wic female parents' behavior and attitudes toward their children's food intake —...
TRANSCRIPT

RESEARCH ARTICLE
WIC Female Parents' Behavior and Attitudes Toward Their Children's Food Intake -
Relationship to Children's Relative Weight
JANET SELL SEAGREN AND RHONDA DALE TERRY
Department of Food Science and Human Nutrition, Iowa State University, Ames, Iowa 500ll
ABSTRACT This study measured female parents' self-reported behavior and attitudes toward selected parent-child food intake interactions, and compared these behaviors and attitudes between female parents of normal weight and obese children. Questionnaires were completed by predominantly white female parents of 130 normal weight and 48 obese threeand four-year old children enrolled in four Iowa WIC programs. Data collected included descriptive characteristics, the female parent's self-reported behavior regarding control of the child's food behavior, and attitudes toward both satisfaction with the child's food behavior and the degree to which she felt her food behavior influenced that of her child. Several significant differences between the two groups were found. Female parents of obese children tended to exercise less control over and to be more dissatisfied with the type of foods their children ate. In addition, these female parents seemed more dissatisfied with the amount of food their children consumed between meals. It appeared that obese children were encouraged less often to eat all the food on their plate and were allowed less often to eat as much food as they would like. Normal weight children tended to be offered sweets only after eating a good meal more often than obese children. Female parents of normal weight children appeared more likely than those of obese children to feel their children played too much while eating.
UNE 23:223-230, 1991)
INTRODUCTION
The prevalence of obesity among America's children appears to be increasing (1). This trend is of concern to health and nutrition professionals, since childhood obesity has been documented as increasing a child's risk for adverse physical and psychological health consequences, as reviewed by Gortmaker et al. (1) and Counts et al. (2). While many factors have been implicated as contributing to childhood obesity, increasing attention has been directed toward the influence of behavioral inter-
Address for correspondence: Rhonda Dale Terry, Ph.D., R.D., Department of Food Science and Human Nutrition, 107 MacKay Hall, Iowa State University, Ames, IA 50011-1120; (515) 294-7316 or 294-4436. 0022-3182/9112305-0223$03.00/0 © 1991 SOCIETY FOR NUTRITION EDUCATION
223
actions between parents and their children regarding food intake. The most direct support for the influence of such interactions is provided by observational studies. For example, when compared with parents of average weight children, parents of obese children have been observed to give their children more prompts to eat (3, 4) but less approval and guidance during mealtime (5). Satter, in publications for both professional (6) and lay audiences (7, 8), has described feeding interactions between parents and their children that may promote childhood obesity.
Obesity is the most prevalent nutrition risk factor among certain groups of children participating in the Special Supplemental Food Program for Women, Infants, and Children (WIC) (9). Since parent-child feeding interactions may promote this problem, an assessment of the prevalence of obesity-potentiating behaviors and attitudes among parents of these children would allow for the development of appropriate nutrition education interventions. Therefore, the purpose of this study was to measure WIC female parents' self-reported behaviors and attitudes toward selected parent-child food intake interactions, and to compare these behaviors and attitudes between female parents of normal weight and obese children.
METHODS
Instrument development. The research instrument, a questionnaire, was designed during the first phase of the study. The behavioral and attitudinal statements in the questionnaire were developed from a table of specifications organized into major parent-child feeding interactions thought to influence a child's relative weight (3-8, 10). In addition, in order to ensure that the statements were relevant to the research population, the senior author spent time as an observer in a WIC clinic and interviewed WIC personnel prior to developing the items.
The questionnaire included three sections. In the first
224 Seagren & Terry / WIC MOTHERS' ATTITUDES
section, the respondent was asked to respond to 15 behavioral items that addressed the degree to which the female parent controlled her child's food behavior. Responses to these items indicated a degree of permissiveness or regulation of the female parent toward the child's food behavior. Items addressed the time, frequency, amount, and type of food eaten, the location within the home where eating occurs, the type of nonfood activities the child engages in while eating, and the use of food as a reward. A five-point response scale ranging from "always" to "never" was used to indicate the frequency with which the behavior stated in each item was controlled by the female parent.
Fifteen attitudinal items developed using Sims' (11) concept of attitudes were included in section II. Ten of these attitudinal items measured the degree to which the female parent was satisfied with the child's food behavior with regard to the time, frequency, amount, and type of food eaten, the location within the home where eating occurs, and the type of nonfood activities the child engages in while eating. The remaining five attitudinal items measured the degree to which the female parent felt her food behavior influenced that of her child. A fivepoint Likert-type response scale ranging from strongly agree to strongly disagree was used for these items.
The last section of the questionnaire elicited demographic and descriptive characteristics. These included the age of the respondent, employment status outside of the home, level of education completed, race, size of the household, number of individuals in the household under age 18, and the respondent's perception of her child's weight.
The instrument was reviewed by nine professionals. These reviewers were selected based on three criteria: experience with young children, knowledge of the research subject matter, and familiarity with the WIC program and clientele. The reviewers included child psychologists, nutrition education experts, and WIC dietitians. To establish content validity, these professionals reviewed the statements organized within the table of specifications to ensure the congruence between each item and the parent-child interaction it was intended to measure (12). Based on these reviews, minor modifications were made prior to pilot testing the instrument. It was administered to seven female parents who met the subject selection criteria but were not participating in a WIC program later included in the study. Pilot testing established that both the directions and items were clear and easy for subjects to respond to (13).
