who drug informationapps.who.int/medicinedocs/documents/s14169e/s14169e.pdf · locally manufactured...
TRANSCRIPT
W H O D R U G
INFORMATION V O L U M E 12 N U M B E R 3 • 1 9 9 8
R E C O M M E N D E D I N N L I S T 40 I N T E R N A T I O N A L N O N P R O P R I E T A R Y N A M E S F O R P H A R M A C E U T I C A L S U B S T A N C E S
W O R L D H E A L T H O R G A N I Z A T I O N • G E N E V A
Volume 12, Number 3, 1998 World Health Organization, Geneva
WHO Drug Information
i
Contents
General Policy IssuesStarting materials for pharmaceutical
products: safety concerns 129Glycerol contaminated with diethylene glycol 129Pharmaceutical excipients: certificates of
analysis and vendor qualification 130Quality assurance and supply of starting
materials 132Implementation of vendor certification 134Control and safe trade in starting materials
for pharmaceuticals: recommendations 134
Reports on Individual DrugsTamoxifen in the prevention and treatment
of breast cancer 136Selective serotonin re-uptake inhibitors and
withdrawal reactions 136Triclabendazole and fascioliasis 138
Current TopicsReverse transcriptase activity in vaccines 140Consumer protection and herbal remedies 141Indiscriminate antibiotic use in animals —
public health implications 142Future trends in biological standardization 143
Regulatory MattersMibefradil: harmful interactions 145HIV vaccine trial approved 145Counterfeiting: halothane replaced by
chloroform 145Warfarin interaction with miconazole oral gel 145Nandrolone-containing products withdrawn 146Sibutramine scheduled as a controlled
substance 146Bromfenac withdrawal 146Discontinuation of international antibiotic
reference preparations 146
Seratrodast and hepatic dysfunction 146Meloxicam safety similar to other NSAIDs 147Proxibarbal withdrawn from the market 147Cholestin an unapproved drug 147Vigabatrin and visual defects 147
ATC/DDD Classification (final) 148
ATC/DDD Classification(temporary) 150
Essential DrugsWHO Model Formulary:Immunosuppressives, antineoplastics and drugs used in palliative careImmunosuppresive drugs 153
Azathioprine 153Ciclosporin 154
Cytotoxic drugs 154Asparaginase 157Bleomycin 157Calcium folinate 157Chlormethine 158Cisplatin 158Cyclophosphamide 158Cytarabine 159Dacarbazine 159Dactinomycin 159Doxorubicin 159Etoposide 160Fluorouracil 160Levamisole 160Mercaptopurine 160Methotrexate 161Procarbazine 161Vinblastine 161Vincristine 162
Hormones and antihormones 161Prednisolone 162Tamoxifen 163
Drugs used in palliative care 163
.../...

WHO Drug Information Vol. 12, No. 3, 1998
40
World Health Organization, Geneva
Contents (continued)
ii
Recent Publications and DocumentsGuidance for industry: active pharmaceutical
ingredients 165Guidance for industry: human plasma-derived
biological products 165WHO Expert Committee on drug dependence 165WHO Expert Committee on Biological
Standardization: Forty-sixth report 166Use of antimicrobials in food-producing
animals 166
Recommended InternationalNonproprietary Names: List 40
167
129
WHO Drug Information Vol. 12, No. 3, 1998
General Policy Issues
Starting materials forpharmaceutical products:safety concernsMany developing countries are wholly dependenton the importation of starting materials for use inthe local production of essential and generic medi-cines. Starting materials are defined as thosematerials which are used in the manufacture of apharmaceutical product or those which come intocontact with the product during its manufacture.They may include raw materials, active and inactiveingredients, excipients, propellants, containers andpackaging material.
Starting materials often change hands many timesbefore reaching the manufacturer or assembler ofthe final marketed product and there are manyopportunities for the material to undergo relabellingalong the distribution and trade chain. As a result,chemicals and materials required for production ofpharmaceutical products can become contaminatedor undergo a change in identity, either accidentallyor as a result of negligence, and sometimes fraud.For these reasons, it is important for the manufac-turer to implement good manufacturing practices(GMP) and carry out analytical testing on all startingmaterials used in the production of pharmaceuti-cals.
The most documented incidents of contaminationinvolve diethylene glycol, which is now held respon-sible for hundreds of unnecessary deaths through-out the world. Ingestion of diethylene glycol oftenleads to death through kidney failure. In Haiti in1996, some 100 children died after taking paediatricsyrup containing glycerol contaminated with diethy-lene glycol. International action is urgently neededto prevent similar incidents and tighten controls onthe distribution, trade and manufacture of startingmaterials.
Perhaps the single, most important handicap tocontrolling starting materials stems from the prac-tice of transshipment and multiple trading. Startingmaterials invariably pass through the hands ofagents or traders, and can be repackaged and re-labelled at any stage of the distribution chain. Bythe time a container has reached its destination, it
may no longer have an accurate description of itscontents either on the labelling or the certificate ofanalysis which accompanies it. Substitution of acheaper, substandard, more easily available prod-uct is, of course, of financial benefit to the supplier— but it can have a tragic effect on the health of theconsumer.
Given the need for immediate action, a meetingwas recently convened by the Division of DrugManagement and Policies of the World HealthOrganization on the control and safe trade in start-ing materials for pharmaceuticals. Participants fromregulatory authorities, nongovernmental organiza-tions, consumer organizations and representativesof the major pharmacopoeias as well as inspectors,pharmacists, traders, customs officials and chemi-cal and pharmaceutical manufacturers, were in-vited. The meeting formulated several recommen-dations which are set out on page 134.
Glycerol contaminated withdiethylene glycol
G. Pierce, DirectorDivision of Emergency and InvestigationalOperationsFood and Drug AdministrationUnited States of America
In Haiti, between November 1995 and June 1996,88 children died of acute renal failure after takinglocally manufactured paracetamol (acetaminophen)elixir, an anti-fever syrup. A major component of thesyrup is glycerol (USAN: glycerin), which was laterfound to have been contaminated with approxi-mately 20% diethylene glycol (DEG). DEG is anindustrial chemical not intended for pharmaceuticalor food use which can cause severe kidney dam-age when ingested.
In June 1996, the US Food and Drug Administration(FDA) and the US Centers for Disease Control andPrevention (CDC) in collaboration with the PanAmerican Health Organization (PAHO) and theHaitian Ministry of Health, identified DEG in twobrands of paracetamol syrup available in Haiti. TheFDA was requested to assist in the investigation ofthis product and its manufacture.

130
WHO Drug Information Vol. 12, No. 3, 1998General Policy Issues
The two brands of paracetamol syrup in questionwere available in either 4-ounce bottles or as oraldrops for neonates in 2-ounce bottles; both hadidentical formulations. The syrup was found tocontain 12–17% DEG and the oral drops contained3–5% DEG. One shipment of glycerol was used infive lots of the paracetamol. Later FDA analysis ofresidue left in two drums suspected to originatefrom the glycerol shipment showed 16–24% DEG,32% water, 23% sugar and 1–4% of the labelledglycerol in one drum and 26% DEG in the seconddrum.
Further investigation revealed that the manufacturerof the finished dosage form did not test the rawmaterials upon delivery, had no in-process qualitycontrol, and no finished product testing other thanpH. Because of inadequate recording and lack ofmanufacturing controls, it was impossible to estab-lish which lots of the finished product were manu-factured from the contaminated glycerol shipment.The company recalled all products which containedglycerol.
The FDA investigators traced the glycerol by visit-ing the shipper in the Netherlands. This disclosedthat the glycerol was shipped from the Netherlands,but the shipping record showed that the productwas billed through a company in Germany. Recordsof the German company disclosed that the glyceroloriginated in China. A sample of the glycerol heldby the company in the Netherlands was collectedby FDA officials and analysed. The analysis dis-closed 11% glycerol and 21% DEG.
Previous analysis of the shipment of glycerol toHaiti showed a purity of 53% rather than 95%, asreflected on the invoice. This information wascommunicated to the distributor in China whohandled the sale of glycerol, with information that asecond sample would be taken for further analysis.The distributor in China did not receive the resultsof the second analysis: by then, the shipment wasalready on its way to Haiti.
With assistance from the US Embassy in Beijing,FDA officials visited the distributor and manufac-turer in China. Between 1993 and 1995, the glyc-erol was manufactured by a fermentation processand glycerol was the company's only product. Atthe time of the investigation in November 1997, thecompany had moved to a new plant and therecords, which are normally kept for one year, hadbeen destroyed.
The carbon source of the fermentation media wascane sugar and DEG was not used for the produc-tion of glycerol. Purification would bring the concen-tration to 95, 96 or 98% depending on the grade ofglycerol being made. The glycerol was tested tomeet USP 21 by both the company and the distribu-tor, but the original certificate of analysis of thesetests was not available.
It is hoped that the informal consultation recentlyheld by WHO on the control and safe trade instarting materials will emphasize the importance ofthe safety and quality of pharmaceutical startingmaterials such as glycerol and will provide theapproach and exposure necessary to prevent futureincidents such as the Haiti tragedy.
Pharmaceutical excipients:certificates of analysis andvendor qualification
A.J. FalkVice ChairmanInternational Pharmaceuticals ExcipientCouncil (Americas)
Before purchasing or trading in excipients or otherstarting materials takes place, it is common practicewithin the pharmaceutical industry to request acertificate of analysis (COA). A COA relates specifi-cally to the results of tests carried out on a repre-sentative sample drawn from the material to bedelivered and will contain information on the resultsof analytic and performance tests, thereby providinga trustworthy indication of the quality of the materialto be supplied. COAs are of significant value whenproperly used.
Experience shows, however, that these certificatesare not always accurate or reflective of the materialthey describe, and when this occurs the situationcan become dangerous. Because COAs appear tobe official, the information they contain is acceptedas valid and decisions are made based on the datathey contain. However, when false information isprovided on the quality of the material, it can lead toserious complications. From the public healthperspective, a product that has a severely reducedor no therapeutic value can have negative conse-quences for the consumer and, if the product fails,can represent a significant loss in investments andreputation.
The company in Haiti described in the previousreport, accepted a shipment of glycerol and used it

131
WHO Drug Information Vol. 12, No. 3, 1998
to manufacture their product on the basis of infor-mation provided in a COA, only to discover that itwas heavily contaminated with diethylene glycol.Subsequent investigation showed that the datacontained in the COA did not correspond to resultsof analysis of the material in question.
As a result of this and similar incidents, the Interna-tional Pharmaceutical Excipients Council (IPEC)has developed the Good manufacturing guide forbulk pharmaceutical excipients (1) to qualify ven-dors and set out basic requirements for the manu-facture, packaging, storage, and testing of material.The Guide was compiled in collaboration with WHOand closely follows the WHO good manufacturingpractices: supplementary guidelines for the manu-facture of pharmaceutical excipients (3). Applicationof the advice contained in this simple guide wouldhave prevented the tragic incident in Haiti.
Two basic principles are set out in the guide. Firstly,the manufacturer of the final pharmaceutical prod-uct is ultimately responsible for the safety andquality of that product. Secondly, a certificate ofanalysis must reflect the actual results obtained orobserved for both qualitative and quantitative data.The COA should additionally include the name ofthe company, where the material was manufac-tured, and the signature of a person within thecompany having authority to attest to the results.The guideline clearly states that compliance withstandards and specifications established for excipi-ents, either through the national or regional phar-macopoeia or by a user or manufacturer of anexcipient, are insufficient to assure the safety,purity, and key characteristics of the material. Inorder to supply this information, performance testsare also needed.
Chemical analyses have now attained new levels ofprecision and sensitivity, advances in chromatogra-phy have permitted new and more rigorous defini-tions of purity, while dissolution tests and bioavail-ability-bioequivalence studies of drug products haveraised questions concerning the potential impactthat excipients may have on the product and theimportance of the consistency of their characteris-tics. The SUPAC Guidelines established within theUnited States by the Food and Drug Administration(2) contain minimum requirements to ensure thatany potential changes during manufacture of thefinal drug product are appropriately transparent andadequately controlled.
Despite advances in technology, one principleremains uncontested. Quality can only be "built in":it is only through consistent adherence to goodmanufacturing practices (GMP) that the safety,purity and consistency of the excipient can beassured. The guideline recommends that once asupplier is identified as a source or potential sourceof material to be used as an excipient, the manufac-turer should confirm the supplier’s ability to adhereto GMP. Should the supplier turn out to be a dis-tributor, adherence to GMP by the manufacturer willneed to be confirmed. It is important to know if alloperations are performed by the manufacturer, ifsubcontractors, such as contract packagers, areused, or if the material is sold to repackagers priorto acquisition by the company responsible for thefinal product. In the event that contractors orrepackagers are used, their adherence to GMPshould be confirmed. If the excipient distributor ormanufacturer is found to have an adequate GMPprogramme this may be used to confirm adherenceto GMP, which should then be periodicallyreconfirmed.
If the material is set out in the relevant pharmaco-poeia, the manufacturer’s tests and specificationsmust conform to pharmacopoeial or other nationalrequirements. If a modified or non-pharmacopoeialmethod is used, the method must be validated toensure that results are reliable and equivalent torequirements. In accepting a COA the followingcriteria must be met:
1. The supplier’s ability to adhere to GMP should beconfirmed.
2. Analytical methods should be identical or vali-dated as equivalent throughout all testing.
3. An adequate number of batch samples should beevaluated to compare results with those con-tained in the COA. Results for quantitative assaysmust be comparable and within specifications.For tests other than quantitative assays, allresults must be within specifications.
4. Any material qualified by the above procedureshould be periodically subjected to completetesting to reconfirm the reliability of the supplier’sCOA results.
Finally, an agreement should be formalized as partof the procurement procedure stipulating that allmaterial must be traceable during its life cycle, and
General Policy Issues
132
WHO Drug Information Vol. 12, No. 3, 1998
that the user will be notified in the event of anysignificant changes in procedures and quality of thematerial.
As can be seen, the information contained in theCOA needs to be confirmed by a testing laboratory.However, some pharmaceutical companies may nothave laboratories equipped to perform these tests.In such circumstances, it is recommended that anindependent central laboratory be utilized for thispurpose. It is only through correct analysis that thesuitability of the material can be confirmed.
As a continuation of the guidance document proce-dures, IPEC is currently working on more detailedguidlines covering some of the key steps for qualify-ing vendors. It is anticipated that the majority ofthese projects will be completed during 1999. In themeantime, the Guide establishes a basic frameworkfor determining the suitability of starting materials.
References
1. Good manufacturing practices guide for bulk excipientspublished by The International Pharmaceutical ExcipientsCouncil and available from: Dr E. Izeboud, IPEC Europe,Kerkweide 27, 2265 DM Leidschendam, Netherlands.email: [email protected] or Mr L. Blecher, IPECAmericas, ISP, 1361 Alps Road, Bldg 3, Wayne, NJ07470, USA.
2. Guidance for industry. Scale-Up and Post ApprovalChange (SUPAC) Expert Working Group, ChemistryManufacturing Controls Coordinating Committee, Centerfor Drug Evaluation and Research, Food and DrugAdministration, 7500 Standish Place, Rockville, MD20855, USA.
3. Good manufacturing practices: supplementaryguidelines for the manufacture of pharmaceuticalexcipients. Report of the 35th Expert Committee onSpecifications for Pharmaceutical Preparations. Annex 5.WHO Technical Report Series (In press).
Quality assurance and supplyof starting materials
R. Baxt & M. SiewertHoechst Marion Roussel AGFrankfurt, Germany
Given today's level of sophistication in analyticalmethodology, fatal events resulting from contamina-tion of starting materials used in pharmaceuticalproducts are unacceptable. Concepts such as goodmanufacturing practices (GMP) and Total Qualitymake incidents involving contamination of glycerolwith diethylene glycol difficult to comprehend.
Good manufacturing practices lay out the groundrules for the pharmaceutical industry, and tools areavailable for application throughout every compo-nent of the supply chain. The decision not to usethe tools, or the casual and careless use of them, isinexcusable. The following practices reflect effortsundertaken by the pharmaceutical industry to avoidsituations such as that which has occurred in Haiti.
Sampling proceduresThe classical approach to quality assurance ofstarting materials is based on a sampling procedurein preparation for testing and release. Startingmaterials should meet predetermined compliancespecifications using prescribed methods. Theprocess involves a carefully designed samplingmethod to assess the level of purity and check forthe absence of foreign matter. A company willtypically create standard operating proceduresbased on this method and an overall sampling planwill also be drawn up to permit the statistical inter-pretation of data. These two elements combinedwill ensure with confidence that the material presentin an array of containers is of uniform quality andfree from unwanted contamination.
No matter how well designed the sampling processand interpretation of guidelines, a guarantee cannever be obtained that the material to be used istotally free of foreign matter. However, for a mate-rial to be as clean as possible, the sampling per-formance skills of trained personnel are important.The ability to remain focused and observant duringthe task will provide an increased level of confi-dence. Anything that appears different or unusual,such as a broken or missing seal, different outerpackaging, material clumping, strange appearance,or odour not observed on previous occasions —can provide important indicators of the need forspecific additional analysis and, perhaps, an in-creased sampling regimen.
In addition to the importance of ensuring that thesample or series of samples statistically representthe delivery as a whole, the environment in whichthe sampling takes place should be considered.Facilities must be arranged in such a way as toeliminate the possibility of incorporation of un-wanted contaminants into the material being sam-pled. Isolation compartments and the use of filteredair provide such an environment and should beconsidered as mandatory for certain materials.
Upon completion of sampling, adequate records aremade of the sampling process, and the appropriate
General Policy Issues

133
WHO Drug Information Vol. 12, No. 3, 1998
records and labels are filled out and affixed tocontainers to provide ease of traceability at a laterdate. The samples are then taken to the qualitycontrol laboratory for testing.
Quality control testingDuring quality control testing, only standard analyti-cal equipment and validated methods should beused. In order to remain within budget limits, costand time of testing require strict rationalization. Thismust be based on scientific appropriateness andsound judgement and must not compromise theappropriate interpretation of quality. In order tosuccessfully apply this rationalization process, theindustry has devised a tracking system to plot theanalytical results of successive batches of materialpurchased from the same vendor or manufacturerover time. This tracking allows the individual qualitycontrol unit to evaluate whether reduced testingprogrammes can be applied in light of the quality ofthe material being provided.
When used in collaboration with a supplier certifica-tion programme, reduced testing will cut costswithout compromising quality. This is of value in theeffective and efficient use of resources. Whetherthe samples brought to the laboratory for qualitytesting are subjected to full testing or to reducedtesting, strict adherence to instructions must beobserved. In Haiti, if the sample of glycerol contami-nated with diethylene glycol had been subjected tothe USP titration method, it would have failed theassay and would have been rejected as not reach-ing acceptable standards for use in the manufac-ture of a pharmaceutical product.
The need for built-in qualityThe most important objective of GMP is to ensurethat quality is built into a product. This cannothappen after end-user quality control testing hasidentified the sample as unacceptable. Thus, atten-tion should be paid to product quality throughoutthe manufacturing process, with particular attentionto purification methods or controls designed toeliminate introduction of impurities. Specific effortsshould be made to avoid contamination duringsampling and any opening of containers or handlingof material should be undertaken with caution. It isalso important that packaging and repackagingshould be considered as part of the manufacturingprocess as well as a pharmaceutical operation.
Supplier qualification is an important and logicalsystem and auditing a supplier provides evidence ofthe vendor's capability to consistently produce andassure the intended and specified quality of therespective product or starting material. Confidencein reliable customer service, including quality ofproducts and conditions of delivery can only be builtup over time.
A supplier certification programme provides aninnovative opportunity to formalize collaborativerelationships between vendor and purchaser. Thisis not a new concept, and such programmes makegood sense. They are readily applicable to finishedproducts and active ingredients which have aclearly defined use. However, it becomes morecomplex when starting materials are at issue whichare not particularly destined for pharmaceutical use.Vendors cannot be expected to alter their operatingmechanisms when the pharmaceutical industryrepresents but a small percentage of the totalcustomer portfolio. In such cases, where GMP isnot applied throughout the manufacturing process,other quality management systems — such as ISO9000 series — may be useful, although not equiva-lent to analysis and GMP, in providing a basis forcustomer-supplier information.
In many cases, international pharmaceutical com-panies are associated with a parent chemicalcompany or are themselves manufacturers ofseveral chemicals, whether as active or inactiveingredients. In this situation, supplier certificationprogrammes and production and control to thesame level of quality is not only possible but is alogical operating requirement.
Manufacture, quality assurance and documentationin accordance with GMP are key factors in thesuccessful operation of pharmaceutical production.An efficient response to quality failure reports ispossible only if the contents of all batches aretraceable and identifiable. It must be rememberedthat the responsibility for the quality, safety andefficacy of a marketed product will ultimately fall onthe marketing authorization holder.
As we move into the next millennium and witnessthe emergence of even larger industrial conglomer-ates, we must be vigilant and foster effective com-munication with supply partners. Through carefuldefinition of requirements, suppliers can betterserve the needs of the pharmaceutical industry andhelp provide better and safer medicines.
General Policy Issues
134
WHO Drug Information Vol. 12, No. 3, 1998
Implementation ofvendor certificationWithin the pharmaceutical industry, there has beenconsiderable interest in establishing and imple-menting vendor certification, and a number ofcompanies have grouped together to explore thepotential. As a result, guidelines for vendor certifica-tion were established in 1989 by the Pharmaceuti-cal Manufacturers Association (PMA)* with theintention of assisting member firms and their suppli-ers in setting up a certification programme. Theguidelines also define terminology and describe theconcepts to be considered.
The guidelines apply to bulk pharmaceutical chemi-cals and raw materials, drug product components,containers, closures and other packaging materials,currently referred to as starting materials. They listthe critical elements which make up a successfulvendor certification programme. However, becom-ing certified requires many kinds and differentlevels of effort from the many parties involved.Furthermore, circumstances may vary dependingon the type of operation, the nature of the processinvolved, or product standard requirements — sothat a certain amount of latitude and judgement isan essential component in implementing the guide-lines.
Vendor certification constitutes an important com-ponent of a total quality management system toensure that a product is manufactured, assembled,packaged and shipped under a controlled processthat results in consistent conformity with customerrequirements. It is based on the principle of defectprevention as opposed to defect detection andselection. It supports the concept of quality at thesource by correct application of procedures andelimination or reduction of the need for final qualityinspections by the customer. If successfully imple-mented, vendor certification should improve qualityand delivery performance, increase productivity,and reduce costs.
*PMA Guidelines for vendor certification. Available fromPharmaceutical Research and Manufacturers of America(PhRMA), 110 15th Street, NW, Washington DC 20005,USA. Fax: 001-202-835-3597 e-mail: [email protected]
Control and safe trade in startingmaterials for pharmaceuticals:recommendationsAs a result of the tragic incident in Haiti and similarsituations which have occurred previously through-out the world, a meeting on the control and safetrade in starting materials for pharmaceuticals wasorganized by the Division of Drug Management andPolicies, at WHO Headquarters, Geneva, from 25to 27 May 1998. The purpose of the meeting was toevaluate the international public health impact ofthese events and to forge ways in which to preventsimilar incidents from occurring in the future.
As an intergovernmental organization, WHO is in aunique position to provide a global forum for discus-sion of the problem of contaminated and substand-ard pharmaceuticals. The meeting, which wasmade up of the major interested parties, proposedthe following recommendations.
All parties should:
• Ensure that starting materials meet quality controlrequirements.
• Ensure that starting materials meet the labelledpharmacopoeial requirements.
• Ensure that starting materials are manufactured,handled and distributed in accordance with goodmanufacturing practices.
• Collaborate in the free and unbiased exchange ofinformation.
National authorities should:
• Extend legislation to include all starting materials.
• Ensure that all parties manufacturing or handlingstarting materials or pharmaceutical products arelegally authorized to carry out such an activity.Appropriate sanctions should be established in theevent of failure to comply with national regula-tions.
• Monitor GMP compliance through regular inspec-tion, and extend inspection to free ports.
General Policy Issues
135
WHO Drug Information Vol. 12, No. 3, 1998
• Ensure that a fully equipped and accreditednational quality control laboratory is available.
• Only allow use of starting materials where facilitiesfor analysis and performance testing are available.
• Extend regulatory approval procedures to coverexcipients, and include excipients in drug masterfiles.
Manufacturers should:
• Ensure that production plants contain or haveaccess to an analytical testing laboratory to con-trol the quality of starting materials and relatedproducts.
•�Ensure access to a fully equipped and accreditedquality control laboratory before producing orhandling sophisticated materials.
Traders should:
• Establish a national trade association.
• Only accept materials which are manufactured inaccordance with GMP.
• Ensure that starting materials are traceable at allpoints in the distribution chain and keep records,in particular of any relabelling.
WHO should:
• Issue guidelines on the correct use and applica-tion of certificates of analysis (COA).
• Only support local manufacture which is carriedout according to GMP.
• Develop an international nomenclature system forexcipients.
• Develop a model for risk assessment of startingmaterials and identify high risk starting materials.
• Encourage development of skills for personnelhandling or dealing with starting materials.
• Extend the WHO Certification Scheme to cover allstarting materials.
• Continue to develop simple alternative test meth-ods for inclusion in the International Pharmaco-peia.
• Develop guidelines on requirements for the pur-chase of starting materials.
A report of the meeting on the control and safe trade instarting materials for pharmaceuticals is available from theDivision of Drug Management & Policies, World HealthOrganization, 1211 Geneva 27, Switzerland.
General Policy Issues
136
WHO Drug Information Vol. 12, No. 3, 1998
Reports on Individual Drugs
Tamoxifen in the prevention andtreatment of breast cancerWhen diagnosed in time, breast cancer and alldetectable cancer tissue can be removed surgically.However, because micrometastatic deposits of thedisease can remain, adjuvant tamoxifen is routinelyadministered immediately following surgery. Al-though this practice has been shown to improve the10-year survival rate of patients (1), uncertaintyremains concerning which patients should receivetreatment, and for how long.
In order to clarify this issue, the Early Breast Can-cer Trialists Collaborative Group (EBCTCG) hascarried out a meta analysis of 55 clinical trialsconducted in 15 countries and involving 37 000women diagnosed with early breast cancer (2).Results of the study showed that, when tamoxifenis started immediately following surgery and irre-spective of age, relapse is prevented in 1 in 6women and mortality in 1 in 12.
Furthermore, 5 years of tamoxifen therapy signifi-cantly reduced breast cancer recurrence by 42%and mortality by 22%.These results were similar forwomen under 50 years of age and older women.Among women who had received both chemo-therapy and adjuvant tamoxifen for five years, 61%had no recurrence of disease after ten years,compared with 40% who were receiving chemo-therapy alone. The results also showed an almost50% reduction in new cancers in the contralateralbreast during five year tamoxifen therapy.
However, for the 8000 women who had low or zerolevel estrogen-receptor protein in the primarytumour, the overall effects of tamoxifen appeared tobe small. In the light of these results, the authorsconclude that for women with estrogen receptorprotein negative tumours, the benefit of adjuvanttamoxifen is not yet proved.
A recent clinical trial on the prophylactic use oftamoxifen in healthy women with a family history ofbreast cancer was terminated 14 months earlywhen it was shown that tamoxifen reduced breastcancer incidence by 45% across all age groupscompared with placebo. The trial, run by the Na-
tional Cancer Institute and the National SurgicalAdjuvant Breast and Bowel Project in the UnitedStates of America, was scheduled to last six years,and involved over 13 000 women (3).
It remains to be seen from the results of theselatest trials, whether genetic screening for womenat high risk for breast cancer might be beneficial inidentifying those in need of prophylactic therapy (4).
References
1. Early Breast Cancer Trialists Collaborative StudyGroup. Systemic treatment of early breast cancer byhormonal, cytotoxic or immune therapy: 133 randomizedtrials involving 31 000 recurrences and 24 000 deathsamong 75 000 women. Lancet, 339: 1–15 (1992).
2. Early Breast Cancer Trialists Collaborative StudyGroup. Tamoxifen for early breast cancer: an overview ofthe randomized trials. Lancet, 351: 1451–1467 (1998).
3. Ault, A. Bradbury, J. Experts argue about tamoxifenprevention trial. Lancet, 351: 1107 (1998).
4. Dove, A. Tamoxifen, raloxifene findings unlikely toencourage genetic screening for breast cancer. NatureMedicine, 4: 647 (1998)
Selective serotonin re-uptakeinhibitors and withdrawal reactionsSelective serotonin re-uptake inhibitors (SSRIs)are a relatively new class of antidepressants.Although the first product in this family of drugs wasintroduced as early as 1982, a significant increasein the use of SSRIs was observed only when fluox-etine, the third drug of this family, was launched in1988 under the brand name, Prozac®. The successof fluoxetine resulted in a rapid expansion of theantidepressant market and, during the 1990s,additional SSRIs such as sertraline, paroxetine,venlafaxine, citalopram and nefazodone were alsomarketed.
However, despite a general belief that SSRIs didnot create dependence or lead to symptoms ofwithdrawal when discontinued after long-term use,it was not long before case reports of withdrawalsymptoms were received. The first reported case
137
WHO Drug Information Vol. 12, No. 3, 1998
involved a 32-year-old man who had experiencedagitation, inability to concentrate and insomniawithin 48 hours of discontinuation of fluoxetine (1).In the following year, a case was reported of a 30-year-old woman, treated with fluvoxamine 100 mg/day, who was overwhelmed by strong feelings ofaggression when she tried to stop taking the medi-cation (2). Similar isolated case reports continuedto be received.
In an open study, when 14 patients were withdrawnfrom fluvoxamine after 7–8 months of treatment,new symptoms developed in 12 of the patients.These included dizziness, incoordination, head-aches, nausea and irritability, and were distinguish-able from the panic disorder for which the drug wasprescribed. Symptoms usually peaked on day 5after withdrawal (3).
Reports of withdrawal symptoms did not excludethe newer SSRIs. In 1993, the British Committeeon Safety of Medicines cited 78 reports of symp-toms occurring upon withdrawal of paroxetine,including dizziness, sweating, nausea, insomnia,tremor and confusion (4). A case of sertralinewithdrawal was reported in 1994 (6) and the firstreports on venlafaxine withdrawal were publishedtwo years later, citing such symptoms as muscleaches, fatigue, headache, nausea and dizziness(6). A substitution study suggested that nefazodonewould not be an exception (7).
Isolated case reports of withdrawal symptomsassociated with individual SSRIs have been sup-ported by a number of observations. Severalrecent studies compare spontaneous reports ofwithdrawal symptoms from different SSRIs col-lected by adverse drug reaction monitoring pro-grammes. According to data on adverse drugreactions from the United Kingdom, the rates ofwithdrawal reaction reports were different for differ-ent SSRIs: 0.3 per 1000 prescriptions for paroxet-ine, 0.03 per 1000 for sertraline and fluvoxamine,and 0.002 per 1000 for fluoxetine (8).
Drug surveillance data from France indicate thatwithdrawal reactions with fluvoxamine and paroxet-ine occur in a greater proportion of reports than withfluoxetine (9). A careful review of the WHO ad-verse drug reaction data base in relation to drugsales statistics converted into DDDs (defined dailydoses) reveals that the reporting rate of withdrawalreactions for paroxetine was higher than that forsertraline and fluoxetine in Australia, the UnitedKingdom and the USA, which were selected for
detailed analyses, as well as for all 16 reportingcountries combined (10). With an increasingnumber of reports of this kind, SSRI withdrawal hasbecome the topic of several review papers. Al-though an early review concluded that withdrawalsymptoms associated with the discontinuation offluoxetine had not been established (11), morerecent reviews explain the lower incidence offluoxetine withdrawal symptoms in relation to itslong half-life, the incidence appearing higher withshorter half-life agents (12). Common physicalwithdrawal symptoms appear as problems of bal-ance, gastrointestinal and flu-like symptoms, andsensory and sleep disturbances. Psychologicalsymptoms include anxiety, agitation, crying spells,and irritability. Some symptoms are similar to thosereported with discontinuation of tricyclic antidepres-sants. However, SSRI discontinuation is alsoassociated with novel symptom clusters, includingsensory abnormalities and possibly aggressive andimpulsive behaviour (13).
