wells criteria - continuing medical education - ucsf ... tracy minichiello, m.d. associate professor...
TRANSCRIPT

1
Tracy Minichiello, M.D.Associate Professor of Medicine
Chief, SF VA Anticoagulation Services
Cases in Venous Thromboembolic Disease
Objectives
� Determine pre-test probability of PE � Appropriate diagnostic algorithm for evaluation of VTE� Perform risk stratification for patients with PE� Anticoagulation for various presentations of thrombosis� Management of warfarin-related coagulopathy
A 66 year-old man presents to the ER with acute shortness of breath and pleuritic chest pain. His HR is 110. How do you assess his pre-test probability of PE?
Well
’s cri
teri...
Rev
ised G
enev
a...
Per
form
a be
ds...
59%
31%
10%
1. Well’s criteria2. Revised Geneva risk score3. Perform a bedside “Aunt
Minnie”
Wells CriteriaClinical symptoms of DVT (leg swelling, pain with palpation) 3.0Other diagnosis less likely than pulmonary embolism 3.0Heart rate >100 1.5Immobilization ( 3 days) or surgery in the previous four weeks 1.5Previous DVT/PE 1.5Hemoptysis 1.0Malignancy 1.0
Wells et al J Intern Med 1998

2
Wells CriteriaTraditional score/prevalenceHigh >6 (78%) Moderate 2-6 (28%)Low <2 (3%)
Wells et al J Intern Med 1998; Van Belle, A, et al. JAMA 2006; 295:172
Revised Geneva Risk ScoreAge>65 1Previous VTE 3Surgery 2Active cancer 2Unilateral limb pain 3Hemoptysis 2HR 75-94 3HR >94 5Pain and edema 4
Le Gal, et al Ann Intern Med 2006
Revised Geneva Risk ScoreProbability Score Prevalence
Low 0-3 8%
Intermediate 4-10 28%
High ≥11 74%
Le Gal, et al Ann Intern Med 2006
Appropriateness of Diagnostic Management and Outcomes of Suspected Pulmonary EmbolismLow prob
� any d-dimer
� Low prob V/Q
� CTa
Int prob� High sens d-dimer
� Neg V/Q� Multi detector CTa
� Cta + U/S
high prob� -PAgram� Nml V/Q
Roy, P.-M. et. al. Ann Intern Med 2006
3
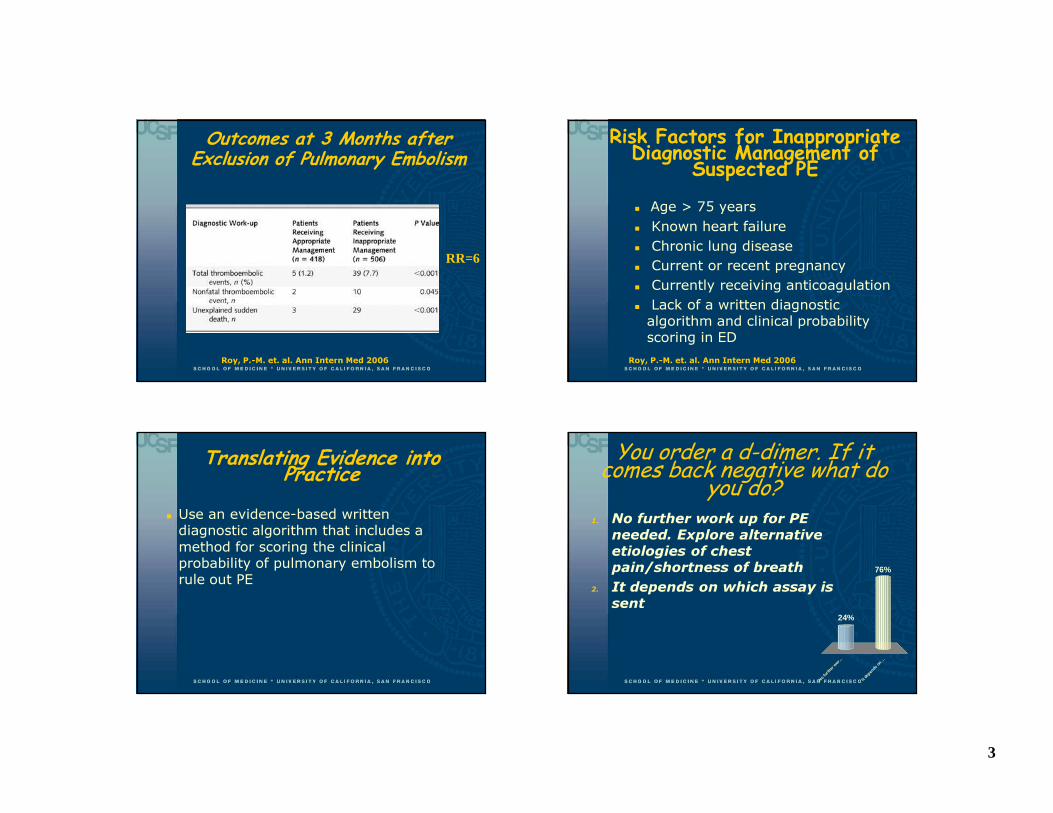
Roy, P.-M. et. al. Ann Intern Med 2006
Outcomes at 3 Months after Exclusion of Pulmonary Embolism
RR=6
Risk Factors for Inappropriate Diagnostic Management of Suspected PE� Age > 75 years� Known heart failure� Chronic lung disease� Current or recent pregnancy � Currently receiving anticoagulation � Lack of a written diagnostic algorithm and clinical probability scoring in ED
Roy, P.-M. et. al. Ann Intern Med 2006
Translating Evidence into Practice� Use an evidence-based written diagnostic algorithm that includes a method for scoring the clinical probability of pulmonary embolism to rule out PE
You order a d-dimer. If it comes back negative what do you do?
No
furth
er w
o r ...
It de
p ends
on ..
.
76%
24%
1. No further work up for PE needed. Explore alternative etiologies of chest pain/shortness of breath
2. It depends on which assay is sent

