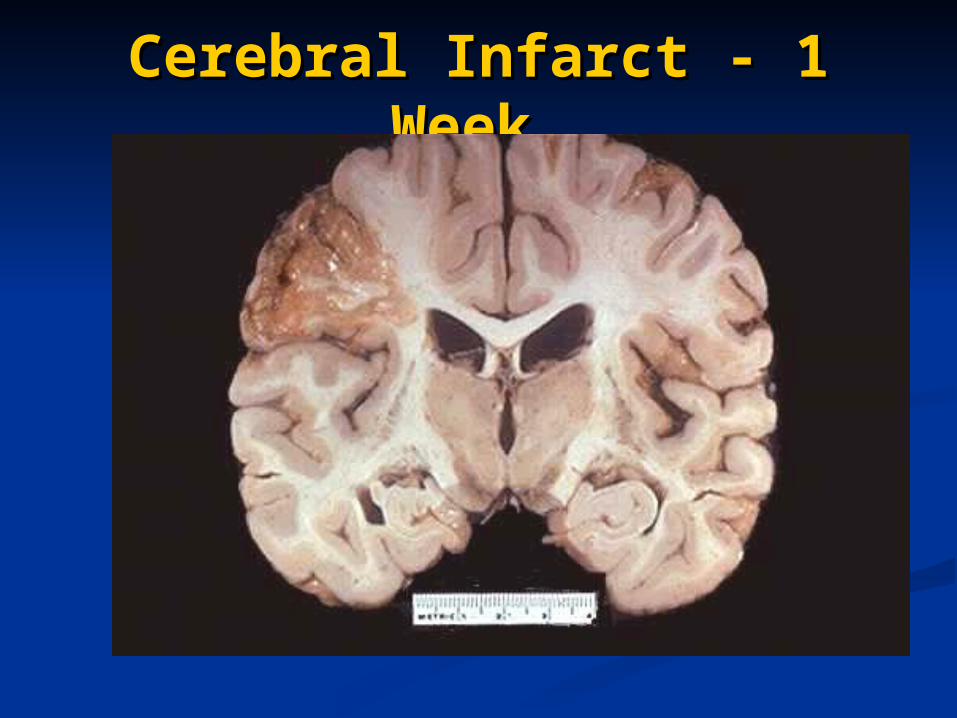
Cerebral Infarct - 1 WeekCerebral Infarct - 1 Week
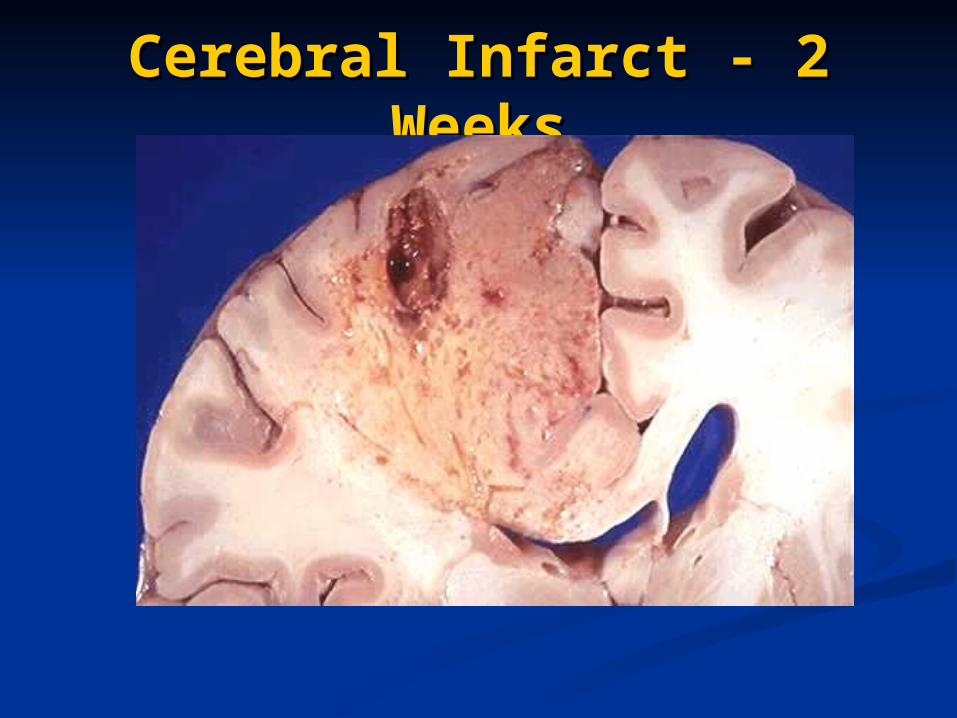
Cerebral Infarct - 2 Cerebral Infarct - 2 WeeksWeeks
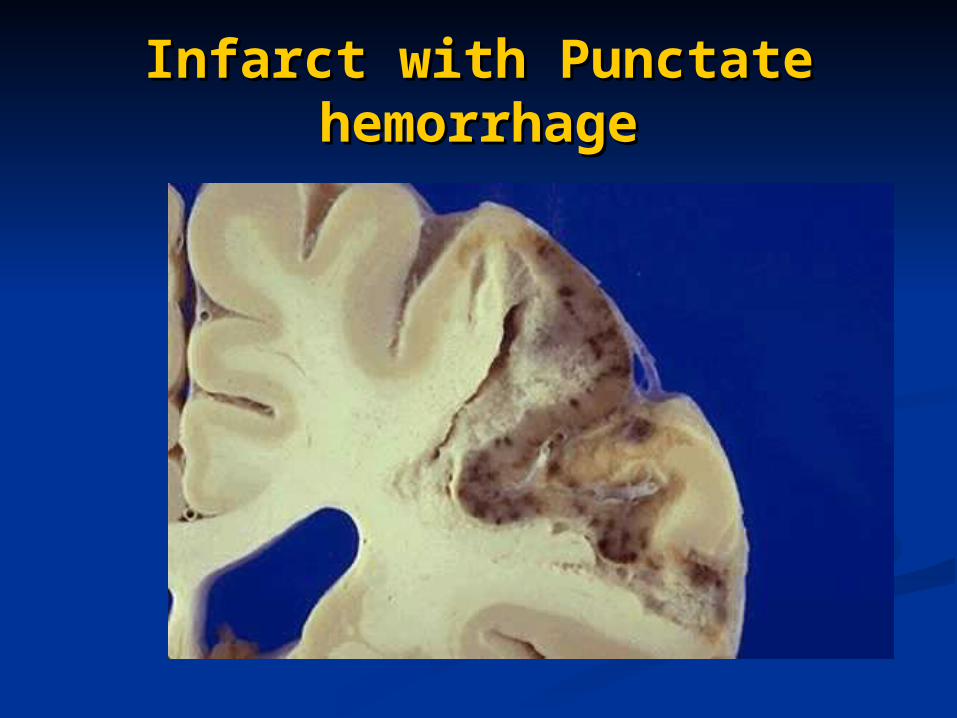
Infarct with Punctate Infarct with Punctate hemorrhagehemorrhage
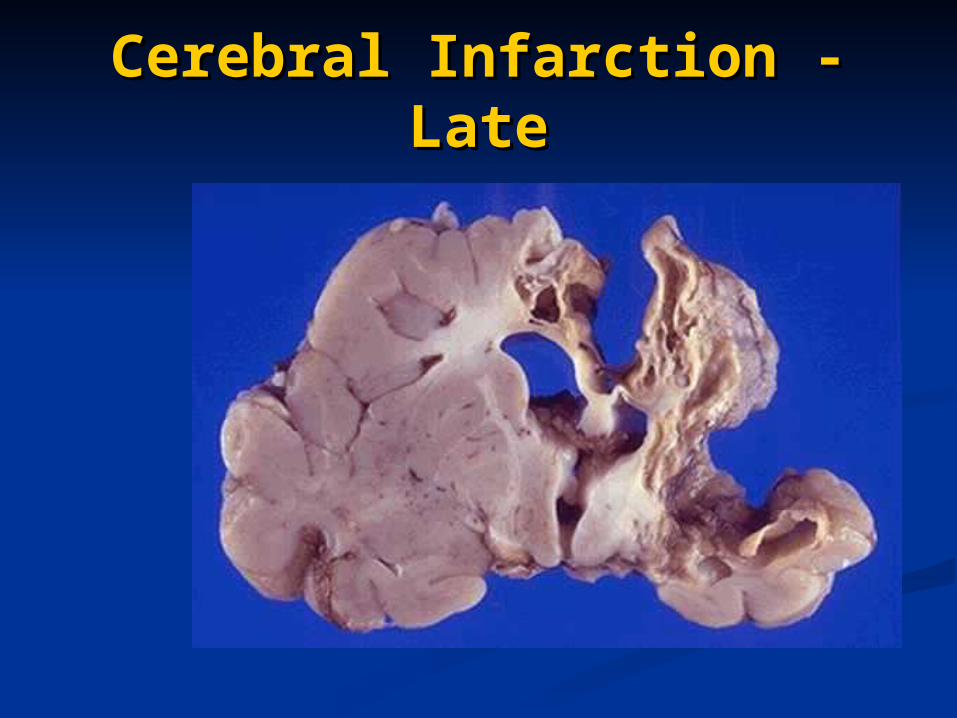
Cerebral Infarction - Cerebral Infarction - LateLate
Types of Strokes: Types of Strokes: Hemorrhagic StrokesHemorrhagic Strokes
Two types of hemorrhagic strokes:Two types of hemorrhagic strokes:
1. Intracranial 1. Intracranial Hemorrhage/ICH(usually caused by Hemorrhage/ICH(usually caused by Aneurysm’s or AVMs)Aneurysm’s or AVMs)
2. Subarachnoid Hemorrhage/SAH2. Subarachnoid Hemorrhage/SAH
Intracranial Hemorrhage:Intracranial Hemorrhage:
TRAUMA: Epidural Subdural
VASCULAR & TRAUMA Intracerebral Subarachnoid
Mixed cerebral-subarachnoid
• Intracerebral - Hypertension• Subarachnoid - Berry aneurysm + HTN• Mixed cerebral – Vascular malformations.
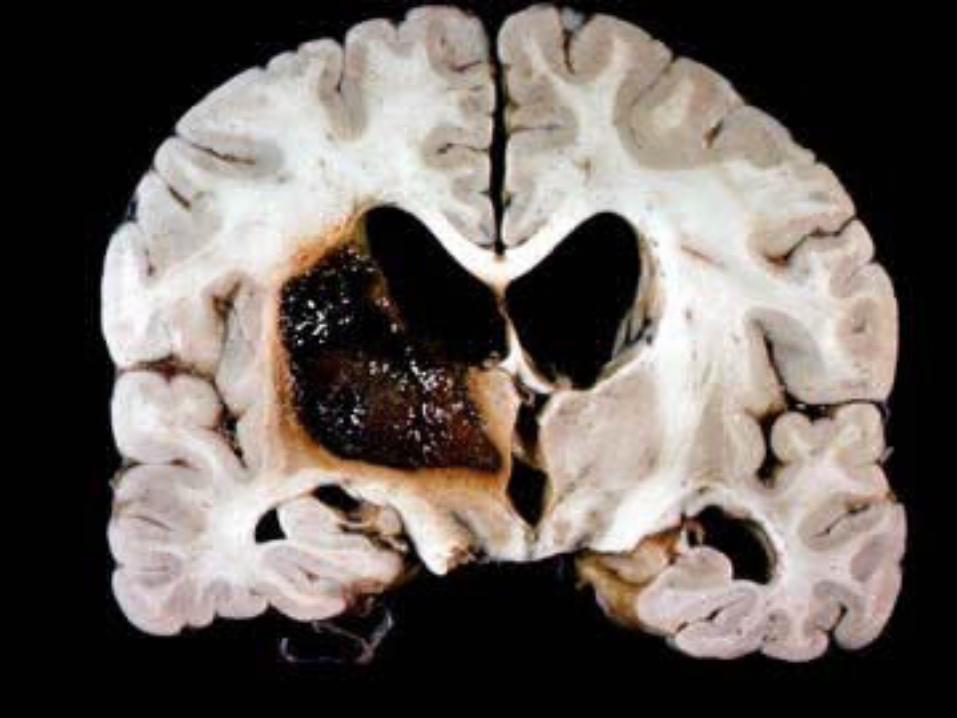
Hypertensive CVDHypertensive CVD
Massive Intracerebral HemorrhageMassive Intracerebral Hemorrhage Ganglionic & Lobar hemorrhagesGanglionic & Lobar hemorrhages Putamen(60%), thalamus, ventricles.Putamen(60%), thalamus, ventricles.
