wellone primary medical care program for medical clinical staff diabetic foot screening click here...
TRANSCRIPT

WellOne Primary Medical CareProgram for Medical Clinical Staff
DIABETIC FOOT SCREENING
Click here to move on

Diabetes and Amputation
Diabetes is the cause of over 50% of all the non-traumatic amputations in the United States.
The risk of ulcers or amputations is increased in people who have had diabetes >10 years, are male, have poor glucose control, or have cardiovascular, retinal, or renal complications.
The loss of a lower extremity, or even part of a lower extremity, significantly impacts quality of life
Click here to move on
Click here to view
previous screen

True of False: Diabetes is the cause of over 50% of all the non-traumatic amputations in the United
States.
True
False
Click here to select this
answerClick here to select this
answer
Click here to view
previous screen

The correct answer is
TRUE
5-15% with diabetes will undergo amputation in lifetime
That’s up to 30 amputations in 200 patientsAbout 84,000 people with diabetes have lower
extremity amputations each year (Centers for Disease Control and
Prevention. Diabetes: disabling, deadly and on the rise, 2004..)
Click here to move on
Click here to view
previous screen

Diabetes and Amputation
Someone, somewhere, loses a leg because of diabetes every 30 seconds of everyday..."
- Lancet. 2005;366:1674
Click here to move on
Click here to view
previous screen

Risk Factors: Peripheral Neuropathy (PN)
High levels of glucose are toxic to the nerves
Peripheral neuropathy (PN) is damage to the nerves that connect the spinal cord to the arms and legs (the peripheral nerves)
PN is the # 1 risk factor for diabetic foot ulcer and amputation
Click here to move on
Click here to view
previous screen

True of False: Peripheral Neuropathy is the #1 risk factor for foot ulcer and amputation.
True
False
Click here to select this
answerClick here to select this
answer
Click here to view
previous screen

The correct answer is
TRUEAbout 60% to 70% of all people with diabetes will
eventually develop peripheral neuropathy, although not all suffer pain. This leads to painless trauma, ulceration, infection, and finally amputation.
Because of the lack of pain, the diabetic with neuropathy is prone to foot trauma/injury unawareness. A lack of pain when an ulcer is noted may lull the patient into a false sense of security, perceiving the ulcer to be of little or no significance. Thus, the patient may neglect and/or delay appropriate treatment for their problem.
Click here to move on
Click here to view
previous screen

PN: Symptoms
Symptoms can range from mild to severe and perhaps disabling.
Sometimes PN is present even without symptoms.
When people first get PN, they normally feel sensations like tingling, weakness, numbness, pinching, buzzing or stiffness in their toes and feet or fingers and hands.
As it gets worse, people report having a cramping, burning, throbbing or shooting pain.
Some refer to the pain as "frostbite", "pins and needles sticking in", "a lit match held to my foot" or "walking on broken glass". This could be so severe that wearing clothes or sleeping under blankets is painful.
Symptoms of PN vary from person to person. They can appear suddenly, come and go, or persist over time. They usually affect both sides of the body at the same time, and they may get worse at night.
When the nerves going into the feet are damaged, sensation is impaired
Normally pain is protective, letting us know there is a problem.
With PN there may be little to no pain when an injury has occurred Click here
to move on
Click here to view
previous screen

Peripheral Neuropathy
Click here to move on
Click here to view
previous screen
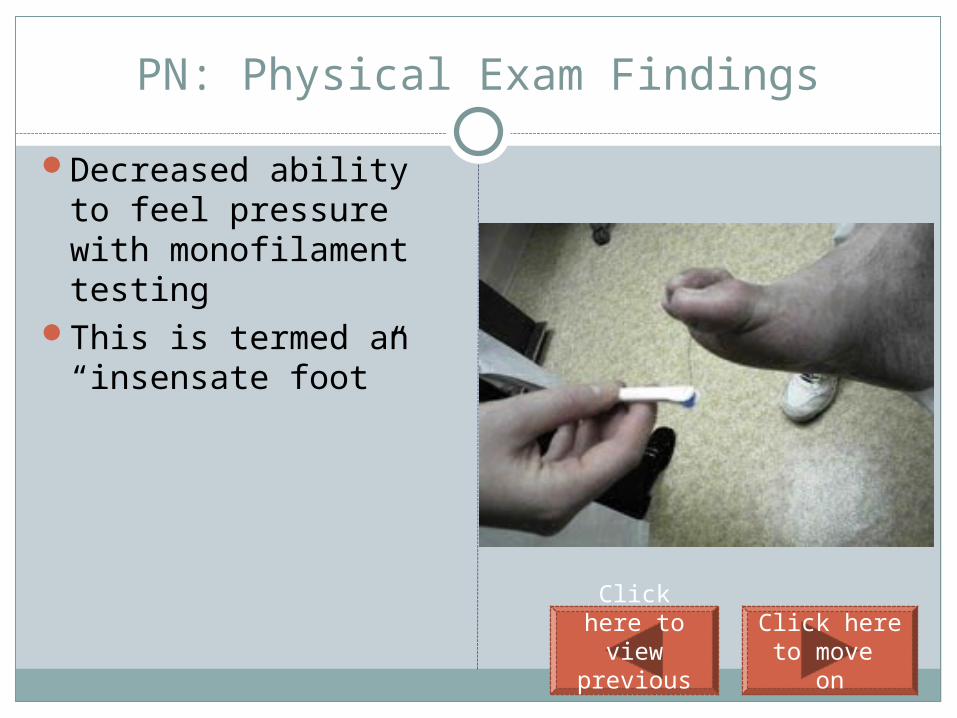
PN: Physical Exam Findings
Decreased ability to feel pressure with monofilament testing
This is termed an “insensate foot”
Click here to move on
Click here to view
previous screen

