welcome to ward 30 (neurology) - northumbria university · pdf filewelcome to ward 43 ... ward...
TRANSCRIPT

Student’s Name_______________________
Welcome to Ward 43
Neuromedicine
Neuroscience Directorate
Royal Victoria Infirmary

Added to Practice Placements, Northumbria University Website July 2012 2
This is your information pack please look after it
We hope that you find this helpful as you begin your placement on our ward.
The ward telephone number is 0191 282 6043
A useful website which outlines neurological conditions (without
overwhelming you with information) can be found at www.ninds.nih.gov.
The ward also has some patient information leaflets and text books that you
may find helpful, please ask your mentor about these.
Ward Checklist Try to get this completed shortly after you start your placement
Fire Safety Signature
of mentor
Shown location of fire extinguishers and fire panel
Action to be taken on hearing the fire alarm explained
Action to be taken on discovering a fire
Shown location on of assembly point
Evacuation procedure explained
Hand washing
Given hand washing techniques.
Observed correctly washing hands
Computers
Shown how to access the Intranet
Shown how to access policies and procedures
Multi-disciplinary team (where possible)
Opportunity to work with a qualified dietician.
Opportunity to work with OT.
Opportunity to work with physiotherapists.

Added to Practice Placements, Northumbria University Website July 2012 3
The Newcastle upon Tyne Hospitals NHS Foundation Trust
Ward 43 Royal Victoria Infirmary
Ward Profile
Ward 43 is a Neuromedical Ward comprising of 23 in patient beds and 6 day
case facilities. The ward is part of the Neuroscience Directorate.
The Senior Ward Sister is Eve Garside.
Ward 43 welcomes student nurses at all stages of their nurse training and aims
to provide an excellent and interesting learning environment.
A mentor will be allocated prior to you commencing your placement.
The shift times are:
Early 07.30 - 15.45
Late 12.30 - 20.30
Long Day 07.30 – 20.30
Night Duty 20.00 - 08.00
Ward 43 cares for a wide variety of patients; who have neurological
conditions such as Multiple Sclerosis, Parkinson’s Disease and Motor Neurone
Disease. Many patients will be given a new diagnosis which is potentially
debilitating and as such will require a great deal of emotional support. There
are other patients suffering from chronic conditions who are well known to the
ward staff and in some instances patients are admitted for terminal care.
There are many Consultants who work within the ward, all of whom have a
special area of neurological interest. The nursing staff work towards achieving
the ward philosophy and strive to offer a high standard of quality care to
patients with neurological conditions.
The nursing model used on Ward 43 (and across the Trust) is Essence of Care,
based around the original 9 elements (communication; continence, bowel
and bladder care; nutrition; pressure ulcers; personal and oral hygiene;
privacy and dignity; record keeping; safety and self care). Team nursing is
practiced on the ward and opportunities are provided to observe a number
of neurological investigations.
Ward 43 provides an excellent opportunity for students to appreciate the
effect a chronic illness can have upon a person and their carers and
therefore works closely with all members of the multi-disciplinary team.
Emergency telephone numbers are:
Cardiac Arrest 2222
Security 25704 (for routine enquiries)
Fire/Security 333 or 399 (for emergencies)
The resuscitation trolley is situated at the bottom of the main corridor.

Added to Practice Placements, Northumbria University Website July 2012 4
Profile of Learning Opportunities

