what is the progression of contemporary periodontology for the rdh ... · contemporary...
TRANSCRIPT

Timothy J. Hempton, DDS
Periodontal Co-therapist 1
Contemporary Periodontology for the RDH.
Timothy J. Hempton, DDS Adjunct Clinical
Professor Tufts University School of Dental
Medicine
What is the progression of What is the progression of periodontal disease in the periodontal disease in the patient ?patient ?
6 Months
Non Non --Surgical TherapySurgical Therapy
••Mechanical TherapyMechanical Therapy
••Systemic Antibiotic TherapySystemic Antibiotic Therapy
••Local Antibiotic therapyLocal Antibiotic therapy
••Systemic Host modulation Systemic Host modulation therapytherapy-- PeriostatPeriostat
Subgingival Ultrasonic debridement results in disruption of the non-adherent flora effecting a qualitative change on subgingival plaque
Infrabony defects associated with maxillary molars are difficult to acesss
Non-surgical therapy and intrabony defects, how can we achieve effectiveness in these areas

Timothy J. Hempton, DDS
Periodontal Co-therapist 2
Are there limitations to Subgingival Are there limitations to Subgingival ScalingScaling and Root Planing?and Root Planing?
Antibiotic TherapyAntibiotic Therapy
Can Antibiotics helpCan Antibiotics help with these limitations?
Antibiotic TherapyAntibiotic Therapy
•Acute Infection•Acute Infection
•Chronic Infection
Systemic Antibiotic Systemic Antibiotic TherapyTherapyT t t f A t P i d t l DiTreatment of Acute Periodontal Disease
Treatment of Chronic Periodontal Disease
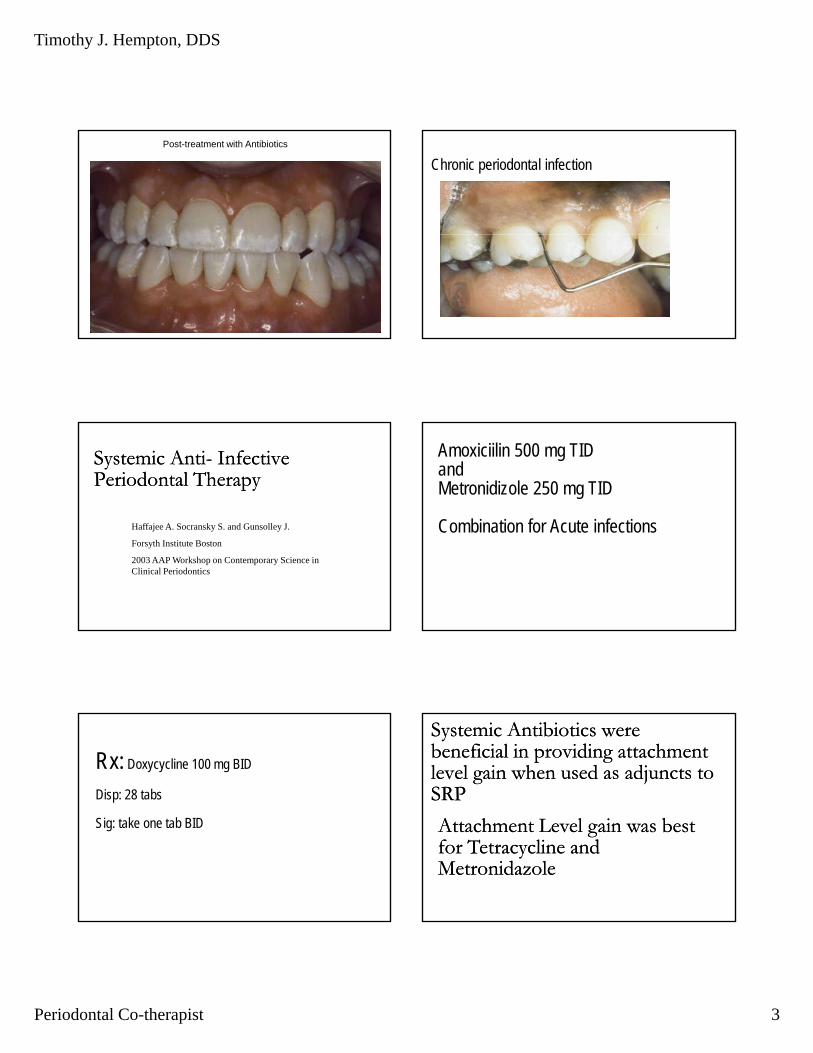
Acute periodontal infectionAcute infection
Timothy J. Hempton, DDS
Periodontal Co-therapist 3
Post-treatment with Antibiotics
Chronic periodontal infection
Systemic AntiSystemic Anti-- Infective Infective Periodontal TherapyPeriodontal Therapy
Haffajee A Socransky S and Gunsolley JHaffajee A. Socransky S. and Gunsolley J.
Forsyth Institute Boston
2003 AAP Workshop on Contemporary Science in Clinical Periodontics
Amoxiciilin 500 mg TIDand Metronidizole 250 mg TID
Combination for Acute infectionsCombination for Acute infections
Rx: Doxycycline 100 mg BID
Disp: 28 tabs
SSig: take one tab BID
Systemic Antibiotics were Systemic Antibiotics were beneficial in providing attachment beneficial in providing attachment level gain when used as adjuncts to level gain when used as adjuncts to SRPSRP
Attachment Level gain was best Attachment Level gain was best for Tetracycline and for Tetracycline and MetronidazoleMetronidazole