The clinical implications of SSRI withdrawal shouldbe considered in the context of duration of treat-ment, clinical management of withdrawal, and riskof dependence and abuse. Because the symptomsof SSRI discontinuation include changes in mood,appetite and sleep, they are sometimes mistakenfor signs of a relapse into depression (14). This canlead to continued prescribing even after depressionhas been treated. With regard to clinical manage-ment of withdrawal, gradual tapering is recom-mended, particularly for short half-life SSRIs (15).Concerning the risk of dependence and abuse,opinions are mixed. Some reviewers consider thatSSRIs are not associated with dependence or drug-seeking behaviour. However, the same authorsnoted that SSRI discontinuation symptoms could betroublesome and there were several case reportswhere symptoms occurred consistently despiterepeated attempts to taper therapy (12).
There is obviously some confusion about the con-cept of dependence in such discussions. Thesimplest definition of drug dependence given byWHO is "a need for repeated doses of the drug tofeel good or to avoid feeling bad" (16). Whenthe patient needs to take repeated doses of thedrug to avoid the bad feelings caused by withdrawalreactions, the person is dependent on the drug.Those who have difficulty coming off the drugeven with the help of tapered discontinuationshould be regarded as dependent, unless a relapseinto depression is the reason for their inability tostop the antidepressant medication.
Reports on Individual Drugs
138
WHO Drug Information Vol. 12, No. 3, 1998Reports on Individual Drugs
In general, all unpleasant withdrawal reactions havea certain potential to induce dependence and thisrisk may vary from person to person. Dependencewill not occur if the withdrawal reactions are so mildthat all patients can easily tolerate them. Withincreasing severity, the likelihood of withdrawalreactions leading to dependence also increases.Although reporting rates of SSRI withdrawal are lowin comparison with prescribed doses, it is prudentto recommend the monitoring of patient withdrawalsymptoms even when SSRIs are prescribed atmodest doses (17).
References
1. Stoukides, J.A., Stoukides, C.A. Extrapyramidalsymptoms upon discontinuation of fluoxetine. AmericanJournal of Psychiatry, 148: 1263 (1991).
2. Szabadi, E. Fluvoxamine withdrawal syndrome. BritishJournal of Psychiatry, 160: 283–284 (1992).
3. Black, D.W., Wesner, R. Gabel, J. The abrupt dis-continuation of fluvoxamine in patients with panic disorder.Journal of Clinical Psychiatry, 54: 146–149 (1993).
4. Committee on Safety of Medicines, Medicines ControlAgency. Dystonia and withdrawal symptoms with paroxe-tine (Seroxat®). Current Problems, Number 19, 1993.
5. Louie, A.K., Lannon, R.A., Ajari, L.J. Withdrawalreaction after sertraline discontinuation. American Journalof Psychiatry, 151: 450–451 (1994).
6. Rauch, S.L., O’Sullivan, R.L., Jenike, M.A. Open treat-ment of obsessive-compulsive disorder with venlafaxine: aseries of ten cases. Journal of Clinical Psychopharmaco-logy, 16: 81–84 (1996).
7. Castañeda, R., Levy, L.M., Westreich, L.M., Sussman,N. Drug craving and other negative reactions after abruptsubstitution of nefazodone for other serotonergic agents.Journal of Clinical Psychiatry, 57: 485–486 (1996).
8. Price, J.S., Waller, P.C., Wood, S. et al. A comparisonof the post-marketing safety of four selective serotonin re-uptake inhibitors including the investigation of symptomsoccurring on withdrawal. British Journal of ClinicalPharmacology, 42: 757–763 (1996).
9. Blayac, J.P., Hillaire-Buys, D., Peyrière H. Lapharmacovigilance des nouveaux antidépresseurs:évaluation des troubles neuropsychocomportementaux.Thérapie, 52: 117–122 (1997).
10. Stahl, M.M., Lindquist, M., Pettersson, M. et al.Withdrawal reactions with selective serotonin re-uptakeinhibitors as reported to the WHO system. EuropeanJournal of Clinical Pharmacology, 53: 163–169 (1997).
11. Lazowick, A.L., Levin, G.M. Potential withdrawalsyndrome associated with SSRI discontinuation. Annals ofPharmacotherapy, 29: 1284–1285 (1995).
12. Schatzberg, A.F., Haddad, P., Kaplan, E.M. et al.Serotonin re-uptake inhibitor discontinuation syndrome: ahypothetical definition. Discontinuation consensus panel.Journal of Clinical Psychiatry, 58(Suppl. 7): 5–10 (1997).
13. Haddad, P. Newer antidepressants and the dis-continuation syndrome. Journal of Clinical Psychiatry,58(Suppl. 7): 17–21 (1997).
14. Lejoyeux, M., Ades, J. Antidepressant discontinuation:a review of the literature. Journal of Clinical Psychiatry,58(Suppl. 7): 11–15 (1997).
15. Rosenbaum, J.F., Zajecka, J. Clinical management ofantidepressant discontinuation. Journal of ClinicalPsychiatry, 58(Suppl. 7): 37–40 (1997).
16. World Health Organization. Lexicon of alcohol anddrug terms, Geneva, 1994.
17. Rosenstock, H.A. Sertraline withdrawal in twobrothers: a case report. International Clinical Psycho-pharmacology, 11: 58–59 (1996).
Triclabendazole and fascioliasisIt is estimated that 2.4 million people suffer fromfascioliasis infections worldwide, and a further 180million are at risk of infection. Outbreaks can causesevere illness, and in some areas over 60% of thepopulation can be infected. Typical symptomsinclude fever, abdominal pain, gastrointestinaldisturbances, urticaria, hepatomegaly, anaemiaand jaundice caused by the inflammatory responseand lesions in the abdominal cavity and liver.
The liver flukes Fasciola hepatica and F. giganticaare flat worms which live in the bile ducts of theirdefinitive hosts: either ruminants or man. Infectionoccurs through consumption of uncooked aquaticvegetables which have been contaminated withencysted parasitic larvae. Larvae migrate from thesmall intestine, across the intestinal wall, into theabdominal cavity. Within 24 hours of ingestion, thelarvae have become immature worms and move tothe liver to feed on liver tissue. While in the bileducts, the worms mature into adult form. Eachproduces eggs which are then released into thebiliary passages and are shed in the faeces.
Until recently, treatment of fascioliasis has beendifficult because praziquantel — effective againstmost trematode infections — is inactive against

139
WHO Drug Information Vol. 12, No. 3, 1998 Reports on Individual Drugs
Fasciola species. Triclabendazole has been usedeffectively in veterinary practice for fascioliasissince 1983 and, following its successful use inhumans during an outbreak in 1989 in the IslamicRepublic of Iran, WHO concluded an agreementwith the company Ciba-Geigy (now Novartis) toundertake human clinical studies to evaluate itseffect. As a result of this agreement, a developmentprogramme of clinical trials in Bolivia, Chile, Cuba,the Islamic Republic of Iran and Peru has now beensuccessfully concluded.
The most efficient dosage of triclabendazole for thisindication was demonstrated to be 10 mg/kg givenin two equal doses. During all trials, the drug waswell tolerated and cases of transient biliary obstruc-tion were attributed to the accumulation of deadworms during treatment. Triclabendazole wasdemonstrated to be highly efficacious and was notassociated with serious adverse effects. As a result,the drug has been included in the WHO model listof essential drugs. On a population basis, treatmentprovides immediate relief to infected individuals andreduces the prevalence and intensity of the diseaseburden.
140
WHO Drug Information Vol. 12, No. 3, 1998
Current Topics
Reverse transcriptaseactivity in vaccinesReverse transcriptase is an RNA-dependent DNApolymerase enzyme. Although such enzyme activityis also known to derive from other sources, it isgenerally related to the group of viruses known asretroviruses. Because the replication cycle ofretroviruses involves a double-stranded DNA copyof the viral genome which integrates into the chro-mosome of the host, most animal and avian spe-cies contain evolutionary remnants of ancientinfections as part of their genetic make-up. Theseremnants are known as endogenous proviral ge-nomes or retroviral-like elements and generally theyno longer encode a functional viral genome. Thus,the presence of genes for reverse transcriptase inthe absence of infectious virus has been identifiedin a variety of mammalian and avian cells.
Many vaccines are produced using chicken embryocells, and these should be derived from closelymonitored specific pathogen free (SPF) flockswhich are free of infectious avian retroviruses, incompliance with WHO requirements (1). The testsfor retroviruses include assays for reverse tran-scriptase (RTase) and, based on the newer nucleicacid amplification techniques, several laboratorieshave developed assays with improved sensitivity.Application of these more sensitive assays (2) hasdetected low levels of RTase in vaccines producedusing chicken embryo cells, including live attenu-ated vaccines for measles, mumps and yellow feverwhich have been manufactured in compliance withWHO requirements. No such activity has beenreported in vaccines produced using human diploidcells (2, 3).
The detection of low levels of RTase in vaccinesderived from chicken cells has given rise to concernthat a previously unidentified avian retrovirus couldbe present in vaccines prepared using chickencells. The results of laboratory and other investiga-tions were first reviewed by a group of experts at aWHO Consultation in 1995 and by the WHO ExpertCommittee on Biological Standardization (ECBS) in1996 which concluded that WHO requirements (1)continue to be appropriate and that there was no
evidence to suggest that the presence of RTasehas any medical significance for humans (5). Muchwork has been undertaken since and, in April 1998,WHO convened a follow-up meeting of experts invirology, vaccine production and epidemiology toreview the latest scientific data (5).
Most recent studies indicate that the RTase activityfound in chicken cells and in derived vaccines isassociated with particles. This particle-associatedRTase activity is common to all chicken cells and isnot related specifically to vaccines. Notwithstand-ing, it was recommended that further studies shouldbe undertaken to clarify the reason for the presenceof low levels of RTase activity in cell substrateswhich are used in the manufacture of vaccines andother biological products. WHO will set up a taskforce of scientists, regulatory authorities and spe-cialists from industry to conduct collaborativeresearch on the characterization, quality control andsafety assessment of all cell substrates intended forvaccine production.
The meeting concluded that the risk of vaccine-preventable disease is real and quantifiable, andshould supervene the theoretical and remote riskposed by RTase activity in chicken cell derivedparticles. Vaccines, such as those against measles,have a long and safe record of extensive interna-tional use and their beneficial effects in preventingmortality and morbidity are well established. It wastherefore recommended that chicken cell derivedvaccines, which have a major role in internationalimmunization programmes, should continue to beused.
Moreover, it was considered that the cell substrateused in the production of a live vaccine is a criticalparameter in the level of attenuation or virulence oflive vaccine viruses. If the cells used for productionare changed, there could be unknown effects onthe safety and efficacy of these vaccines. Thus, anyalternative cell substrate developed for the produc-tion of a live viral vaccine would be considered asnovel development. In this case, the vaccine wouldneed to be resubmitted for regulatory approval,thereby halting the continued production of vac-cines which are urgently needed for public healthprogrammes.
141
WHO Drug Information Vol. 12, No. 3, 1998
References
1. WHO Expert Committee on Biological Standardization.Weekly Epidemiological Record, 71: 105–112 (1996).
2. World Health Organization. Requirements for measles,mumps and rubella vaccines and combined vaccine (live).In: WHO Expert Committee on Biological Standardization:forty-third report. WHO Technical Report Series, No. 840,1994.
3. Böni, J., Stalder, J. Reigel, F. Detection of reversetranscriptase activity in live attenuated virus vaccines.Clinical and Diagnostic Virology, 5:43–53 (1996).
4. Bauer, G., Hofschneider, P.H. An RNA-dependent DNApolymerase, different from the known viral reversetranscriptases, in the chicken system. Proceedings of theNational Academy of Science, 73: 3025–3029 (1976).
5. World Health Organization. Consultation on issuesrelated to the presence of reverse transcriptase activityand chicken-cell derived vaccines. Unpublished documentWHO/BLG/RTASE 98.1.
Consumer protection andherbal remedies
Mohamed H. FarahUppsala Monitoring CentreSweden
The use of herbal remedies has increased signifi-cantly in developed countries in the last decade,and this trend shows every sign of continuing.Herbal preparations have recognized medicinalvalue, and many are free of the problems associ-ated with some synthetic pharmaceuticals. Becausethey have been used to treat illness for hundreds ofyears, it is assumed that they must be safe. How-ever, with the rise in popularity and increased use itis necessary to assure product quality and safetyand implement regulatory control of the manufactur-ing process and licensing of traders.
An essential element in the quality assurance ofherbals is the correct identification of a product.This may be difficult to achieve since, in manycases, a common, local name is used. Alternatively,the product may have been adulterated or substi-tuted by other mixtures. There may be no routinetests to monitor the intended amounts of activeingredient before and after processing. A singlespecies may be known by different Latin namesand also by many common names which can varyfrom country to country.
Moreover, it is not unusual for a common name tobe used for two or more different species. Unlessthe names of herbal plants follow an internationalsystem of plant nomenclature, the potential forconfusion when exchanging information is enor-mous. The information attached to a name is thuscrucial. As an example, because common namesare often used, heliotrope (Heliotropiumeuropaeum) — containing potent hepatotoxins — isoften confused with garden heliotrope (Valerianaofficinalis), which is used as a sedative and musclerelaxant. Identification of the herbal preparation bythe Latin binomial system, in addition to the com-mon name, is therefore essential.
When administering herbals, the dose of an activesubstance determines its usefulness and safety.Manufacturing controls are therefore important todetermine potency and manufacturers of herbalremedies should develop international standards ofidentity and quality control. In order to regulateunrealistic claims on retail products, labelling andadvertising should comply with accepted criteria forpromotional practice.
A review of medical literature will often fail to pro-vide full information on the safety and efficacy ofthe overwhelming majority of herbal remedies.Adverse effects vary greatly, and will depend on theparticular species of plant, when and how it isharvested, the part of the plant being used and howthe plant material is processed. The Uppsala Moni-toring Centre in Sweden has recently begun collect-ing data on the safety and toxicity of herbal medi-cines from all over the world. These data are ofimmediate relevance to health professionals andproducers of herbal medicines.
The Centre represents a component of the WHOInternational Drug Monitoring Programme which ismade up of over 50 national monitoring centres.Reports of suspected adverse reactions to pharma-ceuticals, vaccines and, now, herbal remedies aresent by health professionals to national monitoringcentres and from there forwarded to the data baselocated at the Centre. With more and more coun-tries joining the programme, the number of reportsof adverse reactions to herbal preparations isincreasing. However, to be able to effectivelymonitor the safety of all herbal medicines, thereporting system has to be developed further andreporting should be promoted among health profes-sionals.
Current Topics

142
WHO Drug Information Vol. 12, No. 3, 1998Current Topics
Any physician who has a patient taking a particularherbal medicine should document and report anyclinical events which may result. If the patient isalso taking a prescription medicine, interactionsmust be noted. If any of the active ingredients isexpected to act in an antagonistic or synergisticmanner, an alternative medication should be soughtor the herbal remedy changed.
In order to enter information into the data base, anATC (anatomical, therapeutic, chemical) classifica-tion is being developed. Several internationalexperts and centres, including the Royal Garden atKew in the United Kingdom, are involved in settingup the data base. It is hoped that in the future amonograph will be available for each plant speciesor active part of a plant.
It is very important that regulations on herbal medi-cines should clearly distinguish between plantswhich can safely be used under most circum-stances and at reasonable quantities, and specificherbs with potent, addictive, or otherwise danger-ous properties.
Information on the data base can be obtained from:Uppsala Monitoring Centre, S75320 Uppsala, Sweden.e-mail: [email protected]; internet: http://www.who.pharmasoft.se
Indiscriminate antibiotic use inanimals — public healthimplicationsThe frequency of resistant bacteria and the numberof drugs to which they are resistant is increasing atan unprecedented rate and has begun to compro-mise the efficient treatment of patients. Althoughthe gravity of the problem has been brought to theattention of governments, industry and the generalpublic, action is urgently needed if the problem isnot to escalate into a full-scale public health disas-ter.
Reports of importation into the United Kingdom ofEscherichia coli resistant to all beta-lactam antibi-otics (1) further demonstrate that antibiotic resist-ance knows no boundaries. A recent study hasshown that the prevalence of multidrug-resistantsalmonella infections in the United States ofAmerica has increased from 0.6% in 1980 to 34%in 1996 (2). The trend is the same for other coun-tries, as confirmed by a recent report from theSelect Committee on Science and Technology
commissioned by the House of Lords in the UnitedKingdom (3). Isolates that were already resistant toampicillin, chloramphenicol, streptomycin, sul-phonamides and tetracycline were found to be 14%resistant to ciprofloxacin and 24% resistant totrimethoprim in 1996. This finding was even morestriking because there was no resistance five yearspreviously in 1991 (4). An analysis of approximately25 000 pathogens by the SENTRY antimicrobialsurveillance programme indicated a 46% rate ofpenicillin-resistant Streptococcus pneumoniae inthe USA and a rate ranging between 0.1 and 30%in European countries.
Two major factors contribute to antibiotic resist-ance, namely, the antibiotic itself and the type ofresistance traits under selection (5). As a furthercomplication, these traits can be spread amongdifferent bacteria. Resistance displayed by bacteriareflects the environment in which the organismthrives and genes that have been prevalent inpathogenic bacteria for many years develop pointmutations conferring resistance to broad-spectrumantibiotics.
Certain antimicrobials used for treatment or growthpromotion in agriculture are also used for diseasecontrol in humans and it has been estimated thatmore than 50% of antimicrobials are produced forpurposes other than human medical use. In theUnited States, of the 23 million kilograms of antibi-otics produced annually, over 40% are for animaluse. Of this amount, 80% is used subtherapeutic-ally as a growth promoter. The use of antibiotics atsubthera-peutic concentrations to enhance growthin animals and for farming purposes has increasedresistance (5). Animal use of avoparcin, a glyco-peptide growth promoter is, at least in part, respon-sible for the emergence of vancomycin-resistantenterococci in animals and the same vancomycin-resistant clone of enterococci has been found inanimals and humans (6). These findings have led toa ban on avoparcin in the European Union and asimilarly acting product, virginiamycin, in Denmark(5).
Use of antibiotics in animals for therapeutic indica-tions has also caused concern. A Food and DrugAdministration expert panel has recommendedcaution in the approval of quinolones for use inanimals because of the potential consequences forpeople. Use of fluoroquinolones, including enro-floxacin and danofloxacin, in animal husbandry hasalready led to antibiotic resistance among thezoonotic pathogens campylobacter and salmonella(7).
143
WHO Drug Information Vol. 12, No. 3, 1998
Thus, antibiotic resistance, which was initially aproblem for hospitals and developing countries,now affects the world at large. Its control will requireaction that focuses not only on medical but onveterinary, agricultural and aquacultural use inorder to minimize the environmental impact. Misuseof antibiotics for viral diseases should be addressedby education of consumers and prescribers. Fur-thermore, use in animals should be limited totreatment which does not perpetuate the selectionof resistance. The smaller the extent of exposure toantibiotics, the less likely the selection and transferof resistance traits among environmental bacteriaand the lower the probability that a resistant patho-gen will arise.
References
1. M'Zali, F.H., Heritage, J., Gascoyne-Binzi, D.M. et al.Transcontinental importation into the UK of Escherichiacoli expressing a plasmid-mediated AmpC-type b-lactamase exposed during an outbreak of SHV-5extended spectrum b-lactamase in a Leeds Hospital.Journal of Antimicrobial Chemotherapy, 40: 823–831(1997).
2. Glynn, M.K., Bopp, C., Dewitt, W. Emergence ofmultidrug resistant Salmonella enterica serotypetyphimurium DT104 infections in the United States. TheNew England Journal of Medicine, 338: 1333–1338(1998).
3. House of Lords Select Committee on Science andTechnology: Resistance to Antibiotics and other antimicro-bial agents. 7th report. Session 1997–1998. The Station-ary Office, London, 1998.
4. Threlfall, E.J. Ward, L.R., Rowe, B. Incidence ofresistance to trimethoprim and ciprofloxacin in epidemicSalmonella typhimurium DT104 in England and Wales.Eurosurveillance, 2: 81–84 (1997).
5. Levy, S.B. Multidrug resistance — a sign of the times.The New England Journal of Medicine, 338: 1376–1378(1998).
6. van den Bogaard, A.E., Jensen, L.B., Strobberingh,E.E. Vancomycin-resistant enterococci in turkeys andfarmers. New England Journal of Medicine, 337: 1558–1559 (1997).
7. Endtz, H.P., Ruijs, G.J., van Kilingeren, B. et al.Quinolone resistance in campylobacter isolated from manand poultry following the introduction of fluoroquinolonesin veterinary medicine. Journal of Antimicrobial Chemo-therapy, 27: 199–208 (1991).
Future trends inbiological standardizationThe report of the WHO Expert Committee on Bio-logical Standardization (ECBS), which held its 48thmeeting in Geneva in October 1997, will shortly bepublished in the WHO Technical Report Series. Thepurpose of the ECBS is to review developmentsand recommend procedures to assure the quality,safety and efficacy of biological substances used inmedicine. The increasing complexity and sophisti-cation of these substances, as well as the rapidgrowth in their volume, present a considerablechallenge for regulatory authorities, especially inthe developing world.
Many of the items on the agenda of the ECBSmeeting reflect the expanding capacity of biologicaltechnology and the increased diversity of newproducts. Some traditional substances have nowbeen replaced by recombinant DNA products, andnew diagnostic processes such as gene amplifica-tion techniques for virological safety testing of bloodand blood products have been developed. Newapproaches to in-process testing procedures usingmolecular-based techniques are also set to reducetesting in animals. The complexity of availablebiological products underlines the importance ofWHO as a source of expertise and a facilitator ofthe exchange of information worldwide.
During the meeting, the ECBS adopted guidelinesfor the production and quality control of syntheticpeptide vaccines. Development of this kind ofvaccine is still at an early stage and a flexibleapproach to control is needed. The importance ofproviding evidence of consistency from batch tobatch based on physicochemical techniques isemphasized, but biological characterization will alsoplay a critical role. Because synthetic peptidevaccines are not all produced in the same way,each vaccine will need to be given careful individualconsideration of its specific features. Flexibilityshould be exercised in the application of the guide-lines in order to reflect the intended clinical use.
Requirements for inactivated tick-borne encephalitisvaccine were also adopted by the ECBS. Tick-borne encephalitis is an acute viral infection causedby two closely-related viruses of the Flaviviridaefamily, and transmitted to man by ticks. The dis-ease is endemic in forested areas of central Europeand in Asia, where vaccination is considered animportant public health measure. The requirementshave been formulated to take account of currentmanufacturing processes and controls and provide
Current Topics
144
WHO Drug Information Vol. 12, No. 3, 1998
for production of vaccine in chicken embryos or oncontinuous cell lines. The vaccines are preparedfrom harvested virus propagated on appropriatecells and this procedure is followed by inactivation,purification and formulation.
In addition, guidelines for thromboplastins andplasma used to control oral anticoagulant therapywere adopted. These represent the current state ofthe art. In producing the guidelines, major changeswere made to the previous requirements estab-lished in 1983 following extensive consultation anddiscussions with international associations andexperts.
The test for potency to be performed by manufac-turers on recombinant hepatitis B vaccines wasestablished in 1989. Since that time, in vitro po-tency tests based on ELISA have been developed.
Current Topics
These assays are product specific and have beenvalidated by demonstrating a correlation withmouse immunogenicity test results. An amendmentto the requirements has thus been adopted by theECBS to permit the use of in vitro tests validated bycorrelation with the immune response in humans orwith results obtained in mouse immunogenicitytests.
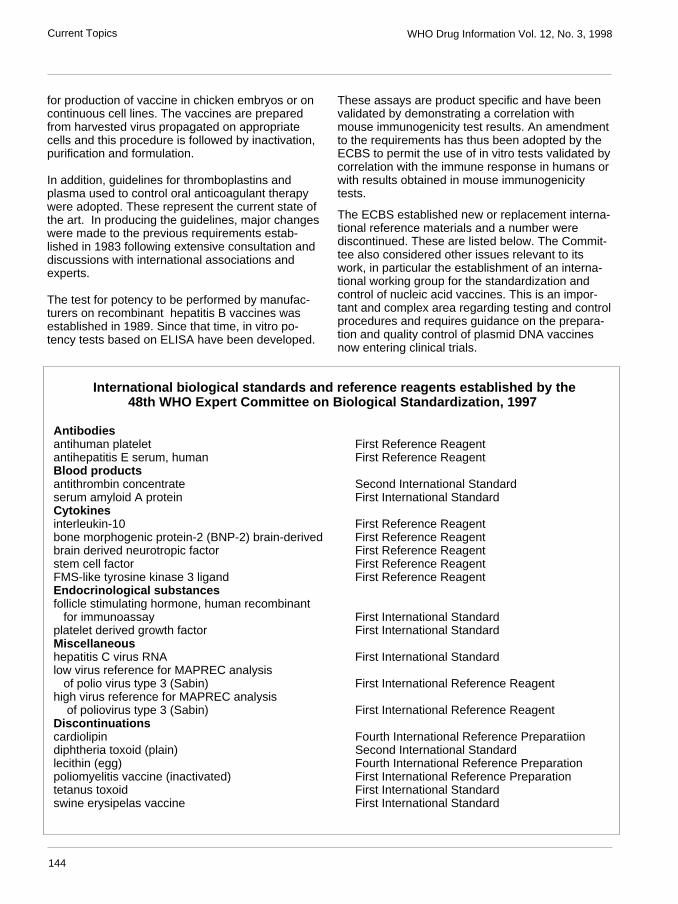
The ECBS established new or replacement interna-tional reference materials and a number werediscontinued. These are listed below. The Commit-tee also considered other issues relevant to itswork, in particular the establishment of an interna-tional working group for the standardization andcontrol of nucleic acid vaccines. This is an impor-tant and complex area regarding testing and controlprocedures and requires guidance on the prepara-tion and quality control of plasmid DNA vaccinesnow entering clinical trials.
International biological standards and reference reagents established by the48th WHO Expert Committee on Biological Standardization, 1997
Antibodiesantihuman platelet First Reference Reagentantihepatitis E serum, human First Reference ReagentBlood productsantithrombin concentrate Second International Standardserum amyloid A protein First International StandardCytokinesinterleukin-10 First Reference Reagentbone morphogenic protein-2 (BNP-2) brain-derived First Reference Reagentbrain derived neurotropic factor First Reference Reagentstem cell factor First Reference ReagentFMS-like tyrosine kinase 3 ligand First Reference ReagentEndocrinological substancesfollicle stimulating hormone, human recombinant for immunoassay First International Standardplatelet derived growth factor First International StandardMiscellaneoushepatitis C virus RNA First International Standardlow virus reference for MAPREC analysis of polio virus type 3 (Sabin) First International Reference Reagenthigh virus reference for MAPREC analysis of poliovirus type 3 (Sabin) First International Reference ReagentDiscontinuationscardiolipin Fourth International Reference Preparatiiondiphtheria toxoid (plain) Second International Standardlecithin (egg) Fourth International Reference Preparationpoliomyelitis vaccine (inactivated) First International Reference Preparationtetanus toxoid First International Standardswine erysipelas vaccine First International Standard
145
WHO Drug Information Vol. 12, No. 3, 1998
Regulatory Matters
Mibefradil: harmful interactionsThe new selective calcium channel blocker, mibe-fradil, which is indicated for hypertension andchronic stable angina, has been voluntarily with-drawn from the market by the manufacturer as aresult of new information about potentially harmfulinteractions with other drugs, making safe use ofthe drug too complex (1, 2).
As reported previously (3), mibefradil interactsdangerously with many commonly prescribedcardiovascular drugs. Principally, it inhibits theactivity of certain liver enzymes which are importantfor drug elimination, resulting in an accumulation atdangerous levels.
More than 25 drugs are presently known to bepotentially dangerous if used with mibefradil and,since the drug has not been shown to offer benefitsover and above those of drugs in the same thera-peutic group which are currently marketed, its useis considered to be an unreasonable risk to con-sumers (1). Patients taking mibefradil are advisednot to discontinue treatment, but to consult a physi-cian about appropriate alternative therapy.
References:
1. Dear Doctor letter from Roche Laboratories Inc. datedJune 8 1998 and circulated under cover of FDA TalkPaper T98-33, 1998
2. Dear Doctor letter from Roche Products Ltd. dated 8June 1998 and circulated by Medicines Control Agency onhttp://www.open.gov.uk/mca.
3. WHO Drug Information, 12: 14–15 (1998).
HIV vaccine trial approvedUnited States of America — The Food and DrugAdministration has given an FDA investigationalnew drug approval for the first phase III clinical trialof a candidate HIV-1 vaccine (1, 2).
The trial will be a placebo controlled study of 5000healthy volunteers who have tested negative forHIV, but are at high risk of contracting the disease.Approval has also been requested for a similar trial
to be carried out in 2500 injecting drug users inThailand (3).
The vaccine is composed of recombinant gp120envelope antigens from two HIV-1 strains. In earlierphase I and II trials carried out in some 1200 peo-ple, the vaccine induced a strong circulating anti-body response in 99% of subjects. The presentphase III trials are meant to demonstrate whetherand to what extent these antibodies protect againstHIV (4).
References
1. Letter dated 2 July 1998 to WHO from the Office ofVaccines Research and Review, Center for BiologicsEvaluation and Research, Food and Drug Administration,United States of America.
2. Communication to UNAIDS from Don Francis, VaxGen,dated 10 July 1998.
3. Approval given for trials of AIDS vaccine. BritishMedical Journal, 316: 1769 (1998).
4. 1. HIV-1 vaccine trial go-ahead reawakens ethicsdebate. Lancet, 351: 1789 (1998).
Counterfeiting: halothanereplaced by chloroformPakistan — The provincial drug testing laboratoryin Peshawar has detected a counterfeit productlabelled as a general anaesthetic containing halo-thane. However, the genuine active ingredient hasbeen replaced with chloroform, a hepatotoxiccompound. The counterfeit product, which isclaimed to be produced by Zeneca in the UnitedKingdom, was purchased in a local market but isalso believed to be supplied to a number of privateand public hospitals.
Reference: The Network Newsletter, December 1997.
Warfarin interaction withmiconazole oral gelAustralia — The Adverse Drug Reaction AdvisoryCommittee has received 11 reports documenting an
146
WHO Drug Information Vol. 12, No. 3, 1998Regulatory Matters
interaction between warfarin and miconazole oralgel. Antifungal agents are known to inhibit cyto-chrome P450 enzymes and potentiate the anti-coagulant effect of warfarin. The internationalnormalized ratio (INR) in some cases was elevatedto as high as 15.6. Five cases were symptomless,but 6 patients developed bruising, haematuria ormucocutaneous bleeding.
Since miconazole oral gel is applied topically, it ispresumed that absorption is limited. However,systemic absorption is possible through inflamedmucosa and ingestion from the gastrointestinaltract.
In many countries miconazole oral gel is availablewithout prescription and warfarin patients will needto be warned of this interaction.
Reference: Australian Adverse Drug Reactions Bulletin,May 1998.
Nandrolone-containingproducts withdrawnFrance — All medical products containing theanabolic steroid, nandrolone, have been withdrawnfrom the market following a re-evaluation of theclinical data supporting efficacy. These productswere indicated for malnutrition in the elderly, post-surgical treatment and for major burns. One eye-drop formulation remains on the market.
Reference: Letter to WHO from the Agence duMédicament dated 3 April 1998.
Sibutramine scheduled as acontrolled substanceUnited States of America — In November 1997,sibutramine was approved by the Food and DrugAdministration as an oral anorectic for the long-termmanagement of obesity.
Sibutramine produces central nervous stimulationand amphetamine effects in humans. It has nowbeen placed under schedule IV of the ControlledSubstances Act since it is considered as having alow abuse potential which may lead to limitedphysical and psychological dependence.
Reference: Federal Register, 63(28): 6862–6864 (1998).
Bromfenac withdrawalUnited States of America — In July 1997, theFood and Drug Administration approvedbromfenac, a nonsteroidal anti-inflammatory drug,for the short-term management of pain. Followingreports of severe liver failure requiring transplanta-tion, the labelled warning was reinforced by themanufacturer in February 1998 (1).