Added to Practice Placements, Northumbria University Website July 2012 5
L
Ward 43
ITU Outreach
PEG Team
Social Worker
Chaplaincy
Epilepsy Nurse Specialist
Home Ventilation Team
MND Nurse Specialist
Tissue Viability
Nurse Consultant
Diabetic Team
Patient Services Co-ordinators
Dietician Physiotherapist
Neuro-Investigation Unit
MS Specialist Nurse
Speech and
Language Therapist
Continence Nurse
Consultant
Palliative Care Team
Occupational Therapist Link Nurses PD Nurse Specialist
District Hospitals
UNN
Social Services
Community Continence Advisors
MS Support Team Community Physiotherapist
Carers
GP’s
Community OT
District Nurses Macmillan Nurses
Hospices
Ambulance Service
Added to Practice Placements, Northumbria University Website July 2012 6
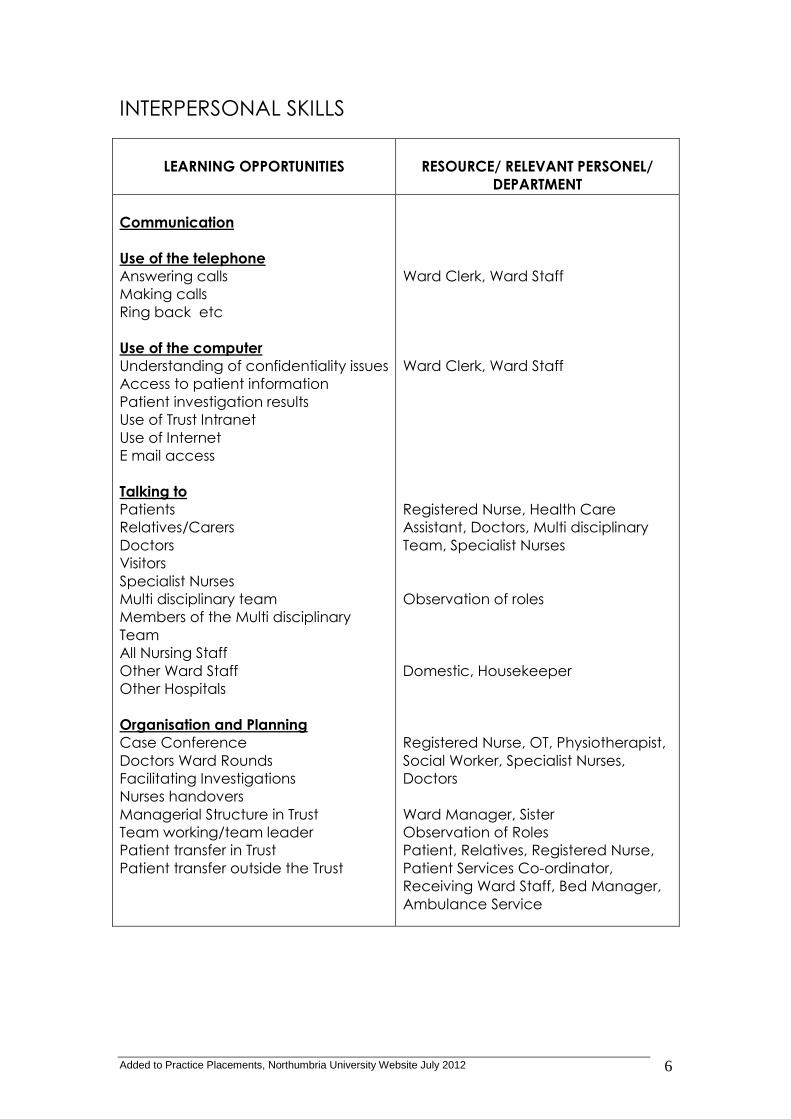
INTERPERSONAL SKILLS
LEARNING OPPORTUNITIES
RESOURCE/ RELEVANT PERSONEL/
DEPARTMENT
Communication
Use of the telephone
Answering calls
Making calls
Ring back etc
Use of the computer
Understanding of confidentiality issues
Access to patient information
Patient investigation results
Use of Trust Intranet
Use of Internet
E mail access
Talking to
Patients
Relatives/Carers
Doctors
Visitors
Specialist Nurses
Multi disciplinary team
Members of the Multi disciplinary
Team
All Nursing Staff
Other Ward Staff
Other Hospitals
Organisation and Planning
Case Conference
Doctors Ward Rounds
Facilitating Investigations
Nurses handovers
Managerial Structure in Trust
Team working/team leader
Patient transfer in Trust
Patient transfer outside the Trust
Ward Clerk, Ward Staff
Ward Clerk, Ward Staff
Registered Nurse, Health Care
Assistant, Doctors, Multi disciplinary
Team, Specialist Nurses
Observation of roles
Domestic, Housekeeper
Registered Nurse, OT, Physiotherapist,
Social Worker, Specialist Nurses,
Doctors
Ward Manager, Sister
Observation of Roles
Patient, Relatives, Registered Nurse,
Patient Services Co-ordinator,
Receiving Ward Staff, Bed Manager,
Ambulance Service