Timothy J. Hempton, DDS
Periodontal Co-therapist 4
Borderline significance in Borderline significance in Attachment level gain was Attachment level gain was observed for the combination of observed for the combination of A i illi l M id lA i illi l M id lAmoxicillin plus MetronidazoleAmoxicillin plus Metronidazole
Subjects receiving systemic antibiotics show greater improvement in PD and AL post therapy than those not receiving systemic antibiotics
4 to 6 mm pockets mean benefit 0.29 mm
Greater than 6 mm mean pocket benefit 0.45
4 to 6 mm pockets mean benefit 0.29 mm
Greater than 6 mm mean pocket benefit 0.45
0.45 mm
Systemic antibiotics provide the greatest benefit at sites with initially deeper pockets and in subjects with more disease
Tentative clinical guideline for antibiotic use based on level of disease: > 16 sites with BPD > 5 mm
Timothy J. Hempton, DDS
Periodontal Co-therapist 5
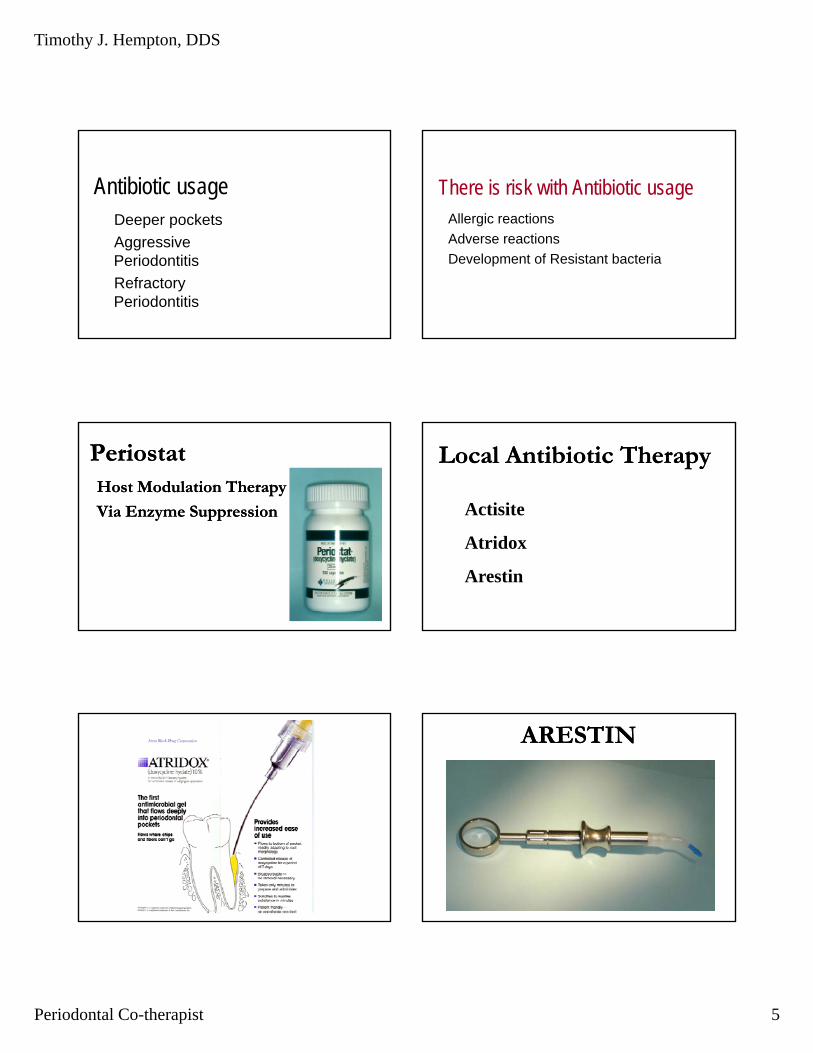
Antibiotic usageDeeper pockets
Aggressive Periodontitis
Refractory Periodontitis
There is risk with Antibiotic usageAllergic reactions
Ad tiAdverse reactions
Development of Resistant bacteria
PeriostatPeriostatHost Modulation TherapyHost Modulation Therapy
Via Enzyme SuppressionVia Enzyme Suppression
Local Antibiotic TherapyLocal Antibiotic Therapy
Actisite
Atridox
Arestin
ARESTINARESTIN

Timothy J. Hempton, DDS
Periodontal Co-therapist 6
What is the condition of the root surface at the What is the condition of the root surface at the time of placement of a local antimicrobial?time of placement of a local antimicrobial?
Local Antimicrobial Therapy
Periochip
Chlorhexidine has significant Chlorhexidine has significant Substantivity Substantivity
Chlorhexidine causes cell lysis Chlorhexidine causes cell lysis Chlorhexidine interferes with microbial adherenceChlorhexidine interferes with microbial adherence
BiofilmBiofilm
Biofilms Biofilms -- Strategy for SuccessStrategy for Success
Surface Adhesion Surface Adhesion P t ti M t iP t ti M t iProtective MatrixProtective MatrixWater Channels i.e. circulationWater Channels i.e. circulationQuorum Sensing i.e. SignalingQuorum Sensing i.e. Signaling

