workplace safety committee agenda start … · workplace safety committee agenda company name: date...
TRANSCRIPT
WORKPLACE SAFETY COMMITTEE AGENDA
Company Name:
Date of Meeting:
Start Time:
Committee Purpose: To reduce the frequency and severity of work-related injuries and to ensure safety committee certification requirements are met.
1. Reviewed and Posted Minutes from Previous Safety Committee Meeting 2. Read Mission Statement 3. Safety Inspection Walk Through 4. Any Injuries, Accidents, or Near Misses? 5. Review of any Injuries, Accidents or Near Misses 6. Review/Update OSHA 300 Log 7. Review of any Workplace Safety Concerns/Trainings/Inspections 8. Review of any Workplace Safety Accomplishments 9. Health & Safety Topic Checklist 10. Additional Safety Issues
1
WORKPLACE SAFETY COMMITTEE MEETING MINUTES
Company Name:
Date of Meeting:
Members - Present
Members - Absent
2
STATE REQUIREMENTS INCLUDE:
1. Minutes from the previous safety committee meeting were:
Reviewed.Posted for other employees to read.
2. Read the following mission statement:
To eliminate injuries through effective injury prevention education, training and vigilance.
3. The State requires a periodic Safety Inspection Walk-Through. Has one been conducted recently?
Yes No
If you answered "YES", complete the following:
What was the date of the inspection?
Who conducted the inspection?
What location or department of the workplace was inspected?
What safety issues were identified during the inspection?
How were the safety issues addressed?
3
TO REDUCE THE FREQUENCY AND SEVERITY OF WORK-RELATED INJURIES:
4. Any injuries, accidents, or near misses?
Were there any injured employees requiring professional medical attention?
Yes No
If there was an injury, did the injured employee bring the letter to the medical treatment provider detailing what tests needed to be performed and forms needed to be completed?
Yes No Not Applicable
If there was an injury, was a drug & alcohol test completed?
Yes No Not Applicable
If there was an injury, was a Physical Capacities Evaluation form completed by the medical treatment provider?
Yes No Not Applicable
If there was an injury, was an Employee Incident Report completed & signed by a supervisor at the time of the incident?
Yes No Not Applicable
If there was an injury, did the injured employee sign the Notice of Employees' Rights and Duties?
Yes No Not Applicable
Were there any accidents [damage to property or equipment OR employees NOT requiring professional medical attention such as burns, strains/sprains, cuts, bruises, falls or slips]?
Yes No
Were there any near misses? (Ex: Wet, slippery or uneven surfaces; Electrical cords or obstructions in aisles/walkways; Signage (emergency or non-emergency) that was not displayed or lit)
Yes No
5. Review of any injuries, accidents, or near misses:
How did it/they occur? What is being done to reduce the probability it/they will occur in the future?
4
6. Review/Update OSHA 300 Log. Where there any incidents involving any of the following?
Death
Yes No
Days Away from Work
Yes No
Job Transfer or Work Restriction
Yes No
Medical Treatment Beyond First Aid
Yes No
Explain:
7. Review of any workplace trainings, inspections or certifications:
Were there any (1) safety-related trainings, (2) inspections of fire extinguishers or equipment, or (3) certifications for driving vehicles or operating forklifts? Any upcoming trainings, inspections or certifications?
Yes No
Explain:
5
8. Review of any workplace safety accomplishments including training, safety equipment maintenance/purchases, PPE issues, etc.:
Have you purchased any new equipment, materials, or software for your workplace?
Yes No
Have you serviced or cleaned any equipment in the workplace (HVAC, Plumbing, Computer, Mechanical, Tools, Machines, etc)?
Yes No
Have you cleaned or organized your workplace recently?
Yes No
Have you instituted any new policies or procedures designed to keep your workplace safer and or cleaner?
Yes No
Have you posted any new signage in or around your workplace?
Yes No
Have you replaced any lighting in the workplace? Emergency lighting?
Yes No
Are employees wearing the proper personal protective equipment when necessary? (Example: safety glasses, face shields, gloves, boots, etc.)
Yes No
Do you have a safety incentive plan to encourage employees to practice and promote safety in the workplace?
Yes No
Explain:
6
9. Health & Safety Topic: Workplace Self-Inspection See attached Checklist. After reviewing the Checklist, our discussion included: 1. What are our MOST critical areas of concern? 2. What can be done NOW that will reduce potential injury risks? 3. Are there additional concerns that were not addressed in the Checklist?
WORKPLACE SELF-INSPECTION CHECKLIST - the answers to the following questions SHOULD be YES –
1. Do you have an active safety and health program in operation that deals with general safety and health program elements as well as management of hazards specific to your worksite?
Yes No
2. Is one person clearly responsible for the overall activities of the safety and health program?
Yes No
3. Do you have a safety committee or group made up of management and labor representatives that meet regularly and reports in writing on its activities?
Yes No
4. Do you have a working procedure for handling in-house employee complaints regarding safety and health?
Yes No
5. Are you keeping your employees advised of the successful effort and accomplishments you and/or your safety committee have made in assuring they will have a workplace that is safe and healthful?
Yes No
6. Have you considered incentives for employees or workgroups who have excelled in reducing workplace injuries/illnesses?
Yes No
7. Are you assessing the workplace to determine if hazards that require the use of personal protective equipment (for example, head, eye, face, hand, or foot protection) are present or are likely to be present?
Yes No
7
8. If hazards or the likelihood of hazards are found, are you selecting and having affected employees use properly fitted personal protective equipment suitable for protection from these hazards?
Yes No
9. Have the employees been trained on PPE procedures, that is, what PPE is necessary for a job task, when they need it, and how to properly adjust it?
Yes No
10. Are protective goggles or face shields provided and worn where there is any danger or flying particles or corrosive materials?
Yes No
11. Are approved safety glasses required to be worn at all times in areas where there is a risk of eye injuries such as punctures, abrasions, contusions or burns?
Yes No
12. Are employees who need corrective lenses (glasses or contacts) in working environments having harmful exposures, required to wear only approved safety glasses, protective goggles, or use other medically approved precautionary procedures?