Added to Practice Placements, Northumbria University Website July 2012 7
CLINICAL SKILLS
LEARNING OPPORTUNITIES
RESOURCE/ RELEVANT PERSONEL/
DEPARTMENT
Patient hygiene
Bathing and Dressing
Mouth Care
Hair/Nail Care
Skin Care
Pressure care prevention
(Braden Scale)
Maintaining Privacy and Dignity
Promoting Independence
Recording of Physiological
Observations
Blood Pressure
Temperature, Pulse and Respirations
Weight
Oxygen Saturations
Blood Glucose
Forced Vital Capacity
Urine output
Maintaining Accurate Charts
Administration of Medication
Oral
Intramuscular
Subcutaneous
Rectal
Intravenous Drugs
Intravenous infusions
Miscellaneous
Cannulation/care of venflons
Medical Devices
Administration of blood and blood
products
Aseptic Non Touch Techniques
e.g. dressings
Risk Assessment
Body Mass Index
Use of aids/hoists
Infection control
Isolation of patients/Barrier Nursing
Catheter insertion and care
Management of incontinence
Urinalysis
CVP lines
Patient safety/falls.
Checking equipment
Tracheostomy Care
Staff Nurse, Health Care Assistant
Registered Nurse, Health Care
Assistant, Doctor,
Diabetic Specialist Nurse
Registered Nurse, Doctor, Pharmacist
Sister, Registered Nurse, Doctor
Registered Nurse, Home Ventilation

Added to Practice Placements, Northumbria University Website July 2012 8
Non Invasive Ventilation
Insertion and care of PEG feeding
Tube
NG Tube management and feeding
Infection Control
Preparation for Investigations
Consent (informed)
Information – both verbal and written
Invasive radiology
Non-invasive radiology
Team,
PEG Team, Dietician
Sister, Registered Nurse,
Infection Control Team
HEALTH DEVELOPMENT OPPORTUNITIES
LEARNING OPPORTUNITIES
RESOURCE/ RELEVEANT PERSONEL/
DEPARTMENT
Healthy life style strategies in relation
to
Smoking cessation
Obesity
Diabetes
Health education and health
promotion literature
Sister, Registered Nurse, Doctor,
Smoking Cessation Service
Dietician
Diabetes Nurse Specialist
Ward Resources, Specialist Nurses
MANAGEMENT OF CARE

Added to Practice Placements, Northumbria University Website July 2012 9
LEARNING OPPORTUNITIES
RESOURCE/ RELEVANT PERSONEL/
DEPARTMENT
Nursing process
Assessment
Use of Trust Documentation
Use of Nursing Model
Philosophy of Care
Relevance of Information
Collection of Information
Observation
Practice
Risk Assessment Tools
Planning Care
Care plans
Core Care Plans
Evaluation of Care
Discharge planning
Multi-disciplinary plan/working
OT
Physiotherapist
Social Worker
District Nurse
Discharge liaison
Specialist nurses
Relevant departments
Implementation / Evaluation
Ward rounds
Multi-disiplinary Team
Patient and Carer Involvement
Documentation
Standards
Protocols, Policies
Communication/ relatives/patient
Time management
Planning priorities
Dealing with difficult situations
Deceased patients
Patient property/Valuables
Self discharge
Religious Needs
Registered Nurse
Medical Notes
Patients, Carers
Community Staff
Registered Nurse, Social Worker, OT,
Physiotherapist, Doctors, Patient,
Carers
Registered Nurse, Social Worker OT,
Physiotherapist, Doctors, Patient,
Carers
Royal Marsden Handbook, Hospital
Intranet Policies and Procedures
Hospital chaplaincy

Added to Practice Placements, Northumbria University Website July 2012 10
ORGANISATIONAL AND MANAGERIAL ISSUES
LEARNING OPPORTUNITIES
RESOURCE/ RELEVANT PERSONAL/
DEPARTMENT
Organisational Skills
Delegation
Role of the Ward Co-ordinator
Role of the Team leader
Standards of care
Quality Issues
Off duty
Time management
Managing patient work load
Management of Ward/Resources
Stock control
Ordering Drugs
Ward Sisters Responsibilities
Materials management
Managing Risk
Policies and Procedures
Equipment safety checks
Quality control
Weekly environment checks
Infection Control
Moving and Handling
Emergency Situations
Cardiac arrest
Violent Incidents, Security
Fire
Bed alerts
Patient falls
Staff Development
Clinical supervision
Reflective practice
Sister, Registered Nurse
Sister, Registered Nurse
Trust Intranet
Sister, Registered Nurse
Sister, Registered Nurse
Sister, Registered Nurse