Timothy J. Hempton, DDS
Periodontal Co-therapist 7
We need to examine the effect We need to examine the effect of therapy on the bacteria.of therapy on the bacteria.
Thi ill id i hThi ill id i hThis will provide us with a This will provide us with a strategy for success.strategy for success.
Bacteria initiate the Bacteria initiate the process of attachment. process of attachment. losslossloss.loss.
Attached plaque
Unattached plaque
Listgarten 1970sAdherent Flora NonAdherent Flora Non--adherent floraadherent flora
S. oralis S. sanguis
S. mitis
C. rectus
P. intermedia
C. gracilis
V. parvulaA. odontolyticus
COMPLEXES Actinomyces species
SUBGINGIVAL MICROBIAL
Haffajee AD, Socransky SS. Haffajee AD, Socransky SS. Journal of Clinical Journal of Clinical Periodontology Periodontology 1997;24:3241997;24:324--334334
DNA Analysis of Subgingival bacteria
Streptococcus sp. S. gordonii
S. intermediusF. nuc . nucleatum F. nuc . polymorphum F. periodonticum
P. micros F. nuc . vincentii
C. showae
P. intermedia P. nigrescens
E. nodatumS. constellatus T. forsythensis
T. denticola
P. gingivalis
C. sputigenaC. ochracea
C. gingivalis E. corrodens
C. concisus A. actino . a A. actino . b S. noxia
Timothy J. Hempton, DDS
Periodontal Co-therapist 8
Tooth Adherent Planktonic Adherent to soft
Soft tissue
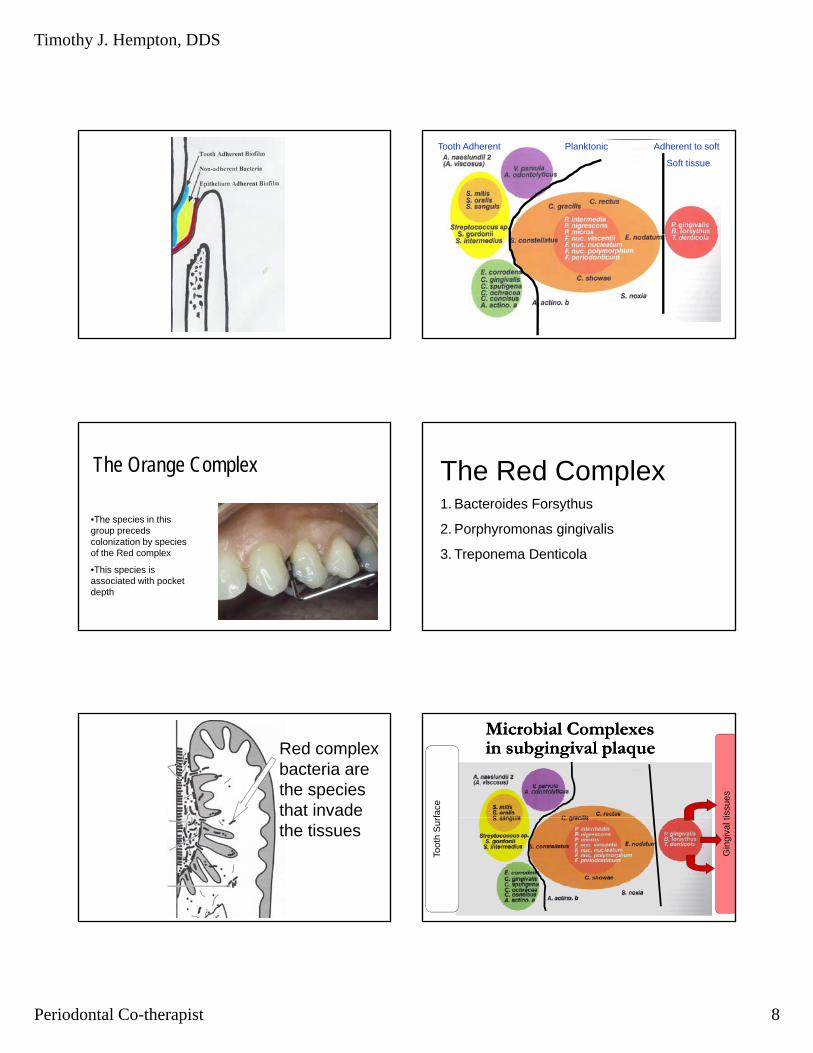
The Orange Complex
•The species in this group preceds colonization by species of the Red complex
•This species is associated with pocket depth
The Red Complex1. Bacteroides Forsythus
2 P h i i li2. Porphyromonas gingivalis
3. Treponema Denticola
Red complex bacteria are the species that invade the tissues
Microbial Complexes Microbial Complexes in subgingival plaquein subgingival plaque
rfa
ce
tissu
es
Toot
h S
ur
Gin
giva
l t