Yes No
13. Are protective gloves, aprons, shields, or other means provided and required where employees could be cut or where there is reasonably anticipated exposure to corrosive liquids, chemicals, blood, or other potentially infectious materials? See 29 CRF 1910.1030(b) for the definition of "other potentially infectious materials."
Yes No
14. Are hard hats provided and worn where danger of falling objects exists?
Yes No
15. Are hard hats inspected periodically for damage to the shell and suspension system?
Yes No
16. Is appropriate foot protection required where there is the risk of foot injuries from hot, corrosive, or poisonous substances, falling objects, crushing or penetrating actions?
Yes No
17. Are approved respirators provided for regular or emergency use where needed?
Yes No
18. Is all protective equipment maintained in a sanitary condition and ready for use?
Yes No
8
19. Do you have eye wash facilities and a quick drench shower within the work area where employees are exposed to injurious corrosive materials? Where special equipment is needed for electrical workers, is it available?
Yes No
20. Where food or beverages are consumed on the premises, are they consumed in areas where there is no exposure to toxic material, blood, or other potentially infectious materials?
Yes No
21. Is protection against the effects of occupational noise exposure provided when sound levels exceed those of the OSHA noise standard?
Yes No
22. Are adequate work procedures, protective clothing and equipment provided and used when cleaning up spilled toxic or otherwise hazardous materials or liquids?
Yes No
23. Are there appropriate procedures in place for disposing of or decontaminating personal protective equipment contaminated with, or reasonable anticipated to be contaminated with, blood or other potentially infectious materials?
Yes No
24. Is a documented, functioning housekeeping program in place?
Yes No
25. Are all work sites clean, sanitary, and orderly?
Yes No
9
8 LAS CAÍDAS DESDE ESCALERAS PUEDEN SER MORTALES: ÚSELAS DE FORMA SEGURA
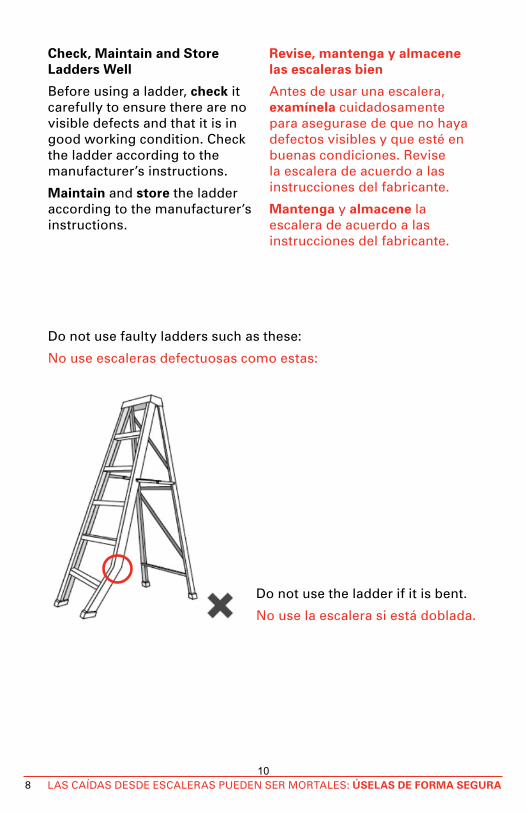
Check, Maintain and Store Ladders Well
Before using a ladder, check it carefully to ensure there are no visible defects and that it is in good working condition. Check the ladder according to the manufacturer’s instructions.
Maintain and store the ladder according to the manufacturer’s instructions.
Revise, mantenga y almacene las escaleras bien
Antes de usar una escalera, examínela cuidadosamente para asegurase de que no haya defectos visibles y que esté en buenas condiciones. Revise la escalera de acuerdo a las instrucciones del fabricante.
Mantenga y almacene la escalera de acuerdo a las instrucciones del fabricante.
Do not use faulty ladders such as these:
No use escaleras defectuosas como estas:
Do not use the ladder if it is bent.
No use la escalera si está doblada.
10
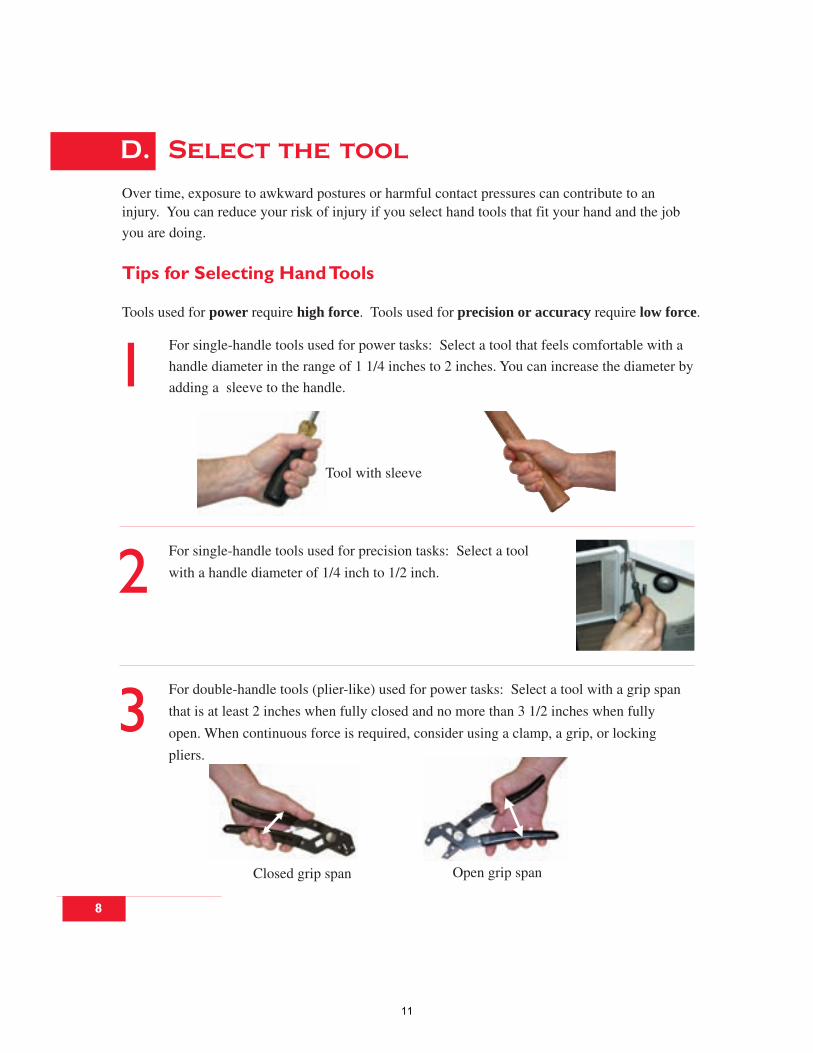
Over time, exposure to awkward postures or harmful contact pressures can contribute to aninjury. You can reduce your risk of injury if you select hand tools that fit your hand and the job
you are doing.
