why read papers: an introduction to evidence based medicine arash etemadi, md phd department of...
TRANSCRIPT

Why read papers: An Introduction to Evidence
Based Medicine
Arash Etemadi, MD PhDDepartment of Epidemiology and
Biostatistics,School of Public Health, Tehran University of
Medical [email protected]

Why do we read articles?
• Browsing
• For information
• For research
• For review
• A paper from someone we know
• For going to sleep!

Do We Read ?
• Self-reported reading time per week. (University setting)– Medical students 60 min.
– Interns none
– Senior residents 10 min.
– Fellows 45 min.
– Attendings graduating
• Post 1975 60 min.
• Pre 1975 30 min.
Do We Read?
• University of Virginia
• Mailing to primary care physicians– 50% had not read a medical journal article in
the last year.– The most commonly sited source of
information was pharmacutical representatives.
Why Don’t We Read ?
• We’re lazy? – The fact of the matter is that none of us likes
feeling out of date. We like it so little in fact that we are willing to work at night and on weekends in an effort to stay current.
• Frustration.– Conflicting information– No one taught us HOW or WHAT to read.

What evidence-based medicine is:
the integration of best research evidence
with clinical expertise
and patient values.

Is EBM …
reading articles?
I. Best Research Evidence:
• clinically relevant research, often from the basic sciences of medicine, but especially from patient centered clinical research.
• Has a short doubling-time.• Replaces currently accepted diagnostic tests
and treatments with new ones that are more powerful, more accurate, more efficacious, and safer.
II. Clinical Expertise:
• rapidly identify each patient's unique health state and diagnosis,
• their individual risks and benefits of potential interventions,
• and their personal values and expectations.
III. Patients’ Values & Expectations
• the unique preferences, concerns and expectations each patient brings to a clinical encounter
• must be integrated into clinical decisions if they are to serve the patient.
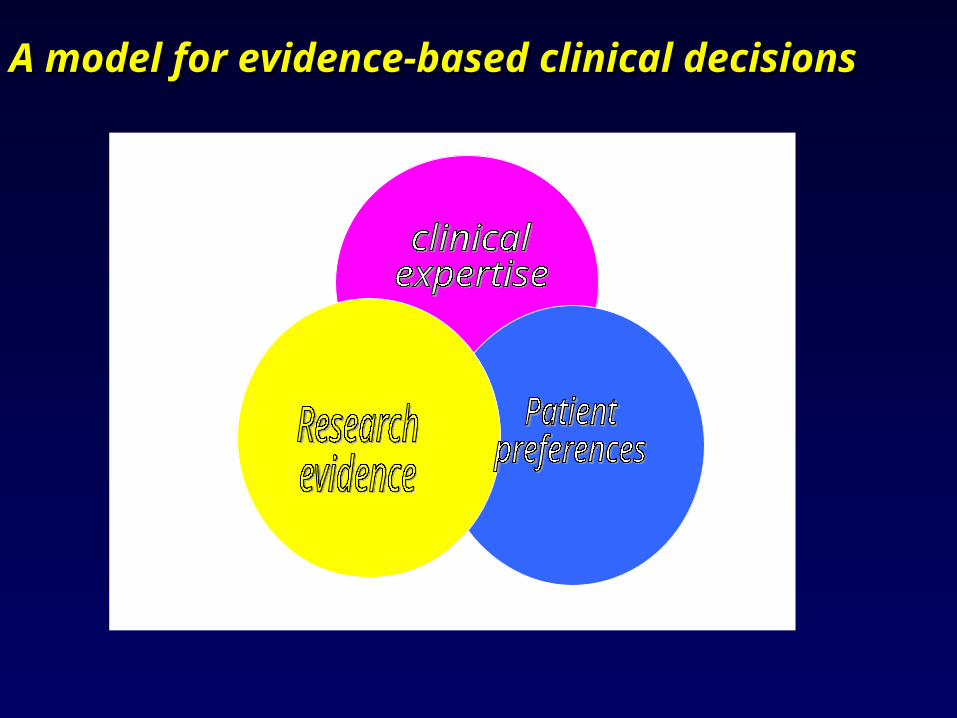
A model for evidence-based clinical A model for evidence-based clinical decisionsdecisions
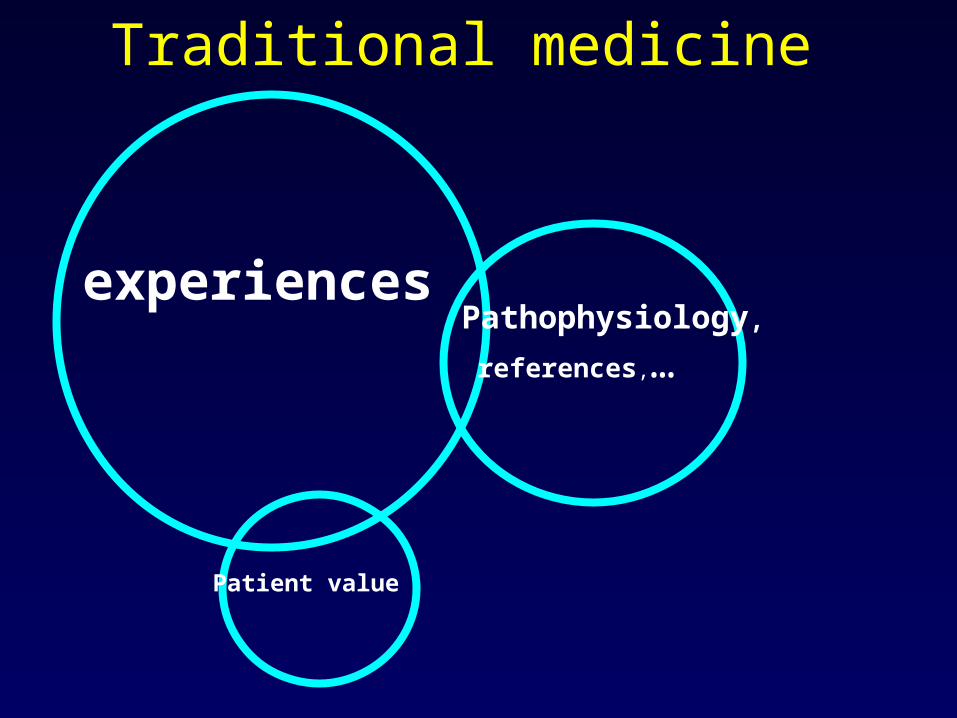
Traditional medicine
experiencesPathophysiology,
references,…
Patient value
Practice Based
On Theory