Timothy J. Hempton, DDS
Periodontal Co-therapist 9
T. forsythensis T. denticola
P. gingivalis
Bleeding on probingBleeding on probing
Red Complex
Tannerela Forsythensis (New name)
T D ti lTreponema Denticola
Porphomonas Gingivalis
Is our goal the Is our goal the elimination of pockets?elimination of pockets?
Is our goal stopping the Is our goal stopping the progression of attachment progression of attachment loss?loss?
Do these goals coincide?Do these goals coincide?The Effect of SRP on the Clinical The Effect of SRP on the Clinical and Microbiological Parameters and Microbiological Parameters Periodontal DiseasesPeriodontal DiseasesHaffajee AD, Socransky SS. Journal of Haffajee AD, Socransky SS. Journal of
Clinical Periodontology 1997;24:324Clinical Periodontology 1997;24:324--334334

Timothy J. Hempton, DDS
Periodontal Co-therapist 10
Before After
Hand and Power- driven instruments are equally effective in reducing the probing depth, attaining attachment level gains and reducing inflammation by removal of plaque bacteria, calculus, and endotoxin.
Ultrasonic debridement is more effective than manual scaling in Class II and Class III furcation invasion
Shigeru O et al. Current concepts and advances in manual and power-driven instrumentation. Periodontology 2000, Vol. 36,2004 page 45-58

Timothy J. Hempton, DDS
Periodontal Co-therapist 11
OraqixOraqixLidocaine and Prilocaine gel 2.5% / 2.5 %
Provides Provides soft tissuesoft tissue anesthesia anesthesia for about 20 minutesfor about 20 minutes
Effect of subgingival instrumentation on Effect of subgingival instrumentation on counts of subgingival microbial floracounts of subgingival microbial flora
Counts of bacteria associated Counts of bacteria associated with the Red Complex drop with the Red Complex drop significantlysignificantlysignificantly significantly
The Effect of Apically Repositioned The Effect of Apically Repositioned Flap Surgery on Clinical Parameters Flap Surgery on Clinical Parameters and theand the Composition of the Composition of the Subgingival Microbiota: 12 Subgingival Microbiota: 12 -- Month Month DataDataDataData
Levy R, Giannobile W, Levy R, Giannobile W, International Journal Perio Rest International Journal Perio Rest Dent. Vol 22, 2002 Dent. Vol 22, 2002
The effect of pocket elimination The effect of pocket elimination
surgery on the microbial habitatsurgery on the microbial habitatCounts of bacteria associated Counts of bacteria associated with the Red Complex and with the Red Complex and some species of the orange some species of the orange p gp gComplex drop significantlyComplex drop significantly

Timothy J. Hempton, DDS
Periodontal Co-therapist 12
We can utilize surgery to We can utilize surgery to eliminate pockets via; eliminate pockets via;
Resective therapyResective therapyResective therapyResective therapyRegenerative surgeryRegenerative surgery
Surgery can effect a Surgery can effect a change in the bacterial change in the bacterial habitathabitatAs probing depths are decreasedAs probing depths are decreasedAs probing depths are decreasedAs probing depths are decreased
Oxygen levels IncreaseOxygen levels Increase
Remember Bacteria Remember Bacteria Causes Periodontal Causes Periodontal DiseaseDiseaseDiseaseDisease
Gingival Curettage
Does it have any benefit?

Timothy J. Hempton, DDS
Periodontal Co-therapist 13
Gingival Curettage after scaling and root planing using mechanical instruments has been shown to have no added benefit over routine scaling and root planing
Echeverria and Caffesse
Effects of gingival currettage when performed 1 month after root instrumentation. A biometric evaluation. JXlin Perio 1983
AAP Position paper
A six months, no statistically or clinically significant difference observed between usage of an ultrasonic scaler as compared to an Er:YAG laser for non-surgical debridement
Sculean A et al.Periodontal treatment with an Er:YAG laser compared to ultrasonic instrumentation. J Periodontology 2004
What home care techniques What home care techniques can a patient utilize to effect can a patient utilize to effect the activities of the subgingival the activities of the subgingival microbial flora ?microbial flora ?microbial flora ?microbial flora ?
The supragingival plaque The supragingival plaque serves as a reservoir for the serves as a reservoir for the subgingival plaquesubgingival plaqueApproximal surfaces Approximal surfaces --
Brushing with a toothbrush Brushing with a toothbrush or an electric toothbrushor an electric toothbrush
Proximal surfacesProximal surfaces-- flossing flossing and rubber tipping and rubber tipping
A Waterpick can disrupt the nonA Waterpick can disrupt the non--adherent floraadherent flora
Subgingival Irrigation

