workshop on traveling with diabetes
TRANSCRIPT

4/06/2015
1
Traveling with Chronic Medical Conditions:
Anticoagulation, Diabetes, andSleep Apnea
Mary-Louise Scully, CaliforniaFons Van Gompel, Belgium
Workshop on Traveling with Diabetes
Fons Van Gompel, ITM-Antwerp BelgiumMary-Louise Scully, California

4/06/2015
2
Remarks before embarking
• We are not endocrinologist / diabetologist –we are travel medicine specialist
• We are not going to discuss efficacy / indications / contra-indications / side-effects of the different methods for treatment, nor the treatment goals
• Patients themselves are deeply involved in the treatment of their disease, they are partners
• Wide spectrum of situations

4/06/2015
3
Case 1 = 30 year old female travelling to South-east Asia for 3 months
–arrival in Bangkok 1st of May– 4 week visit Myanmar– 2 week visit Laos – volunteer work (lessons
English, gardening)– 4 week visit Cambodia– End of June back home departure from Bangkok
•Insulin pump – basal dosing & bolus injections•Insulin pens with Lantus & Novorapid – no disposable ones •Glucometer, Friobags, carbohydrates, …. •Not traveling alone !!!! ……..
E-mails : …….

4/06/2015
4
Case 2Another more classic case (courtesy Dr Johan Wens, Belgium)
John and Jonathan, grandfather & grandson
Hobby = seashells
Flight to the Caribbean = 1 longer day
Jonathan = shortacting insuline & glucometer in handluggage
John = no problems, swollen feet
The first day at the beach, however, the problems started…..
4/06/2015
5
Case 3Lady who forgot to put off the blue-tooth connection between glucometer and insulin pump in the airplane at the take off …. big difficulty …(courtesy Dr Tania Daems, Belgium)
Many Topics : • Irregular meals, other foodstuff• Stress, irregular efforts• Vaccinations (flu – pneumo ? ) / Infections (TD & amoeba’s ?,
skin & candidiasis, TB ?, Melioidosis ?, Dengue ?)
• What to pack / insuline & glucose unit changes ? • Airplane (= altitude) & day of travel - time shift• Hypo / Keto-acidosis• Heat / Cold• Altitude ; Diving; Sailing• Quid travel with extreme obesity, travel after
bariatric surgery ? • Etc, etc, ,,,,,

4/06/2015
6
Outline Introduction
• Some Numbers of traveling diabetic persons• Some Studies on traveling diabetic persons • Some basics• Advices
15,440 travelers - 5 clinics “greater Boston area” March 1, 2008, - July 31, 2010,2769 (17.9%) were high-risk
– 2056 of 2769 (74.3%) had medical comorbidities • 244 of 2769 (11.9%) had diabetes mellitus

