what epidural opioid results in the best analgesia ... · copyright © 2014 international...
TRANSCRIPT

Copyright © 2014 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.XXX 2014 Volume XXX Number XXX www.anesthesia-analgesia.org 1
Copyright © 2014 International Anesthesia Research SocietyDOI: 10.1213/ANE.0000000000000377
Epidural opioids have been widely used for facilita-tion of central neuraxial blockade and postopera-tive analgesia. Although they may be used alone in
this regard, multiple studies have shown that analgesia is more effective when they are combined with local anes-thetics.1–3 Such mixtures minimize the risk of respiratory depression, somnolence, and pruritus associated with soli-tary narcotic use, while also reducing incidence of motor block, and hypotension associated with local anesthetics. Even more importantly, this multimodal approach has been shown to provide superior postoperative analgesia to that of IV patient-controlled analgesia with opioids.2 Despite the effectiveness of such epidural combinations, differences
in analgesic efficacy and side effect rates among opioids remain to be elucidated. This may be a function of physician preference, hospital-specific policies, or the specific opioids available on formulary. Given the unique pharmacologic properties of each opioid and studies that show different rates of accumulation in the cerebrospinal fluid, there is biologic plausibility for differences in the side effect profiles and analgesia among different opioids.4–7 No single large randomized controlled trial (RCT) has definitively identi-fied the ideal opioid for a postoperative epidural infusion, either with or without local anesthetic. This ideal opioid should improve subjective postoperative analgesia while minimizing the aforementioned side effects.
As such, we conducted a meta-analysis of all RCTs com-paring perioperative epidural opioid infusions. Most of these trials involved local anesthetic–opioid mixtures. Specifically, we sought to determine which opioid offers the best epidural analgesia in terms of postoperative visual analog scale (VAS) pain scores while minimizing opioid side effects after surgery.
METHODSEthicsThe HIREB (Hamilton Integrated REB) does not require ethics approval for systematic reviews, including network meta-analyses, because there are no data being collected from patients. We only evaluated and synthesized data that had been reported in published trials, and only used aggre-gate level data reported from the original trials.
BACKGROUND: Epidural opioids are widely used for central neuraxial blockade and postopera-tive analgesia. However, differences in analgesic efficacy and side effect rates among individual opioids remain controversial.METHODS: We conducted a random-effects meta-analysis of randomized controlled trials that compared at least 2 continuous epidural infusions for acute postoperative analgesia over at least 24 hours. Individual study data were weighted by the inverse-variance method. Visual analog scale (VAS) pain scores were the primary outcome. Secondary outcomes included opioid side effects, such as pruritus, postoperative nausea and vomiting (PONV), sedation, hypoten-sion, and respiratory depression.RESULTS: Nineteen of the 24 trials included compared 2 of the following opioids: morphine, fentanyl, or sufentanil. The total subjects studied were 1513. Pooled analysis by type of surgery showed no clinically significant differences in VAS pain scores at any time after surgery. There were more PONV (OR = 1.91; 95% CI, 1.14–3.18; P = 0.014) and perhaps pruritus (OR = 1.64; 95% CI, 0.98–2.76; P = 0.162) with morphine compared to fentanyl. Total opioid consumption differed only in the trials comparing morphine and fentanyl, where patients in the morphine group required 1.2 mg (of morphine equivalent) less (95% CI, 0.27–2.18). Use of analgesic adjuncts was similar for all but 2 studies.CONCLUSIONS: Analgesic outcome, in terms of VAS pain score, was similar between the epi-dural opioids studied. These similarities in analgesia may reflect the common practices of con-currently using epidural local anesthetics with the opioids and titrating infusion rates according to a patient’s pain status. With respect to side effects, the incidence of PONV and possibly pru-ritus was higher with morphine compared with fentanyl, despite there being similar total opioid consumption between those groups. (Anesth Analg 2014;XXX:00–00)
What Epidural Opioid Results in the Best Analgesia Outcomes and Fewest Side Effects After Surgery?: A Meta-Analysis of Randomized Controlled TrialsNayer Youssef, MD,* David Orlov, MD,† Tristan Alie, MSc, MD,* Matthew Chong, MD,‡ Ji Cheng, MSc,§צ Lehana Thabane, PhD,*§צ and James Paul, MD, MSc, FRCPC*
From the *Department of Anesthesia, McMaster University, Hamilton, Ontario; †Department of Anesthesia, University of Toronto, Toronto, Ontario; ‡Michael G. School of Medicine, McMaster University, Hamilton, Ontario; §Department of Clinical Epidemiology and Biostatistics, McMaster University, Hamilton, Ontario; and צBiostatistics Unit, St. Joseph’s Health-care Hamilton, Hamilton, Ontario.Accepted for publication June 3, 2014.Funding: This study was supported by the Department of Anesthesia, McMaster University.The authors declare no conflicts of interest.Parts of this report were presented at the 2013 ASA meeting in San Francisco.Reprints will not be available from the authors.Address correspondence to James Paul, MD, MSc, FRCPC, Department of Anesthesia, McMaster University, HSC-2U, 1280 Main St. West, Hamilton, ON L8S 4K1. Address e-mail to [email protected].

Copyright © 2014 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.2 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Meta-Analysis: Best Epidural Opioid with Least Side Effects
Literature SearchComputerized searches of Ovid MEDLINE (from 1950 to November 2013), EMBASE (from 1980 to December 2013), and the Cochrane Controlled Trials Register (CCTR up to November 2013) were conducted. While identifying clinical trials, a sensitive search strategy developed by Haynes et al.8 was used along with free text combinations and MeSH terms (Appendix, Supplemental Digital Content 1, http://links.lww.com/AA/A931). The searches were designed to be sensitive and identify the maximum number of RCTs that compared at least 2 different perioperative epidural opioid infusions. The search was restricted to studies pub-lished or translated to the English language. Unpublished studies were not sought.
Study SelectionInclusion for data abstraction was determined by reviewing each study abstract identified by the search. All abstracts were read by 2 authors, and agreement was reached by con-sensus to either include or exclude a study. Full articles were obtained so that reference lists could be reviewed to further identify additionally relevant studies. The reviewers were not blinded to the authors’ names, affiliated institutions, or the journal of publication for any of the studies.
PopulationStudies were included if they enrolled male or female par-ticipants of any age undergoing either elective or emergency surgery. Studies involving epidural analgesia in parturients during labor were excluded for many potential confound-ing factors, including differences between labor and postop-erative pain, variability in epidural insertion site, and time use during labor.9
InterventionStudies must have compared at least 2 different continu-ous epidural opioid infusions ceteris paribus for at least 24 hours postoperatively. Studies were limited to opioids used in common practice, which include morphine, fentanyl, hydromorphone, oxycodone, or sufentanil. In most cases, opioids were combined with local anesthetics. Studies were excluded if comparisons involved only varying concentra-tions of the same opioid or various types of local anesthetics.
OutcomesAnalgesia in terms of VAS pain scores measured for at least 24 hours was the primary outcome. Secondary outcomes included opioid side effects, such as nausea/vomiting, pru-ritus, and respiratory depression. No a priori definition was set for the latter, although in the majority of studies it was defined as administration of naloxone.
Study DesignOnly RCTs were included in our review, regardless of the quality of assessment or results. Crossover trials were not included due to the potential for inadequate washout period between compared opioids.
Study EvaluationEach study included in the analysis was assessed indepen-dently by each author, and any discrepancies were resolved
by consensus. The assessment was performed using a modi-fied version of the 5-point methodological quality scale designed by Jadad et al.10 To receive full points, a study had to meet the following criteria: be randomized; be double-blind; include appropriate follow-up for 24 hours at a mini-mum; use suitable techniques to create the randomization sequence; and describe an acceptable blinding method. To satisfy the follow-up criteria of the modified Jadad scale, withdrawals/dropouts must be described or all study par-ticipants accounted for in the results.10 Funnel plots were constructed of the primary outcome to evaluate for publica-tion bias.
Data ExtractionThe methodological data were extracted and later veri-fied. The extracted methodological data included the type of surgery and detail of the anesthetics. Medications used at induction, maintenance, and emergence were recorded. Descriptions of the epidural included the level of insertion, initiation of the epidural within the delivery of anesthesia, and time course for epidural administration. Additionally, the number and baseline characteristics of subjects in each treatment group were recorded. Numerical data were extracted and also verified. These data included VAS pain scores at rest (primary outcome) and incidence of opioid-related side effects (secondary outcomes). Pain scores could not be extracted from the study by Coppe and Willaert11 because poor graphical quality precluded differentiation of the treatment arms. Numerous attempts to contact the authors were unsuccessful, and only partial data (concern-ing opioid side effects) were included.