Timothy J. Hempton, DDS
Periodontal Co-therapist 14
Irrigation with a water Pik disrupts the Non Adherent Flora
Effecting a qualitative change on subgingival change on subgingival plaque can result in an improvement of the gingival index
Is our goal the elimination of pockets?Is our goal stopping the progression of attachment loss?
Are there benefits to periodontal Surgery ?
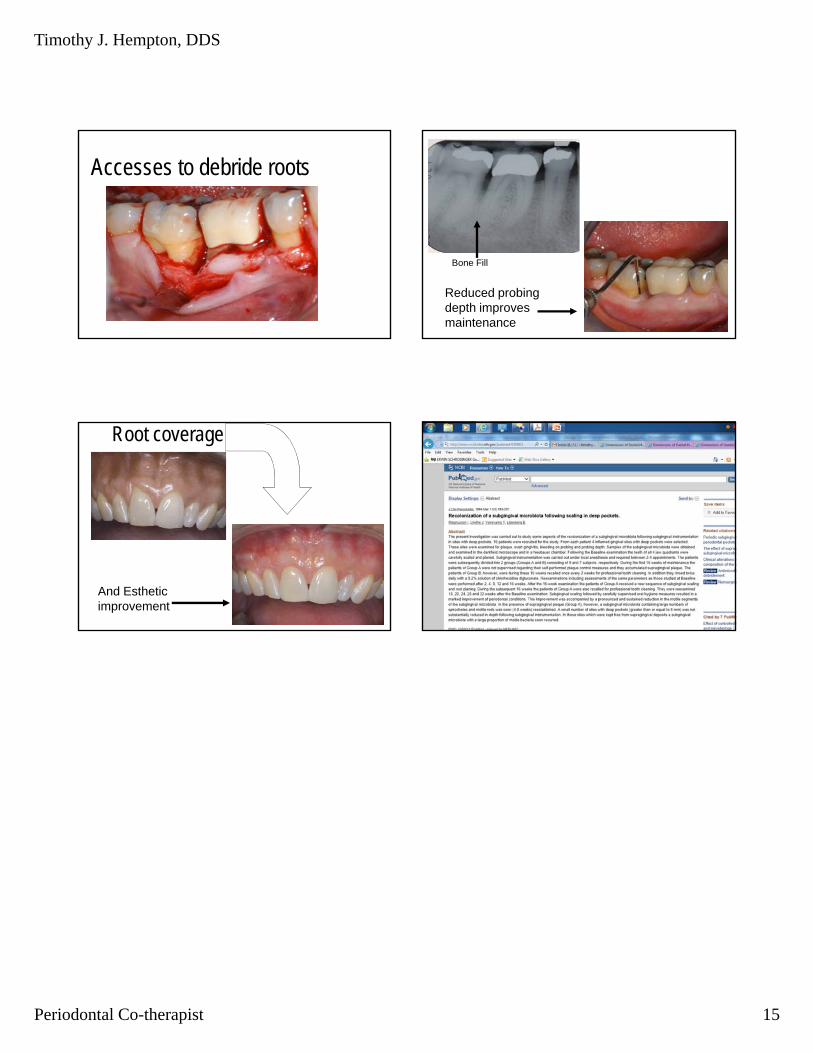
Accesses to debride roots
Root coverageRoot coverage
Esthetic improvement
Accesses to debride roots and reduce probing depths
Timothy J. Hempton, DDS
Periodontal Co-therapist 15
Accesses to debride roots
Bone Fill
Reduced probing depth improves maintenance
Root coverage
And Esthetic improvement