Slit hemorrhages.Slit hemorrhages. Microhemorrhages heal as slit spaces.Microhemorrhages heal as slit spaces.
Lacunar infarctsLacunar infarcts Brain stem pale infarcts – arteriolar sclerosisBrain stem pale infarcts – arteriolar sclerosis
Hypertensive encephalopathyHypertensive encephalopathy Headache, confusion, vomiting – raised ICP.Headache, confusion, vomiting – raised ICP.
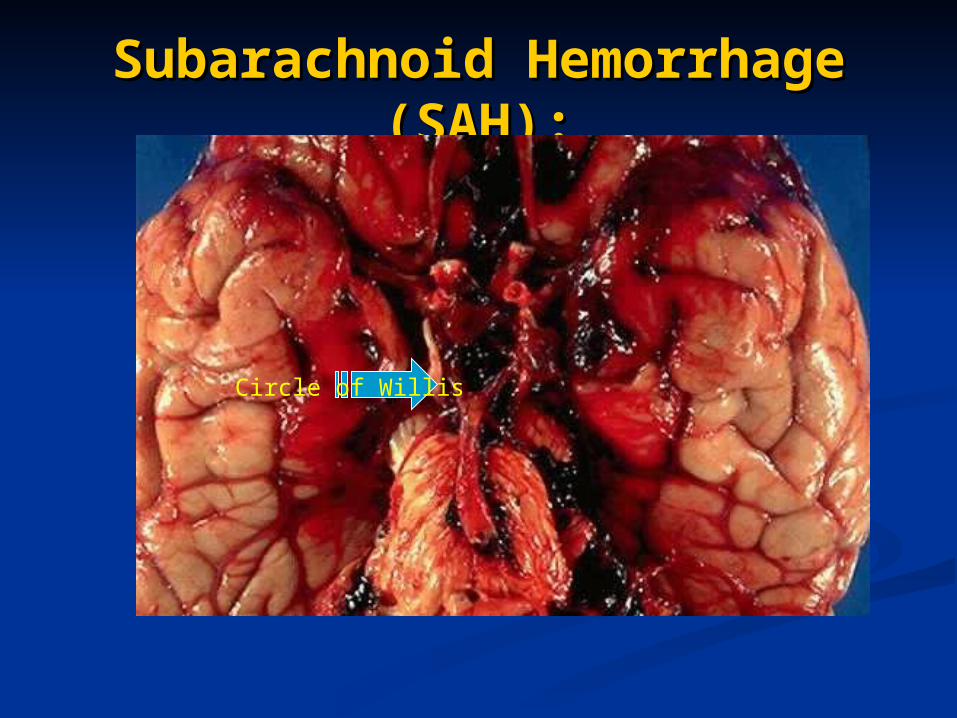
Subarachnoid Hemorrhage Subarachnoid Hemorrhage (SAH):(SAH):
Circle of Willis
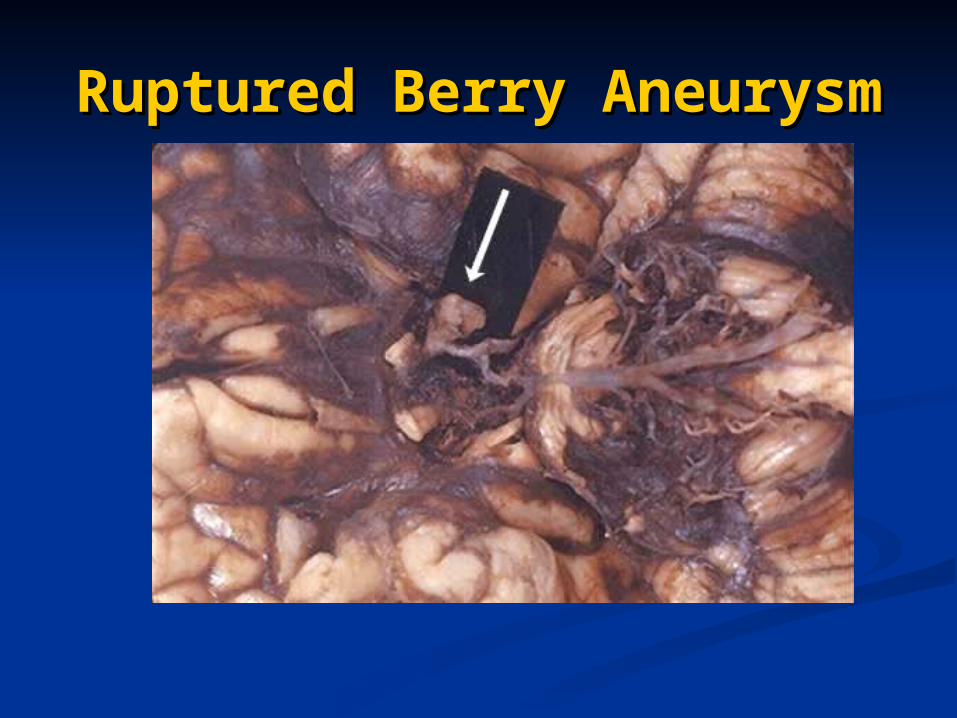
Ruptured Berry Ruptured Berry AneurysmAneurysm
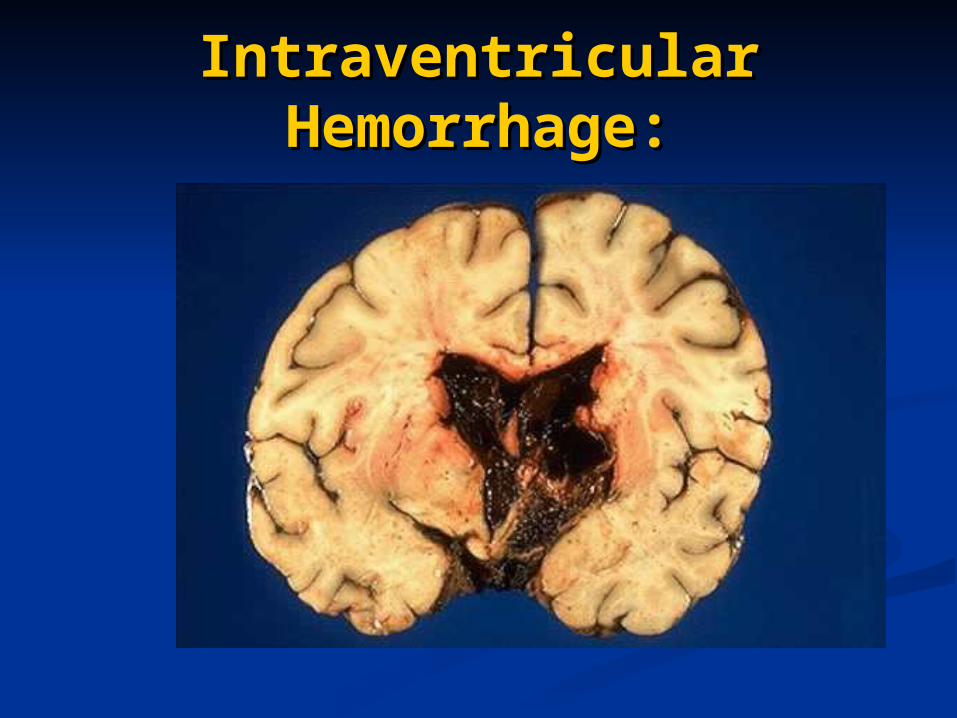
Intraventricular Intraventricular Hemorrhage:Hemorrhage:
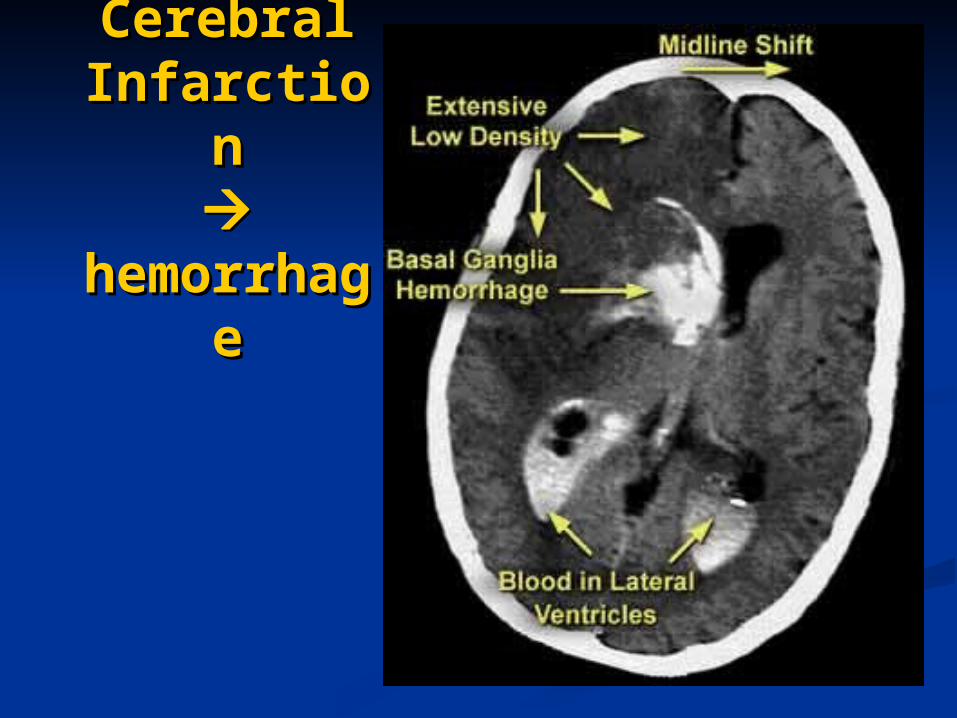
Cerebral Cerebral InfarctioInfarctio
nn
hemorrhhemorrhageage
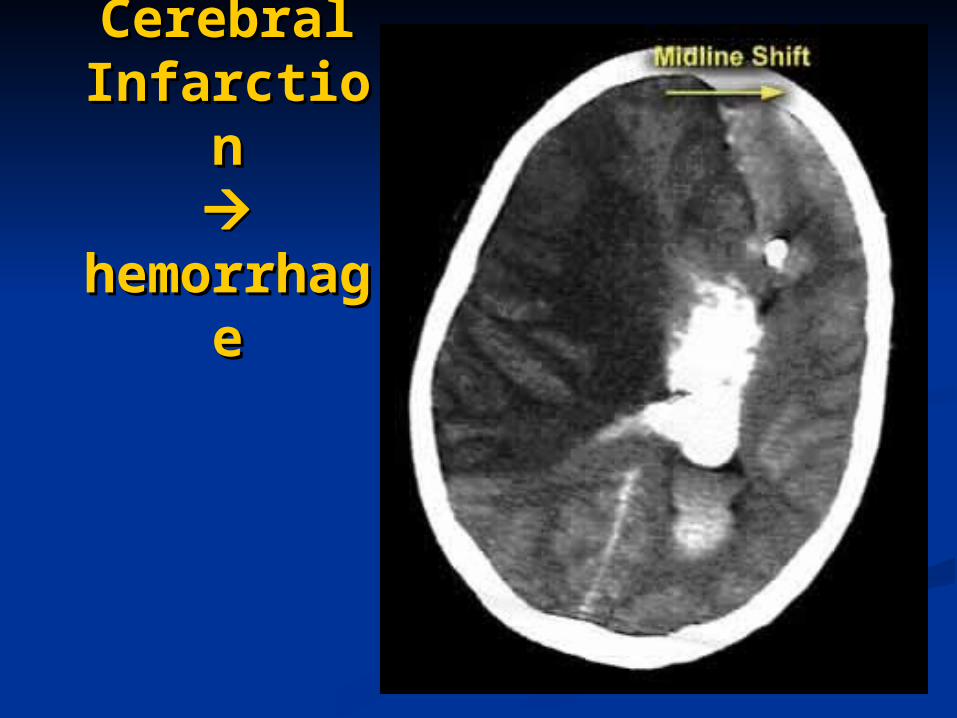
Cerebral Cerebral InfarctioInfarctio
nn
hemorrhhemorrhageage
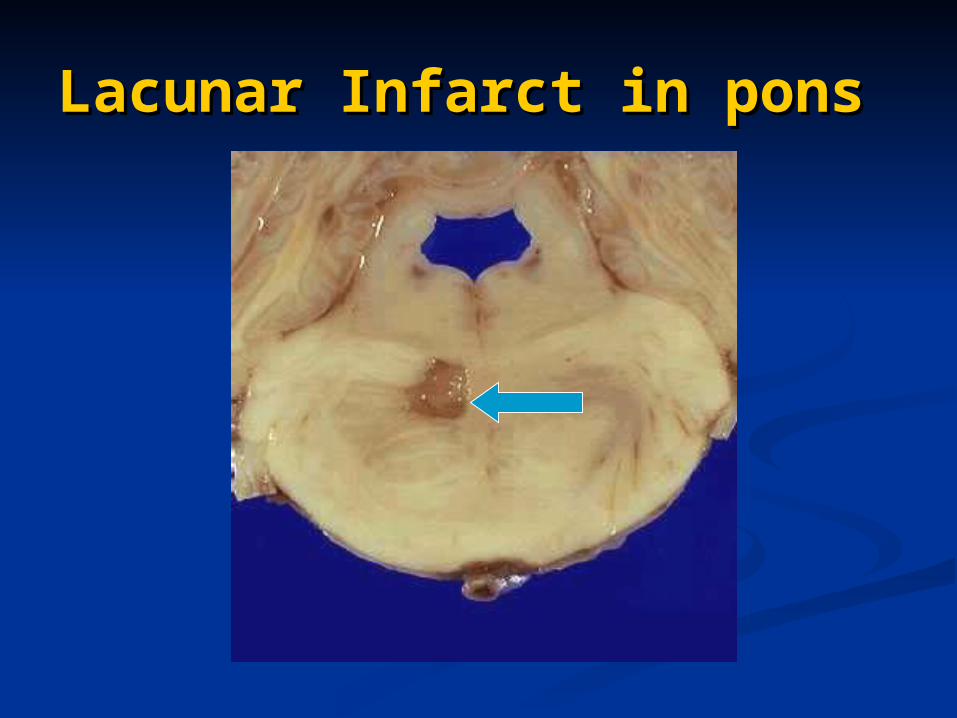
Lacunar Infarct in ponsLacunar Infarct in pons
Types of Strokes:Types of Strokes:Transient Ischemic Attacks Transient Ischemic Attacks
(TIAs)(TIAs) Warning Signs for Possible StrokeWarning Signs for Possible Stroke
Temporary Effects, gradually resolveTemporary Effects, gradually resolve
•A Transient Ischemic Attack (TIA) is a brief episode in which neurologic deficits suddenly occur, but then disappear completely
• Most TIAs last a few minutes to an hour.
• No neurologic deficits remain once a TIA has ended, because little or no brain tissue is permanently damaged.
• A TIA is an indicator that the stage is set for an ischemic stroke.
• Treatment of patients with TIAs can significantly reduce their risk of having a stroke.
TIAs: What are they? TIAs: What are they?
• Patients commonly describe a gray or black fog or a mist clouding vision in all or part of one eye.
• Attacks are typically brief (1-5 minutes), and afterwards vision is fully restored.
• TMB often signals the presence of severe ipsilateral carotid artery disease in older adults.
• TMB can also be caused by migraine.
TMB (also known as amaurosis fugax) occurs when the retina becomes temporarily ischemic.
TIAs: Carotid Territory Transient monocular blindness (TMB)
TIAs: Carotid Territory Transient monocular blindness (TMB)
Two Ideas:1. Thrombus from ulcerated atherosclerotic plaque at the origin of the internal carotid artery enters ophthalmic artery and plugs retinal vessel.
• A small embolic particle can produce retinal ischemia or block the central retinal artery. • If the embolus (often a platelet-fibrin aggregate) falls apart, blood flow is restored and and vision returns.
2. Low perfusion in the internal carotid artery, putting distal structures like the retina at risk.
• This mechanism implies presence of severe carotid stenosis that significantly impairs blood flow.
TMB: What causes it? TMB: What causes it?