Added to Practice Placements, Northumbria University Website July 2012 11
NEUROLOGICAL DISORDERS
LEARNING OPPORTUNITIES
RESOURCE/ RELEVANT PERSONEL/
DEPARTMENT
Knowledge Nursing care of Patients
with :
Multiple Sclerosis
Parkinson’s Disease
Motor Neurone Disease
Chronic and Acute Neuropathy
Guillan Barre Syndrome
Epilepsy
Encephalitis
Creutzfeid Jakob Disease
Meningitis
Mysthenia Gravis
Headaches
Mitocondrial Disorders
Observation and Assistance with: (if
applicable)
Magnetic Resonance Imaging (MRI)
Computerised Axial Tomography (CT)
Electroencephalograph (EEG)
Electromyography (EMG’s)
Evoked Potentials (EP’s)
Visual Evoked Responses (VEP’s)
Muscle Biposy
Neuropsychometery
Addenbrookes Assessment
Neurological Observations
Patient Information Leaflets, Text
Books, Internet (www.ninds.gov.uk)
Sister, Registered Nurse, Doctor,
Specialist Nurses
Radiology
Neurophysiology
Theatre
Doctor
Registered Nurse

Added to Practice Placements, Northumbria University Website July 2012 12
Learning Opportunities within the MDT
S/N J Kane
Name Date
Neuro Theatre
– spinal surgery
– brain surgery
– intubation/anaesthetics
Neuro x-ray
- angiogram
- MRI
Neurophysiology
- EMG
- EEG
Physiotherapist
Dietitian
Occupational Therapist
Speech Therapist
Outreach Team
Pain Team
Palliative Care Team
Parkinsons Disease Specialist Nurse
MS Specialist Nurse
MND Specialist Nurse
Epilepsy Specialist Nurse
Head Injury Specialist Nurse
Neuro Oncology Specialist Nurse
Added to Practice Placements, Northumbria University Website July 2012 13
Ward Philosophy
Ward 43 RVI
Our ward aim is to provide the best possible quality of care and support for
our patients, relatives and carers to help them to reach their full potential in
spite of any disability.
We also aim for our nursing staff to achieve job satisfaction and have the
opportunity to work within the Multi-Disciplinary Team in reaching our ultimate
goal of providing high quality, evidence based practice in looking after our
patients.
Ward 43 is recognised as being a Practice Development Unit, promoting a
pro-active environment, delivering high standards of holistic care where
everyone’s opinions are valued and respected.
Finally our staff endeavours to provide a friendly and professional atmosphere
in which patients and visitors will feel able to approach staff with any queries
and concerns. Maintaining good relationships between staff, patients and
visitors is essential in meeting our ultimate goal of providing the best quality of
care for patients.

Added to Practice Placements, Northumbria University Website July 2012 14
List of Agreed Abbreviations
(taken from The Newcastle upon Tyne Hospitals NHS Foundation Trust
Clinical Record Keeping Policy November 2010)
Common Medical Conditions
AIDS Acquired Immunodeficiency Syndrome
Ca Cancer
CCF Congestive Cardiac Failure
COAD Chronic Obstructive Airways Disease
DVT Deep Vein Thrombosis
MI Myocardial Infarction
MRSA Methicillin Resistant Staphylococcus Aureus
PE Pulmonary Embolus
STAPH Staphylococcus
TB Tuberculosis
UTI Urinary Tract Infection
# Fracture
Patient Investigation (Radiology)
AxR Abdominal X-Ray
Ba Barium
CT SCAN Computerised Tomography
CXR Chest X-Ray
MRI Magnetic Resonance Imaging
U/S Ultrasound
Common Tests/Procedures
CPR Cardio Pulmonary Resuscitation
PEG Percutaneous Endoscopic Gastroscopy
TENS Trans Cutaneous Electro Nerve Stimulation
TPN Total Parenteral Nutrition
TPR Temperature Pulse Respiration
Medication/Drugs
IM Intra Muscular
Inh Inhaler
IV Intravenous
Neb Nebulisation
Oral
PO By Mouth
PR Per Rectum
PV Per Vagina
SC Sub Cutaneous
S/L Sub Lingual
Top Topical
CD Controlled Drug
IVI Intravenous Infusion
TTO To Take Home (Drugs)

