welcome! please take a moment to complete the short in your packet. your participation will help us...
TRANSCRIPT

Welcome!Welcome!Please take a moment to complete the short Please take a moment to complete the short
pre-program survey in your packet. Your in your packet. Your participation will help us assess the effectiveness participation will help us assess the effectiveness of this program and shape future CME activities.of this program and shape future CME activities.


Faculty DisclosuresFaculty DisclosuresThe faculty reported the following relevant financial relationships that they or their spouse/partner have with commercial interests:•Presenter, MD: Research: Pharma Company; Consultant: Pharma Company
TO BE FILLED IN BY PRESENTING PHYSICIAN(S)
Off-label discussion disclosure:
This educational activity may contain discussion of published and/or investigational uses of agents that are not indicated by the Food and Drug Administration. PCME does not recommend the use of any agent outside of the labeled indications. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications and warnings. The opinions expressed are those of the presenters and are not to be construed as those of the publisher or grantors.
Steering Committee DisclosuresSteering Committee Disclosures
The Steering Committee reported the following relevant financial relationships that they or their spouse/partner have with commercial interests:
•Deborah K. Armstrong, MD: Advisory Board: Genentech; Clinical Trials: Genentech, Medimmune, Morphotek; Clinical Development Advisory Panel (CDAp): California Institute for Regenerative Medicine (CIRM); Data Safety Monitoring Board: Merrimack, Quintiles; Drugs Advisory Committee: Oncology Drugs Advisory Committee (ODAC) to the US FDA; Independent Safety Officer: Astellas; Member: Integration Panel (IP) for Department of Defense (DOD) Ovarian Cancer Research Program (OCRP); Dr. Armstrong’s spouse’s institution also receives funding from: Eisai, Exelixis•Bradley J. Monk, MD, FACOG, FACS: Consultant: Array, Astellas, Boehringer Ingelheim, GlaxoSmithKline, Morphotek, Nektar, Roche/Genentech; Researcher: Amgen, Genentech, Merck, Novartis; Speaker: Johnson & Johnson, Roche/Genentech

Non-faculty DisclosuresNon-faculty Disclosures
Non-faculty content contributors and/or reviewers reported the following relevant financial relationships that they or their spouse/partner have with commercial interests:
Latha Shivakumar, PhD; Bradley Pine; Blair St. Amand; Jay Katz, CCMEP; CME Peer Review: Nothing to Disclose

Educational ObjectivesEducational Objectives
At the conclusion of this activity, participants should be able to demonstrate the ability to:
•Review the recently updated clinical practice guidelines for advanced ovarian cancer•Compare the available treatment regimens and platinum-sensitive or platinum-resistant recurrent settings and choose the optimal treatment based on patient characteristics and recently presented clinical trial data•Identify key investigational regimens in currently ongoing clinical studies for advanced ovarian cancer and counsel patients accordingly

Basis for Basic Current Standard Systemic TherapyBasis for Basic Current Standard Systemic Therapy
• Studies showing paclitaxel/cisplatin superior to cyclophosphamide/cisplatin – GOG Protocol 111[1]
– EORTC-NCIC OV 10[2]
• Studies showing paclitaxel/carboplatin at least equivalent to paclitaxel/cisplatin in efficacy– AGO Trial[3]
– GOG Protocol 158[4]
1. McGuire WP et al. N Eng J Med .1996;334:1-6. 2. Piccart MJ et al. J Natl Cancer Inst. 2000;92:699-708.3. DuBois A et al. J Natl Cancer Inst. 2003;95:1320-1329. 4. Ozols RF et al. J Clin Oncol. 2003;21:3194-3200.
First-line Therapy: Acceptable ApproachesFirst-line Therapy: Acceptable Approaches
• Neoadjuvant chemotherapy• Intraperitoneal chemotherapy• Weekly dosing• Adding a targeted agent (e.g. bevacizumab)• Maintenance or consolidation chemotherapy after complete
remission

First-line Therapy: Acceptable ApproachesFirst-line Therapy: Acceptable Approaches
• Neoadjuvant chemotherapy• Intraperitoneal chemotherapy• Weekly dosing• Adding a targeted agent (e.g. bevacizumab)• Maintenance or consolidation chemotherapy after complete
remission

RandomizationRandomization
Randomised EORTC-GCG/NCIC-CTG trial on NACT + IDS versus PDSRandomised EORTC-GCG/NCIC-CTG trial on NACT + IDS versus PDS
Ovarian, tubal or peritonal cancerFIGO stage IIIc-IV (n = 718)
Ovarian, tubal or peritonal cancerFIGO stage IIIc-IV (n = 718)
3 x Platinum based CT3 x Platinum based CT 3 x Platinum based CT3 x Platinum based CT
≥ 3 x Platinum based CT≥ 3 x Platinum based CT
Primary Debulking SurgeryPrimary Debulking Surgery Neoadjuvant chemotherapyNeoadjuvant chemotherapy
Interval debulking (not obligatory)
Interval debulking (not obligatory)
Interval debulking if no PDInterval debulking if no PD
≥ 3 x Platinum based CT≥ 3 x Platinum based CT
Primary Endpoint: Overall survival Secondary endpoints: Progression Free Survival, Quality of Life, Complications
IGCS Meeting October 25, 2009; N Engl J Med. 2010;363:943-953.
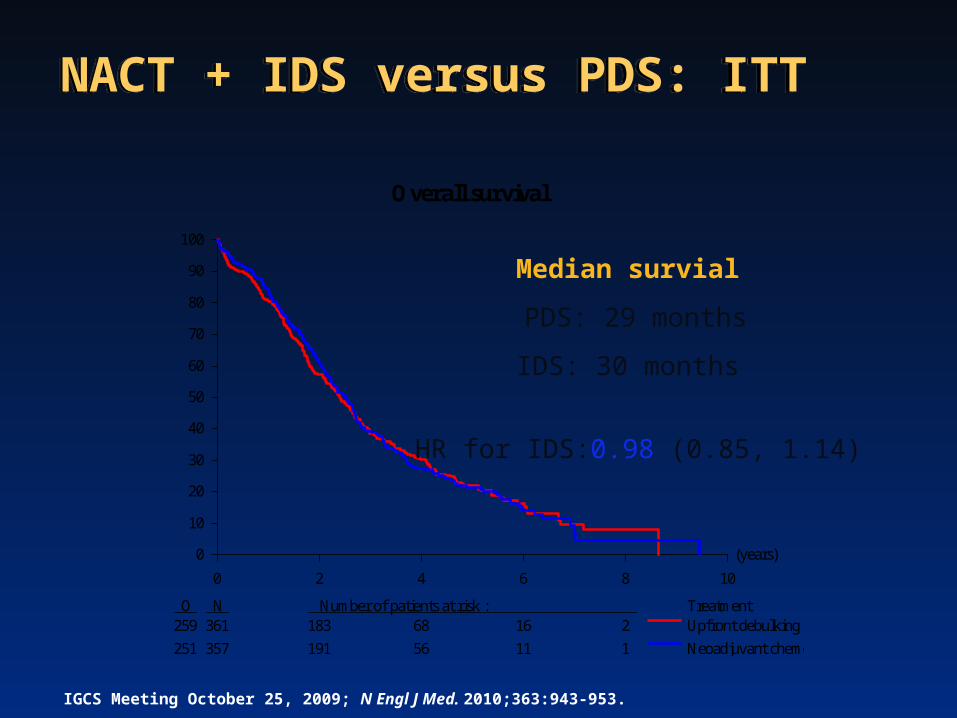
NACT + IDS versus PDS: ITT
NACT + IDS versus PDS: ITT
(years)
0 2 4 6 8 10
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment259 361 183 68 16 2
251 357 191 56 11 1
Upfront debulking surgery
Neoadjuvant chemotherapy
Overall survival
Median survial
PDS: 29 months
IDS: 30 months
HR for IDS:0.98 (0.85, 1.14)
IGCS Meeting October 25, 2009; N Engl J Med. 2010;363:943-953.

