who needs a swan ? : an evidence based approach
TRANSCRIPT

Who Needs a Swan?:
An Evidence Based Approach
Monica R. Shah, MD
Financial disclosures: None
American College of Cardiology Session:
Treatment Strategies for Hospitalized Heart Failure Patients
March 16, 2015

Review the Guidelines
Evaluate the Evidence
Strategies to Implement the Guidelines
Refractory Questions
Who Needs A Swan?: An Evidence Based
Approach

The Evidence Based Medicine Triad
Best External
Evidence
Individual
Clinical
Expertise
Patient Values &
Expectations Evidence Based
Medicine
www.cochrance.org/about-us/evidence-based-health-care
Classification of Recommendations Class I – Intervention is useful
Class II – Questions about usefulness of intervention
- IIA – weight of evidence/opinion in favor
- IIB – less well established by evidence/opinion
Class III – Intervention is harmful
Level of Evidence A – Multiple clinical trials
B – Single randomized trial or non-randomized studies
C – Expert opinion
Guidelines: Evidence Based Scoring System
Circulation; 2006; 114: 1761-1791

Who Needs a Swan?: Review the Guidelines
Yancy C, et al. J Am Coll Cardiol & Circ, 2013;
Hunt S, et al. J Am Coll Card & Circ, 2009

Class I
Invasive hemodynamic (HD) monitoring should
be performed in patients with respiratory distress
or in patients with clinical evidence of impaired
perfusion in whom the adequacy or excess of
intra-cardiac filling pressures cannot be
determined from clinical assessment
Level of Evidence C
Who Needs a Swan?: Review the Guidelines
Yancy C, et al. J Am Coll Cardiol & Circ, 2013;
Hunt S, et al. J Am Coll Card & Circ, 2009

Class I: Review the Evidence

Patient decompensating and/or unstable
Respiratory distress, cardiogenic shock
Need to make decisions about interventions
Inotropes and/or urgent mechanical
support/cardiac transplant
Aggressive diuretics and/or more advanced renal
replacement therapies
Class I: Implementing the Guidelines

Who Needs A Swan?: Review the Guidelines
Class III
Routine use of invasive HD monitoring in
normotensive patients with acute decompensated
HF and congestion with symptomatic response to
diuretics and vasodilators is not recommended
Level of Evidence B
Yancy C, et al. J Am Coll Cardiol & Circ, 2013;
Hunt S, et al. J Am Coll Card & Circ, 2009

Class III: Review the Evidence
ESCAPE Investigators, JAMA, 2005; Shah MR, JAMA, 2005;
Rajaram SS, Cochrane Collaboration, 2013
RCT, n=433
13 RCT;
n=5686
13 RCT;
n=5051

Review the Evidence: ESCAPE
ESCAPE
• n=433
• NYHA class IV HF,
equipoise about
pulmonary
artery catheter (PAC)
• Intervention – PAC vs.
Clinical Assessment
• OR 1.0
(95% CI 0.82-1.21;
p=0.99)
ESCAPE Investigators. JAMA 2005;294:1625-1633

PACs are not useful in this population
Patients who needed a PAC were excluded
PAC is a diagnostic tool – choice of therapies
may have influenced outcome
~40% of patients in PAC Arm received inotropes
Short-term improvements in HD unlikely to have
long-term effects unless maintained in the
outpatient setting
Improving HF outcomes requires a continuum of care
ESCAPE: Results Debated

Class III: Review the Evidence – Meta-Analyses
Survival – No Difference with PAC
2005 2013
Shah MR, JAMA, 2005; Rajaram SS, Cochrane Collaboration, 2013

Use of invasive HD monitoring is not
indicated for routine management of
decompensated HF
But there are still some key “refractory
questions”
Class III: Implementing the Guidelines

Who Needs A Swan?: Review the Guidelines
Class IIA Invasive HD monitoring can be useful for carefully
selected patients with acute HF who have persistent symptoms despite empiric adjustment of standard therapies, and:
- Whose fluid status, perfusion, or systematic or pulmonary vascular resistance are uncertain
- Whose SBP remains low or is associated with symptoms, despite initial therapy
- Whose renal function is worsening with therapy
- Who require parenteral vasoactive agents
- Who may need consideration for advanced therapy or transplantation
Level of Evidence C
Yancy C, et al. J Am Coll Cardiol & Circ, 2013;
Hunt S, et al. J Am Coll Card & Circ, 2009