• One-sided limb weakness, clumsiness or paralysis
• One-sided numbness, paresthesia, or sensory loss
• Difficulty with language production or comprehension
• Inability to articulate words clearly, often described as ‘I slurred my words’ (dysarthria)
• Partial or complete homonymous visual field defects (patients seldom describe these)
Problems typically produced
TIAs: Carotid Territory Transient hemispheric attacks
TIAs: Carotid Territory Transient hemispheric attacks
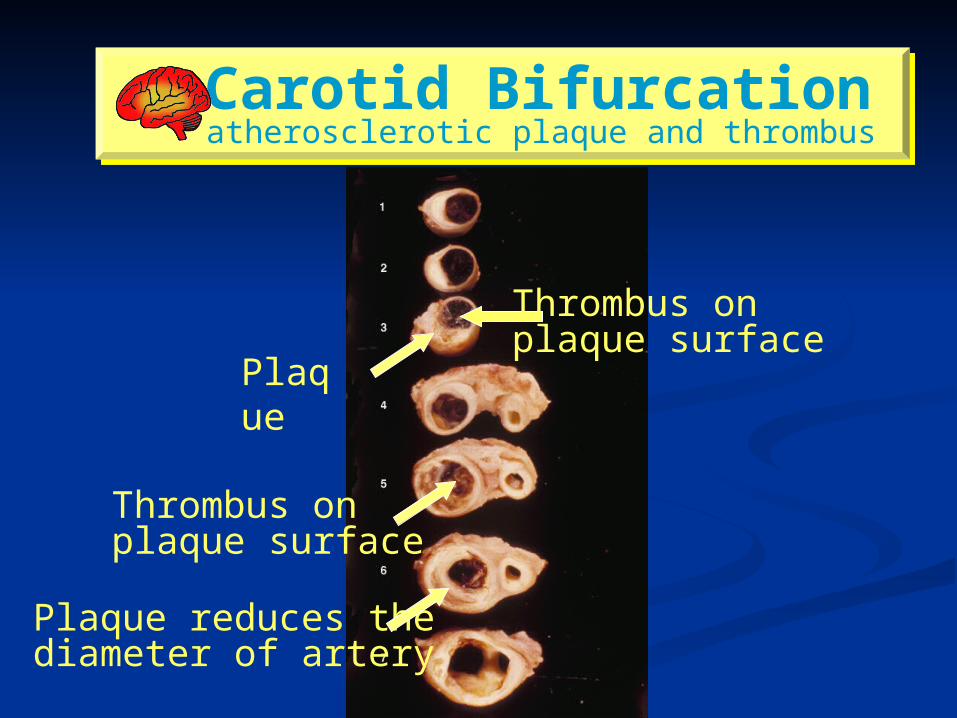
Carotid Bifurcation atherosclerotic plaque and thrombus Carotid Bifurcation atherosclerotic plaque and thrombus
Plaque
Thrombus onplaque surface
Thrombus onplaque surface
Plaque reduces thediameter of artery
• Vertigo or dizziness
• Unilateral or bilateral weakness or clumsiness
• Unilateral or bilateral numbness or sensory loss
• Limb ataxia or coarse tremor, staggering gait
• Dysarthria
• Visual field defect, blindness, or diplopia
• Nystagmus (‘it jumps around when I look at it’)
Problems typically produced
TIAs: Vertebral-Basilar Various combinations may be present
TIAs: Vertebral-Basilar Various combinations may be present
Because the episode of impaired function is brief, patients may not tell you about it unless you ask.
Seniors with somewhat impaired memory may simply not recall such brief events.
• TIAs in carotid territory predict severe atherosclerosis in the proximal internal carotid artery.
• Tests can determine actual blood flow in the carotid.
• The odds of stroke in the next 1-2 weeks are great!
• If severe narrowing is present, surgical and medical treatments can help to reduce stroke risk.
Patients may ignore TIAs! Patients may ignore TIAs!
Summary of Stroke Summary of Stroke Causes:Causes:
Stroke: Acute neurological deficit - ClinicalStroke: Acute neurological deficit - Clinical Cerebrovascular Accident – pathology.Cerebrovascular Accident – pathology. Ischemic/HemorrhagicIschemic/Hemorrhagic Thrombosis, Embolism/HemorrhageThrombosis, Embolism/Hemorrhage Atherosclerosis, Hypertension, Heart Disease.Atherosclerosis, Hypertension, Heart Disease. Global – Systemic Hypoxia – Watershed infarctGlobal – Systemic Hypoxia – Watershed infarct Focal – Thrombosis, Embolism or HemorrhageFocal – Thrombosis, Embolism or Hemorrhage Liquifaction necrosis Liquifaction necrosis Cyst formation, gliosis. Cyst formation, gliosis. Hypertension – Pale, Lacunar infarcts, slit Hypertension – Pale, Lacunar infarcts, slit
hemorrhagehemorrhage
Risk factors of Strokes:Risk factors of Strokes:
Non modifiableNon modifiable AgeAge Male sexMale sex RaceRace HeredityHeredity
ModifiableModifiable HypertensionHypertension DiabetesDiabetes SmokingSmoking HyperlipidemiaHyperlipidemia Excess AlcoholExcess Alcohol Heart disease (AF) Heart disease (AF) Oral Oral
contraceptivescontraceptives HypercoagulabilityHypercoagulability
..