It has now been decided to withdraw the product asa result of 4 deaths, 8 cases of liver transplantationand 12 reports of liver damage. In patients whohave taken the drug for longer than the recom-mended 10 days, it has been estimated that severeliver injury occurs in 1 in every 10 000–20 000people. Given the availability of other therapies, itwas not considered practical to implement therestrictions necessary to ensure safe use of lessthan 10 days.
References
1. WHO Drug Information 12: 2 (1998).
2. FDA Talk Paper, June 1998.
Discontinuation of internationalantibiotic reference preparationsWorld Health Organization — The WHO ExpertCommittee on Biological Standardization hasdiscontinued the international reference prepara-tions for a number of antibiotics because require-ments in major pharmacopoeias no longer imposea microbiological assay. The antibiotics in questionare doxycycline, demecycline (demethylchlor-tetracycline), minocycline, oxytetracycline, andtetracycline.
It should be noted that discontinuation of the inter-national reference preparation for these antibioticswill automatically mean discontinuation of theinternational unit (IU) for these substances.
Reference: Biologicals Unit, Division of Drug Manage-ment and Policies, World Health Organization, Geneva.
Seratrodast and hepaticdysfunctionJapan — The Ministry of Health and Welfare hasissued a warning regarding hepatic dysfunction
147
WHO Drug Information Vol. 12, No. 3, 1998 Regulatory Matters
associated with the use of seratrodast, for thetreatment of bronchial asthma. Hepatic dysfunctionwas reported in 49 patients, of whom 4 died fromfulminant hepatitis. The product information hasbeen amended to advise that liver function testsshould be performed periodically. In the event ofabnormal tests, treatment should be interrupted.
Reference: Pharma Japan, Number 11594, April 1998.
Meloxicam safety similar toother NSAIDsSweden — The Medical Products Agency hasanalysed reports of adverse drug reactions re-ceived for meloxicam, a cyclooxygenase (COX-2)inhibitor that has been claimed to cause less gas-trointestinal reactions than other NSAIDs.
During the first year of marketing, 15 adversereactions have been reported. Of these, 5 caseswere for skin reactions and 6 of gastrointestinaldisturbances. Although use of the drug has beenlimited, these reports suggest that meloxicam mayhave a similar safety profile to other NSAIDs.
Reference: Info från Läkemedelsverket, 2: 56 (1998).
Proxibarbal withdrawnfrom the marketFrance — The barbiturate, proxibarbal, which hasbeen marketed since 1977 has been re-evaluatedby the Adverse Drug Reactions Board of the Medi-cines Agency. In carrying out the review it wasconcluded that proxibarbal may induceimmunoallergenic thrombopenia with potentiallysevere health consequences. The marketing au-thorization has consequently been suspended andthe manufacturer has withdrawn the product fromthe market. Proxibarbal is still available in Hungaryand Poland.
Reference: Communication to WHO from the Agence duMédicament, April 1998.
Cholestin an unapproved drugUnited States of America — The Food and DrugAdministration has determined that cholestin, a
product marketed as a dietary supplement intendedto affect cholesterol levels, is an unapproved drug.Cholestin is derived from yeast grown on red ricebut also contains lovastatin and unsaturated fattyacids.
Since November 1997, the Food and Drug Adminis-tration has made an extensive review to determinewhether to regulate cholestin. Lovastatin is theactive ingredient of an already marketed prescrip-tion drug to lower cholesterol levels. It was there-fore considered that cholestin cannot be consideredpurely as a food supplement (1).
Meanwhile, the company has contested the deci-sion and will be allowed to continue marketingduring the appeal period. When a final decision onthis case has been reached, a clearer definition ofthe regulatory status of drugs, dietary supplementsand food will have been established (2).
References
1. FDA Talk Paper, T98–28, May 1998.
2. SCRIP, No. 2348, 1 July 1998.
Vigabatrin and visual defectsVigabatrin is indicated for the treatment of epilepsynot satisfactorily controlled by other drugs and asmonotherapy for infantile spasms. The Committeeon Safety of Medicines has reminded physiciansthat since 1989, 41 reports of visual field defectshave been received in connection with this product(1). Epidemiological studies suggest that 15 out of10 000 patients treated yearly within Europe experi-ence symptoms of visual field defects (2). Onsetcan vary from one month to several years aftertaking vigabatrin.
Patients should be warned to report any new visualsymptoms and they must be referred to an ophthal-mologist if this occurs.
References
1. Medicines Control Agency. Current Problems, Number24, 1998.
2. Info från Läkemedelsverket, 2: 57 (1998).

148
WHO Drug Information Vol. 12, No. 3, 1998
ATC level INN/common name ATC code
New ATC level codes (other than 5th level):Colony stimulating factors L03A AInterferons L03A BInterleukins L03A CNucleoside reverse transcriptase inhibitors J05A FNon-nucleoside reverse transcriptase inhibitors J05A G
New ATC 5th level codes: alteplase S01X A13ancestim L03A A12betamethasone S02B A07capecitabine L01B C06cerivastatin C10A A06copper usnate G01A X15daclizumab L04A A08desogestrel G03A C09entacapone N04B X02etonogestrel G03A C08fibrinogen, human B02B C10glatiramer acetate L04A A07grepafloxacin J01M A11haemoglobin crosfumaril B05A A08heparinoid, combinations C05B A51magnesium pyridoxal 5-phosphate glutamate C10A X07nucleoside reverse transcriptase inhibitors, combinations J05A F30phentolamine G04B E05rituximab L01X X20sodium phenylbutyrate A16A X03tasosartan C09C A05technetium (99mTc) apcitide V09G A07tolterodine G04B D07vorozole L02B G05
Change of name:previous: (cytokines)new: colony stimulating factor L03A A
The following final classifications were agreed at a meeting of the WHO International Drug UtilizationWorking Group which took place from 27–28 October 1997 in Oslo. They came into force on 30 April 1998.All requests for classification should be forwarded to the WHO Collaborating Centre for Drug StatisticsMethodology, P.O. Box 100, Veivet, 0518, Oslo, Norway (telephone: 00 47 22 16 9811, fax: 0047 22 16 9818,e-mail: [email protected]). The inclusion of a substance in the lists does not imply any recommendation ofuse in medicine or pharmacy.
ATC/DDD Classification (final)
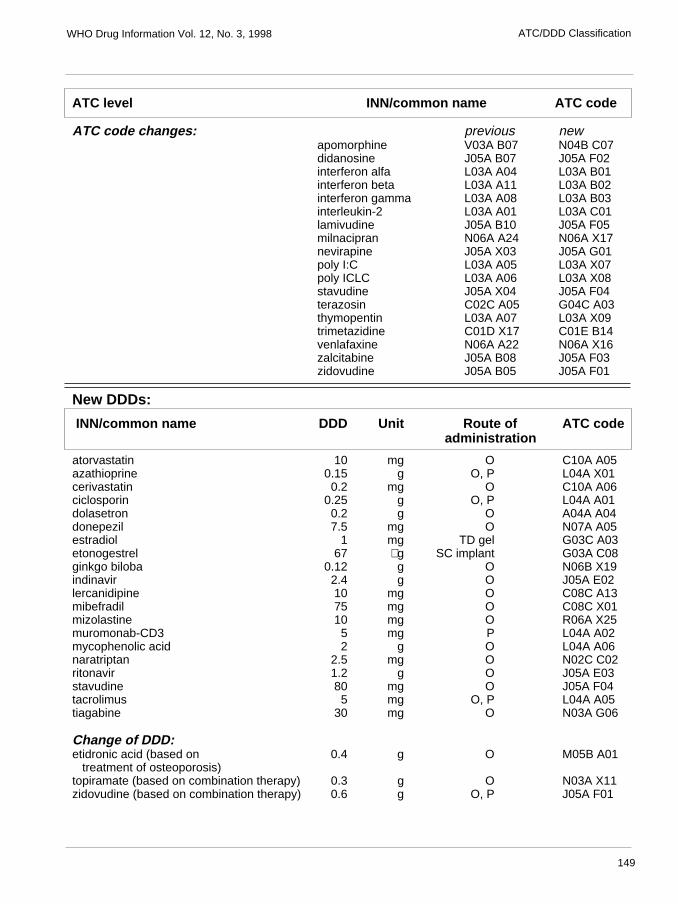
149
WHO Drug Information Vol. 12, No. 3, 1998
ATC level INN/common name ATC code
ATC code changes: previous newapomorphine V03A B07 N04B C07didanosine J05A B07 J05A F02interferon alfa L03A A04 L03A B01interferon beta L03A A11 L03A B02interferon gamma L03A A08 L03A B03interleukin-2 L03A A01 L03A C01lamivudine J05A B10 J05A F05milnacipran N06A A24 N06A X17nevirapine J05A X03 J05A G01poly I:C L03A A05 L03A X07poly ICLC L03A A06 L03A X08stavudine J05A X04 J05A F04terazosin C02C A05 G04C A03thymopentin L03A A07 L03A X09trimetazidine C01D X17 C01E B14venlafaxine N06A A22 N06A X16zalcitabine J05A B08 J05A F03zidovudine J05A B05 J05A F01
New DDDs:
INN/common name DDD Unit Route of ATC code administration
atorvastatin 10 mg O C10A A05azathioprine 0.15 g O, P L04A X01cerivastatin 0.2 mg O C10A A06ciclosporin 0.25 g O, P L04A A01dolasetron 0.2 g O A04A A04donepezil 7.5 mg O N07A A05estradiol 1 mg TD gel G03C A03etonogestrel 67 µg SC implant G03A C08ginkgo biloba 0.12 g O N06B X19indinavir 2.4 g O J05A E02lercanidipine 10 mg O C08C A13mibefradil 75 mg O C08C X01mizolastine 10 mg O R06A X25muromonab-CD3 5 mg P L04A A02mycophenolic acid 2 g O L04A A06naratriptan 2.5 mg O N02C C02ritonavir 1.2 g O J05A E03stavudine 80 mg O J05A F04tacrolimus 5 mg O, P L04A A05tiagabine 30 mg O N03A G06
Change of DDD:etidronic acid (based on 0.4 g O M05B A01 treatment of osteoporosis)topiramate (based on combination therapy) 0.3 g O N03A X11zidovudine (based on combination therapy) 0.6 g O, P J05A F01
ATC/DDD Classification
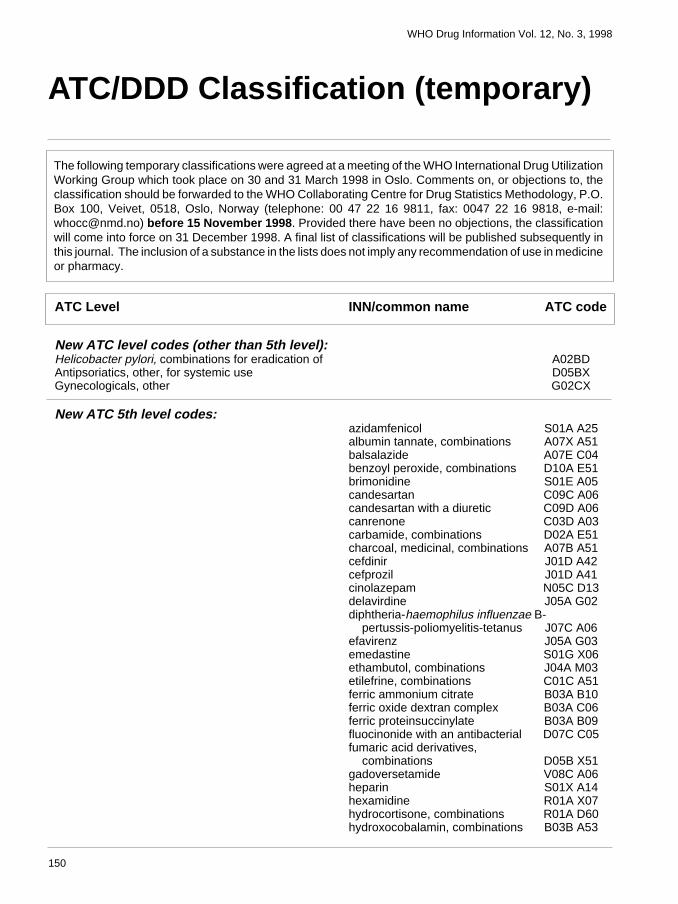
150
WHO Drug Information Vol. 12, No. 3, 1998
ATC/DDD Classification (temporary)
The following temporary classifications were agreed at a meeting of the WHO International Drug UtilizationWorking Group which took place on 30 and 31 March 1998 in Oslo. Comments on, or objections to, theclassification should be forwarded to the WHO Collaborating Centre for Drug Statistics Methodology, P.O.Box 100, Veivet, 0518, Oslo, Norway (telephone: 00 47 22 16 9811, fax: 0047 22 16 9818, e-mail:[email protected]) before 15 November 1998. Provided there have been no objections, the classificationwill come into force on 31 December 1998. A final list of classifications will be published subsequently inthis journal. The inclusion of a substance in the lists does not imply any recommendation of use in medicineor pharmacy.
ATC Level INN/common name ATC code
New ATC level codes (other than 5th level):Helicobacter pylori, combinations for eradication of A02BDAntipsoriatics, other, for systemic use D05BXGynecologicals, other G02CX
New ATC 5th level codes:azidamfenicol S01A A25albumin tannate, combinations A07X A51balsalazide A07E C04benzoyl peroxide, combinations D10A E51brimonidine S01E A05candesartan C09C A06candesartan with a diuretic C09D A06canrenone C03D A03carbamide, combinations D02A E51charcoal, medicinal, combinations A07B A51cefdinir J01D A42cefprozil J01D A41cinolazepam N05C D13delavirdine J05A G02diphtheria-haemophilus influenzae B- pertussis-poliomyelitis-tetanus J07C A06efavirenz J05A G03emedastine S01G X06ethambutol, combinations J04A M03etilefrine, combinations C01C A51ferric ammonium citrate B03A B10ferric oxide dextran complex B03A C06ferric proteinsuccinylate B03A B09fluocinonide with an antibacterial D07C C05fumaric acid derivatives, combinations D05B X51gadoversetamide V08C A06heparin S01X A14hexamidine R01A X07hydrocortisone, combinations R01A D60hydroxocobalamin, combinations B03B A53
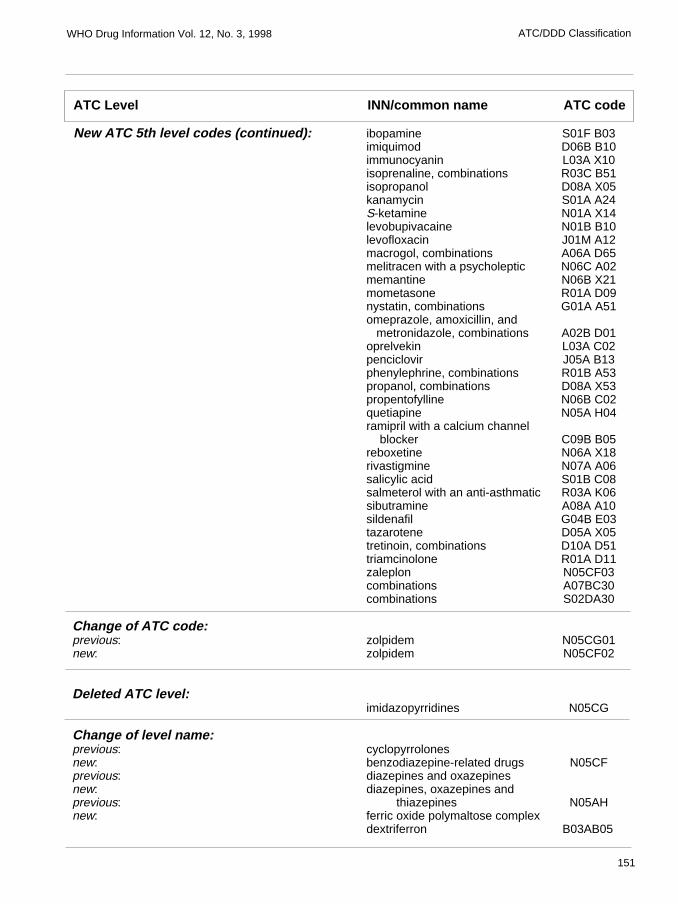
151
WHO Drug Information Vol. 12, No. 3, 1998
ibopamine S01F B03imiquimod D06B B10immunocyanin L03A X10isoprenaline, combinations R03C B51isopropanol D08A X05kanamycin S01A A24S-ketamine N01A X14levobupivacaine N01B B10levofloxacin J01M A12macrogol, combinations A06A D65melitracen with a psycholeptic N06C A02memantine N06B X21mometasone R01A D09nystatin, combinations G01A A51omeprazole, amoxicillin, and metronidazole, combinations A02B D01oprelvekin L03A C02penciclovir J05A B13phenylephrine, combinations R01B A53propanol, combinations D08A X53propentofylline N06B C02quetiapine N05A H04ramipril with a calcium channel blocker C09B B05reboxetine N06A X18rivastigmine N07A A06salicylic acid S01B C08salmeterol with an anti-asthmatic R03A K06sibutramine A08A A10sildenafil G04B E03tazarotene D05A X05tretinoin, combinations D10A D51triamcinolone R01A D11zaleplon N05CF03combinations A07BC30combinations S02DA30
Change of ATC code:previous: zolpidem N05CG01new: zolpidem N05CF02
Deleted ATC level:imidazopyrridines N05CG
Change of level name:previous: cyclopyrrolonesnew: benzodiazepine-related drugs N05CFprevious: diazepines and oxazepinesnew: diazepines, oxazepines andprevious: thiazepines N05AHnew: ferric oxide polymaltose complex
dextriferron B03AB05
ATC Level INN/common name ATC code
New ATC 5th level codes (continued):
ATC/DDD Classification
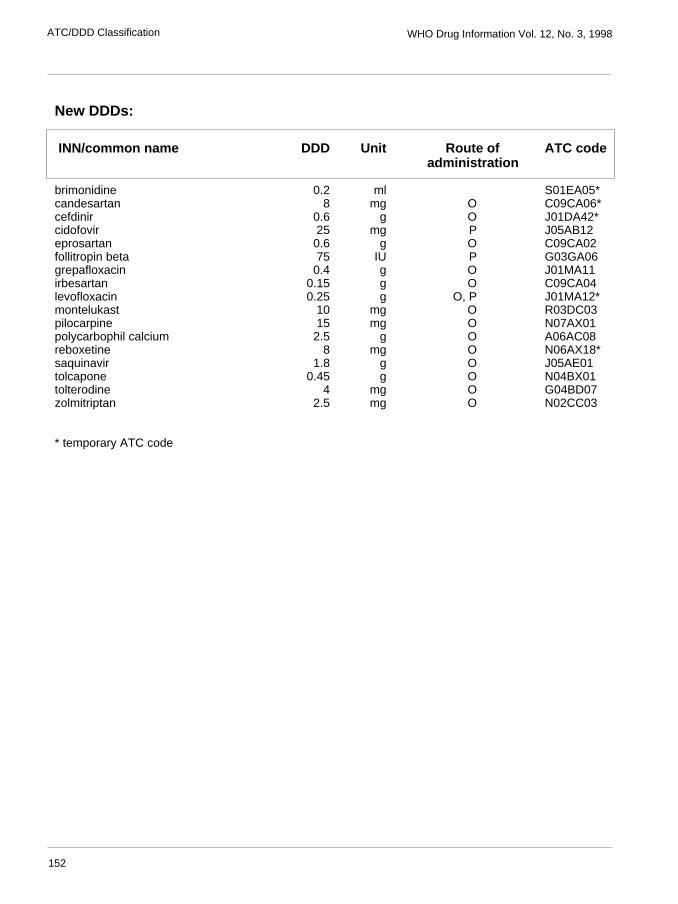
152
WHO Drug Information Vol. 12, No. 3, 1998ATC/DDD Classification
New DDDs:
INN/common name DDD Unit Route of ATC code administration
brimonidine 0.2 ml S01EA05*candesartan 8 mg O C09CA06*cefdinir 0.6 g O J01DA42*cidofovir 25 mg P J05AB12eprosartan 0.6 g O C09CA02follitropin beta 75 IU P G03GA06grepafloxacin 0.4 g O J01MA11irbesartan 0.15 g O C09CA04levofloxacin 0.25 g O, P J01MA12*montelukast 10 mg O R03DC03pilocarpine 15 mg O N07AX01polycarbophil calcium 2.5 g O A06AC08reboxetine 8 mg O N06AX18*saquinavir 1.8 g O J05AE01tolcapone 0.45 g O N04BX01tolterodine 4 mg O G04BD07zolmitriptan 2.5 mg O N02CC03
* temporary ATC code
153
WHO Drug Information Vol. 12, No. 3, 1998
Essential Drugs
As described in previous issues of this journal, work is now under way on the WHO ModelFormulary, and draft texts will be published regularly to obtain comments on the materialproposed for publication. Observations concerning the following sections should be addressedto: Drug Selection and Information (DSI), Division of Drug Management & Policies, WorldHealth Organization, 1211 Geneva 27, Switzerland.
WHO Model Formulary
Immunosuppressives, anti-neoplastics and drugs usedin palliative care
Immunosuppressive drugsImmunosuppressive drugs are administered to reci-pients of tissue or organ transplants to suppress therejection mechanism, or as a second-line drug inrheumatology and dermatology. Because immuno-suppressives are non-specific in their action, carefulmonitoring of the peripheral blood count is required,with dose adjustments to prevent bone-marrowtoxicity. Patients receiving these drugs are particu-larly prone to atypical infections. Treatment shouldonly be initiated by a specialist.
Azathioprine is the most widely used drug fortransplant recipients. It is useful when corticosteroidtherapy alone has proven inadequate or for otherconditions when a reduction in the dosage of con-currently administered corticosteroids is required. Itis metabolized to mercaptopurine and doses there-fore need to be reduced when this drug is usedconcurrently with allopurinol. The predominant toxiceffect is myelosuppression, although hepatic toxic-ity is also a known reaction.
Ciclosporin is a potent immunosuppressant which isvirtually free of myelotoxic effects, but is markedlynephrotoxic. It is particularly useful for prevention ofgraft rejection or graft-versus-host disease. Thedose is adjusted by monitoring blood-ciclosporinconcentrations (trough concentration) and renalfunction. Dose-related increases in serum creati-nine and blood urea nitrogen (BUN) during the firstfew weeks may necessitate dose reduction.
Corticosteroids such as prednisolone have signifi-cant immunosuppressant activity and can also beused to prevent rejection of organ transplants.
AZATHIOPRINETablet: 50 mgPowder for injection: 100 mg (as sodium salt)in vial
Uses: As an adjunct to prevent rejection in trans-plant recipients and as a disease-modifying agentin other conditions in which corticosteroids are theprimary treatment, in order to reduce their use.
Dosage:3 mg/kg/day 1–3 days prior to surgery and at thetime of surgery. 1–2 mg/kg single daily dose asmaintenance therapy. Reduce the dose in theevent of renal or hepatic impairment and in elderlypatients.
Contraindications: Hypersensitivity to azathioprineand mercaptopurine.
Precautions: Weekly blood counts necessary forthe first 8 weeks of treatment and every 3 monthsthereafter.
Adverse effects: Hypersensitivity reactions, ma-laise, dizziness, vomiting, fever, muscular pains,arthralgia, disturbed liver function, cholestaticjaundice, arrhythmia, hypotension or interstitialnephritis call for immediate withdrawal.
Haematological toxicity includes leukopenia andthrombocytopenia, which may be reversible uponwithdrawal, and increased susceptibility to infec-tions. Gastrointestinal disturbances include nausea,vomiting and hepatotoxicity.
154
WHO Drug Information Vol. 12, No. 3, 1998Essential Drugs
Drug interactions: These will appear in tabulatedform in the appendix of the published edition of theWHO Model Formulary.
CICLOSPORINCapsule: 25 mgConcentrate for injection: 50 mg/ml in 1-mlampoule
Uses: In combination with corticosteroids, to pre-vent rejection of renal, hepatic and cardiac trans-plants. Treatment of chronic rejection in patientspreviously treated with other immuno-suppressants.Treatment of graft-versus-host disease after bone-marrow transplantation.
Dosage:Prevention of transplant rejectionOral administration adults and children:12–15 mg/kg daily administered 4–12 hours prior toand for 1–2 weeks after surgery. 5–10 mg/kg dailythereafter.
Intravenous infusion adults and children: 2–6 mg/kgdaily administered 4–12 hours prior to and followingsurgery until the patient can tolerate oral dosageforms. If necessary, one-third of the oral dose canbe given by intravenous infusion over 2–6 hours.
When given concomitantly with other immuno-suppressants, lower dosages should be used.
Prevention and treatment ofgraft-versus-host diseaseIntravenous infusion adults and children: 3–5 mg/kgdaily over 2–6 hours beginning on the day beforetransplant surgery to 2 weeks after surgery.
Oral administration adults and children: 12.5 mg/kgorally for 3–6 months, with a gradual dosage reduc-tion.
Precautions: Emergency care and facilities shouldbe available in the event of adverse reactions tociclosporin. Monitor renal and hepatic functions andblood pressure.
Adverse effects: Frequently, dose-related andreversible nephrotoxicity resulting in increases inserum creatinine and BUN unrelated to rejection,may require dosage adjustments. Electrolyte distur-bances including hyperkalaemia, hepatic dysfunc-tion, hypertension (especially in heart transplantpatients), incidence of malignancies and lympho-proliferation disorders, increased susceptibility to
infections due to immunosuppression, gynaeco-mastia, gastrointestinal disturbances, gingivalhyperplasia, allergic reactions, thrombocytopenia(sometimes with haemolytic uraemic syndrome)have been reported. Also, mild anaemia, tremors,convulsions, neuropathy, myopathy, or muscleweakness.
Drug interactions: These will appear in tabulatedform in the appendix of the published edition of theWHO Model Formulary.
Cytotoxic drugsThe treatment of cancer with drugs, radiotherapyand surgery is complex and should only be under-taken by an oncologist. For this reason, the follow-ing information is provided merely as a guideand the products mentioned should only be admin-istered by specialized medical personnel.
Chemotherapy may be curative, or used to alleviatesymptoms, or to prolong life. Where the conditioncannot be managed with cytotoxic drugs, alterna-tive palliative treatment (see page 163) should beconsidered. For some tumours, single-agentchemotherapy may be adequate, but for manymalignancies a combination of drugs provides thebest response. Examples of combination therapyinclude:
CHOP (cyclophosphamide, doxorubicin, vincristine,prednisolone) for non-Hodgkin disease.
ABVD (doxorubicin, bleomycin, vinblastine, dacar-bazine) for Hodgkin disease.
MOPP (mustine, vincristine, procarbazine, pred-nisolone) also for Hodgkin disease.
Drug combinations are, however, more toxic thansingle agents. Cytotoxic drugs are often combinedwith other classes of drugs in the treatment ofmalignant conditions. Such drugs include hormoneagonists and antagonists, corticosteroids andimmunostimulant drugs. The following informationcovers drugs that have specific antitumour activity.However, they are toxic and should be used withgreat care and monitoring. The specific doses forcytotoxic drugs have been omitted from this sectionsince treatment should be undertaken by specialistsusing agreed regimens. Health authorities may wishto formulate their own regimens on the basis ofexpert advice.
Precautions: Treatment with cytotoxic drugsshould be initiated only after baseline tests of liver
155
WHO Drug Information Vol. 12, No. 3, 1998 Essential Drugs
and kidney function have been performed andblood counts established. As a result of these tests,it may be necessary to modify or delay treatment incertain circumstances. The patient should also bemonitored regularly during chemotherapy andcytotoxic drugs withheld if there is significant dete-rioration in bone-marrow, liver or kidney function.Doses should be calculated carefully with regard toindividual variation of drug metabolism, particularlyfluorouracil and mercaptopurine. This variation canmake a considerable difference to the dosagerequirements. Many cytotoxic drugs are teratogenicand should not be administered during pregnancy,especially in the first trimester. Contraceptivemeasures are required both during therapy and forsome time afterwards. Cytotoxic drugs should beadministered in such a way as to avoid unduetoxicity to the patient or exposure during handlingby the health care provider.
Adverse effects: Cytotoxic drugs have a consider-able potential to damage normal tissue. Specificadverse effects apply, but a number of effects arecommon to all cytotoxics such as bone-marrow andimmunological suppression. Furthermore, theconcomitant use of immunosuppressive drugs willenhance susceptibility to infections. Fever associ-ated with neutropenia or immunosuppressionrequires immediate treatment with antibiotics.
Nausea and vomiting following administration ofcytotoxic drugs and abdominal radiotherapy areoften distressing and could compromise furthertreatment. Nausea and vomiting may occur within24 hours of cytotoxic treatment or later. In somecases, anticipatory nausea and vomiting occur priorto the next dose of treatment and can be managedby administering an appropriate anti-emetic.
Hyperuricaemia may complicate treatment ofconditions such as non-Hodgkin lymphoma andleukaemia. Renal damage may result from theformation of uric acid crystals. Patients should beadequately hydrated, and hyperuricaemia can bemanaged with allopurinol initiated 24 hours beforetreatment and continued for 7–10 days afterwards.Alopecia is common during treatment with cytotoxicdrugs. There is no treatment, but the condition oftenreverses spontaneously once treatment hasstopped.
Extravasation of intravenously administered cyto-toxic drugs can result in severe pain and necrosisof surrounding tissue. If extravasation occurs, theaffected limb should be elevated and treated with
cold compresses until the inflammation subsides. Insevere cases, hydrocortisone cream may be ap-plied topically to the site of inflammation.
Alkylating agents are among the most widely useddrugs in cancer chemotherapy. They act by damag-ing DNA and therefore interfering with cell replica-tion. However, there are two complications. Firstly,they affect gametogenesis and may cause perma-nent male sterility; in women, the reproductivespan may be shortened by the onset of prematuremenopause. Secondly, they are associated with amarked increase in the incidence of acute non-lymphocytic leukaemia, in particular when com-bined with extensive radiation therapy.
Cyclophosphamide is one of many alkylatingagents used in cancer therapy. It has the advan-tage of requiring hepatic activation before it isfunctional: it can therefore be given orally and is nota vesicant when given intravenously. Like allalkylating agents, its major toxic effects are myelo-suppression, alopecia, nausea and vomiting. It canalso cause haemorrhagic cystitis.
Cyclophosphamide is used either as part of curativetreatment or as an adjuvant in non-Hodgkin lym-phoma, breast cancer, childhood leukaemia, andovarian cancer. It is also employed in severalpalliative regimens.
Chlormethine (mustine) is an alkylating agent whichinterferes with DNA replication and RNA transcrip-tion thereby disrupting nucleic acid function. It ispart of the MOPP regimen used in the treatment ofadvanced Hodgkin disease and malignant lympho-mas. Its toxicity causes myelosuppression, nausea,vomiting, alopecia and phlebitis.
Cytotoxic antibiotics are widely used in cancerchemotherapy. Simultaneous use of radiotherapyshould be avoided since this may result in markedlyenhanced toxicity to normal tissue.
Bleomycin is a unique antitumour antibiotic whichcauses DNA strand cleavage. However, it hasseveral antineoplastic drug toxicities: it is known tocause a dose-related pneumonitis which can befatal, and it is associated with rare acute hypersen-sitivity reactions. Cutaneous toxicity has also beenreported. Bleomycin is a component of curativeregimens for Hodgkin disease (ABVD) and testicu-lar cancer (bleomycin, etoposide and cisplatin).
Dactinomycin is also an antineoplastic antibiotic. Itsmechanism of action is not fully understood but it is
156
WHO Drug Information Vol. 12, No. 3, 1998Essential Drugs
thought to inhibit DNA-dependent RNA synthesis byintercalating with base pairs and inhibiting DNAtemplate activity. It is used primarily to treat paedi-atric cancers. Its toxicity is similar to that of doxoru-bicin, except for cardiotoxicity.
Doxorubicin is the most widely used anthracyclineantineoplastic. It is incorporated into DNA and maycause cellular damage by a variety of mechanisms,the most important of which is now thought to beinhibition of topoisomerase II. Its primary toxiceffects are myelosuppression, alopecia, nausea,vomiting, and dose-related cardiac dysfunction. It isalso a vesicant and can cause severe skin ulcera-tion with extravasation. Doxorubicin is used foracute leukaemias although other anthracyclines aremore commonly used in these circumstances.Doxorubicin also plays a palliative role in the treat-ment of other malignancies.