Retrolental Fibroplasia Lesson(1)(Silverman, 1977, Scientific American)
• In early 1940’s, epidemic of retrolental fibroplasia began in premature infants
Case reviews indicated “state of the art” care, including high concentration of O2
• Suspicion arose that cause occurred after birth resulting in progressive changes in retina blood vessels
• Early 1950’s, ACTH treatment proposed and RCT tested
Arm Results
ACTH 1/3 Blind
vs. ACTH = adrenocorticotrophichormone
Placebo 1/5 Blind
Retrolental Fibroplasia Lesson(2) (Silverman, 1977, Scientific American)
• Search for a cause– High dose O2 suspected based on anecdotal evidence of
147 infants
– Another observational series of 479 infants claimed benefit
• One study attempted to lower O2 dose– But nurses would turn O2 on at night and off in a.m.
– Felt no or low O2 unethical

Retrolental Fibroplasia Lesson(3)(Silverman, 1977, Scientific American)
• 1953 NIH Conference - Two opinions1. Need controlled study2. No need, O2 already convicted
• 1953 RCT began on 800 infants % Blinded
- standard O2 dose 23%
- 50% O2 dose only for clinical indications7%
Also found a dose response
• 1954 Results published, high O2 practice stopped and epidemic subsided
However, not before 10,000 infants had been blinded

Failure to Use Therapy Based on Theory
Chronic Heart Failure
• Not many good therapies in 1980’s
• Beta blockers known to be effective in post MI patient care– Reduces mortality– Lowers blood pressure– Slows and regulates heart rate
• Proscribed for heart failure patients
Beta-Blocker HFTrial Features
• Class II-IV heart failure
• Low ejection fraction
• Beta-blocker vs. placebo
• Randomized double blind
• Several thousand patients