Tips for Selecting Hand Tools
Tools used for power require high force. Tools used for precision or accuracy require low force.
D. Select the tool
Tool with sleeve
For single-handle tools used for precision tasks: Select a tool
with a handle diameter of 1/4 inch to 1/2 inch.
1
2
3
Closed grip span Open grip span
For single-handle tools used for power tasks: Select a tool that feels comfortable with a
handle diameter in the range of 1 1/4 inches to 2 inches. You can increase the diameter by
adding a sleeve to the handle.
For double-handle tools (plier-like) used for power tasks: Select a tool with a grip span
that is at least 2 inches when fully closed and no more than 3 1/2 inches when fully
open. When continuous force is required, consider using a clamp, a grip, or locking
pliers.
8
11
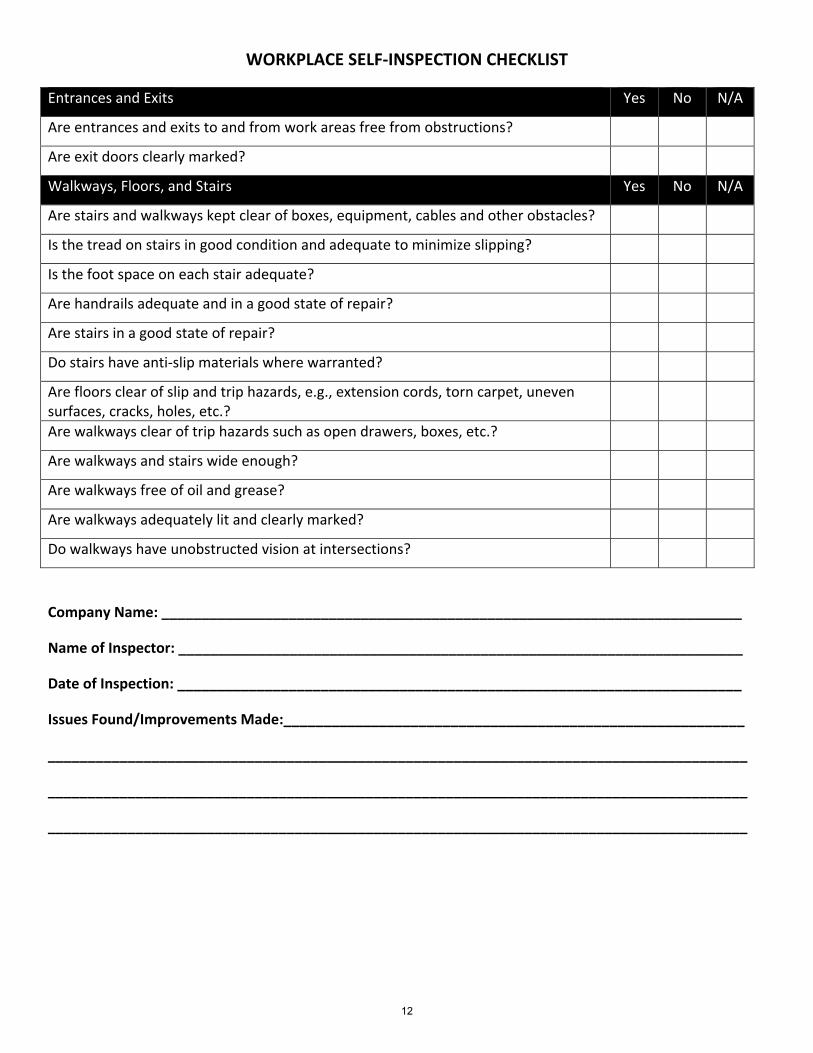
WORKPLACE SELF‐INSPECTION CHECKLIST
Entrances and Exits Yes No N/A
Are entrances and exits to and from work areas free from obstructions?
Are exit doors clearly marked?
Walkways, Floors, and Stairs Yes No N/A
Are stairs and walkways kept clear of boxes, equipment, cables and other obstacles?
Is the tread on stairs in good condition and adequate to minimize slipping?
Is the foot space on each stair adequate?
Are handrails adequate and in a good state of repair?
Are stairs in a good state of repair?
Do stairs have anti‐slip materials where warranted?
Are floors clear of slip and trip hazards, e.g., extension cords, torn carpet, uneven surfaces, cracks, holes, etc.?
Are walkways clear of trip hazards such as open drawers, boxes, etc.?
Are walkways and stairs wide enough?
Are walkways free of oil and grease?
Are walkways adequately lit and clearly marked?
Do walkways have unobstructed vision at intersections?