First-line Therapy: Acceptable ApproachesFirst-line Therapy: Acceptable Approaches
• Neoadjuvant chemotherapy• Intraperitoneal chemotherapy• Weekly dosing• Adding a targeted agent (e.g. bevacizumab)• Maintenance or consolidation chemotherapy after complete
remission
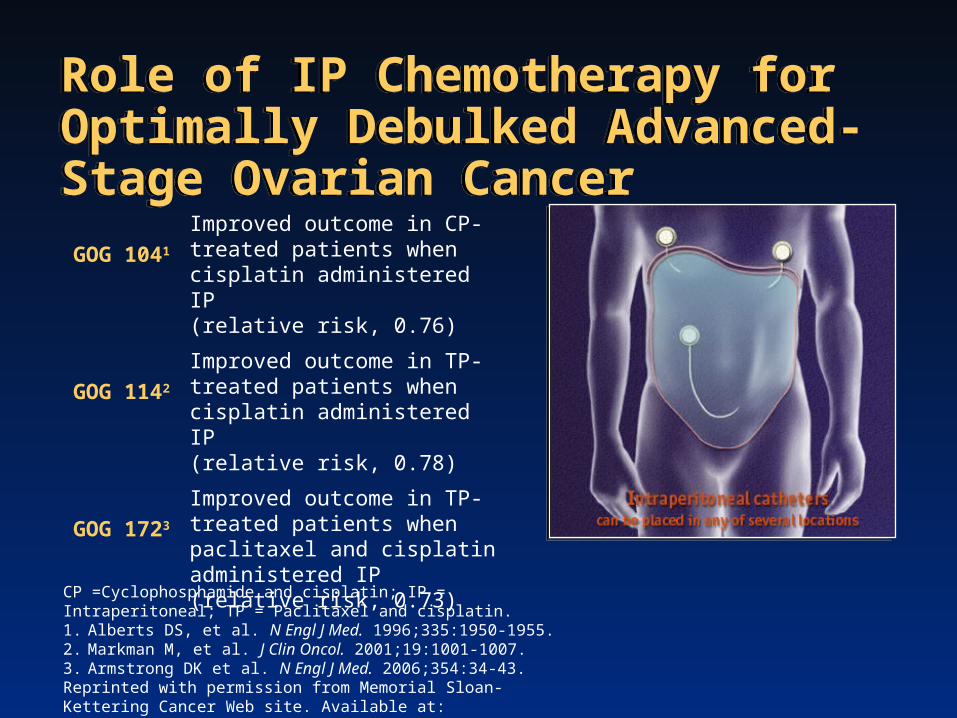
Role of IP Chemotherapy for Optimally Debulked Advanced-Stage Ovarian CancerRole of IP Chemotherapy for Optimally Debulked Advanced-Stage Ovarian Cancer
GOG 1041
Improved outcome in CP-treated patients when cisplatin administered IP (relative risk, 0.76)
GOG 1142
Improved outcome in TP-treated patients when cisplatin administered IP (relative risk, 0.78)
GOG 1723
Improved outcome in TP-treated patients when paclitaxel and cisplatin administered IP(relative risk, 0.73)
CP =Cyclophosphamide and cisplatin; IP = Intraperitoneal; TP = Paclitaxel and cisplatin.1. Alberts DS, et al. N Engl J Med. 1996;335:1950-1955. 2. Markman M, et al. J Clin Oncol. 2001;19:1001-1007. 3. Armstrong DK et al. N Engl J Med. 2006;354:34-43.Reprinted with permission from Memorial Sloan-Kettering Cancer Web site. Available at: www.mskcc.org/patient_education/html/ 41495.cfm. Accessed March 9, 2006.

GOG Protocol 172GOG Protocol 172
IV = Intravenous; IP = IntraperitonealArmstrong DK,et al. N Engl J Med. 2006;354:34-43.
By Treatment GroupP
ropo
rtion
Sur
vivi
ng
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Months on Study0 12 24 36 48 60
Rx Group Alive Dead Total IV 93 117 210
Alive Dead Total
IP 117 88 205
IV median overall survival = 49.7 months
IP median overall survival = 65.6 months
Relative risk of death = 0.75 (95% CI: 0.58, 0.97) P = .03
Rx Group Lost to Alive Dead TotalFollow-up
IV 5 78 127 210IP 11 93 101 205
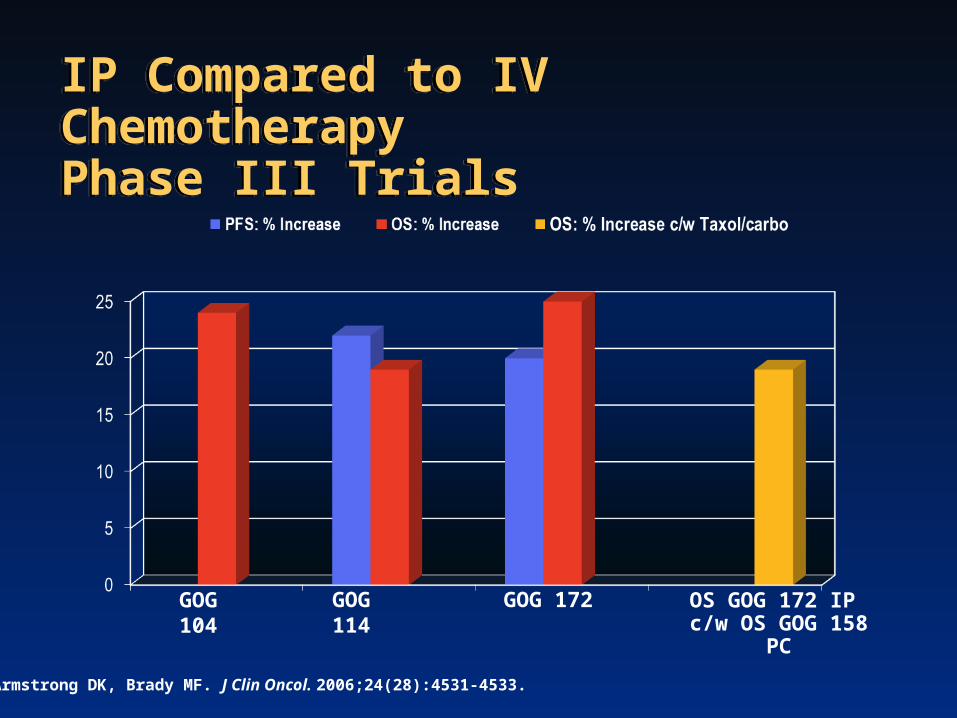
IP Compared to IV Chemotherapy Phase III TrialsIP Compared to IV Chemotherapy Phase III Trials
GOG 104 GOG 114 GOG 172 OS GOG 172 IP c/w OS GOG 158 PC
Armstrong DK, Brady MF. J Clin Oncol. 2006;24(28):4531-4533.
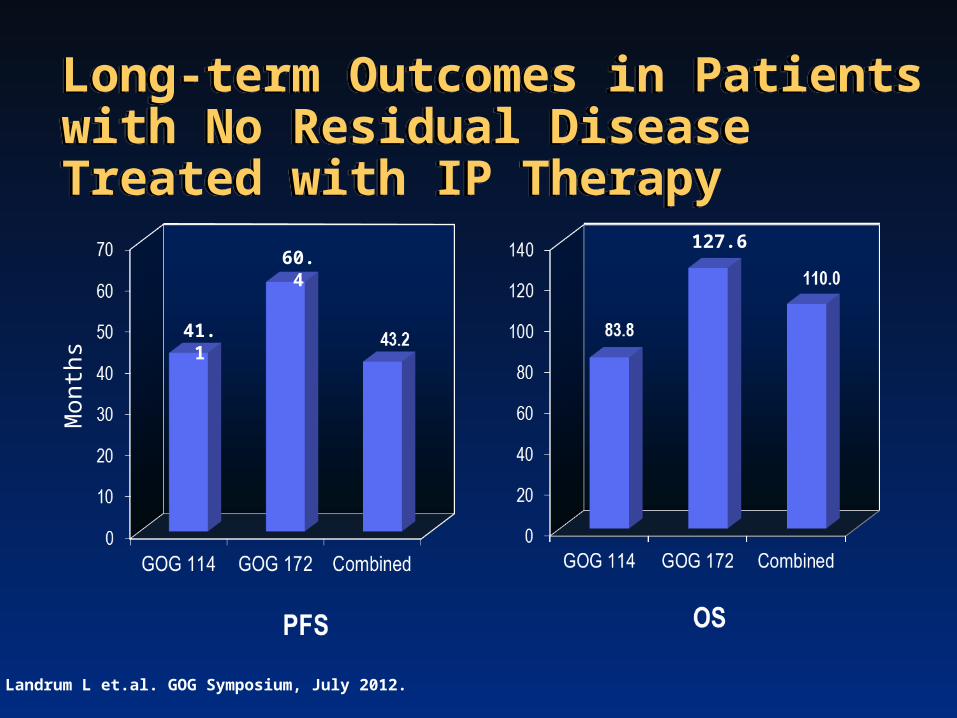
Long-term Outcomes in Patients with No Residual Disease Treated with IP TherapyLong-term Outcomes in Patients with No Residual Disease Treated with IP Therapy
Mon
ths
60.4
41.1
127.6
Landrum L et.al. GOG Symposium, July 2012.

GOG 252 Stage II/III Disease: Small Volume ResidualGOG 252 Stage II/III Disease: Small Volume Residual
Cisplatin 75 mg/m2 (IP d2)Paclitaxel 135 mg/m2 (d1, 3h)Paclitaxel 60 mg/m2 (d8, IP)Bevacizumab (C2+ C22) x 21 days
• Epithelial Ovarian Cancer• Optimal Stage III• No prior therapy
• Phase III• PFS primary endpoint
Open: 27 Jul 2009Closed: 30 Nov 2011Accrual: 1100Study Chair: J Walker
III
IICarboplatin AUC=6 (IP)Paclitaxel 80 mg/m2 (d1, 8, 15 3h)Bevacizumab (C2+ C22) x 21 days
ClinicalTrials.gov Identifier: NCT00951496
ICarboplatin AUC=6 (IV)Paclitaxel 80 mg/m2 (d1, 8, 15 3h)Bevacizumab (C2+ C22) x 21 days
First-line Therapy: Acceptable ApproachesFirst-line Therapy: Acceptable Approaches
• Docetaxel instead of paclitaxel• Neoadjuvant chemotherapy• Intraperitoneal chemotherapy• Weekly dosing• Adding a targeted agent (e.g. bevacizumab)• Maintenance or consolidation chemotherapy after complete
remission

JGOG: Dose-dense Weekly PaclitaxelJGOG: Dose-dense Weekly Paclitaxel
Paclitaxel 180 mg/m2 Carbolatin AUC = 6
Carbolatin AUC = 6Paclitaxel 80 mg/m2/w x3
• Epithelial Ovarian or Peritoneal• Stage II - IV• No prior therapy• Stratfied: residual disease,
stage, and histology• Primary endpoint: PFS• Secondary endpoint: OS
• Epithelial Ovarian or Peritoneal• Stage II - IV• No prior therapy• Stratfied: residual disease,
stage, and histology• Primary endpoint: PFS• Secondary endpoint: OS
Accrual: 637 pts (intent-to-treat)
I
II
Isonishi S et al. J Clin Oncol. 2008;26:A5506.
x6-9
x6-9
• Dose-dense paclitaxel associated with greater hematologic toxicity, and fewer patients completed all protocol therapy
• Improved PFS with dose-dense weekly paclitaxel

JGOG: Dose-dense Weekly PaclitaxelJGOG: Dose-dense Weekly Paclitaxel
Katsumata N et al Lancet. 2009;374:1331-1338.

