why this course? our context
DESCRIPTION
Why this course? Our Context. Module 1b. Measuring Quality in Indian Health. IHS Director’s Priorities. To renew and strengthen our partnership with tribes In the context of national health insurance reform, to bring reform to IHS To improve the quality of and access to care - PowerPoint PPT PresentationTRANSCRIPT

Why this course? Our Context.
Module 1b.
Measuring Quality in Indian Health

IHS Director’s Priorities
1. To renew and strengthen our partnership with tribes
2. In the context of national health insurance reform, to bring reform to IHS
3. To improve the quality of and access to care
4. To make all our work accountable, transparent, fair and inclusive
The Environment We Are In
• IOM reports get the ball rolling– Crossing the Chasm– To Error is Human– Performance Measurement—Accelerating
Improvement
• National Performance Measurement Initiatives, i.e., HEDIS, NCQA*
• JCAHO—ORYX Measures• CMS Reporting & Quality Initiatives
*Health Effectiveness Data and Information Set National Committee on Quality Assurance

Quality Measurement in Health Care Reform

Quality Measurement in HealthCare Reform
• Many Provisions of PPQCA.
• Chronic Care Model & Medical Homes
• Payment Reform– Feds and States want to pay for quality, not
procedures.– Example: CMS and Re-hospitalization.

Quality Improvement and Measurementis taking off in Public Health as well……

State health departments have formed the same kind of learning collaborative as clinical facilities do to improve healthcare.

Within Indian Health Care:The Initiatives that Surround Us
• GPRA, EO, Meaningful Use, and other CRS Adventures.
• Special Diabetes Program for Indians
• Improving Patient Care Initiative
• Patient Safety
• Ongoing Injury Surveillance
• Other, Other, Other, and Other.

The 4 Contexts
ContinuousQuality Improvement
PublicAccountability
Quality Surveillance
Evaluation
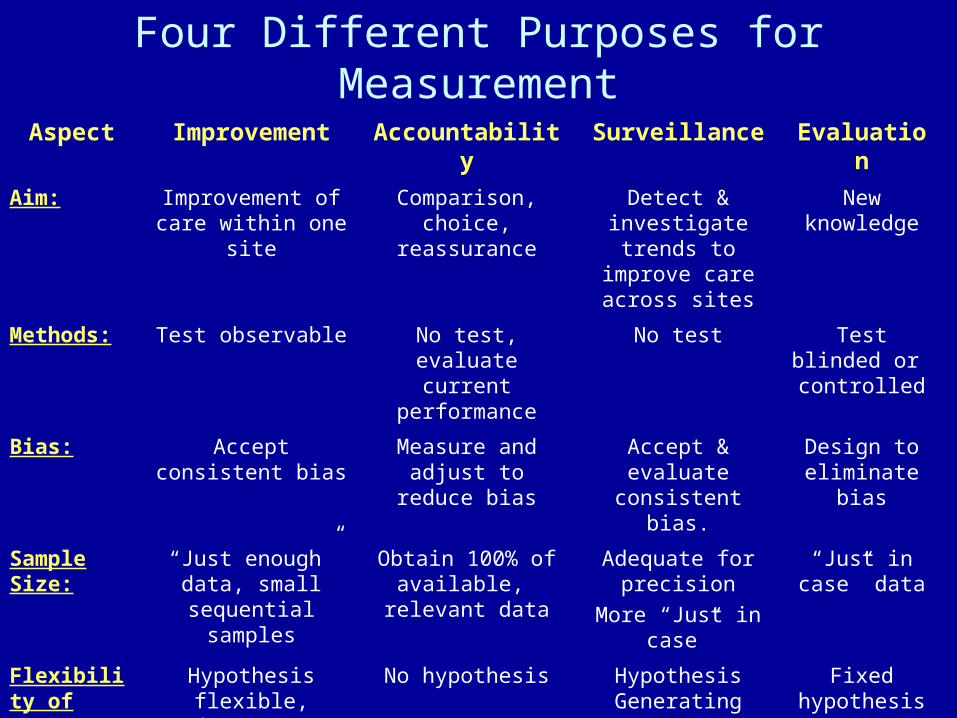
Four Different Purposes for Measurement
Aspect Improvement Accountability Surveillance Evaluation
Aim: Improvement of care within one site
Comparison, choice, reassurance
Detect & investigate trends to improve care
across sites
New knowledge
Methods: Test observable No test, evaluate current performance
No test Test blinded or controlled
Bias: Accept consistent bias
Measure and adjust to reduce bias
Accept & evaluate consistent bias.
Design to eliminate bias
Sample Size:
“Just enough” data, small sequential
samples
Obtain 100% of available, relevant
data
Adequate for precision
More “Just in case”
“Just in case” data
Flexibility of
Hypothesis:
Hypothesis flexible, changes as learning
takes place
No hypothesis Hypothesis Generating
Fixed hypothesis

Four Different Purposes for Measurement (Cont.)
Aspect Improvement Accountability Surveillance Evaluation
Testing Strategy:
Sequential tests No tests No Tests One set of tests
Determining if a Change is anImprovement:
Run charts or Shewhart control
charts
No change focus Trend w/ Confidence
Intervals
Hypothesis, statistical tests (t-
test, F-test, chi square, p-values)
Confidentiality of the Data:
Data used only by those involved with improvement
Data available for public
consumption and review
Individual identities protected
Research subjects’ identities protected
Frequency of Use:
Daily, weekly, monthly
Quarterly, annually
Weekly to annually
At end of project

Improved health and wellness for American Indian and Alaska Native individuals, families, and
communities
Delivery SystemDesign
DecisionSupport
ClinicalInformation
Systems
Self-Management
Support
C ommunity
Health Care Organization
DRAFT IPC Care Model
Activated Family and Community
Informed Activated Patient
Prepared Proactive Care Team
Prepared,Proactive
Community PartnersEFFECTIVE RELATIONSHIPS
EfficientSafe EffectiveEquitable
TimelyPatient-Centered
IPC Care Model

See The Carey and Lloyd RoadmapSPC as a process improvement strategy.

Benchmarks vs. Benchmarking
• Benchmarking—A complete improvement process
“Search for industry best practices that leads to superior performance.” Camp, 1989
1. Measure
2. Identify benchmark performers (companies, clinics)
3. Learn from them.
4. Modify and implement best practices
5. Measure.

Model for Improvement

IHI Breakthrough Series Model
Planning Group
Identify Change
Concepts
Prework
LS 1
P
S
A DP
S
A D
LS 3LS 2
Supports
Email Conference Calls Assessments Senior Leader Reports Site Visits Listserv
Time for setting aims, allocating resources, preparing baseline data leading to the first two-day
meeting.
Action Period 1: Adapt and test the ideas for
improved system of care
Action Period 2: Further develop the system of care at the pilot site and spread the system to other
sites and/or practitioners
Harvesting and Spread
Expert Panel

The Triple Aim
“improving the experience of care, improving
the health of populations, and reducing per capita costs of health care”
Don Berwick- Health Affairs, 2008