Company Name: _________________________________________________________________________
Name of Inspector: _______________________________________________________________________
Date of Inspection: _______________________________________________________________________
Issues Found/Improvements Made:__________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
12
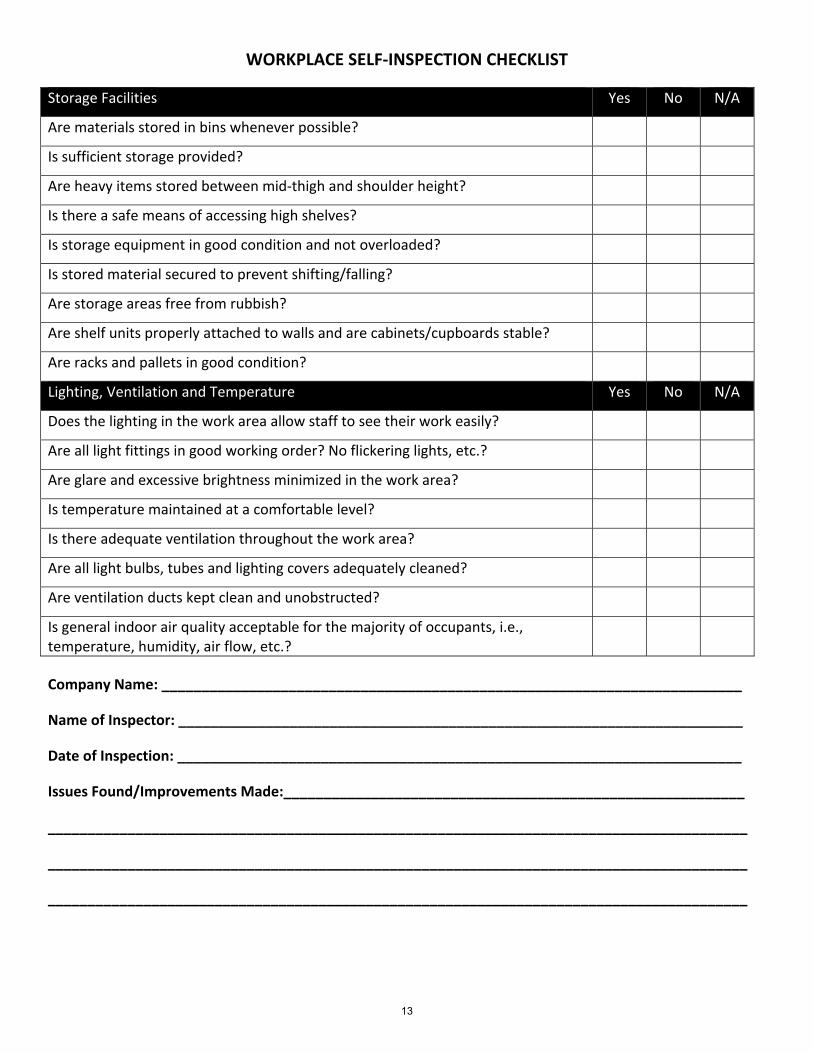
WORKPLACE SELF‐INSPECTION CHECKLIST
Storage Facilities Yes No N/A
Are materials stored in bins whenever possible?
Is sufficient storage provided?
Are heavy items stored between mid‐thigh and shoulder height?
Is there a safe means of accessing high shelves?
Is storage equipment in good condition and not overloaded?
Is stored material secured to prevent shifting/falling?
Are storage areas free from rubbish?
Are shelf units properly attached to walls and are cabinets/cupboards stable?
Are racks and pallets in good condition?
Lighting, Ventilation and Temperature Yes No N/A
Does the lighting in the work area allow staff to see their work easily?
Are all light fittings in good working order? No flickering lights, etc.?
Are glare and excessive brightness minimized in the work area?
Is temperature maintained at a comfortable level?
Is there adequate ventilation throughout the work area?
Are all light bulbs, tubes and lighting covers adequately cleaned?
Are ventilation ducts kept clean and unobstructed?
Is general indoor air quality acceptable for the majority of occupants, i.e., temperature, humidity, air flow, etc.?
Company Name: _________________________________________________________________________
Name of Inspector: _______________________________________________________________________
Date of Inspection: _______________________________________________________________________
Issues Found/Improvements Made:__________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
13
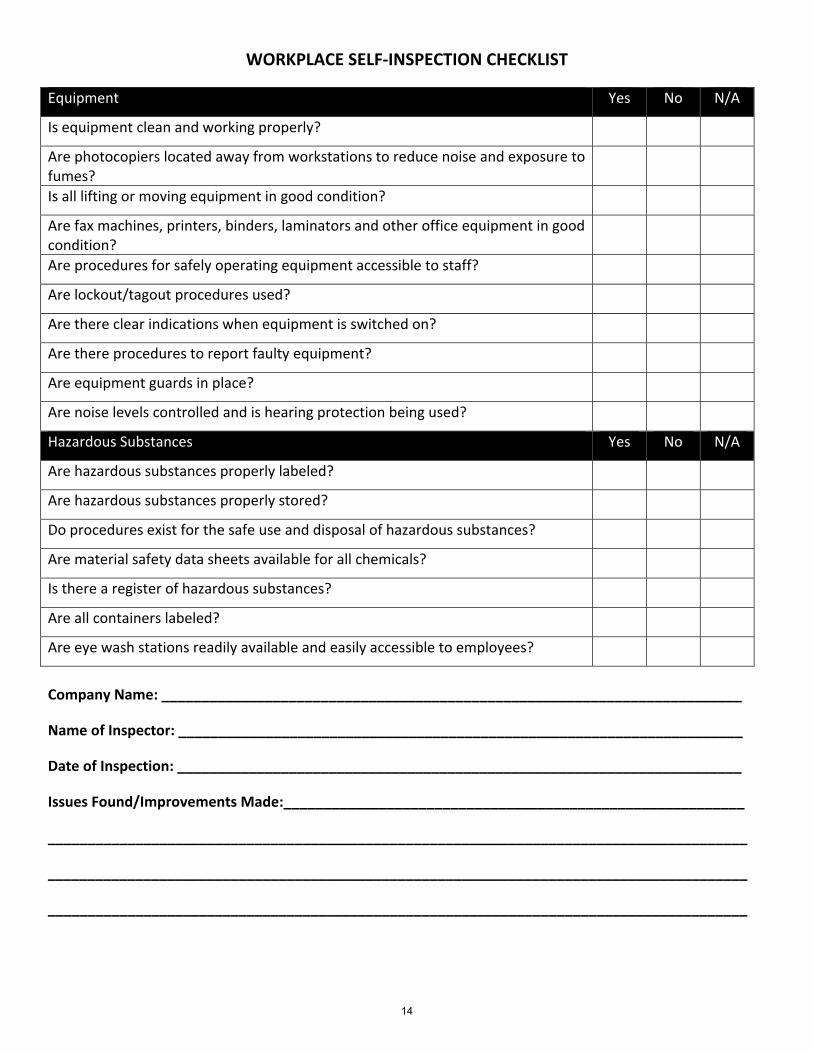
WORKPLACE SELF‐INSPECTION CHECKLIST
Equipment Yes No N/A
Is equipment clean and working properly?