MERITTotal Mortality

CIBIS-II
Lancet, 1999
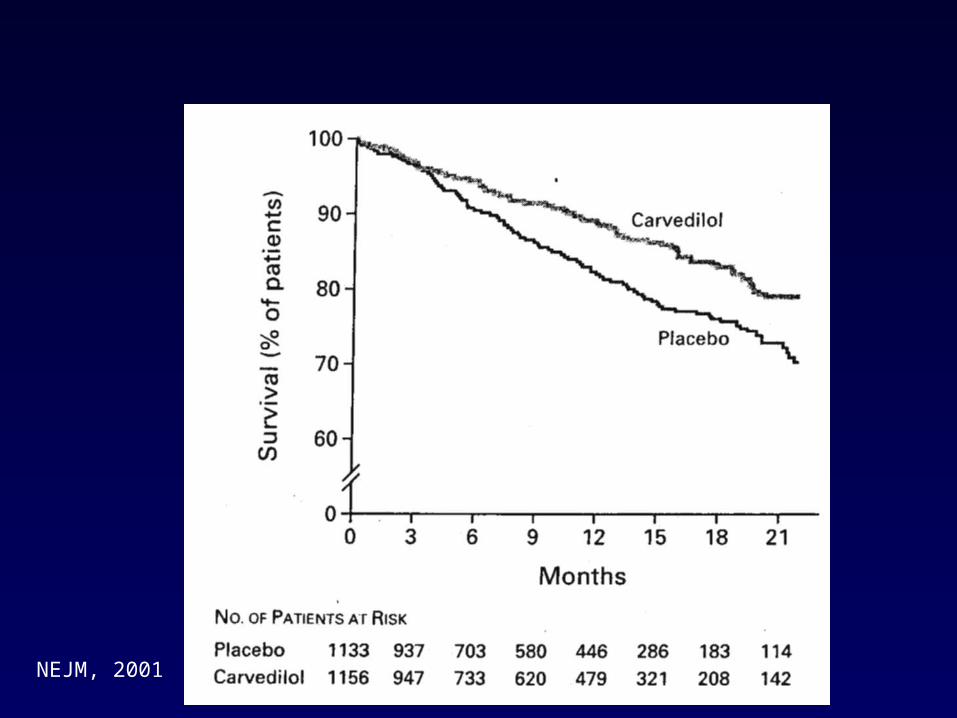
COPERNICUS
NEJM, 2001
Long Standing Treatment
Based on Theory and
Observation/Association

• Hypothesis that HRT reduced coronary heart disease
• Supportive data– Lipid lowering– Non-human primate studies– Observational studies
Hormone Replacement Therapy (HRT)
Observational Studies
• Example – Refs:1) Stampfer & Coldiz (Prev Med 1991)
Nurses Health Study
2) Grady (Ann Int Med 1992)
3) Cauley, Cummings, et al. (Am J OB/GYN, 1990)
4) Grodstein, Stempfer, Manson (NEJM 1996)
• Suggest 40-50% reduction in CHD risk
HRT POPULAR
• 1/3 of post-menopausal women use HRT
• Second most prescribed drugs
• Year 2000, 46 million prescriptions for Premarin (Estrogen)
• $1 billion in sales
• 22 million prescriptions for PremPro (E+P)

HORMONE REPLACEMENT THERAPY FOR POSTMENOPAUSAL
WOMEN• Secondary Prevention
HERS: Hully S, Grady D, Bush T, Furberg C, Herrington D, Riggs B, Vittinghoff E; for the HERS Research Group: Randomized trial of estrogen plus progestin for secondary prevention of coronary
heart disease in postmenopausal women. JAMA 28(7):605-13, 1998.
• Primary PreventionWHI: Writing Group for the Women’s Health Initiative Investigators: Risks and benefits of estrogen plus progestin in healthy postmenopausal women. Principal results from the Women’s Health Initiative Randomized Controlled trial. JAMA 288:321-333, 2002.
HERS JAMA 28(7):605-13, 1998
• Postmenopausal women• Secondary prevention, patients had
documented cardiovascular disease• Estrogen-progestin vs. placebo• Randomized double blind• Outcomes
– CVD mortality
– Fractures

