welcome to this speechpathology.com live expert e...
TRANSCRIPT
1
Welcome to this SpeechPathology.com Live Expert e-Seminar!Delightful Dysphagia Dining
Presented By:
Gale Estes-Waddell, M.A., CCC-SLP
Moderated By:
Amy Hansen, M.A.,CCC-SLP, Managing Editor, SpeechPathology.com
Please call technical support if you require assistance
1-800-242-5183
Live Expert eSeminarATTENTION! SOUND CHECK!Unable to hear anyone speaking at this time?Please contact Speech Pathology for technical support at 800 242 5183
TECHNICAL SUPPORTTECHNICAL SUPPORTNeed technical support during event?Please contact Speech Pathology for technical support at 800 242 5183Submit a question using the Chat Pod - please include your phone number.
Earning CEUsEARNING CEUS•Must be logged in for full time requirement•Must pass short multiple-choice exam
Post-event email within 24 hours regarding the CEU exam ([email protected])
•Click on the “Start e-Learning Here!” button on the SP home page and login.•Must pass exam within 7 days of today•Two opportunities to pass the exam

2
Peer Review Process
Interested in Becoming a Peer Reviewer?
APPLY TODAY!
3+ years SLP Clinical experience 3+ years SLP Clinical experience Required
Contact: Amy Hansen [email protected]
Sending Questions
iType question or comment and click the send button
Download Handouts
Click to highlight handout
Click Save to My Computer

3
Delightful Dysphagia DiningDining
Gale Estes Waddell, M.A. CCC-SLP
Learner Outcomes
1) Identify 4 normal anatomical and physiological changes in the aging population that may affect eating and overall nutrition.
2) Identify 3 dysphagia/swallowing symptoms/ ) y y p g g y pdifficulties that may require a modified dysphagia diet.
3) Demonstrate 3 interventions to facilitate a safe swallow and improve PO intake.
4) Identify 3 methods to improve PO intake of a puree and thickened liquid diet.
Dysphagia
• Loss or impairment of the chewing and swallowing skills involving the oral, pharyngeal and/or esophageal phases of deglutition.
• Aspiration is passage of food and/or liquid into the larynx through the vocal folds.
4
Normal Aging & The Oral Phase
-Decreased sensation
-Changes in taste sensitivity (bitter, sweet & salty)
-Reduced lip posturing
-Decreased saliva volume & viscosity
-Mandibular/gum changes result in increased chewing strokes
-Decreased lingual strength
Normal Aging & The Pharyngeal Phase
The tongue base and hyoid lower due to soft tissue laxity.
Decreased strength results in residue.g Decreased airway protection and reduced epiglottic
flexibility. Orthopedic Changes and Diverticula may develop Changes in the UES due to orthopedic and ligament
laxity.
Normal Aging & The Esophageal Phase
Reduced peristalsis increases transit time.
Increased gastroesophageal reflux (GERD)
Mechanical Obstructions
Motility Disorders