Data collection. Of the 22 WIC agencies in the state, subjects were drawn from the four that had the highest prevalence rates of obesity among participating children during 1987. Of 16,733 three- and four-year old children examined in the state's WIC agencies in 1987, 7.2% were
obese. Obesity rates for the four agencies chosen for this study averaged 9.6%.
Weight-for-height percentiles (14) were used to establish normal weight and obese categories. This classification is used by WIC, and defines normal weight as weight-for-height percentiles > 25th but :5 75th and obesity as > 95th weight-for-height percentile. In order to identify normal weight and obese children eligible to participate in this study, a computerized list of all threeand four-year old children from the four WIC agencies was obtained from the WIC state office. Information obtained from these records included each child's sex, birthdate, height, weight, and the date on which anthropometric measurements were taken. From these data, weight-for-height, weight-for-age, and height-for-age percentile groups were determined for all children between 36 and 59 months of age (14). One hundred eightyfour individuals in the normal weight category were randomly selected from a list of 1,059 potential study participants. Conversely, due to a small potential sample size, all 72 children in the obese weight category were identified as potential participants. Fifty-nine percent of the three- and four-year old children from these agencies had weight-for-height percentiles falling outside the normal weight and obese classifications and were not eligible to participate in this study. Those having weight-forheight percentiles :5 25th were 15.5% of the children, while 43.5% were> 75th but :5 95th.
N either the length of time individuals had participated in WIC nor the specific reasons for WIC eligibility were addressed or identified in this sample. A child up to age five may have been eligible for WIC when the household annual income was below 185% of current poverty guidelines and the child had been identified as at nutritional risk by a health professional. Criteria for establishing nutritional risk in children were based on height and weight parameters, hematocrit levels, and health and dietary assessments (15). Because criteria for being considered at nutritional risk vary, there may have been nutritional and/or physiological differences between the two weight-for-height percentile groups of children (>25th but :575th, and >95th) that were not identified.
The mother or female guardian of each identified child, referred to in this paper as the female parent, was asked to complete the questionnaire during a regular WIC clinic visit. She was also asked to sign an informed consent form allowing information about her child to be used in this research. The data collection period lasted one month. Of the 256 eligible female parents to whom questionnaires were given, the questionnaires were filled out by 191, giving a response rate of 75%. Thirteen of these questionnaires were eliminated due to extensive missing data. Questionnaires were either not filled out or were eliminated for 33% of the individuals selected to participate from the obese weight category, compared with 29% from the normal weight category.

J. of Nutr. Educ. Vol. 23, No.5
Data analysis. Statistical procedures were carried out using a packaged computer program (16). Frequencies and percentages were calculated for all variables. Overall mean scores were computed for the one set of behavioral and the two sets of attitudinal items. For example, for each of the 15 behavioral items, the five responses on the response scale were coded, after reversing the response scale for negatively stated items, such that "always" = 5 to "never" = 1. Next, the numerical value of each female parent's responses was summed. The sum was then divided by either 15 or, if the respondent did not answer all 15 items, by the number of items answered. The same procedure was used for calculating a score for the ten attitudinal items t}lat measured the female parent's satisfaction with her child's food behavior, and for calculating a score for the five attitudinal items that measured the degree to which the female parent felt her food behavior influenced that of her child. After reversing negatively stated items, the response scale for attitudinal items was coded such that 5 = "strongly agree" to 1 = "strongly disagree." These scores represent a relative ranking of individual's responses to groups of items.
Significant differences between groups of variables were investigated using t-tests and chi-square tests, and Spearman's correlation coefficients were computed to determine correlations. Cronbach's alpha was computed to determine reliability. The level of statistical significance was set at p :S 0.05.
RESULTS AND DISCUSSION
Description of respondents and children. The ages of the 178 female parents responding to the questionnaire ranged from 18 to 67 years, with 40.2% between 25 and 30 years of age. A majority of the female parents did not work outside of the home (62.4%), and over half (51.1 %) had received a high school diploma. Most were Caucasian (98.9%), were from households of four to five persons (54.0%), and had one or two children under the age of 18 living in the household (52.3%).
There was a good representation of both three- and four-year old children in this study. Three-year olds comprised 54.5% of the sample, while the remaining 45.5% were four-year oIds. Although both sexes were represented in the sample, males predominated at 58.4%. A majority of the children were in the normal weight category (73.0%) as defined by their weight-for-height percentiles. The remaining 27.0% were in the obese category.
Statistically significant correlations were found between several demographic and descriptive characteristics. Older children tended to be heavier, as defined by their weight-for-height and weight-for-age percentile categories (r= .23, p :S .001; r= .26, p :S .001). In ad-
October 1991 225
dition, it appeared that heavier children, as defined by their weight-for-height and weight-for-age categories, were more likely than lighter weight children to be perceived as overweight by their female parents (r= .53, p :S .001; r= .50, p :S .001). No statistically significant differences were found between the demographic characteristics of female parents of normal weight and obese children.