GOG 262 Stage III/IV Disease: Large Volume ResidualGOG 262 Stage III/IV Disease: Large Volume Residual
Paclitaxel 80 mg/m2 IV every week + Carboplatin AUC 6 IV every 3 weeks x 6 cycles with optional Bevacizumab 15 mg/kg IV starting with cycle 2 until disease progression
RANDOMIZE
n = 625Primary Endpoint = Progression free survivalActivated: Sep 27 2010Study Chair: J Chan
Paclitaxel 175 mg/m2 IV + Carboplatin AUC 6 IV every 3 weeks x 6 cycles with optional Bevacizumab 15 mg/kg IV starting with cycle 2 until disease progression
ClinicalTrials.gov Identifier: NCT01167712

First-line Therapy: Acceptable ApproachesFirst-line Therapy: Acceptable Approaches
• Docetaxel instead of paclitaxel• Neoadjuvant chemotherapy• Intraperitoneal chemotherapy• Weekly dosing• Adding a targeted agent (e.g. bevacizumab)• Maintenance or consolidation chemotherapy after complete
remission

GOG-0218: SchemaGOG-0218: Schema
Front-line: Epithelial OV, PP or FT cancer
• Stage III optimal (macroscopic)• Stage III suboptimal• Stage IV
n=1800 (planned)
Carboplatin (C) AUC 6
Paclitaxel (P) 175 mg/m2
PlaceboBEV 15 mg/kgBEV 15 mg/kg
II
Stratification variables:• GOG performance status (PS)• Stage/debulking status
1:1:11:1:1
15 months
Paclitaxel (P) 175 mg/m2
Carboplatin (C) AUC 6
PlaceboPlacebo
I
ArmArm
Cytotoxic (6 cycles)
Carboplatin (C) AUC 6
Paclitaxel (P) 175 mg/m2III
Maintenance(16 cycles)
BEV 15 mg/kg
Burger RA et al. N Engl J Med. 2011;365:2473-2483.

GOG-0218: Investigator-assessed PFSGOG-0218: Investigator-assessed PFS
Arm I CP
(n=625)
Arm IICP + BEV(n=625)
Patients with event, n (%) 423 (67.7)
418 (66.9)
Median PFS, months 10.3 11.2
Stratified analysis HR (95% CI)
0.908(0.759–1.040)
One-sided P-value (log rank) 0.080*
+ BEV (Arm II)CP (Arm I)
*P-value boundary = 0.0116
+ BEV → BEV maintenance (Arm III)
Prop
ortio
n su
rvivi
ng p
rogr
essio
n fre
ePr
opor
tion
surv
iving
pro
gres
sion
free
Months since randomization
1.01.0
0.90.9
0.80.8
0.70.7
0.60.6
0.50.5
0.40.4
0.30.3
0.20.2
0.10.1
0000 1212 2424 3636
Arm IIICP + BEV BEV
(n=623)
360 (57.8)
14.1
0.717 (0.625–0.824)
<0.0001*
Burger RA et al. N Engl J Med. 2011;365:2473-2483.

GOG-0218CA-125 to Determine ProgressionGOG-0218CA-125 to Determine Progression
Protocol-definedPFS analysis
CA-125-censoredPFS analysis
Median PFS
CP (Arm I) 10.3 months 12.0 months
CP + BEV BEV (Arm III) 14.1 months 18.0 months
Absolute diff. median PFS 3.8 months 6.0 months
Hazard ratio 0.717 0.645
Censored for CA125, %
CP (Arm I) 0 20
CP + BEV BEV (Arm III) 0 29
Burger RA et al. N Engl J Med. 2011;365:2473-2483.

GOG-0218Interim Survival Analysis GOG-0218Interim Survival Analysis
Prop
ortio
n Al
ive
Months since randomization
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
00 12 24 36 48
aStratified analysis625/625/623 442/432/437 173/162/171 46/39/40
No. at risk
Arm ICP
(n=625)
Arm IICP + BEV(n=625)
Arm IIICP + BEV BEV
(n=623)
Patients with events, n (%)
156 (25.0)
150 (24.0)
138 (22.2)
Median, months 39.3 38.7 39.7
HRa
(95% CI)1.036
(0.827–1.297)0.915
(0.727–1.152)
One-sided P value 0.361 0.252
Burger RA et al. N Engl J Med. 2011;365:2473-2483.

ICON7: Study DesignICON7: Study Design
Stratification variables: • Stage/surgery• Time since surgery• GCIG group *Might vary based on GCIG group
**Omit cycle 1 bevacizumab if <4 weeks from surgery
Paclitaxel 175 mg/m2
Carboplatin AUC 6*
AVASTINAVASTIN
Carboplatin AUC 6*
Paclitaxel 175 mg/m2
Arm A
Arm B
12 months
Front-line EOC, PP or FT cancer
• Stage I-IIA (Gr 3 or CC) • Stage IIB/C• Stage III• Stage IV
n=1528
Front-line EOC, PP or FT cancer
• Stage I-IIA (Gr 3 or CC) • Stage IIB/C• Stage III• Stage IV
n=1528
Bevacizumab 7.5 mg/kg****
Primary endpoints: PFS
Secondary endpoints: OS, RR, safety, QOL, cost-effectiveness,translational
No IRC present
Perren T et al. N Engl J Med. 2011;365:2484-2496.Perren et al. ESMO 2010.

ICON 7Summary of Updated ResultsICON 7Summary of Updated Results
ParameterProtocol-defined
AnalysisBulk Disease
Analysis
PFS HR = 0.87, P = 0.039
CP 17.4 months
CP + BEVBEV 19.8 months
OS HR = 0.84, P = 0.099 HR = 0.64, P = 0.002
CP 28.8 months
CP + BEVBEV 36.6 months
Kristensen G et al. J Clin Oncol. 2011;29: suppl; abstr LBA5006).Perren T et al. N Engl J Med. 2011;365:2484-2496.
First-line Therapy: Acceptable ApproachesFirst-line Therapy: Acceptable Approaches
• Docetaxel instead of paclitaxel• Neoadjuvant chemotherapy• Intraperitoneal chemotherapy• Weekly dosing• Adding a targeted agent (e.g. bevacizumab)• Maintenance or consolidation chemotherapy after
complete remission

GOG 178—Investigating Paclitaxel as ConsolidationGOG 178—Investigating Paclitaxel as Consolidation
Markman M et al. J Clin Oncol. 2003;21:2460-2465.
277 stage III/IV patients in completeclinical remission
Paclitaxel 175 mg/m2 every 28 days × 3 monthsPaclitaxel 175 mg/m2 every 28 days × 3 months
Paclitaxel 175 mg/m2 every 28 days × 12 monthsPaclitaxel 175 mg/m2 every 28 days × 12 months
CR = Complete response.
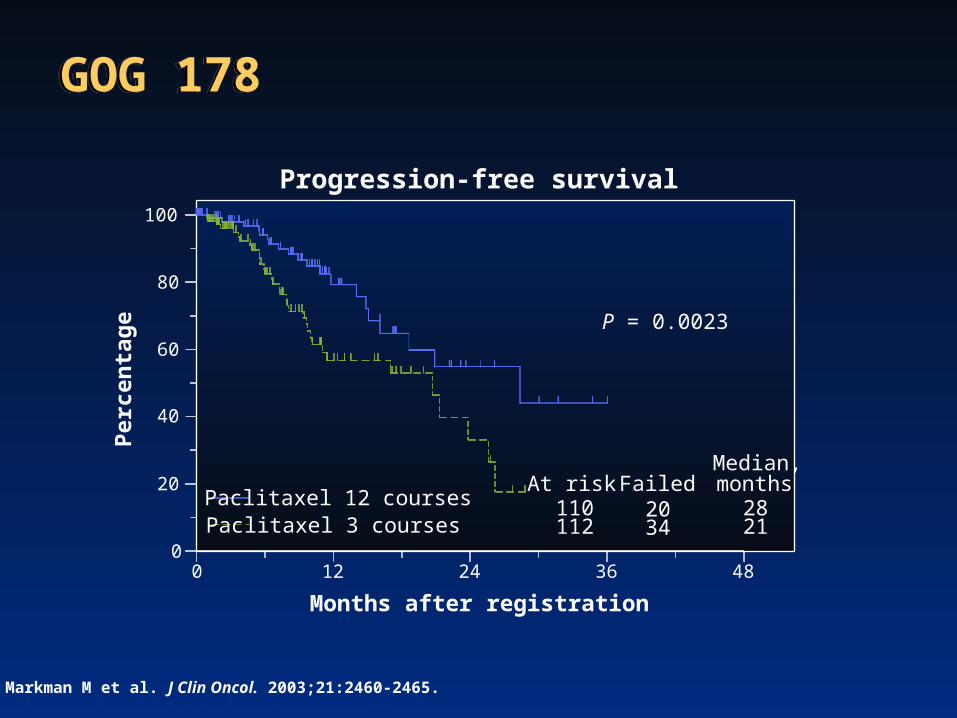
Progression-free survival
0
20
40
60
80
100
0 12 24 36 48
Months after registration
Paclitaxel 12 coursesPaclitaxel 3 courses
110At risk
112
Failed2034
Median,months
2821
P = 0.0023
Perc
enta
ge
Markman M et al. J Clin Oncol. 2003;21:2460-2465.
GOG 178GOG 178