Added to Practice Placements, Northumbria University Website July 2012 15
Administration
Appt Appointment
ASAP As Soon As Possible
DNA Did Not Attend
DOB Date Of Birth
FU Follow Up
S/A Same Address
S/B Seen By
TCI To Come In
Equipment
ET Tube Endotracheal Tube
NGT Naso Gastric Tube
TED Thrombo Embolic Deterrents
People
CPN Community Psychiatric Nurse
Dr Doctor
F (1 or 2) Foundation trainee (year 1 or 2)
GP General Practitioner
HV Health Visitor
ST(n) Specialist Trainee (n= year of training)
SALT Speech And Language Therapist
SR Sister
S/N Staff Nurse
ST/N Student Nurse
Specialty
ENT Ear Nose and Throat
GI Gastro Intestinal
GYNAE Gynaecology
HDU High Dependency Unit
OPD Out Patients Department
OT Occupational Therapy
PAEDS Paediatrics
Patient Investigation (Blood)
FBC Full Blood Count
FFP Fresh Frozen Plasma
HB Haemoglobin
K Potassium
Na Sodium
PCV Packed Cell Volume
U/E Urea and Electrolytes
WCC White Cell Count

Added to Practice Placements, Northumbria University Website July 2012 16
Patient Assessment/ Examination
BMI Body Mass Index
BP Blood Pressure
CNS Central Nervous System
CVP Central Venous Pressure
H/O History of
Ht Height
ICP Intracranial Pressure
NAD No Abnormality Detected
NBI No Bony Injuries
NOK Next Of Kin
PMH Past Medical History
SOB Shortness Of Breath
TPR Temperature Pulse Respirations
Wt Weight
Patient Investigation (General)
C&S Culture And Sensitivity
CSF Cerebro-Spinal Fluid
ECG Electro Cardiogram
LP Lumbar Puncture
MC&S Microscopy Culture And Sensitivity
MSU Mid Stream Urine
Other
LA Local Anaesthetic
GA General Anaesthetic
NBM Nil By Mouth
POST OP After Operation
PRE OP Before Operation
RTA Road Traffic Accident
ROS Removal Of Sutures

Added to Practice Placements, Northumbria University Website July 2012 17
Neuroscience Abbreviations
(That you may see in documentation)
Medical/Surgical Conditions
A.C.D.F. Anterior Cervical Discectomy and Fusion
A.V.M. Arterio-Venous Malformation
C.V.A. Cerebro-Vascular Accident
E.D.H. Extra-Dural Haematoma
G.B.M. Glioblastoma Multiforma
I.C.H. Intra-Cerebral Haematoma
S.A.H. Subarachnoid Haemorrhage
S.D.H Sub-dural Haematoma
S.O.L. Space Occupying Lesion
T.I.A. Transient Ischaemic Attack
C.I.D.P. Chronic Inflammatory Demylinating Polyneuropathy
M.N.D. Motor Neurone Disease
M.S. Multiple Sclerosis
Procedures and Investigations
C.V.P Central Venous Pressure
E.E.G. Electro-encephlogram
E.M.G. Electro-myography
E.V.D. External Ventricular Drain
G.C.S Glasgow Coma Scale
I.C.P. Inter-cranial Pressure
L.P. shunt Lumbar-peritoneal Shunt
M.A.P. Mean Arterial Pressure
P.E.A.R.L Pupils equal and reacting to light
RESPS Respirations
V.P. shunt Ventriculo-peritoneal shunt
Bx Biposy
E.P. Evoked Potentials
I.V.I.G. Intra-venous Immunoglobulin
M.D.T. Multi-disiplinary Team