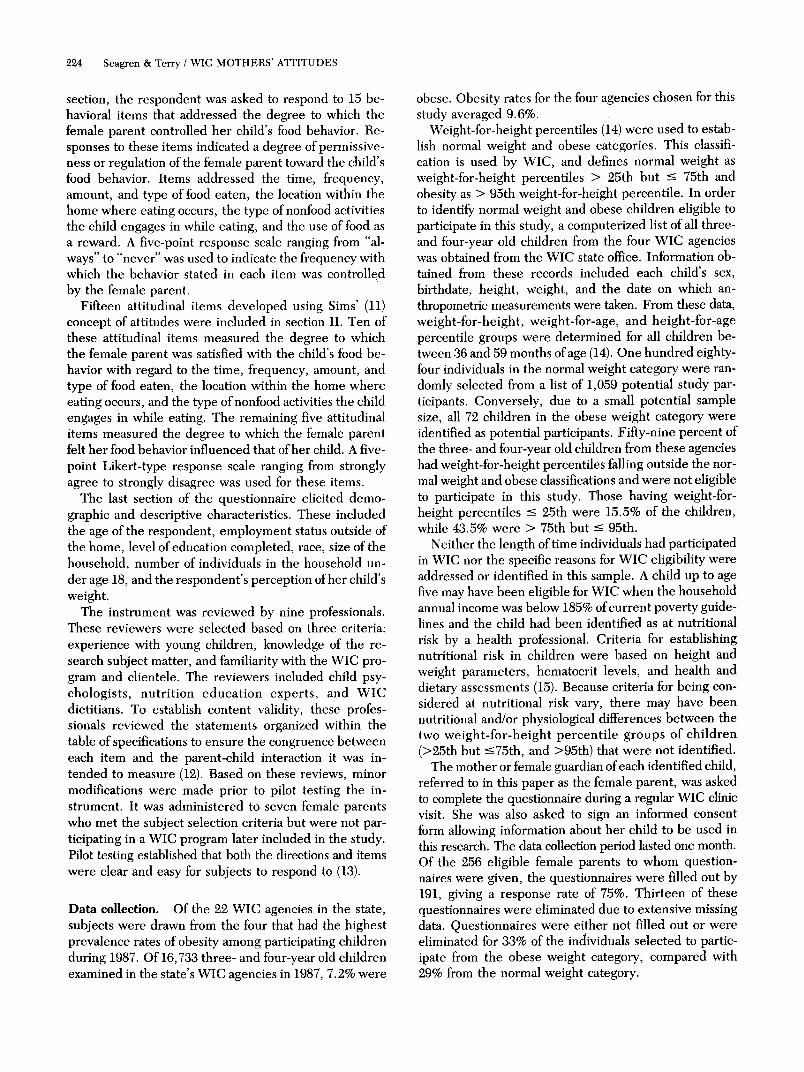
Female parents' reported control of their children's food behavior. Responses to items on the questionnaire that dealt with the frequency with which the female parent controlled the child's food behavior are shown in Table 1. Responses indicate that many female parents frequently controlled the time, frequency, and type offood eaten by their children. On the other hand, most of the female parents in this study frequently did not seem to control the amount of food eaten by their children, with the exception that many of these children were often encouraged to clean their plates at meals. Control over the location of children's eating within the home and their involvement in selected activities, such as playing with toys or watching TV while eating meals, was often maintained by many of these female parents. However, control seemed to be exerted less frequently over snacking while watching TV.
Although the children's food preferences were reportedly often considered by most respondents in making food selections in the grocery store, most of these female parents reported that food purchases were seldom or never influenced by their children's misbehavior in the grocery store. However, misbehavior was not specifically defined for the respondents. Although a majority of the respondents indicated that they seldom or never promised a favorite food to get their children to behave, they did tend to offer sweets more frequently to their children when the children had eaten a "good" meal.
Statistically significant differences were found in responses to four of the 15 items between female parents of normal weight and obese children. Female parents of obese children seemed to control the type of food they allowed their children to eat for snacks less frequently than did the female parents of normal weight children (p :S .05). Although the specific types offoods children consumed were not examined, it is possible that the reported lesser degree of control that female parents of obese children exerted over the type of snack foods their children consumed could be a contributing factor to their obesity.
Female parents of normal weight children tended to allow their children to have sweets only after having eaten a good meal more often than did female parents of obese children (p :S .05). This finding is supportive of other research on parental attitudes toward the use of food as a reward (17). Female parents of obese children were less likely to encourage their children to eat all of
226 Seagren & Terry I WIC MOTHERS' ATTITUDES
Table 1. Female parents' self-reported control of their children's food behavior (n = 178).