GOG-0212Phase III Maintenance Therapy TrialGOG-0212Phase III Maintenance Therapy Trial
Primary endpoint: survivalSecondary endpoints: PFS, toxicity, QoL
www.clinicaltrials.gov/ct2/show/NCT00108745.
Macromolecular complexMacromolecular complex of paclitaxel poliglumexof paclitaxel poliglumex
Patients with stage III/IV epithelial ovarian or primary peritoneal cancer, GOG PS ≤ 2, and complete response after surgery plus taxane and carboplatin
(Planned n = 1400-1550)
Paclitaxel Every 28 days for up to 12 courses
Paclitaxel Every 28 days for up to 12 courses
No treatmentNo treatment
Paclitaxel poliglumex Every 28 days for up to 12 courses
Paclitaxel poliglumex Every 28 days for up to 12 courses

Summary: Initial Treatment of Advanced Ovarian CancerSummary: Initial Treatment of Advanced Ovarian Cancer
• Surgery– Attempt at maximal surgical cytoreduction– Neoadjuvant chemo before surgery is an option for poor surgical candidates
• Chemotherapy– 6-8 cycles taxane-platinum combination is standard– IP admin benefits patients with low volume (optimal) disease but has
increased toxicity NED patients treated with IP have a median survival of over 9 years
– Weekly (dose-dense) paclitaxel improves outcome in one study Confirmatory North American trials recently completed
– Bevacizumab during and after chemotherapy improves PFS but not OS

Case DiscussionsCase Discussions

Case 1: A Newly Diagnosed Patient With Ovarian Cancer
Case 1: A Newly Diagnosed Patient With Ovarian Cancer • 58 year old real estate broker with controlled hypertension
presents with a pelvic mass, omental caking, and a CA125 of 2,056. She has no malnutrition or change in her weight. She is a PS=0.
What would you recommend for this patient? 1.Neoadjuvant chemotherapy2.Primary radical debulking surgery

What Would You Recommend for This Patient? What Would You Recommend for This Patient?
• Neoadjuvant chemotherapy• Primary radical debulking surgery
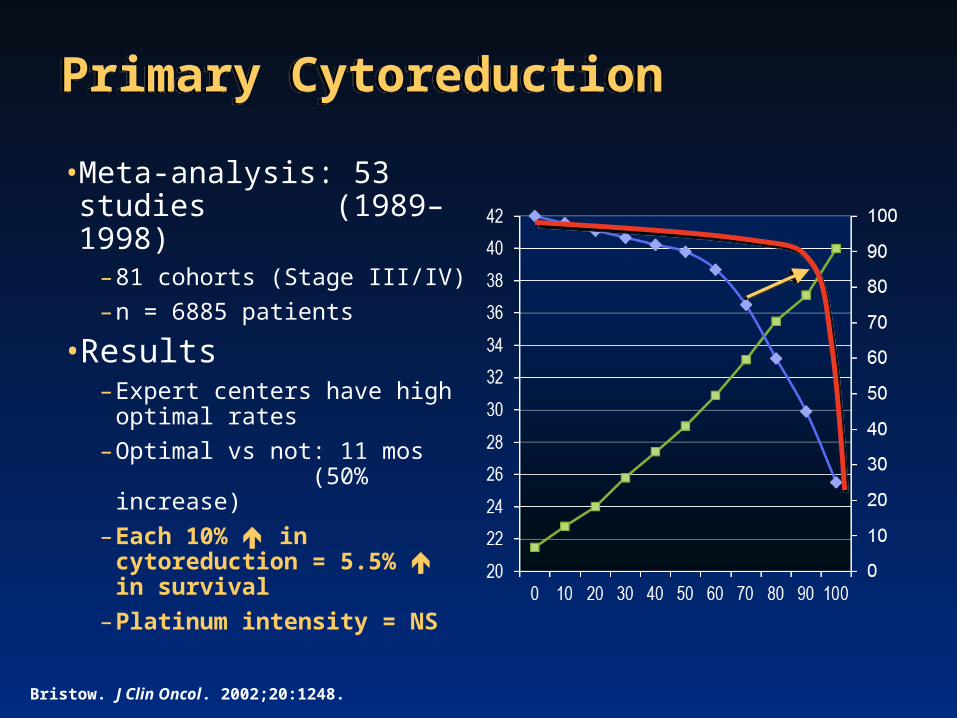
Primary CytoreductionPrimary Cytoreduction
• Meta-analysis: 53 studies (1989–1998)
– 81 cohorts (Stage III/IV)– n = 6885 patients
• Results– Expert centers have high optimal
rates– Optimal vs not: 11 mos
(50% increase)– Each 10% in cytoreduction =
5.5% in survival – Platinum intensity = NS
Bristow. J Clin Oncol. 2002;20:1248.
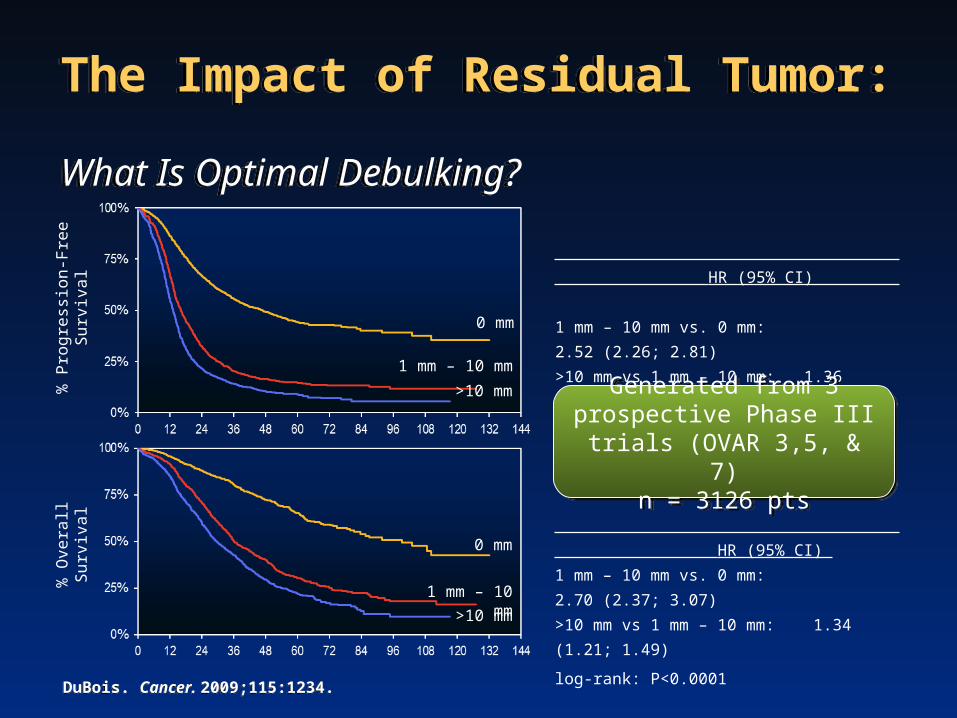
The Impact of Residual Tumor: What Is Optimal Debulking?The Impact of Residual Tumor: What Is Optimal Debulking?
% P
rogr
essio
n-Fr
ee S
urviv
al
0 mm
1 mm – 10 mm
>10 mm
HR (95% CI)
1 mm – 10 mm vs. 0 mm: 2.52 (2.26; 2.81)
>10 mm vs 1 mm – 10 mm: 1.36 (1.24; 1.50)
log-rank: P<0.0001
% O
vera
ll Sur
vival
0 mm
1 mm – 10 mm>10 mm
HR (95% CI)
1 mm – 10 mm vs. 0 mm: 2.70 (2.37; 3.07)
>10 mm vs 1 mm – 10 mm: 1.34 (1.21; 1.49)
log-rank: P<0.0001
Generated from 3 prospective Phase III trials (OVAR 3,5, & 7)
n = 3126 pts
Generated from 3 prospective Phase III trials (OVAR 3,5, & 7)
n = 3126 pts
DuBois. Cancer. 2009;115:1234. DuBois. Cancer. 2009;115:1234.

Case 1 Case 1
• She has a TAH BSO, transverse colectomy, omentectomy and spends 7 days in the hospital (2 in the ICU). Except for an open wound with a wound-vac and getting 4 units of blood, she does well…
• The pathology shows a high-grade serous carcinoma.
• The surgeon noted small volume residual (5-9mm) disease throughout the abdomen.
What would you recommend for this patient at this point?
1.IP chemotherapy
2.IV chemotherapy
3.Adding bevacizumab to either IV or IP
Case 1 Question 2 Case 1 Question 2
What would you recommend for this patient at this point?1.IP chemotherapy
2.IV chemotherapy
3.Adding bevacizumab to either IV or IP
All the above answers are reasonable treatment choices.• When would you start the bevacizumab?• Cycle 1, 2 or 3? • After the chemotherapy (maintenance)?