4
Copyright ©2005 BMJ Publishing Group Ltd.
Roy, P.-M. et al. BMJ 2005
Negative Likelihood Ratios (NLR) for D-Dimer Tests for Pulmonary Embolism
Quant
ELISA
Quant
latex
Semi-quant
latex
Translating Evidence into Practice� Know which d-dimer assay your institution uses
� A highly sensitive d-dimer assay safely excludes PE in low and moderate pretest probability
� A moderate sensitivity assay excludes PE only in low probability patients (or Wells ≤4)
A CT angiogram reveals bilateral pulmonary emboli. The patient is hemodynamically stable. ECG reveals sinus tachycardia. How would you assess his risk of PE-related mortality and complications now?
get
an
ECHO re
view th
e CT
...
ord
er B
NP and
...
any c
omb in
atio..
. I w
o uldn
’ t bot...
28%
9%
20%
24%
20%1. get an ECHO2. review the CT scan3. order BNP and troponin4. any combination of A,B,C5. I wouldn’t bother
RV Dysfunction and MortalitySource Patients RV
DysfunctionNl RV Function
Goldhaber 101 4.3 0Kasper 317 12.6 0.9Ribeiro 126 12.8 0Grifoni 162 4.6 0Total 706 9.3 0.4
Kreitt JW Chest 2004

5
Prognostication in PE� Evidence of RV strain, despite normal BP, associated with increased 30-day mortality
� Normal ECHO-in hospital mortality < 1%
Copyright ©2004 American Heart Association
Schoepf, U. J. et al. Circulation 2004; Quiroz, R. et al. Circulation 2004
CT for Prognostication in PE
Risk Stratification in PE
Aujesky et al Eur Heart Journal 2006;27:476
Risk Factor Points Age Points=age Male 10 Cancer 30 Heart failure 10 Chronic lung disease 10 HR > 110 20 SBP < 100 mmHG 20 RR >30 20 Temp < 36 20 ∆ mental status 60 O2 sat <90% 20
Risk Stratification in PESeverity class Points 30 day mortality I 0-65 <1.7% II 66-85 <3.5% III 86-105 <7.1% IV 106-125 4-11% V >125 10-25%
Aujesky et al Eur Heart Journal 2006;27:476