Are photocopiers located away from workstations to reduce noise and exposure to fumes?
Is all lifting or moving equipment in good condition?
Are fax machines, printers, binders, laminators and other office equipment in good condition?
Are procedures for safely operating equipment accessible to staff?
Are lockout/tagout procedures used?
Are there clear indications when equipment is switched on?
Are there procedures to report faulty equipment?
Are equipment guards in place?
Are noise levels controlled and is hearing protection being used?
Hazardous Substances Yes No N/A
Are hazardous substances properly labeled?
Are hazardous substances properly stored?
Do procedures exist for the safe use and disposal of hazardous substances?
Are material safety data sheets available for all chemicals?
Is there a register of hazardous substances?
Are all containers labeled?
Are eye wash stations readily available and easily accessible to employees?
Company Name: _________________________________________________________________________
Name of Inspector: _______________________________________________________________________
Date of Inspection: _______________________________________________________________________
Issues Found/Improvements Made:__________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
14
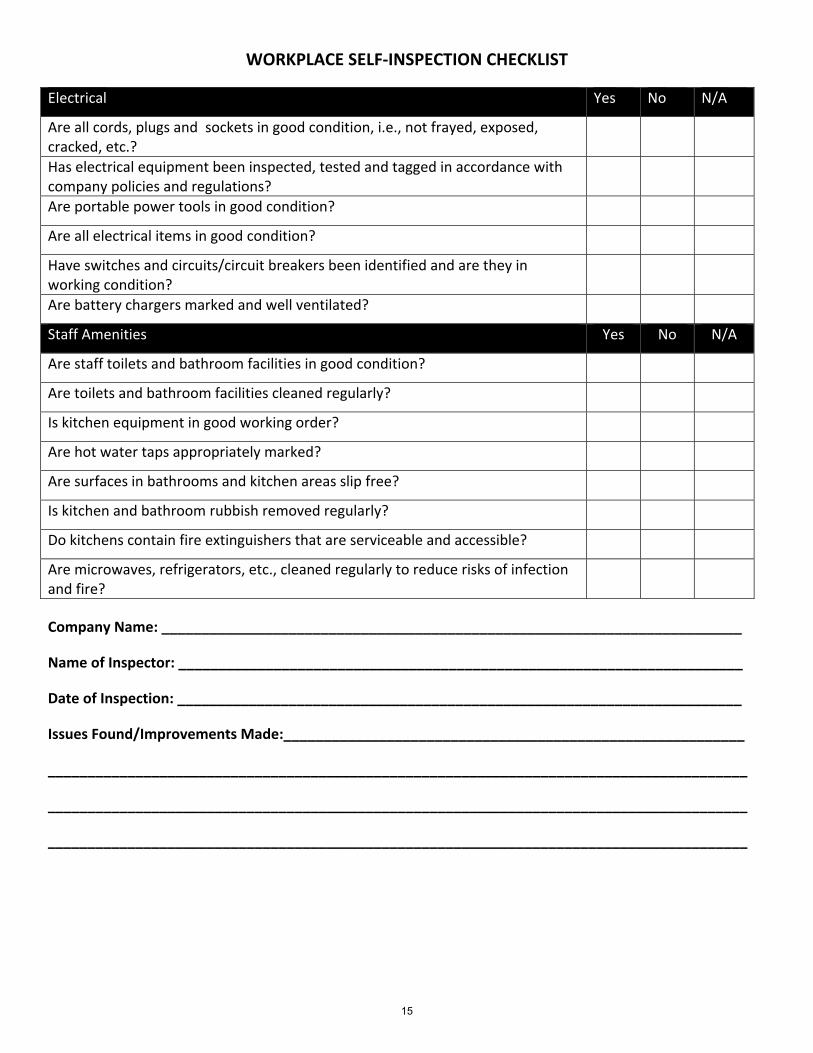
WORKPLACE SELF‐INSPECTION CHECKLIST
Electrical Yes No N/A
Are all cords, plugs and sockets in good condition, i.e., not frayed, exposed, cracked, etc.?
Has electrical equipment been inspected, tested and tagged in accordance with company policies and regulations?
Are portable power tools in good condition?
Are all electrical items in good condition?
Have switches and circuits/circuit breakers been identified and are they in working condition?
Are battery chargers marked and well ventilated?
Staff Amenities Yes No N/A
Are staff toilets and bathroom facilities in good condition?
Are toilets and bathroom facilities cleaned regularly?
Is kitchen equipment in good working order?
Are hot water taps appropriately marked?
Are surfaces in bathrooms and kitchen areas slip free?
Is kitchen and bathroom rubbish removed regularly?
Do kitchens contain fire extinguishers that are serviceable and accessible?
Are microwaves, refrigerators, etc., cleaned regularly to reduce risks of infection and fire?