HERS• Observed early clotting problems
– DVTs– PEs
• Fracture trend for benefit
• Early negative trend in mortality that reverses to neutrality (non-definitive)
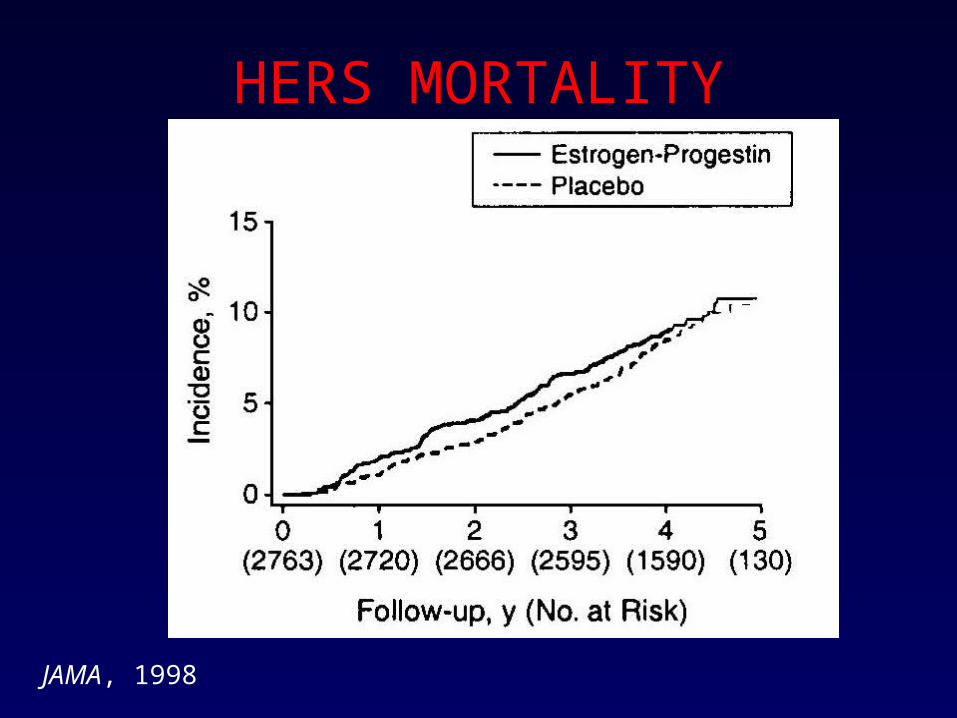
HERS MORTALITY
JAMA, 1998
HERS IMPACT
• Many believed results only applied in secondary prevention
• Many interpreted trend reversal as suggesting benefit if longer follow-up
• No perceptible impact on HRT use since HRT has other benefits
WOMEN’S HEALTH INITIATIVE
JAMA 288(3):321-33, 2002• A large factorial trial evaluating HRT, low
fat diet and calcium
• Multiple outcomes for each treatment
• For HRT– Coronary heart disease (MI & CHD death)– Invasive breast cancer– Global index– Fractures

WHI373,092 Women Initiated Screening
18,845 Provided Consent & Reported No Hysterectomy
8506 Assigned to Receive Estrogen + Progestin
8102 Assigned to Receive Placebo
16,608 Randomized
Status on April 30, 2002
7968 Alive & Outcomes Data Submitted in Last 18 Months307 Unknown Vital Status231 Deceased
Status on April 30, 2002
7608 Alive & Outcomes Data Submitted in Last 18 Months276 Unknown Vital Status218 Deceased
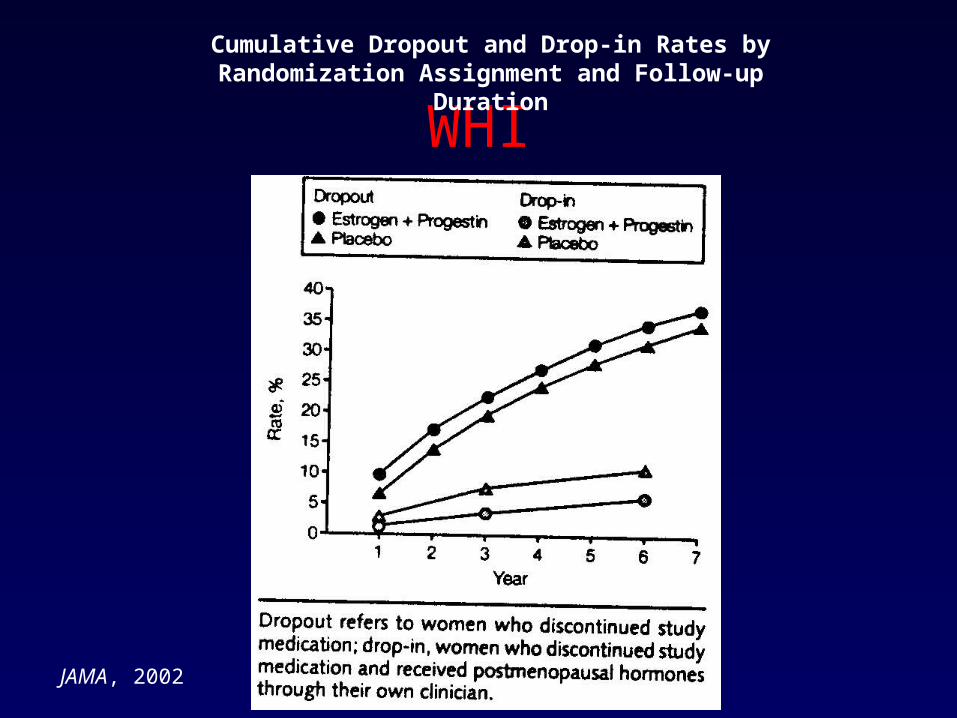
WHI
Cumulative Dropout and Drop-in Rates by Randomization Assignment and Follow-up Duration
JAMA, 2002