Statistical AnalysisThe reporting of this review was done in accordance with the PRISMA guideline.12 The selection process for articles is summarized using a flow diagram. Due to interstudy variability in the timing of pain assessment, pain scores were grouped in 6- to 8-hour intervals where necessary. In cases where the standard deviation (SD) was not reported, it was derived from range or interquartile range. When studies reported multiple infusion rates for the same opi-oid, data for the most equipotent dose (the one most simi-lar to the comparison opioid in the trial) were retained for analysis. Categorical outcomes (e.g., none, mild, and severe) were converted into binary data by summing the number of patients who experienced the outcome, regardless of severity.
Due to the known dose dependency of opioid analge-sia and side effects,13 we conducted subgroup analyses to explore (1) whether equipotent infusion rates were used within individual studies and (2) whether comparable doses of the same opioid were used among studies. Equipotency was determined by comparing the relative average rates of infusion within a study to epidural equianalgesic tables.14 Total opioid consumption was also analyzed for studies that administered opioids via equianalgesic infusions and a non-fixed amount of opioid.
Under each predefined clinical outcome, the eligible studies with available data were pooled using the random-effects model, which incorporated statistical heterogeneity. The weight of each individual study was calculated using

Copyright © 2014 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
XXX 2014 Volume XXX Number XXX www.anesthesia-analgesia.org 3
the inverse-variance method. The overall pooled estimates were reported as weighted mean difference and odds ratio with the associated confidence intervals for continuous and dichotomous outcomes, respectively. The statistical hetero-geneity was quantified as the I2 statistic, which measures the between-study variance as a percentage of total vari-ance. The Q test was used to test heterogeneity. The criteria used to define statistical significance were set at α = 0.01 for continuous data (because there were multiple comparisons over time) and α = 0.05 for dichotomous data. The over-all pooled estimates and individual studies included were graphically presented using forest plots. Bias was assessed through funnel plots and Egger’s regression. Stata 12.0 (StataCorp, College Station, TX) was used to conduct the meta-analyses and assessment of bias.
A Priori Hypothesis for Sources of HeterogeneityBefore analyzing the results, potential sources of heterogene-ity among studies were identified, and hypotheses were for-mulated to explain this heterogeneity. Much of the possible heterogeneity from RCTs comparing opioids was thought to depend on dose dependency of opioid analgesia and side effects.13 First, inconsistent use of analgesic adjuncts (nonste-roidal anti-inflammatory drugs or local anesthetics) among studies may result in an opioid-sparing effect, which may decrease rates of side effects and give rise to synergistic or additive benefits.15 Second, deviation from equianalgesic dosing within a study may inflate the number of side effects in patients receiving inappropriately large amounts of opi-oid or increase pain in those receiving too little. Third, it is important to consider the infusion rates of the same opioid between each study, which in some cases varied by approxi-mately 10-fold. Higher rates of infusion may lead to better analgesia and a higher incidence of side effects.13