Signs and symptoms of StrokeSigns and symptoms of Stroke
Sudden onset of:Sudden onset of:– numbness or weakness of the face, arm or leg, numbness or weakness of the face, arm or leg,
especially on one side of the body especially on one side of the body – confusion, trouble speaking or understanding confusion, trouble speaking or understanding – trouble seeing in one or both eyes trouble seeing in one or both eyes – trouble walking, dizziness, loss of balance or trouble walking, dizziness, loss of balance or
coordination coordination – severe headache with no known cause severe headache with no known cause
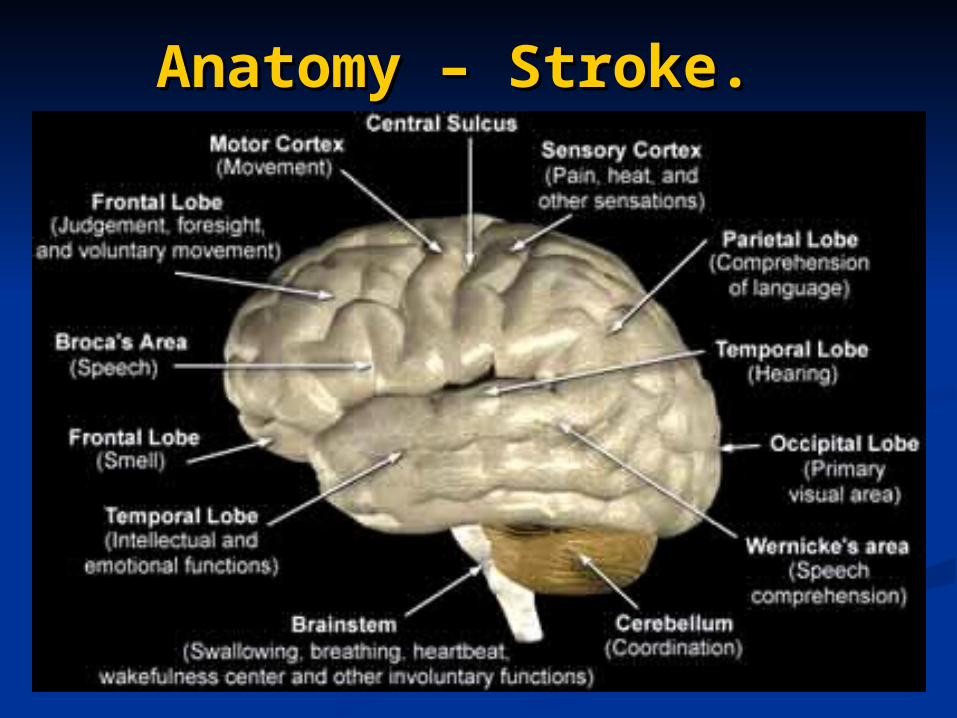
Anatomy – Stroke.Anatomy – Stroke.
Left (Dominant) Hemisphere Stroke: Left (Dominant) Hemisphere Stroke: Common PatternCommon Pattern
AphasiaAphasia RightRight hemiparesishemiparesis Right-sided sensory loss Right-sided sensory loss Right Right visualvisual field defect field defect Poor right conjugate gaze Poor right conjugate gaze Dysarthria Dysarthria Difficulty reading, writing, or Difficulty reading, writing, or
calculatingcalculating
Right (Non-dominant) Hemisphere Right (Non-dominant) Hemisphere Stroke: Common PatternStroke: Common Pattern
Defect of Defect of leftleft visualvisual field field Extinction of left-sided stimuli Extinction of left-sided stimuli LeftLeft hemiparesishemiparesis Left-sided sensory loss Left-sided sensory loss Left visual field defect Left visual field defect Poor left conjugate gaze Poor left conjugate gaze DysarthriaDysarthria Spatial disorientation Spatial disorientation
Brain Stem Stroke: Common PatternBrain Stem Stroke: Common Pattern
Pure MotorPure Motor - - Weakness of Weakness of face and face and limbslimbs on one side of the body without on one side of the body without abnormalities of higher brain function, abnormalities of higher brain function, sensation, or vision (MCA/ACA)sensation, or vision (MCA/ACA)
Pure SensoryPure Sensory - Decreased sensation - Decreased sensation of of face and limbsface and limbs on one side of the on one side of the body without abnormalities of higher body without abnormalities of higher brain function, motor function, or brain function, motor function, or vision (PCA).vision (PCA).
Brain Stem / Cerebellum / Post Brain Stem / Cerebellum / Post Hemisp. Patterns.Hemisp. Patterns.
Motor or sensory loss in Motor or sensory loss in all four limbsall four limbs Crossed signs Crossed signs Limb or gait Limb or gait ataxiaataxia Dysarthria Dysarthria Dysconjugate gaze Dysconjugate gaze Nystagmus Nystagmus Amnesia Amnesia Bilateral visualBilateral visual field defects field defects
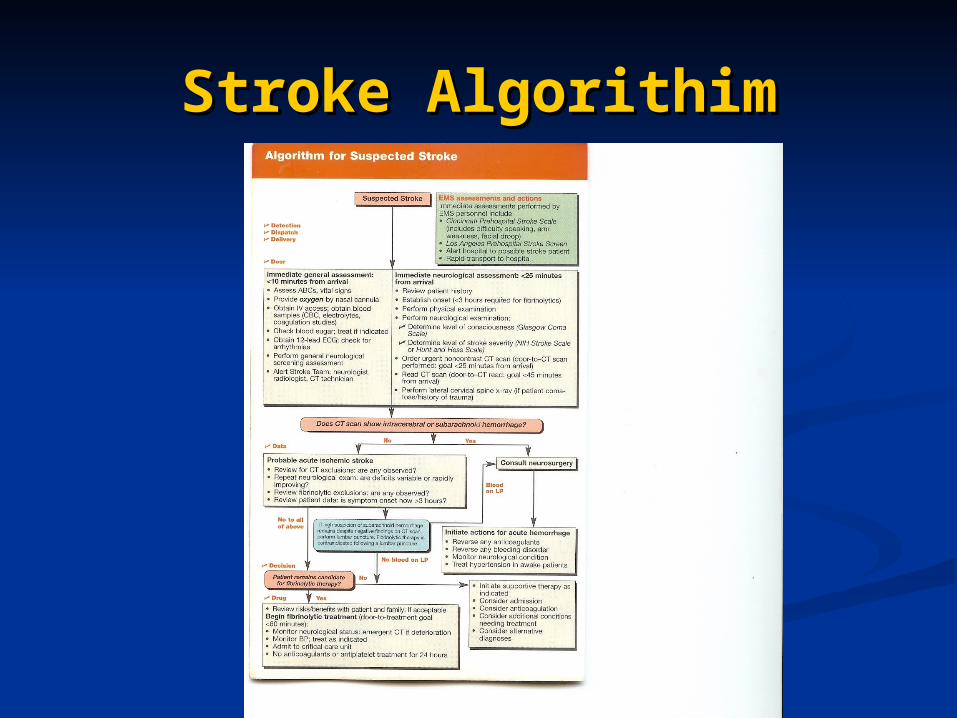
Stroke AlgorithimStroke Algorithim
Once a patient suffers from a stroke, Once a patient suffers from a stroke, the clock starts ticking.the clock starts ticking.
ACLS (Advanced Cardiac Life Support) ACLS (Advanced Cardiac Life Support) follows the Stroke Algorithim to assess follows the Stroke Algorithim to assess the patient’s condition and determine the patient’s condition and determine the appropriate method of treatment.the appropriate method of treatment.
The following slide shows the ACLS The following slide shows the ACLS algorithim.algorithim.
Stroke AlgorithimStroke Algorithim
Stroke AlgorithimStroke Algorithim
As you may have noticed, As you may have noticed, unfortunately there are times when unfortunately there are times when a patient may not be a candidate for a patient may not be a candidate for a Neuro Intervention.a Neuro Intervention.
A summary of the indications and A summary of the indications and contraindications for thrombolysis contraindications for thrombolysis are noted in the next several slides.are noted in the next several slides.
Indications for Neuro Indications for Neuro Intervention in StrokesIntervention in Strokes
Score of > 4 on NIHSS (Stroke Scale)Score of > 4 on NIHSS (Stroke Scale)
Time window of 6 hours or less of onset (3 Time window of 6 hours or less of onset (3 hours for IV therapy vs. 6 hours for IA therapy)hours for IV therapy vs. 6 hours for IA therapy)
Initial CT w/o Intracranial Hemorrhage and no Initial CT w/o Intracranial Hemorrhage and no large hypodensitieslarge hypodensities
Intracranial intraluminal clot present on Intracranial intraluminal clot present on angiogramangiogram
Absolute Contraindications Absolute Contraindications for Neuro Interventional for Neuro Interventional
Treatment of StrokeTreatment of Stroke
Acute Intracranial HemorrhageAcute Intracranial Hemorrhage
Large hypodense area or mass effect Large hypodense area or mass effect on CTon CT
Know serious sensitivity to contrast Know serious sensitivity to contrast agentsagents
Relative Contraindications Relative Contraindications (Relevant to Acute Stroke)(Relevant to Acute Stroke)
Improving neurological symptomsImproving neurological symptoms Suspected Lacunar infarctSuspected Lacunar infarct ComaComa Score of >30 on NIHSSScore of >30 on NIHSS History of Stroke within 6 weeksHistory of Stroke within 6 weeks Seizure at onset of strokeSeizure at onset of stroke Clinical presentation of SAH even if CT is normal Clinical presentation of SAH even if CT is normal
(Bloody Spinal Tap)(Bloody Spinal Tap) Previous know ICH or SAHPrevious know ICH or SAH Presumed Septic EmbolusPresumed Septic Embolus
Relative Contraindications Relative Contraindications (General Contraindications (General Contraindications
to Thrombolysis)to Thrombolysis) Baseline platelets less than 100,000/microliter, Baseline platelets less than 100,000/microliter,
Hematocrit less than 25 vol % or INR >1.7Hematocrit less than 25 vol % or INR >1.7 Uncontrollable HTN (>180/100 mmHg)Uncontrollable HTN (>180/100 mmHg) Presumed pericarditis post AMIPresumed pericarditis post AMI Recent Trauma (<30 days)Recent Trauma (<30 days) Recent Head Trauma (<90 days)Recent Head Trauma (<90 days) Any active or recent hemorrhage (<30 days)Any active or recent hemorrhage (<30 days) Known hereditary or acquired hemorrhagic Known hereditary or acquired hemorrhagic
diathesisdiathesis
Preprocedure Preprocedure PreparationPreparation
Correct Diagnosis (NIHSS & CT)Correct Diagnosis (NIHSS & CT)
Varify time of onset Varify time of onset
Neurological localization principles (In Neurological localization principles (In what area/region of the brain did the what area/region of the brain did the stroke occur?)stroke occur?)