Wisconsin State Journal2002
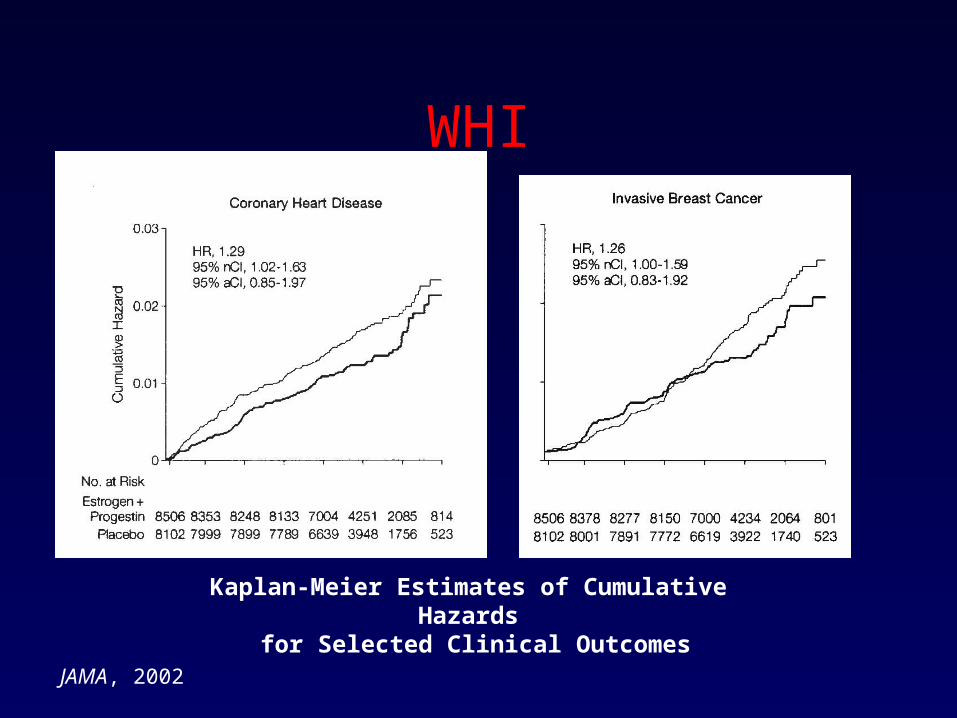
WHI
JAMA, 2002
Kaplan-Meier Estimates of Cumulative Hazards for Selected Clinical Outcomes

WHI
JAMA, 2002
Kaplan-Meier Estimates of Cumulative Hazards for Global Index and Death