Company Name: _________________________________________________________________________
Name of Inspector: _______________________________________________________________________
Date of Inspection: _______________________________________________________________________
Issues Found/Improvements Made:__________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
15
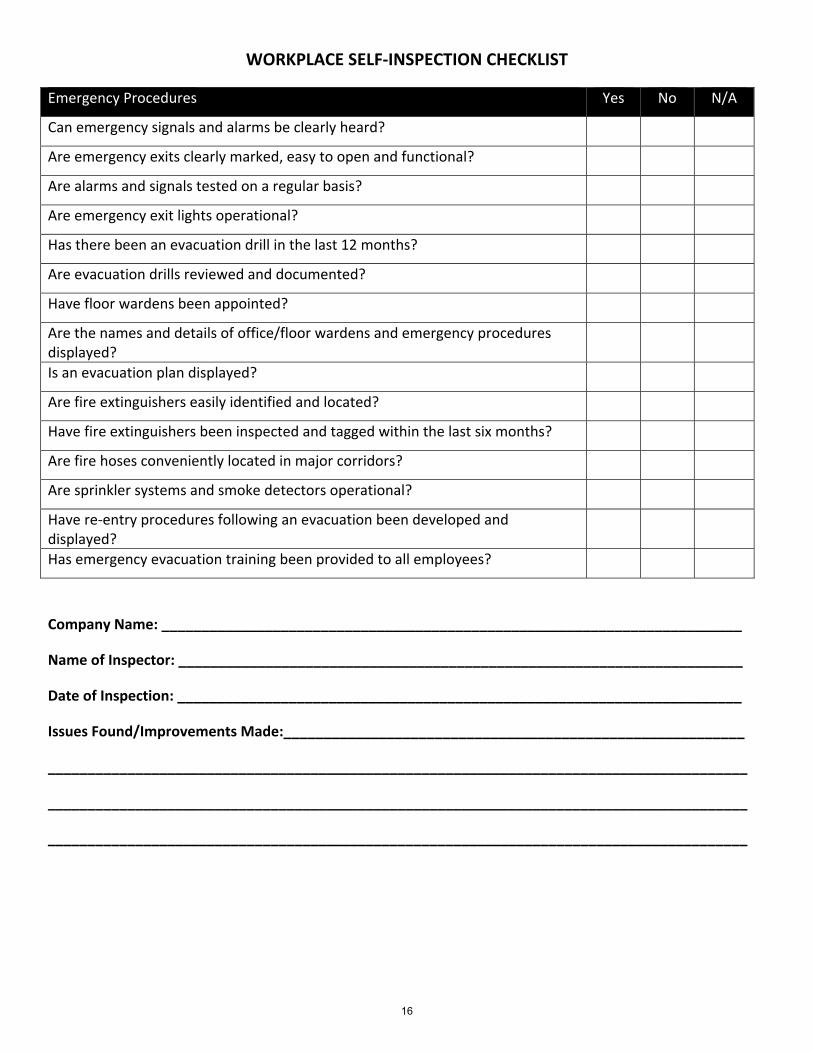
WORKPLACE SELF‐INSPECTION CHECKLIST
Emergency Procedures Yes No N/A
Can emergency signals and alarms be clearly heard?
Are emergency exits clearly marked, easy to open and functional?
Are alarms and signals tested on a regular basis?
Are emergency exit lights operational?
Has there been an evacuation drill in the last 12 months?
Are evacuation drills reviewed and documented?
Have floor wardens been appointed?
Are the names and details of office/floor wardens and emergency procedures displayed?
Is an evacuation plan displayed?
Are fire extinguishers easily identified and located?
Have fire extinguishers been inspected and tagged within the last six months?
Are fire hoses conveniently located in major corridors?
Are sprinkler systems and smoke detectors operational?
Have re‐entry procedures following an evacuation been developed and displayed?
Has emergency evacuation training been provided to all employees?
Company Name: _________________________________________________________________________
Name of Inspector: _______________________________________________________________________
Date of Inspection: _______________________________________________________________________
Issues Found/Improvements Made:__________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
16
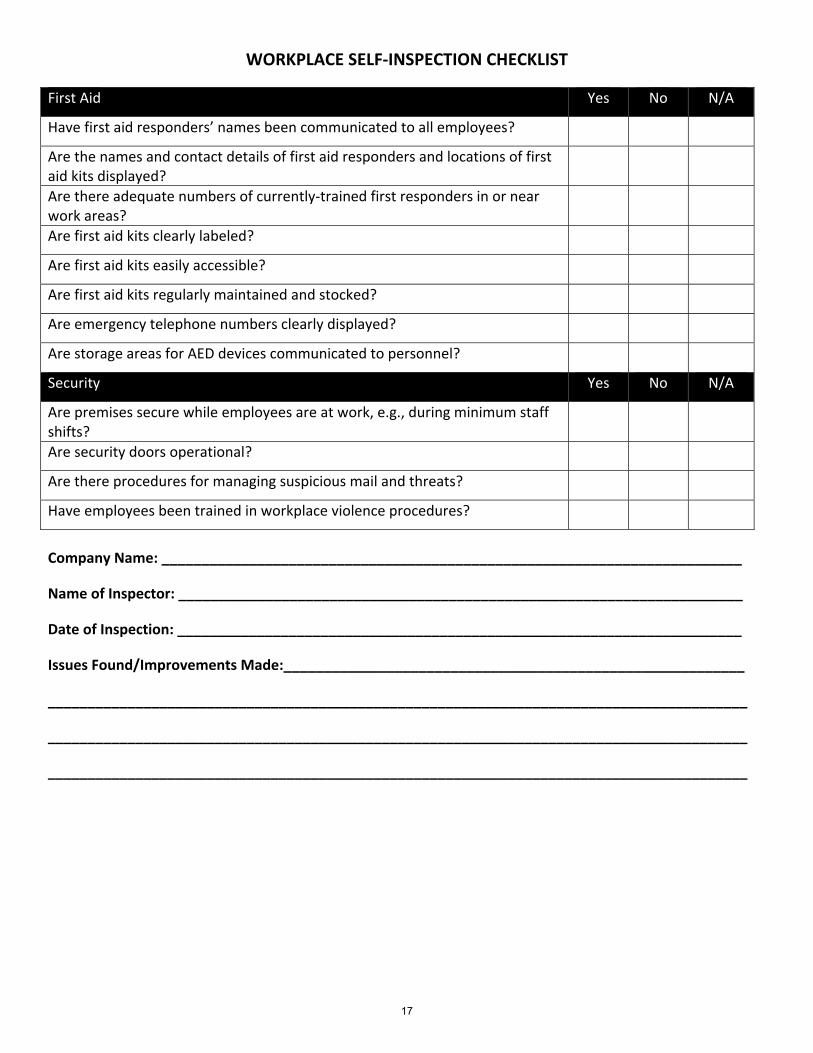
WORKPLACE SELF‐INSPECTION CHECKLIST
First Aid Yes No N/A
Have first aid responders’ names been communicated to all employees?