Preprocedure EvaluationPreprocedure Evaluation
Complete H & PComplete H & P Neurological Exam (NIHSS, Barthel Neurological Exam (NIHSS, Barthel
Index or Rankin scaleIndex or Rankin scale Labs (CBC, BUN,Creatinine, PT/PTT, Labs (CBC, BUN,Creatinine, PT/PTT,
INR)INR) Chest RadiographChest Radiograph Uninfused (Noncontrast) CT Uninfused (Noncontrast) CT Patient Consent (Emergent or Family Patient Consent (Emergent or Family
Consent)Consent)
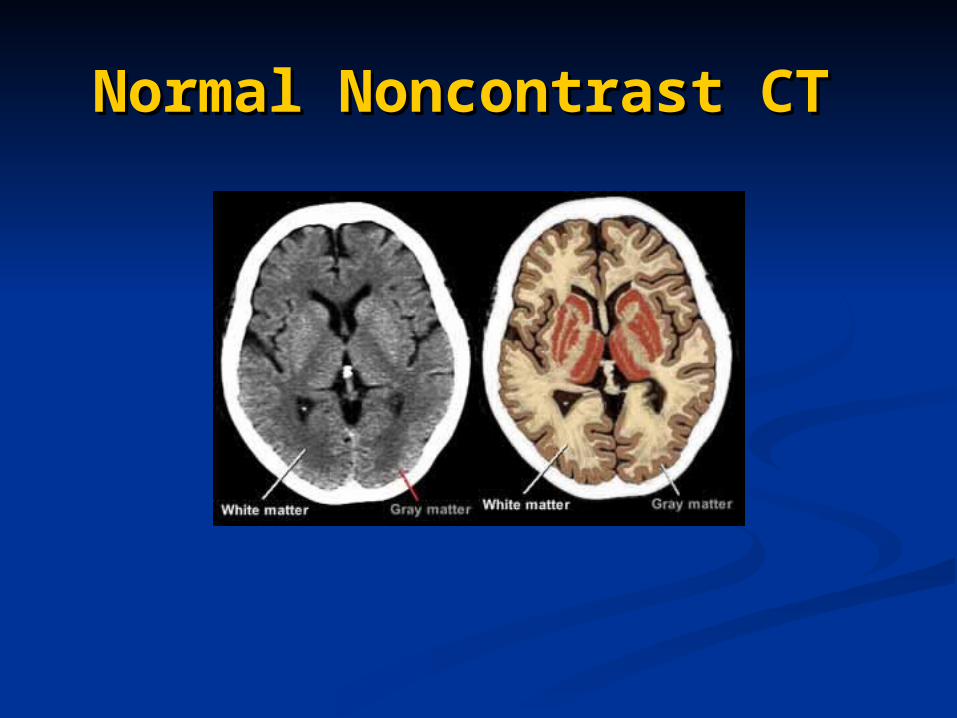
Normal Noncontrast CTNormal Noncontrast CT
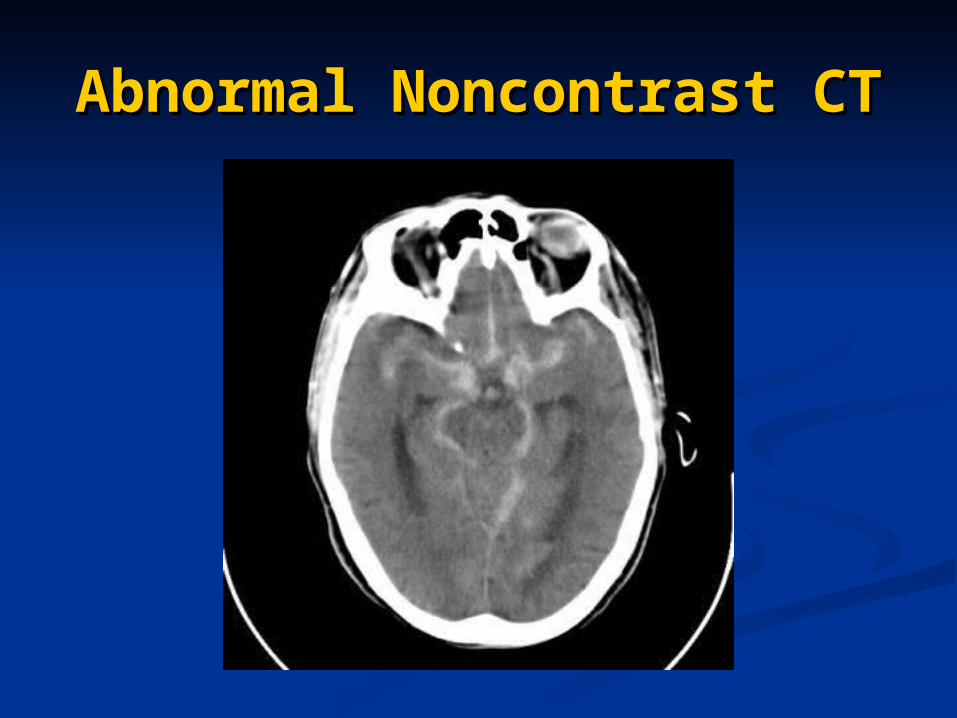
Abnormal Noncontrast Abnormal Noncontrast CTCT
Treatment of StrokeTreatment of Stroke
Ischemic stroke is treated by removing Ischemic stroke is treated by removing obstruction and restoring blood flow to the obstruction and restoring blood flow to the brain.brain.
In hemorrhagic stroke treatment is directed In hemorrhagic stroke treatment is directed towards prevention of rupture and bleeding of towards prevention of rupture and bleeding of aneurysms and arteriovenous malformations.aneurysms and arteriovenous malformations.
Treatment Treatment (continued)(continued) Ischemic StrokeIschemic Stroke
– Acute TreatmentAcute Treatment• Clot-busters, e.g., tPA Clot-busters, e.g., tPA • must be administered within a three-hour window must be administered within a three-hour window
from onset of symptoms for most effective usefrom onset of symptoms for most effective use• only 3 to 5 percent of those reach the hospital in only 3 to 5 percent of those reach the hospital in
time to be considered for this treatmenttime to be considered for this treatment
– Preventative TreatmentPreventative Treatment• Anticoagulants/AntiplateletsAnticoagulants/Antiplatelets• Carotid EndarterectomyCarotid Endarterectomy• Angioplasty/StentsAngioplasty/Stents
Treatment Treatment (continued)(continued)
Hemorrhagic StrokeHemorrhagic Stroke– Surgical InterventionSurgical Intervention
• Surgical treatment is often recommended to either Surgical treatment is often recommended to either place a metal clip at the base, called the neck, of place a metal clip at the base, called the neck, of the aneurysm or to remove the abnormal vessels the aneurysm or to remove the abnormal vessels comprising an Arteriovenous Malformation comprising an Arteriovenous Malformation (AVM). (AVM).
– Endovascular Procedures, e.g., "coils"Endovascular Procedures, e.g., "coils"• less invasive and involves the use of a catheter less invasive and involves the use of a catheter
introduced through a major artery in the leg or armintroduced through a major artery in the leg or arm• catheter is guided to the aneurysm or AVM where catheter is guided to the aneurysm or AVM where
it deposits a mechanical agent, such as a coil, to it deposits a mechanical agent, such as a coil, to prevent ruptureprevent rupture
When Patient Arrives in When Patient Arrives in Neuro Suite, the Staff will Neuro Suite, the Staff will
begin to….begin to…. Monitor (EKG, Pulse Ox, BP Cuff)Monitor (EKG, Pulse Ox, BP Cuff) Perform Neurologic exam (pre and post)Perform Neurologic exam (pre and post) Have ACT (Activated Clotting Time) Have ACT (Activated Clotting Time)
machine readymachine ready Start IV Access (if applicable)Start IV Access (if applicable) Prep PatientPrep Patient Notify the Physician, who will in turn:Notify the Physician, who will in turn:
Administer local anesthesiaAdminister local anesthesia Select Common Carotid ArterySelect Common Carotid Artery Perform DSA(Digital Subtraction Angiography)- Perform DSA(Digital Subtraction Angiography)-
(Diagnostic run)(Diagnostic run)
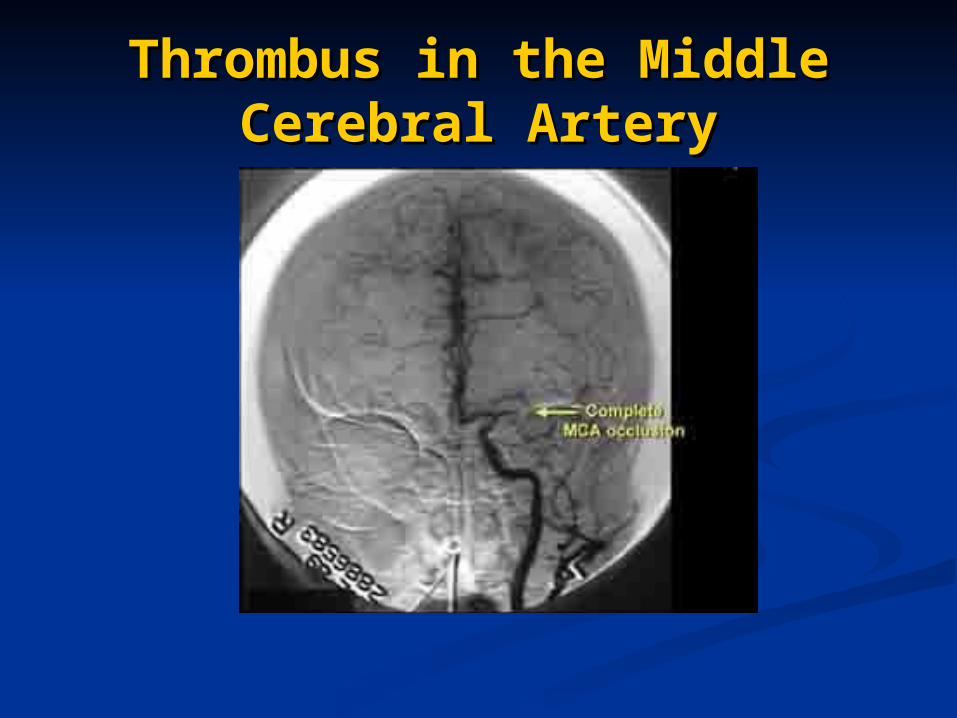
Thrombus in the Middle Thrombus in the Middle Cerebral ArteryCerebral Artery
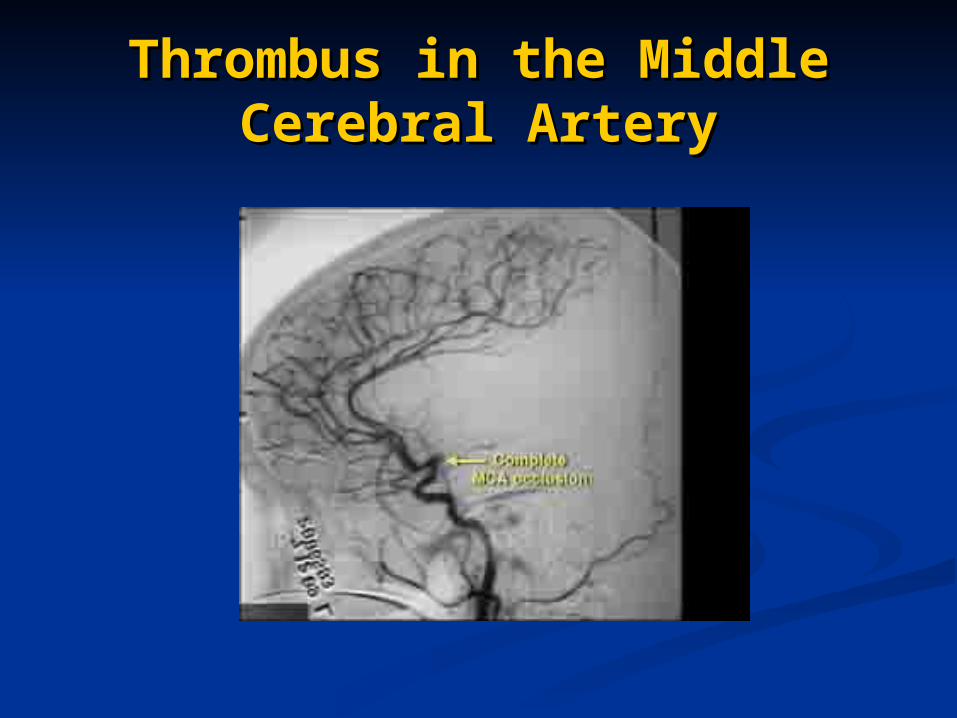
Thrombus in the Middle Thrombus in the Middle Cerebral ArteryCerebral Artery
Procedure Set-UpProcedure Set-Up
As you will note, the beginning set-As you will note, the beginning set-up is the same for all interventional up is the same for all interventional cases.cases.