Percent
Most of About half Attribute and item Always the time the time Seldom Never
Time/frequency meals and snacks are eaten I allow my child to eat snacks 1.7 9.6 32.0 47.8 9.0
whenever he/she wants to. I allow my child to eat meals 1.7 3.9 7.9 42.1 44.4
whenever he/she wants to
Types of food eaten for meals and snacks There are some foods that I do 30.3 30.3 15.7 17.4 5.1
not allow my child to eat for snacks.-
For meals, I fix only the foods I 2.8 14.6 40.4 25.3 16.3 know my child likes
If my child does not like what I 3.9 9.0 16.3 38.2 32.0 have fixed for a meal, I give him/her something else to eat.
Amount of food eaten for meals and snacks I encourage my child to eat more 4.5 2.8 12.4 36.0 44.4
than he/she seems to want. I encourage my child to eat all 43.3 32.0 10.7 7.3 6.2
the food on his/her plate at meals.-
I allow my child to eat as much 29.8 36.0 16.3 14.6 2.8 food as he/she would like.-
Designated areas for eating meals and snacks within the home
I allow my child to eat meals in 56.7 24.2 6.2 6.7 5.1 only one or two places in our home.
I allow my child to eat snacks 2.2 8.4 13.5 36.0 39.3 anywhere he/she wants to in our home.
Nonfood activities occurring while eating meals and snacks
I allow my child to play with toys 0.6 1.1 1.1 6.7 89.9 while eating meals.
I allow my child to eat meals 2.2 6.2 18.0 38.8 33.7 while watching TV.
I allow my child to eat snacks 3.4 14.6 34.3 34.3 12.4 while watching TV.
Types of food purchased When my child misbehaves in 0.6 0.6 1.1 23.0 74.7
the grocery store, I am forced to buy certain foods he/she wants.
In the grocery store, I buy mostly 4.5 19.7 44.4 21.3 10.1 foods I know my child likes.
Food as a reward To get my child to behave, I 0.0 2.2 9.6 39.9 47.8
promise him/her a favorite food.
I allow my child to have sweets 15.2 24.2 27.0 24.7 8.4 only if he/she has eaten a good meaL-
_ Responses were significantly different for female parents of normal weight children and female parents of obese children.
the food on their plate (p :'5 .01) or to eat as much food they would like (p :'5 .001). Two interpretations of these data are possible. First, these findings may suggest that female parents of obese children felt their children ate
adequate amounts of food, and consequently they did not feel the need to encourage them to eat more. However, observational studies have found that parents of obese children give more prompts to eat than those of
J. of Nutr. Educ. Vol. 23, No.5 October 1991 227
Table 2. Female parents' satisfaction with their children's food behavior (n = 178).
Percent
Strongly Strongly Attribute and item agree Agree Neutral Disagree disagree
Time/frequency food is eaten I think my child should eat on a 8.4 26.4 32.0 21.3 10.1
more regular schedule. I think my child should not eat 15.2 47.2 23.0 12.9 1.7
so often between meals. Type of food eaten
I am satisfied with the kinds of 18.5 56.2 20.2 3.9 0.0 food my child eats for snacks.·
I am satisfied with the kinds of 32.0 52.8 11.2 3.4 0.0 food my child eats for meals.·
Amount of food eaten I think my child eats too much 1.7 10.7 20.8 59.6 6.2
food between meals.· I think my child does not eat 3.9 14.6 27.0 41.6 11.8
enough food at meals. I think my child eats about the 14.6 59.0 15.7 8.4 1.7
right amount of food. Location of eating
I think my child eats in too many 0.6 4.5 9.0 55.1 30.3 places in our home.
Activities involved in while eating I think my child should watch TV 11.8 24.7 22.5 19.1 19.1
less while eating I think my child should play less 23.0 21.9 23.0 15.2 12.4
while eating.·
• Responses were significantly different for female parents of normal weight children and female parents of obese children.
thin children (3, 4). An alternative interpretation is that some female parents of obese children may have been trying to restrict their children's eating as a means of weight control.
A mean control score was calculated from responses to all items dealing with female parental control of the child's food behavior. The possible range for this score was 1.00 to 5.00, with a higher score representing more frequent reported control and, therefore, greater parental regulation of the child's food behavior. A negative correlation was found between the control score and the number of hours the respondent worked outside of the home each week (r= - .14, p::; .05). Females who worked a greater number of hours outside the home tended to exert less control over their children's food behavior. Other statistical relationships between demographic characteristics and this score were not significant.