Antimetabolites are incorporated into new nuclearmaterial or combine irreversibly with vital cellularenzymes, thereby preventing normal cell division.
Cytarabine inhibits DNA metabolism by severalmechanisms. Its effects are highly dependent uponthe schedule of administration. It can cause myelo-suppression, mucositis and, in high doses, centralneurotoxicity. Its almost exclusive role is in thetreatment of acute leukaemia, primarily in adults.
Fluorouracil is an antimetabolite which affects DNAand RNA metabolism. In addition, its site of actionappears to be modified by the administration ofother drugs, such as folinic acid, and by the methodof administration, whether by bolus injection or bycontinuous infusion.
Fluorouracil causes myelosuppression but onlyminimal nausea and vomiting. When its action ismodified by other drugs, its toxicity profile canchange and mucositis and diarrhoea becomeimportant problems. Central neurotoxicity can alsooccur. Fluorouracil is primarily used in the adjuvanttreatment of colorectal and breast cancer. It is alsoemployed in the palliative treatment of other malig-nancies.
Mercaptopurine is an antimetabolite whose mecha-nism of action is unclear. It can be administeredorally and myelosuppression and nausea are theonly important toxic effects. It is frequently used inthe therapy of childhood leukaemia.
Another antimetabolite, methotrexate, acts byinterfering with folic acid metabolism. Like fluorour-
acil it is myelotoxic, but nausea and vomiting areminimal. It also causes mucositis. Renal impairmentreduces methotrexate excretion and can exacer-bate toxicity. Methotrexate has been used for manyyears to treat a variety of malignancies and was thefirst cytotoxic to cure a solid tumour (choriocarci-noma). Currently, it plays a major role as an adju-vant for the therapy of breast cancer.
Calcium folinate is used to counteract the folateantagonist action of methotrexate and thus speedrecovery from methotrexate-induced mucositis ormyelosuppression. Calcium folinate also interactswith fluorouracil and an enhanced effect has beendemonstrated when the two are used together formetastatic colonic cancer.
The vinca alkaloids, vinblastine and vincristine,are primarily used in the treatment of haematologicmalignancies, although vinblastine is a componentof some regimens used for solid tumours, and theyact by disrupting the mitotic spindle. They cancause neurotoxicity, although this is much more ofa clinical problem with vincristine. Myelosuppres-sion is more common with vinblastine.
Vincristine is part of the CHOP (cyclophosphamide,doxorubicin, vincristine, and prednisolone) regimenused in the management of non-Hodgkin lym-phoma. It is also employed in the therapy of acutechildhood lymphocytic leukaemia. The most impor-tant use of vinblastine is as one of the agents in theABVD (doxorubicin, bleomycin, vinblastine, dacar-bazine) regimen for Hodgkin disease.
Etoposide is one of the two epipodophyllotoxinsused in cancer therapy. It is thought to inhibittopoisomerase II. Like other antineoplastics, itcauses myelosuppression and alopecia, and it cancause hypotension during infusion. It does notproduce significant nausea and vomiting. Etoposideis an important component of the curative therapyof testicular carcinoma and is used in severalregimens for non-small-cell and small-cell lungcancers.
The only enzyme used in cancer therapy, asparagi-nase depletes cellular stores of asparagine thusdisrupting protein synthesis. Its toxicity profile isbroad and the drug must be carefully administered.It is an important component in the management ofchildhood leukaemia, but is not used in any othermalignancy.
A simple metal-containing compound, cisplatin, isthought to act by covalent binding to DNA. It is only
157
WHO Drug Information Vol. 12, No. 3, 1998 Essential Drugs
mildly myelosuppressive and produces slight alo-pecia. However, it causes severe, dose-relatednausea and vomiting. It is also nephrotoxic andneurotoxic. Nephrotoxicity can be reduced bymaintaining high urine output during cisplatin ad-ministration and immediately afterwards, but neuro-toxicity is often dose-limiting. Cisplatin is of primaryimportance in the treatment of ovarian and testicu-lar malignancies. It is also a component of regi-mens used in non-small-cell and small-cell lungcancer and plays a palliative role in other malignan-cies.
Dacarbazine is a unique agent which, althoughdeveloped as an antimetabolite, is thought to act asan alkylating agent. Its major toxic effects aremyelosuppression, nausea and vomiting. It is aprimary component of the ABVD regimen for Hodg-kin disease. It is also used in the�palliative therapyof malignant melanoma.
Levamisole is an anthelminthic with immunostimu-lating properties. In doses used in humans, itsmajor toxic effects are a variety of CNS symptoms,nausea, and dermatitis. It is used in combinationwith fluorouracil as adjuvant therapy for colorectalcancer. Its mode of action in that combination isunknown.
Procarbazine is thought to inhibit protein, DNA andRNA synthesis. It is used in the treatment of ad-vanced Hodgkin disease. It is often used in combi-nation with chlormethamine, vincristine and pred-nisolone (MOPP regimen). Toxic effects includemyelosuppression, nausea, vomiting, CNS symp-toms and depression. Procarbazine possesses aweak monoamine oxidase inhibitory effect.
ASPARAGINASEPowder for injection: 10 000 IU in vial
Uses: Acute lymphocytic leukaemia.
Contraindications: Hypersensitivity. History ofpancreatitis.
Precautions: Because of the possibility of hyper-sensitivity reactions, resuscitation equipment andtreatment should be readily available. Hepatic,renal and pancreatic function, blood counts, andblood glucose concentration should be determinedbefore, and periodically after, therapy.
Adverse effects: Allergic reactions are sometimessevere and include elevation of liver enzymes,
hypofibrinogenaemia, leukopenia, prerenal azotae-mia with increased calcium and phosphorus excre-tion. Rarely, transient proteinuria, acute renal failureand fatal renal insufficiency have occurred. Impair-ment of pancreatic function, fatal acute haemor-rhagic hepatitis, hyperosmolar, non-ketotic hyper-glycaemia with glycosuria and polyuria which maybe reversible upon withdrawal, have also beenreported. CNS effects include EEG changes, de-pression, hyperexcitability, somnolence, lethargy,fatigue, convulsions, hallucinations and, rarely,Parkinson-like syndrome, or acute organic brainsyndrome similar to acute alcoholic delirium tre-mens. Nausea, vomiting, abdominal cramps, ano-rexia, diarrhoea, stomatitis, intestinal ulcers andfatal hyperthermia have also been reported.
BLEOMYCINPowder for injection: 15 IU (sulfate) in vial
Uses: As an adjunct to surgery and radiationtherapy in the palliative treatment of Hodgkin andnon-Hodgkin lymphomas including reticulum cellsarcoma and lymphosarcoma, carcinomas ofthe head, neck, larynx, cervix, penis, skin, vulva,testicles and including embryonal cell carcinoma,choriocarcinoma and teratocarcinoma
Contraindications: Hypersensitivity.
Precautions: Patients should be monitored and ifsigns of pulmonary toxicity appear the drug shouldbe withdrawn. Auscultation of the lungs and a chestX-ray are recommended before and at periodicintervals during therapy.
Adverse effects: Pneumonitis may progress topulmonary fibrosis, especially at cumulative dosesgreater than 300 units and in the elderly. Mucositis,including stomatitis and dermatological effects,hypaesthesia followed by hyperaesthesia, urticaria,ichthyosis, or rashes frequently occur. Myocardialinfarction, thrombotic microangiopathy or cerebralarteritis, Raynaud syndrome, fever and chillsfollowing injection, thrombocytopenia, leukopenia,slight haemoglobinaemia, nausea, vomiting, fa-tigue, hypotension and phlebitis are rarely reported.Early hypersensitivity reactions may also occur.
CALCIUM FOLINATETablet: 15 mgInjection: 3 mg/ml in 10-ml ampoule
Uses: Used routinely in high-dose methotrexatetherapy, it is usually given 24 hours after metho-
158
WHO Drug Information Vol. 12, No. 3, 1998Essential Drugs
trexate. It is also used to treat inadvertent over-dosage of methotrexate, in which case it must begiven immediately. It is also used as an adjunct inchemotherapeutic programmes for the manage-ment of several forms of cancer and in combinationwith fluorouracil in the palliative treatment of ad-vanced colorectal cancer.
Contraindications: Hypersensitivity.
Precautions: Care should be taken in detectingpernicious anaemia or other megaloblastic anae-mias due to vitamin B12 deficiency. Calcium folinatecombined with fluorouracil should only be adminis-tered under specialist supervision since calciumfolinate enhances fluorouracil’s toxicity; elderly ordebilitated patients are particularly at risk.
Adverse effects: Rarely, allergic reactions, andpossibility of seizures after parenteral administra-tion.
CHLORMETHINEPowder for injection: 10 mg(hydrochloride) in vial
Uses: Palliative treatment of Hodgkin disease(Stages III and IV) and some non-Hodgkin lympho-mas including lymphosarcoma, chronic myelocyticor chronic lymphocytic leukaemia, polycythaemiavera, mycosis fungoides, and bronchiogenic carci-noma, especially epidermoid, and small-cell carci-nomas, malignant effusions of the pericardium, theperitoneum or the pleura.
Contraindications: Hypersensitivity. Presence ofinfectious diseases.
Precautions: Should be used with great caution inpatients with tumour cell infiltration of bone-marrow.Haematological status should be monitored. Do notadminister when leukocyte count is less than 1000/mm3 or the platelet count is less than 50 000/mm3.Patients should be told to report promptly any signsof sore throat, fever, unusual bleeding or bruising.
Adverse effects: Nausea, severe vomiting, diar-rhoea, and anorexia can occur commonly. Irregularmenstruation, precipitation of herpes zoster, myelo-suppression resulting in increased�susceptibility toinfections, thrombocytopenia, and ototoxicity (athigh doses) have frequently been reported includ-ing hyperuricaemia, thrombosis, thrombophlebitis orextravasation, and alopecia. Allergic reactions,peripheral neuritis, hepatotoxicity, and peptic ulceroccur rarely.
CISPLATINPowder for injection: 10 mg, 50 mg in vial
Uses: Treatment of metastatic testicular tumours,metastatic ovarian tumours, advanced bladdercarcinoma and other neoplasms.
Contraindications: Hypersensitivity; renal or hear-ing impairment; myelosuppression.
Precautions: Administer only under specialistsupervision, monitor blood counts, liver functionand renal function weekly and perform neurologicalexamination regularly. Hydrate.
Adverse effects: Commonly, nausea, vomitingand nephrotoxicity occur for which mandatoryhydration should be given before initiating treat-ment. Myelosuppression, ototoxicity, neurotoxicityand other toxicities may be severe enough tonecessitate dosage reduction or withdrawal. Serumelectrolyte disturbances include hypomagnesaemia,hypocalcaemia, hyponatraemia, hypokalaemia,hypophosphataemia. Ocular toxicity and anaphylac-tic reactions, liver enzyme concentration elevations,cardiac abnormalities, anorexia, and alopecia havealso been reported.
CYCLOPHOSPHAMIDETablet: 25 mgPowder for injection: 500 mg in vial
Uses: Used alone, concurrently or sequentially withother antineoplastic drugs in the treatment of malig-nant lymphomas, Hodgkin disease, lymphocyticlymphoma, Burkitt lymphoma, multiple myeloma,leukaemias, mycosis fungoides, neuroblastoma,adenocarcinoma of the ovary, retinoblastoma, andcarcinoma of the breast.
Contraindications: Hypersensitivity; severe bone-marrow depression.
Precautions: Only to be administered underspecialist supervision. Monitor the full blood countand if myelosuppression occurs, withdraw until theblood and platelet count return to normal. Cautionis needed in patients with leukopenia, thrombocyto-penia, tumour cell infiltration of bone-marrow,previous X-ray therapy, previous treatment withother anti-neoplastic drugs, impaired renal orhepatic function. Extreme care required with inva-sive procedures in patients who develop thrombo-cytopenia during treatment.
159
WHO Drug Information Vol. 12, No. 3, 1998 Essential Drugs
Adverse effects: Potentially serious haemor-rhagic cystitis can occur rarely. Adequate hydrationis mandatory prior to, and for at least 72 hours afteradministration. Discontinue if haemorrhagic cystitisoccurs. Reversible myelosuppression, nausea,vomiting, and anorexia commonly occur. Alopecia,interstitial pulmonary fibrosis (during prolongedtreatment with high doses), metabolic effects in-clude hyperuricaemia, cardiotoxicity (which may befatal), headache, dizziness, myxoedema, anddelayed wound healing frequently occur. Occasion-ally, diarrhoea, haemorrhagic colitis, stomatitis and,rarely, hepatotoxicity and anaphylactic reactionshave been reported.
CYTARABINEPowder for injection: 100 mg in vial
Uses: Treatment of acute lymphocytic leukaemia,acute or chronic myelocytic leukaemia, prophylaxisand treatment of meningeal leukaemia, erythro-leukaemia, and non-Hodgkin lymphoma.
Contraindications: Hypersensitivity.
Precautions: Take frequent platelet and bloodcounts, and bone-marrow examination. Shouldbe used with caution in patients with drug-inducedbone-marrow depression.
Adverse effects: Dose-related myelosuppression,anaemia, leukopenia, thrombocytopenia, megalo-blastosis, reduced reticulocytopenia, increasedsusceptibility to infections, and anaphylactic-likereactions may occur. Nausea and vomiting whichmay follow rapid intravenous injection, anorexia,mucositis, stomatitis, hepatotoxicity, thrombophlebi-tis, and haemorrhagic complications have beenfrequently reported and, less frequently, abdominalpain, urinary retention, renal dysfunction, neuraltoxicity, allergic skin reactions, and alopecia.
DACARBAZINEPowder for injection: 100 mg in vial
Uses: Treatment of metastatic malignant mela-noma, and as first-line therapy for Hodgkin diseasein combination with other antineoplastic agents.
Contraindications: Hypersensitivity.
Precautions: Hospitalization is not always neces-sary, but adequate facilities are required for moni-toring of full blood count and for bone-marrowexamination.
Adverse effects: Withdraw the drug if severemyelosuppression occurs. This may result in throm-bocytopenia and leukopenia which may be fatal.Frequently, nausea, vomiting and anorexia havebeen reported. Hepatotoxicity with hepatic veinthrombosis and hepatocellular necrosis, diarrhoea,influenza-like syndrome with fever, malaise andmyalgia, alopecia, facial flushing, facial paraesthe-sia, erythematous and urticarial rashes, and photo-sensitivity may rarely occur.
DACTINOMYCINPowder for injection: 500 µg in vial
Use: In combination with other antineoplasticagents for the treatment of endometrial carcinoma,trophoblastic tumours, testicular carcinoma, Wilmtumour, Ewing sarcoma, rhabdomyosarcoma.
Contraindications: Hypersensitivity, herpes zosteror chickenpox.
Precautions: Periodic monitoring of hepatic func-tion.
Adverse effects: Amenorrhoea, breakthroughbleeding, irregular menstruation, and weight gainfrequently occur. Dose-related oedema, musclecramps and spasms, virilism, bladder telangiecta-sia, thrombocytopenia, bleeding gums and hepaticdysfunction have been reported less frequently.
DOXORUBICINPowder for injection: 10 mg, 50 mg(hydrochloride) in vial
Uses: Treatment of acute lymphocytic and myelo-cytic leukaemias, treatment of carcinomas of thebreast, bladder, ovary and thyroid, neuroblastoma,Wilm tumour, non-Hodgkin and Hodgkinlymphomas, soft tissue sarcomas, osteosarcoma.
Contraindications: Hypersensitivity. Previoustreatment with full cumulative doses of doxorubicin,daunorubicin, or other anthracyclines and anthra-cenes, myelosuppression induced by drug orradiation therapy.
Precautions: The probability of cardiomyopathyincreases if the cumulative dose exceeds450 mg/m2 body surface area. Use with caution inpatients with previous cardiac disease or those whohave received previous myocardial radiationtherapy. Cardiac monitoring may be necessary anda blood count is required before initiation of
160
WHO Drug Information Vol. 12, No. 3, 1998Essential Drugs
therapy, and weekly thereafter. May cause severetissue necrosis if extravasation occurs. Reducedosage in patients with renal or hepatic impairment.
Adverse effects: Dose-limiting myelosuppressionand cardiomyopathy may occur and, frequently,nausea, severe vomiting, mucositis including sto-matitis and oesophagitis, ulceration and necrosis ofthe colon resulting in bleeding or acute infectionswhich may be fatal (especially in non-lymphocyticleukaemia), complete but reversible alopecia,hyperpigmentation of nail-beds and dermalcreases, and sometimes onycholysis. Rarely,secondary acute myeloid leukaemia with or withoutpreleukaemic phase, hypersensitivity reactionswhich include fever, chills and urticaria, facialflushing on rapid i.v. injection have been reported.
ETOPOSIDECapsule: 100 mgInjection: 20 mg/ml in 5-ml ampoule
Uses: In combination with other antineoplasticagents for treatment of refractory testiculartumours in patients who have received appropriatesurgical, chemotherapeutic and radiationtherapy. In combination with other agents for treat-ment of small-cell lung carcinoma.
Contraindications: Hypersensitivity.
Precautions: Close monitoring for possible hypo-tensive or anaphylactoid reactions. Resuscitationfacilities should be readily available. Full bloodcounts should be taken before and at weekly inter-vals during therapy.
Adverse effects: Dose-related and dose-limitingmyelosuppression, nausea, vomiting, transienthypotension following intravenous administration,anaphylactoid reactions including chills, fever,bronchospasm and dyspnoea may occur. Infre-quently, rashes, fever, pruritus, abdominal pain,constipation, dysphagia, and transient cornealblindness have been reported.
FLUOROURACILInjection: 50 mg/ml in 5-ml ampoule
Uses: Carcinomas of the colorectum, breast,stomach, pancreas, bladder, cervix, prostate, ovaryand endometrium, liver tumours, head and necktumours.
Contraindications: Hypersensitivity, poor nutri-tional status, severe bone-marrow depression,potentially serious infections.
Precautions: Should be used with caution in renalor hepatic impairment.
Adverse effects: Commonly, nausea, vomiting,stomatitis, diarrhoea, anorexia, leukopenia, alo-pecia, dermatitis, and acute cerebellar syndromewhich may persist after discontinuation, may occur.
LEVAMISOLETablet: 50 mg (as hydrochloride)
Uses: In combination with fluorouracil for thetreatment of colorectal carcinoma after completeresection of primary tumour with little or no evi-dence of local or distant metastases.
Contraindications: Hypersensitivity.
Precautions: Haematological monitoring essentialbecause of the risk of agranulocytosis which maybe fatal. Patients should be instructed to report anysigns of fever, chills or unusual discomfort or weak-ness.
Adverse effects: When used as a single agent,effects are usually mild; however, when combinedwith fluorouracil, haematological and gastrointesti-nal effects may frequently occur. Less frequently,blood dyscrasias including agranulocytosis, leuko-penia or thrombocytopenia, mild stomatitis are alsoreported. CNS toxicity (including ataxia, confusion,and paranoia, seizures, tardive dyskinesia), exfolia-tive dermatitis, periorbital oedema, hallucinations,elevation of serum creatinine and alkaline phos-phatase may rarely occur.
MERCAPTOPURINETablet: 50 mg
Uses: Treatment of acute lymphocytic, acutemyelocytic and acute myelomonocytic leukaemias.
Contraindications: Hypersensitivity.
Precautions: Weekly blood count and hepaticfunction monitoring necessary.
Adverse effects: Potentially serious myelosup-pression frequently occurs leading to leukopenia,thrombocytopenia and anaemia which can be life-threatening, hepatotoxicity or biliary stasis. Less
161
WHO Drug Information Vol. 12, No. 3, 1998 Essential Drugs
frequently, hyperuricaemia, nausea, vomiting andanorexia, gastrointestinal ulceration, and stomatitisare reported.
METHOTREXATETablet: 2.5 mg (as sodium salt)Powder for injection: 50 mg (as sodium salt)in vial
Uses: Carcinoma of the breast, head, neck, andlung. Trophoblastic tumours, acute lymphocyticleukaemia. Prophylaxis and treatment of meningealleukaemia, treatment of non-Hodgkin diseaseincluding advanced cases of lymphosarcoma, andadvanced cases of mycosis fungoides. In combina-tion with other antineoplastic agents, for treatmentof non-metastatic osteosarcoma in patients whohave undergone primary surgical treatment.
Contraindications: Severe renal or hepatic impair-ment, pregnancy, breast-feeding.
Precautions: Complete haematological analysisshould be undertaken before treatment is initiatedincluding renal and hepatic function tests, followedby weekly monitoring throughout. Use with extremecaution in cases of peptic ulceration, ulcerativecolitis and diarrhoea. Withdraw if stomatitis occurssince this may be the first sign of gastrointestinaltoxicity.
Adverse effects: Pulmonary toxicity, photosensi-tivity, hepatic toxicity, haematological toxicity, andgastrointestinal toxicity have been reported.
Drug interactions: Concurrent administration ofacetylsalicylic acid or NSAID may reduce excretionof methotrexate and increase its toxicity. Patientsshould be advised not to use over-the-counterpreparations without consulting the physician incharge of palliative treatment.
PROCARBAZINECapsule: 50 mg (as hydrochloride)
Uses: As part of MOPP chemotherapy in Hodgkindisease, and non-Hodgkin lymphoma.
Contraindications: Hypersensitivity, severe bone-marrow depression.
Precautions: The patient should be hospitalized forinitiation of treatment. Periodic determination ofblood counts is necessary. Alcohol may causedisulfiram-like reaction.
Adverse effects: Myelosuppression, nausea andvomiting, anorexia, abdominal pain, stomatitis, anddryness of mouth may commonly occur. Othereffects include paraesthesia, neuropathy, depres-sion, psychosis, hallucination, myalgia and arthral-gia, lethargy, dermatitis, rash, pruritus and infec-tions.
VINBLASTINEPowder for injection: 10 mg (sulfate) in vial
Uses: Alone or in combination with other antineo-plastic agents as a palliative during treatment ofdisseminated Hodgkin (stage III and IV) and non-Hodgkin lymphoma. It may also be used in combi-nation with other agents for treatment of advancedtesticular carcinoma, breast carcinoma unrespon-sive to endocrine surgery or hormonal therapy, andalone or in combination as a palliative agent forKaposi sarcoma, trophoblastic tumours, Letterer-Siwe disease, or mycosis fungoides.
Contraindications: Hypersensitivity, drug-inducedgranulocytopenia, severe infection.
Precautions: Avoid contact with eyes as vinblast-ine may cause severe irritation or corneal ulcera-tion. Patients should be advised to report signs offever, sore throat, unusual bleeding or bruisingbecause the risks of myelosuppression may befatal. Use with caution in debilitated or elderlypatients.
Adverse effects: Myelosuppression may occurfrequently. Infections, nausea, vomiting, hyperuri-caemia or uric acid nephropathy, stomatitis, tran-sient thrombocytopenia, extravasation have beenreported. Rarely, haemorrhagic colitis, bleedingfrom previous peptic ulcers, and neurotoxicity mayoccur.
VINCRISTINEPowder for injection: 1 mg, 5 mg(sulfate) in vial
Uses: Acute lymphocytic lymphoma, neuroblas-toma, Wilm tumour, Hodgkin and non-Hodgkinlymphomas, rhabdomyosarcoma, Ewing sarcoma.
Contraindications: Hypersensitivity.
Precautions: Use with caution in patients with pre-existing neuromuscular disorder or those receivingother neurotoxic drugs, avoid contact with eyes, asit may cause severe irritation or corneal ulceration.
162
WHO Drug Information Vol. 12, No. 3, 1998Essential Drugs
Adverse effects: Neurotoxicity (as peripheralneuropathy), constipation, abdominal cramps, andalopecia which is reversible on cessation of therapyoccur commonly. Less frequently,�hyponatraemiaas a syndrome of inappropriate ADH secretion,extravasation, allergic reactions such as anaphy-laxis, rash and oedema, hypertension, hypotension,stomatitis, intestinal necrosis and perforation havebeen reported.
Hormones and antihormonesDiethylstilboestrol (DES) is a synthetic estrogen. Itis used to manipulate the hormonal environment inpatients with tumours of hormonally sensitiveorgans (breast and testes). It has little toxicity inwomen, but in men it causes gynaecomastia and,more importantly, increases the risk of cardiovascu-lar disease. The use of DES and other estrogens inbreast cancer has largely been supplanted bytamoxifen. However, it can be employed to sup-press androgen production in patients with prostatecancer, and can play an important palliative andpossibly adjuvant role.
The corticosteroids prednisolone, dexamethasone,and hydrocortisone are synthetic hormones given atpharmacological doses, particularly for haemato-logical malignancies. Their precise mechanism ofaction is not known, but they appear to be cytolytic,at least in lymphoid diseases. Although there is noevidence of therapeutic superiority, prednisolone isa commonly used component of antineoplastic re-gimens. However, chronic use leads to the toxicityassociated with Cushing syndrome. Toxicity ofcorticosteroids is generally experienced as insom-nia, and as hyperglycaemia in diabetics. Predniso-lone is an important component of curative regi-mens for lymphomas and childhood leukaemias,and elsewhere it has a palliative role.
Tamoxifen antagonizes the effects of estrogendespite its estrogenic properties. When given atrecommended doses, it has few adverse effects,although it can induce uterine malignancies. Itsmajor role in cancer therapy is use after surgeryand for palliative management in patients withbreast cancer.
PREDNISOLONETablet: 5 mgPowder for injection: 20 mg, 25 mg, (assodium phosphate or sodium succinate) in vial
Uses: In combination with antineoplastic agents, forthe palliative treatment of acute or chronic lym-
phocytic leukaemia, Hodgkin and non-Hodgkinlymphoma.
Dosage:Adults: 60–100 mg daily or even higher for the firstfew days, with gradual reduction to 20–40 mg daily.
Children: 0.5 mg/kg or 15 mg/m2 four times daily for2–3 weeks, followed by 0.375 mg/kg or 11.25 mg/m2 four times daily for 4–6 weeks.
Contraindications: Known hypersensitivity to anycorticosteroid. Active bacterial, viral or fungalinfection. Unless the benefits outweigh the risks,systemic administration of corticosteroids is con-traindicated in patients with peptic ulcer, osteoporo-sis, psychoses or severe psychoneuroses, conges-tive heart failure, hypertension, diabetes mellitus,epilepsy, glaucoma, ocular herpes simplex, chronicrenal failure or uraemia.
Precautions: Monitor body weight, blood pressure,fluid and electrolyte balance, and blood glucoseconcentrations throughout treatment. The responseto the pituitary-adrenal axis is reduced and mayremain depressed for many months after with-drawal of the drug. If an infection occurs during thisperiod, prednisolone therapy may need to bereinstituted temporarily.
Children on corticosteroid therapy should be treatedwith immunoglobulin if they are exposed to a child-hood viral infection to which they have no acquiredimmunity. They should not receive live-virus vac-cines. To reduce the risk of stunted growth, inter-mittent dosage regimens should be used for chil-dren when therapy is prolonged for more than 6months.
Adverse effects: Infections contracted duringtherapy can be fatal in the absence of effectivetreatment. Quiescent tuberculosis may be reacti-vated.
Long-term treatment at doses of approximately10 mg daily may result in stunting of growth inchildren — which may be averted by giving cortico-trophin and selected alternate-day dosage sched-ules. Effects include hypercorticalism, moon face,acne, bruising, abdominal striae, truncal obesity,muscle-wasting, hypertension, and amenorrhoeaand hirsutism in females, spinal osteoporosis andvertebral collapse (which may be retarded by givingcalcium supplements and small doses of vitaminD), aseptic osteonecrosis, particularly of the femo-
163
WHO Drug Information Vol. 12, No. 3, 1998 Essential Drugs
ral head, subcapsular cataracts and glaucoma,development or aggravation of peptic ulcers, diabe-tes mellitus, depression and psychosis, with risk ofsuicide, raised intracranial pressure and convul-sions, particularly in children, increased coagulabil-ity of blood, delayed tissue healing, myopathycharacterized by weakness of the proximal muscu-lature of arms and legs.
TAMOXIFENTablet: 10 mg, 20 mg (as citrate)
Uses: As adjuvant treatment of axillary node-negative breast cancer in women or axillary node-positive breast cancer in postmenopausal womenfollowing total or segmental mastectomy. Axillarydissection, and breast irradiation, and treatment ofmetastatic breast cancer in men and women.
Dosage:Node-negative and node-positive breast cancerin women10 mg twice daily.Metastatic breast cancer in men and women10 or 20 mg twice daily.
Contraindications: Hypersensitivity.
Precautions: Should be used with caution inpatients with severe bone-marrow depression.Periodic blood counts, including platelet counts, arenecessary, as well as a periodic liver function test inthe rare event of lipoprotein abnormalities. Serumtriglycerides and lipoproteins should be monitoredin patients with preexisting hyperlipoproteinuria.Ophthalmological examination may be necessary todetect ocular toxicity.
Adverse effects: Hot flushes, nausea and vomitingfrequently occur in women and the dosage shouldbe reduced if severe. Vaginal bleeding, vaginaldischarge, menstrual irregularities, exacerbation ofbone pain in patients with bone metastases mayoccur less frequently. Changes in liver enzymelevels and cholestasis, hepatitis and hepatic necro-sis, thromboembolic events, thrombocytopeniahypercalcaemia, dysgeusia, oedema, depression,dizziness, hair thinning or partial alopecia, vaginaldryness, uterine fibroids, risk of endometrial cancer,visual disturbances including corneal changes,cataracts and retinopathy have rarely been re-ported.
Drugs used in palliative carePalliative care for cancer patients includes bothpain relief and the symptomatic relief of dyspnoea,restlessness, confusion, anorexia, constipation,pruritus, nausea, vomiting and insomnia.
Pain relief can be achieved by treatment with drugsor anaesthetics and neurosurgical, psychologicaland behavioural approaches geared to individualpatient needs. If carried out correctly, most patientswith cancer pain can obtain effective relief. Pain isbest treated with a combination of drug and non-drug measures. Analgesics and other drugs consti-tuting the basis of cancer pain management aredescribed in the WHO publication Cancer PainRelief (1).
Anticancer therapy and drugs for cancer pain canbe given concurrently. Some types of pain respondwell to a combination of non-opioid and opioidtreatment. With others, relief is obtained by combin-ing a corticosteroid and an opioid. Neuropathicpains often show little response to non-opioids andopioid analgesics, but may be eased by tricyclicantidepressants and anticonvulsants.
Recognizing when neuropathic pain is resistant toopioids is important for optimal drug treatment.Cancer patients often have many fears and anxie-ties, and may become depressed. Very anxious ordeeply depressed patients may need an appropri-ate psychotropic drug in addition to an analgesic. Ifthis fact is not appreciated, the pain may remainintractable.
In the majority of patients, cancer pain can berelieved with analgesics. If possible, these shouldbe given orally. Rectal suppositories are useful inpatients with dysphagia, uncontrolled vomiting orgastrointestinal obstruction. Continuous subcutane-ous infusion offers an alternative.
Timing: An analgesic should be given at fixed timeintervals and titrated against the degree of pain. Inthis way, the next dose can be given before theeffect of the previous one has fully worn off.
The first and last doses of the day should be linkedto the patient's waking time and bedtime. Ideally,the drug regimen should be written clearly for thepatient and the care provider to follow. The patientshould be warned in advance about possible ad-verse effects.
164
WHO Drug Information Vol. 12, No. 3, 1998
Using the WHO analgesic ladder concept. The firststep will be to give a non-opioid analgesic such asacetylsalicylic acid, paracetamol or ibuprofen and, ifnecessary, an adjuvant drug. If this does not relievethe pain, an opioid for mild to moderate pain suchas codeine should be added. When this combina-tion fails to relieve pain, an opioid for moderate tosevere pain such as morphine should be substi-tuted.
Individually tailored: There are no standard dosesfor opioid drugs. The range for oral morphine isfrom as little as 5 mg to more than 1000 mg every 4hours.
