what you should know about intracranial pressure
DESCRIPTION
Cause I'm always stress...lolTRANSCRIPT

INTRACRANIAL PRESSURE
INTRODUCTION
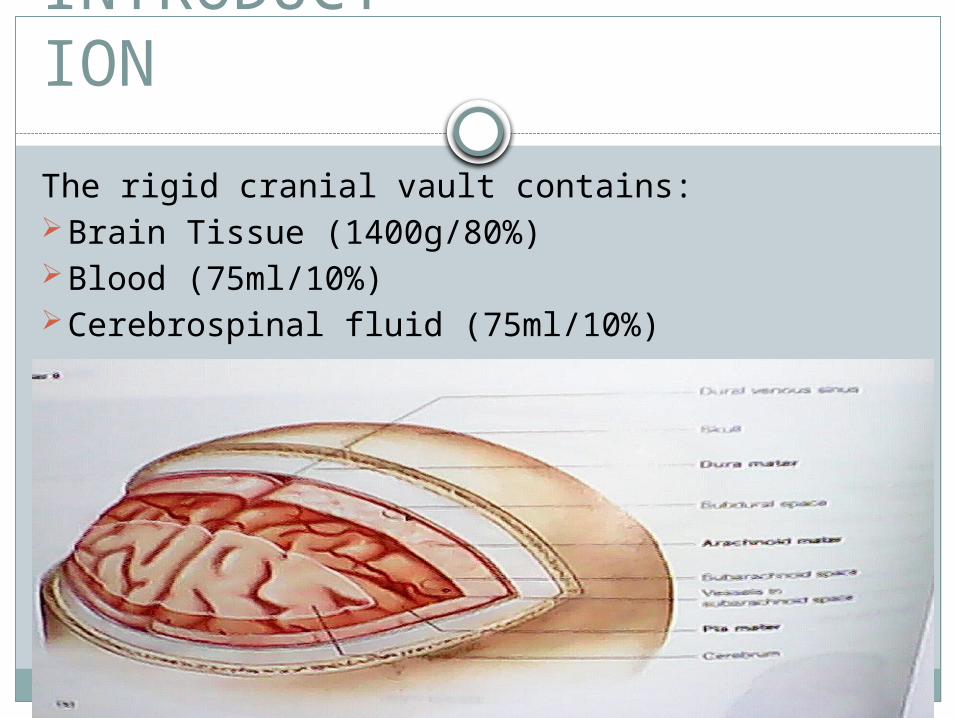
The rigid cranial vault contains:Brain Tissue (1400g/80%)Blood (75ml/10%)Cerebrospinal fluid (75ml/10%)
The volume and pressure of these three components are usually in the state of equilibrium and produce the ICP. ICP is usually measured in the lateral ventricles, with normal pressure being 10-20mmHg.