Risk Factors: Peripheral Arterial Disease
Arterial insufficiency refers to sluggish blood flow through the arteries.
In diabetes, this is usually due to atherosclerosis (plaques that line the blood vessels)
This results in reduced blood flow to the feet and extremitiesClick here
to move on
Click here to view
previous screen

Peripheral arterial disease is usually due to:
Peripheral neuropathy
Nerve damage
Atherosclerosis
Click here to select this
answerClick here to select this
answerClick here to select this
answer
Click here to view
previous screen

The correct answer is:
Peripheral neuropathy
Nerve damage
Atherosclerosis
Click here to select this
answerClick here to select this
answerClick here to select this
answer
Click here to learn more;
select atherosclerosis from the drop down menu
Click here to move on
Click here to view
previous screen

PAD: Symptoms
The reduced blood flow (and lack of oxygen to the tissues) leads to unhealthy tissues and poor wound healing
Many people with diabetes and PAD
do not have any symptoms. Somepeople may experience mild leg
painor trouble walking and believe thatit’s just a sign of getting older.
Othersmay have the following symptoms:
leg pain, particularly when walking or exercising, which disappears after a few minutes of rest (clinical term is intermittent claudication)
numbness, tingling, or coldness in the lower legs or feet
sores or infections on the feet or legs that heal slowly
Click here to move on
Click here to view
previous screen

Peripheral arterial disease
Intermittent claudication
Peripheral Neuropathy
The clinical term for leg/calf pain that occurs with activity and disappears with rest is:
Click here to select this
answerClick
here to select this
answerClick
here to select this
answerClick here
to view previous screen

The correct answer is:
Intermittent claudication
Click here to move on
Click here to view
previous screen

PAD: Physical exam findings
On physical exam, persons with peripheral arterial disease may have:
Weak or absent pulses in lower extremities (pedal pulse)
Coolness of the foot or leg
Shiny skin with or without stasis dermatitis
Hair loss (on the legs and toes)
Toe nail changes (brittle, thickened)
Red to brownish discoloration, known as stasis dermatitis.
Click here to move on
Click here to view
previous screen

Stasis Dermatitis
Intermittent claudication
Peripheral Neuropathy
A red/brown discoloration of the lower extremities that is seen with arterial disease is termed:
Click here to select this
answer
Click here to select this
answerClick
here to select this
answerClick here
to view previous screen

The correct answer is…….
Stasis dermatitis
Click here to move on
Click here to view
previous screen

PAD: Risk Factors or developing
Smoking High blood pressure High cholesterol Overweight/Obesity Physical inactivity Poor control of blood glucose
All of these increase the risk of PAD
Click here to move on
Click here to view
previous screen

Cool extremities
Diminished pedal pulses
Loss of sensation
Decreased hair growth
All of the following are signs of arterial disease except:
Click here to select this
answerClick here to select this
answerClick here to select this
answerClick here to select this
answerClick here
to view previous screen

Cool extremitites
Diminished pedal pulses
Loss of sensation
Decreased hair growth
All of the following are signs of arterial disease except:
Cool
extrem
ities,
decrea
sed
hair
growth
and
diminis
hed
pedal
pulses
are
seen
with
PAD,
wherea
s loss
of
sensati
on
occurs
with
periph
eral
neurop
athy
Click here to move on
Click here to view
previous screen