Case 2: Platinum Sensitive Ovarian CancerCase 2: Platinum Sensitive Ovarian Cancer
• 52-year-old woman with high-grade serous carcinoma of the fallopian tube• Optimally debulked in 2010
– Treated with IV paclitaxel, IP cisplatin and IP paclitaxel completed June 2011• CA125
– at presentation 5800– nadir post therapy 7– In 2012 : Increasing Ca125 (1200)
• Imaging: diffuse peritoneal carcinomatosis; pleural nodularity; mediastinal adenopathy
• Symptomatic: abdominal bloating, early satiety, and mild shortness of breath
• Disease free interval: 10-12 months • Genetic testing: BRCA1/2 negative

Case 2 Question 1Case 2 Question 1
• What treatment would you recommend for this patient?1. Pegylated liposomal doxorubicin (PLD, doxil, lipodox) and
carboplatin
2. PLD, carboplatin and bevacizumab
3. Gemcitabine and carboplatin
4. Gemcitabine, carboplatin and bevacizumab
5. Paclitaxel and carboplatin
6. Weekly paclitaxel and carboplatin
7. Paclitaxel, carboplatin and PARP inhibitor

Case 2, Question 1Case 2, Question 1What treatment would you recommend for this patient?
1. Pegylated liposomal doxorubicin (PLD, doxil, lipodox) and carboplatin (PLD and carboplatin is a reasonable option based on results of the CALYPSO study showing superiority to paclitaxel and carboplatin)
2. PLD, carboplatin and bevacizumab (PLD, carboplatin and bevacizumab has not been tested in a randomized phase III trial)
3. Gemcitabine and carboplatin (Gemcitabine and carboplatin: this is reasonable based on a comparison with carboplatin alone (Pfisterer et.al. 2005)
4. Gemcitabine, carboplatin and bevacizumab (Higher response rates and improved PFS are seen when bevacizumab is added to gem/carbo but OS is not improved (OCEANS trial)
5. Paclitaxel and carboplatin (Paclitaxel and carboplatin can be used but based on prior taxane and results of CALYPSO, is used less)
6. Weekly paclitaxel and carboplatin (Weekly paclitaxel has shown improved outcome when used with carboplatin for newly diagnosed patients but has not been rigorously tested in recurrent disease
7. Paclitaxel, carboplatin and PARP inhibitor (PARP inhibitors are not yet FDA approved , so can only be obtained on a clinical trial. However, this is a very promising direction in ovarian cancer and a clinical trial of paclitaxel and carboplatin +/- olaparib showed improved PFS (Oza et.al. ASCO 2012)

She Asks You Whether There Is Any Role for Surgery for HerShe Asks You Whether There Is Any Role for Surgery for Her
Which of the following are true regarding secondary debulking?1. It is not considered for patients like her who relapse 10-12 months after
completing initial chemotherapy
2. The finding of carcinomatosis is a relatively strong contraindication to secondary debulking surgery
3. Survival is improved for secondary debulking even if all disease can’t be removed at surgery
4. Mediastinal and pleural disease are relatively strong contraindications to secondary debulking surgery
5. 1 and 3
6. 2 and 4
7. All of the above

Secondary DebulkingCandidate SelectionSecondary DebulkingCandidate Selection
Onda et al. J Cancer. 2005;92:1026.

Pujade-Lauraine, Ann Oncol. 2011;22(Supplement 8):viii61–viii64.

GCIG CALYPSO TrialGCIG CALYPSO Trial
Ovarian CancerPlatinum Sens.Stratify:≤ 0.5 cm> 0.5-2 cm
PLD 30 mg/m2
Carboplatin AUC = 5q 28 days x 6
PLD 30 mg/m2
Carboplatin AUC = 5q 28 days x 6
Paclitaxel 175 mg/m2
Carboplatin AUC = 5q 21 days x 6
Paclitaxel 175 mg/m2
Carboplatin AUC = 5q 21 days x 6
GCIG = Gynecologic Cancer IntergroupPFS = progression-free survivalPLD = pegylated liposomal doxorubicin
Accrual 864 ptsPFS primary endpoint
Pujade-Lauraine E et al. J Clin Oncol. 2010;28:3323-3329.
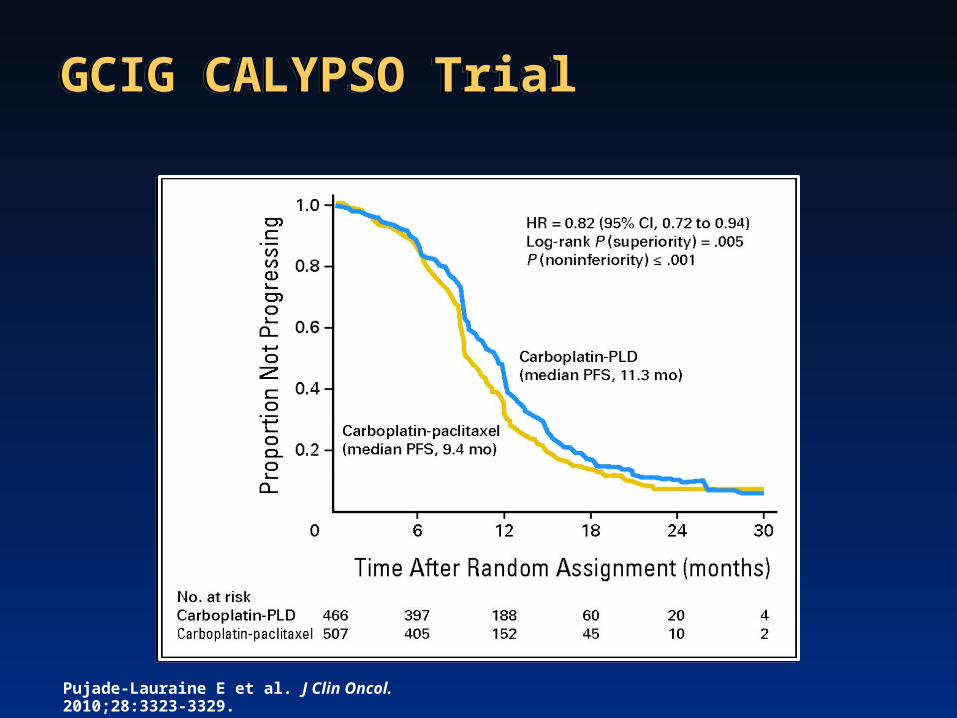
GCIG CALYPSO TrialGCIG CALYPSO Trial
Pujade-Lauraine E et al. J Clin Oncol. 2010;28:3323-3329.

Selected Non-hematologic Toxicities During TreatmentSelected Non-hematologic Toxicities During Treatment
CD (n=466) CP (n=501)
Alopecia grade 2* 7% 84%
Alopecia
*P< 0.001
Pujade-Lauraine E et al. J Clin Oncol. 2010;28:3323-3329.

Targeted Agents in Ovarian CancerTargeted Agents in Ovarian Cancer
• Signaling/Angiogenesis– Bevacizumab/Aflibercept– RTKI’s:
• Pazopanib• Cabozantinib• Sorafenib, etc• Cediranib• Nintedanib
– Trebananib, MEDI-3617– PI3K/Akt/mTOR– MEKi
• Folate:- Vintafolide (EC-145)- Farletuzumab
• NKTR-102• Taxanes/epothilones• Immunotherapy – vaccines
and inducers• EP-100• PARPi• ErbB3
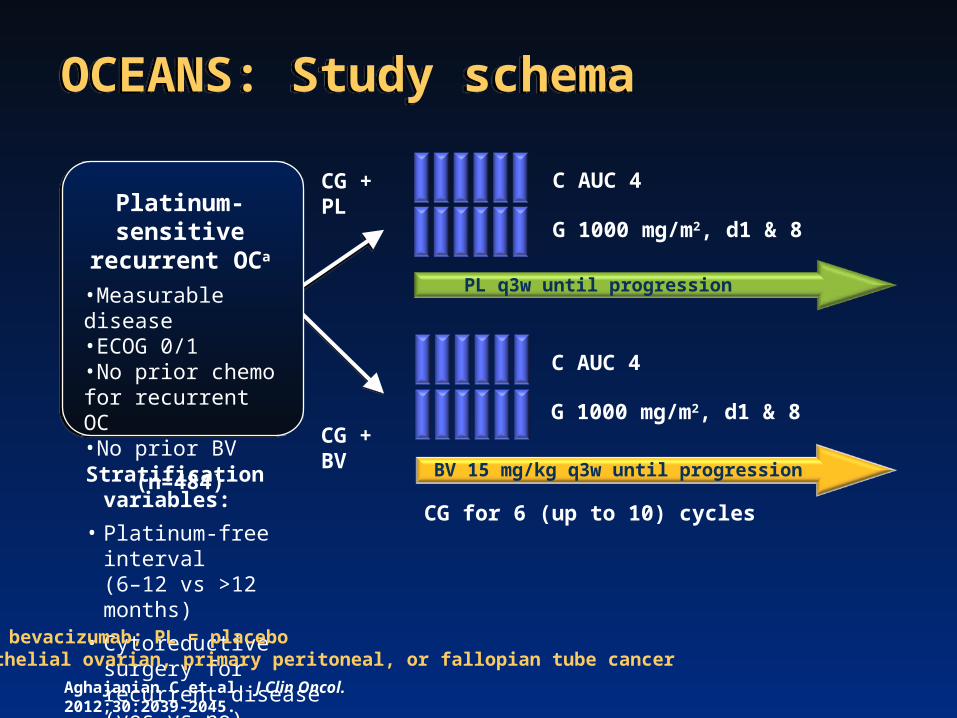
CG + PL
OCEANS: Study schemaOCEANS: Study schema
CG for 6 (up to 10) cycles
Stratification variables:
• Platinum-free interval (6–12 vs >12 months)
• Cytoreductive surgery for recurrent disease (yes vs no)
Platinum-sensitive recurrent OCa
•Measurable disease•ECOG 0/1•No prior chemo for recurrent OC•No prior BV
(n=484)
BV = bevacizumab; PL = placeboaEpithelial ovarian, primary peritoneal, or fallopian tube cancer
G 1000 mg/m2, d1 & 8
C AUC 4
PL q3w until progression
C AUC 4
BV 15 mg/kg q3w until progression
G 1000 mg/m2, d1 & 8CG + BV
Aghajanian C et al. J Clin Oncol. 2012;30:2039-2045.