5
Normal Aging & Digestive System
Rate of absorption slows. Stomach produces reduced number of gastric
enzymes. Liver produces less albumin and affects the
absorption of medications. Decreased esophageal and intestinal motility,
weakened abdominal and pelvic muscles Decreased sensation throughout the digestive
system Constipation
Symptoms/Signs for Possible Modified Dysphagia Diet
Medical Diagnoses Coughing/Choking Poor PO Intake Dehydration Dehydration Unexplained weight loss Pocketing/holding food in the mouth Drooling/ Dry mouth Patient complaint of swallowing difficulties Poor dentition/edentulous
Clinical Dysphagia Evaluation
Presenting Swallowing Problem Medical History & Present Medical Status Interdisciplinary Team Evaluations Oral Phase of Swallowing Pharyngeal Phase of Swallowing Cervical Esophageal Phase of Swallowing Dysphagia Diet Level
6
Implementation of an Oral Feeding Program
Speech Pathologist determines dysphagia diet level, swallowing strategies & advancing diet.
Dietician determines nutritional needs.OT d t i h i l & d ti i t OT determines physical & adaptive equipment needs & self feeding needs.
PT determines physical needs & positioning. Food service determines food likes/dislikes. Nursing determines medical & ADL needs. Physician oversees & approves treatment plans.
1.
9.
8.
1.
3.
2.
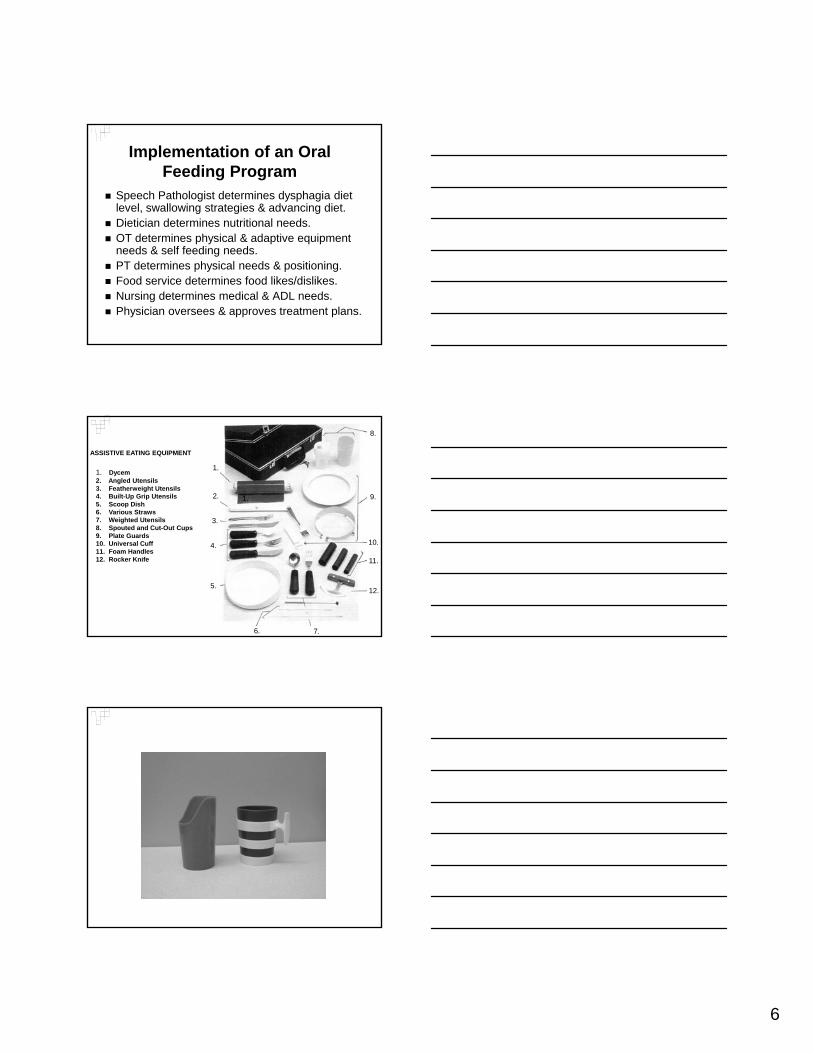
1. Dycem2. Angled Utensils3. Featherweight Utensils4. Built-Up Grip Utensils5. Scoop Dish6. Various Straws7. Weighted Utensils8 S t d d C t O t C
ASSISTIVE EATING EQUIPMENT
5.
11.
10.
12.
4.
7.6.
8. Spouted and Cut-Out Cups9. Plate Guards10. Universal Cuff11. Foam Handles12. Rocker Knife

7
Implementation of an Oral Feeding Program
Speech Pathologist determines dysphagia diet level, swallowing strategies & advancing diet.
Dietician determines nutritional needs.OT d t i h i l & d ti i t OT determines physical & adaptive equipment needs & self feeding needs.
PT determines physical needs & positioning. Food service determines food likes/dislikes. Nursing determines medical & ADL needs. Physician oversees & approves treatment plans.
8
Considerations for the Specific Dysphagia Patient
Psychosocial Issues Fatigue Level Positioning/Seating Environment (auditory visual) Environment (auditory, visual) Group vs. Individual Pain/medical status Oral status (dry mouth, poor dentition) Length of time to eat a meal Staff /Family Attitudes
Psychosocial Issues
Loss of independence
Loss of significant other/familyg y
Social isolation
Economic hardships
Depression
Considerations for the Specific Dysphagia Patient
Psychosocial Issues Fatigue Level Positioning/Seating Environment (auditory visual) Environment (auditory, visual) Group vs. Individual Pain/medical status Oral status (dry mouth, poor dentition) Length of time to eat a meal Staff /Family Attitudes