In addition to factors related to opioid dosage, addi-tional anesthetic and surgical factors should be consid-ered. Intraoperative factors include administration of any antipruritic or antiemetic medication. Furthermore, certain anesthetic drugs are associated with particular side effects, such as nitrous oxide and postoperative nausea and vomit-ing (PONV).16 In addition, administration of opioids intra-operatively may raise the risk of side effects in 1 group if it is unevenly distributed.13 With respect to the type of sur-gery, certain procedures are more invasive than others and thus may give rise to more postoperative pain, leading to increased opioid consumption and systemic side effects.13,17 Additionally, thoracic surgery has relatively higher rates of postoperative respiratory complications compared with other types of operations.18 With respect to data reporting, continuous versus dichotomous outcome measures may give rise to differences in side effect profiles among patients, due to the higher sensitivity of a continuous scale to detect a difference.
With regard to pediatric studies, the measurement of pain in pediatric patients relies on assessing cues, such as crying or facial expression.19 These third-person methods may differ in sensitivity from the standard VAS adminis-tered to adult patients.19 Furthermore, pediatric patients as a group are heterogeneous and experience different rates of side effects based on age.20 Thus, for these reasons, pediatric studies were analyzed separately.
RESULTSLiterature SearchThe initial search retrieved 8219 articles. After title review, 113 studies were retained for abstract and/or full-text review (Fig. 1). Ultimately, 24 of these studies met the inclu-sion criteria (Table 1).11,21–43
Study DescriptionNineteen studies obtained a Jadad quality score of 3/5 or higher. The most common methodological shortcomings were failure to fully describe the randomization or blinding technique.
Abdominal, orthopedic, and cesarean delivery with non-laboring epidural accounted for 10, 7, and 2 of the 24 stud-ies, respectively. Five trials included a mix of abdominal or thoracic surgery. Of the 24 studies, 2 included pediatric patients.
Sufficient data were available to analyze the following secondary outcomes: nausea and vomiting (24/24), pruritus (22/24), respiratory depression (19/24), sedation (17/24), and hypotension (9/24).
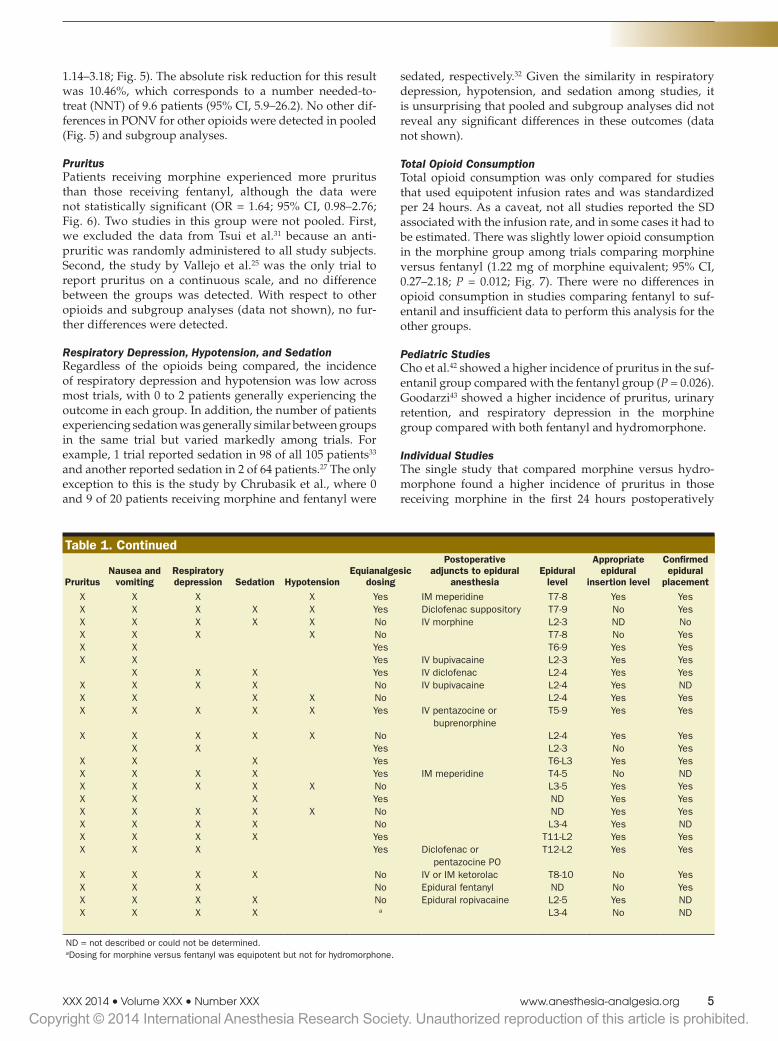
Most studies described confirmation of epidural catheter placement (18/24) at a spinal level appropriate for the spe-cific operations reported (16/24) (Table 1).44 In addition, the majority of trials made a binary comparison between two different opioids, except the pediatric study by Goodarzi that compared morphine, fentanyl, and hydromorphone (Table 1).43
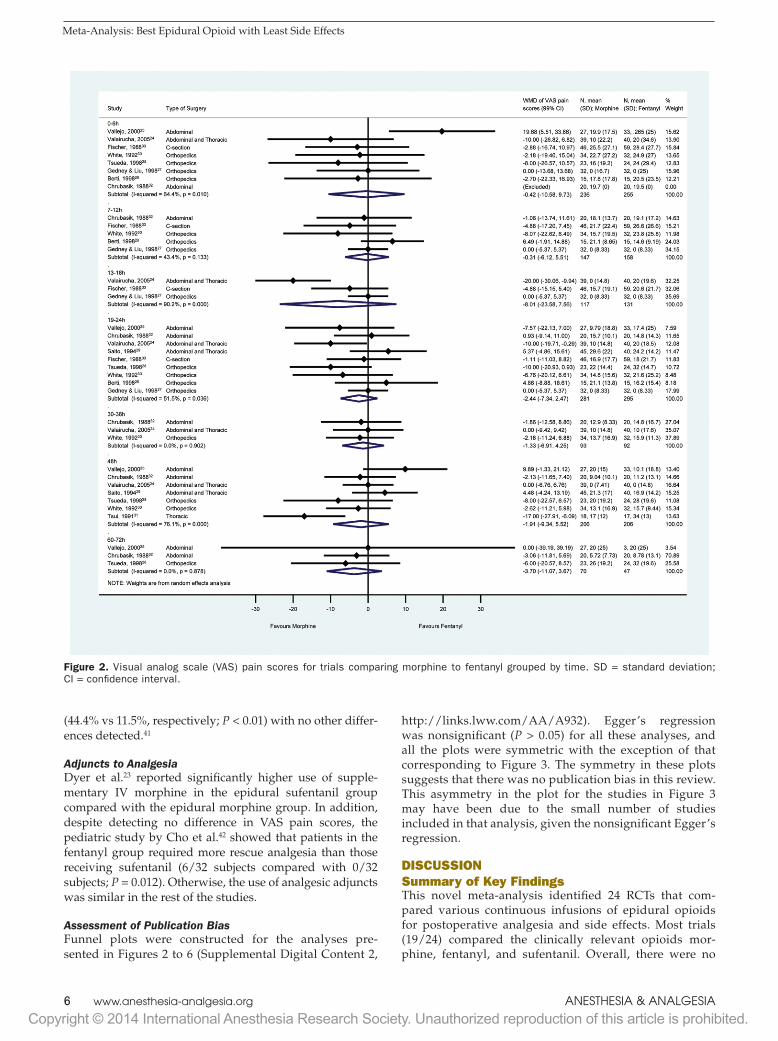
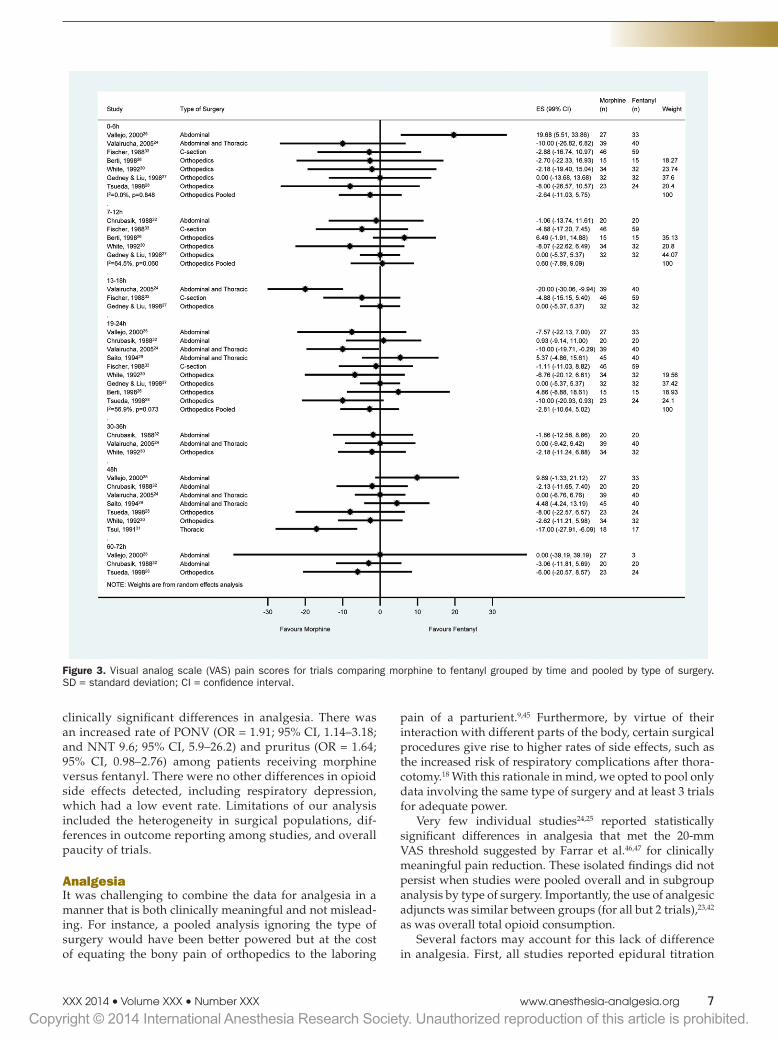
Primary Outcome: VAS Pain ScoresPain scores were compared for at least the first 24 hours among various intervals of time, if pain was assessed dur-ing that interval. For trials comparing morphine to fentanyl, pooled analysis revealed significant heterogeneity at the 0 to 6, 13 to 18, 19 to 24, and 48-hour time intervals. Given the overall small number of studies, this heterogeneity appeared to be primarily driven by certain individual stud-ies that showed significant pain reduction in favor of either opioid (Fig. 2).24–26,28,31 Subgroup analysis by type of surgery significantly reduced the amount of heterogeneity at these time points (Fig. 3). Care was taken not to pool studies in this subgroup analysis unless there were at least 3 studies comparing the same type of surgery at that time interval, in order to avoid presenting a misleading pooled estimate.
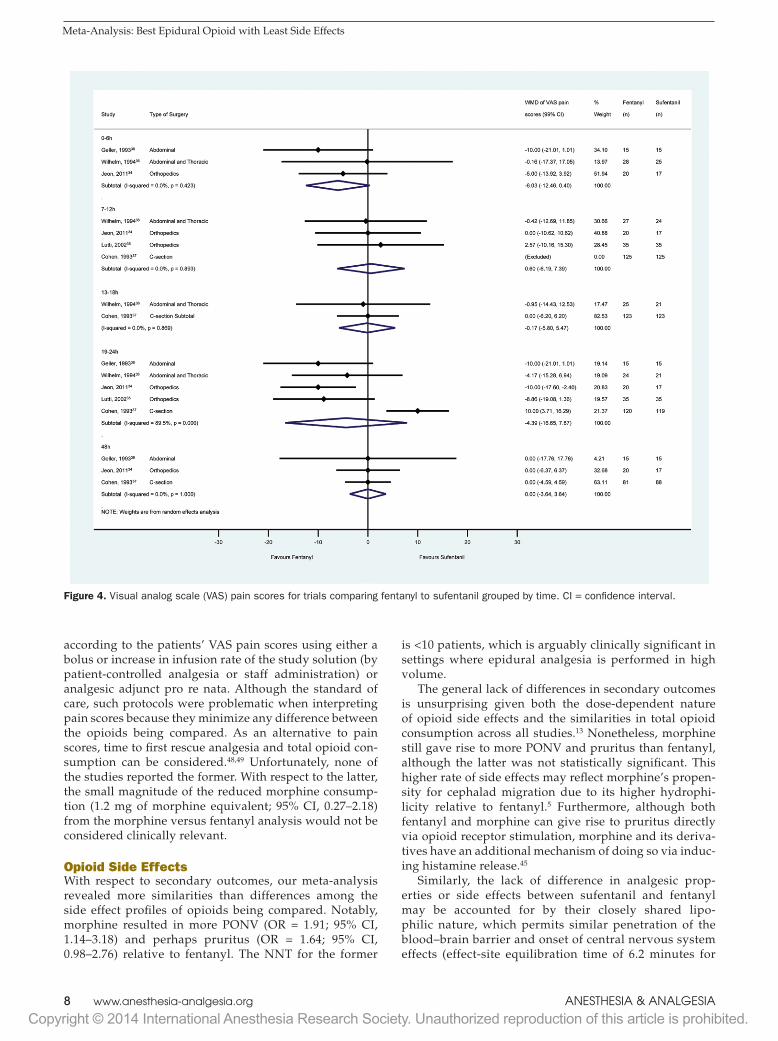
There was no significant difference between pain scores for fentanyl versus sufentanil (Fig. 4). The significant het-erogeneity at the 19- to 24-hour time interval was likely driven by the single discordant study that favored sufent-anil.37 Subgroup analysis was not feasible given the small number of studies.