WHIKaplan-Meier Estimates of Cumulative Hazards
for Selected Clinical Outcomes
JAMA, 2002
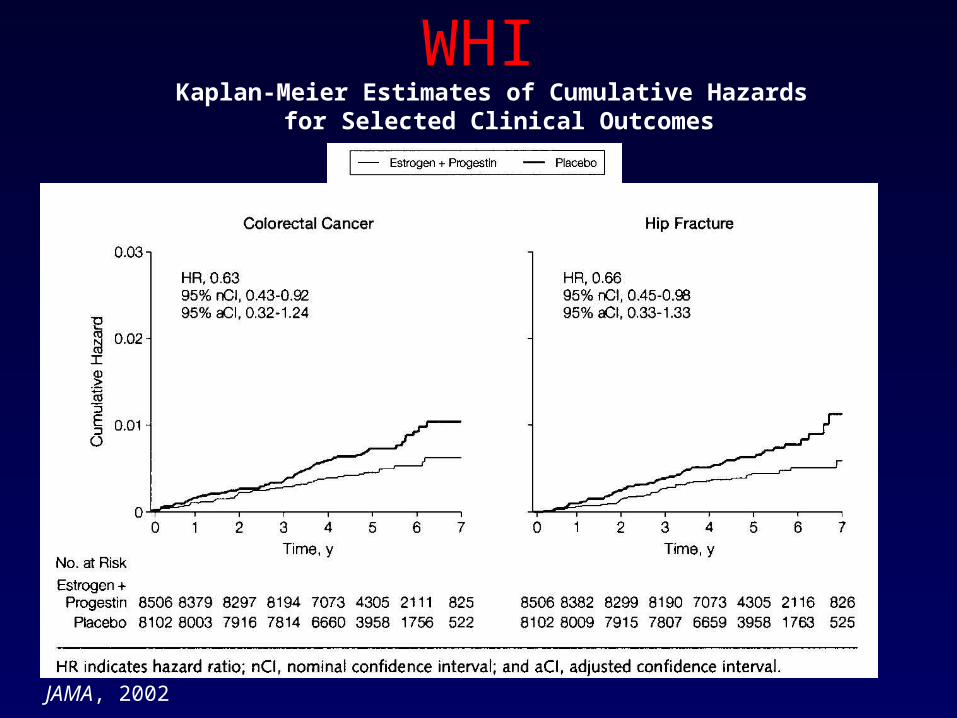
WHIKaplan-Meier Estimates of Cumulative Hazards
for Selected Clinical Outcomes
JAMA, 2002
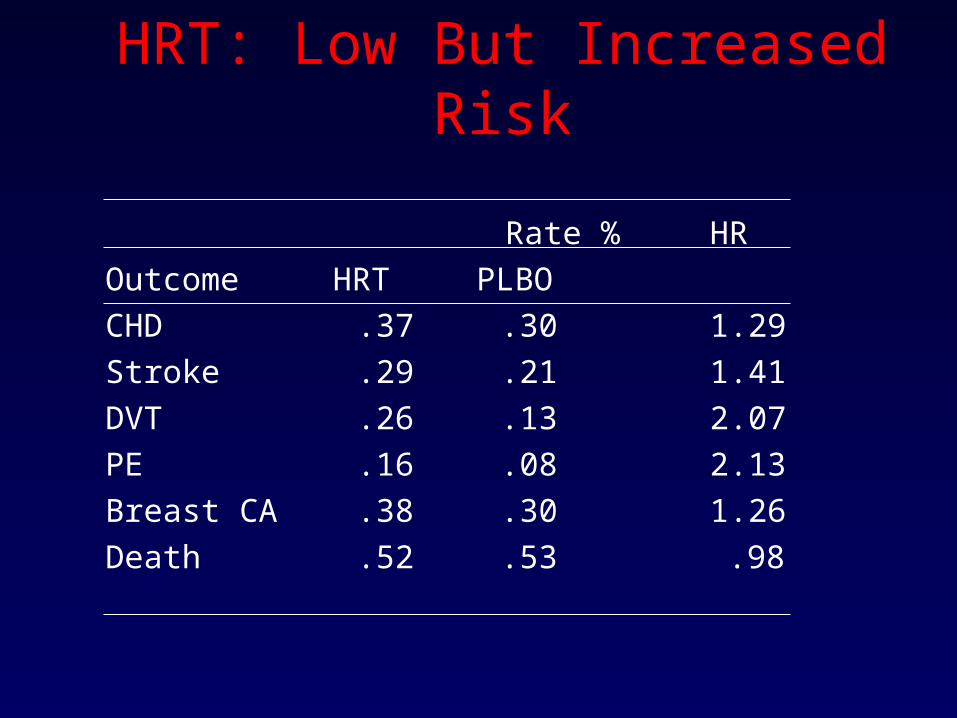
HRT: Low But Increased Risk
Rate %HR
Outcome HRT PLBO
CHD .37 .30 1.29
Stroke .29 .21 1.41
DVT .26 .13 2.07
PE .16 .08 2.13
Breast CA .38 .30 1.26
Death .52 .53 .98

Ann of Int Med 137(4), 2002
Evidence Based Medicine
• For important questions with serious mortality/morbidity, need stronger evidence such as RCTs
• If RCTs not possible, need to be cautious & vigilant about Treatments only based on observation/association or theory

The Hierarchy of EvidenceThe Hierarchy of Evidence
1. Systematic reviews & meta-analyses
2. Randomised controlled trials
3. Cohort studies
4. Case-control studies
5. Cross sectional surveys
6. Case reports
7. Expert opinion
8. Anecdotal

WashingtonMonument
A Year of MEDLINEindexed journals
555 feet
Medical Publishing
Annually:
• 20,000 journals
• 17,000 new books
MEDLINE:
• 4,000 journals
• 6 Million references
• 400,000 new entries yearly

Words used by 41 doctors to describe their information
supply• Impossible Impossible Impossible
Impossible Impossible Impossible• Overwhelming Overwhelming
Overwhelming Overwhelming Overwhelming Overwhelming
• Difficult Difficult Difficult Difficult• Daunting Daunting Daunting• Pissed off• Choked• Depressed• Despairing• Worrisome• Saturation
• Vast• Help• Exhausted• Frustrated• Time consuming• Dreadful• Awesome• Struggle• Mindboggling• Unrealistic• Stress• Challenging Challenging Challenging• Excited• Vital importance

The information paradox
• “Doctors are overwhelmed with information but cannot find information when they need it”
• “Water water everywhere, nor any drop to drink”
My students are dismayed when I say to them “Half of what you are taught as medical students will in 10 years have been shown to be wrong. And the trouble is, none of your teachers knows which half.”
(Dr Sydney Burwell, Dean of Harvard Medical School)

The Slippery Slope
Years since Med School graduation
Knowledgeof best current HTNcare
r = -0.54r = -0.54p<0.001p<0.001. ... ..
. . .... . . . .... . ............ ........
........
......
....
......
Shin,et al: CMAJ;1993: 969-976

Adapted from Slawson et al, J Fam Pract 1994; 38:505-513
Usefulness ofUsefulness ofMedical InformationMedical Information =
RelevanceRelevance x Validity
Work
A Paradigm Shift for Physicians
• From Memory Repositories
• To Information Managers
• From “How do I keep up with new developments in medicine?”
• To “What developments in medicine do I need to keep up with?”