Drugs for neuropathic pain: Patients with neuro-pathic pain may derive benefit from opioids with orwithout a corticosteroid, particularly in the case ofnerve compression. Alternatively, neuropathic painoften responds to a tricyclic antidepressant, such asamitriptyline, an anticonvulsant such as carbamaze-
pine or a local anaesthetic such as intravenouslidocaine.
Adjuvant therapy may be necessary for any one ofthree reasons:
• to treat the adverse effects of the analgesics, e.g.antiemetics such as metoclopramide and laxa-tives.
• to support other pain relief methods, e.g. a corti-costeroid such as prednisolone in nerve compres-sion pain.
• to treat concomitant psychological disturbancessuch as insomnia, anxiety and depression.
Reference:
1. Cancer Pain Relief with a Guide to Opioid Availability.Second edition. World Health Organization, Geneva,1996. ISBN 92 4 154482 1
Essential Drugs
165
WHO Drug Information Vol. 12, No. 3, 1998
Recent Publications and Documents
Guidance for industry: activepharmaceutical ingredientsThis document focuses on the manufacture ofactive pharmaceutical ingredients (APIs) and willprovide guidance to industry on basic requirementsexpected when filing for or renewing new drugapplications within the United States of America. Itmay also prove useful for the manufacture of excipi-ents.
For the moment, the document is circulated as adraft for comments and is not meant for implemen-tation. However, it will give a good indication of therequirements desired in the manufacture andcontrol of APIs for drugs and biologicals, includingchemical isolation and purification steps used forbiological or fermentation processes and sterileAPIs. It does not apply to medical gases, bulkpackaged drug products in final dosage form, andradiopharmaceuticals.
Good manufacturing practices apply to all steps ofthe API manufacturing process, including the use ofstarting materials. Such practices include thevalidation of processes determined to affect thequality and purity of the active pharmaceuticalingredient.
Draft guidance for industry: manufacturing, processing orholding active pharmaceutical ingredients. Available from:Center for Biologics Evaluation and Research, Food andDrug Administration, 1401 Rockville Pike, Rockville MD20852, USA or through http://www.fda.gov/cber.
Guidance for industry: humanplasma-derived biological productsThe Food and Drug Administration has announcedthe availability of a draft guidance for industry forthe establishment of descriptive information forhuman plasma-derived biologicals or animalplasma or serum-derived products. The guidance isintended to assist applicants in the preparation ofthe descriptive section of a licence application forsuch products. This action is intended to reduce
unnecessary burdens for industry without diminish-ing public health protection.
Draft guidance for industry for the submission of chemis-try, manufacturing and controls and establishmentdescription information for human plasma-derivedbiological products or animal plasma or serum-derivedproducts. Available from: Center for Biologics Evaluationand Research, Food and Drug Administration, 1401Rockville Pike, Rockville MD 20852, USA or through http://www.fda.gov/cber.
WHO Expert Committee onDrug DependenceThe scale of drug dependence has grown dramati-cally in the past quarter-century. Preventing de-pendence and reducing the harm associated withthe use of psychoactive substances is a challengefor health services and governments the world over.This WHO Expert Committee report categorizes thedifferent types of harm that can result frompsychoactive substances, whether illicit or legallyavailable, and describes the steps that can betaken to treat health problems and stop them fromoccurring. The report looks at the cost and effec-tiveness of various treatment methods, drawing onevidence from research findings, and gives adetailed outline of the elements needed for aneffective national treatment system. It addressesthe question of whether dependent persons shouldbe given a controlled supply of drugs and proposesfor further review several substances that havepotential for abuse. The Expert Committee's recom-mendations cover drug policies and treatmentservices, as well as training, information needs andresearch. The report lays the foundation for realisticbut sound strategies in national and internationalefforts to reduce the health damage caused by theuse of psychoactive substances.
WHO Expert Committee on Drug Dependence. Thirtiethreport. WHO Technical Report Series, No. 873, 1998.ISBN 92 4 120873 2

166
WHO Drug Information Vol. 12, No. 3, 1998
WHO Expert Committee onBiological Standardization:Forty-sixth reportThis report represents the recommendations of aWHO expert committee commissioned to coordi-nate a range of research and other activities re-quired to assure the purity, potency, safety andstability of biological products used in medicine.The report covers the development and adoption ofdetailed requirements for the manufacturing, licens-ing and control of vaccines and other biologicals.The committee also coordinates the establishmentof international biological reference materials foruse in clinical assays, pharmaceutical research andquality control.
The report is divided into three parts. The firstprovides a brief discussion of general issues thatshape the committee's work. Issues discussedinclude procedures for establishing and distributingreference materials and the rationale for issuing orrevising requirements for specific products. Thesecond part summarizes activities relating to thestatus of some 36 biological reference preparationscategorized as antibiotics, antibodies, antigens andrelated substances; blood products, cytokines,endocrinological substances and toxins.
The third and most extensive part contains detailedrevised requirements for the production and controlof yellow fever vaccine and amended generalrequirements for the sterility of biological sub-stances, modified to reflect new procedures forconducting a sterility test for mycoplasmas. Alsoincluded are a list of laboratories approved by WHOfor the production of yellow fever vaccine and asummary protocol for the routine batch release ofvirus vaccines.
WHO Expert Committee on Biological Standardization.Forty-sixth report. WHO Technical Report Series, No. 8721998. ISBN 92 4 120872 4.
Recent Publications and Documents
Use of antimicrobialsin food-producing animalsIn October 1997, the World Health Organizationconvened a meeting to examine the question ofwhether the use of antimicrobials in livestock pro-duction contributes to the escalation of antimicrobialresistance in humans. Timely public health action isneeded to control medical problems related to thewidespread application of antimicrobials outside themedical sphere. On the agenda were such issuesas the development, licensing and use of antimicro-bials in livestock production, and clinical micro-biology, resistance monitoring and medical infec-tious disease control.
The meeting reviewed antimicrobial use and theknown and potential consequences in food animalproduction. General recommendations were pro-posed for action by national control authorities andcollaboration within the medical, veterinary andagricultural sectors. It was agreed that WHO shouldtake the lead in coordinating international efforts inresistance monitoring . As a matter of urgency,microbiological laboratories capable of developingnetworks on resistance monitoring should bestrengthened. In this way, countries will be able toascertain and monitor the prevalence of resistantbacteria in food-producing animal products.
The use of antimicrobials in animals must balancethe possible benefits to livestock production againstthe medical risk and public health consequencesderiving from their use. It was emphasized thatantimicrobial agents should not be used as a sub-stitute for adequate hygiene in animal husbandry.No antimicrobial should be administered to a foodanimal unless it has been evaluated and authorizedby the national authorities, and prescription andpractice standards should be strictly applied.
The medical impact of the use of antimicrobials in foodanimals: available from the Division of Emerging andOther Communicable Diseases, Surveillance and Control.WHO, Geneva. WHO/EMC/ZOO/97.4.
International Nonproprietary Names for Pharmaceutical Substances (INN) RECOMMENDED International Nonproprietary Names (Rec. INN): List 40
Notice is hereby given that, in accordance with paragraph 7 of the Procedure for the Selection of Recommended International Nonproprietary Names for Pharmaceutical Substances [Off. Rec. Wld Health Org., 1955, 60, 3 (Resolution EB15.R7); 1969, 173, 10 (Resolution EB43 R9)], the following names are selected as Recommended International Nonproprietary Names. The inclusion of a name in the lists of Recommended International Nonproprietary Names does not imply any recommendation of the use of the substance in medicine or pharmacy. Lists of Proposed (1-73) and Recommended (1-35) International Nonproprietary Names can be found in Cumulative List No. 9, 1996.
Dénominations communes internationales des Substances pharmaceutiques (DCI)
Dénominations communes internationales RECOMMENDÉES (DCI Rec): Liste 40
Il est notifié que, conformément aux dispositions du paragraphe 7 de la Procédure à suivre en vue du choix de Dénominations communes internationales recommandées pour les Substances pharmaceutiques [Actes off. Org. mond. Santé, 1955,60,3(résolution EB15.R7); 1969,173,10 (résolution EB43.R9)] les dénominations ci-dessous sont choisises par l'Organisation mondiale de la Santé en tant que dénominations communes internationales recommandées. L'inclusion d'une dénomination dans les listes de DCI recommandées n'implique aucune recommandation en vue de l'utilisation de la substance correspondante en médecine ou en pharmacie. On trouvera d'autres listes de Dénominations communes internationales proposées (1-73) et recommandées (1—
- - 35) dans la Liste récapitulative No. 9, 1996.
Denominaciones Comunes Internacionales para las Sustancias Farmacéuticas (DCI)
Denominaciones Comunes Internacionales RECOMENDADAS (DCI Rec): Lista 40
De conformidad con lo que dispone el párrafo 7 del Procedimiento de Selección de Denominaciones Comunes Internacionales Recomendadas para las Sustancias Farmacéuticas [Act. Of. Mund. Salud, 1955, 60, 3 (Resolución EB15.R7); 1969, 173, 10 (Resolución EB43.R9)], se comunica por el presente anuncio que las denominaciones que acontinuación se expresan han sido seleccionadas como Denominaciones Comunes Internacionales Recomendadas. La inclusión de una denominación en las listas de las Denominaciones Comunes Recomendadas no supone recomendación alguna en favor del empleo de la sustancia respectiva en medicina o en farmacia. Las listas de Denominaciones Comunes Internacionales Propuestas (1-73) y Recomendadas (1-35) se encuentran reunidas en Cumulative List No. 9, 1996.
An ongoing review is under way of the long-standing objections to proposed International Nonproprietary Names (INN). As a result, objections have been withdrawn to the following names which are now included in this list of recommended INNs:
alfacalcidol, almecillin, alverine, amiflamine, anazolene sodium, calcium pantothenate, chloralose, dimepranol, elanzepine, elfazepam, esmolol, fenisorex, fibrinolysin (human), flavamine, glucosamine, iometin (131 I), iometin (125 I), leucocianidol, levocarnitine, lombazole, loprodiol, metformin, mianserin, midaflur, neocinchophen, ribavirin, ropizine, soterenol, sulmazole, thiomersal
Les objections formulées de longue date contre des Dénominations communes internationales (DCI) proposées sont examinées. Des objections ont été retirées à la suite de cet examen et les noms suivants sont donc inclus dans cette liste des DCI recommandées:
alfacalcidol, almécilline, alvérine, amiflamine, anazolene sodique, pantothénate de calcium, chloralose, dimépranol, élanzépine, elfazépam, esmolol, fénisorex, fibrinolysine (humaine), flavamine, glucosamine, iométine (131 I), iométine (125 I), leucocianidol, levocarnitine, lombazole, Ioprodiol, metformine, miansérine, midaflur, néocinchophène, ribavirine, ropizine, sotérénol, sulmazole, thiomersal
Se ha emprendido un examen de las objeciones que se vienen formulando desde hace tiempo a las denominaciones comunes internacionales (DCI) propuestas. Como resultado, se han retirado las objeciones a las denominaciones siguientes, que ahora están incluidas en la presente lista de DCI recomendadas:
alfacalcidol, almecilina, alverina, amiflamina, anazolene sódico, pantotenate de calcio, cloralosa, dimepranol, elanzepina, elfazepam, esmolol, fenisorex, fibrinolisina (humana), flavamine, glucosamina, iometina (131 l), iometina (125 l), leucocianidol, levocarnitin, lombazol, ioprodiol, metformina, mianserina, midaflur, neocincofeno, ribavirina, ropizina, soterenol, sulmazol, tiomersal
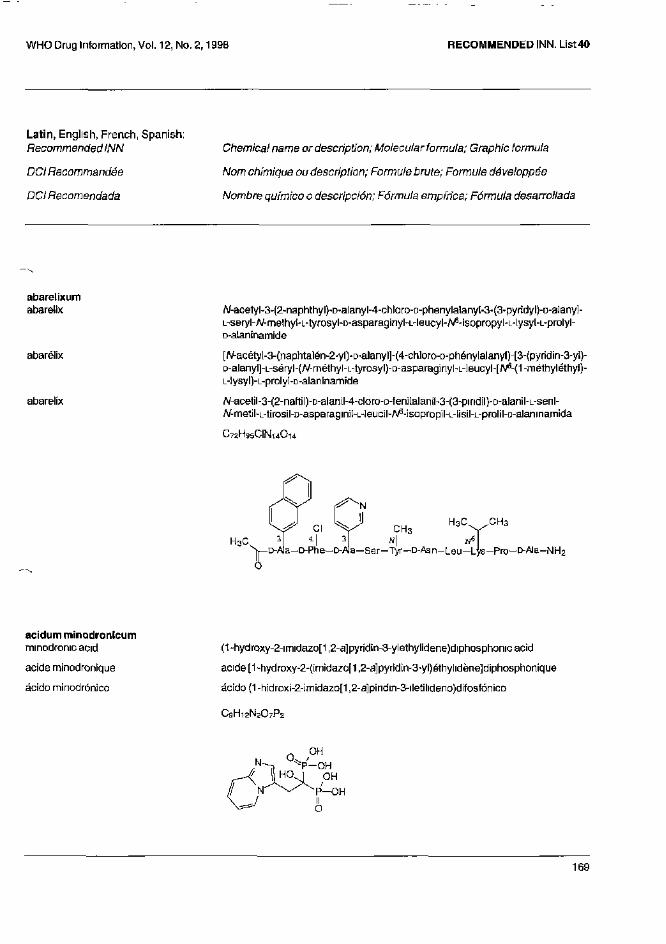
Latin, English, French, Spanish: Recommended INN
DCI Recommandée
DCI Recomendada
Chemical name or description; Molecular formula; Graphic formula
Nom chimique ou description; Formule brute; Formule développée
Nombre químico o descripción; Fórmula empírica; Fórmula desarrollada
abarelixum abarelix
abarelix