Other comparisons involving morphine versus either sufentanil or oxycodone did not reveal any differences (data not shown). There were also no differences detected by the single adult study comparing morphine to hydromorphone and 2 pediatric studies that compared the same opioids.41–43
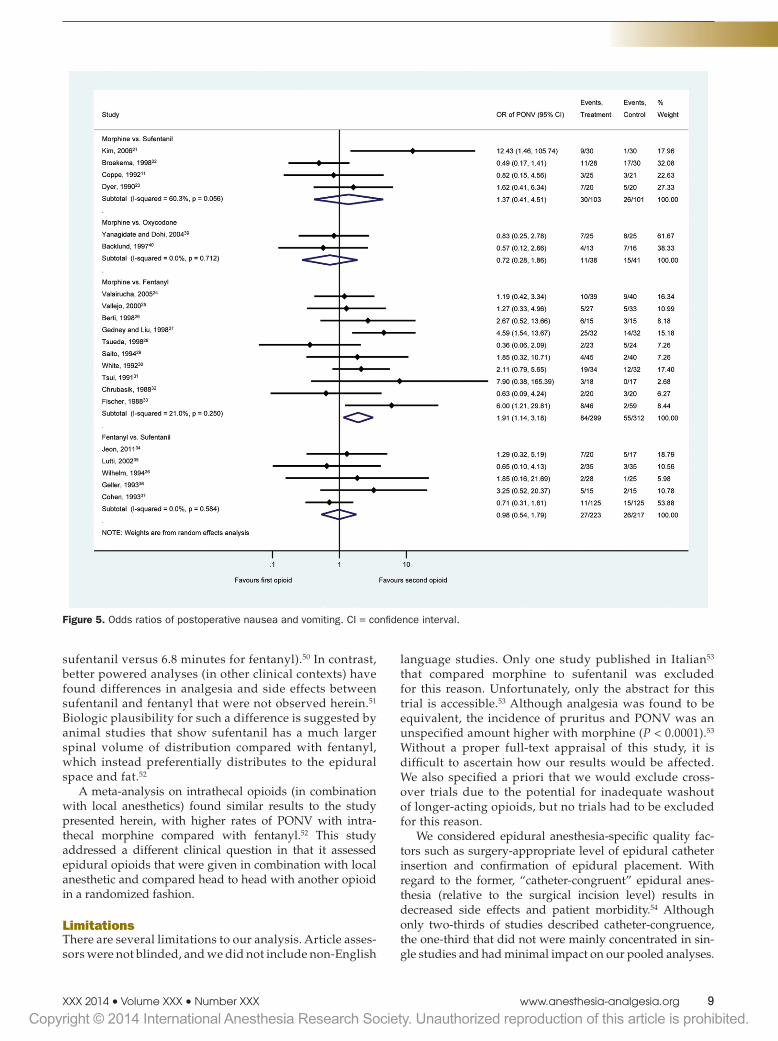
Secondary OutcomesPostoperative Nausea and VomitingThere was a higher incidence of PONV in patients receiv-ing morphine compared with fentanyl (OR = 1.91; 95% CI,

Copyright © 2014 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.4 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Meta-Analysis: Best Epidural Opioid with Least Side Effects
Table 1. Description of Included Studies Table 1. Continued
Comparison ReferenceData extraction
sourceType of surgery
Total subjects
Jadad score
(out of 5) PruritusNausea and
vomitingRespiratory depression Sedation Hypotension
Equianalgesic dosing
Postoperative adjuncts to epidural
anesthesiaEpidural
level
Appropriate epidural
insertion level
Confirmed epidural
placementAdult
patientsMorphine vs sufentanil Kim et al.21 Tables and in-text Abdominal 60 5 X X X X Yes IM meperidine T7-8 Yes Yes
Broekema et al.22 Tables, figures, and in-text Abdominal 59 3 X X X X X Yes Diclofenac suppository T7-9 No YesDyer et al.23 Tables, figures, and in-text Abdominal 40 4 X X X X X No IV morphine L2-3 ND NoCoppe et al.11 Tables and in-text Abdominal 46 4 X X X X No T7-8 No Yes
Morphine vs fentanyl Valairucha et al.24 Tables and in-text Abdominal and thoracic 79 2 X X Yes T6-9 Yes YesVallejo et al.25 Tables, figures, and in-text Abdominal 60 3 X X Yes IV bupivacaine L2-3 Yes YesBerti et al.26 Tables, figures, and in-text Orthopedics 30 5 X X X Yes IV diclofenac L2-4 Yes YesGedney and Liu27 Tables, figures, and in-text Orthopedics 64 3 X X X X No IV bupivacaine L2-4 Yes NDTsueda et al.28 Tables and in-text Orthopedics 47 5 X X X X No L2-4 Yes YesSaito et al.29 Tables, figures, and in-text Abdominal and thoracic 85 2 X X X X X Yes IV pentazocine or
buprenorphineT5-9 Yes Yes
White et al.30 Figures and in-text Orthopedics 66 3 X X X X X No L2-4 Yes YesTsui et al.31 Tables and in-text Abdominal and thoracic 35 2 X X Yes L2-3 No YesChrubasik et al.32 Tables, figures, and in-text Abdominal 40 3 X X X Yes T6-L3 Yes YesFischer et al.33 Figures and in-text C-section 105 4 X X X X Yes IM meperidine T4-5 No ND
Fentanyl vs sufentanil Jeon et al.34 Tables, figures, and in-text Orthopedics 37 2 X X X X X No L3-5 Yes YesLutti et al.35 Tables and in-text Orthopedics 70 2 X X X Yes ND Yes YesWilhelm and Dieleman36 Tables, figures, and in-text Abdominal and thoracic 53 4 X X X X X No ND Yes YesCohen et al.37 Tables, figures, and in-text C-section 250 4 X X X X No L3-4 Yes NDGeller et al.38 Tables and in-text Abdominal 30 5 X X X X Yes T11-L2 Yes Yes
Morphine vs oxycodone Yanagidate and Dohi39 Tables, figures, and in-text Abdominal 50 4 X X X Yes Diclofenac or pentazocine PO
T12-L2 Yes Yes
Backlund et al.40 Figures and in-text Abdominal 29 5 X X X X No IV or IM ketorolac T8-10 No YesMorphine vs hydromorphone Chaplan et al.41 Figures and in-text Abdominal and thoracic 54 5 X X X No Epidural fentanyl ND No Yes
Peds Fentanyl vs sufentanil Cho et al.42 Tables and in-text Abdominal 64 5 X X X X No Epidural ropivacaine L2-5 Yes NDMorphine vs fentanyl vs
hydromorphoneGoodarzi43 Tables, figures, and in-text Orthopedics 60 3 X X X X a L3-4 No ND
ND = not described or could not be determined.aDosing for morphine versus fentanyl was equipotent but not for hydromorphone.
Figure 1. PRISMA flow sheet describing the study selection process.
Copyright © 2014 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
XXX 2014 Volume XXX Number XXX www.anesthesia-analgesia.org 5
1.14–3.18; Fig. 5). The absolute risk reduction for this result was 10.46%, which corresponds to a number needed-to-treat (NNT) of 9.6 patients (95% CI, 5.9–26.2). No other dif-ferences in PONV for other opioids were detected in pooled (Fig. 5) and subgroup analyses.