Added to Practice Placements, Northumbria University Website July 2012 18
Investigations
C.T. Scan (Computerised Tomography)
This scan is carried out using x-rays alone (although an IV injection of a
contrast medium may often be used to clarify even further the pictures
obtained. X-rays are shone through the skull (or spinal column) on a series of
different planes and a computer analyses the results and produces
extraordinarily clear pictures of the skull, brain tissues, ventricles, subarachnoid
space and any abnormalities present in a very short period of time and with
no discomfort to the patient other than having to lie still.
M.R.I (Magnetic Resonance Imaging)
Even for C.T. scanning however there are some areas of the brain (posterior
fossa) which are difficult to illustrate. By exposing the patient’s head to a
powerful, but entirely safe, magnetic field, computers can again reproduce
an image of the skull, brain, CSF pathways and any lesions present in a very
clear picture and on different planes – i.e. as if looking at the brain from the
side. Some lesions show up by this method, which do not clearly show on C.T.
scanning and this applies particularly to the plaques of Multiple Sclerosis. It
can also be applied to muscular disease.
E.E.G. (Electro-encephlogram)
The living brain is constantly discharging small electrical waves, which can be
picked up from the surface of the head, magnified and recorded on paper.
The machine which does this is called an elecroencephalograph, and the
tracing it produces is called an electroencephalogram. Little electrodes are
held onto the scalp and spaced out over the whole skull. These are
connected to the recording pens and the controls of the machine allow
tracings to be made on the moving paper from a combination of these
electrodes.
E.M.G (Electro-myography)
The E.M.G. records electrical discharges given off in muscle fibres. Normally
there are none at rest but they become profuse when the muscle contracts.
Fine electrodes are either attached to the skin or introduced into the muscle
itself and the waves are seen on a little television screen and at the same
time photographed on the moving film so that they can be studied later. By
different wave patterns the E.M.G. helps to distinguish between the muscle
that is weak and wasted because its nerve supply is damaged, i.e. it is
denervated, and one whose disease is in the muscle itself, e.g. Muscular
Dystrophy. It can also be used to measure the speed with which an electrical
stimulus travels from some point on the nerve to the muscle that that nerve
supplies. It is called the nerve conduction time and the nerve conduction
velocity can also be measured. These may be delayed by nerve damage to
the nerve along its course.