—Jackie L. Sanders, RDH, BSManager, Professional Relations
Sunstar Americas Inc
CASE PRESENTATION
Figure 1 is a view of the mandibular left sextant of a 43-year-old man. The patient presented with hypertension controlled by medication and generalized chronic periodontitis. He had been treated with phase I therapy. Probing depths of 5 mm to 7 mm still persisted on the mesial aspect of tooth #19. A radiograph (Figure 2) of the mandibular left posterior sextant indicates an intrabony defect on the mesial aspect of tooth #19. Bleeding on probing can be seen in Figure 3. Periodontal surgery to improve access was performed.
Introduction
Dental implant therapy has quickly become a routine procedure in the world of restorative dentistry. To complement these efforts, bone regeneration has established additional options for patients who do not have sufficient bone to support a new dental implant. The patient education provided by dental hygienists on grafting, augmentation, and osseointegration can be a key element of a patient's treatment success. With these thoughts in mind, Sunstar Americas is pleased to feature Dr. Timothy J. Hempton from Tufts University in the May issue of Sunstar Spotlight. He provides an in-depth look at the placement of barrier membranes, importance of post-operative management, possible complications, and guidance for long-term maintenance. As these procedures become more common, dental hygienists will need to remain up-to-date on this important treatment protocol in order to ensure the provision of quality patient care.
Dental hygienists are often confronted with the frustrating task of debriding root surfaces adjacent to deep pockets. Even after in flam mation has been controlled via nonsurgical treatment, attachment loss may continue because deep pockets generally interfere with the ability to access the contaminated root surface. As a result, patients should be informed about the option to reduce probing depths via periodontal surgery because shallower probing depths allow for easier debridement of the root, and improved access supports removal of subgingival plaque, which is likely to arrest periodontal attachment loss.
Surgical pocket reduction can be achieved via osseous resective therapy or osseous regeneration therapy. While a predictable approach to pocket
Page 1 of 6Dimensions of Dental Hygiene
4/30/2014http://www.dimensionsofdentalhygiene.com/print.aspx?id=16554
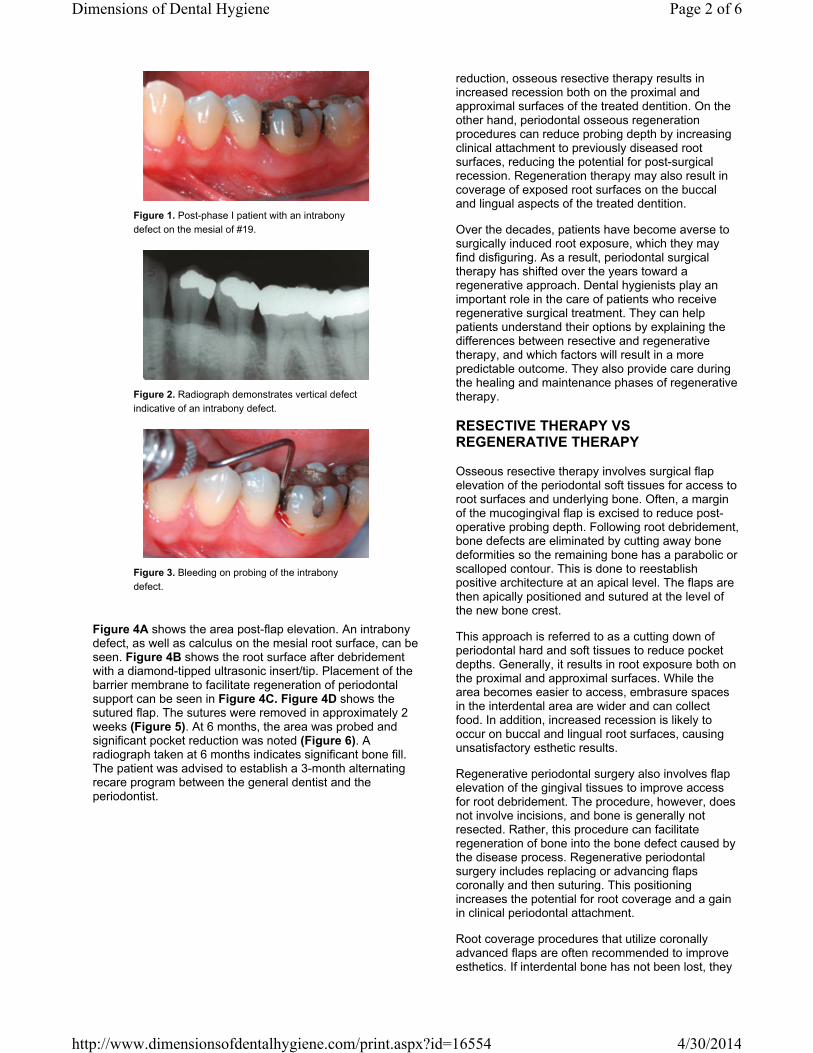
Figure 1. Post-phase I patient with an intrabony defect on the mesial of #19.
Figure 2. Radiograph demonstrates vertical defect indicative of an intrabony defect.
Figure 3. Bleeding on probing of the intrabony defect.
Figure 4A shows the area post-flap elevation. An intrabony defect, as well as calculus on the mesial root surface, can be seen. Figure 4B shows the root surface after debridement with a diamond-tipped ultrasonic insert/tip. Placement of the barrier membrane to facilitate regeneration of periodontal support can be seen in Figure 4C. Figure 4D shows the sutured flap. The sutures were removed in approximately 2 weeks (Figure 5). At 6 months, the area was probed and significant pocket reduction was noted (Figure 6). A radiograph taken at 6 months indicates significant bone fill. The patient was advised to establish a 3-month alternating recare program between the general dentist and the periodontist.
reduction, osseous resective therapy results in increased recession both on the proximal and approximal surfaces of the treated dentition. On the other hand, periodontal osseous regeneration procedures can reduce probing depth by increasing clinical attachment to previously diseased root surfaces, reducing the potential for post-surgical recession. Regeneration therapy may also result in coverage of exposed root surfaces on the buccal and lingual aspects of the treated dentition.
Over the decades, patients have become averse to surgically induced root exposure, which they may find disfiguring. As a result, periodontal surgical therapy has shifted over the years toward a regenerative approach. Dental hygienists play an important role in the care of patients who receive regenerative surgical treatment. They can help patients understand their options by explaining the differences between resective and regenerative therapy, and which factors will result in a more predictable outcome. They also provide care during the healing and maintenance phases of regenerative therapy.
RESECTIVE THERAPY VS REGENERATIVE THERAPY
Osseous resective therapy involves surgical flap elevation of the periodontal soft tissues for access to root surfaces and underlying bone. Often, a margin of the mucogingival flap is excised to reduce post-operative probing depth. Following root debridement, bone defects are eliminated by cutting away bone deformities so the remaining bone has a parabolic or scalloped contour. This is done to reestablish positive architecture at an apical level. The flaps are then apically positioned and sutured at the level of the new bone crest.
This approach is referred to as a cutting down of periodontal hard and soft tissues to reduce pocket depths. Generally, it results in root exposure both on the proximal and approximal surfaces. While the area becomes easier to access, embrasure spaces in the interdental area are wider and can collect food. In addition, increased recession is likely to occur on buccal and lingual root surfaces, causing unsatisfactory esthetic results.
Regenerative periodontal surgery also involves flap elevation of the gingival tissues to improve access for root debridement. The procedure, however, does not involve incisions, and bone is generally not resected. Rather, this procedure can facilitate regeneration of bone into the bone defect caused by the disease process. Regenerative periodontal surgery includes replacing or advancing flaps coronally and then suturing. This positioning increases the potential for root coverage and a gain in clinical periodontal attachment.
Root coverage procedures that utilize coronally advanced flaps are often recommended to improve esthetics. If interdental bone has not been lost, they
Page 2 of 6Dimensions of Dental Hygiene
4/30/2014http://www.dimensionsofdentalhygiene.com/print.aspx?id=16554