6
Serum Biomarkers for Risk Stratification in PE� Troponin�NPV 99-100% PE-related mortality
� BNP (>100pg/ml) or NT-proBNP (600ng/L)�NPV 94-100% for short term mortality and complications
Becattini C, Circulation. 2007; Cavallazzi, Critical Care Medicine 2008; Pulls European Heart Journal 2007
Translating Evidence into Practice� Risk stratify all patients presenting with PE
� Patients with elevated troponin/BNP, RV dysfunction on ECHO, severity class III-V or hemodynamic compromise are at higher risk for death and nonfatal complications of PE
� Clinicians can use this information to guide treatment and triage decisions� Level of care in hospital� Timing of discharge to home� More aggressive therapy?
A 35 year-old woman on OCPs presents with sudden onset severe right leg pain and swelling. An ultrasound reveals a very large iliofemoral DVT. What would you recommend now?
Enter question text...
1. D
ischa
rge p
...
2. C
onsult
IR ...
3. S
tart
antic
...
40%
20%
40%1. 1. Discharge patient on enoxaparin 1mg/kg BID and warfarin
1. 2. Consult IR or vascular for catheter-directed thrombolysis
2. 3. Start anticoagulation and place an IVC filter
Post-Phlebitic Syndrome� Persistent proximal venous obstruction often
causes distal valve incompetence which can lead to post phlebitic syndrome
� Iliofemoral DVT-high risk for PPS�Painful edema-75%�Pigmentation changes 28%�Ulcers 8-15%�Venous claudication- 40%
Delis KT, et al Ann Surg. 2004 Akesson H, et al Eur J Vasc Surg. 1990
7
Rationale for the Use of Thrombolytics� Thrombolytic therapy may reduce the incidence of postthrombotic syndrome by:�promoting rapid recanalization�eliminating obstruction�preventing recurrent thrombosis
Preserving valve function
Catheter-Directed Thrombolysis for Ileofemoral DVT� Retention of normal valve function (89% vs.
59%
� Improved patency (72% vs. 12%)� Improved quality of life
� Major bleeding rates 4-11%
Comerota AJ, et al J Vasc Surg. 2000 Elsharawy M, et al Eur J Vasc Endovasc Surg. 2002
Translating Evidence Into Practice
� ACCP recommends: Consider referral of carefully selected patients with large iliofemoral DVT for catheter-directed thrombolysis� symptoms for less than 14 days� good functional status� life expectancy of at least 1 year� low risk of bleeding
Graduated Compression Stockings� Can reduce risk of post phlebitic
syndrome (OR 0.3)� Most effective if applied early� Recommended to wear for up to 2
years after DVT� Prescribe on discharge � GCS 30-40mmHG to the knee or thigh
Kolbach DN, etal Cochrane Database Syst Rev. 2004
8
Translating Evidence Into Practice
� Prescribe graduated compression stockings for ALL patients with DVT (unless evidence of arterial insufficiency) and instruct to wear for 1-2 years
A 30 year-old woman on OCPs presents with calf pain for 3 days. On exam she has swelling, no erythema, and is able to bear weight. An ultrasound reveals a DVT in the anterior tibial vein and the peroneal vein. For this distal DVT you recommend: A
) LMW
H and wa.
..
B) F
ollow u
p U...
32%
68%
1. A) LMWH and warfarin2. B) Follow up U/S in one
week with plan to treat if signs of progression
Distal/Calf Vein Thrombosis� Progression to proximal DVT�25-30% will progress to involve proximal veins�30% will have recurrence or progression if treated with 5 days of UFH only�Recurrence rates after 3 months of full dose anticoagulation therapy are less than 3%
Kearon, Circulation 2003
Translating Evidence Into Practice
� Symptomatic isolated calf vein thrombosis should be treated with full intensity anticoagulation for 3 months
9
A 50 year-old woman with breast cancer, undergoing chemotherapy presents with RLE pain and swelling. U/S reveals acute thrombosis of the common femoral vein. Which anticoagulant regimen would you recommend?
LMW
H bridg
ing ..
.
LM
WH th
erap
y
33%
67%
1. LMWH bridging to warfarin therapy goal INR 2-3
2. LMWH therapy
Copyright ©2002 American Society of Hematology.
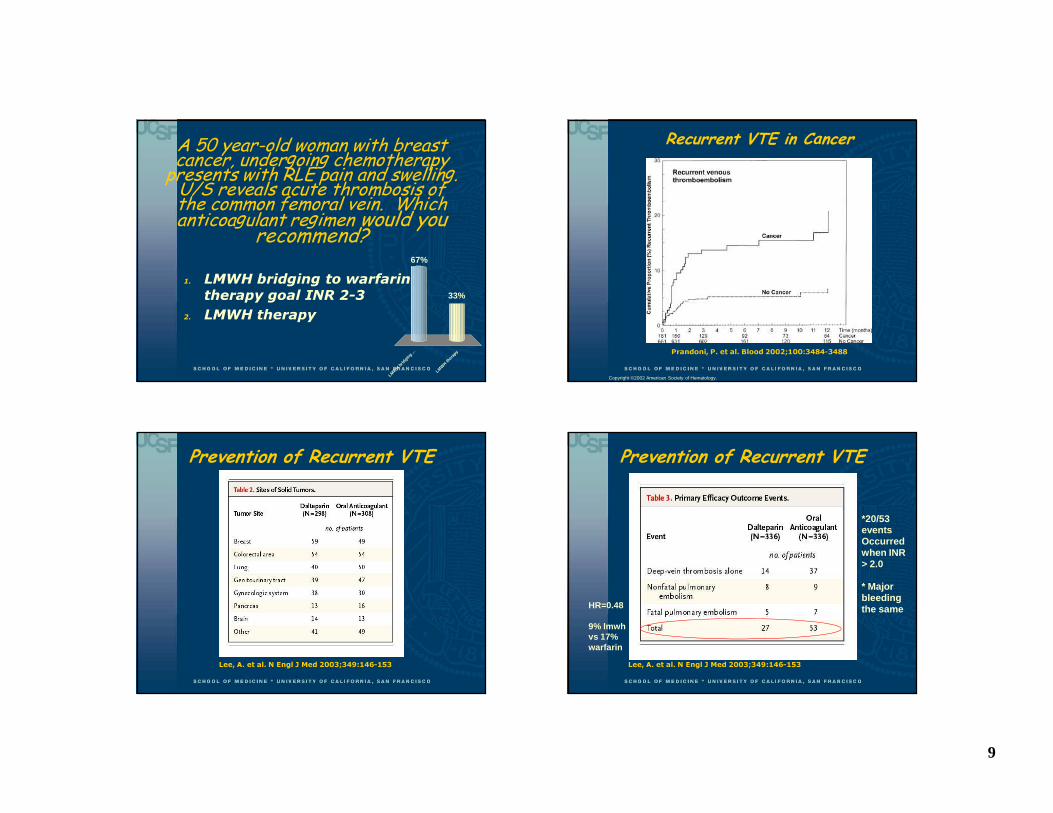
Prandoni, P. et al. Blood 2002;100:3484-3488
Recurrent VTE in Cancer
Prevention of Recurrent VTE
Lee, A. et al. N Engl J Med 2003;349:146-153
Prevention of Recurrent VTE
Lee, A. et al. N Engl J Med 2003;349:146-153
*20/53 eventsOccurred when INR > 2.0
* Major bleeding the sameHR=0.48
9% lmwh vs 17% warfarin