9
Considerations for the Specific Dysphagia Patient
Fatigue level Psychosocial Issues Positioning/Seating Environment (auditory visual) Environment (auditory, visual) Group vs. Individual Pain/medical status Oral status (dry mouth, poor dentition) Length of time to eat a meal Staff /Family Attitudes
10
Considerations for the Specific Dysphagia Patient
Fatigue level Psychosocial Issues Positioning/Seating Environment (auditory visual) Environment (auditory, visual) Group vs. Individual Pain/medical status Oral status (dry mouth, poor dentition) Length of time to eat a meal Staff /Family Attitudes
11
Dysphagia Diet LevelsFoods
Level 1: Puree, pudding/applesauce consistency, soft blended foods with no “pieces/bits” of food. Bolus easy to maintain & p yno chewing.Level 2: Cottage Cheese, scrambled eggs, macaroni & cheese. Soft foods with bolus easy to maintain. Requires slight chewing.

12
Dysphagia Diet LevelsFoods
Level 1: Puree, baby food consistency, soft blended foods with no “pieces/bits” of food. Bolus easy to maintain & no chewingBolus easy to maintain & no chewing.
Level 2: Cottage Cheese, scrambled eggs, macaroni & cheese. Soft foods with bolus easy to maintain. Requires slight chewing.
13
Dysphagia Diet LevelsFoods
Diet Level 3: Minced/chopped meats, casseroles, canned fruits, cooked vegetables, soft breads. Solids requiring
h isome chewing. Diet Level 4/Regular diet: Allows raw
fruits/vegetables, all meats, all breads, nuts. Requires chewing & swallowing WFL.
14
Dysphagia Diet LevelsLiquids
Honey consistency: Thick consistency. Pours like honey, milkshake thickness.
Nectar consistency: Medium consistency Nectar consistency: Medium consistency. Pours like tomato juice, cream soups, buttermilk thickness.
Thin consistency: Thin consistency. Pours like water, popsicles, broth, water thickness.
15