Risk Factor: Obesity
Obesity is a risk factor for diabetic foot disease because:
There is more weight and shear stress on the feet
Obese persons may have a difficult time inspecting and caring for their feet
Click here to move on
Click here to view
previous screen
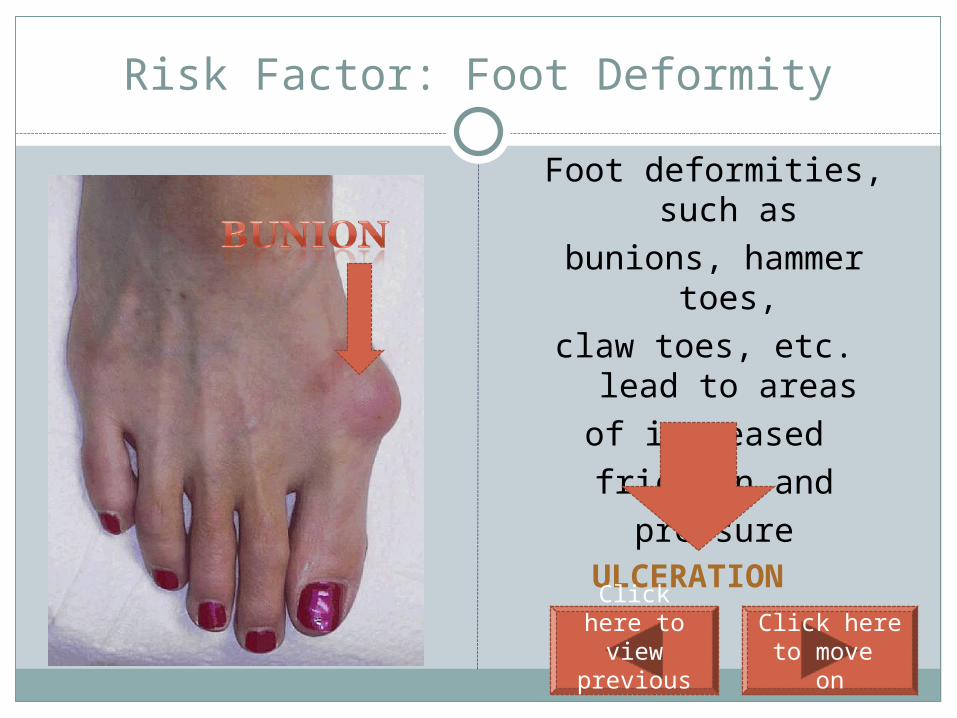
Risk Factor: Foot Deformity
Foot deformities, such as
bunions, hammer toes,claw toes, etc. lead to
areasof increased friction and
pressure
ULCERATION
Click here to move on
Click here to view
previous screen

Additional Risk Factors
Impaired visionPoor glucose control Poor footwear Decreased mobilitySevere nail pathologyHistory of foot ulcers or amputation
Click here to move on
Click here to view
previous screen

These nails are hypertrophied (thickened) from fungal infection in this patient with no prior access to podiatric care. Due to the increased pressure transmitted to underlying tissues, these nails can damage the nail bed which may then become secondarily infected and ulcerate.
Click here to move on
Click here to view
previous screen

The Diabetic Foot Exam
Also known as the LEAP ExamLEAP is an acronym for:
Lower Extremity Amputation Prevention
Click here to move on
Click here to view
previous screen

LEAP PROGRAM
The LEAP Program consists of five relatively simple activities:
Foot screeningPatient educationDaily self inspection of the footAppropriate footwear selectionManagement of simple foot problems
Click here to move on
Click here to view
previous screen

The Bureau of Primary Health Care’s (BPHC) Lower Extremities Amputation Program (LEAP) recommend visual foot exams / inspections at each visit.
All patients with diabetes should have a monofilament test done at least annually.
Who should have a diabetic foot screening?
Click here to visit the BPHC/HRSA website
Click here to move on
Click here to view
previous screen

True of False: A visual foot exam should be performed at every visit with a diabetic patient
True
False
Click here to select this
answerClick here to select this
answer
Click here to view
previous screen

The correct answer is……
True
Click here to move on
Click here to view
previous screen

Level I Diabetic Foot Screening: Step I:Talk with the patient and document responses
Have there been any changes in your feet?
How often do you examine your feet for changes?
Any burning, numbness, tingling, or pain in your feet or calves?
Is there pain in the calf muscles when walking?
Do you smoke?
Click here to move on
Click here to view
previous screen

Peripheral Neuropathy
Arterial Insufficiency
Diabetic nephropathy
Stasis Dermatitis
Burning, numbness and/or tingling in the feet may indicate:
Click here to select this
answerClick here to select this
answerClick here to select this
answerClick here to select this
answerClick here
to view previous screen
Peripheral Neuropathy
Arterial Insufficiency
Diabetic nephropathy
Stasis Dermatitis
The correct answer is:
Click here to move on
Click here to view
previous screen