242242 177177 4545 1111 33 00CG + PLCG + PL
OCEANS: Primary Analysis of PFSOCEANS: Primary Analysis of PFS
CG + PL(n=242)
CG + BV(n=242)
Events, n (%) 187 (77) 151 (62)
Median PFS, months (95% CI)
8.4(8.3–9.7)
12.4(11.4–12.7)
Stratified analysis HR (95% CI)Log-rank P-value
0.484 (0.388–0.605)
<0.0001
MonthsMonthsNo. at riskNo. at risk
242242 203203 9292 3333 1111 00CG + BVCG + BV
1.0
0.8
0.6
0.4
0.2
0
1.0
0.8
0.6
0.4
0.2
0
Prop
ortio
n pr
ogre
ssio
n fr
eePr
opor
tion
prog
ress
ion
free
00 66 1212 1818 2424 3030
Aghajanian C et al. J Clin Oncol. 2012;30:2039-2045.

1.0
0.8
0.6
0.4
0.2
0
1.0
0.8
0.6
0.4
0.2
0
OCEANS: Third Interim OS AnalysisaOCEANS: Third Interim OS Analysisa
GC + PL(n=242)
GC + BV(n=242)
Events, n (%) 142 (58.7) 144 (59.5)
Median OS, months (95% CI)
33.7(29.3 38.7)‒
33.4(30.3 35.8)‒
HR (95% CI) Log-rank P value
0.960 (0.760–1.214)P=0.7360
0 6 12 18 24 30 36 42 48 54 600 6 12 18 24 30 36 42 48 54 60
242 235 221 190 159 117 77 44 23 7 0242 239 226 201 171 127 78 48 27 7 0
242 235 221 190 159 117 77 44 23 7 0242 239 226 201 171 127 78 48 27 7 0
Number at risk: GC + PLGC + BV
Number at risk: GC + PLGC + BV
aData cutoff date: March 30, 2012. Median follow-up 41.9 months in PL arm and 42.3 months in BV arm, with 286 deaths (59.1% of patients)
Prop
ortio
n su
rviv
ing
Months
Aghajanian et al. ESMO 2012.

Asymptomatic relapseAsymptomatic relapse
Single-agent farletuzumab Single-agent farletuzumab Until progressionUntil progression
Single-agent ORRSingle-agent ORR
Compare lengths of first and Compare lengths of first and second remissionssecond remissions
Farletuzumab - MORAb-003-002 Phase II: DesignFarletuzumab - MORAb-003-002 Phase II: Design
Epithelial Ovarian CancerEpithelial Ovarian CancerFirst platinum-sensitive relapseFirst platinum-sensitive relapseFirst remission of 6-18 monthsFirst remission of 6-18 months
Evaluable disease by CA125Evaluable disease by CA125
Symptomatic relapseSymptomatic relapse
Original Carbo/Taxane regimenOriginal Carbo/Taxane regimenPlus farletuzumab x 6Plus farletuzumab x 6
Farletuzumab maintenance RxFarletuzumab maintenance RxFor respondersFor responders
Combination ORRCombination ORR
White AJ et al. J Clin Oncol. 2010;28(15s):Abstract 5001.

MorAb-003-002: Study ConclusionsMorAb-003-002: Study Conclusions
• Overall response rate 70%– Response rate similar in early (6-12 month) and late
(12+ months) recurrent patients • High rates of CA-125 normalization (89%)• 1/5 patients had a PFI2 ≥ PFI1• Phase III studies
– Platinum-sensitive: fully enrolled– Platinum-resistant (weekly paclitaxel): met futility endpoint
White AJ et al. J Clin Oncol. 2010;28(15s):Abstract 5001.

n=66
Randomized, Open-label, Phase II Study in Patients With Platinum-sensitive, Advanced Serous Ovarian Cancer
Randomized, Open-label, Phase II Study in Patients With Platinum-sensitive, Advanced Serous Ovarian Cancer
Paclitaxel 175 mg/m2 (iv, d1)
+ carboplatin AUC6(iv d1)
Maintenancephase
Olaparib 400 mg bid continuously
Completion of 4–6 x 21-day cycles
of chemotherapy
Arm BArm A
n=81
n=81 n=55
Multinational study; 43 sites in 12 countries* Capsule formulation
Patients with:• Platinum-sensitive advanced ovarian cancer
• A serous histology or serous component
• Measurable disease
• ≤3 previous platinum-containing regimens
• Progression free for ≥6 months following completion of last platinum-containing regimen
Patients with:• Platinum-sensitive advanced ovarian cancer
• A serous histology or serous component
• Measurable disease
• ≤3 previous platinum-containing regimens
• Progression free for ≥6 months following completion of last platinum-containing regimen
Maintenancephase
No further study treatment
Olaparib 200 mg bid* (d1–10 every 21 days)
+ paclitaxel 175 mg/m2
(iv, d1)
+ carboplatin AUC4(iv, d1)
Oza A. ASCO 2012; Abstract 5001.

Paclitaxel Carboplatin (P/C) vs P/C Plus Olaparib (O/P/C) In Platinum Sensitive Recurrent Ovarian Cancer: PFS
Paclitaxel Carboplatin (P/C) vs P/C Plus Olaparib (O/P/C) In Platinum Sensitive Recurrent Ovarian Cancer: PFS
Time from randomization (months)0
Prop
ortio
n of
pat
ient
s pr
ogre
ssio
n fr
ee
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
2 4 6 8 10 12 16 20Number of patients at risk
Olaparib + P + C (AUC4)P + C (AUC6)
14 18
81 80 76 71 55 37 34 3 020 081 68 65 57 40 18 15 2 08 1
O/P/CP/C
Oza A. ASCO 2012; Abstract 5001.
O/P/C P/C
Events: Total patients (%) 47:81 (58.0) 55:81 (67.9)
Median (months) 12.2 9.6
Hazard ratio = 0.51 95% CI (0.34, 0.77)
P=0.0012

GOG 9927: Phase I CombinationGOG 9927: Phase I Combination
• Platinum sensitive recurrent EOC• Chemotherapy based on CALYPSO• Primary endpoint: 1st or 2nd cycle DLT• Secondary endpoints: RR, PFS, Toxicity• TR: PARPi in PBMCs, BRCA status
PLD 30 mg/m2 Carboplatin AUC 5
Arm IVeliparib PO daily continuously
Cycles: 28 daysPlanned administration: 6 cycles
Arm IIVeliparib PO daily D1-7
Cycles: 28 daysPlanned administration: 6 cycles
Dose LevelABT-888 Dose (mg, oral, BID)
Level -1 20 mg
Level 1 30 mg
Level 2 50 mg
Level 3 80 mg
Level 4 100 mg
Level 5 150 mg
Level 6 200 mg
Level 7 250 mg
Level 8 300 mg
Level 9 350 mg
Level 10 400 mg
www.clinicaltrials.gov/ct2/show/NCT01459380.

Summary for Platinum-sensitive Recurrent Ovarian CancerSummary for Platinum-sensitive Recurrent Ovarian Cancer
• Consider Secondary Debulking• Platinum retreatment is standard• Treatment with a platinum-based doublet improves
response rate, progression-free survival, and possibly overall survival
• Options:– Taxane Carboplatin: Paclitaxel, Docetaxel (?), Weekly
Paclitaxel (?)– Gemcitabine Carboplatin +/- Bevacizumab– PLD Carboplatin

Case 3: Platinum Resistant Ovarian CancerCase 3: Platinum Resistant Ovarian Cancer
• 60-year-old woman with extensive pelvic and peritoneal implants, ascites and large volume disease at the root of the mesentery
• Diagnosis of ovarian cancer made by paracentesis
• Deemed unresectable by a gynecologic oncologist
• Treated with neoadjuvant paclitaxel and carboplatin x 3 without response
• Then treated with topotecan (daily x 5 regimen) x 3 without response
• Required paracentesis weekly for palliation
• CA-125=6916
• What treatment would you recommend?

Case 3 Question 1Case 3 Question 1
What treatment would you recommend for this patient?1. Pegylated liposomal doxorubicin (PLD, doxil, lipodox)
2. Weekly paclitaxel
3. Gemcitabine
4. Bevacizumab
5. Weekly paclitaxel and bevacizumab
6. Gemcitabine, carboplatin and bevacizumab

Case 3 Question 1Case 3 Question 1
What treatment would you recommend for this patient?1. Pegylated liposomal doxorubicin (PLD, doxil, lipodox) (PLD is a reasonable choice but expected
response rate is 6-16% in a less heavily pretreated population)
2. Weekly paclitaxel (Weekly paclitaxel is also a reasonable option. In GOG protocol 126-N weekly paclitaxel had a response rate of 21% although eligibility limited to one prior treatment regimen)
3. Gemcitabine (although single agent gemcitabine is not FDA approved for treatment of ovarian cancer, the combination of gemcitabine and carboplatin is approved for platinum sensitive patients thus gemcitabine alone is frequently used. Response rates in this population are expected to be less than 10%)
4. Bevacizumab (Bevacizumab is a reasonable choice. In GOG protocol 170D bevacizumab showed a response rate of 21% in this population)
5. Weekly paclitaxel and bevacizumab (Based on Aurelia, the combination of weekly paclitaxel and bevacizumab would be expected to have a higher response rate than weekly paclitaxel alone. Survival data is not yet available. It is not yet clear whether sequential chemotherapy and bevacizumab or the combination is preferable)
6. Gemcitabine, carboplatin and bevacizumab (platinum-based therapy is not indicated in this patient with platinum-refractory disease.)

Assume You Will Be Using Treatment With Bevacizumab: Which of the Following Are True Statements About Bevacizumab for Her
Assume You Will Be Using Treatment With Bevacizumab: Which of the Following Are True Statements About Bevacizumab for Her
1. She will be at increased risk for bowel perforation
2. There is an increased risk of thrombo-embolic phenomena with bevacizumab
3. The response rate of ovarian cancer to single-agent bevacizumab is greater than for any other solid tumors tested to date
4. Hypertension and proteinuria are common side effects of bevacizumab
5. All of the above
All the above are true statements in this case.