Class IIA: Review the Evidence
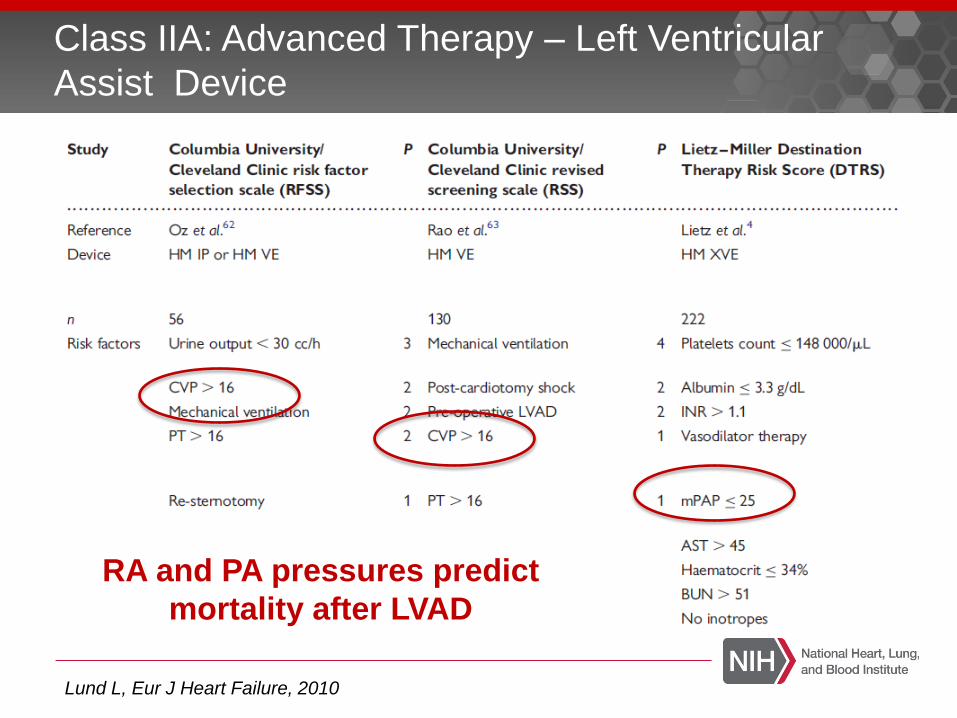
Class IIA: Advanced Therapy – Left Ventricular
Assist Device
Lund L, Eur J Heart Failure, 2010
RA and PA pressures predict
mortality after LVAD

Class IIA: Transplantation
High pre-operative PVR predicts lower survival
after transplantation
ISHLT Registry, 2009

Difficult to assess volume status Obese patients
Significant pulmonary hypertension or RV dysfunction complicating management & adjustment of therapies
Worsening renal function – guide decisions about intervention Cardio-renal syndrome – diuretics, other
decongestive strategies
Poor perfusion – inotropes, advanced therapies
Evaluate & select optimal candidates for LVAD/transplant
Class IIA: Implementing the Guidelines

Can HD monitoring help us better identify and treat persistent congestion prior to discharge?
Would inpatient HD monitoring be more effective if followed by outpatient HD monitoring?
Could we randomize acute HF patients with Class IIA or III indications to - Physician decision inpatient PAC & outpatient HD
monitoring
- Physician decision inpatient PAC & no outpatient HD monitoring
Who Needs A Swan?: Refractory Questions
Shah MR, J Card Fail, 2004

Next Steps: Integrating Inpatient & Outpatient
HD Monitoring?
CHAMPION
• n=550
• Ambulatory NYHA class III,
≥1 HF hosp. in past year
• Standard care guided by
implantable HD device
measurement
vs. standard care
• Primary Endpoint –
Rate of HF Hosp.
Abraham W, Lancet, 2011
OR 0.72 (95% CI 0.6-0.75; p=0.0002)

Decision about use of HD monitoring more clear at the extremes
We still have to use both data & clinical judgment for many of our HF patients
Perhaps the next study of HD monitoring will span both the highly controlled inpatient setting of the hospital
AND
the highly variable outpatient setting of daily life
Who Needs a Swan?: Final Thoughts

Who Needs A Swan?: More Research!

Thank You!