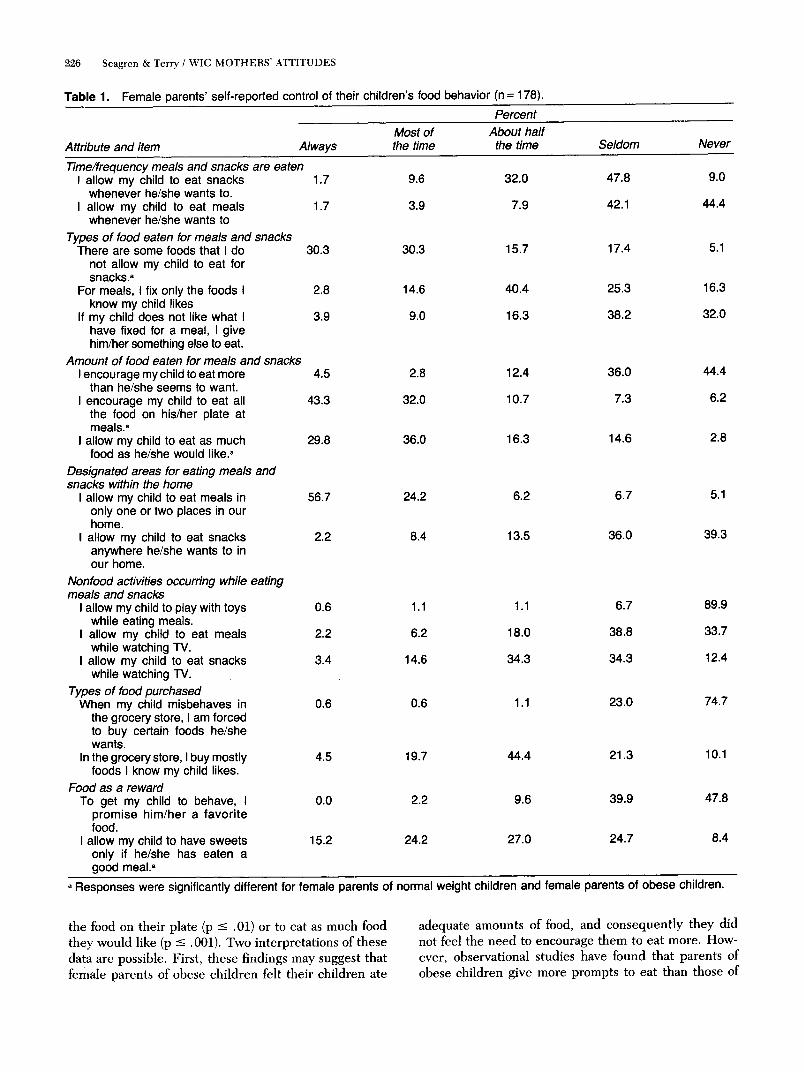
Female parent's satisfaction with their children's food behavior. Responses to attitudinal items that dealt with the female parent's satisfaction with her child's food behavior are shown in Table 2. For the purpose of discussion, responses of strongly agree and agree are collectively referred to as agree, while responses of strongly disagree and disagree are referred to as disagree. Several of the female parents were dissatisfied with the frequency with which their children ate. A comparatively greater
percentage of female parents appeared to be satisfied with the types of food eaten by the children, especially for meals. In addition, most of the female parents expressed satisfaction with the amount of food consumed by their children, as well as the location within the home where eating occurred. In regard to activities children were involved in while eating, many of the female parents in this sample felt their children should play less while eating.
Significant differences were found between female parents of obese and normal weight children for four of the ten items on satisfaction with their children's food behavior. Female parents of obese children tended to be more dissatisfied with the types of food their children ate for meals and snacks than were female parents of normal weight children (p ::; .05; p ::; .05). Female parents of obese children were also more likely to agree that their children ate too much food between meals (p ::; .001) but less likely to agree that their children should play less while eating (p ::; .05). This latter finding is supported by other research that found thinner children spending more time playing with food, hesitating more between bites, and leaving significantly more food on the plate than heavier children (18).
A total satisfaction score was calculated for all items dealing with female parental satisfaction with the child's food behavior. This score ranged from 1.00 to 5.00, and

228 Seagren & Terry / WIC MOTHERS' ATTITUDES
Table 3. Female parents' attitudes toward the influence of their food behavior on their children's food behavior (n = 178).
Strongly Attribute and item agree
Influence on time/frequency food is eaten The time I eat influences the time my 18.0
child wants to eat.
Influence on type of food eaten My food likes and dislikes influence the 16.9
foods my child likes and dislikes
Influence on amount of food eaten The amount of food I eat influences the 6.2
amount my child wants to eat.
Influence on location of eating in the home Where I eat in our home influences where 25.8
my child wants to eat.
Influence on involvement in other activities while eating
If I watch TV while eating, it influences 2.7 my child to do the same.