Added to Practice Placements, Northumbria University Website July 2012 19
L.P. (Lumbar Puncture)
Some neurological diseases produce clear-cut changes in the C.S.F. of great
value in diagnosis. In many others unfortunately the changes are too vague
to be helpful. The fluid can be obtained by L.P. Because the meninges run
further down the vertebral canal than does the cord itself, a sac containing
C.S.F. is formed in the lumbar region into which a needle can be passed and
fluid withdrawn, or substances injected, without damaging the cord.
Normally the patient is positioned to lie on one side, with the back right at the
edge of the bed and not leaning forwards. In order to separate the vertebral
spines, the head and neck are flexed and the knees are brought upwards
towards the chin. Heavy blood staining occurs if blood was already in the
C.S.F. (e.g. in Sub-arachnoid Haemorrage, or if a large vessel beyond the
theca is entered. C.S.F. pressure is measured by connecting a manometer to
the needle. The C.S.F. rises normally to a pressure of 100-150mm (of C.S.F.).
L/P. should not be performed if intracranial pressure is suspected.
E.P. (Evoked Potentials)
Using an electrode on the scalp the time taken for visual, auditory and
sensory stimulus to produce discharge in the brain. This is measured and if
delayed compared to normal this may mean a lesion in the pathways under
examination. For instance, if a patient’s only complaint is dragging the left
foot one may suspect Multiple Sclerosis. The demonstration of Visual Evoked
Potentials of a lesion in the left optic nerve would be evidence of more than
one lesion in the nervous system.
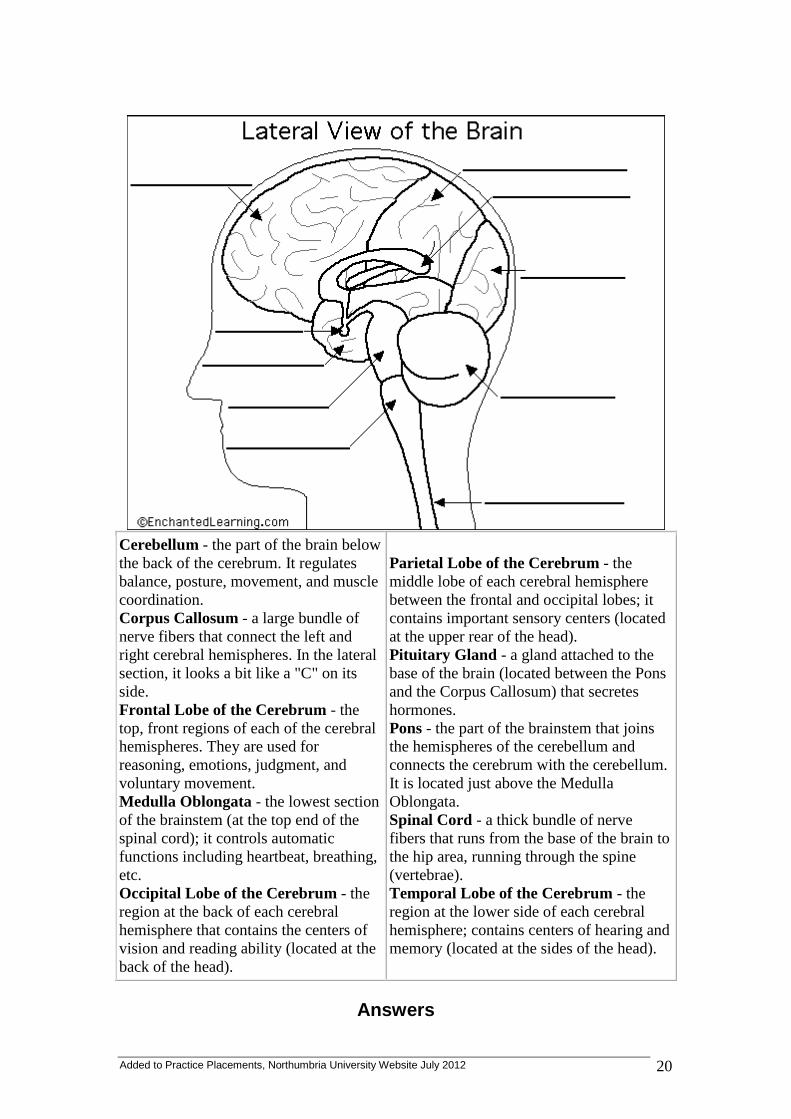
Read the definitions below, then label the brain anatomy diagram.
Added to Practice Placements, Northumbria University Website July 2012 20
Cerebellum - the part of the brain below
the back of the cerebrum. It regulates
balance, posture, movement, and muscle
coordination.
Corpus Callosum - a large bundle of
nerve fibers that connect the left and
right cerebral hemispheres. In the lateral
section, it looks a bit like a "C" on its
side.
Frontal Lobe of the Cerebrum - the
top, front regions of each of the cerebral
hemispheres. They are used for
reasoning, emotions, judgment, and
voluntary movement.
Medulla Oblongata - the lowest section
of the brainstem (at the top end of the
spinal cord); it controls automatic
functions including heartbeat, breathing,
etc.
Occipital Lobe of the Cerebrum - the
region at the back of each cerebral
hemisphere that contains the centers of
vision and reading ability (located at the
back of the head).
Parietal Lobe of the Cerebrum - the
middle lobe of each cerebral hemisphere
between the frontal and occipital lobes; it
contains important sensory centers (located
at the upper rear of the head).
Pituitary Gland - a gland attached to the
base of the brain (located between the Pons
and the Corpus Callosum) that secretes
hormones.
Pons - the part of the brainstem that joins
the hemispheres of the cerebellum and
connects the cerebrum with the cerebellum.
It is located just above the Medulla
Oblongata.
Spinal Cord - a thick bundle of nerve
fibers that runs from the base of the brain to
the hip area, running through the spine
(vertebrae).
Temporal Lobe of the Cerebrum - the
region at the lower side of each cerebral
hemisphere; contains centers of hearing and
memory (located at the sides of the head).
Answers