10
Translating Evidence Into Practice
� Patients with cancer and VTE should receive LMWH instead of warfarin for at least 3-6 months (grade 1A evidence)
Lee AY ASH 2004; Kearon CHEST 2008
Which of these patients need anticoagulation?
A 65
year o
ld ...
A 5
5 ye
ar o
ld ...
Both
Neit
her
8%
72%
7%13%
1. A 65 year old woman recently hospitalized with superficial thrombophlebitis in her right forearm where IV had been placed
2. A 55 year old woman with spontaneous superficial thrombophlebitis on her shin
3. Both4. Neither
Superficial Thrombophlebitis� Superficial thrombophlebitis secondary to infusion therapy � NSAIDS superior to placebo for symptomatic relief, extension exceedingly low
� Spontaneous superficial thrombophlebitis� After 1 week of AC 15% had extension or recurrence at 3 months� High dose UFH for one month reduced extension to 3% vs. 20 % in patients on prophylactic dose UFH
Buller et al, CHEST 2004
Translating Evidence Into Practice
Patients with spontaneous superficial thrombophlebitis (especially longer segments and close to saphenofemoral junction) should be treated with prophylactic or intermediate doses of LMWH for at least 4 weeks. May alternatively be transitioned to warfarin
Kearon CHEST 2008