Are the names and contact details of first aid responders and locations of first aid kits displayed?
Are there adequate numbers of currently‐trained first responders in or near work areas?
Are first aid kits clearly labeled?
Are first aid kits easily accessible?
Are first aid kits regularly maintained and stocked?
Are emergency telephone numbers clearly displayed?
Are storage areas for AED devices communicated to personnel?
Security Yes No N/A
Are premises secure while employees are at work, e.g., during minimum staff shifts?
Are security doors operational?
Are there procedures for managing suspicious mail and threats?
Have employees been trained in workplace violence procedures?
Company Name: _________________________________________________________________________
Name of Inspector: _______________________________________________________________________
Date of Inspection: _______________________________________________________________________
Issues Found/Improvements Made:__________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
17
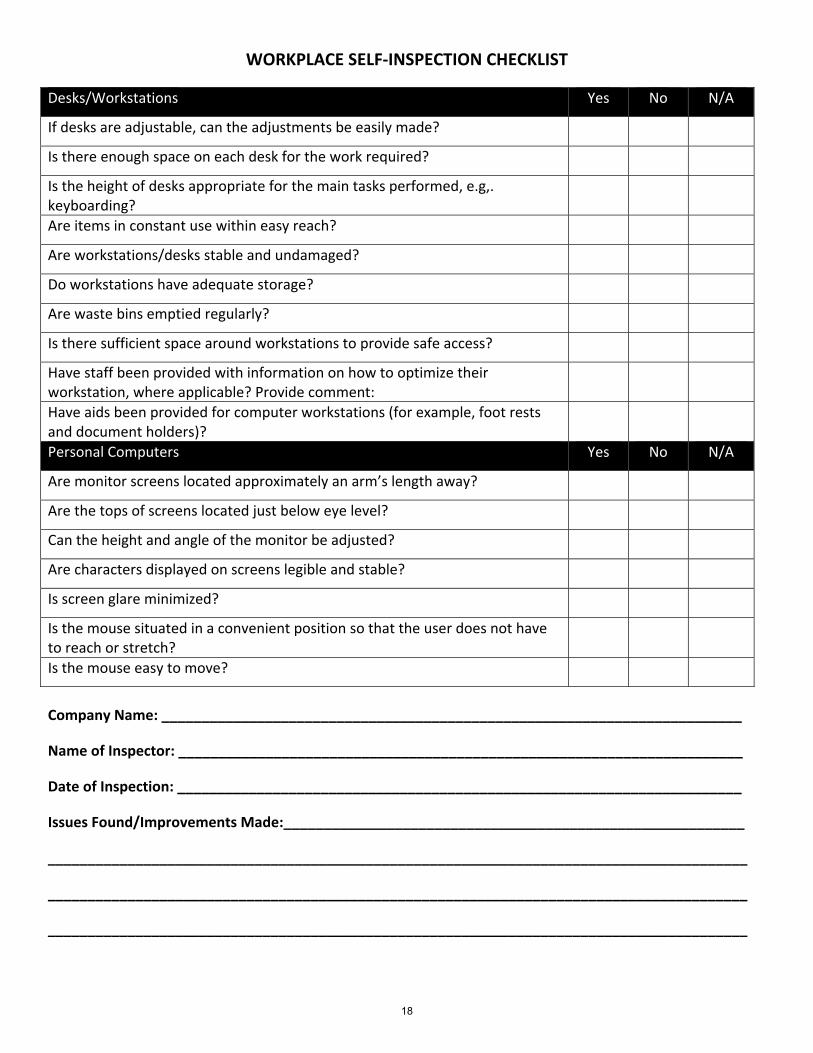
WORKPLACE SELF‐INSPECTION CHECKLIST
Desks/Workstations Yes No N/A
If desks are adjustable, can the adjustments be easily made?
Is there enough space on each desk for the work required?
Is the height of desks appropriate for the main tasks performed, e.g,. keyboarding?
Are items in constant use within easy reach?
Are workstations/desks stable and undamaged?
Do workstations have adequate storage?
Are waste bins emptied regularly?
Is there sufficient space around workstations to provide safe access?
Have staff been provided with information on how to optimize their workstation, where applicable? Provide comment:
Have aids been provided for computer workstations (for example, foot rests and document holders)?
Personal Computers Yes No N/A
Are monitor screens located approximately an arm’s length away?
Are the tops of screens located just below eye level?
Can the height and angle of the monitor be adjusted?
Are characters displayed on screens legible and stable?
Is screen glare minimized?
Is the mouse situated in a convenient position so that the user does not have to reach or stretch?
Is the mouse easy to move?