Figure 4A. Following flap elevation, calculus is noted on the mesial root surface.
Figure 4B. After root debridement, this intrabony defect will likely fill with bone.
Figure 4C. A barrier membrane is placed over the intrabony defect.
Figure 4D. The flaps are sutured over the barrier membrane.
Figure 5. Site at 14 days post-surgery after sutures have been removed.
can be very predictable in gaining clinical attachment and patient satisfaction in the esthetic outcome.
FACTORS FOR SUCCESS
Three types of osseous defects associated with periodontitis respond well to periodontal regenerative therapy, including intrabony defects, osseous dehiscences, and class II furcation invasion associated with mandibular molars with intact interdental bone.
Intrabony defects are pockets that extend within the bone. They can be identified via periodontal probing in conjunction with radiographs exhibiting angular or vertical osseous loss adjacent to the affected dentition (Figure 1 to Figure 3).
Bony dehiscences are suprabony pockets associated with bone loss on either the buccal or lingual aspects of the affected dentition. Bony dehiscences associated with periodontal attachment loss are not evident on radiographs but are detected clinically via probing on the buccal or lingual aspects of the affected dentition.
Class II mandibular molar furcation invasion is attachment loss associated with the buccal or lingual aspect of a mandibular molar. It is essentially a dehiscence on the buccal or lingual aspect of the molar caused by periodontitis.
Research shows that intrabony defects treated with open flap surgical procedures with root debridement will result in bone regeneration.1,2 Without placement of a bone graft or commercially available regenerative material, thorough root debridement will, in the human body, result in regeneration of its own bone into intrabony defects. By simply gaining access to remove the contaminants on the root, significant bone growth may occur. How much bone regrowth occurs is dependent not only on thorough root debridement, but also the morphology of the intrabony defect.
The possibility of successfully regenerating bone in an intrabony defect increases when the angle of the intrabony defect visualized on the radiograph is narrow and the defect is not wide. The angle is formed by the interdental wall of the defect and the diseased root surface. As this angle becomes narrower than 45°, the likelihood of bone growth greatly increases. As the defect width decreases, the success rate increases. The surprise is that deep defects do very well in obtaining bone fill. This occurs as long as the defect has not extended to the apex of the tooth where the nerve enters the root.
The predictability for successful gain in clinical attachment of a pocket-related bony dehiscence depends on thorough root debridement followed by replacement or coronal advancement of the flap. Failure of therapy will occur if attachment loss has approached the apex of the tooth where the nerve enters the root.
Page 3 of 6Dimensions of Dental Hygiene
4/30/2014http://www.dimensionsofdentalhygiene.com/print.aspx?id=16554

Figure 6. Patient at 6-months postsurgery. Probing can now be performed.
Figure 7. Radiograph of the successfully treated intrabony defect at 6 month recare appointment.
PRODUCTS IN PRACTICE
Solutions to Support Periodontal Health
Sunstar's mission is to improve patients' overall systemic health by helping people of all ages to maintain stronger, healthier teeth and gums. To this end, Sunstar is committed to providing quality products to support the needs of both consumers and dental professionals.
In an effort to improve the management and prevention of periodontal diseases, Sunstar has developed a variety of products to help dental professionals and their patients achieve better health outcomes. The line includes the following solutions:
• GUIDOR® is the Sunstar product line developed to assist with matrix barrier procedures and bone
augmentation. GUIDOR Allograft encompasses sterile, natural products that deliver proven results
in the treatment of periodontal defects, sinus
If the only procedure provided when treating mandibular molar class II furcation invasion is open flap debridement, the potential for successful gain in clinical attachment is very small. This outcome dramatically changes, however, when barrier membranes are used.
RATIONALE FOR PLACEMENT OF BARRIER MEMBRANES
An open flap debridement for the aforementioned defects is likely to result in a long junctional epithelium after healing is complete. Although bone will regenerate in intrabony defects and new clinical attachment will occur in osseous dehiscence defects, the nature of the attachment is essentially a repair.
A barrier membrane affects the nature of the attachment to the previously diseased root surface. Barrier membranes essentially interfere with normal wound healing, inhibiting the epithelium from completely closing the wound. The barrier membrane allows primitive cells from the periodontal ligament at the base of the defect to differentiate into new cementum on the debrided root surface. The new cementum subsequently attaches to new periodontal ligament fibers. Basically, the original attachment architecture of the surrounding periodontal hard and soft tissues to the root is regenerated.
Another advantage for placing barrier membranes is the potential for increasing clinical attachment. Evidence shows that the use of barrier membranes can lead to enhanced gain in attachment.3 For treatment of mandibular class II furcation invasion, barrier membranes are critical for establishing a significant gain in clinical attachment (see the Products In Practice sidebar).
POST-OPERATIVE MANAGEMENT
After open flap debridement is completed and the barrier membrane is placed (Figure 4A to Figure 4D), the dental team should advise the patient that post-operative management and long-term maintenance are just as important as the surgical procedure. The patient should be informed that smoking negatively affects wound healing.
A dressing or periodontal pack may be placed over the surgical area. The patient needs to use a chlorhexidine mouthrinse twice a day to inhibit plaque formation in the surgical area (see the Products In Practice sidebar). The patient should return to the office at 7 days for dressing removal and gentle supragingival debridement. A new periodontal dressing may be placed. At 14 days, the patient should return to have the sutures removed in addition to gentle supragingival plaque debridement (Figure 5). Once the sutures are removed, the dental hygienist should instruct the patient on effective self-care with a soft toothbrush to gently deplaque the surgically treated area. The patient should continue using the chlorhexidine mouthrinse for 1 month.
Wound healing is a continuous process that takes weeks, and varies from patient to patient. To ensure
Page 4 of 6Dimensions of Dental Hygiene
4/30/2014http://www.dimensionsofdentalhygiene.com/print.aspx?id=16554