abarelix
N-acetyl-3-(2-naphthyl)-D-alanyl-4-chloro-D-phenyla]any[-3-(3-pyridyl)-D-alanyI" L-seryl-N-methyl-L-tyrosyl-D-asparaginyl-L-leucyl-^-isopropyl-L-lysyl-L-prolyl-D-alaninamide
[N-acétyl-3-(naphtalén-2-yl)-D-alanyl]-(4-chloro-D-phénylalanyl)-[3-{pyrid¡n-3-yl)-D-alanyll-L-seryl-(N-methyl-L-tyrosyO-D-asparaginyl-L-leucyl-[N6-(1-méthyléthyl)-L-lysyl)-L-prolyl-D-alaninamide
N-acetil-3-(2-naftil)-D-alanil-4-claro-D-fenilalanil-3-(3-pindil)-D-alanil-L-seril-N-metíl-L-tirosil-D-asparaginii-L-Ieucil-A^-isopropil-L-tisil-L-prolil-D-alaninamida
C72H95CIN14O14
acidum minodronicum
minodronic acid
acide minodronique
ácido minodrónico
(1-hydroxy-2-imidazo[1,2-a]pyridín-3-ylethylidene)diphosphonicac¡d
acide [1-hydroxy-2-{imidazo[1,2-a]pyridin-3-yl)éthylidène]diphosphonique
ácido (1 -hidroxi-2-imídazo[1,2-a]p¡ridin-3-iletilideno)difosfón¡co
C9H12N2O7P2
alfacalcidolum
alfacalcidol
alfacalcidol
alfacalcidol
(5Z,7E)-9,10-secocholesta-5,7,10(19)-triene-1 a,3p-diol
(5Z,7E)-(1R,3R)-9,10-sécocholesta-5,7,10(19)triène-1,3-diol
(5Z,7E)-9,10-secocolesta-5,7,10(19}-trieno-1a,33-diol
C27H44O2
almecillinum almecillin
almécilline
almecilina
[(allylthio)methyl]penicillin
acide (2S,5R,6R)-3,3-diméthyl-7-oxo-6-[[2-[(prop-2-ényl)sulfanyl]acétyl] amino]-4-thia-1-azabicyclo[3.2.0]heptane-2-carboxylique
[(aliltio)metiJJpenicilina
C1 3H1 6N2O4S2
alverinum
alverine
alvérine
alverina
N-ethyl-3,3'-diphenyldipropylamine
N-éthyl-3-phényl-N-(3-phénylpropyl)propan-1-amine
N-etíl-3,3'-difenildipropilamina
C20H27N
amiflaminum
amiflamine
amiflamine
amiflamina
(+)-4-(dimethylamino)-α,2-dimethylphenethylamine
(2S)-1-[4-(diméthylamino)-2-méthyIphényl]propan-2-amine
(+)-4-(dimetiIamino)-α,2-dimetilfenetilarn¡na
C12H20N2
anazolenum natricum
anazolene sodium
anazolène sodique
anazoleno sódico
4-[(4-amilino-5-su[fo-1-naphthyl)azo]-5-hydroxy-2,7-naphthaIenedisulfonic acid, trisodium salt
4-hydroxy-5-[[4-(phénylamino)-5-sulfonatonaphtalén-1-yl]diazényl]naphtalène-2,7-disulfonate de trisodium
sal trisódica del ácido 4-[(4-anilino-5-sulfo-l-naftil)azo]-5-hidroxi-2,7-naftalenodisulfónico
C26H16N3Na3O10S3
atreleutonum atreleuton
atréleuton
atreleutón
1-[(R)-3-[5-(p-fluorobenzyl)-2-thienyl]-1-methy]"2-propynyl]-1-hydroxyurea
1-[(1R)-3-[5-(4-fluorobenzy])thiophén-2-yl]-1-méthy]prop-2-ynyl]-1-hydroxyurée
1-[(R)-3-[5-(p-fluorobencif)-2-tienil]-1"metil-2-propinil]"1-riidroxiurea
C16H15FN2O2S
aviptadilum aviptadil
aviptadil
aviptadil
L-histidyl-L-seryl-L-aspartyl-L-alanyl-L-valyl-L-phenylalanyl-L-threonyl-L-aspartyl-L-asparaginyl-L-tyrosyl-L-threonyl-L-arginyI-L-leucyl-L-arginyl-L-tysyl-L-glutaminyl-L-methionyl-L-alanyl-L-valyl-L-lysyl-L-lysyl-L-tyrosyl-L-leucyl-L-asparaginyl-L-seryl-L-isoleucyl-L-leucyl-L-asparagine
L-histidyl-L-séryl-L-aspartyl-L-alanyl-L-valyl-L-phénylalanyl-L-thréonyl-L-aspartyl-L-asparaginyl-L-tyrosyI-L-thréonyl-L-arginyl-L-leucyl-L-arginyl-L-lysyl-L-glutaminyl-L-rnéthionyl-L-alanyl-L-valyl-L-lysyl-L-lysyl-L-tyrosyl-L-lGucyl-L-asparag¡nyl-L-séryl-L-isoleucyl-L-leucyl-L-asparagine
L-histidil-L-seril-L-aspartil-L-alanil-L-valil-L-fenilalanil-L-treonil-L-aspartil-L-asparaginil-L-tirosil-L-treonil-L-arginil-L-leucil-L-arginil-L-lisil-L-glutaminil-L-metionil-L-alanil-L-valil-L-fisil-L-lisil-L-tirosil-L-leucil-L-asparaginil-L-seril-L-isoleucil-L-leucil-L-asparagina
C 1 4 7 H 2 3 8 N 4 4 O 4 2 S
belaperidonum belaperidone
bélapéridone
belaperidona
(+)-3-[2-[(1S,5R,6S)-6-(p-fluoroprienyl)-3-azabicyclo[3.2.0]hept-3-yl]ethyI]-2,4(1H,3H)-quinazolinedione
(+)-3-[2-[(1S,5R,6S)-6-(4-fluorophényl)-3-azab¡cyclo[3.2.0]hept-3-yl]éthyl]= quina2oline-2,4(1H,3H)-dione
(+)-3-[2-[(1S,5R,6S)-6-(p-fluorofenil)-3-azabiciclo[3.2.0]hept-3-il]etil]-2,4(1H,3H)-quinazolinadiona
C22H22FN3O2
bepotastinum bepotastine
bépotastine
bepotastina
(+)-4-[[(S)-p-chloro-α-2-pyridylbenzyl]oxy]-1-piperid¡nebutyricacid
acide (+)-4-[4-[(S)-(4-ch]orophényl)(pyridin-2-yl)méthoxy]pipéridin-1 -yl]butanoíque
ácido (+)-4-[[(S)-p-cloro-α-2-piridiIbencil]oxi]-1-piperidinabutírico
C21H25CIN2O3
bibapcitidum bibapcitide
bibapcitide
bibapcitida
13,13'-[oxybis[me1hylene(2,5-dioxo-1,3-pyrroIidinediyl)]]bis[A/-{mercaptoacetyi)-D-tyrosyl-S-(3-amínopropyl)-L-cysteinylglycyl-L-a-aspartyl-L-cysteinylglycylglycyl-S-(acetamidomethyl)-L-cysteínylglycyl-S-(acetamidomelhyl)-L-cysteinylglycylgIycyl-L-cysteinarníde cyclic ( 1 - 5 ) , ( 1 ' - 5') bis(sulfide)
( 1 - 5 ) , ( 1 ' - 5')-bis(sulfure cyclique) du 13,13'-[oxybis[méthylène{2,5-dioxopyrrolidine-1,3-diyl)]]bís[[N-(sulfanylacétyÍ)-D-tyrosyi]-[S-(3-aminoprapyl)-L-cystéinyl]-glycyl-L-aspartyl-L-cystéinyl-gIycyl-glycyl-[fî-[(acétylamino)méthyl]-L-cystéinyl]-glycyl-[S-[(acétylamino)méthyl]-L-cystéinyl]-glycyl-glycyl-L-cystéinamide]
(1- 5 ) , (1 ' - 5')-bis(sulfuro cíclico) de 13,13'-[oxibis[metileno(2,5-dioxo-1,3-pirrolidinadiil)]]bis[N-(mercaptoacetil)-D-tirosil-S-(3-aminopropil)-L-cisteinilglicil-L-a-aspartil-L-cisteinilglicilglicil-S-(acetamidometil)-L-cisteinilglicil-S-{acetamidometil)-L-cisteinilglicilghcil-L-cisteinamida cíclica
C112H162N36O43S10
biricodarum
biricodar
biricodar
biricodar
4-(3-pyndyI)-1 -[3-(3-pyridyl)propyl]butyl (S)-1 -[(3,4,5-trimethoxyphenyl)glyoxyloyl]pipecolate
(2S)-1-[2-oxo-2-(3,4,5-triméthoxyphényl)acétyl]pipéridine-2-carboxylatede 4-(pyridin-3-yl)-1-[3-(pyndin-3-yl)propyl]butyle
(S)-1 -[{3,4,5-trimetoxi(enil)glioxiloil]pipecolato de 4-(3-piridil)-1 -[3-(3-piridil)propil]butilo
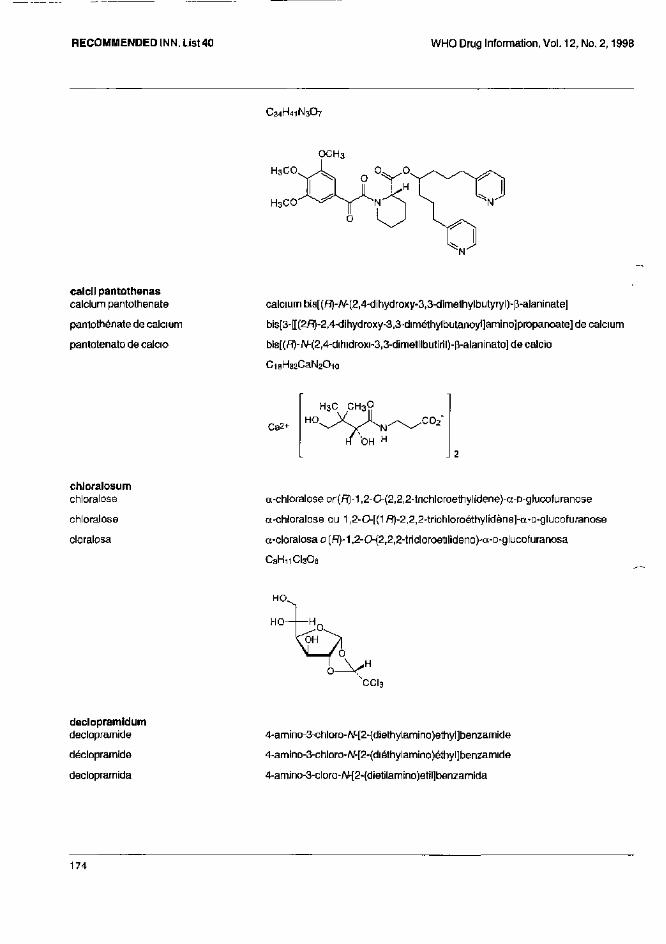
C34H41N3O7
calcli pantothenas
calcium pantothenate
pantothénate de calcium
pantotenato de calcio
calcium bis[(R)-N-(2,4-dihydroxy-3,3-d¡methylbutyryl)-p-alaninate]
bis[3-[[(2R)-2,4-dihydroxy-3,3-diméthylbutanoyl]am¡no]propanoate] de calcium
bis[(R)-N-(2,4-dihidroxi-3,3-dimetilbutiril)-β-alaninato] de calcio
C18H32CaN2O10
chloralosum
chloralose
chloralose
cloralosa
α-chlofaloseor(R)-1,2-0-(2,2,2-tnchloroethylidene)-a-D-glucofuranose
α-chloralose ou 1,2-0-[(1R)-2,2,2-trichloroéthylidène]-a-D-glucofuranose
α-cloralosao(R)-1,2-0-(2,2,2-tricloroetil¡deno)-a-D-glucofuranosa
C8H11CI3O6
declopramidum
decloprarnide
déclopramide
declopramida
4-amino-3-chloro-N-[2-(diethylamino)ethyl]benzamide
4-amino-3-chloro-N-[2-(diéthylamino)éthyl]benzamide
4-amino-3-cloro-N-[2-(dietilamino)etil]benzamida
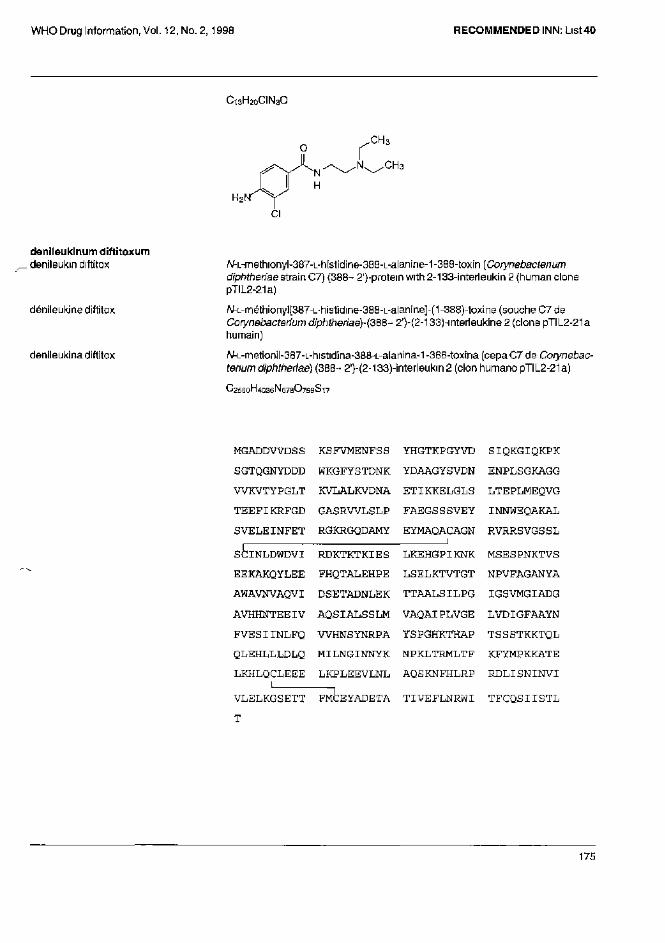
C13H20CIN3O
denileukinum diftitoxum denileukin diftitox
dénileukine diftitox
denileukina diftitox
N-L-methionyl-387-L-histidine-388-L-alanine-1-388-toxin (Corynebactenum diphtheriae strain C7) (388-2')-protem with 2-133-interleukin 2 (human clone pTIL2-21a)
N-L-rnéthiony][387-L-histidine-388-L-alanine]-(1-388)-tox¡ne (souche C7 de Corynebactenum diphtheriae)-(388-2')-(2-133)-interleukine 2 (clone pTIL2-21a humain)
N-L-rnelionil-387-L-histidina-388-L-alanina-1 -388-toxina (cepa C7 de Corynebactenum diphtheriae) (388- 2')-(2-133)-interleukin 2 (clon humano pTIL2-21a)
C2560H4036N678O799S17
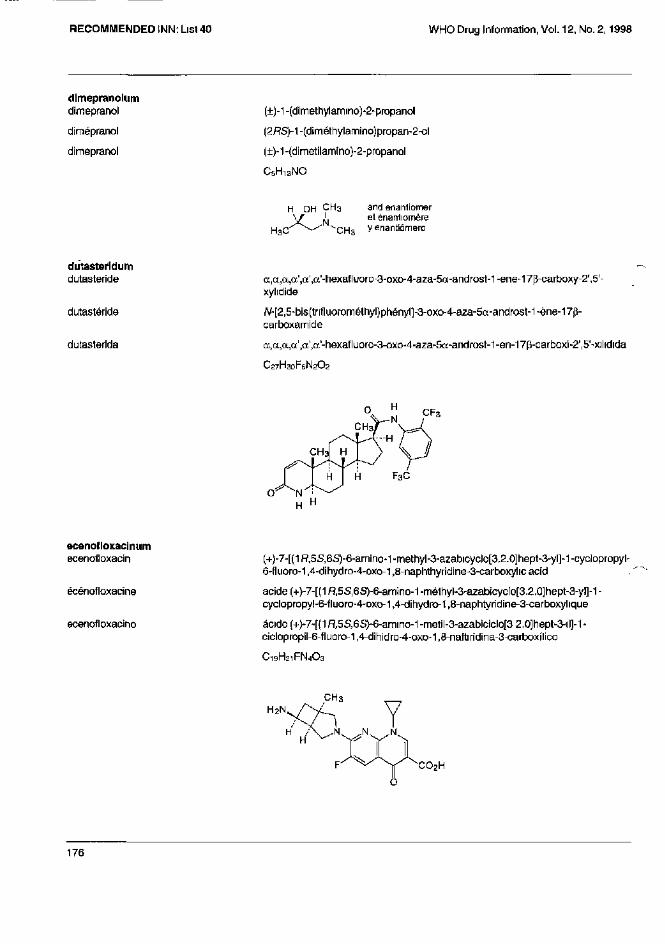
dimepranolum
dimepranol
dimepranol
dimepranol
(±)-1-(dimethylamino)-2-propanol
(2RS)-1-(dirnéthylarnino)propan-2-ol
(±)-1 -(dimetilamino)-2-propanol
C5H13NO
dutasteridum
dutasteride
dutastéride
dutasterida
α,α,α',α',α'-hexafluoro-3-oxo-4-aza-5α-androst-1-ene-17β-carboxy-2' 5'-xylidide
N-[2,5-bis(trifluorométhyl)phényl]-3-oxo-4--aza-5a-androst-1-ène-17p-carboxamide
α,α,α,α',α',α'-hexafluoro-3-oxo-4-aza-5a-androst-1-en-17p-carboxi-2',5'-xilidida
C27H30F6N2O2
ecenofloxacinum ecenofloxacin
écénofloxacine
ecenofloxacino
(+)-7-[(1R,5S,6S)-6-amino-1-methyl-3-azabicyclo[3.2.0]hept-3-yI]-1 -cyclopropyl-6-fluoro-1,4-dihydro-4-oxo-1,8-naphthyridine-3-carboxyhc acid
acide {+)-7-[(1R,5S,6S)-6-am¡no-1 -méthyl-3-azabicyclo[3.2.0]hept-3-yl]-1 -cyclopropy!-6-fluoro-4-oxo-1,4-dihydro-1,8-naphtyridine-3-carboxylique
ácido (+)-7-[(1R,5S,6S)-6-amino-1-metil-3-azabiciclo[3 2.0]hept-3-il]-1-ciclopropil-6-fluoro-1,4-d¡hidro-4-oxo-1,8-naftirid¡na-3-carboxílico
C19H21FN4O3
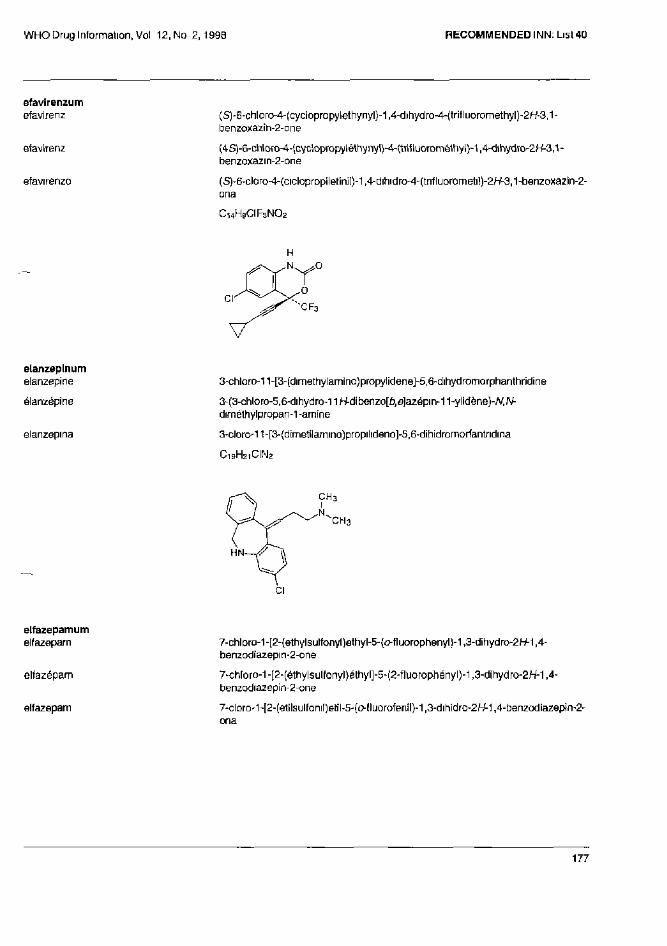
efavirenzum
efavirenz
efavirenz
efavirenza
(S)-6-chloro-4-(cyclopropylethynyl)-1,4-dihydro-4-(trifluoromethyl)-2/-/-3,1-benzoxazin-2-one
(4S)-6-chloro-4-(cyclopropyléthynyl)-4-(trifluoromé1hyl)-1,4-dihydro-2H-3,1-benzoxazin-2-one
(S)-6-cloro-4-(ciclopropile[iniI)-1,4-dihidro-4-(trifluorometi])-2/-/-3,1-benzoxazin-2-ona
C14H9CIF3NO2
elanzepinum elanzepine
élanzépine
elanzepina
3-chloro-11-[3-(dimelhylamino)propylidene]-5,6-dihydromorphanthridine
3-(3-chloro-5,6-dihydro-11 H-dibenzo[£?,e]azëpin-11-yIidène)-/V,/V-dimélhylpropan-1 -amine
3-cloro-11-[3-(dimetilamino)propilideno]-5,6-dihidromorfantndina
C19H21CIN2
elfazepamum
elfazepam
elfazépam
elfazepam
7-chlorû-1-[2-(ethylsulfonyl)ethyl-5-{o-fluorophenyl}-1,3-dihydro-2H-1,4-benzodiazepi n-2-one
7-chloro-1 -[2-(é1hylsulfonyl)éthyl]-5-(2-fluorophényl)-1,3-dihydro-2H-1,4-benzodiazepin-2-one
7-cloro-1-[2-(etilsulfoniI)eiil-5-(o-lluorofenil)-1,3-dihidro-2W-1,4-benzodiazepin-2-ona
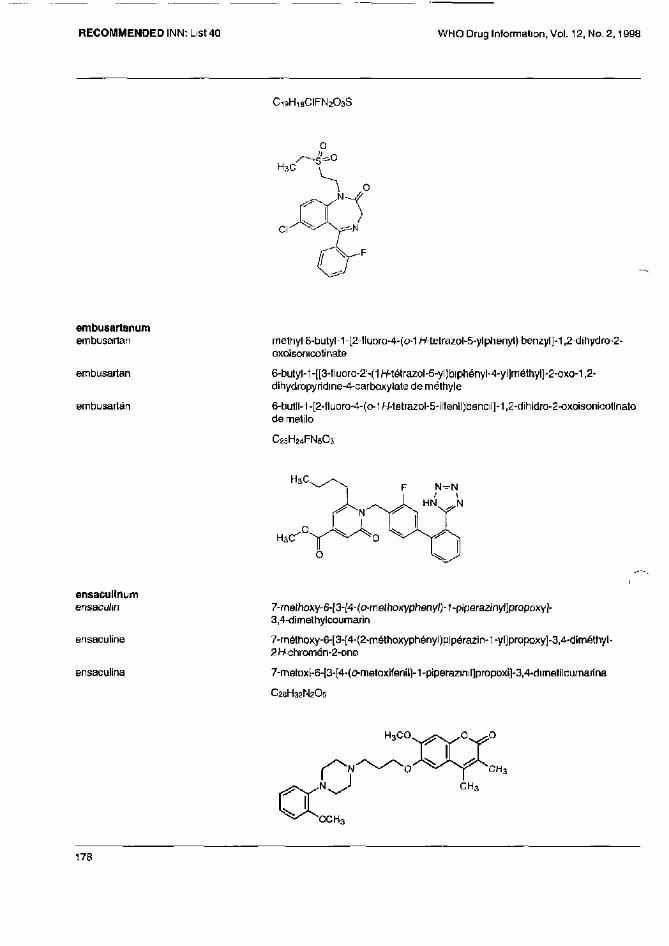
C 1 9 H 1 8 CIFN 2 O 3 S
embusartanum embusartan
embusartan
embusartan
methyl 6-butyl-1 -[2-fluoro-4-(o-1 H-tetrazol-5-yIphenyl) benzyl]-1,2-dihydro-2-oxoisonicotinate
6-butyl-1-[[3-fluoro-2'-(1H-tétrazol-5-yl)biphényl-4-yl]méthyl]-2-oxo-1,2-dihydropyridine-4-carboxylate de méthyle
6-butil-1 -[2-fluoro-4-(o-1H-tetrazo1-5-ilfenil)bencil]-1,2-dihidro-2-oxoisonicotinato de metilo
C25H24FN5O3
ensaculinum
ensaculin
ensaculine
ensaculina
7-methoxy-6-[3-[4-(o-methoxyphenyl)-1-piperazinyl]propoxy]-3,4-dirnethylcoumarin
7-méthoxy-6-[3-[4-(2-méthoxyphényl)pipérazin-1-yl]propoxy]-3,4-d¡méthyl-2H-chromén-2-one
7-rnetoxi-6-[3-[4-(o-metoxifenil)-1-piperazinil]propoxi]-3,4-dimetilcumarina
C26H32N2O5
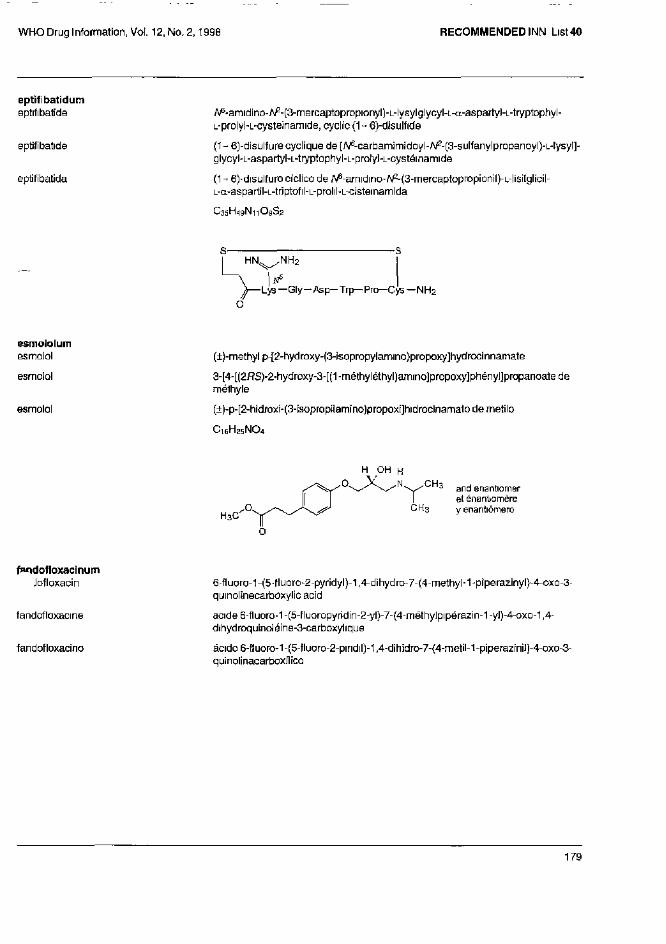
eptifibatidum
eptifibatide
eptifibatide
eptifibatida
N6-amidíno-N2-(3-mercaptopropionyl)-L-lysylglycyl-L-a-aspartyl-L-tryptophyl-L-prolyl-L-cysteinamide, cyclic (1- 6)-disulfide
(1 - 6)-disulfure cyclique de [N6-carbamimidoyl-N2-(3-sulfanylpropanoylJ-L-lysyl]-glycyl-L-aspartyl-L-tryptophyl-L-prolyl-L-cystéinamide
(1 - 6)-disulfuro cíclico de N6-amidino-ZV^ía-mercaptopropionilJ-L-lisilglicil-L-a-aspartil-L-triptofil-L-prolil-L-cistemamida
C35H49N11O9S2
esmololum esmolol
esmolol
esmolol
(±)-methylp-[2-hydroxy-(3-isopropylamino)propoxy]hydrocinnarnate
3-[4-[(2RS)-2-hydroxy-3-[(1-méthyléthyl)amino]propoxy]phényl]propanoatede mélhyle
(±)-p-[2-hidroxi-(3-isapropilamino)propoxi]hidrocinamato de metilo
C16H25NO4
fandofloxacinum fandofloxacin
fandofloxacine
fandofloxacino
6-fluoro-1-(5-tluoro-2-pyridyl)-1,4-dihydro-7-(4-methyl-1-piperazinyl}-4-oxo-3-quinolinecarboxylic acid
acide 6-fluoro-1 -(5-fluoropyridin-2-yl)-7-(4-méthyIpipérazin-1 -yl)-4-oxo-1,4-dihydroquinoléine-3-carboxyhque
ácido 6-(luoro-1-(5-fluoro-2-pindil)-1,4-dihidro-7-{4-metil-1-piperaz¡nil)-4-oxo-3-quinolinacarboxílico
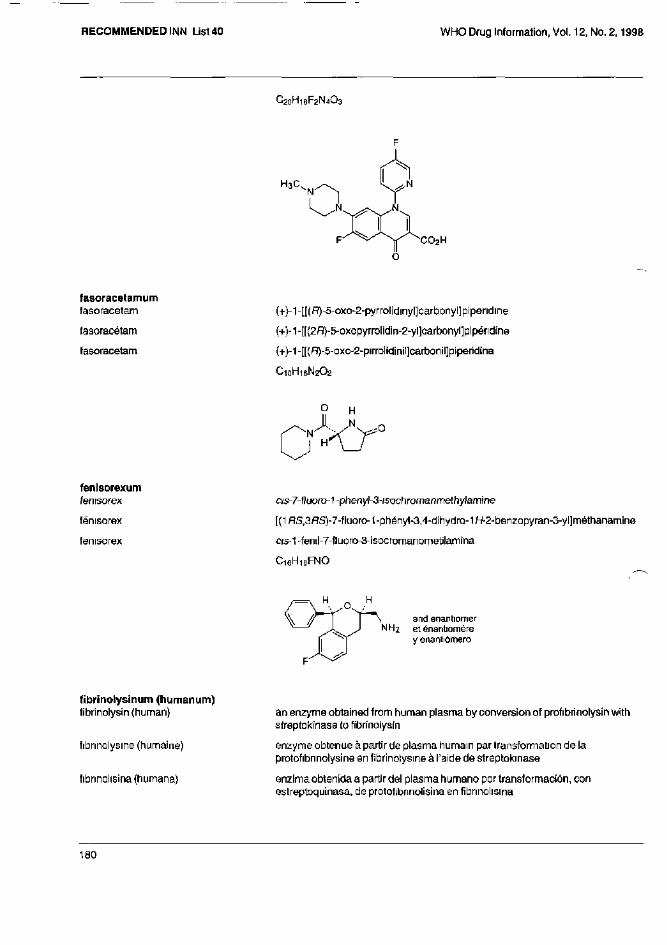
C20H18F2N4O3
fasoracetamum
fasoracetam
fasoracétam
fasoracetam
(+}-1-[[(R)-5-oxo-2-pyrrolidinyl]carbonyl]pipendine
(+)-1-[[(2R)-5-oxopyrrolidin-2-yl]carbonyl]pipéndine
(+)-1-[[(R)-5-oxo-2-pirrolidinil]carbonil]piperidina
C1 0H1 6N2O2
fenisorexum
fenisorex
fénisorex
fenisorex
c/s-7-fluoro-1-phenyl-3-isochromanrnethylamine
[(1RS,3RS)-7-fluoro-1-phényl-3,4-dihydro-1H-2-benzopyran-3-yl]méthanamine
crs-1-fenil-7-fluoro-3-isocromanometilarnina
C16H16FNO
fibrinolysinum (humanum)
fibrinolysin (human)
fibrinolysine (humaine)
fibrinolisina (humana)
an enzyme obtained from human plasma by conversion of profibrinolysin with streptokinase to fibrinolysin
enzyme obtenue à partir de plasma humain par transformation de la protofibrinolysine en fibrinolysine à l'aide de streptokinase
enzima obtenida a partir del plasma humano por transformación, con estreptoquinasa, de protofibrinolisina en fibrinolisina
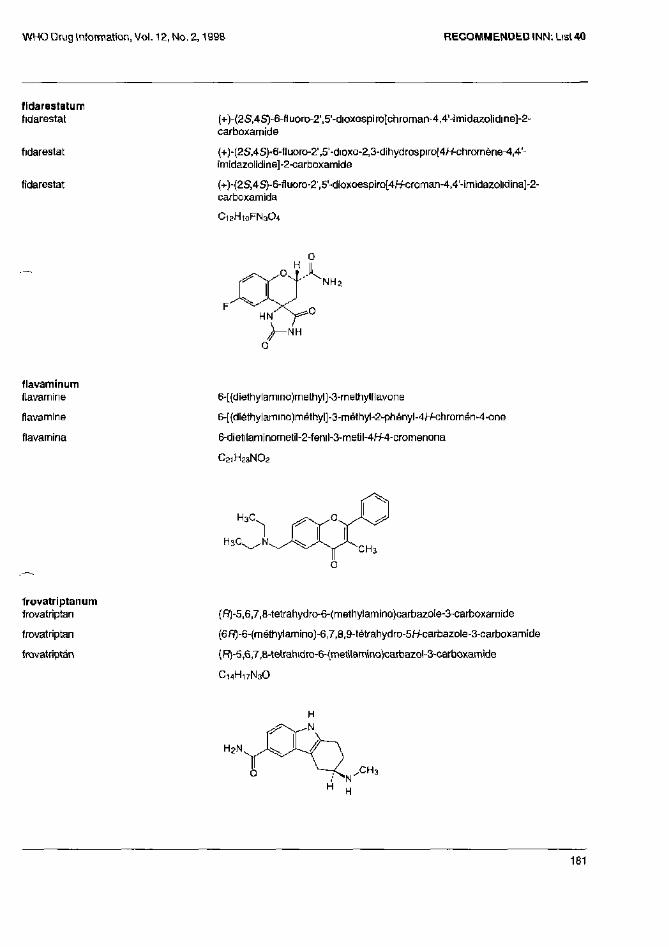
fidarestatum fidarestat
fidarestat
fidarestat
(+)-(2S,4S)-6-fluoro-2',5'-dioxospiro[chroman-4,4'-imidazolidine]-2" carboxamide
(+)-(2S,4S)-6-fluoro-2',5'-dioxo-2,3-dihydrospiro[4/-/-chrDmène-4,4'-imidazolidine]-2-carboxamide
(+)-(2S,4S)-6-fluoro-2',5'-dioxoespiro[4H-croman-4,4'-imidazolldina]'2-carboxamida
C12H10FN3O4
flavaminum
flavamine
flavamine
flavarnina
6-[(diethylamino)methyl]-3-methylflavone
6-[(diéthylamino)méthyl]-3-méthyl-2-phényl-4W-criromén-4-one
6-dietilaminornetil-2-fenil-3-metil-4H-4-cromenona
C21H23NO2
frovatriptanum
frovatriptan
frovatriptan
frovatriptan
(R)-5,6,7,8-tetrahydro-6-(methylamino)carbazo[e-3-carboxamide
(6R)-6-(méthylamino)-6,7,a,9-tétrahydro-5/-/-carbazole-3-Garboxam¡de
(R)-5,6,7,8-tetrariidro-6-{metilamino)carbazol-3"Carboxamide
C14H17N3O
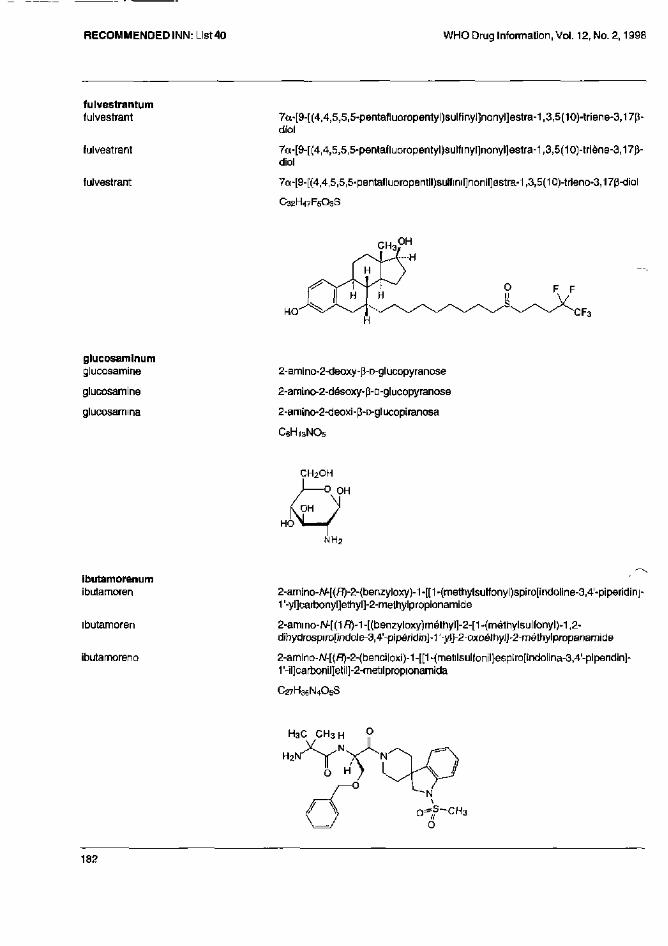
fulvestrantum
fulvestrant
fulvestrant
fulvestrant
7α-[9-[{4,4,5,5,5-pentafluoropentyl)sulfinyl]nonyl]estra-1,3,5(10)-triene-3,17p-diol
7α-[9-[(4,4,5,5,5-pentafluoropentyl)sulfinyl]nonyl]estra-1,3,5(10)-triène-3,17p-diol
7α-[9-[(4,4,5,5,5-pentafluoropentil)sulfinil]nonil]estra-1,3,5(10)-trieno-3,17β-diol
C32H47F5O3S
glucosaminum
glucosamine
glucosamine
glucosamma
2-amino-2-deoxy-p-D-glucopyranose
2-amino-2-désoxy-β-D-glucopyranose
2-amino-2-deoxi-β-D-glucopiranosa
C6H13NO5
ibutamorenum
ibutamoren
ibutamoren
ibutamoreno
2-amino-N-[(R)-2-(benzyloxy)-1-[[1-(methylsulfonyl)spiro[indoline-3,4'-piperidinj-1'-yl]carbonyl]ethyl]-2-methylpropionamide
2-ammo-N-[(1R)-1-[(benzyloxy)méthyl]-2-[1-(méthylsulfonyl)-1,2-dihydrospiro[indole-3,4'-pipéridin]-1'-yl]-2-oxoéthyl]-2-méthylpropanamide