Continued….
CSF is produced by the Choroid Plexuses, specialized structures made of ependymal cells which are located in the ventricles.
CSF fills the brain ventricles, the central canal of the spinal cord and the subarachnoid space.
CSF bathes the brain and spinal cord , providing a protective cushion around the CNS.
CSF should be clear and transparent in appearance.
1 . CSF IS PRODUCED BY THE CHOROID PLEXUS IN EACH OF THE FOUR VENTRICLES.
LATERAL VENTRICLE Anterior Horn Inferior Horn Posterior Horn
2 . CSF FROM THE LATERAL VENTRICLES FLOWS TO THE THIRD VENTRICLE.
3 . CSF FLOWS FROM THE THIRD VENTRICLE THROUGH THE CEREBRAL AQUEDUCT TO THE FOURTH VENTRICLE.
Flow of CSF
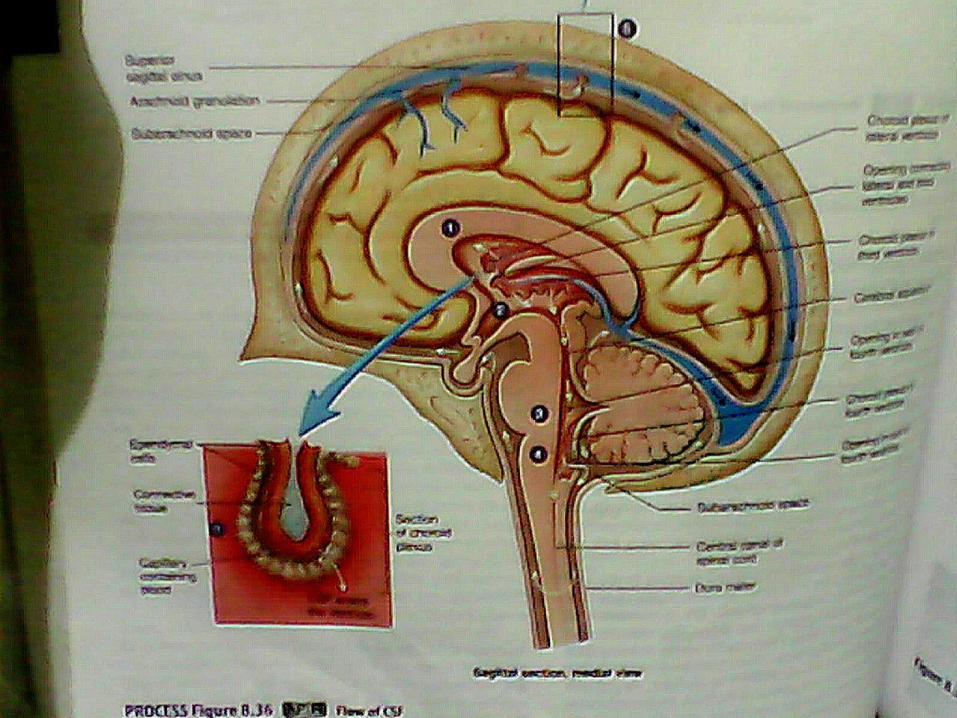
4 . CSF EXITS THE FOURTH VENTRICLE THROUGH OPENING IN THE WALL OF THE FOURTH VENTRICLES AND ENTERS THE SUBARACHNOID SPACE. SOME ENTERS THE CENTRAL CANAL OF THE SPINAL CORD.
5 . CSF FLOWS THROUGH THE SUBARACHNOID SPACE TO THE ARACHNOID GRANULATION IN THE SUPERIOR SAGITAL SINUS, WHERE IT ENTERS THE VENOUS CIRCULATION
Continued….
MONRO-KELLIE HYPOTHESIS..
States that, because of the limited space for expansion within the skull, an increase in any one components causes a change in the volume of the others.
______________________________________Because the brain tissue has limited space to expand,
compensation typically is accomplished by displacing or shifting CSF, increasing the absorption or diminishing the production, or decreasing the cerebral blood volume. Without such changes, ICP will begin to rise. Under normal circumstances, minor changes in blood volume and CSF volume occur constantly due to alterations in intrathoracic pressure, posture, bp and systemic O2 and CO2 levels.
ICP OF MORE THAN 20 MMHG .
INCREASED INTRACRANIAL
PRESSURE
Decrease in Cranial Blood FlowIschemia in early stages stimulates vasomotor
center causing systemic pressure to rise to maintain cerebral blood flow.
Blood pressure, pulse and respirations are suggestive of increase in ICP.
Increase in PaCO2 in blood and brain tissue causes cerebral vasodilation leading to inrease CBF AND ICP.
Decrease in PaCO2 has a vasoconstrictive effect, limiting blood flow to the brain.
Decreased venous flow may also increase Cerebral blood volume, thus incresing in ICP

Cerebral EdemaAbnormal accumulation of fluid in
intracellular, extracellular or interstitial space or both. As braintissue swells within the rigid skull several mechanisms attempt to compensate for Increase in ICP, it includes:
Autoregulation-brains ability to change the diameter of its blood vessels automatically to maintain a constant CBF during alterations in Systemic Blood Pressure.

Cerebral ResponseArterial Systemic Blood Pressure is 50-
150mmHg. ICP changes are closely linked with Cerebral Perfusion Pressure and ICP is less than 40mmhg.Normal CPP is 70-100mmHg.
Patients with less than 50 mmHg CPP experience irreversible neurologic damage therefore CPP must be maintained at 70-80mmHg to ensure adequate blood flow.
CBF decreases significantly causing a Cushing Response/Reflex.