a higher score indicated greater satisfaction with children's food behavior. Significant relationships were not found between demographic characteristics and this score. However, the correlation between the satisfaction score and the control score was significant (r = .22, p ::; .001). The reliability coefficient for this group of items was a = 0.61, approaching the guideline of 0.65 suggested by Mehrens and Lehmann (12),
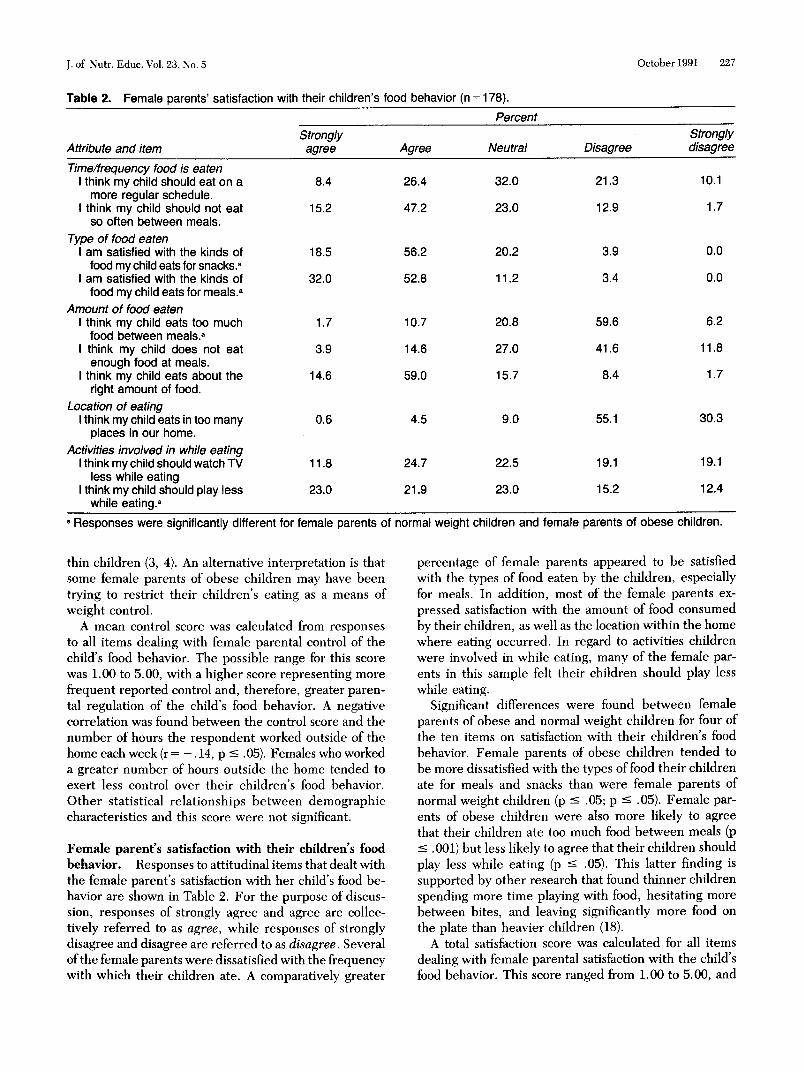
Female parents' attitudes toward the influence of their food behavior on their children's food behavior. Responses to items that dealt with the degree to which the female parent felt her food behavior influenced that of her child are shown in Table 3. In this study, many of the respondents agreed that their children's food behavior was influenced by their own food behavior with regard to time of eating, types of food liked or disliked, places where eating occurs in the home, and watching television while eating. However, few female parents agreed that the amount of food they ate influenced the amount their children ate. Conflicting results have been reported by other researchers regarding parental influence on children's food preferences and behavior. For example, in a food preference study of preschool children and their parents, a significant relationship was not found between stated food preferences of the children and those of their parents (19). On the other hand, Hertzler found, through a review of literature, that several investigators supported the theory that parental food behavior influences that of their children (20). In this study, the perceived influence of male parents' food behaviors on that of their children was not addressed. Although the influence of mothers vs, fathers in the formation of children's food preferences was not found to be significantly different in one study (21), further research on the influence
Percent Strongly
Agree Neutral Disagree disagree
52.8 17.4 9.0 2.8
39.3 15.7 22.5 5.1
24.7 22.5 36.5 9.0
58.4 7.3 6.7 0.6
55.6 6.7 7.9 1.1
of male parents' food behavior on that of their children would be beneficial.
Statistically significant differences in responses to individual items about influence were not found between female parents of obese and normal weight children. A total influence score was calculated for all items dealing with attitudes toward female parental influence on the child's food behavior, with a possible range of 1.00 to 5.00, and a higher score representing greater perceived influence. A significant negative correlation was found between the number of hours the respondent worked outside the home each week and the influence score (r = - .13, p ::; .05). Therefore, female parents in this sample seemed to feel their food behavior had less influence on their children's food behavior as the amount of time spent working outside the home increased. The influence score was not significantly correlated with either the control score or the satisfaction score. The reliability coefficient for this group of items was a = 0.69, a level considered acceptable for research items (12).
CONCLUSIONS
The results from this study of a predominantly white, Midwestern sample cannot be generalized to all American children. However, several preliminary conclusions can be drawn. First, the self-reported behaviors and attitudes toward parent-child feeding interactions gathered in this study have not previously been reported in the literature, The questionnaire designed to gather these data appeared easy for subjects to respond to, as determined through pilot testing, and revealed a range of responses for items, Whether self-reported behaviors reflect actual or desired behavior is unknown when using

J. of Nutr. Educ. Vol. 23, No.5
a questionnaire. Therefore, validity studies that compare parents' observed behavior with self-reported behavior on a questionnaire such as this would be desirable. If parent-child interactions are believed to be influential in the development of children's food behaviors, a valid, reliable instrument similar to the questionnaire used in this study would be useful to diet counselors for general pediatric clinic screening.
The data from this sample revealed a range of behaviors and attitudes toward parent-child feeding interactions for both female parents of normal weight and obese children. Therefore, it appears that education on appropriate parent-child feeding interactions, such as that described in the literature (5-8, 17, 19, 20), is desirable for all female parents in the population from which this sample was drawn, not just female parents of obese children. Furthermore, this sample represented only low income female parents, predominantly from the Caucasian race. Further research is needed with other caretakers such as fathers, and other socioeconomic groups, geographic regions, and racial groups. These data would facilitate nutrition education on appropriate parent-child feeding interactions.
