what a headache !/? paul hart consultant neurologist epsom +st helier0208 296 3355(m tu th) amw sgh...
TRANSCRIPT
WHAT A HEADACHE !/?
Paul Hart
Consultant Neurologist
Epsom +St Helier 0208 296 3355 (M Tu Th)
AMW SGH 0208 725 4107 (Wed Fri)
RMH

Headaches
• Common
1 in 3 suffer a severe HA at some stage in life
Lifetime prevalence: M 90%; F 95%
Migraine M 6.5%; F 18.2% = 28 million in USA
112 million bed ridden days per year
$13 billion / year
WHO : Among the most disabling medical conditions experienced worldwide

What causes pain ?• Ray + Wolfe 1930s
Intracranial:– Circle of Willis + 1st few cms of branches– Meningeal (dural)arteries– Large veins + dural venous sinuses– Portions of dura near bv’s
Extracranial: ECA + branches, scalp + neck muscles, skin +cut nerves,
cervical n’s + nerve roots, sinus mucosa, teeth.(via V VII IX and X to CNS)
• Pain localisation
• Pain modulation
Headache Classification
• International Headache Society 2004
Primary Headaches– 1 Migraine
– 2 Tension-type Headache
– 3 Cluster HA and other trigeminal autonomic cephalalgias
– 4 Other primary headaches

• International Headache Society 2004
Secondary Headaches– 5 HA attributed to head + neck trauma– 6 HA attributed to cranial or cervical vascular disorder– 7 HA attributed to non-vascular intracranial disorder– 8 HA attributed to a substance or its withdrawal– 9 HA attributed to infection– 10 HA attributed to disorder of homeostasis– 11 HA or facial pain attributed to cranium, neck, eyes, nose,
sinuses, teeth, mouth or other facial or cranial structures– 12 HA attributed to psychiatric disorders– 13 Cranial neuralgias and central causes of facial pain– 14 Other HA, cranial neuralgia, central or primary facial
pain

Primary Headaches 1 - Migraine
• Hemikranios• 200 AD Aretaeus of Cappadocia
• 90% Onset <40 years• F = 20% M = 6%• 90% FHx• Unilateral Throbbing Mod-severe• Prodrome in 60%• Duration 4 – 72 hours• Worse with exercise• Anorexia N + V• Photo phono osmo – phobia• HA history: Current HA(s), Past HA(s), other…• HA behaviour
Migraine cont …
• Migraine without aura– Prodrome (hrs – days)
• Mood or energy change
• Thirst
• Yawning
• Food craving
– Unilateral / bilateral pain
– Or lower half headache
– Postdrome• Tired, listless, exacerbation of pain
• Frequency• Inter + intrapatient variability - Catamenial

Migraine cont …
• Migraine with aura – (15% of migraineurs)
– Visual
– Sensory
– Motor
– Language
– Other focal cerebral or brainstem symptoms
– Differential diagnosis
• Migraine equivalent / Acephalic migraine– Usually past history of MwA
– Any age (usually>40)

Migraine cont …
• Basilar migraine
• Ophthalmoplegic migraine
• Complications of Migraine– Hemiparesis
– Facioplegic migraine
– Field defect
– Migraine + stroke
• O/E
• Investigations

Migraine cont …• Genetics
– FHM 50% chromosome 19p13CACNA1Aalpha 1 subunit of a brain specific VG P/Q type Ca channel(EA type 1)
chromosome 1q31neuronal Ca channel alpha 1E subunit
gene
• Pathophysiology– Lashley 1941– Leao 1944
Migraine cont …
• Treatment + Management– Explain + reassure– Trigger factors (diet stress tobacco drugs sleep)
– Pharmacotherapy• Symptomatic
• prophylactic
Frequency
Long duration
Dread of attack
Severe neuro symptoms
Failed symptomatic Rx
Menstrual migraine
Migraine cont …
• Symptomatic treatment– Take as early as possible (except sc sumatriptan)
– Simple oral analgesics
– + caffeine
– Metoclopramide
– Sleep etc.. Headache treatment centres
– Ergots DHE Isometheptene
– Triptans - selective agonists -