Cushing ResponseIs present when Ischemic, the vasomotor
center triggers an increase in arterial pressure in an effort to overcome Increase in ICP. A Sympathetically mediated response cause an increase in the systolic blood pressure with the widening of the pulse pressure and cardiac slowing.
Increase in Systolic Blood Pressure, widening of pulse pressure and reflex slowing of the heart rate.
CONCEPT MAP
Secondary effect in Brain Tumors, Subarachnoid Hemorrhage and toxic and viral Encephalopathies
Head Injury
Increase in Intracranial Pressure
A-ltered respiration (cheyne stroke)
P-rojectile vomitingR-restlessnessI-rritabilityL-evel of consciousness B-bradycardia
Decrease Cerebral Perfusion
Cerebral ischemia and cell death

May shift brain tissue through openings in the
rigid dura or presses down on the brain stem
HERNIATION
Cessation of blood flow to the brain leading to irreversible brain anoxia and brain death
Stimulates further swelling AutoregulationRestlessness without apparent
causeConfusion or increasing drowsiness
Becomes stuporousNeurologic functioning deterioratesCommatose---Decortication ---Decerebration

MEDICAL MANAGEMENT
Medical Management
Maintain Cerebral OxygenationDecrease Intracranial PressureCerebral PerfusionHyperventilationPrevent ComplicationMonitor ICPPrevent Intracranial Pressure

PHARMACOLOGIC MANAGEMENT

Mannitol
Classification: Diagnostic agent, Osmotic diuretics, Urinary irrigant
Indication: reduction of intracranial pressure and treatment of cerebral edema.
Contraindication: contraindicated with anuria due to severe renal disease.

MannitolPrecautions: use cautiously with
pulmonary congestion, active intracranial bleeding (except during craniotomy), dehydration, renal disease, heart failure, pregnancy, lactation.
Availability: given in bolus doses
Side Effects: increased urination, GI upset, dry mouth, headache, blurred vision.
Mannitol
NURSING RESPONSIBILITIES:Assess patient’s history of pulmonary
congestion, active intracranial bleeding, dehydration, renal disease, heart failure, pregnancy, lactation.
Assess skin color, lesions, edema, hydration, orientation, muscle strength, reflexes, pupils, pulses, BP, perfusion, RR patterns, adventitious sounds, urinary output patterns, S. electrolytes, urinalysis, renal function test.
Do not expose solutions to low temperatures, crystallization may occur.
Monitor serum electrolytes periodically with prolonged therapy.
Inform patient that he/she may experience side effects.
Encourage to report difficulty breathing and chest pain.

PHENYTOIN
Classification: antiarrhythmic, group 1b; antiepileptic; hydantoin
Indication: prevention of siezures.
Contraindication: hypersensitivity to hydantoins, sinus bradycardia, sinoatrial block, strokes-adams syndrome, pregnancy, lactation.

PHENYTOIN
Precautions: use cautiously with acute intermittent porphyria, hypotension, severe myocardial insufficiency, DM, hyperglycemia.
Side effects: drowsiness, dizziness, confusion, blurred vision, GI upset.

PHENYTOIN
Nursing Responsibilities:Monitor injection sites carefully, drug
solutions are very alkaline and irritating.Give oral drug with or without food in
consistent manner.Monitor hepatic function periodically during
long-term therapy; monitor bld. Counts and urinalysis monthly.