Added to Practice Placements, Northumbria University Website July 2012 21
Cerebellum - the part of the brain below
the back of the cerebrum. It regulates
balance, posture, movement, and muscle
coordination.
Corpus Callosum - a large bundle of
nerve fibers that connect the left and
right cerebral hemispheres. In the lateral
section, it looks a bit like a "C" on its
side.
Frontal Lobe of the Cerebrum - the
top, front regions of each of the cerebral
hemispheres. They are used for
reasoning, emotions, judgment, and
voluntary movement.
Medulla Oblongata - the lowest section
of the brainstem (at the top end of the
spinal cord); it controls automatic
functions including heartbeat, breathing,
etc.
Occipital Lobe of the Cerebrum - the
region at the back of each cerebral
hemisphere that contains the centers of
vision and reading ability (located at the
back of the head).
Parietal Lobe of the Cerebrum - the
middle lobe of each cerebral hemisphere
between the frontal and occipital lobes; it
contains important sensory centers (located
at the upper rear of the head).
Pituitary Gland - a gland attached to the
base of the brain (located between the Pons
and the Corpus Callosum) that secretes
hormones.
Pons - the part of the brainstem that joins
the hemispheres of the cerebellum and
connects the cerebrum with the cerebellum.
It is located just above the Medulla
Oblongata.
Spinal Cord - a thick bundle of nerve
fibers that runs from the base of the brain to
the hip area, running through the spine
(vertebrae).
Temporal Lobe of the Cerebrum - the
region at the lower side of each cerebral
hemisphere; contains centers of hearing and
memory (located at the sides of the head).

Added to Practice Placements, Northumbria University Website July 2012 22

Added to Practice Placements, Northumbria University Website July 2012 23
-30 sec 40-60
Staff Guidance for MRSA Patient Screening All patients who are to receive treatment from the Newcastle upon Tyne NHS Foundation Trust are screened for MRSA. This is a simple process involving swabs being taken from the nose, throat and perineum of all patients. Patients who have wounds and/or urinary catheters must have further relevant specimens taken. A full explanation must be given in all cases prior to commencement of the procedure. Privacy and dignity must be maintained at all time. All swabs must be labelled prior to use with the patient’s name, DOB, hospital number, ward and hospital. All accompanying documentation must have the aforementioned data as well as the named Consultant and clinical condition so that the laboratory is able to process the samples correctly. Specimens for screening must be labelled MRSA screen (If infection is a concern then request culture and sensitivity on the form as well). How to take the swabs Nose
Wash hands
Open the swab. Remove the container and twist off the plastic end.
Remove the swab without touching the cotton bud.
Place the cotton bud into one nostril and then the other touching the skin all around the inside of the resident’s nose.
Place the swab back into its container.
Throat
Wash hands
Open the swab. Remove the container and twist off the plastic end.
Remove the swab without touching the cotton bud.
Ask the patient to open their mouth wide and gently touch the back of their throat with the cotton bud until they gag.
Place the swab back into its container. * In paediatrics consider the age and feasibility of achieving a throat swab. Do not take unless achievable.
Remember to swab both
nostrils
Remember to swab the back of the throat
Added to Practice Placements, Northumbria University Website July 2012 24
Perineum *The perineum is the area of skin just in front of your anus or back passage. Allow the patient if able to complete this swab themselves. In paediatrics if inappropriate do not take perineum swab.
Wash hands
Open the swab. Remove the container and twist off the plastic end.
Remove the swab without touching the cotton bud.
Touch the perineum with the cotton bud.
Place the swab back into its container.
Wash hands. Wounds
Wash hands.
Put on disposable gloves and apron.
Remove the dressing and clean/irrigate the wound with normal saline as per local protocol and Trust aseptic technique (This will include de gloving at appropriate time, washing hands and donning new gloves.
Open the swab. Remove the container and twist off the plastic end.
Remove the swab without touching the cotton bud.
Touch the clean part of the wound and swab towards the dirty with the cotton bud in a zig-zag motion.
Place the swab back into its container.
Complete wound re dressing as per local protocol and Trust aseptic technique.
Wash hands. Collection of a catheter specimen of urine
Wash hands.
Put on disposable gloves and apron.
Clean the access point with 70% isopropyl alcohol impregnated swab and allow to dry thoroughly.
Do not break the closed system. Using a needless sampling port and following an aseptic technique insert the syringe firmly into the centre of the sampling port (following manufacturer’s instructions). Aspirate the required amount of urine and disconnect the syringe.
Clean access point with a swab saturated with 70% isopropyl alcohol.
Place the specimen in a sterile container.
Remove apron and gloves and wash hands. Record all information on swabs/specimens taken in appropriate documentation.
Gill Lishman March 2009