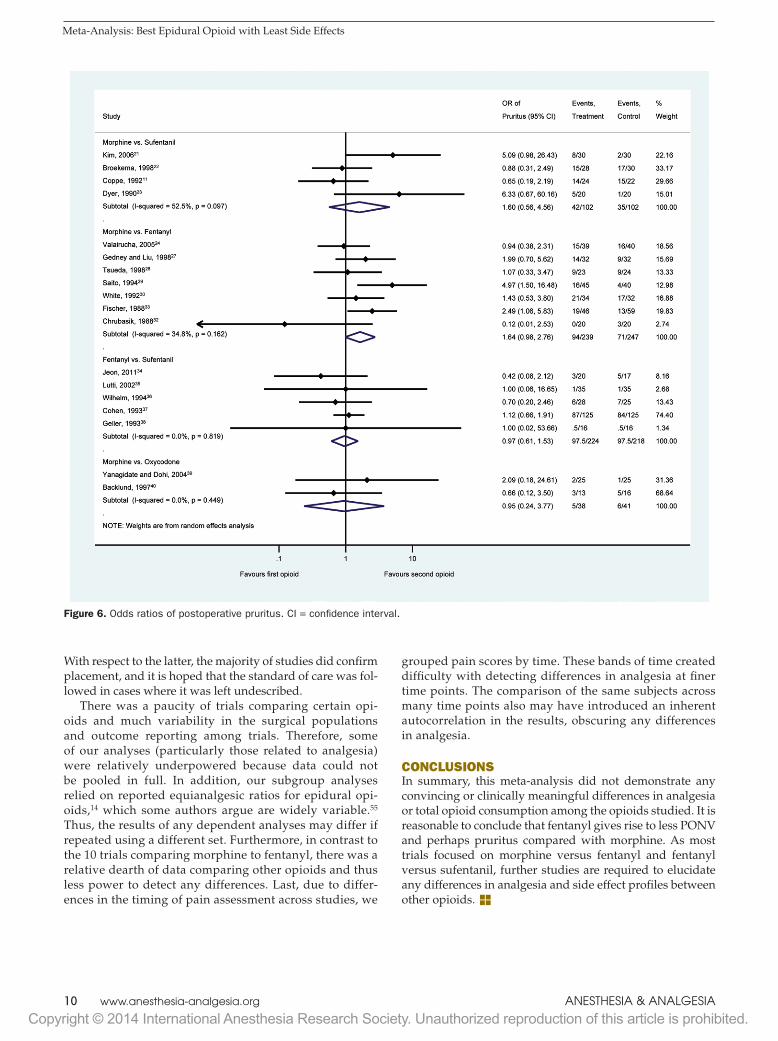
PruritusPatients receiving morphine experienced more pruritus than those receiving fentanyl, although the data were not statistically significant (OR = 1.64; 95% CI, 0.98–2.76; Fig. 6). Two studies in this group were not pooled. First, we excluded the data from Tsui et al.31 because an anti-pruritic was randomly administered to all study subjects. Second, the study by Vallejo et al.25 was the only trial to report pruritus on a continuous scale, and no difference between the groups was detected. With respect to other opioids and subgroup analyses (data not shown), no fur-ther differences were detected.
Respiratory Depression, Hypotension, and SedationRegardless of the opioids being compared, the incidence of respiratory depression and hypotension was low across most trials, with 0 to 2 patients generally experiencing the outcome in each group. In addition, the number of patients experiencing sedation was generally similar between groups in the same trial but varied markedly among trials. For example, 1 trial reported sedation in 98 of all 105 patients33 and another reported sedation in 2 of 64 patients.27 The only exception to this is the study by Chrubasik et al., where 0 and 9 of 20 patients receiving morphine and fentanyl were
sedated, respectively.32 Given the similarity in respiratory depression, hypotension, and sedation among studies, it is unsurprising that pooled and subgroup analyses did not reveal any significant differences in these outcomes (data not shown).
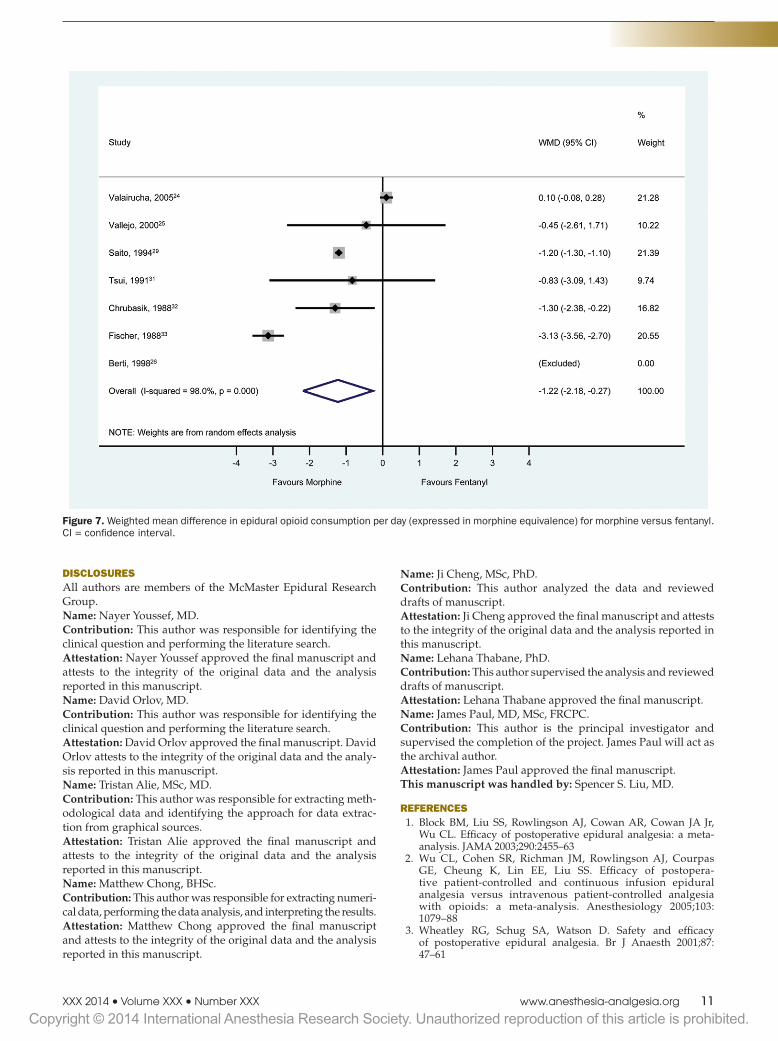
Total Opioid ConsumptionTotal opioid consumption was only compared for studies that used equipotent infusion rates and was standardized per 24 hours. As a caveat, not all studies reported the SD associated with the infusion rate, and in some cases it had to be estimated. There was slightly lower opioid consumption in the morphine group among trials comparing morphine versus fentanyl (1.22 mg of morphine equivalent; 95% CI, 0.27–2.18; P = 0.012; Fig. 7). There were no differences in opioid consumption in studies comparing fentanyl to suf-entanil and insufficient data to perform this analysis for the other groups.
Pediatric StudiesCho et al.42 showed a higher incidence of pruritus in the suf-entanil group compared with the fentanyl group (P = 0.026). Goodarzi43 showed a higher incidence of pruritus, urinary retention, and respiratory depression in the morphine group compared with both fentanyl and hydromorphone.