• Table 75-9. Oral serotonin (5-HT) agonists
• Drug Dose Headache response (%)* Recurrence†
(mg) 1 hr 2 hr 4 hr
Almotriptan 12.5 35 57 NA 23%Eletriptan 20.0 20 49 NA 30 40.0 30 60 NA 22Frovatriptan 2.5 NA 42 61 10-25%Naratriptan 1.0 19 42 51 17-28% 2.5 21 48 67 Rizatriptan 5.0 30 60 NA 30-35% 10.0 37 67-77 NA Sumatriptan 25 NA 52 68 35-40% 50 NA 50 70 100 NA 56 75 Zolmitriptan 2.5 38 64 75 31% 5.0 44 66 77 *Headache response is defined as a reduction in headache severity from moderate or severe pain
to mild or no pain.†Recurrence of headache within 24 hours after initial headache response.Note: Composite data from product information inserts and literature.NA = not available.

Migraine cont …TriptansTable 75-8. Subcutaneous and intranasal serotonin (5-HT)
agonistsHeadache response (%)*
Drug Dose (mg) 1 hr 2 hr 4 hr Recurrence†
• Dihydroergotamines.c. 1 57 73 85 18I.n. 2 46 47-61 56-70 14
• Sumatriptan s.c. 6 70 75 83 35-40 I.n. 20 55 60 NA 35-40
• Zolmitriptan I.n. 5 55 70 78 25
Headache response is defined as a reduction of headache severity from moderate or severe pain to mild or no pain.†Recurrence of headache within 24 hours after initial headache response.NA = not available.
Migraine cont …
• Side effects + Contraindications
• Which triptan– N+V: sc or in
– Headache peaks rapidly: Almo Riza Zolmi
– Benign but intolerable triptan SE’s:
Almo Nara Frova
– Recurrent HA after initial benefit:
Nara Frova DHE
– Combine with simple analgesia or antiemetic

Migraine cont …
• Prophylaxis– Propranolol – effective in 55-93%
– Antidepressants - Amitriptyline
Imip Nortrip Desip
(SSRIs MAOIs)
– 5HT agents – Methysergide (cyproheptadine)
– Ca blockers - verapamil nimodipine flunarazine
– AEDs – valproate gabapentin topirimate
– Others – Mg, riboflavin, alternate day aspirin, botox
Migraine cont …
• Hormones + migraine– Menstrual migraine– Contraception– Pregnancy– Menopause
– IHS task-force evidence based recommendations for the use of contraceptives and HRT in migraineurs (Bousser 2000)

• Identify + evaluate risk factors• Diagnose migraine type (MwA MxA)• Stop smoking before starting COCs• Treat other risk factors (HT lipids)• Consider non-ethylestradiol methods• High dose COCs should be avoided esp if containing 1st
generation progestogens
Migraine symptoms that may necessitate further evaluation or cessation:
• New persisting HA• New onset of migraine aura• Increased HA freq or intensity• Development of prolonged or unusual aura
Primary Headaches 2 - Tension Type Headaches
• TTHA ------- Migraine• Generally bilateral• Tight band / pressure / bursting• No N, V, photo, phono, phobia• Rx
– Psychological– Physical– Pharmacological Asp NSAIDs (avoid codeine)
Amitriptyline or….