11
How would you manage this elevated INR?� A 45 yo with DVT dx 2 months ago presents with epistaxis and INR of 6.0� A 75 yo sent to ER for evaluation after labs showed INR of 11 today. No obvious bleeding� A 75 yo on warfarin for afib admitted with headache found to have subdural hematoma, INR 4.5
Supratherapuetic INR� Medications (amio,
macrolides, azoles, Bactrim, statins)
� Alcohol� Diet� Diseases (CHF,
liver, thyroid)� Herbal
Management of Elevated INRs
CHEST Supplement May 2008 Antithrombotic and Thrombolytic Therapy: ACCP Evidence-Based Clinical Practice Guidelines
Clinical Situation
INR Recommendations
Above therapeutic range but < 5.0
-Lower dose or omit dose -Monitor more frequently and resume at lower dose when INR falls within therapeutic range (if INR slightly above range, may not be necessary to decrease dose)
No significant bleed
≥ 5.0 but < 9.0
-Hold next 1-2 doses -Resume therapy at lower dose when INR falls within therapeutic range -Pts with high bleed risk: Hold warfarin PLUS give vitamin K1 ≤ 2.5 mg po , check INR in 24-48 h to assure response to therapy)
High risk:Renal failureHypertensionElderlyFallsLiver dzGI/GU bleed
Management of Elevated INRs
CHEST Supplement May 2008 Antithrombotic and Thrombolytic Therapy: ACCP Evidence-Based Clinical Practice Guidelines
Clinical Situation
INR Recommendations
≥ 9.0 -Hold warfarin -Vitamin K1 2.5-5.0mg po x 1; may repeat -Resume therapy at lower dose when INR within therapeutic range -Contact MD to determine appropriate triage

12
Warfarin-Associated ICHRisk Factors
� Antiplatelet therapy� Age� Hypertension� Race� INR >3.5� Abnormal MRI
Outcome� 50% die in 30days� INR correlates with progression of hematoma and survival
� ICH expansion delayed in warfarin patients
Management of Warfarin-Associated ICH� IV Vit K� FFP� PCC� rFVIIA
Brody et al Neurocrit Care. 2005.
Management of Elevated INRsClinical Situation
INR Recommendations
Serious/life-threatening bleed
Any elevation
Give vitamin K, 10mg slow IV push and FFP or PCC or recombinant factor VIIa
CHEST Supplement May 2008 Antithrombotic and Thrombolytic Therapy: ACCP Evidence-Based Clinical Practice Guidelines
Translating Evidence Into Practice
� Use evidence based guidelines for management of warfarin-associated coagulopathy
� Arrange close follow up for all patients on warfarin who present to the ER.
Kearon CHEST 2008

13
Questions?