Individual StudiesThe single study that compared morphine versus hydro-morphone found a higher incidence of pruritus in those receiving morphine in the first 24 hours postoperatively
Table 1. Description of Included Studies Table 1. Continued
Comparison ReferenceData extraction
sourceType of surgery
Total subjects
Jadad score
(out of 5) PruritusNausea and
vomitingRespiratory depression Sedation Hypotension
Equianalgesic dosing
Postoperative adjuncts to epidural
anesthesiaEpidural
level
Appropriate epidural
insertion level
Confirmed epidural
placementAdult
patientsMorphine vs sufentanil Kim et al.21 Tables and in-text Abdominal 60 5 X X X X Yes IM meperidine T7-8 Yes Yes
Broekema et al.22 Tables, figures, and in-text Abdominal 59 3 X X X X X Yes Diclofenac suppository T7-9 No YesDyer et al.23 Tables, figures, and in-text Abdominal 40 4 X X X X X No IV morphine L2-3 ND NoCoppe et al.11 Tables and in-text Abdominal 46 4 X X X X No T7-8 No Yes
Morphine vs fentanyl Valairucha et al.24 Tables and in-text Abdominal and thoracic 79 2 X X Yes T6-9 Yes YesVallejo et al.25 Tables, figures, and in-text Abdominal 60 3 X X Yes IV bupivacaine L2-3 Yes YesBerti et al.26 Tables, figures, and in-text Orthopedics 30 5 X X X Yes IV diclofenac L2-4 Yes YesGedney and Liu27 Tables, figures, and in-text Orthopedics 64 3 X X X X No IV bupivacaine L2-4 Yes NDTsueda et al.28 Tables and in-text Orthopedics 47 5 X X X X No L2-4 Yes YesSaito et al.29 Tables, figures, and in-text Abdominal and thoracic 85 2 X X X X X Yes IV pentazocine or
buprenorphineT5-9 Yes Yes
White et al.30 Figures and in-text Orthopedics 66 3 X X X X X No L2-4 Yes YesTsui et al.31 Tables and in-text Abdominal and thoracic 35 2 X X Yes L2-3 No YesChrubasik et al.32 Tables, figures, and in-text Abdominal 40 3 X X X Yes T6-L3 Yes YesFischer et al.33 Figures and in-text C-section 105 4 X X X X Yes IM meperidine T4-5 No ND
Fentanyl vs sufentanil Jeon et al.34 Tables, figures, and in-text Orthopedics 37 2 X X X X X No L3-5 Yes YesLutti et al.35 Tables and in-text Orthopedics 70 2 X X X Yes ND Yes YesWilhelm and Dieleman36 Tables, figures, and in-text Abdominal and thoracic 53 4 X X X X X No ND Yes YesCohen et al.37 Tables, figures, and in-text C-section 250 4 X X X X No L3-4 Yes NDGeller et al.38 Tables and in-text Abdominal 30 5 X X X X Yes T11-L2 Yes Yes
Morphine vs oxycodone Yanagidate and Dohi39 Tables, figures, and in-text Abdominal 50 4 X X X Yes Diclofenac or pentazocine PO
T12-L2 Yes Yes
Backlund et al.40 Figures and in-text Abdominal 29 5 X X X X No IV or IM ketorolac T8-10 No YesMorphine vs hydromorphone Chaplan et al.41 Figures and in-text Abdominal and thoracic 54 5 X X X No Epidural fentanyl ND No Yes
Peds Fentanyl vs sufentanil Cho et al.42 Tables and in-text Abdominal 64 5 X X X X No Epidural ropivacaine L2-5 Yes NDMorphine vs fentanyl vs
hydromorphoneGoodarzi43 Tables, figures, and in-text Orthopedics 60 3 X X X X a L3-4 No ND
ND = not described or could not be determined.aDosing for morphine versus fentanyl was equipotent but not for hydromorphone.
Copyright © 2014 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.6 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Meta-Analysis: Best Epidural Opioid with Least Side Effects
(44.4% vs 11.5%, respectively; P < 0.01) with no other differ-ences detected.41
Adjuncts to AnalgesiaDyer et al.23 reported significantly higher use of supple-mentary IV morphine in the epidural sufentanil group compared with the epidural morphine group. In addition, despite detecting no difference in VAS pain scores, the pediatric study by Cho et al.42 showed that patients in the fentanyl group required more rescue analgesia than those receiving sufentanil (6/32 subjects compared with 0/32 subjects; P = 0.012). Otherwise, the use of analgesic adjuncts was similar in the rest of the studies.
Assessment of Publication BiasFunnel plots were constructed for the analyses pre-sented in Figures 2 to 6 (Supplemental Digital Content 2,
http://links.lww.com/AA/A932). Egger’s regression was nonsignificant (P > 0.05) for all these analyses, and all the plots were symmetric with the exception of that corresponding to Figure 3. The symmetry in these plots suggests that there was no publication bias in this review. This asymmetry in the plot for the studies in Figure 3 may have been due to the small number of studies included in that analysis, given the nonsignificant Egger’s regression.
DISCUSSIONSummary of Key FindingsThis novel meta-analysis identified 24 RCTs that com-pared various continuous infusions of epidural opioids for postoperative analgesia and side effects. Most trials (19/24) compared the clinically relevant opioids mor-phine, fentanyl, and sufentanil. Overall, there were no
Figure 2. Visual analog scale (VAS) pain scores for trials comparing morphine to fentanyl grouped by time. SD = standard deviation; CI = confidence interval.
Copyright © 2014 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
XXX 2014 Volume XXX Number XXX www.anesthesia-analgesia.org 7
clinically significant differences in analgesia. There was an increased rate of PONV (OR = 1.91; 95% CI, 1.14–3.18; and NNT 9.6; 95% CI, 5.9–26.2) and pruritus (OR = 1.64; 95% CI, 0.98–2.76) among patients receiving morphine versus fentanyl. There were no other differences in opioid side effects detected, including respiratory depression, which had a low event rate. Limitations of our analysis included the heterogeneity in surgical populations, dif-ferences in outcome reporting among studies, and overall paucity of trials.
AnalgesiaIt was challenging to combine the data for analgesia in a manner that is both clinically meaningful and not mislead-ing. For instance, a pooled analysis ignoring the type of surgery would have been better powered but at the cost of equating the bony pain of orthopedics to the laboring
pain of a parturient.9,45 Furthermore, by virtue of their interaction with different parts of the body, certain surgical procedures give rise to higher rates of side effects, such as the increased risk of respiratory complications after thora-cotomy.18 With this rationale in mind, we opted to pool only data involving the same type of surgery and at least 3 trials for adequate power.
Very few individual studies24,25 reported statistically significant differences in analgesia that met the 20-mm VAS threshold suggested by Farrar et al.46,47 for clinically meaningful pain reduction. These isolated findings did not persist when studies were pooled overall and in subgroup analysis by type of surgery. Importantly, the use of analgesic adjuncts was similar between groups (for all but 2 trials),23,42 as was overall total opioid consumption.
Several factors may account for this lack of difference in analgesia. First, all studies reported epidural titration
Figure 3. Visual analog scale (VAS) pain scores for trials comparing morphine to fentanyl grouped by time and pooled by type of surgery. SD = standard deviation; CI = confidence interval.
Copyright © 2014 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.8 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Meta-Analysis: Best Epidural Opioid with Least Side Effects
according to the patients’ VAS pain scores using either a bolus or increase in infusion rate of the study solution (by patient-controlled analgesia or staff administration) or analgesic adjunct pro re nata. Although the standard of care, such protocols were problematic when interpreting pain scores because they minimize any difference between the opioids being compared. As an alternative to pain scores, time to first rescue analgesia and total opioid con-sumption can be considered.48,49 Unfortunately, none of the studies reported the former. With respect to the latter, the small magnitude of the reduced morphine consump-tion (1.2 mg of morphine equivalent; 95% CI, 0.27–2.18) from the morphine versus fentanyl analysis would not be considered clinically relevant.
Opioid Side EffectsWith respect to secondary outcomes, our meta-analysis revealed more similarities than differences among the side effect profiles of opioids being compared. Notably, morphine resulted in more PONV (OR = 1.91; 95% CI, 1.14–3.18) and perhaps pruritus (OR = 1.64; 95% CI, 0.98–2.76) relative to fentanyl. The NNT for the former
is <10 patients, which is arguably clinically significant in settings where epidural analgesia is performed in high volume.
The general lack of differences in secondary outcomes is unsurprising given both the dose-dependent nature of opioid side effects and the similarities in total opioid consumption across all studies.13 Nonetheless, morphine still gave rise to more PONV and pruritus than fentanyl, although the latter was not statistically significant. This higher rate of side effects may reflect morphine’s propen-sity for cephalad migration due to its higher hydrophi-licity relative to fentanyl.5 Furthermore, although both fentanyl and morphine can give rise to pruritus directly via opioid receptor stimulation, morphine and its deriva-tives have an additional mechanism of doing so via induc-ing histamine release.45
Similarly, the lack of difference in analgesic prop-erties or side effects between sufentanil and fentanyl may be accounted for by their closely shared lipo-philic nature, which permits similar penetration of the blood–brain barrier and onset of central nervous system effects (effect-site equilibration time of 6.2 minutes for
Figure 4. Visual analog scale (VAS) pain scores for trials comparing fentanyl to sufentanil grouped by time. CI = confidence interval.
Copyright © 2014 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
XXX 2014 Volume XXX Number XXX www.anesthesia-analgesia.org 9
sufentanil versus 6.8 minutes for fentanyl).50 In contrast, better powered analyses (in other clinical contexts) have found differences in analgesia and side effects between sufentanil and fentanyl that were not observed herein.51 Biologic plausibility for such a difference is suggested by animal studies that show sufentanil has a much larger spinal volume of distribution compared with fentanyl, which instead preferentially distributes to the epidural space and fat.52
A meta-analysis on intrathecal opioids (in combination with local anesthetics) found similar results to the study presented herein, with higher rates of PONV with intra-thecal morphine compared with fentanyl.52 This study addressed a different clinical question in that it assessed epidural opioids that were given in combination with local anesthetic and compared head to head with another opioid in a randomized fashion.