Company Name: _________________________________________________________________________
Name of Inspector: _______________________________________________________________________
Date of Inspection: _______________________________________________________________________
Issues Found/Improvements Made:__________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
18
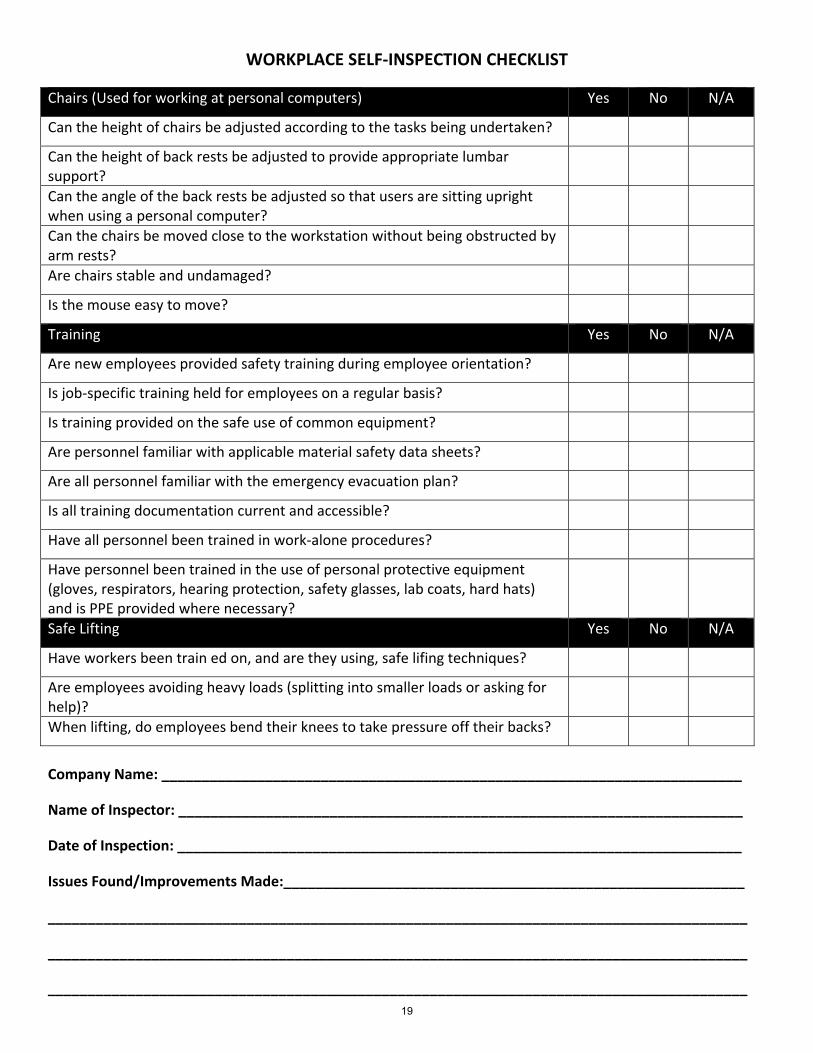
WORKPLACE SELF‐INSPECTION CHECKLIST
Chairs (Used for working at personal computers) Yes No N/A
Can the height of chairs be adjusted according to the tasks being undertaken?
Can the height of back rests be adjusted to provide appropriate lumbar support?
Can the angle of the back rests be adjusted so that users are sitting upright when using a personal computer?
Can the chairs be moved close to the workstation without being obstructed by arm rests?
Are chairs stable and undamaged?
Is the mouse easy to move?
Training Yes No N/A
Are new employees provided safety training during employee orientation?
Is job‐specific training held for employees on a regular basis?
Is training provided on the safe use of common equipment?
Are personnel familiar with applicable material safety data sheets?
Are all personnel familiar with the emergency evacuation plan?
Is all training documentation current and accessible?
Have all personnel been trained in work‐alone procedures?
Have personnel been trained in the use of personal protective equipment (gloves, respirators, hearing protection, safety glasses, lab coats, hard hats) and is PPE provided where necessary?
Safe Lifting Yes No N/A
Have workers been train ed on, and are they using, safe lifing techniques?
Are employees avoiding heavy loads (splitting into smaller loads or asking for help)?
When lifting, do employees bend their knees to take pressure off their backs?
Company Name: _________________________________________________________________________
Name of Inspector: _______________________________________________________________________
Date of Inspection: _______________________________________________________________________
Issues Found/Improvements Made:__________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
19
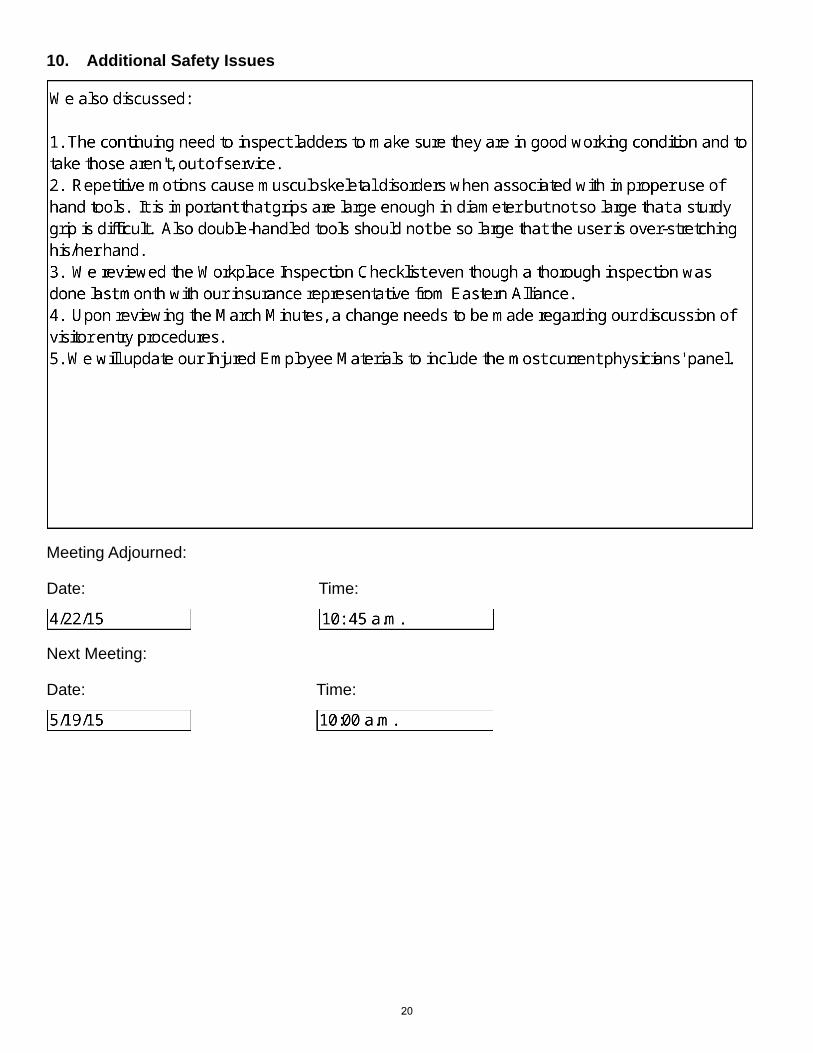
10. Additional Safety Issues
Meeting Adjourned:
Date: Time:
Next Meeting:
Date: Time:
20