Primary Headaches 3 - Cluster Headaches and other Trigeminal
Autonomic Cephalalgias
• Most painful• Most stereotyped• Most names• Most often misdiagnosed ?• 10-50 times less common than migraine • Episodic: daily for days to months, respite for
weeks to years• Chronic (10 or 20): >1 year without a remission of
>2 weeks

Cluster cont…• Clinical features
– M>F– Onset 20-30 (1-70)– Clusters 6-12 weeks; 1-3 per day– 50% remit; 10% chronic– Onset – peaks over 5-10 min– Unilateral retro-orbital or temporal– Steady, boring, severe– Duration 45min – 2 hours (? 4 hours)– Behaviour during attack– Autonomic features– ?? photo, phono, N (50%) + V (rare)– Offset gradual with possible exacerbations
Cluster cont…
• Investigations– Imaging ?
• Treatment + Management– Acute symptomatic
• Oxygen, Imigran, DHE, Zolmitriptan, i.n. lidocaine
– Transitional prophylaxis• Steroids, Ergotamine, DHE, (triamcinalone, Mpred),
ipsilateral occipital n block
– Maintenance prophylaxis• Verapamil, Methysergide, Lithium
Indomethacin-Responsive Headache syndromes
• Prompt, absolute, and often permanent response to Indomethacin
• May be confused with cluster– But shorter duration + higher frequency
• Paroxysmal hemicrania– Episodic (2w-5m, remissions 1-36m)– Chronic– Age 10-30 F:M 2:1– Daily attacks (5/day) of severe short lived (20
min) unilateral pain (orbital temporal)– At least 1 autonomic feature

Cluster cont…
• Hemicrania continua– Continuous unilateral hemicrania or focal area– Moderate intensity– Onset 28 (5-67)– F:M 2:1– Autonomic features more subtle
• Indomethacin

SUNCT• 15-120 seconds
• In or around eye
• May be triggered
• 1 per day – 30 per hour
• V ophth (cf TN)
• Rx: CZP LTG Gaba Top
Primary stabbing HA
• Patients with M, Cluster, TTHA etc
Other types of headache + facial pain
• CO2 CO
• Hypoxia
• Hypoglycemia
• HT
• Phaeochromocytoma
• (Pre) eclampsia

Primary Headaches 4 - Other Primary Headaches
• Cough Headache– Secs – mins– M:F 4:1 Age 55 (19-77)– Suboccipital/occipital/bilateral– Underlying structural abnormality in 50%– Rx Indomethacin
• Exertional Headache– Bilateral throbbing HA precipitated by sustained
physical exercise– Non explosive– 5 min – 24 hours– Benign or symptomatic– Cardiac cephalalgia
Primary Headaches 4 - Other Primary Headaches …cont…
• Headache associated with sexual activity– usually benign– gradual onset or sudden onset (?SAH)– or post orgasm with postural component
resembling low csf state– M>F– Rarely recurs– Rx Indomethacin, propranolol, diltiazem

Secondary Headaches7 - HA attributed to non-vascular, non-infectious
intracranial disorders
• High CSF pressure
• Low CSF pressure
• Non-infectious inflammatory disorders
• Intracranial neoplasms
• Chiari malformations
• Seizure + headache
• Mass lesions– 50% of patients with brain tumours have
headache– Primary complaint in 1/3 (17%)– Pain depends upon
• Location of lesion• Rate of growth• Affect on CSF flow• Cerebral oedema
Features of raised ICPam>pm; N+V; worse with cough sneeze + strain
• Warning signs of a non-benign HA (Purdy 2001 Med Clin North Amer)– Subacute + progressive
– New onset in those >40 years
– Change in headache pattern
– N or V in non migraine headache
– Nocturnal headache
– Awakening headache
– Precipitation or worsening with valsalva
– Confusion
– Seizures
– Weakness
– Abnormal neurological examination

• Intraventricular tumours– Rare but can present dramatically
• Colloid cyst
• Intraventricular meningioma
• Choroid plexus papilloma
– CASE

• Colloid cyst– Sudden severe HA– May be precipitated or relieved by change in
posture or precipitated by valsalva– Usually slowly enlarging HC resulting in a
generalised constant HA with episodes of catastrophic increase in headache.
– N + V– Possibly LOC
NB most cough or exertional headaches are benign
Abnormalities of CSF Circulation
• Obstruction of CSF pathways– Colloid cyst, Dandy-walker cyst, Arnold-Chiari– SAH, meningitis, venous occlusion
• Low CSF pressure
• Idiopathic Intracranial Hypertension