1. Burn your (traditional) textbooks
• For a textbook to be dependable in the modern era:
· it should be revised frequently (at least once a year)
· it should be heavily referenced, at least for declarations about diagnosis and management (so readers can get to original sources for details and can also easily determine the date of a given claim)
UpToDate
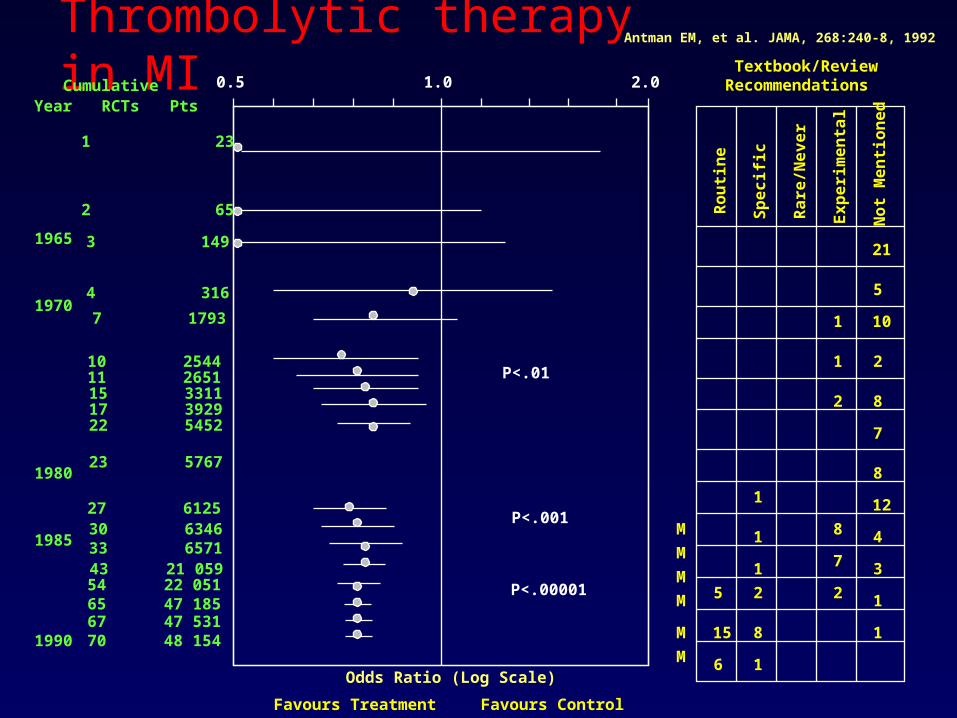
Thrombolytic therapy in MI
21
5
101
1 2
8
7
8
12
4
3
1
1
2
8
7
2
1
1
1
2
8
1
5
15
6
No
t M
en
tio
ne
d
Ro
uti
ne
Ex
pe
rim
en
tal
Ra
re/N
ev
er
Sp
ec
ific
M
M
M
M
M
M
Textbook/ReviewRecommendations
Odds Ratio (Log Scale)
0.5 1.0 2.0
Favours Treatment Favours Control
RCTs Pts
1 23
2 65
3 149
4 316
7 1793
10 254411 265115 331117 392922 5452
P<.01
23 5767
27 612530 634633 657143 21 05954 22 051
67 47 53165 47 185
70 48 154
P<.001
P<.00001
CumulativeYear
1965
1970
1980
1985
1990
Antman EM, et al. JAMA, 268:240-8, 1992
Lag time from time of “knowing” to time of implementation
• 13 yrs for thrombolytic therapy.
• 10 yrs for corticosteroids to speed fetal lung maturity.

Our textbooks are out-of-date
• Fail to recommend Rx up to ten years after it’s been shown to be efficacious.
• Continue to recommend therapy up to ten years after it’s been shown to be useless.
2. Invest in evidence databases
• ACP Journal Club http://www.acponline.org/journals/acpjc/jcmenu.htm
• Best Evidence www.acponline.org/
• Cochrane Library
• UpToDate
• MEDLINE
• Harrison’s Online
• Medscape www.medscape.com/Home/Topics/homepages.html
• MD Consult www.mdconsult.com

Does CME Work?
• Davis D A, et al. Changing physician performance. A systematic review of the effect of continuing medical education strategies. JAMA 1995; 274: 700-1.
• Sibley J C, A randomized trial of continuing medical education. N Engl J Med 1982; 306: 511-5.
• Conclusion– Traditional CME in a nice place with
pleasant after lecture diversions is, unfortunately, completely ineffective in changing our behavior.
• Another reason to read!