In this study, many variables potentially related to parent-child feeding interactions and relative weight were not studied, such as parents' weights. For example, several studies indicate that both genetics and learned behavior are important predictors of obesity among family members (22). In addition, nutrition knowledge, dietary intake, single-parent vs. dual-parent family interactions, and two-way interaction between parent and child were not measured. It is quite possible that these factors influenced the responses of these females. D
ACKNOWLEDGMENTS
The authors express appreciation to the Iowa WIC staff who contributed to the data collection for this project.
This study was submitted as a thesis by Janet Sell Seagren in partial fulfillment of the requirements for the Master of Science degree.
NOTES AND REFERENCES
1 Gortmaker, S.L., W.H. Dietz, A.M. Sobol, and C.A. Wehler. Increasing pediatric obeSity in the United States. AmericanJournal of Diseases of Children 141:535-540, 1987.
2 Counts, C.R, c. Jones, C.L. Frame, G.J. Jamie, and C.C. Strauss. The perception of obeSity by normal-weight versus obese schoolage children. Child Psychology and Human Development 17:113-120, 1986.
3 Klesges, RC., T.J. Coates, G. Brown, J. Sturgeon-Tillisch, L.M. Moldenhauer-Klesges, B. Holzer, J. Woolfrey, and J. Volimer. Parental influences on children's eating behavior and relative weight. Journal of Applied Behavior Analysis 16:371-378, 1983.
4 Klesges, RC., J.M. Malott, P.F. Boschee, and J.M. Weber. The effects of parental influences on children's food intake, physical activity, and relative weight. International Journal of Eating Disorders 5:335-345, 1986.
October 1991 229
5 Birch, L.L., D.W. Marlin, L. Kramer, and C. Peyer. Mother-child interaction patterns and the degree of fatness in children. Journal of Nutrition Education 13:17-21, 1981.
6 Satter, E. The feeding relationship. Journal of the American Dietetic Association 86:352-356, 1986.
7 Satter, E. Child of mine-feeding with love and good sense. Palo Alto, California: Bull Publishing Company, 1983.
8 Satter, E. How to get your kid to eat . .. but not too much. Palo Alto, California: Bull Publishing Company, 1987.
9 Dobson, B. Personal communication. Nutrition Education Coordinator, Nutrition Division, Iowa Department of Public Health, Des Moines, Iowa.
10 A copy of the table of specifications and instrument may be obtained from R.D. Terry, 107 MacKay Hall, Iowa State University, Ames, IA 50011.
11 Sims, L. S. Toward an understanding of attitude assessment in nutrition research. Journal of the American Dietetic Association 78:460-466, 1981.
12 Mehrens, W.A. and I.J. Lehmann. Measurement and evaluation in education and psychology, 2nd edition. New York: Holt, Rinehart, and Winston, 1978.
13 The Iowa State University Committee on the Use of Human Subjects in Research approved the instrument and research procedures.
14 Hammill, P.V., T.A. Drizd, C.L. Johnson, RB. Reed, A.F. Roche, and W.M. Moore. Physical growth: National Center for Health Statistics percentiles. The American Journal of Clinical Nutrition 32:607-629, 1979.
15 Iowa Department of Health. What health care professionals need to know about the Supplemental Food Program for Women, Infants, and Children. No. PR7124. Des Moines: Iowa Department of Health, 1989.
16 SPSS Inc. SPSSx user's guide. Chicago: McGraw Hill, 1983. 17 Patterson, R.E., J.T. Typpo, and G.F. Krause. Factors related to
obesity in preschool children. Journal of the American Dietetic Association 86:1376--1381, 1986.
18 Marston, A.R., P. London, and L.M. Cooper. A note on the eating behavior of children varying in weight. Journal of Child Psychology and Psychiatry 17:221-224, 1976.
19 Birch, L.L. The relationship between children's food preferences and those of their parents. Journal of Nutrition Education 12:14-18, 1980.
20 Hertzler, A.A. Children's food patterns-a review: II. Family and group behavior. Journal of the American Dietetic Association 83:555-560, 1983.
21 Burt, J. V. and A.A. Hertzler. Parental influences on the child's food preference. Journal of Nutrition Education 10:127-128,1978.