LimitationsThere are several limitations to our analysis. Article asses-sors were not blinded, and we did not include non-English
language studies. Only one study published in Italian53 that compared morphine to sufentanil was excluded for this reason. Unfortunately, only the abstract for this trial is accessible.53 Although analgesia was found to be equivalent, the incidence of pruritus and PONV was an unspecified amount higher with morphine (P < 0.0001).53 Without a proper full-text appraisal of this study, it is difficult to ascertain how our results would be affected. We also specified a priori that we would exclude cross-over trials due to the potential for inadequate washout of longer-acting opioids, but no trials had to be excluded for this reason.
We considered epidural anesthesia-specific quality fac-tors such as surgery-appropriate level of epidural catheter insertion and confirmation of epidural placement. With regard to the former, “catheter-congruent” epidural anes-thesia (relative to the surgical incision level) results in decreased side effects and patient morbidity.54 Although only two-thirds of studies described catheter-congruence, the one-third that did not were mainly concentrated in sin-gle studies and had minimal impact on our pooled analyses.
Figure 5. Odds ratios of postoperative nausea and vomiting. CI = confidence interval.
Copyright © 2014 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.10 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Meta-Analysis: Best Epidural Opioid with Least Side Effects
With respect to the latter, the majority of studies did confirm placement, and it is hoped that the standard of care was fol-lowed in cases where it was left undescribed.
There was a paucity of trials comparing certain opi-oids and much variability in the surgical populations and outcome reporting among trials. Therefore, some of our analyses (particularly those related to analgesia) were relatively underpowered because data could not be pooled in full. In addition, our subgroup analyses relied on reported equianalgesic ratios for epidural opi-oids,14 which some authors argue are widely variable.55 Thus, the results of any dependent analyses may differ if repeated using a different set. Furthermore, in contrast to the 10 trials comparing morphine to fentanyl, there was a relative dearth of data comparing other opioids and thus less power to detect any differences. Last, due to differ-ences in the timing of pain assessment across studies, we
grouped pain scores by time. These bands of time created difficulty with detecting differences in analgesia at finer time points. The comparison of the same subjects across many time points also may have introduced an inherent autocorrelation in the results, obscuring any differences in analgesia.
CONCLUSIONSIn summary, this meta-analysis did not demonstrate any convincing or clinically meaningful differences in analgesia or total opioid consumption among the opioids studied. It is reasonable to conclude that fentanyl gives rise to less PONV and perhaps pruritus compared with morphine. As most trials focused on morphine versus fentanyl and fentanyl versus sufentanil, further studies are required to elucidate any differences in analgesia and side effect profiles between other opioids. E
Figure 6. Odds ratios of postoperative pruritus. CI = confidence interval.
Copyright © 2014 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
XXX 2014 Volume XXX Number XXX www.anesthesia-analgesia.org 11
DISCLOSURESAll authors are members of the McMaster Epidural Research Group.Name: Nayer Youssef, MD.Contribution: This author was responsible for identifying the clinical question and performing the literature search.Attestation: Nayer Youssef approved the final manuscript and attests to the integrity of the original data and the analysis reported in this manuscript.Name: David Orlov, MD.Contribution: This author was responsible for identifying the clinical question and performing the literature search.Attestation: David Orlov approved the final manuscript. David Orlov attests to the integrity of the original data and the analy-sis reported in this manuscript.Name: Tristan Alie, MSc, MD.Contribution: This author was responsible for extracting meth-odological data and identifying the approach for data extrac-tion from graphical sources.Attestation: Tristan Alie approved the final manuscript and attests to the integrity of the original data and the analysis reported in this manuscript.Name: Matthew Chong, BHSc.Contribution: This author was responsible for extracting numeri-cal data, performing the data analysis, and interpreting the results.Attestation: Matthew Chong approved the final manuscript and attests to the integrity of the original data and the analysis reported in this manuscript.
Name: Ji Cheng, MSc, PhD.Contribution: This author analyzed the data and reviewed drafts of manuscript.Attestation: Ji Cheng approved the final manuscript and attests to the integrity of the original data and the analysis reported in this manuscript.Name: Lehana Thabane, PhD.Contribution: This author supervised the analysis and reviewed drafts of manuscript.Attestation: Lehana Thabane approved the final manuscript.Name: James Paul, MD, MSc, FRCPC.Contribution: This author is the principal investigator and supervised the completion of the project. James Paul will act as the archival author.Attestation: James Paul approved the final manuscript.This manuscript was handled by: Spencer S. Liu, MD.
REFERENCES 1. Block BM, Liu SS, Rowlingson AJ, Cowan AR, Cowan JA Jr,
Wu CL. Efficacy of postoperative epidural analgesia: a meta- analysis. JAMA 2003;290:2455–63
2. Wu CL, Cohen SR, Richman JM, Rowlingson AJ, Courpas GE, Cheung K, Lin EE, Liu SS. Efficacy of postopera-tive patient-controlled and continuous infusion epidural analgesia versus intravenous patient-controlled analgesia with opioids: a meta-analysis. Anesthesiology 2005;103: 1079–88
3. Wheatley RG, Schug SA, Watson D. Safety and efficacy of postoperative epidural analgesia. Br J Anaesth 2001;87: 47–61
Figure 7. Weighted mean difference in epidural opioid consumption per day (expressed in morphine equivalence) for morphine versus fentanyl. CI = confidence interval.
Copyright © 2014 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.12 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Meta-Analysis: Best Epidural Opioid with Least Side Effects
4. Gourlay GK, Cherry DA, Cousins MJ. Cephalad migration of morphine in CSF following lumbar epidural administration in patients with cancer pain. Pain 1985;23:317–26
5. Bromage PR, Camporesi EM, Durant PA, Nielsen CH. Rostral spread of epidural morphine. Anesthesiology 1982;56:431–6
6. de Leon-Casasola OA, Lema MJ. Postoperative epidural opioid analgesia: what are the choices? Anesth Analg 1996;83:867–75
7. Roy SD, Flynn GL. Solubility and related physicochemical properties of narcotic analgesics. Pharm Res 1988;5:580–6
8. Haynes RB, Wilczynski N, McKibbon KA, Walker CJ, Sinclair JC. Developing optimal search strategies for detecting clini-cally sound studies in MEDLINE. J Am Med Inform Assoc 1994;1:447–58
9. Lowe NK. The nature of labor pain. Am J Obstet Gynecol 2002;186:S16–24
10. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 1996;17:1–12
11. Coppe E, Willaert J. Postoperative analgesia for major abdomi-nal surgery with continuous thoracic epidural infusion of bupi-vacaine with sufentanil, versus bupivacaine with morphine. A randomized double blind study. Acta Anaesthesiol Belg 1992;43:131–7
12. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interven-tions: explanation and elaboration. J Clin Epidemiol 2009;62: e1–34
13. Chaney MA. Side effects of intrathecal and epidural opioids. Can J Anaesth 1995;42:891–903
14. Cousins MJ, Bridenbaugh PO, Carr DB, Horlocker TT. Cousins and Bridenbaugh’s Neural Blockade in Clinical Anesthesia and Pain Medicine. 4th ed. China. Philadelphia, PA: Lippincott Williams & Wilkins, 2008