16
Dysphagia Diet LevelsLiquids
Honey consistency: Thick consistency. Pours like honey, milkshake thickness.
Nectar consistency: Medium consistency Nectar consistency: Medium consistency. Pours like tomato juice, cream soups, buttermilk thickness.
Thin consistency: Thin consistency. Pours like water, popsicles, broth, water thickness.
17
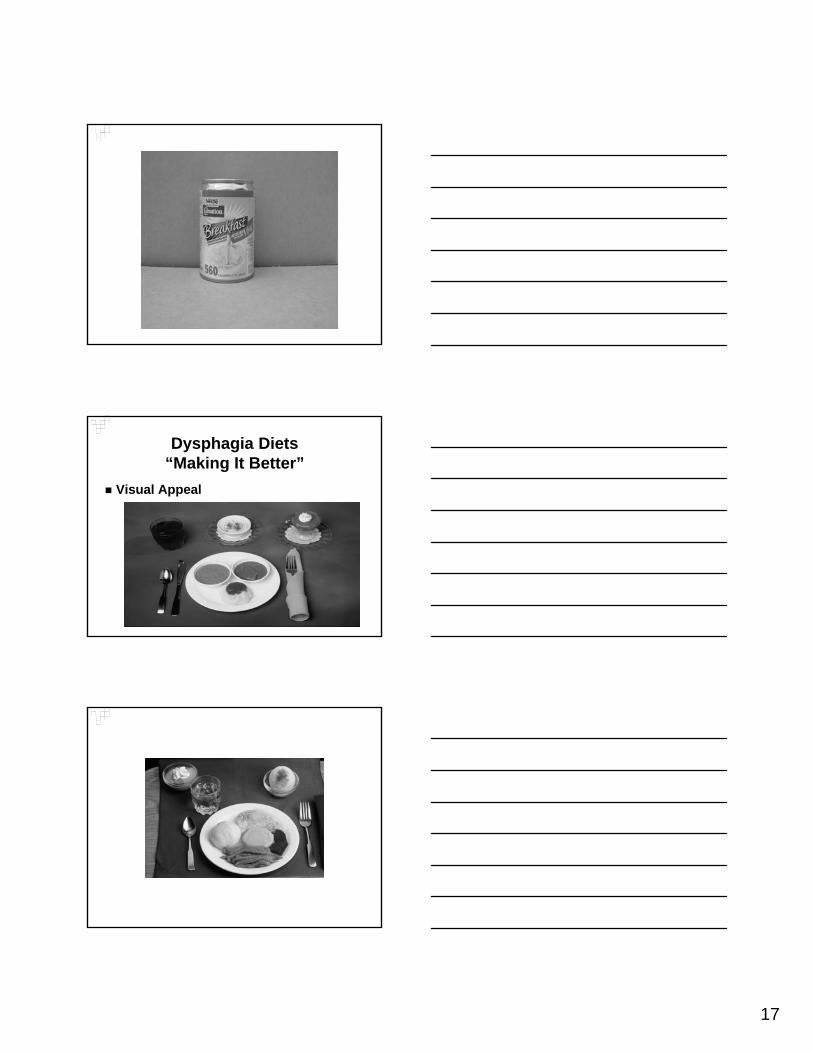
Dysphagia Diets“Making It Better”
Visual Appeal
18
Dysphagia Diets“Making It Better”
Free Water Protocol/Frazier Water Protocol-Water between meals.Water between meals.
-No thin liquids with food and/or meds.
-No water 30 minutes before or after meal.
Dysphagia Diets“Making It Better”
Tastes/Flavors-Ketchup -Mayonnaise/Salad Dressings-Hot Sauce/Taco -Pizza SauceH /S D S i Mi-Honey/Syrup -Dry Seasoning Mixes
-Sour Cream -Horseradish Sauce-Soy Sauce -Gravy-Steak Sauce -Soft Cream Cheese-Mustards -Barbecue Sauce-Cheese Sauces -Ice Cream Toppings
19
Dysphagia Diets“Making It Better”
Purees/Grocery Shopping-Ham, chicken, potted meat spreads-Smooth bean dip-Applesaucepp-Pie fillings/custards/jello/pudding cups-Jelly/Fruit spreads-Mashed Potatoes-Cereals/Oatmeal/Grits-Cheese Spreads/Sauces-Yogurts
Dysphagia Diets“Making It Better”
Thickened Liquids/Grocery Shopping-Magic Cups-Smoothies-Lattes-Buttermilk-Nectars-Tomato Juice-Vegetable Juice-Added flavorings-Carbonation-Smoothies/Milkshakes-Egg Nog/Custards-Lattes
20
Dysphagia Food Preparation Tips
Meats, sauces, gravies and/or broths should be warm when blending.
Save liquids from canned fruits/vegetables to use if need to thin a puree consistency.Add ll f hi k if b Add small amounts of thickener if purees become too thin.
Use cake decorating tips and tubes to make puree foods more visually appealing.
Cook casseroles. Puree finished casserole. Puree peas, corn, beans & strain out husks. Frozen dinners can be thawed, pureed and refrozen.