Annals of Oncology 22 (Supplement 8): viii61–viii64, 2011.

Active Agents in Ovarian CancerActive Agents in Ovarian Cancer

Platinum-resistant Ovarian Cancer Cytotoxic TherapyPlatinum-resistant Ovarian Cancer Cytotoxic Therapy
STUDY* AGENT N RESPONSE RATE
126-J Docetaxel 58 22%
126-N Weekly Paclitaxel 48 21%
126-M Ixabepilone 50 14%
126-Q Pemetrexed 48 21%
126-R nab-Paxlitaxel 47 23%Thresholds: 10%, 25%
Randomized phase II, NKTR-102*
145 mg/m2 q14 d 33 21%
145 mg/m2 q21 d 31 23%*Median of 3 prior lines
*1 prior line
Vergote IB et al. J Clin Oncol 2010;28:15s(suppl; abstr 5013).

Bevacizumab in Relapsed Ovarian CancerBevacizumab in Relapsed Ovarian Cancer
GOG 170-D*(N = 62)
NCI 5789**(N = 70)
Phase II Study***(N = 44)
Study Treatment
Single agent BV 15 mg/kg q 3 wk
BV 10 mg/kg q 2 wks + low dose oral
cyclophos.
Single agent BV 15 mg/kg
q 3 wk
Prior Regimens
1 – 21/62 (34%) 2 - 41/62 (62%)
Median = 2Range 1-3
2 - 23/44 (52%)3 - 21/44 (48%)
Platinum Resistant
42% 40% 100%
Efficacy ORR 6-mo PFS
21%39%
24%56%
16%27%
GIP or fistula 0 4 (6%) 5 (11%)
*Burger RA et al. J Clin Oncol 2007; 25: 5165–5171. **Garcia AA et al. J Clin Oncol 2008; 26: 76–82.***Cannistra SA et al. J Clin Oncol 2007; 25: 5180–5186.
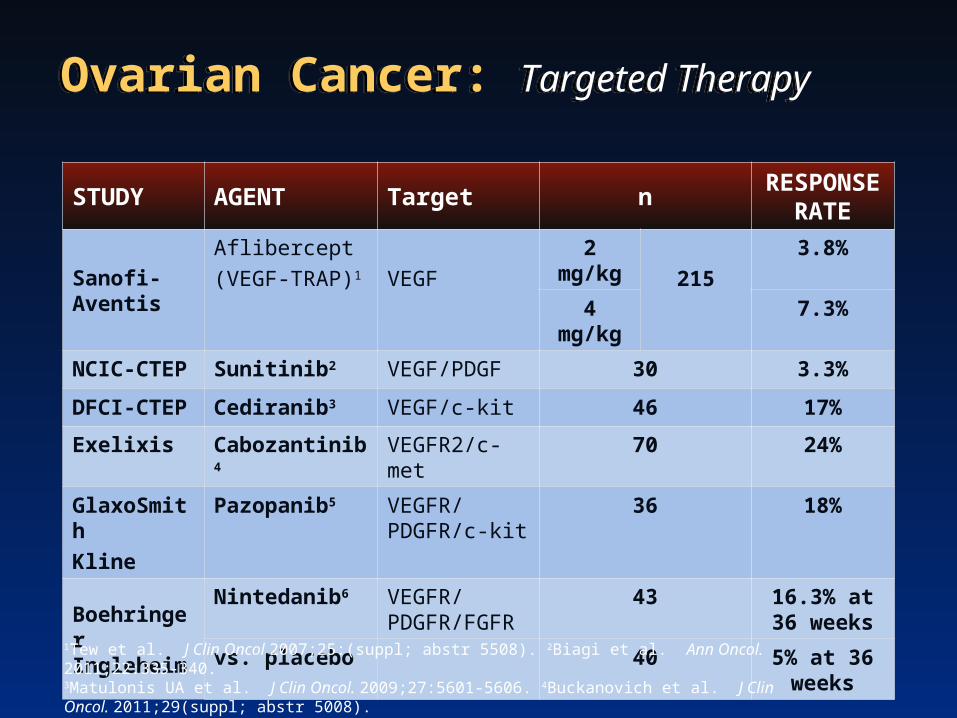
Ovarian Cancer: Targeted TherapyOvarian Cancer: Targeted Therapy
STUDY AGENT Target nRESPONSE
RATE
Sanofi-AventisAflibercept(VEGF-TRAP)1 VEGF
2 mg/kg
215
3.8%
4 mg/kg 7.3%
NCIC-CTEP Sunitinib2 VEGF/PDGF 30 3.3%
DFCI-CTEP Cediranib3 VEGF/c-kit 46 17%
Exelixis Cabozantinib4 VEGFR2/c-met 70 24%
GlaxoSmith
Kline
Pazopanib5 VEGFR/PDGFR/c-kit
36 18%
Boehringer Ingleheim
Nintedanib6 VEGFR/PDGFR/FGFR
43 16.3% at 36 weeks
vs. placebo 40 5% at 36 weeks
1Tew et al. J Clin Oncol 2007;25:(suppl; abstr 5508). 2Biagi et al. Ann Oncol. 2011;22:335-340. 3Matulonis UA et al. J Clin Oncol. 2009;27:5601-5606. 4Buckanovich et al. J Clin Oncol. 2011;29(suppl; abstr 5008).5Friedlander et.al. Gyn Oncol. 2010,. 6Ledermann et al. J Clin Oncol. 2011;29:3798.

PDPD
Recurrent Ovarian Cancer Randomized Phase II StudiesRecurrent Ovarian Cancer Randomized Phase II Studies
Weekly PaclitaxelWeekly PaclitaxelAMG-386 10 mg/kg IV weeklyAMG-386 10 mg/kg IV weekly
n=53n=53
Weekly PaclitaxelWeekly PaclitaxelAMG-386 3 mg/kg IV weeklyAMG-386 3 mg/kg IV weekly
n=53n=53
Weekly PaclitaxelWeekly PaclitaxelPlaceboPlacebo
n=55n=55Paclitaxel 80 mg/m2 IV weekly, 3 weeks on/1 week off
AMG-386AMG-38610 mg/kg IV10 mg/kg IV
weeklyweekly
10 mg/kg 3 mg/kg Placebo
*Median PFS, months 7.2 5.7 4.6*HR (Arm A+B vs placebo) = 0.76 (80% CI, 0.59, 0.98), p=0.17, Trend test, p=0.037
ORR (CR+PR) 37% 19% 27%
Ovarian, primary Ovarian, primary peritoneal, or peritoneal, or fallopian tube fallopian tube
cancercancern=161n=161
1-3 prior lines1-3 prior lines
Karlan BY et al. J Clin Oncol. 2010;28:15s(suppl; abstr 5000).

Recurrent Ovarian Cancer Randomized Phase II StudiesRecurrent Ovarian Cancer Randomized Phase II Studies
STUDY* AGENTS
186-GBevacizumab-Everolimus vsBevacizumab-Placebo
Completed accrual
186-IBevacizumab-Fosbretabulin vsBevacizumab
Accrual in progress
186-JWeekly Paclitaxel-Pazopanib vsWeekly Paclitaxel-Placebo
Accrual in progress
Primary endpoint: PFS*1-3 prior lines
www.clinicaltrials.gov

Olaparib: An Orally Active PARP Inhibitor in Ovarian CancerOlaparib: An Orally Active PARP Inhibitor in Ovarian Cancer
Provides clinical evidence of activity in ovarian cancer patients with and without BRCA1/2 mutationsProvides clinical evidence of activity in ovarian cancer patients with and without BRCA1/2 mutations
1. Fong PC et al. J Clin Oncol 2010;28:2512–2519. 2. Audeh MW et al. Lancet 2010;376:245–251.3. Gelmon KA et al. Lancet Oncol 2011;12:852–861.
*Complete response (CR) + partial response (PR) + stable disease (SD)
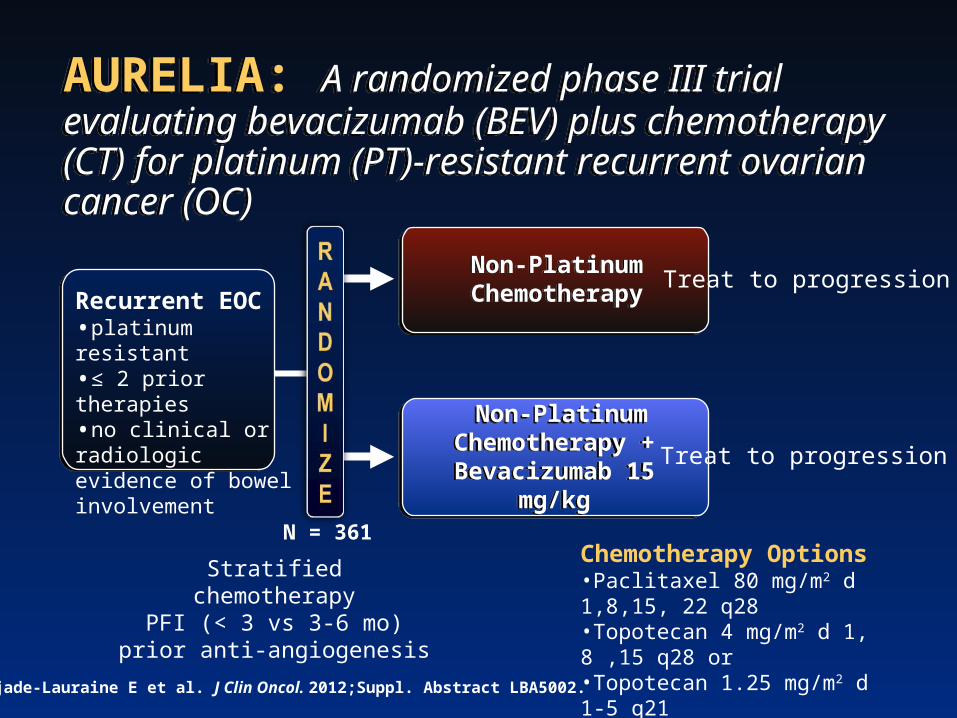
AURELIA: A randomized phase III trial evaluating bevacizumab (BEV) plus chemotherapy (CT) for platinum (PT)-resistant recurrent ovarian cancer (OC)
AURELIA: A randomized phase III trial evaluating bevacizumab (BEV) plus chemotherapy (CT) for platinum (PT)-resistant recurrent ovarian cancer (OC)
Recurrent EOC•platinum resistant•≤ 2 prior therapies•no clinical or radiologic evidence of bowel involvement
Non-Platinum ChemotherapyNon-Platinum Chemotherapy
Non-Platinum Chemotherapy +
Bevacizumab 15 mg/kg
Non-Platinum Chemotherapy +
Bevacizumab 15 mg/kg
Chemotherapy Options•Paclitaxel 80 mg/m2 d 1,8,15, 22 q28•Topotecan 4 mg/m2 d 1, 8 ,15 q28 or •Topotecan 1.25 mg/m2 d 1-5 q21•PLD 40 mg/m2 d 1 q28
Stratifiedchemotherapy
PFI (< 3 vs 3-6 mo)prior anti-angiogenesis
Treat to progression
Treat to progression
N = 361
Pujade-Lauraine E et al. J Clin Oncol. 2012;Suppl. Abstract LBA5002.