Monitor bld. urine sugar of patients with DM regularly.
Monitor bld. proteins to detect early malfunction of the immune system.
Inform client that he/she may experience side effects.
Encourage to report rash, severe nausea and vomiting, drowsiness, slurred speech, impaired coordination (ataxia), swollen glands, bleeding, swollen and tender gums, yellowish discoloration of the skin and eyes, joint pain, unexplained fever, sore throat, persistent headache, malaise.
PENTOBARBITAL
Classification: antiepileptic; barbiturate; hypnotic; sedative or hypnotic
Indication: sedativeContraindication: contraindicated with
hypersensitivity to barbiturates, manifest or latent porphyria, marked liver impairment, nephritis, severe respiratory distress, previous addiction to sedative-hypnotic drugs, pregnancy.
PENTOBARBITAL
Precautions: use cautiously with acute or chronic pain, seizure disorders, fever, hyperthyroidism, DM, severe anemia, pulmonary or cardiac disease, status asthmaticus, shock, uremia.
Availability: injection 50mg/mL
Side Effects: drowsiness and anxiety
PENTOBARBITAL
Nursing Responsibilities:Do not administer intra-arterially; may
produce arteriospasm, thrombosis, or gangrene.
Administer IV doses slowly.Administer IM doses deep in a muscle mass.Do not use parenteral form if solution is
discolored or contains precipitate.
PENTOBARBITAL
Monitor injection sites carefully for irritation, and extravasation (IV use); solutions are alkaline and very irritating to the tissues.
Monitor BP, Pulse, and respiration carefully during IV administration.
Inform client that he/she may feel drowsy and less anxious.
Instruct client not to try to get up after receiving this drug.

Other Drugs that may be used:
STEROIDS
HYPERTENSIVE DRUGS
NEUROMUSCULAR BLOCKING AGENTS
NURSING DIAGNOSIS
INEFFECTIVE CEREBRAL TISSUE PERFUSION RELATED TO INCREASED ICP
GOAL: Within 8 hours of nursing interventions patient will have stable or improving levels of consciousness.

Nursing Interventions
INDEPENDENT:Note customary baseline data (e.g., usual BP,
weight, mentation, ABGs, and other appropriate study values).
Rationale: provide comparison with current findings.

Determine presence of visual, sensory/motor changes, headache, dizziness, altered mental status, personality changes.
Rationale: this may indicate presence increased
intracranial pressure.
Note history of brief/intermittent periods of confusion/blackout.
Rationale: This suggests transient ischemic attacks-
TIAs
Elevate head of the bed 30 degrees and maintain head/neck in midline or neutral position.
Rationale: To promote circulation/venous drainage.
Assist with/monitor hypothermia therapy.Rationale: Which may be used to decrease metabolic
and oxygen needs.
Encourage client to quit smoking (if he/she does), join smoke-out, and other stop-smoking program.
Rationale: Smoking causes vasoconstriction and may
further compromise perfusion
Avoid emotional stress, frequent arousal from sleep, and environmental stimuli (noise, conversation).
Rationale: This may increase ICP.
DEPENDENT:Administer medications such as diuretics
(mannitol), anticonvulsant (phenytoin) as ordered.
Rationale: These drugs are used to decrease cerebral
edema and prevent seizure.

Ineffective airway clearance related to neuromuscular dysfunction
GOAL: Within 30 minutes of nursing intervention interventions client will demonstrate absence/reduction of congestion, improved oxygen exchange.

Nursing InterventionsINDEPENDENT:Position head midline with flexion
appropriate for age/condition.Rationale: To open or maintain open airway in at-rest
or compromised individual.
Elevate the head of the bed.Rationale: may aid in clearing secretions as well as
improving venous drainage of the brain.

Auscultate breath sounds and assess air movement.
Rationale: To ascertain status and note progress.
Discourage coughing. Rationale: because it increases ICP.
Suction with care the secretions obstructing the airway
Rationale: because transient elevations of ICP occur with suctioning.
Provide opportunities for rest; limit to level of respiratory tolerance.
Rationale: Prevents/lessens fatigue.
Maintain a neurologic observation record. Rationale: Repeated assessments of the patient are made
frequently to immediately note improvement or deterioration.