2-arnino-N-[(R)-2-(benciloxi)-1-[[1-(metil5ulfonil)espiro[indolina-3,4'-pipendin]-1'-il]carbonil]etil]-2-metilpropionamida
C27H36N4O5S
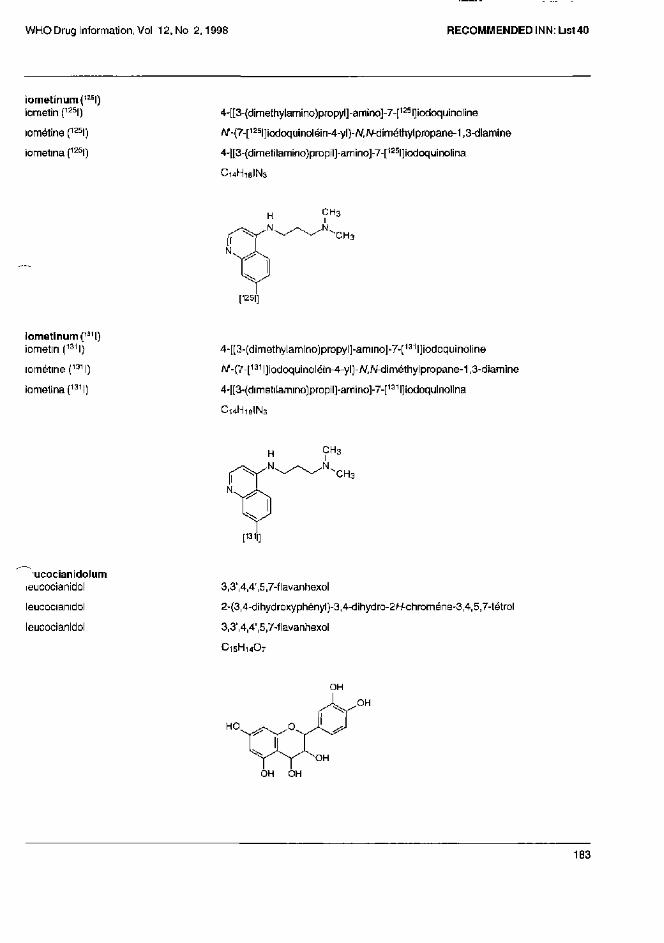
iometinum(125l)
iometin (125l)
lométine (125l)
iometina (125l)
4-[[3-(dimethylamino)propyl]-amino]-7-[125l]iodoquinoline
N-(7-[125|]iodoquinoléin-4-yl)-N,N-diméthylpropane-1,3-diamine
4-[[3-(dimetilamino)propil]-amino]-7-[125l]iodoquinolina
C14H18IN3
iometinunn(131l)
iometin (131l)
iométine (131l)
iometina(131l)
4-[[3-(dimethylarnino)propyl]-amino]-7-[131l]iodoquinoline
N-(7-[131l]iodoquinoléin-4-yl)-N,N-diméthylpropane-1,3-diamine
4-[[3-(dimetilamino)propil]-amino]-7-[131l]iodoquinolina
C14H18 IN3
leucocianidolum
leucocianidol
leucocianidol
leucocianidol
3,3',4,4',5,7-flavanhexol
2-(3,4-dihydroxyphényl)-3,4-dihydro-2/+chroméne-3,4,5,7-tétrol
3,3',4,4',5,7-flavanhexol
C15H14O7
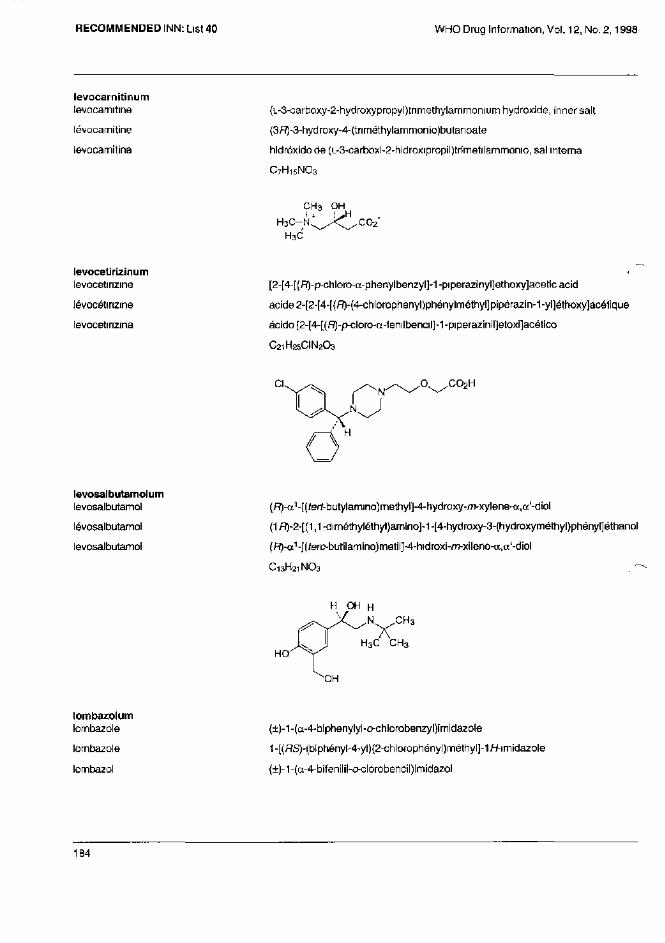
levocarnitinum
levocarnitine
lévocarnitine
levocarnitina
(L-3-carboxy-2-hydroxypropyl)tnmethylamrnonium hydroxide, inner salt
(3R)-3-hydroxy-4-(tnméthylammonio)butanoate
hidróxído de (L-3-carboxi-2-hidroxipropil)trimetilamrnonio, sal interna
C7H15NO3
levocetirizinum
levocetirizine
lévocétirizine
levocetirizina
[2-[4-[(R)-p-chloro-α-prienylbenzyl]-1-piperazinyl]ethoxy]aceticacid
acide 2-[2-[4-[(R)-(4-chlorophenyl)phénylméthyl]pipérazin-1-yl]éthDxy]acétique
ácido [2-[4-[(R)-p-cloro-α-fenilbencil]-1-piperazinil]etoxi]acé1ico
C21H25CIN2O3
levosalbutamolum
levosalbutamol
lévosalbutamol
levosalbutamol
(R)-α1-[(tert-butylamino)methyl]-4-hydroxy-m-xylene-a,a'-diol
(1R)-2-[(1,1-diméthyléthyl)amino]-1-[4-hydroxy-3-(hydroxyméthyl)phényl]éthanol
(R)-α1-[(terc-butilamino)rnetil]-4-hidroxi-m-xileno-a,a'-diol
C13H21NO3
lombazolum
lornbazole
lornbazole
lombazol
(±)-1-(α-4-biphenylyl-o-chlorobenzyl)imidazole
1-[(RS)-(biphényl-4-yl)(2-chlorophónyl}méthyl]-1H-imidazole
(±)-1-(α-4-bifenilil-o-clorobencil)imidazol
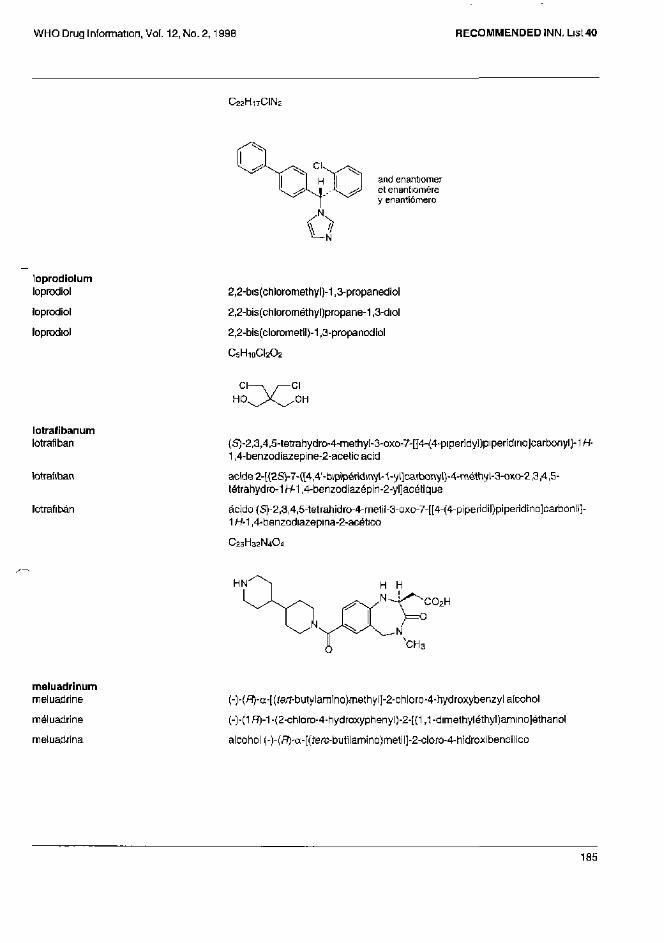
C 2 2 H 1 7 CIN 2
and enantiomer et enantiomère y enantiómero
loprodiolum
loprodiol
loprodiol
loprodiol
2,2-bis(chloromethyl)-1,3-propanediol
2,2-bis(chlorométhyl)propane-1,3-diol
2,2-bís(clorometíl)-1,3-propanodiol
C5H10CI2O2
lotrafibanum
lotrafiban
lotrafiban
lotrafibán
(S)-2,3,4,5-tetrahydro-4-methyI-3-oxo-7-[[4-(4-piperidy])piperidino]carbonyl]-1H-1,4-benzod¡azepine-2-acetic acid
acide 2-[(2S)-7-([4,4'-bipipéridinyl-1-yl]carbonyl)-4-méthyl-3-oxo-2,3,4,5-tétrahydro-1 H-1,4-benzodiazépin-2-yl]acétique
ácido {S)-2,3,4,5-tetrahidro-4-metil-3-oxo-7-[[4-(4-piperidil)pipendino]carbonil]-1 H-1,4-benzodiazepina-2-acético
C23H32N4O4
meluadrinum
meluadrine
méluadrine
meluadrina
(-)-(R)-α-[(tert-butylamino)methyl]-2-chloro-4-hydroxybenzyl alcohol
(-)-(1R)-1 -(2-chloro-4-hydroxyphenyl)-2-[(1,1 -dimethyléthyl)amino]éthanol
alcohol (-)-(R)-α-[terc-butilamino}meti]]-2-cloro-4-hidroxibencílico
C12H18CINO2
mespiperonum (11C)
mespiperone(11C)
mespipérone(11C)
mespiperona(11C)
8-[3-(p-fluorobenzoyl)propyl]-3-[11C]methyl-1-phenyl-1,3,8-triazaspiro[4.5]decan-4-one
a-[4-(4-fluorophényl)-4-oxobutyl]-3-[11C]méthyl-1-phényl-1,3,8-triazasp¡ro[4.5]décan-4-one
8-[3-(p-fluorobenzoil)propil]-3-[11C]metil-1 -fenil-1,3,8-triazaspiro[4.5]decan-4-ona
C 2 3 [ 1 1 C]H 2 8 FN 3 O 2
metforminum
metformin
metformine
metformina
1,1 -dimethylbiguanide
1,1 -diméthylbiguanide
1,1-dimetilbiguanida
C4H11N5
miansennum mianserin
miansérine
mianserina
1,2,3,4,10,14b-hexahydro-2-methyldibenzo[c,i]pyrazino[1,2-a]azepine
(14bRS)-2-rnéthyl-1,2,3,4,10,14b-hexahydrodibenzo[c,/]pyrazino[1,2-a]azépine
1,2,3,4,10,14b-hexahidro-2-metildibenzo[c,r]pirazino[1,2-a]azepina
C18H20N2
and enantiomer et énantiomère y enantiómero
midaflurum
midaflur
midaflur
midaflur
4-armino-2,2,5,5-tetrakis(trifluoromethyl)-3-imidazoline
2,2,5,5-tétrak¡s(trifluorométhyl)-2,5-d¡hydro-1H-imidazol-4-amine
4-ammo-2,2,5,5-tetrakis(trifluorametil)-3-imidazolina
C7H3F12N3
mitiglinidum mitiglinide
mitiglinide
mitiglinida
(-)-(2S,3a,7a-cis)-α-benzylhexahydro-y-oxo-2-isoindolinebutyricacid
(-)-acide{2S)-2-ben2yl-4-[(3aR-octahydro-2W-iso¡ndol-2-yl]-4-oxobutanoique
ácido (-)-(2S,3a,7a-cis)-α-bencilhe)(ahidro-Y-oxo-2-isoindounbutirico
C19H25NO3
moxifloxacinum
moxifloxacin
moxifloxacine
moxifloxacina
1-cyclopropyI-6-fluoro-1,4-dÍhydro-8-methoxy-7-[(4aS,7aS)-octahydro-6/+ pyrrolo[3,4-b]pyridin-6-yl]-4-oxo-3-quinolinecarboxylicacid
acide 1-cyclopropyl-6-fluoro-8-rnéthoxy-7-[(4aS,7aS)-oclahydro-6H-pyrrolo[3,4-6]pyridin-6-yl]-4-oxo-1,4-dihydroquinaléme-3-carboxyl¡que
ácido 1-ciclopropil-6-fluoro-1,4-dihidro-8-metoxi-7-[(4aS,7aS)-octahidro-6H-pirrolo[3,4-6]piridin-6-il]-4-oxo-3-quinolinacarboxilica
C21H24FN3O4
moxilubantum moxilubant
moxilubant
moxilubant
4-[[5-(p-amidinophenoxy)pentyl]oxy]-N,N-dilsopropyl-3-methoxybenzamide
4-[[5-(4-carbamimidoylphénoxy)pentyl]oxy]-3-méthoxy-/V,N-bis(1-méthyléthyl)benzamide
4-[[5-(p-amidinofenoxi)pentil]oxi]-N,N-dilsopropil-3-metoxibenzamída
C26H37N3O4
neocinchophenum
neocinchophen
néocinchophène
neocincofeno
ethyl 6-methyl-2-phenylquinoline-4-carboxylate
6-méthyl-2-phénylquinoléine-4-carboxylated'éthyle
2-fenil-6-metil quinolina-4-carboxilato de etilo
C19H17NO2
nepadutantum nepadutant
népadutant
nepadutant
cyclo[N-(2-acetamido-2-deoxy-[i-D-glucopyranosyl)-L-asparaginyl-L-a-aspartyl-L-tryptophyl-L-phenylalanyl-L-2,3-diaminopropionyl-L-leucyl], cyclic (2- 5)-peptide
(2- 5)-peptide cyclique du cyclo[[N4-[2-(acétylamino)-2-désoxy-β-D-glucopyranosyl]-L-asparaginyl]-L-aspartyl-L-tryptophyl-L-phénylalanyl-{3-amino-L-alanyl)-L-leucyl]
(2- 5)-péptido cíclico de ciclo[N-(2-acetamido-2-desoxi-β-D-glucopiranosil)-L-asparaginil-L-α-aspartil-L-triptofil-L-fenilalanil-L-2,3-diaminopropionil-L-leucil]
C45H58N10O13
nepafenacum
nepafenac
népafénac
nepafenaco
2-(2-amino-3-benzoylphenyl)acetamide
2-(2-amino-3-benzoylphényl)acétamide
2-(2-amino-3-benzoilfenil)acetamida
C1 5H1 4N2O2
nepicastatum nepicastat
népicastat
nepicastat
5-(aminomethyl)-1-[(S)-5,7-difluoro-1,2,3,4-tetrahydro-2-naphlhyl]-4-imidazoline-2-thione
5-(aminométhyl)-1-[(2S)-5,7-difluoro-1,2,3,4-tétrahydronaphtalén-2-yl]-1,3-dihydro-2H-imidazole-2-ihione
5-(aminometil)-1-[(S)-5,7-difluoro-1,2,3,4-tetrahidro-2-naftil]-4-imidazolina-2-tiona
C14H15F2N3S
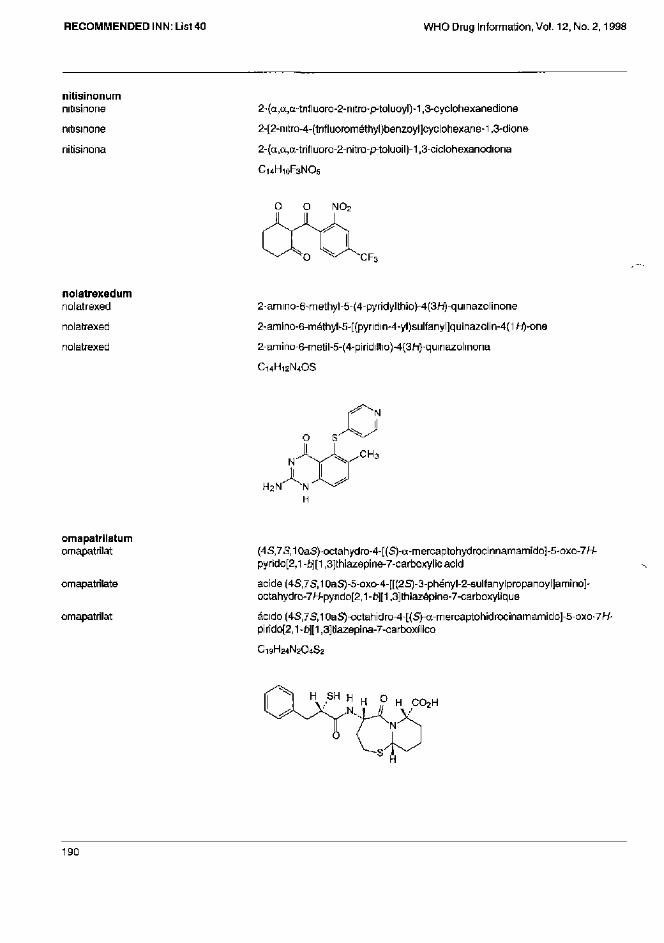
nitisinonum
nitisinone
nitisinone
nitisinona
2-(α,α,α-trifluoro-2-nitro-p-toluoyl)-1,3-cyclohexanedione
2-[2-nitro-4-(trifluorométhyl)benzoyl]cyclohexane-1,3-dione
2-(α,α,α-trifluoro-2-nitro-p-toluoil)-1,3-ciclohexanodiona
C14H10F3NO5
nolatrexedum
nolatrexed
nolatrexed
nolatrexed
2-amino-6-methyl-5-(4-pyridylthio)-4(3H)-qumazolinone
2-amino-6-méthyl-5-[(pyridin-4-yl)sulfanyl]quinazolin-4{1H)-one
2-amino-6-rnetil-5-(4-piridiltio)-4(3H)-quinazolinona
C14H12N4OS
omapatrilatum
omapatrilat
omapatrilate
omapatrilat
(4S,7S,10aS)-octahydro-4-[(S)-a-mercaptohydrocinnamamido]-5-oxo-7H-pyrido[2,l-b][l,3]Ihiazepine-7-carboxylicacid
acide (4S,7S,10aS)-5-oxo-4-[[(2S)-3-phényl-2-sulfanylpropanoyl]amino]-octahydro-7W-pyndo[2,1-b][1,3]thiazépine-7-carboxylique
ácido (4S,7S,10aS)-octahidro-4-[(S)-α-mercaptohidrocinamamido]-5-oxo-7W-pirido[2,1-b)][l,3]tiazepina-7-carboxílico
C19H24N2O4S2
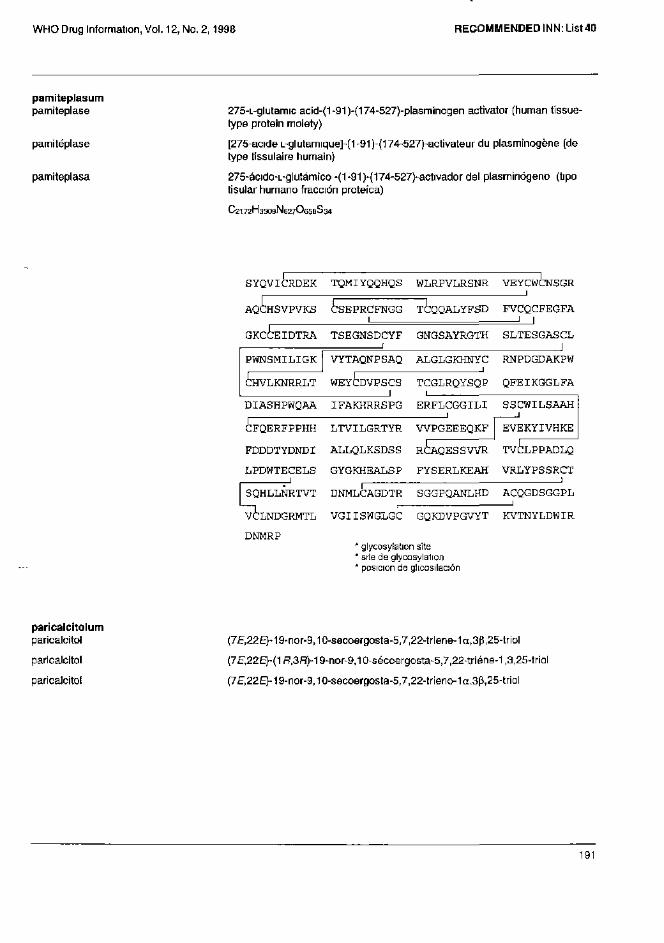
pamiteplasum pamiteplase
pamitéplase
pamiteplasa
275-L-glutamic acid-(1-91)-(174-527)-plasminogen activator (human tissue-type protein moiety)
[275-acide L-glutamique]-(1-91)-(174-527)-activateur du plasminogène (de type tissulaire humain)
275-ácido-L-glutámico -(1-91)-(174-527)-activador del plasminógeno (tipo tisular humano fracción proteica)
C2172H3309N627O658S34
* glycosylation site * site de glycosylation * posicion de glicosilación
paricalcitolum
paricalcitol
paricalcitol
paricalcitol
(7E,22E)-19-nor-9,10-secoergosta-5,7,22-triene-1a,3p,25-triol
(7E,22E)-(1R,3R19-nor-9,10-sécoergosta-5,7,22-triéne-1,3,25-triol
(7E,22E)-19-nor-9,10-secoergosta-5,7,22-trieno-1a.3[l,25-triol
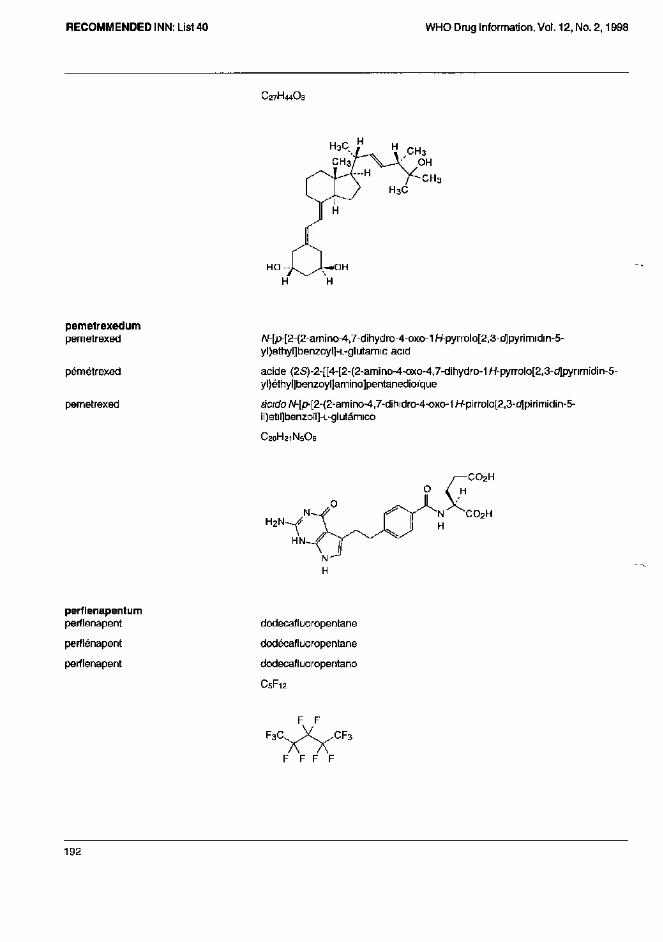
C27H44O3
pemetrexedum
pemetrexed
pémétrexed
pemetrexed
N-[p-[2-(2-amino-4,7-dihydro-4-oxo-1H-pyrrolo[2,3-d]pyrimidin-5-yl)ethyl]benzoyl]-L-glutamic acid
acide (2S)-2-[[4-[2-{2-amino-4-oxo-4,7-dihydro-1H-pyrrolo[2,3-d|pynmidin-5-yl)éthyl]benzoyl]amino]pentanedioíque
ácido N-[p-[2-(2-am¡no-4,7-dihidro-4-oxo-1H-pirrolo[2,3-c(lpirimid¡n-5-il)etil]benzoil]-L-glutámico
perflenapentum
perflenapent
perflénapent
perflenapent
dodecafluoropentane
dodécafluoropentane
dodecafluoropentano
C5F12
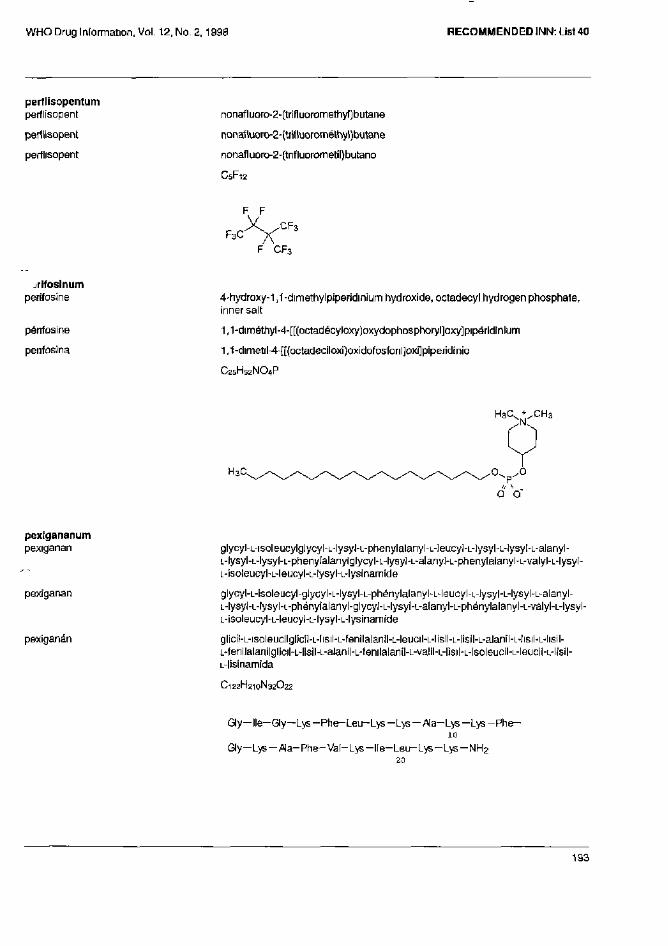
perilisopentum
perflisopent
perflisopent
perflisopent
nonafIuoro-2-(trifIuoromethyl)butane
nonafluoro-2-(trifluorométhyl)butane
nonafluoro-2-(trifluorometil}bulano
C5F12
perifosinum perifosine
périfosine
penfosina
4-hydroxy-1,1-dimethylpiperidinium hydroxide, octadecyl hydrogen phosphate, inner salt
1,1-diméthyl-4-[[(octadécyloxy)oxydophosphoryl]oxy]pipéridinium
1,1-dimetil-4-[[(octadeciloxi}oxidofosfonl]oxi]piperidinio
C25H52NO4P
pexigananum pexiganan
pexiganan
pexiganan
glycyl-L-isoleucylglycyl-L-lysyl-L-phenylalanyl-L-Ieucyl-L-]ysyl-L-Iysyl-L-alanyl-L-lysyl-L-lysyl-L-phenylalanylglycyl-L-lysyl-L-alanyl-L-phenylalanyl-L-valyl-L-lysyl-L-isoleucyl-L-leucyl-L-lysyl-L-lysinamide
glycyl-L-isoleucyl-glycyl-L-lysyl-L-phénylalanyl-L-leucyl-L-Iysyl-L-lysyl-L-alanyl-L-lysyl-L-lysyl-L-phénylalanyl-glycyl-L-lysyl-L-alanyl-L-phénylalanyl-L-valyl-L-lysyl-L-isoleucyl-L-leucyl-L-lysyl-L-lysinamide
glícil-L-isoleucilglicil-L-lisil-L-fenilalanil-L-leucil-L-lisil-L-lisil-L-alanil-L-Iisil-L-lisil-L-fenilalanilglicil-L-lisil-L-alanil-L-fenilalanil-L-valil-L-lisil-L-ísoleucil-L-leucil-L-lisil-L-lisinamida
C122H210N32O22
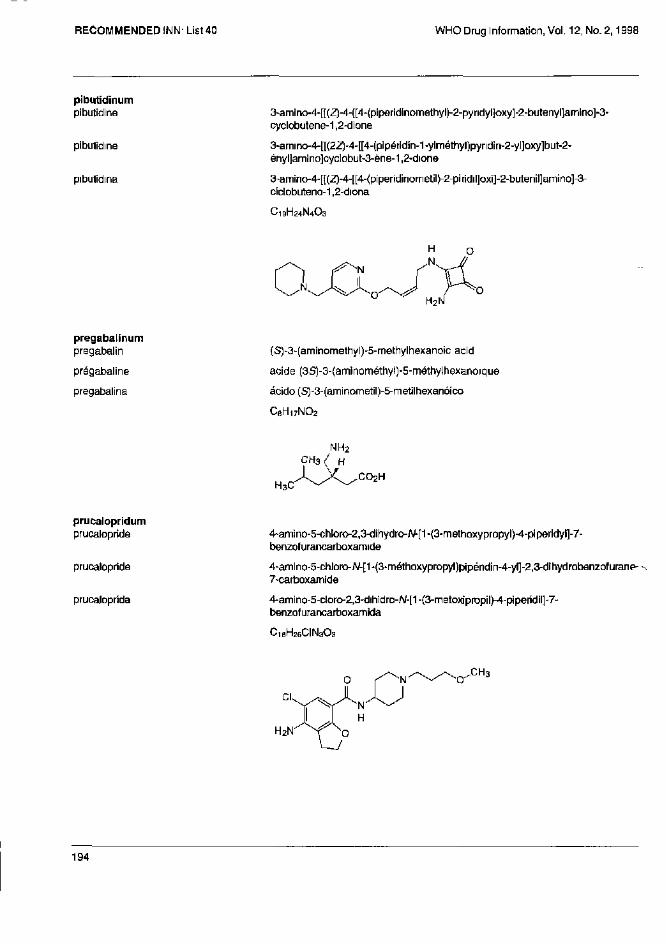
pibutidinum
pibutidine
pibutidine
pibutidina
3-amino-4-[[(Z}-4-[[4-(piperidinomethyl)-2-pyridyl]oxy]-2-butenyl]amino]-3-cyclobutene-1,2-dione
3-amino-4-[[(22)-4-[[4-{pipéridin-1-ylméthyl)pyndin-2-yl]oxy]but-2-ényl]amino]cyclobut-3-ène-1,2-dione
3-amino-4-[[(Z)-4-[[4-(p¡per¡dinometil)-2-piridil]oxi]-2-butenil]amino]-3-ciclobuteno-1,2-diona
C19H24N4O3
pregabalinum
pregabalin
prégabaline
pregabalina
(S)-3-(aminomethyl)-5-methylhexanoic acid
acide (3S)-3-{aminométhyl)-5-méthylhexanoique
ácido (S)-3-(aminornetil)-5-metilhexanóico
C6H17NO2
prucalopridum
prucalopríde
prucalopride
prucaloprida
4-amino-5-chloro-2,3-dihydro-N-[1-(3-methoxypropyl)-4-piperidyi]-7-benzofurancarboxamide
4-amino-5-chloro-N-[1-(3-méthoxypropyl)pipéndin-4-yl]-2,3-dihydrobenzofuranP' 7-carboxamide
4-amino-5-cloro-2,3-dihidro-A/-[1-{3-metoxipropil)-4-piperidil]-7-benzofurancarboxamida
C18H26CIN3O3
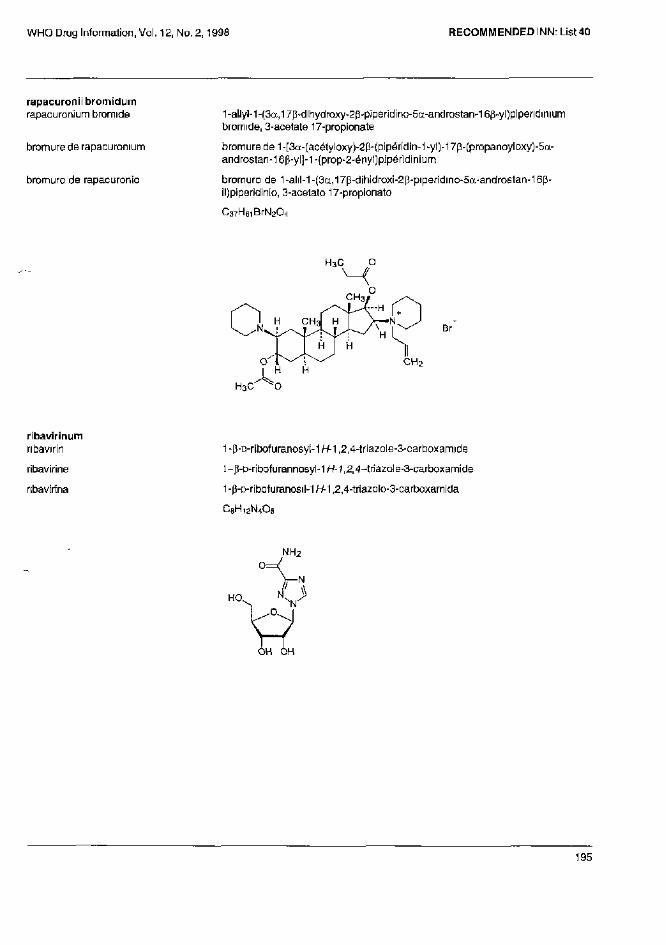
rapacuronii bromidum
rapacuronium bromide
bromure de rapacuronium
bromuro de rapacuronio
1-allyl-1-(3a,17β-dihydroxy-2β-piperidino-5α-androstan-16p-yl)piperidinium bromide, 3-acetate 17-propionate
bromure de 1-[3α-(acétyloxy)-2p-{pipéridin-1-yl)-17β-(propanoyloxy)-5α-androstan-16β-yl]-1-(prop-2-ényt)pipéridinium
bromuro de 1-alil-1-(3α,17β-dihidroxi-2p-piperïdino-5a-androstan-16p-il)piperidinio, 3-acetato 17-propionato
C37H61BrN2O4
ribavirinum
ribavirin
ribavirine
nbavirina
1 -p-o-ribofuranosyl-1 H-1,2,4-triazole-3-carboxamide
l-p-D-ribofurannosyl-1H-1,2,4-triazole-3-carboxamide
1 -β-D-ribofuranosil-1H-1,2,4-triazolo-3-carboxamida
C8H12N4O5
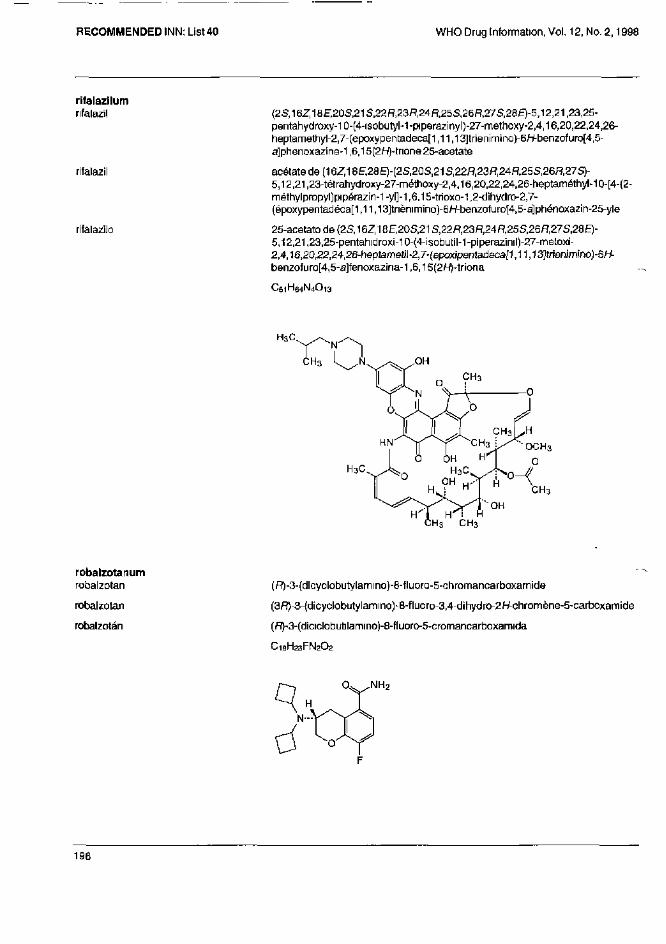
rifalazilum rifalazil
rifalazil
rifalazilo
(2S,16Z,1BE,20S,21S,22R,23R,24R,25S,26ñ,27S,28£)-5,12,21,23,25-pentahydroxy-10-(4-isobutyl-1-piperazinyl)-27-methoxy-2,4,16,20,22,24,26-heptamethyl-2,7-(epoxypentadeca[1,11,13]trienimino)-6/-/-benzof uro[4,5-a]phenoxazine-1,6,15(2H)-trione25-acetate
acétate de (16Z,18E,28E)-(2S,20S,21S,22ñ,23ñ,24ñ,25S,26ñ,27S)-5,12,21,23-tétrahydroxy-27-méthoxy-2,4,16,20,22,24,26-heptaméthyl-10-[4-{2-méthylpropyl)pipérazin-1-yl]-1,6,15-trioxo-1,2-d¡hydro-2,7-(époxypentadéca[1,11,13]tnènimino)-6H-benzofuro[4,5-a]phénoxazin-25-yle
25-acetato de (2S,16Z, 18E,20S,21S,22fí,23fí,24ñ,25S,26fí,27S,28E)-5,12,21,23,25-pentahidroxi-10-(4-isobutil-1-piperaz¡nil)-27-meloxi-2,4,16,20,22,24,26-heptamet¡l-2,7-(epox¡pentadeca[1,11,13]trienimino)-6/-í-benzofuro[4,5-a]fenoxazina-1,6,15 (2H)-triona
C51H64N4O13
robalzotanum
rabalzotan
rabalzotan
robalzotán
(R)-3-(dicyclobutylammo)-8-fluoro-5-chromancarboxamÍde
(3R)-3-(dicyclobutylamino)-8-fluoro-3,4-dihydro-2H-chromène-5-carboxamide
(R)-3-(diciclobutilamino)-8-fluoro-5-cromancarboxamida
C18H23FN2O2
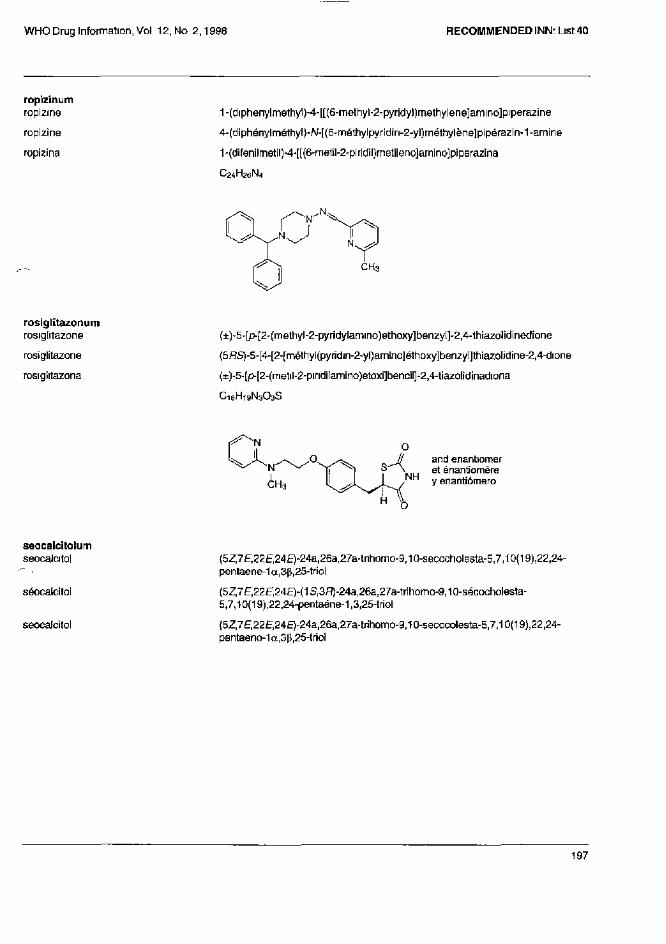
ropizinum
ropizine
ropizine
ropizina
1-(diphenylmethyl)-4-[[(6-methyl-2-pyridyl)methylene]ammo]piperazine
4-(diphénylméthyl)-N-[(6-méthylpyridin-2-yl)méthylène]pipérazin-1-amine
1-(difenilmetil)-4-[[(6-metil-2-piridil)metileno]amino]piperazina
C24H26N4
rosiglitazonum
rosiglitazone
rosiglitazone
rosiglitazona
(±)-5-[p-[2-(methyl-2-pyridylamino)ethoxy]benzyl]-2,4-thiazolidinedione
(5RS)-5-[4-[2-[rnéthyl(pyridin-2-yl}amino]éthoxy]benzy]]thiazolidine-2,4-dione
(±)-5-[p-[2-(metil-2-piridilamino)etoxi]bencil]-2,4-tiazolidinadiona
C18H19N3O3S
seocalcitolum
seocalcitol
séocalcitol
seocalcitol
{5Z,7E,22E,24E)-24a,26a,27a-trihomo-9,10-secocholesta-5,7,10(19),22,24-pentaene-1α,3β,25-triol
(5Z,7E,22E,24E)-(1S,3R)-24a,26a,27a-trihomo-9,10-sécocholesta-5,7,10(19),22,24-pentaéne-1,3,25-triol
(5Z,7E,22E,24E)-24a,26a,27a-trihomo-9,10-secocolesta-5,7,10(19),22,24-pentaeno-1α,3β,25-triol
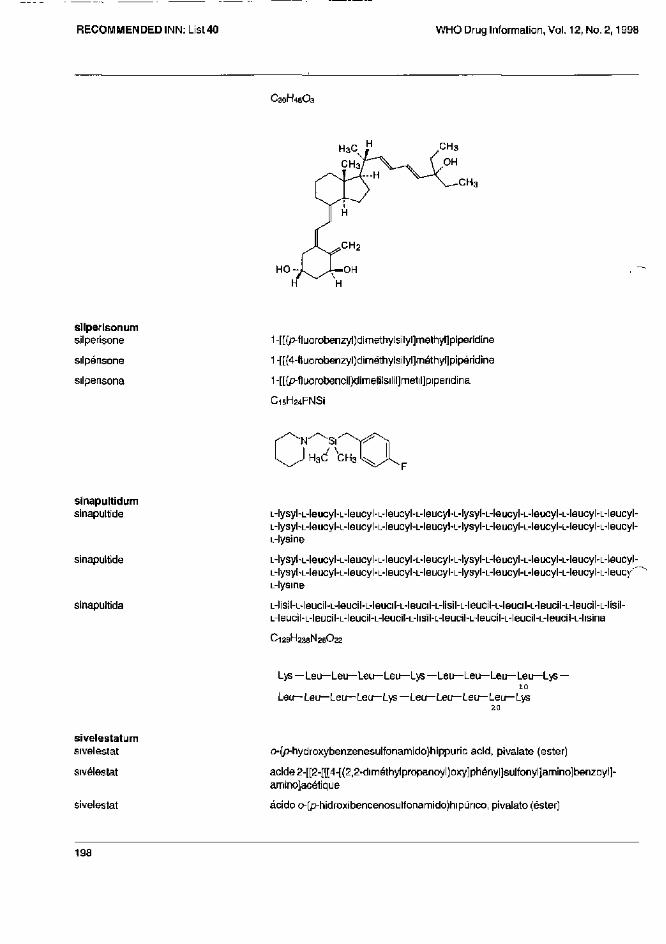
C30H46O3
CH3
silperisonum
silperisone
silpérisone
silperisona
1-[[(p-fluorobenzyl)dimethylsilyl]methyl]piperidine
1-[[(4-fluorobenzyl)diméthylsily1]méthy1]pipéridine