The following slides will review the The following slides will review the following:following: Pressure Bag Set-upPressure Bag Set-up Sheath or Guide Catheter positioningSheath or Guide Catheter positioning
Pressure Line Set-UpsPressure Line Set-Ups
Don’t Forget To Label Both Don’t Forget To Label Both Ends!Ends!
Tuohy-Borst AdapterTuohy-Borst Adapter
Three-Way StopcockThree-Way Stopcock
Before Screwing to Sheath Before Screwing to Sheath or Guide Catheter…or Guide Catheter…
Carefully FlushCarefully Flush Check for bubblesCheck for bubbles Hook to Pressure Bag LineHook to Pressure Bag Line Check and Re-Check for BubblesCheck and Re-Check for Bubbles

The Flow of things…the The Flow of things…the Pressure BagPressure Bag
Most times the pressure bags are Most times the pressure bags are even done ahead of time due to the even done ahead of time due to the non-invasive studies already done non-invasive studies already done prior to angiography.prior to angiography.
The Flow of things…The Flow of things…Placement of the Catheter, Placement of the Catheter,
Shuttle Sheath or Guide Shuttle Sheath or Guide CatheterCatheter Depending on the Physician and the situation, the Depending on the Physician and the situation, the
Physician may either leave the diagnostic catheter Physician may either leave the diagnostic catheter in place or exchange for either the Shuttle Sheath in place or exchange for either the Shuttle Sheath or Guide Cath.or Guide Cath.
If the diagnostic catheter is left in a If the diagnostic catheter is left in a microcathetermicrocatheter is selected and placed inside the diagnostic is selected and placed inside the diagnostic catheter.catheter.
If either a Guiding Catheter or Shuttle Sheath is If either a Guiding Catheter or Shuttle Sheath is chosen, they are placed in the Common Carotid chosen, they are placed in the Common Carotid and the diagnostic/microcatheter combo is and the diagnostic/microcatheter combo is rinserted after being properly flushed with saline.rinserted after being properly flushed with saline.
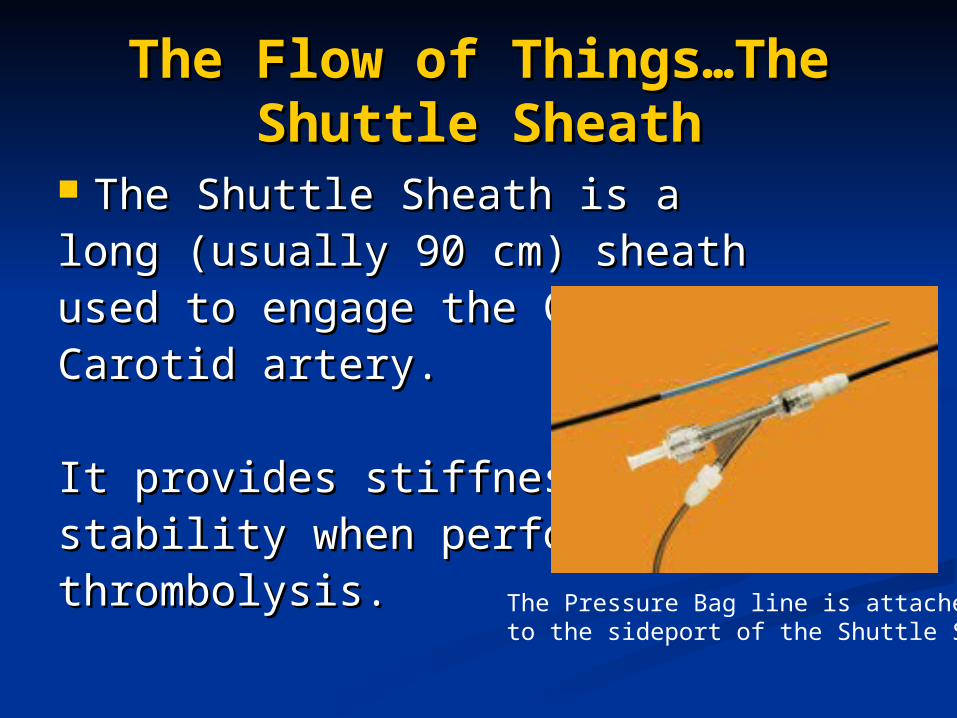
The Flow of Things…The The Flow of Things…The Shuttle SheathShuttle Sheath
The Shuttle Sheath is a The Shuttle Sheath is a long (usually 90 cm) sheath long (usually 90 cm) sheath used to engage the Commonused to engage the CommonCarotid artery.Carotid artery.
It provides stiffness andIt provides stiffness andstability when performing stability when performing thrombolysis.thrombolysis. The Pressure Bag line is attached
to the sideport of the Shuttle Sheath
MicroCathetersMicroCatheters This is one of several types of This is one of several types of
microcatheters (there are also microcatheters (there are also microwires used with the microwires used with the microcatheters).microcatheters).
They are positioned proximal to the They are positioned proximal to the thrombus where the thrombolytics thrombus where the thrombolytics are infused.are infused.
Roadmapping and Steering Roadmapping and Steering of Coaxial Systemof Coaxial System
Use of Bi-plane fluoroscopyUse of Bi-plane fluoroscopy Use of Roadmapping feature may be Use of Roadmapping feature may be
helpfulhelpful Advance system carefully Advance system carefully
(Intracranial arteries are thinner than (Intracranial arteries are thinner than peripheral arteries- less media and peripheral arteries- less media and adventitia)adventitia)
Hand injections should be done Hand injections should be done carefully so as not to rupture any carefully so as not to rupture any perforators.perforators.
The Flow of Things…The The Flow of Things…The Infusion of the Infusion of the ThrombolyticsThrombolytics
Once the area of occlusion is identified and the Once the area of occlusion is identified and the microcatheter is in place, infusion of the microcatheter is in place, infusion of the thrombolytics is started.thrombolytics is started.
Infusion may be accomplished by hand injections Infusion may be accomplished by hand injections or pump infusion.or pump infusion.
Follow-up DSA runs are periodically acquired to Follow-up DSA runs are periodically acquired to check the progression of the clot lysis.check the progression of the clot lysis.
It is a good idea to start a timer, usually found It is a good idea to start a timer, usually found within the equipment , to record the total time of within the equipment , to record the total time of infusion.infusion.
The Flow of Things…The The Flow of Things…The Infusion of the Infusion of the ThrombolyticsThrombolytics
The infusion will probably last for several The infusion will probably last for several hours, so one to consider, does the patient hours, so one to consider, does the patient have or require a Foley catheter?have or require a Foley catheter?
Another note about the drugs/lytics. When Another note about the drugs/lytics. When mixing the drug, some have a tendency to mixing the drug, some have a tendency to foam if mixed in a hurried or rapid fashion. foam if mixed in a hurried or rapid fashion.
The best thing to do is when mixing the The best thing to do is when mixing the drugs, don’t shake it, rather slowly roll the drugs, don’t shake it, rather slowly roll the vial between your hands until all particles vial between your hands until all particles have or are dissolved.have or are dissolved.
Technique of Technique of Intracranial Intracranial
ThrombolysisThrombolysis Regional Infusions- Through Regional Infusions- Through
Diagnostic CatheterDiagnostic Catheter
Locally- Through Coaxial Locally- Through Coaxial Microcatheter systemMicrocatheter system
Regional InfusionRegional Infusion
Infusion is through diagnostic catheter in Infusion is through diagnostic catheter in either the internal carotid artery or the either the internal carotid artery or the vertebral arteryvertebral artery
Technically less involvedTechnically less involved Delivery of thrombolytic agent less Delivery of thrombolytic agent less
reliable and go to surrounding perfusing reliable and go to surrounding perfusing arteries.arteries.
Recanalization less effective, less Recanalization less effective, less desirable clinical resultsdesirable clinical results
Local InfusionLocal Infusion
Infusion is throught a microcatheter Infusion is throught a microcatheter which is embedded in or near the which is embedded in or near the clot.clot.
More technically involved, More technically involved, superselective positioning of superselective positioning of microcatheter.microcatheter.
Delivery is more controlledDelivery is more controlled Recanalization more effective, better Recanalization more effective, better
clinical resultsclinical results
Fibrinolytics “Clot-Fibrinolytics “Clot-Busters”Busters”
Here are a few thrombolytics that have Here are a few thrombolytics that have been or are currently being utilized.been or are currently being utilized.