What About Guidelines?
• Guidelines can be very useful– Problems
• Surprise! They don’t all agree.
• Which ones do we use? (Determining validity)
• How do we implement? (How do we remember to do what they say?)
– Once validity is established they can be an excellent resource

The Experts ?
• Remember, they’re in the same position we are with information overload.
• They often look at a patient and a disease in a fundamentally different way because they deal with a selected patient population.
• Excellent resource once reliability has been established.
Evidence Based
Medicine


EBM process
1. Ask
2. Search
3. Appraise
4. Apply
5. Evaluate
Ask
• We need it twice for every 3 outpatients and 2 times for every inpatient
• Questions are most likely to be about treatment
• Most of the questions generated in consultations go unanswered.
EBM process
When caring for patients creates the need for information:
1 Translation to an answerable question
(patient/maneuver/outcome).

4 Parts of ACQ (PICO)
• P – Patient and problem
• I – Intervention (treatment, test, prognostic factor, etiology, etc.)
• C – Comparison (if necessary)
• O - Outcome

Treatment
• P – In a child with frequent febrile seizures
• I – would anticonvulsant therapy
• C – compared to no treatment
• O – result in seizure reduction?
Diagnosis
• P – In an otherwise healthy 7-year-old boy with sore throat,
• I - how does the clinical exam
• C – compare to throat culture
• O – in diagnosing GAS infection?
Prognosis
• P - In children with Down syndrome,
• I - is IQ an important prognostic factor
• C –
• O – in predicting Alzheimer’s later in life?
Etiology/Harm
• P – controlling for confounding factors, do otherwise healthy children
• I - exposed in utero to cocaine,
• C – compared to children not exposed
• O – have increased incidence of learning disabilities at age six years?
Good ACQ?
• Is Amoxicillin an effective treatment for children with otitis media?

EBM process
1. Ask
2. Search
3. Appraise
4. Apply
5. Evaluate
EBM process
2Efficient track-down of the best evidence –Secondary (pre-appraised) sources e.g.,– Cochrane (systematic reviews)
– E-B Journals
–primary literature


EBM process
1. Ask
2. Search
3. Appraise
4. Apply
5. Evaluate
EBM process
3-Critical appraisal of the evidence for its validity and clinical applicability
• Perhaps most published articles belong in the bin, and should certainly not be used to inform practice.

Why do I have to bother?Can’t I trust the editors?
Percent of articles meeting quality criteria
NEJM 12.6
Ann Int Med 7.6
JAMA 7.2
Lancet 6.2
BMJ 4.4
Arch Int Med 2.4

The Hierarchy of EvidenceThe Hierarchy of Evidence
1. Systematic reviews & meta-analyses
2. Randomised controlled trials
3. Cohort studies
4. Case-control studies
5. Cross sectional surveys
6. Case reports
7. Expert opinion
8. Anecdotal

EBM process
1. Ask
2. Search
3. Appraise
4. Apply
5. Evaluate

EBM process4 Integration of that critical appraisal
with clinical expertise and the patient’s unique biology and beliefs action.
5 Evaluation of one’s performance.

"I know that most men (sic), including those at ease with problems of the greatest complexity, can seldom accept even the simplest and most obvious truth if it be such as would oblige them to admit
the falsity of conclusions which they have delighted in explaining to colleagues, which they
have proudly taught to others, and which they have woven, thread by thread, into the fabric of
their lives.” Leo Tolstoy
"I know that most men (sic), including those at ease with problems of the greatest complexity, can seldom accept even the simplest and most obvious truth if it be such as would oblige them to admit
the falsity of conclusions which they have delighted in explaining to colleagues, which they
have proudly taught to others, and which they have woven, thread by thread, into the fabric of
their lives.” Leo Tolstoy

Recommended Reading
• Gordon Guyatt, Drummond Rennie. Users’ Guides To The Medical Literature, A Manual for Evidence-Based Clinical Practice. AMA.
• Sackett DL, Straus SE, Richardson WS, Rosenberg W, Haynes RB. Evidence-based Medicine:How to Practice and Teach EBM. Second Edition.Churchill Livingstone: Edinburgh, 2000
• Trisha Greenhalgh : How to read a paper; the basis of evidence based medicine. BMJ 2001.

Thank You!