Level I Diabetic Foot Screening: Step II: Perform a visual
screening of footwear and lower extremities
Explain to the patient that you will be performing a foot screening
Ask the patient to remove both the shoes and socks
Inspect the shoes for signs of excess wear and the presence of objects such as pebbles, sharp areas, etc
Visually inspect the lower extremities- paying particular attention to look between the toes and the back of the heal. Feel for the temperature and condition of the skin.
Note any deformities and skin problems
Redness and
pressure areas
Dry, cracked skin
Calloused areas
Deformity
Tight & Shiny Skin
Edema
Click here to move on
Click here to view
previous screen

Footwear and socks
Areas between the toes
The heels of the feet
All of the above
The visual portion of the diabetic foot screening includes inspection of:
Click here to select this
answerClick here to select this
answerClick here to select this
answerClick here to select this
answerClick here
to view previous screen

The correct answer is…….
All of the above
Click here to move on
Click here to view
previous screen

Level I Diabetic Foot Screening: Step III: Perform the monofilament screening
Explain exam and demonstrate on hand
Position for comfort
Have patient close their eyes. Ask patient to say “yes” when they feel filament
Touch monofilament to testing area, creating a C shaped bend and remove; avoid dragging; avoid calloused areas
Click here to move on
Click here to view
previous screen

The Monofilament Screening
Is used to determine if there is loss of protective sensation (LOPS)
A lack of sensation in any area with monofilament screening means the patient is at increased risk of foot ulceration and this usually prompts the health care practitioner to refer the patient to a podiatrist
Click here to move on
Click here to view
previous screen

Tell the patient to let you know when he/she feels the sensation
Ask the patient to blink 3 times when he/she feels the sensation
Ask the patient: “Do you feel this?”
What is the preferred way to establish if the patient feels the monofilament?
Click here to select this
answer
Click here to select this
answer
Click here to select this
answer
Click here to view
previous screen

The correct answer is…….
Tell the patient to let you know when he/she feels the sensation. This avoids the examiner “prodding” the patient to report the sensation. If the patient does not respond to the monofilament, the examiner should note negative sensation in the area and move on with the screening.
Click here to move on
Click here to view
previous screen

True of False: The proper amount of pressure for monofilament testing is that which causes an indentation to be left in the skin.
True
False
Click here to select this
answerClick here to select this
answer
Click here to view
previous screen

The correct answer is…..
False……the correct pressure is applied by touching the monofilament to the testing area and creating a C shaped bend.
Click here to move on
Click here to view
previous screen

MONOFILAMENT SCREENING
A simplified monofilament examination using only 4 sites per foot (total 8 sites) detected 90% of patients with an abnormal 16-site monofilament evaluation.
J Gen Intern Med. 1999 July; 14(7): 418–424. doi: 10.1046/j.1525-1497.1999.05208.x.
Click here to move on
Click here to view
previous screen

The 4 test sites
Click here to move on

Demonstrate themonofilament on thePatient’s hand or arm
Lubricate themonofilament
Prior to performing the monofilament screening, it is important that the examiner:
Click here to select this
answer
Click here to select this
answer
Click here to view
previous screen

The correct answer is……
………..Demonstrate the monofilament on the patient’s arm or hand
This lets the patient know that the monofilament does not hurt and what the monofilament is “suppose to” feel like.
Click here to move on
Click here to view
previous screen

Throughout the screening and following the screening….Provide patient education
Awareness of personal risk factors Daily self inspection of feetProper nail and skin care Injury prevention When to seek help or specialized referral; For a foot finding call
immediately; do not delayNever walk barefootFor a foot finding call immediately; do not delaySmoking cessationCheck water temperature for bathingMoisturize but not between toesProper foot wear selection
Click here to move on
Click here to view
previous screen

Education and Goal Setting Is Important
It is estimated that the risk of diabetes-related foot complications can be reduced by 49% to 85% by proper preventive measures, patient education, and foot self-care.
(Apelqvist J, Bakker K, van Houtum WH, Nabuurs-Franssen MH, Schaper NC. International consensus and practical guidelines on the management and the prevention of the diabetic foot. International Working Group on the Diabetic Foot. Diabetes Metab Res Rev. 2000;16:S84–S92.)
Click here to move on
Click here to view
previous screen

Lastly, Be sure to…..
Document all findings and educationVerbally report findings to the PCP
Click here to view
previous screen
Click here to move on

You have reached the end of this program…..
Once you are confident that you are comfortable with all the materials presented, proceed to the Diabetic Foot Screening post-test at http://www.classmarker.com/professional/
Your username is the first initial of your first name followed by your full last name. Your password is= nwhealth
Click here to go back and review previous slide
Start Over Exit