Urokinase (UK)Urokinase (UK)
Rt-PARt-PA
RetavaseRetavase
Pro-UKPro-UK
Clinical Trials for New Clinical Trials for New AgentsAgents
ASP (Ancrod Stroke Protocol) II ASP (Ancrod Stroke Protocol) II Program is another thrombolytic Program is another thrombolytic currently under trial for possible use currently under trial for possible use in the treatment of strokein the treatment of stroke
ViprinexViprinex
Administration of LyticsAdministration of Lytics
InfusionInfusion LacingLacing Pulse-sprayPulse-spray Probing with wireProbing with wire
Follow-Up ArteriographyFollow-Up Arteriography
Check progress every 15 to 30 minutesCheck progress every 15 to 30 minutes
Time the infusion (Total time of infusion)Time the infusion (Total time of infusion)
When to stop infusion:When to stop infusion:
Thrombus no longer visible or occlusive Thrombus no longer visible or occlusive (Residual clot could be (Residual clot could be heparinized)heparinized)
Intracranial HemorrhageIntracranial Hemorrhage
Results Of ThrombolysisResults Of Thrombolysis
Recanalization occurs within 50%- Recanalization occurs within 50%- 80% of cases80% of cases
Acute vertebrobasilar occlusions Acute vertebrobasilar occlusions have poor outcomes especially with have poor outcomes especially with increased ageincreased age
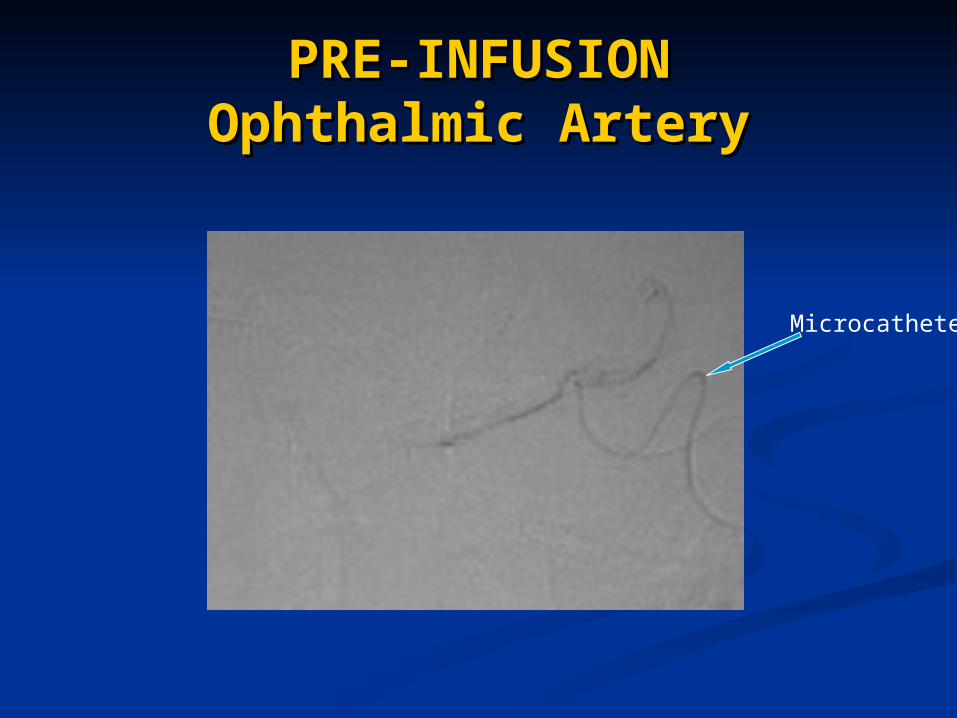
PRE-INFUSIONPRE-INFUSIONOphthalmic ArteryOphthalmic Artery
Microcatheter
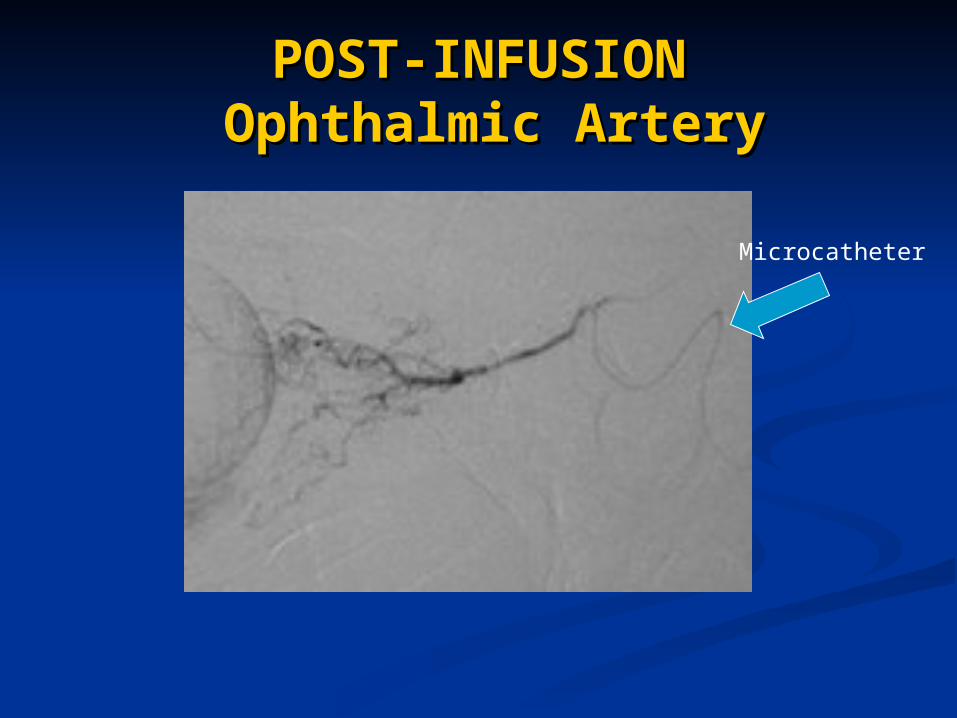
POST-INFUSIONPOST-INFUSION Ophthalmic Artery Ophthalmic Artery
Microcatheter
Complications Associated Complications Associated with Thrombolytic Infusionwith Thrombolytic Infusion
Intracerebral HemorrhageIntracerebral Hemorrhage
HTN complicates post-infusion (keep HTN complicates post-infusion (keep below 150/80 mmHgbelow 150/80 mmHg
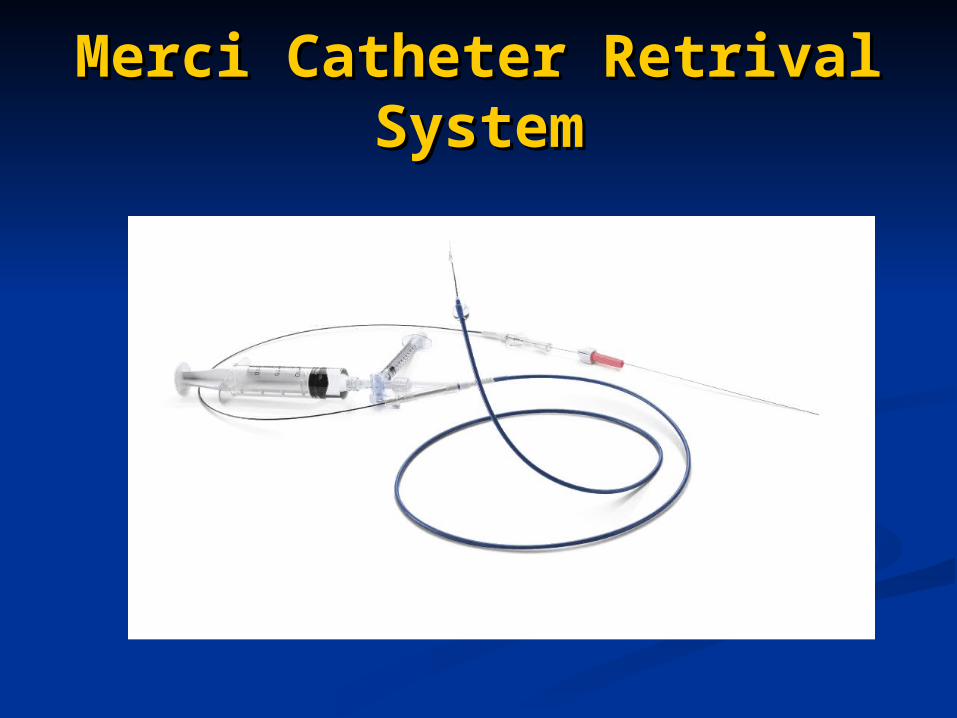
Merci Catheter Retrival Merci Catheter Retrival SystemSystem
Merci Catheter Retrival Merci Catheter Retrival SystemSystem
• The Merci Catheter system is a fairly new device used in the treatment of Stroke.
View Concentric-Medical’s website at the following link:http://www.concentric-medical.com/resources.html and see how the Merci Catheter works.
•The next several slides demonstrate how the device is used and the results it can give.
Pre Merci Catheter (AP Pre Merci Catheter (AP view)view)
Pre Merci Catheter Pre Merci Catheter (Lateral view)(Lateral view)
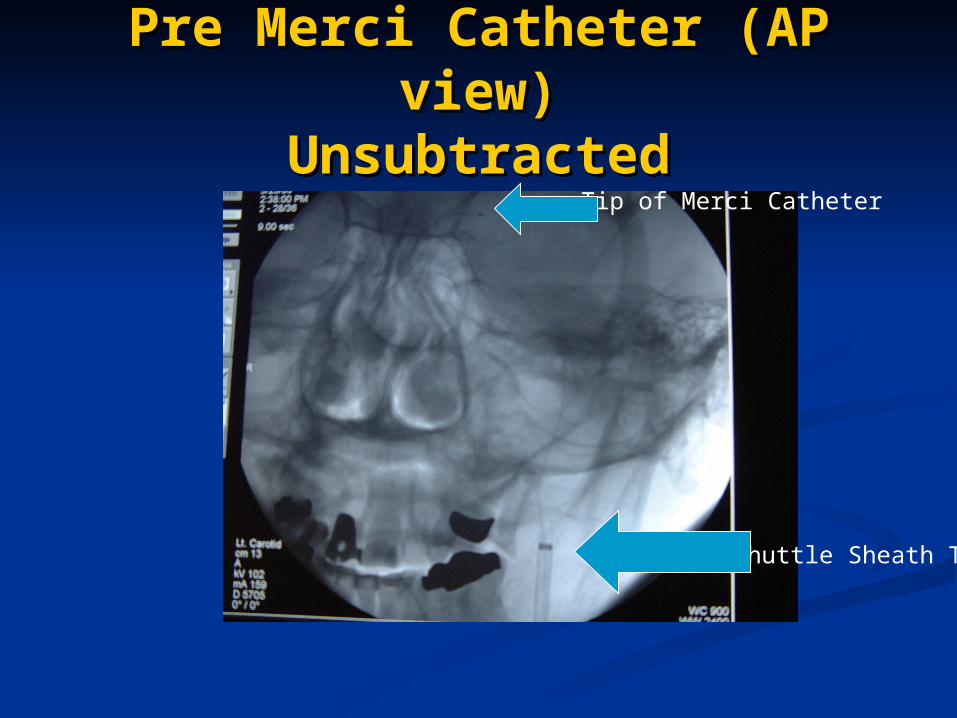
Pre Merci Catheter (AP Pre Merci Catheter (AP view)view)
UnsubtractedUnsubtracted
Shuttle Sheath Tip
Tip of Merci Catheter
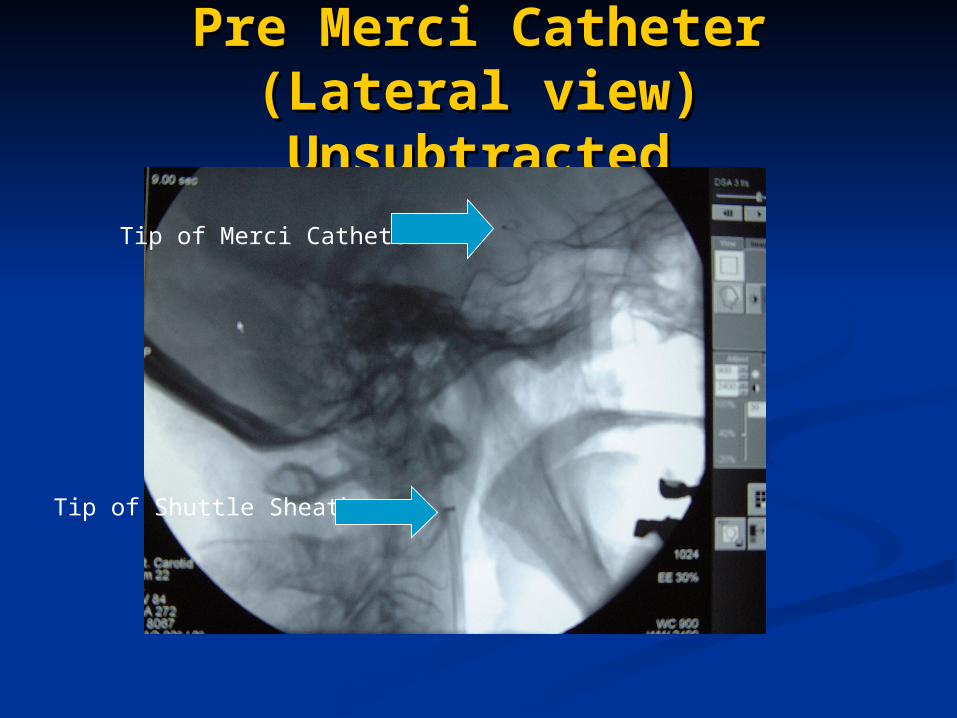
Pre Merci Catheter (Lateral Pre Merci Catheter (Lateral view)view)
UnsubtractedUnsubtractedTip of Merci Catheter
Tip of Shuttle Sheath
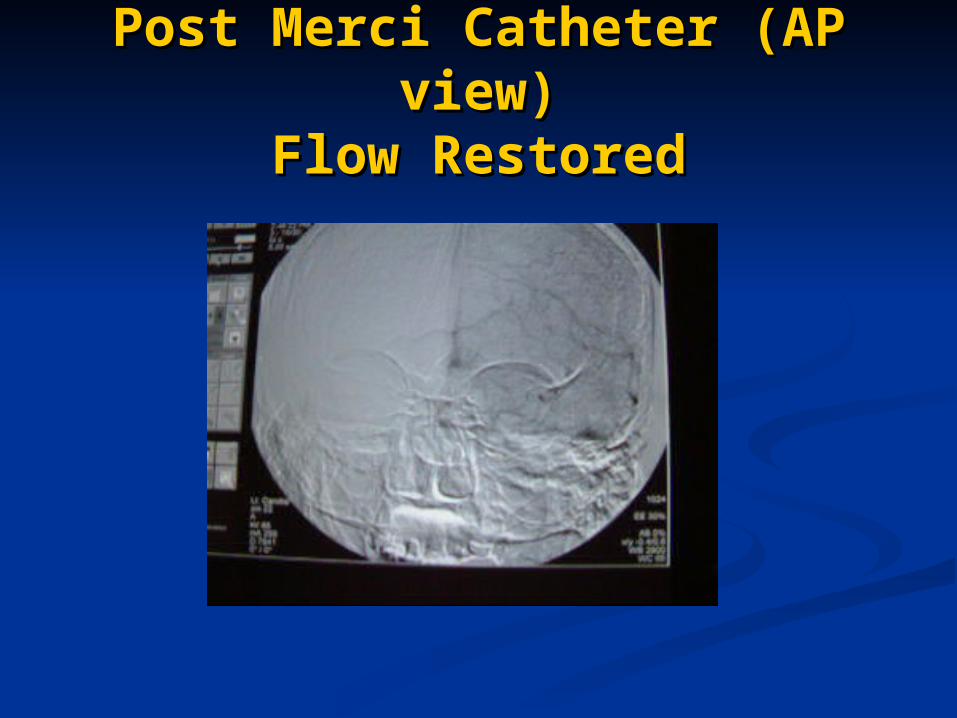
Post Merci Catheter (AP Post Merci Catheter (AP view)view)
Flow RestoredFlow Restored