Diagnostic Findings
CEREBRAL ANGIOGRAPHYCOMPUTED TOMOGRAPHY (CT) SCANNINGMAGNETIC RESONANCE IMAGINGPOSITRON EMISSION TOMOGRAPHY (PET)TRANSCRANIAL DOPPLERLUMBAR PUNCTURE
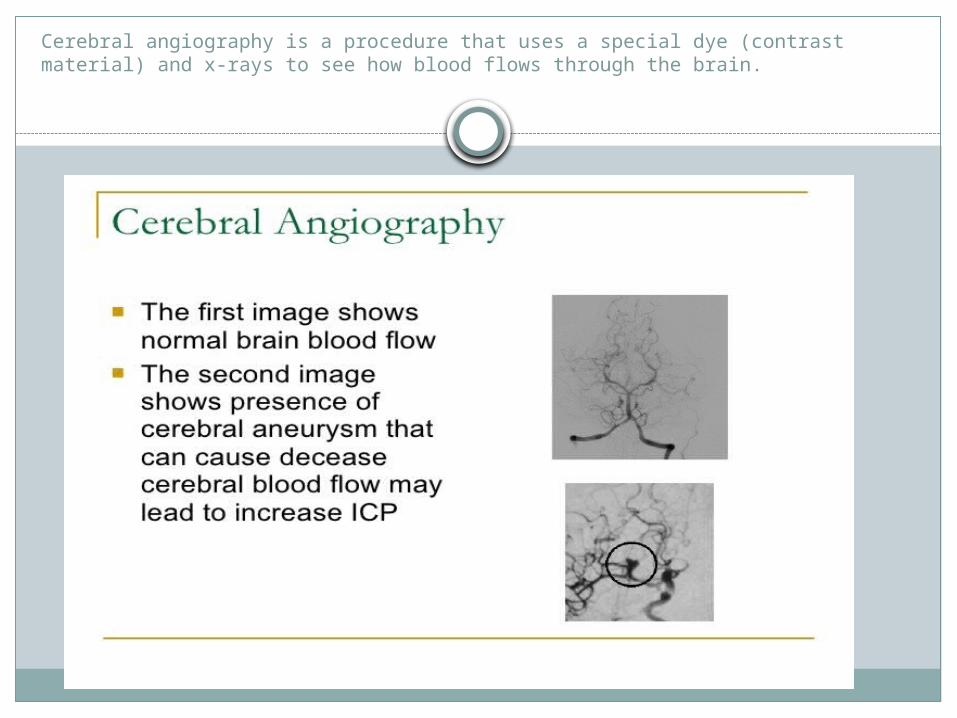
Cerebral angiography is a procedure that uses a special dye (contrast material) and x-rays to see how blood flows through the brain.

A computed tomography (CT) scan is an imaging method that uses x-rays to create pictures of cross-sections of the body.

Magnetic Resonance Imaging is a test that uses a magnetic field and pulses of radio wave energy to make pictures of organs and structures inside the body.

Is a test that uses a special type of camera and a tracer (radioactive chemical) to look at organs in the body. The tracer usually is a special form of a substance (such as glucose) that collects in cells that are using a lot of energy, such as cancer cells.
During the test, the tracer liquid is put into a vein (intravenous, or IV) in your arm. The tracer moves through your body, where much of it collects in the specific organ or tissue. The tracer gives off tiny positively charged particles (positrons). The camera records the positrons and turns the recording into pictures on a computer.
PET scan pictures do not show as much detail as computed tomography (CT) scans or magnetic resonance imaging (MRI) because the pictures show only the location of the tracer. The PET picture may be matched with those from a CT scan to get more detailed information about where the tracer is located.
A PET scan is often used to evaluate cancer, check blood flow, or see how organs are working.
Positron emission tomography (PET)


Transcranial Doppler is a test used to measures the velocity of blood flow through the brains blood vessels

Is a diagnostic and at times therapeutic procedure that is performed to collect a sample of cerebrospinal fluid for biochemical, microbiological and cytological analysis.
Shows that you have high pressure in the cerebrospinal fulid that sorrounds your brain and spinal cord.
Rarely as a treatment (therapeutic lumbar puncture) to relieve increased intracranial pressure.
Lumbar Puncture
Shunt Surgery -where a catheter (a thin, flexible tube) is inserted into the fluid-filled sapace in your brain or spine to divert excess fluid to another part of the body.
Types Lumboperitoneal shunting - Shunting fluid from the spine
to the abdomen Ventriculoperitoneal shunting- from the brain to the abdomen
Ventriculoatrial shunting- from the brain to the heart
Surgical Management
BY:NAPOLEON DWIGHT
ABONALES
THANK YOU for Listening..!