1-[[(p-fluorobencil)dimetilsilil]metil]pipendina
C15H24FNSi
sinapultidum sinapultide
sinapultide
sinapultida
L-lysyl-L-leucyl-L-leucyl-L-leucyl-L-leucyl-L-lysyl-L-leucyl-L-leucyl-L-leucyl-L-leucyl-L-lysyl-L-leucyl-L-leucyl-L-leucyl-L-leucyl-L-lysyl-L-leucyl-L-leucyl-L-leucyl-L-leucyl-L-lysine
L-lysyl-L-leucyl-L-leucyl-L-leucyl-L-leucyl-L-lysyl-L-leucyl-L-leucyl-L-leucyl-L-leucyl-L-lysyl-L-leucyl-L-leucyl-L-leucyl-L-leucyl-L-lysyl-L-leucyl-L-leucyl-L-leucyl-L-leuc/' L-lysine
L-lisil-L-leucil-L-leucil-L-leucil-L-leucil-L-lisil-L-leucil-L-leucil-L-leucil-L-leucil-L-lisil-L-leucil-L-leucil-L-leucil-L-leucil-L-hsil-L-leucil-L-leucil-L-leucil-L-leucil-L-hsina
C126H238N26O22
sivelestatum sivelestat
sivélestat
sivelestat
o-(p-hydroxybenzenesulfonamido)hippuric acid, pivalate (ester)
acide 2-[[2-[[[4-[(2,2-diméthyl propanoyl)oxy]phényl]sultonyl]amino]benzoyl]-amino]acétique
ácido o-(p-hidroxibencenosulfonamido)hipunco, pivalato (ester)
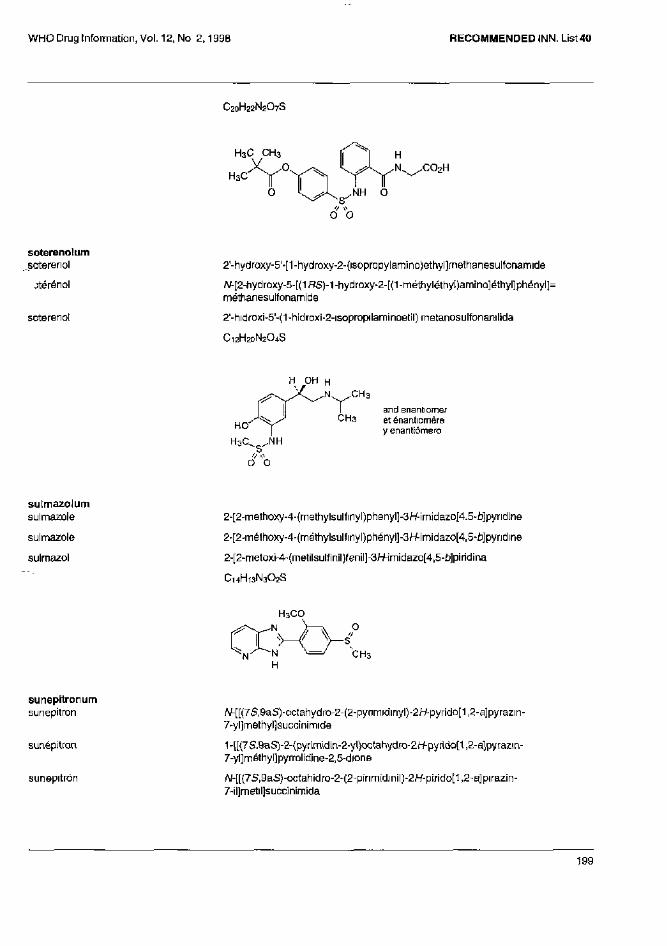
C20H22N2O7S
soterenolum soterenol
sotérénol
soterenol
2'-hydroxy-5'-[1-hydroxy-2-{isopropylamino)ethyl]rnethanesulfonamide
N-[2-hydroxy-5-[(1RS)-1 -hydroxy-2-[(1 -méthyléthyI)amino]éthyI]phenyl]; méthanesulfonamide
2'-hidroxi-5'-(1-hidroxi-2-isopropilaminoetil) rnetanosulfonanilida
C12H20N2O4S
and enantiomer et énantiomère y enantiómero
sulmazolum
sulmazole
sulmazole
sulmazol
2-[2-methoxy-4-(methylsulfinyl)phenyl]-3H-imídazo[4.5-b]pyridine
2-[2-mélhoxy-4-(méthylsulfinyl)phényl]-3H-imidazo[4,5-ù]pyndine
2-[2-metoxi-4-(metilsulfinil)fenil]-3H-imidazo[4,5-£)]piridina
C14H13N3O2S
sunepitronum
sunepitron
sunépitron
sunepitrón
N-[[(7S,9aS)-octahydro-2-(2-pyrimidinyl)-2/-/-pyrido[1,2-a]pyrazin-7-yl]rnethyl]succinimide
1-[[(7S,9aS)-2-(pyrimidin-2-yl)octahydro-2H-pyrido[1,2-a]pyrazin-7-yl]méthyI]pyrrolidine-2,5-dione
N-[[(7S,9aS)-octahidro-2-(2-pirimidinil)-2H-pirido[1,2-a]pirazin-7-il]metil]succinimida
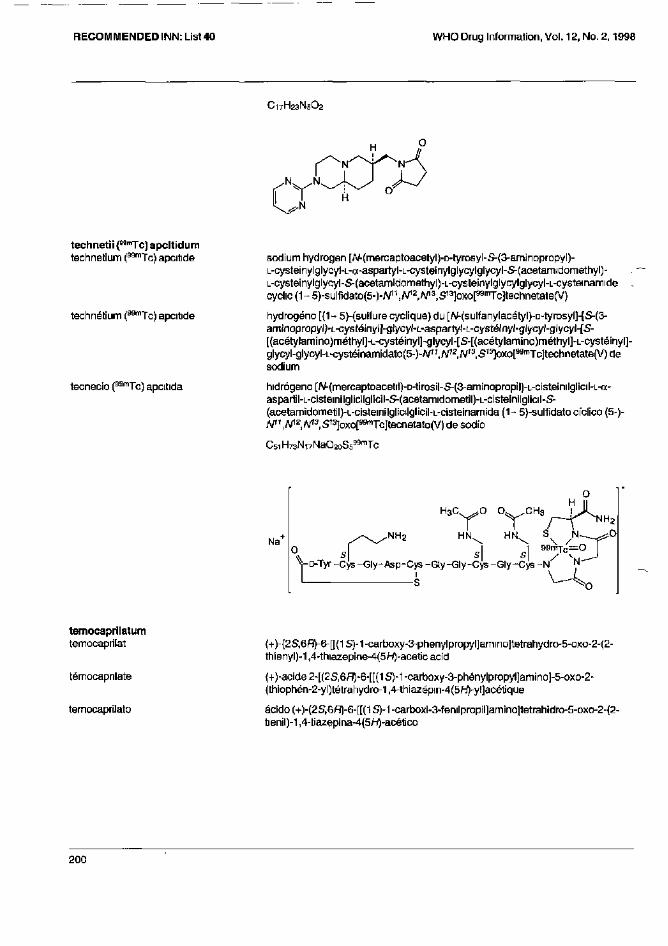
C17H23N5O2
technetii (99mTc) apcitidum technetium (99mTc) apcitide
technétium (99mTc) apcitide
tecnecio (99mTc) apcitida
sodium hydrogen [N-(mercaptoacetyl)-D-tyrosyl-S-(3-aminopropyl)-L-cysteinylglycy]-L-a-aspartyl-L-cysteinylglycylglycyl-S-(acetamidomethyl)-L-cysteinylglycyl-S-(acetamidomethyl)-L-cysteinylglycylglycyl-L-cysteinamide cyclic (1-5)-sulfidato(5-)-N11,N12,N13,S13]oxo[99mTc]technetate(V)
hydrogéno [(1 - 5)-{sulfure cyclique) du [N-(sulfanylacétyl)-D-tyrosyl]-[S-(3-aminopropyl)-L-cystéinyl]-glycyl-L-aspartyl-L-cystéinyl-glycyl-glycyl-[S-[(acétylamino)méthyl]-L-cystéinyl]-glycyl-[S-[(acétylamino)méthyl]-L-cystéinyl]-glycyl-g|ycyl-L-cystéinamidato(5-)-N11,N12,N13,S13]oxo[99mTc]technetate(V)de sodium
hidrógeno [N-(mercaptoacetil)-D-tirosil-S-(3-aminopropil)-L-cisteinilglicil-L-a-aspartil-L-cisteinilglicilglicil-S-(acetamidometil)-L-cisteinilglicil-S-(acetamidometil)-L-cisteinilglicilglicil-L-cisteinamida (1 - 5)-sulf¡dato cíclico (5-)-N11,N12,N13,S13]oxo[99mTc]tecnetato(V) de sodio
C51H73N17NaO20S599mTc
temocaprilatum
temocaprilat
témocaprilate
temocaprilato
(+)-{2S,6R)-6-[[(1S)-1-carboxy-3-phenylpropyl]amino]tetrahydro-5-oxo-2-(2-thienyl)-1,4-thiazepine-4(5H)-acetic acid
{+)-acide 2-[(2S,6R)-6-[[(1 S)-1 -carboxy-3-phénylpropyl]amino]-5-oxo-2-{thiophën-2-yl)tétrahydro-1,4-thiazépin-4(5H)-yl]acétique
ácido (+)-(2S,6R)-6-[[(1 S)-1 -carboxi-3-fenilpropil]amino]tetrahidro-5-oxo-2-(2-tienil)-1,4-tiazepina-4(5/-/)-acético
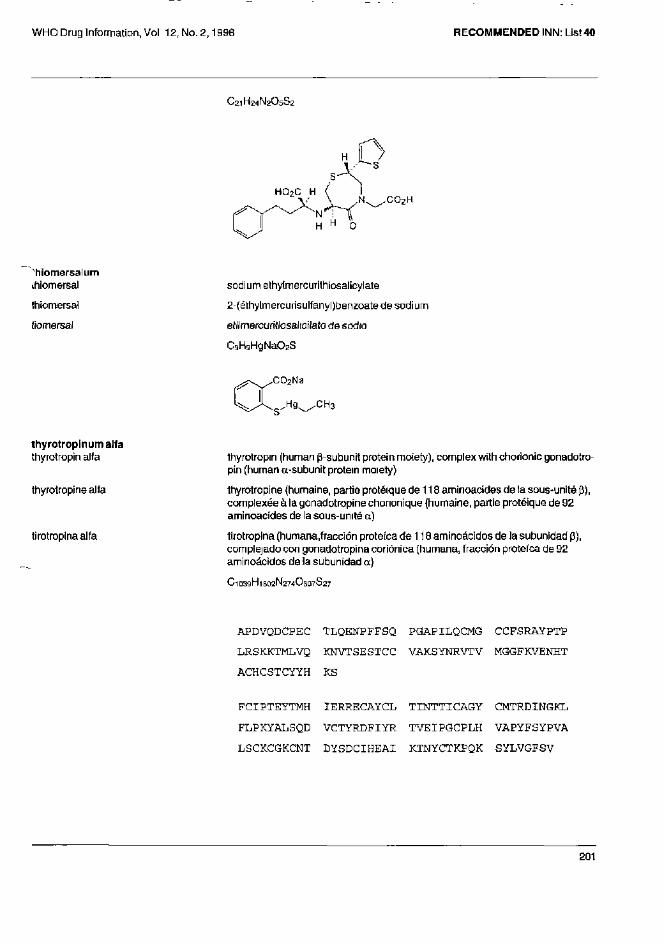
C21H24N2O5S2
thiomersalum
thiomersal
thiomersal
tiomersal
sodium ethylmercurithiosalicylate
2-(éthylmercurisulfanyl)benzoate de sodium
etilrnercuritiosalicilato de sodio
C9H9H9NaO2S
thyrotropinumalfa thyrotropin alfa
thyrotropinealfa
tirotropina alfa
thyrotropin (human β-subunit protein moiety), complex with chorionic gonadotropin {human α-subunit protein moiety)
thyrotropine (humaine, partie protéique de 118 aminoacides de la sous-unité β), complexée à la gonadotropine chononique (humaine, partie protéique de 92 aminoacides de la sous-unité a)
tirotropina (humana fracción proteica de 118 aminoácidos de la subunidad β), complejado con gonadotropina coriónica (humana, fracción proteica de 92 aminoácidos de la subunidad a)
C 1 0 3 9 H 1 6 0 2 N 2 7 4 O 3 0 7 S 2 7
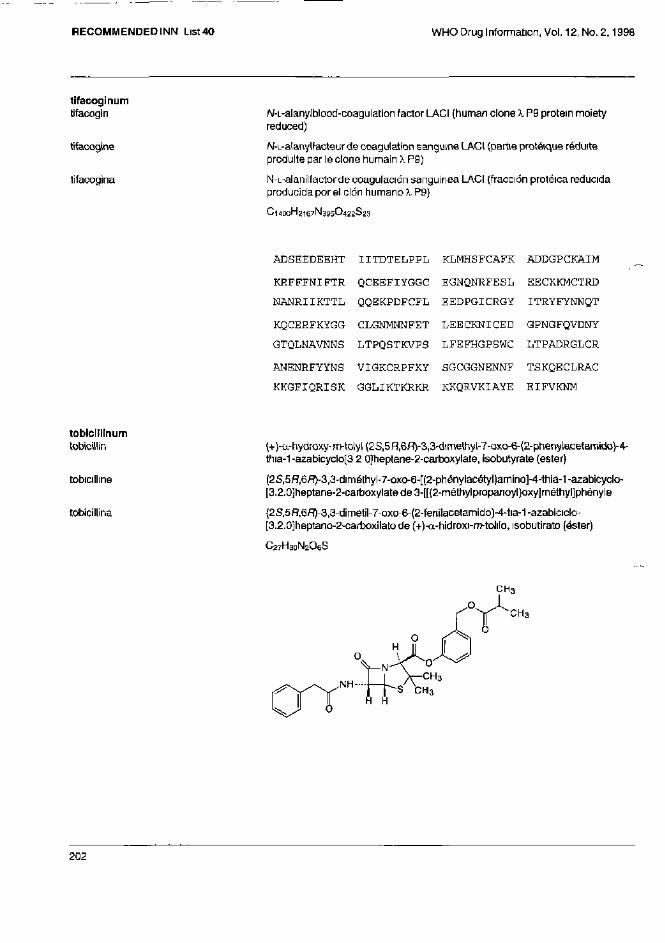
tifacoginum
tifacogin
tifacogine
tifacogina
N-L-alanyIblood-coagulation factor LACI (human clone A P9 protein moiety reduced)
N-L-alanyIfacteur de coagulation sanguine LACI (partie protéique réduite produite par le clone humain λ P9)
N-L-alanilfactor de coagulación sanguínea LACI (fracción protéica reducida producida por el clon humano λ P9)
C 1 4 0 0 H 2 1 6 7 N 3 9 5 O 4 2 2 S 2 3
tobicillinum
tobicillin
tobicilline
tobicillina
(+)-a-hydroxy-m-tolyl(2S,5H,6fl)-3,3-dimethyl-7-oxo-6-(2-phenylacetamido)-4-thia-1 -azabicyclo[3 2 0]heptane-2-carboxylate, isobutyrate (ester)
(2S,5H,6R-3,3-dimétriyl-7-oxo-6-[(2-priénylacétyl)amino]-4-th¡a-1-azabicyclc-[3.2.0]heptane-2-carboxylate de 3-[[(2-méthylpropanoyl)oxy]méthyl]phényle
(2S,5R,6R)-3,3-dimetil-7-oxo-6-(2-fenilacetam¡do)-4-tia-1-azabiciclo-[3.2.0]heptano-2-carboxilato de (+)-α-hidroxi-m-tolilo, isobutirato (éster)
C27H30N2O6S
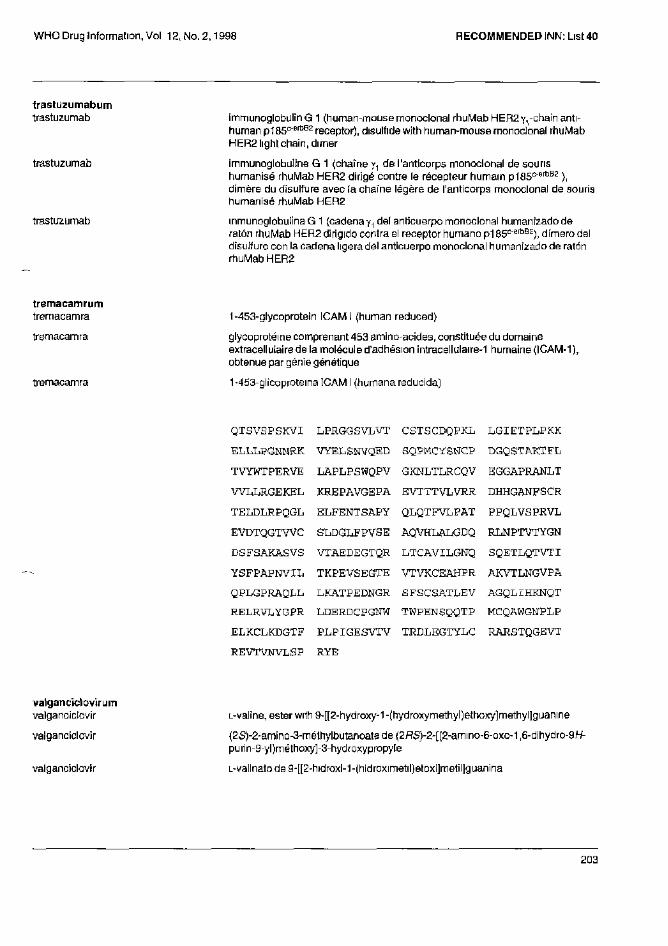
trastuzumabum trastuzumab
trastuzumab
trastuzumab
immunoglobulin G 1 (human-mouse monoclonal rhuMab HER2 y1-chain anti-human p185c-erbB2 receptor), disulfide with human-mouse monoclonal rhuMab HER2 light chain, dimer
immunoglobuline G 1 (chaîne y1 de l'anticorps monoclonal de souris humanisé rhuMab HER2 dirigé contre le récepteur humain p185c-erbB2 ), dimère du disulfure avec ¡a chaîne légère de l'anticorps monoclonal de souris humanisé rhuMab HER2
inmunoglobulina G 1 (cadena γ1 del anticuerpo monoclonal humanizado de ratón rhuMab HER2 dirigido contra el receptor humano p185c-erbB2), dímero del disulfuro con la cadena ligera del anticuerpo monoclonal humanizado de ratón rhuMab HER2
tremacamrum tremacamra
tremacamra
tremacamra
1-453-glycoprotein ICAM l (human reduced)
glycoproteins comprenant 453 amino-acides, constituée du domaine extracellulaire de la molécule d'adhésion intracellulaire-1 humaine (ICAM-1), obtenue par génie génétique
1 -453-glicoprotema ICAM I (humana reducida)
valganciclovirum valganciclovir
val ganciclovir
valganciclovir
L-valine, ester with 9-[[2-hydroxy-1 -(hydroxymethyl)ethoxy]methyl]guanine
(2S)-2-amino-3-méthylbutanoate de (2RS)-2-[(2-amino-6-oxo-1,6-dihydro-9H-purin-9-yl)méthoxy]-3-hydroxypropy[e
L-valinato de 9-[[2-hidroxi-1-(hidroximetil)etoxi]metil]guanina
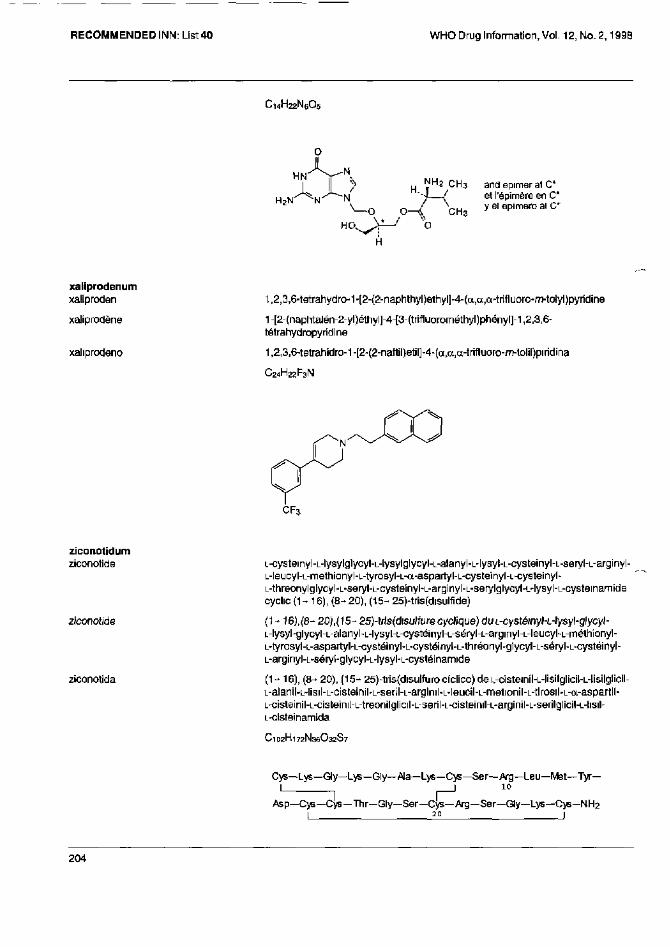
C14H22N6O5
xaliprodenum xaliproden
xaliprodène
xalipradeno
1,2,3,6-tetrahydro-1-[2-{2-naphthyl)ethyl]-4-(a,a,a-trifluoro-m-tolyl)pyridine
1-[2-(naphtalén-2-yl)éthyl]-4-[3-(trifluorométhyl)phényl]-1,2,3,6-tétrahydropyridine
1,2,3,6-tetrahidra-1-[2-(2-naftil)et¡l]-4-(a,a,a-trifluoro-m-lolil)piridina
C24H22F3N
ziconotidum ziconotide
ziconotide
ziconotida
L-cysteinyl-L-lysylglycyl-L-lysylglycyl-L-alanyl-L-ly5yl-L-cysteinyl-L-seryl-L-arginyl-L-leucyl-L-methionyl-L-tyrosyl-L-a-aspartyl-L-cysteinyl-L-cysteinyl-L-threonylglycyl-L-seryl-L-cysteinyl-L-arginyl-L-serylglycyl-L-lysyl-L-cysteinamide cyclic (1 - 16), (8- 20), (15- 25)-tris(disulfide)
( 1 - 16),(6-20),(15- 25)-tris(disulfure cyclique) du L-cystéinyl-L-lysyl-glycyl-L-lysyl-glycyl-L-alanyl-L-lysyl-L-cystéinyl-L-séryl-L-arginyl-L-leucyhL-mélhionyl-L-tyrosyl-L-aspartyl-L-cystéinyl-L-cystéinyl-L-thréonyl-glycyl-L-séryl-L-cystéinyl-L-arginyl-L-séryl-glycyl-L-lysyl-L-cystéinamide
(1 - 16), (8- 20), (15- 25)-tris(disulfuro cíclico) de L-cisteinil-L-lisilglicil-L-lisilglicil-L-alanil-L-lisil-L-cisteinil-L-seril-L-arginil-L-leucil-L-metionil-L-tirosil-L-a-aspartil-L-cisteinil-L-cisteinil-L-treonilglicil-L-seril-L-cisteinil-L-arginil-L-serilglicil-L-lisil-L-cisteinamida
C102H172N36O32S7
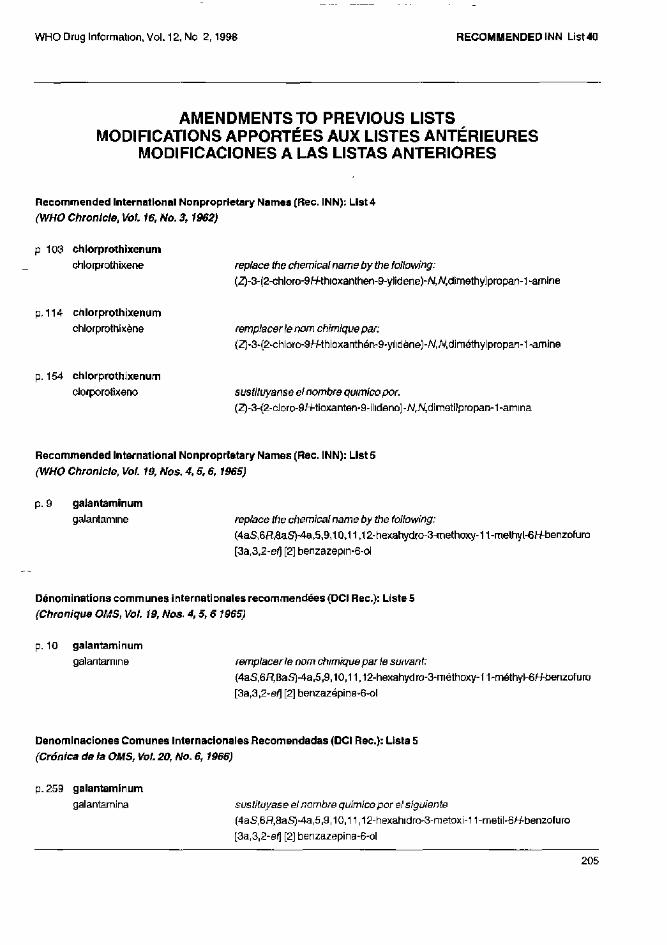
AMENDMENTS TO PREVIOUS LISTS MODIFICATIONS APPORTÉES AUX LISTES ANTÉRIEURES
MODIFICACIONES A LAS LISTAS ANTERIORES
Recommended International Nonproprietary Names (Rec. INN): List 4
(WHO Chronicle, Vol. 16, No. 3,1962)
p 103 chlorprothixenum
chlorprothixene replace the chemical name by the following:
(Z)-3-(2-chloro-9H- thioxanthen-9-ylidene)-N,N,dimethylpropan-1-amine
p. 114 chlorprothixenum
chlorprothixene remplacer le nom chimique par:
(Z)-3-(2-chloro-9H-thioxanthén-9-ylidène)-W,W,diméthylpropan-1-amine
p. 154 chlorprothixenum
clorporotixeno sustituyanse el nombre químico por.
(Z)-3-(2-cloro-9H-tioxanten-9-ílideno)-N,N,dimetilpropan-1-amina
Recommended International Nonproprietary Names (Rec. INN): List 5
(WHO Chronicle, Vol. 19, Nos. 4, 5, 6,1965)
p. 9 galantaminum
galantarnine replace the chemical name by the following:
(4aS,6RS)-4a,5,9,10,11,12-hexahydro-3-rnethoxy-11-methyl-6H-benzofuro
[3a,3,2-ef] [2] benzazepin-6-ol
Dénominations communes internationales recommendées (DCI Rec) : Liste 5
(Chronique OMS, Vol. 19, Nos. 4, 5, 6 1965)
p. 10 galantaminum
galantarnine remplacer le nom chimique par le suivant:
(4aS,6H8aS)-4a,5,9,10,11,12-hexahydro-3-rnéthoxy-11-méthyl»6/+benzofuro
[3a,3,2-ef] [2] benzazépine-6-ol
Denominaciones Comunes Internacionales Recomendadas (DCI Rec) : Lista 5
(Crónica de la OMS, Vol. 20, No. 6, 1966)
p. 259 galantaminum
galantamina sustituyase el nombre químico por el siguiente
(4aS,6R,8aS)-4a,5,9,10,11,12-hexahidro-3-metoxi-11-metil-6/^benzofuro
[3a,3,2-ef] [2] benzazepina-6-ol
Recommended International Nonproprietary Names (Rec. INN): List 31 Dénominations communes Internationales recommendées (DCI Rec): Liste 31 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Liste 31 (WHO Drug Information, Vol. S, No. 3,1991)
p. 9 nadroparinum calcium nadroparin calcium replace the definition by the following:
Calcium salt of a low molecular mass heparin obtained by nitrous acid depolyrnerization of heparin from pork intestinal mucosa, followed by fractionation to eliminate selectively most of the chains with a molecular mass lower than 2000; the majority of the components have a 2-O-sulfo-α-L-idopyranosuronic acid structure at the non-reducing end and a 6-Osulfo-2,5-anhydro-D-mannitol structure at the reducing end of their chain; the mass-average molecular mass ranges between 3600 and 5000 with a characteristic value of about 4300; the degree of sulfatation is about 2.1 per disaccharidic unit.
p. 109 nadroparine calcique remplacer la description par la suivante: Sel calcique d'une héparine de basse masse moléculaire obtenue par
dépolymerisation, au moyen d'acide nitreux, d'héparine de muqueuse
intestinale de porc; la majorité des composants de la nadroparine sodique
possèdent une structure acide 2-Osulfo-α-L-idopyranosuronique à l'extrémité
non réductrice de leur chaîne et une structure 6-O-sulfo-2,5-anhydro-D-
mannitol à l'extrémité réductrice de leur chaîne; la masse moléculaire relative
moyenne est de 3600 à 5000, avec une valeur caractéristique de 4300 environ;
le degré de sulfatation est 2.1 environ par unité disaccharidique.
p. 110 nadroparina calcica sustituyase la descripción por la siguiente:
Sal cálcica de una heparins de baja masa molecular obtenida por
despolimerización con ácido nitroso de la heparina de la mucosa intestinal de
cerdo seguida de fraccionamiento a fin de eliminar selectivamente la mayor
parte de las cadenas de masa molecular inferior a 2000; la mayoría de los
componentes tienen una estructura de ácido 2-O-sulfo-α-L-idopiranosurónico
en el extremo no reductor y una estructura de 6-O-sulfo-2,5-anhidro-D-manitol
en el extremo reductor de la cadena; la masa molecular relativa media es de
3600 a 5000, con un valor característico de 4300 aproximadamente; el grado
de sulfatación es de 2.1 por unidad de disacárido.
Recommended International Nonproprietary Names (Rec. INN): List 35 Dénominations communes internationales recommendées (DCI Rec): Liste 35 Denominaciones Comunes Internacionales Recomendadas (DCI Rec): Liste 35 (WHO Drug Information, Vol. 9, No. 3, 1995)
p. 8 delete/suppnmer/suprtmase insert/insérer/insértese
daclixirnabum daclizumabum
dacliximab daclizumab
dacliximab daclizumab
dacliximab daclizumab
Denominaciones Comunes Internacionales Recomendadas (DCI Rec): Lista 38 (WHO Drug Information, Vol. 11, No. 3, 1997)
p. 174 suprimase insértese
omiloxetino omiloxetina
Procedure and Guiding Principles/ Procédure et Directives /Procedimientos y principios generales
The text of the Procedures for the Selection of Recommended International Nonproprietary Names for Pharmaceutical Substances and General Principles for Guidance in Devising International Nonproprietary Names for Pharmaceutical Substances will be reproduced in uneven numbers of proposed INN lists only.
Les textes de la Procédure à suivre en vue du choix de dénominations communes internationales recommandées pour les substances pharmaceutiques et des Directives générales pour la formation de dénominations communes internationales applicables aux substances pharmaceutiques seront publiés seulement dans les numéros impaires des listes des DCIs proposées.
El texto de los Procedimientos de selección de denominaciones comunes internacionales recomendadas para las sustancias farmacéuticas y de los Principios generales de onentación para formar denominaciones comunes internacionales para sustancias farmacéuticas aparece solamente en los números impares de las listas de DCI propuestas.
Printed in Malta 97/11900 -Interprint- 5300