21
22
Dysphagia Diets“Making It Better”
Slurry (Pureed bakery foods) Slurry Recipe
-1 Tablespoon commercial thickener-2 Cups Water
-Remove hard surfaces. Use a fork /toothpick, pierce the baked product. More holes allows more absorption of the thickener. Put the bakery item in a serving dish/pan. Pour the mixture over the food making sure it is saturated. Cover & sit in frig for 2 hours. Remove excess liquid on & around the food.
Dysphagia Diets“Making It Better”
Pasta Recipe (8 servings) -4 Cups well cooked pasta-1/2 Cup non-fat milk powder-1/3 Cup oil/melted margarine-8 Tablespoons Parmesan cheese-1 Teaspoon garlic powderSoak cooked pasta in cold water for 30 min. Drain. Combine
pasta, milk powder, oil & water in food processor & blend until smooth/creamy. Add water gradually & continue to blend until the mixture resembles thick muffin batter. Blend in Parmesan cheese & garlic powder. Use icing tips to make noodles or spread in casserole.
Dysphagia Diets“Making It Better”
Sloppy Joe Recipe-1/2 lb. ground meat-1 tsp. onion powder-1/2 C water-1/2 C. water
Brown meat & onion powder in a skillet. Add barbecue sauce & ½ C. water. Simmer 20 minutes
or until meat is tender/soft.Puree mixture in food processor until smooth. Add
thickener or liquid to thicken or thin to correct consistency.

23
Dysphagia Diets“Making It Better”
Green Bean Au Gratin Recipe-1 can cut green beans/french style beans-1 can condensed cream of mushroom soup1 can condensed cream of mushroom soup-1/4 C. grated sharp cheese Drain green beans & save liquid. Puree
warm green beans & warm soup. Add grated cheese. Thin mixture with warm liquid as needed. Place in casserole dish. Cook at 350 degrees until hot.
Dysphagia Diets“Making It Better”
Apple Dessert-1 ½ C. peeled sliced apples-1 C. plain yogurt-1/2 tsp. vanilla-1/4 tsp. cinnamon-1 tsp. brown sugar (optional)Cook apples in ¼ C. water until very soft.
Combine cooked apples with remaining ingredients. Puree/blend until smooth. Garnish withwhipped topping (optional).
Thank You
-Audience
-SpeechPathology.com
24
References
American Dietetic Association. “ National Dysphagia Diet: Standardization for Optimal Care.” National Dysphagia Diet Task Force. (Google)
Beare, P.G., & Myers, J.L. (1998). Adult Health Nursing. St. Louis: Mosby.Caruso, A.J. & Mueller, P.B. (1997). “Age-Related Changes in Speech, Voice
and Swallowing.” Aging and Communication: By Clinicians for Clinicians. Pp. 117-134.
Gleeson DCL: “Oropharyngeal Swallowing & Aging: A Review ” JGleeson DCL: Oropharyngeal Swallowing & Aging: A Review. J. Communication Disorders, 32, 373-396, 1999.
Groher, M. (1992). Dysphagia: Diagnosis and Management. Boston: Butterworth-Heinemann.
Logemann, Jeri A. (1998). Evaluation and Treatment of Swallowing Disorders. Austin, Texas: Pro-ed, Inc.
Panther, Kathy: “The Frazier Free Water Protocol.” Swallow and Swallowing Disorders March 2005
References
Robbins, J. & Hamilton, J.W. “Oropharyngeal Swallowing In Normal Adults of Different Ages.” Gastroenterology. 1992; 103: 823-829.
Robbins, JA: “Old Swallowing & Dysphagia.” Nut Clin Prac, 14,S21-S26, 1999.
Robbins JA Levine R Wood J Roecker EB Luschei E 1995 “AgeRobbins, JA, Levine R, Wood J Roecker EB, Luschei E, 1995. Age Effects on lingual pressure generation as a risk factor for dysphagia.” J Geron 50, M257-M262.
Shaker, R. “Effect of Aging on the Deglutitive Oral, Pharyngeal and Esophageal Motor Function.” Dysphagia. 1994; 9: 221-228.
Shaker, R. “Esophageal Disorders in the Elderly.” Gastroenterology Clinics of North America. Philadelphia, PA: WB Saunders, Co, 2001:335.
Website References and Commercial Products
American Speech Language & Hearing Associationwww.asha.org
American Dietetic Association. “ National Dysphagia Diet: Standardization for Optimal Care.” National Dysphagia Diet Task ForceDiet Task Force.
Dysphagia-Diet. www.dysphagia-diet.com 800-6333438 NeuroDevelopmental Treatment Association, Inc.
www.ndta.orgHormel Health Labs www.hormelhealthlabs.comNovartis Nestle Resources. www.resourcethickenupSysco Foods. www.sysco.com