22 Garn, S.M., M. LaVelle, and J.J. Pilkington. Obesity and living together. Marriage and Family Review 7:33-47, 1984.
RESUME Cette etude a compare Ie comportement et les attitudes envers des interactions parent-enfant concernant la consommation alimentaire, entre les parents d'enfants de poids normal et d'enfants obeses. Ces donnees ont ete obtenues it partir d'un questionnaire rempli par des parents feminins principalement de race blanche dont les enfants de trois et quatre ans etaient inscrits dans quatre programmes WIC de l'Iowa. Cent trente (130) enfants etaient de poids normal et 48 etaient obeses. Les donnees recueillies comprenaient des caracteristiques descriptives, Ie rapport fait par Ie parent du controle exerce sur Ie comportement alimentaire de l'enfant, et les attitudes quant it la satisfaction envers ce comportement et quant it !'influence percue sur ce comportement. Plusieurs differences significatives ont ete observees entre les deux groupes. Les parents d' enfants obeses tendaient it exercer moins de controle sur Ie genre d'aliments consommes et etaient plus insatisfaits de l'alimentation de leurs enfants. De plus, ces parents semblaient plus insatisfaits de la quantite d'aliments que leurs enfants consommaient entre les repas. On a constate que les enfants obeses etaient moins souvent encourages a "finir leur assiette" et etaient moins souvent autorises it manger autant

230 Seagren & Terry / WIC MOTHERS' ATTITUDES
que bon leur semble. Les enfants de poids normal tendaient plus sou vent que les enfants obeses a se voir offrir des sucreries seulement apres avoir pris un bon repas. Les parents feminins d'enfants de poids normal semblaient plus enclins a trouver que leurs enfants jouaient trop en mangeant.
IJNE 23:223--230, 1991)
Translated by janine Choquette
RESUMEN En el presente estudio se medieron las practicas y actitudes reportadas por un grupo de madres, hacia una seleccion de interacciones alimentarias entre madre-hijo. Se compararon las practicas y actitudes de un grupo de madres con hijos de peso normal con las de un grupo de madres con hijos obesos. Los cuestionarios fueron completados por un grupo de madres de 130 niiios con peso normal y 48 niiios obesos, la poblacion fue predominantemente de origen Caucasico, con niiios entre 3 y 4 aiios de edad de cuatro programas especiales para mujeres y niiios (WIC) en Iowa. La informacion recabada
incluyo caracteristicas descriptivas del grupo de participantes, reportes de sus conductas (practicas) y actitudes con respecto de la alimentacion, sus actitudes de satisfaccion con las practicas ailmentarias de sus hijos, y con el grado de influencia que elias percibian haber tenido sobre los habitos alimentarios de sus hijos. Varias diferencias significativas entre los grupos de madres fueron observadas Las madres con niiios obesos reportaron un menor control sobre el tipo de alimentos que consumian sus hijos, elias tam bien manifestaron menos satisfaccion con la alimentacion de sus hijos. Asi mismo, estas madres indicaron desatisfaccion con la cantidad de alimentos que los niiios consumian entre comidas. Parece ser que los niiios obesos fueron menos alentados a comer toda su com ida y con menor frecuencia fueron permitidos a comer todo 10 que querian. Las madres de los niiios de peso normal indicaron ofrecer dulces solo despues de la com ida con mayor frecuencia que las de los niiios obesos. Las madres de los niiios con peso normal indicaron sentir que sus hijos jugaban demasiado durante la com ida. IJNE 23:223--230, 1991)
Translated by Maria Teresa Cerqueira
CALCIUM: EFFECT OF DIFFERENT AMOUNTS ON NONHEME-IRON AND HEME-IRON ABSORPTION IN HUMANS
Hallberg et al. investigated the dose-dependent effect of calcium on nonheme-iron and heme-iron absorption in humans (American journal of Clinical Nutrition 53:112-119, 1991). Prior animal studies had concluded that calcium may be detrimental to iron uptake in the intestinal mucosa or may interfere with subsequent transfer of iron into the blood stream.
The dietary effect of calcium on iron absorption was studied utilizing a basal diet, consisting of wheat rolls and butter served with water. The diet contained no known inhibitors or enhancers of iron uptake. In the first series of ten experiments subjects received the basal diet with or without the incorporation of calcium (as calcium chloride) into the rolls before or after baking; all rolls contained nonheme-iron in the form of ferrous sulphate. Subjects in the second set of two experiments were fed the basal diet with or without consumption of dairy products (the calcium source); rolls contained the same amount of ferrous sulphate as the first series. A final trial employed the same regime as the first series, with the addition of hemeiron in the form of a hamburger patty. Nonheme-iron and heme-iron uptakes were measured by absorption of radio-isotopically labeled iron in ferrous sulphate or hemoglobin. This study used 126 people for the 13 trials (10 ± 2 people per trial).
Calcium inhibited iron uptake indirectly by preventing phytate degradation, and directly by impeding iron uptake via intestinal cell receptor inhibition. The study demonstrated inhibition of iron absorption as a function of both calcium level and its point of addition into the foodstuff. Compared with basal calcium intake levels, calcium doses of 40 to 300 mg significantly reduced iron absorption. Inhibition of iron absorption was statistically greater when calcium was added before baking rather than afterwards. Calcium in dairy products significantly decreased nonheme-iron absorption. A significant reduction in heme-iron absorption due to calcium was observed.
These hypothesized indirect and direct mechanisms by which calcium inhibits iron absorption have some important nutritional ramifications. The current trend by physicians and nutritionists to encourage increased calcium intake may inadvertently be increasing the risk of iron deficiency. If this effect of calcium on iron absorption is substantiated, an interesting risklbenefit question arises-Do the benefits of increased calcium intake outweigh the increased risk iron deficiency? More importantly, how can the diet be formulated to allow optimal uptake of both calcium and iron? (29 references)
Summary by Philip j. Baney, IV