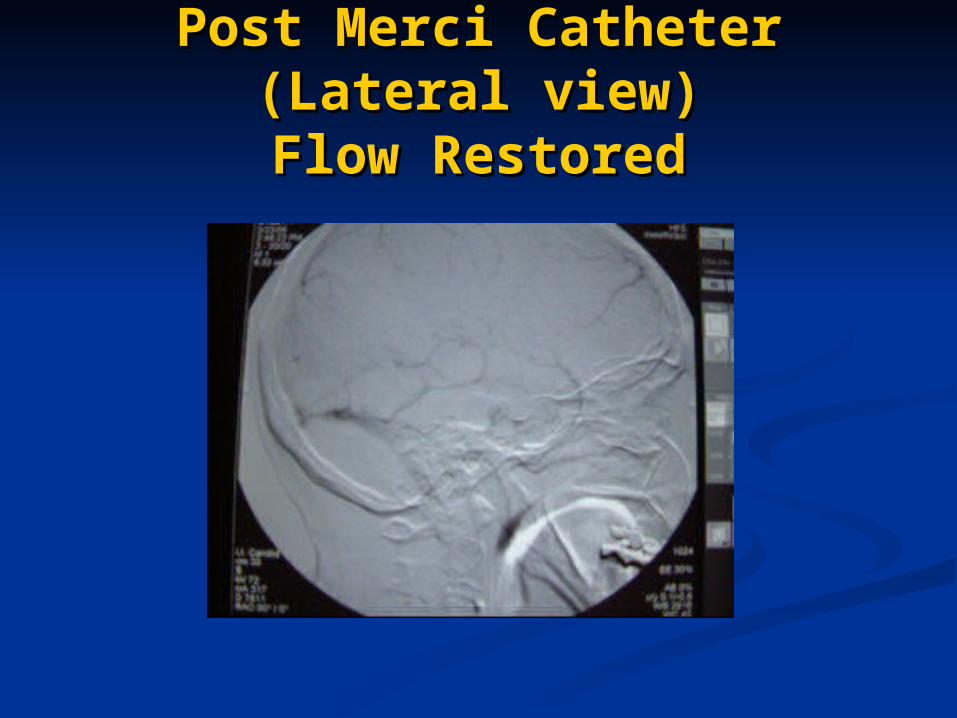
Post Merci Catheter Post Merci Catheter (Lateral view)(Lateral view)Flow RestoredFlow Restored
SummarySummary
Now that we have reviewed Arterial Now that we have reviewed Arterial thrombolysis, let’s turn our attention thrombolysis, let’s turn our attention toward Venous thrombolysis.toward Venous thrombolysis.
Neuroradiology: Venous Neuroradiology: Venous ThrombolysisThrombolysis
Venous OcclusionsVenous Occlusions
Typically is an underdiagnosed Typically is an underdiagnosed cause of neurologic deteroration.cause of neurologic deteroration.
Clinical signs are sometimes non-Clinical signs are sometimes non-specificspecific
Imaging is critical in the detection of Imaging is critical in the detection of venous thrombosis.venous thrombosis.
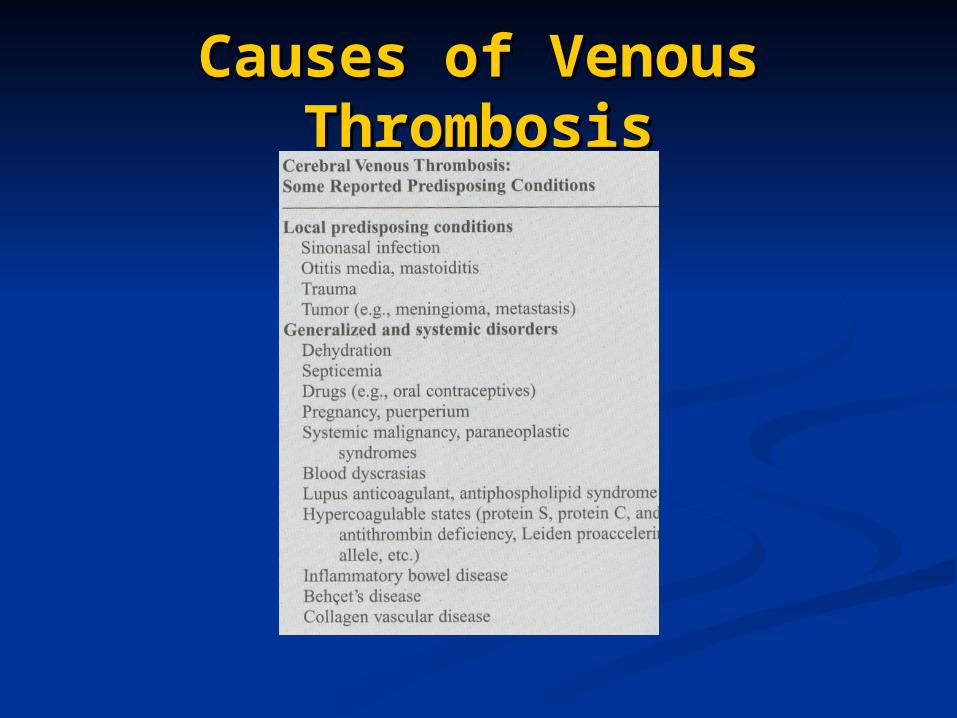
Causes of Venous Causes of Venous ThrombosisThrombosis
Signs and Symptoms of Signs and Symptoms of Venous ThrombosisVenous Thrombosis
Some of the potential signs and symptoms Some of the potential signs and symptoms include:include:
HeadacheHeadache Increased Intracranial PressureIncreased Intracranial Pressure Vomiting Vomiting LethargyLethargy Mild ParesisMild Paresis Visual DisturbancesVisual Disturbances SeizureSeizure ComaComa
Imaging for Venous Imaging for Venous ThrombosisThrombosis
Non-Invasive imaging (CT, MR or Non-Invasive imaging (CT, MR or Ultrasound) may be utilized.Ultrasound) may be utilized.
When performing Cerebral When performing Cerebral Angiography to rule thrombosis, Angiography to rule thrombosis, always make sure you image all of always make sure you image all of the venous flow as well as the the venous flow as well as the arterial flow.arterial flow.
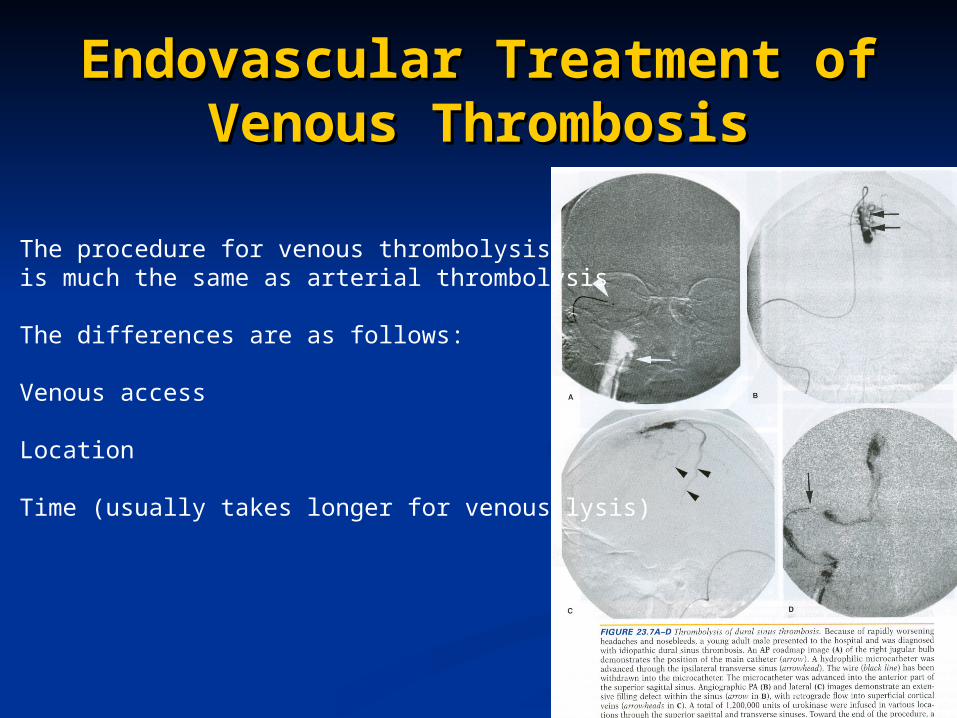
Endovascular Treatment of Endovascular Treatment of Venous ThrombosisVenous Thrombosis
The procedure for venous thrombolysisis much the same as arterial thrombolysis
The differences are as follows:
Venous access
Location
Time (usually takes longer for venous lysis)
Homework AssignmentsHomework Assignments
Read Chapter 23 (pp. 443-455)Read Chapter 23 (pp. 443-455)
ReferencesReferences
Morris, P.P. Morris, P.P. Practical NeuroradiographyPractical Neuroradiography, 2nd , 2nd Edition, 2007Edition, 2007
Osborn, A.G. Osborn, A.G. Handbook of NeuroradiologyHandbook of Neuroradiology, 2, 2ndnd Edition, 1999Edition, 1999
Bontrager, K.L. Bontrager, K.L. TEXTBOOK of Radiographic TEXTBOOK of Radiographic Positioning and Related AnatomyPositioning and Related Anatomy , 5 , 5thth Edition, Edition, 20012001
Snopek, A.M Snopek, A.M Fundamentals of Special Fundamentals of Special Radiographic ProceduresRadiographic Procedures, 5, 5thth Edition, 2006 Edition, 2006
Tortorici, M.R. Tortorici, M.R. Fundamentals of AngiographyFundamentals of Angiography, , 19821982
Various other Internet sourcesVarious other Internet sources