15. Chen JY, Ko TL, Wen YR, Wu SC, Chou YH, Yien HW, Kuo CD. Opioid-sparing effects of ketorolac and its correlation with the recovery of postoperative bowel function in colorectal surgery patients: a prospective randomized double-blinded study. Clin J Pain 2009;25:485–9
16. Tramèr M, Moore A, McQuay H. Omitting nitrous oxide in general anaesthesia: meta-analysis of intraoperative awareness and postoperative emesis in randomized controlled trials. Br J Anaesth 1996;76:186–93
17. Unruh AM. Gender variations in clinical pain experience. Pain 1996;65:123–67
18. Nomori H, Kobayashi R, Fuyuno G, Morinaga S, Yashima H. Preoperative respiratory muscle training. Assessment in tho-racic surgery patients with special reference to postoperative pulmonary complications. Chest 1994;105:1782–8
19. Manworren RC, Hynan LS. Clinical validation of FLACC: pre-verbal patient pain scale. Pediatr Nurs 2003;29:140–6
20. Cohen MM, Cameron CB, Duncan PG. Pediatric anesthesia morbidity and mortality in the perioperative period. Anesth Analg 1990;70:160–7
21. Kim JY, Lee SJ, Koo BN, Noh SH, Kil HK, Kim HS, Ban SY. The effect of epidural sufentanil in ropivacaine on urinary retention in patients undergoing gastrectomy. Br J Anaesth 2006;97:414–8
22. Broekema AA, Veen A, Fidler V, Gielen MJ, Hennis PJ. Postoperative analgesia with intramuscular morphine at fixed rate versus epidural morphine or sufentanil and bupivacaine in patients undergoing major abdominal surgery. Anesth Analg 1998;87:1346–53
23. Dyer RA, Anderson BJ, Michell WL, Hall JM. Postoperative pain control with a continuous infusion of epidural sufentanil in the intensive care unit: a comparison with epidural mor-phine. Anesth Analg 1990;71:130–6
24. Valairucha S, Maboonvanon P, Napachoti T, Sirivanasandha B, Suraseranuvongse S. Cost-effectiveness of thoracic patient-controlled epidural analgesia using bupivacaine with fentanyl vs bupivacaine with morphine after thoracotomy and upper abdominal surgery. J Med Assoc Thai 2005;88:921–7
25. Vallejo MC, Edwards RP, Shannon KT, Kaul B, Finegold H, Morrison HL, Ramanathan S. Improved bowel function after gynecological surgery with epidural bupivacaine-fentanyl than bupivacaine-morphine infusion. Can J Anaesth 2000;47:406–11
26. Berti M, Fanelli G, Casati A, Lugani D, Aldegheri G, Torri G. Comparison between epidural infusion of fentanyl/bupiva-caine and morphine/bupivacaine after orthopaedic surgery. Can J Anaesth 1998;45:545–50
27. Gedney JA, Liu EH. Side-effects of epidural infusions of opioid bupivacaine mixtures. Anaesthesia 1998;53:1148–55
28. Tsueda K, Mosca PJ, Heine MF, Loyd GE, Durkis DA, Malkani AL, Hurst HE. Mood during epidural patient-controlled analge-sia with morphine or fentanyl. Anesthesiology 1998;88:885–91
29. Saito Y, Uchida H, Kaneko M, Nakatani T, Kosaka Y. Comparison of continuous epidural infusion of morphine/bupivacaine with fentanyl/bupivacaine for postoperative pain relief. Acta Anaesthesiol Scand 1994;38:398–401
30. White MJ, Berghausen EJ, Dumont SW, Tsueda K, Schroeder JA, Vogel RL, Heine MF, Huang KC. Side effects during continu-ous epidural infusion of morphine and fentanyl. Can J Anaesth 1992;39:576–82
31. Tsui SL, Chan CS, Chan AS, Wong SJ, Lam CS, Jones RD. Postoperative analgesia for oesophageal surgery: a com-parison of three analgesic regimens. Anaesth Intensive Care 1991;19:329–37
32. Chrubasik J, Wüst H, Schulte-Mönting J, Thon K, Zindler M. Relative analgesic potency of epidural fentanyl, alfentanil, and morphine in treatment of postoperative pain. Anesthesiology 1988;68:929–33
33. Fischer RL, Lubenow TR, Liceaga A, McCarthy RJ, Ivankovich AD. Comparison of continuous epidural infusion of fentanyl-bupivacaine and morphine-bupivacaine in management of postoperative pain. Anesth Analg 1988;67:559–63
34. Jeon HR, Chae WS, Lee SJ, Lee JH, Cho SH, Kim SH, Jin HC, Lee JS, Kim YI. A comparison of sufentanil and fentanyl for patient-controlled epidural analgesia in arthroplasty. Korean J Anesthesiol 2011;60:41–6
35. Lutti MN, Vieira JL, Eickhoff DR, de Carli D, de Carvalho MA. Patient controlled analgesia with fentanyl or sufentanil in the postoperative period of knee ligament reconstruction: compar-ative study. Rev Bras Anestesiol 2002;52:166–74
36. Wilhelm AJ, Dieleman HG. Epidural fentanyl and sufentanil for intra- and postoperative analgesia. A randomized, double-blind comparison. Pharm World Sci 1994;16:7–12
37. Cohen S, Amar D, Pantuck CB, Pantuck EJ, Goodman EJ, Widroff JS, Kanas RJ, Brady JA. Postcesarean delivery epi-dural patient-controlled analgesia. Fentanyl or sufentanil? Anesthesiology 1993;78:486–91
38. Geller E, Chrubasik J, Graf R, Chrubasik S, Schulte-Mönting J. A randomized double-blind comparison of epidural sufen-tanil versus intravenous sufentanil or epidural fentanyl anal-gesia after major abdominal surgery. Anesth Analg 1993;76: 1243–50
39. Yanagidate F, Dohi S. Epidural oxycodone or morphine follow-ing gynaecological surgery. Br J Anaesth 2004;93:362–7
40. Backlund M, Lindgren L, Kajimoto Y, Rosenberg PH. Comparison of epidural morphine and oxycodone for pain after abdominal surgery. J Clin Anesth 1997;9:30–5
41. Chaplan SR, Duncan SR, Brodsky JB, Brose WG. Morphine and hydromorphone epidural analgesia. A prospective, random-ized comparison. Anesthesiology 1992;77:1090–4
42. Cho JE, Kim JY, Kim JE, Chun DH, Jun NH, Kil HK. Epidural sufentanil provides better analgesia from 24 h after surgery compared with epidural fentanyl in children. Acta Anaesthesiol Scand 2008;52:1360–3
43. Goodarzi M. Comparison of epidural morphine, hydromor-phone and fentanyl for postoperative pain control in children undergoing orthopaedic surgery. Paediatr Anaesth 1999;9:419–22
44. Jaffe RA, Samuels SI. Anesthesiologist’s Manual of Surgical Procedures. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2009
45. Chelly JE, Ben-David B, Williams BA, Kentor ML. Anesthesia and postoperative analgesia: outcomes following orthopedic surgery. Orthopedics 2003;26:s865–71

Copyright © 2014 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
XXX 2014 Volume XXX Number XXX www.anesthesia-analgesia.org 13
46. Farrar JT, Berlin JA, Strom BL. Clinically important changes in acute pain outcome measures: a validation study. J Pain Symptom Manage 2003;25:406–11
47. Farrar JT, Portenoy RK, Berlin JA, Kinman JL, Strom BL. Defining the clinically important difference in pain outcome measures. Pain 2000;88:287–94
48. McQuay HJ. Pre-emptive analgesia. Br J Anaesth 1992;69:1–3 49. Ong CK, Lirk P, Seymour RA, Jenkins BJ. The efficacy of pre-
emptive analgesia for acute postoperative pain management: a meta-analysis. Anesth Analg 2005;100:757–73
50. Scott JC, Cooke JE, Stanski DR. Electroencephalographic quan-titation of opioid effect: comparative pharmacodynamics of fentanyl and sufentanil. Anesthesiology 1991;74:34–42
51. Davey J, Turner RM, Clarke MJ, Higgins JP. Characteristics of meta-analyses and their component studies in the Cochrane
Database of Systematic Reviews: a cross-sectional, descriptive analysis. BMC Med Res Methodol 2011;11:160
52. Pöpping DM, Elia N, Marret E, Wenk M, Tramèr MR. Opioids added to local anesthetics for single-shot intrathecal anesthesia in patients undergoing minor surgery: a meta-analysis of ran-domized trials. Pain 2012;153:784–93
53. Gianferrari P, Clara ME, Borghi B, Marzullo A, Voltolina M, De Paolis P, Montone N. [Sufentanil vs morphine combined with ropivacaine for thoracic epidural analgesia in major abdominal surgery]. Minerva Anestesiol 2001;67:155–9
54. Brown AK, Christo PJ, Wu CL. Strategies for postoperative pain management. Best Pract Res Clin Anaesthesiol 2004;18:703–17
55. Pereira J, Lawlor P, Vigano A, Dorgan M, Bruera E. Equianalgesic dose ratios for opioids. A critical review and proposals for long-term dosing. J Pain Symptom Manage 2001;22:672–87