Secondary Headaches9 - HA attributed to infection
• Meningitis– Acute
– Chronic• TB
• Fungal
• Meningoencephalitis
• Sinusitis
• Mastoiditis
• Epidural / intraparenchymal abscess
• Skull osteomyelitis
Secondary Headaches6 - HA attributed to cranial or cervical vascular
disorders
• Aneurysms, AVMs, and thunderclap headache
• Parenchymal haemorrhage
• Cerebral ischaemia
• Dissection
• Giant cell arteritis
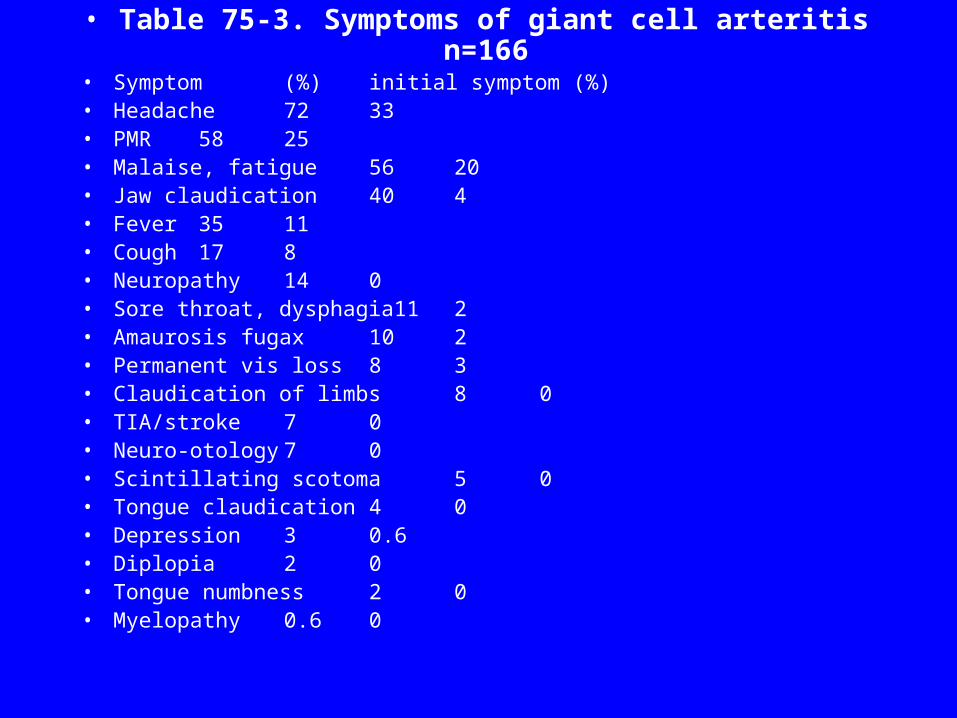
• Table 75-3. Symptoms of giant cell arteritis n=166 • Symptom (%) initial symptom (%)• Headache 72 33• PMR 58 25• Malaise, fatigue 56 20• Jaw claudication 40 4• Fever 35 11• Cough 17 8• Neuropathy 14 0• Sore throat, dysphagia11 2• Amaurosis fugax 10 2• Permanent vis loss 8 3• Claudication of limbs 8 0• TIA/stroke 7 0• Neuro-otology 7 0• Scintillating scotoma 5 0• Tongue claudication 4 0• Depression 3 0.6• Diplopia 2 0• Tongue numbness 2 0• Myelopathy 0.6 0
Secondary Headaches11 - HA caused by disorders of…..
• Eyes
• Nose
• TMJ
• Other dental disorders
• Cervical spine
• Other facial + cranial structures
Headaches: Top Tips
• An accurate diagnosis of the headache syndrome is essential
• It’s all in the history
• Investigations – atypical features or secondary headache
• Treatment rules - multimodal; adequate trials of adequate doses; improve not cure