AURELIA Progression-free SurvivalAURELIA Progression-free Survival
1.0
0.8
0.6
0.4
0.2
0.0
6 12
Time (months)
Estim
ated
Pro
babi
lity
18 3024
182 93 37 8 1 1 0 020179 140 88 18 4 1 149
0
BEV + CTC TNumber at risk
Events, n (%)
Median PFS, months(95% CI)
166 (91%)3.4
(2.2-3.7)
135 (75%)
C T(n = 182)
BEV + C T(n = 179)
6.7(5.7-7.9)
HR (unadjusted)(95% CI)Log-rnak P -value(2-sided, unadjusted)
0.48(0.38-0.60)
< 0.001
3.4 6.7
Pujade-Lauraine E et al. J Clin Oncol. 2012;Suppl. Abstract LBA5002.

Response Rates For Chemotherapy Alone Weekly Paclitaxel, Pegylated Liposomal Doxorubicin or Topotecan) or With Bevacizumab (BEV + CT)
Response Rates For Chemotherapy Alone Weekly Paclitaxel, Pegylated Liposomal Doxorubicin or Topotecan) or With Bevacizumab (BEV + CT)
aTwo-sided chi-square test with Schouten correction
P=0.001aP<0.001a P<0.001a
Patie
nts
(%)
Pujade-Lauraine E et al. J Clin Oncol. 2012;Suppl. Abstract LBA5002.

Questions about AURELIAQuestions about AURELIA
• Given known single agent response to bevacizumab, how would a bevacizumab alone arm compare?
• Is it better to use chemo with bevacizumab rather than sequentially?
– This should be answered by the overall survival data due in 2013, since patients on the chemo alone arm could subsequently get bevacizumab
• Should we limit this therapy to patients at low risk of GI perforation?
• Will these same benefits be seen in patients who had bevacizumab with initial chemotherapy?

Randomized 1:1:1
Randomized 1:1:1
Olaparib 200 mg bid
n=32
Olaparib 200 mg bid
n=32 PD or withdrawal from treatment for
other reason
PD or withdrawal from treatment for
other reason
As above or max lifetime cumulative
dose reached
As above or max lifetime cumulative
dose reached
Primary objective: Compare efficacy (PFS) of 2 dose levels of olaparib (200 mg and 400 mg bid) with pegylated liposomal doxorubicin (PLD)
Phase II Trial of Olaparib vs PLD in BRCA-associated Recurrent Ovarian CancerPhase II Trial of Olaparib vs PLD in BRCA-associated Recurrent Ovarian Cancer
Olaparib 400 mg bid
n=32
Olaparib 400 mg bid
n=32
Patients: •BRCA1/2 germline mutation•Recurrent Ovarian Cancer
Patients in PLD group were allowed to cross-over to olaparib 400 mg bid on confirmed PD
One cycle=28 days
Kaye SB et al. J Clin Oncol. 2012;30:372-379.
PLD 50 mg/m2 IVn=33
PLD 50 mg/m2 IVn=33

RECIST and CA-125 ResponsesRECIST and CA-125 Responses
Patients, n (%)
Olaparib 200 mg bid
(n=32)
Olaparib 400 mg bid
(n=32)PLD
(n=33)
Confirmed RECIST response 8 (25) 10 (31) 6 (18)
CA-125 response by GCIG* 11 (34) 18 (56) 11 (33)
Confirmed RECIST response and/or CA-125 response† 12 (38) 19 (59) 13 (39)
*GCIG criteria is confirmed ≥50% reduction in CA-125 levels that had to be maintained for ≥28 days; †CA-125 response in the absence of RECIST progression
Kaye SB et al. J Clin Oncol. 2012;30:372-379.
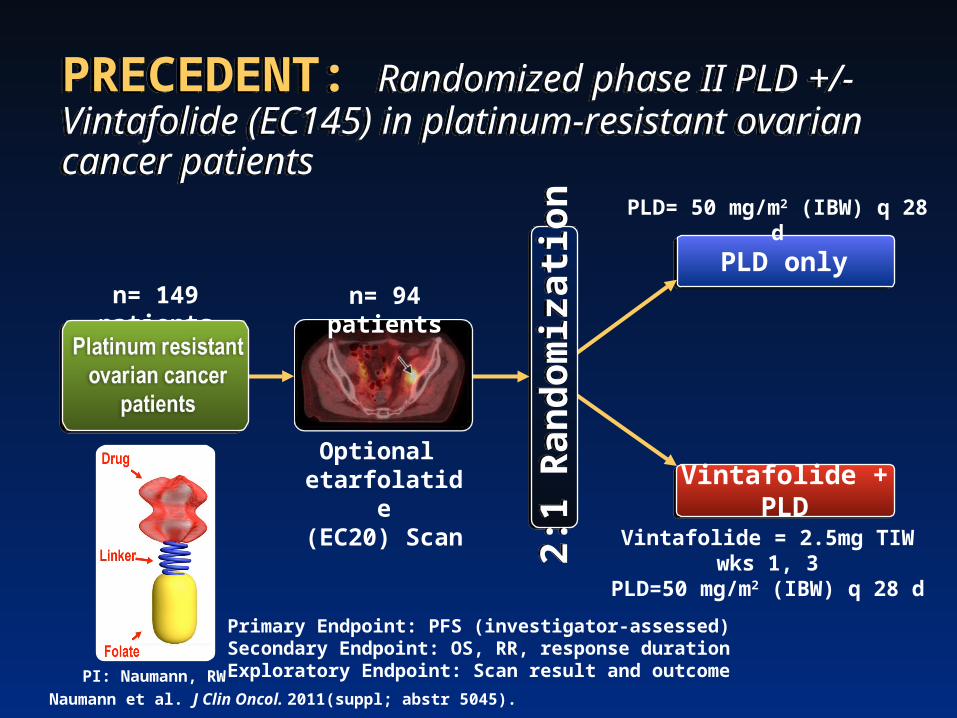
PRECEDENT: Randomized phase II PLD +/- Vintafolide (EC145) in platinum-resistant ovarian cancer patientsPRECEDENT: Randomized phase II PLD +/- Vintafolide (EC145) in platinum-resistant ovarian cancer patients
n= 149 patients
2:1
Ran
dom
izat
ion
2:1
Ran
dom
izat
ion
Vintafolide + PLD
PLD only
Optional etarfolatide(EC20) Scan
Vintafolide = 2.5mg TIW wks 1, 3PLD=50 mg/m2 (IBW) q 28 d
PLD= 50 mg/m2 (IBW) q 28 d
n= 94 patients
PI: Naumann, RW
Primary Endpoint: PFS (investigator-assessed)Secondary Endpoint: OS, RR, response durationExploratory Endpoint: Scan result and outcome
Naumann et al. J Clin Oncol. 2011(suppl; abstr 5045).

Primary Endpoint PFS ResultsPrimary Endpoint PFS Results
PFSEC145+PLD
n=100PLDn=49
Median time to event 5.0 months 2.7 months
HR (2-sided p-value) 0.63 (P-value=0.031)
PLD AlonePLD Alone Vintafolide + PLDVintafolide + PLD
Naumann et al. J Clin Oncol. 2011(suppl; abstr 5045).

Summary for Platinum-resistant Recurrent Ovarian CancerSummary for Platinum-resistant Recurrent Ovarian Cancer
• No benefit for combination chemotherapy• Sequential single-agent chemotherapy is standard• Multiple targeted agents with some demonstrated activity• Multiple trials of chemotherapy plus a targeted agent
showing increased ORR or PFS (but none to date with OS advantage)
– Chemotherapy plus bevacizumab (Aurelia)– Weekly paclitaxel plus trebananib (AMG-386)– PLD plus vintafolide

Thank you for joining us today!Thank you for joining us today!
Please remember to turn in your Please remember to turn in your evaluation form.evaluation form.
Your participation will help shape future CME activities.Your participation will help shape future CME activities.