grafting procedures, and extraction socket
maintenance. GUIDOR Bioresorbable Matrix Barrier aids in bone regeneration and
augmentation.
• GUM® Paroex™ an Alcohol-Free Chlorhexidine Oral Rinse contains 0% alcohol.
• GUM Post-Surgical Toothbrush with extremely soft bristles is ideal for post-surgical cleaning, including
implants and grafts.
a positive outcome, the patient should return to the dental office for visits at 1 month, 2 months, 3 months, and at 6 months. The visits at 1 month and 2 months involve additional supragingival plaque removal, a review of oral hygiene, and reinforcement of smoking cessation if needed. Patients can floss subgingivally at 2 months. The area, however, should not be probed.
At 3 months and 6 months, a prophylaxis can be provided. Extensive subgingival debridement at 3 months is not recommended. Probing the area is generally not recommended until 6 months (Figure 6). If successful, a post-operative radiograph can be taken at 6 months (Figure 7). Successfully treated intrabony defects will demonstrate osseous fill on the radiograph at 6 months.
POST-OPERATIVE COMPLICATIONS
As with any surgical procedure, postoperative complications may occur, including bleeding, pain, swelling, infection, and exposure of the barrier membrane. The patient must be closely monitored during the post-operative phase so problems can be immediately addressed. If the membrane becomes significantly exposed, the patient should gently swab the area with a Q-tip dipped in chlorhexidine. If infection occurs, the patient should be placed on an antibiotic.
Post-operative pain can be greatly reduced by ensuring that the tissues are kept moist during the surgical procedure, and avoiding any tobacco use during the healing phase. Pain can be managed with nonsteroidal anti-inflammatory drugs (NSAIDs) or opioids, if needed.
To reduce post-operative swelling, ice packs should be administered immediately following the procedure and continued for the rest of the day. The next day, the patient can apply moist heat to reduce swelling. NSAIDs can also reduce post-operative edema.
LONG-TERM MAINTENANCE
The key to success for any periodontal surgical procedure is long-term maintenance. Research indicates that model bacteria associated with periodontal disease will develop at approximately 90 days.4 As a result, patients need to be on a 3-month recare program. This allows the dental hygienist to remove plaque, which will facilitate healing and long-term stability. Patients who do not participate in postoperative maintenance programs have poorer results. In comparison, patients who remain on long-term maintenance programs most often achieve excellent outcomes.5
Regenerative surgical treatment to reduce pocket depth can improve periodontal health while also providing patients with the esthetic results they desire. As successful outcomes of these procedures depend on effective postoperative care, long-term maintenance, and patient compliance, dental hygienists are integral to achieving these benchmarks.
ACKNOWLEDGEMENT
The author would like to thank Charles E. Hawley, DDS, PhD, for his dedication to the specialty of periodontology and his inspiration in the writing of this paper.
Timothy J. Hempton, DDS, is associate clinical professor and interim director of post-doctoral periodontology at Tufts University School of Dental Medicine in Boston. He is a diplomate of the American Board of Periodontology and also maintains a private practice limited to perio dontology and implantology in Dedham, Mass. Hempton is a member of Dimensions of Dental Hygiene’s Editorial Advisory Board.
Page 5 of 6Dimensions of Dental Hygiene
4/30/2014http://www.dimensionsofdentalhygiene.com/print.aspx?id=16554

References
1. Becker W, Becker BE, Berg L, Samsam C. Clinical and volumetric analysis of three-wall intrabony defects following open flap debridement. J Periodontol. 1986;57:277–285. 2. Cortellini P, Tonetti MS. Clinical and radiographic outcomes of the modified minimally invasive surgical technique with and without regenerative materials: a randomized-
controlled trial in intra-bony defects. J Clin Periodontol. 2011;38:36–373. 3. Needleman IG, Worthington HV, Giedrys- Leeper E, Tucker RJ. Guided tissue regeneration for periodontal infra-bony defects. Cochrane Database Syst Rev.
2006;2:CD001724. 4. Listgarten MA, Levin S. Positive correlation between the proportions of subgingival spirochetes and motile bacteria and susceptibility of human subjects to periodontal
deterioration. J Clin Periodontol. 1981;8:122–1238 5. Cortellini P, Tonetti MS. Long-term tooth survival following regenerative treatment of intrabony defects. J Periodontol. 2004;75:672–678.
From Dimensions of Dental Hygiene. May 2013; 11(5): 19–22.
Copyright 2002-2014 • Belmont Publications, Inc. • 3621 Harbor Blvd., Suite 265, Santa Ana, CA 92704 • ISSN 1542-7919
Page 6 of 6Dimensions of Dental Hygiene
4/30/2014http://www.dimensionsofdentalhygiene.com/print.aspx?id=16554