4/06/2015
7
Of the 644 immunocompromised persons,• 265 (41.2%) had non-HIVeassociated immunodeficiencies,• 148 (23.0%) had HIV/AIDS,• 100 (15.5%) had autoimmune disorders, • 74 (11.5%) had active cancer, • 23 (3.6%) weretransplant recipients, • 21 (3.3%) had thymic disease, and • 13 (2.1%) had a history of splenectomy or splenic dysfunction. Of the 2056 persons with medical comorbidities, • 633 (30.8%) had pulmonary disease, • 379 (18.4%) had cardiac arrhythmias, • 244 (11.9%) had diabetes mellitus, • 225 (10.9%) had a history of immunodeficiency, • 220 (10.7%) had psychiatric disease, • 182 (8.9%) had heart disease, • 112 (5.5%) had seizures or neurologic disease, • 52 (2.5%) had cirrhosis, and • 9 (0.4%) had renal disease requiring dialysis.
19,410 travelers, between 1/1/2005 and 31/12/200716,681 were included in the study3,046 had chronic illnesses
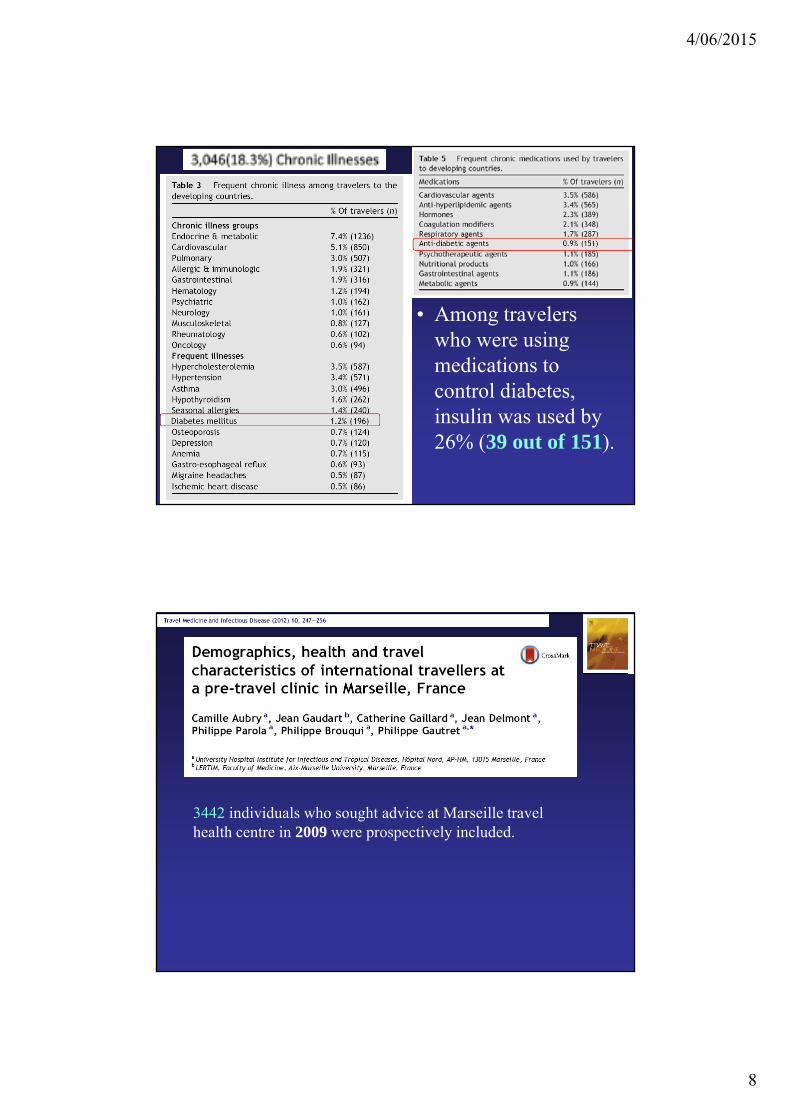
4/06/2015
8
• Among travelers who were using
• Among travelers who were using medications to control diabetes, insulin was used by 26% (39 out of 151).
3442 individuals who sought advice at Marseille travel health centre in 2009 were prospectively included.
4/06/2015
9
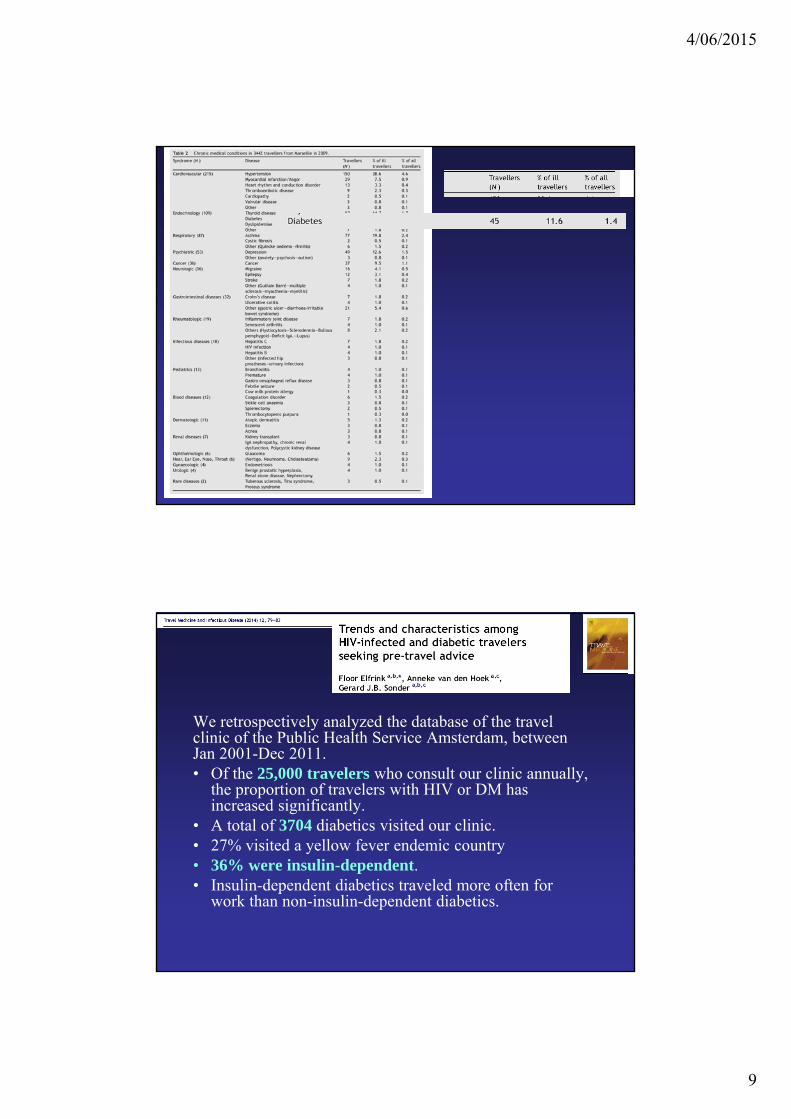
We retrospectively analyzed the database of the travel clinic of the Public Health Service Amsterdam, between Jan 2001-Dec 2011.• Of the 25,000 travelers who consult our clinic annually,
the proportion of travelers with HIV or DM has increased significantly.
• A total of 3704 diabetics visited our clinic. • 27% visited a yellow fever endemic country • 36% were insulin-dependent.• Insulin-dependent diabetics traveled more often for
work than non-insulin-dependent diabetics.
4/06/2015
10
Outline Introduction
• Some Numbers of traveling diabetic persons• Some Studies on traveling diabetic persons • Some basics• Advices
DRIESSEN JTM 1999
• Retrospective : 19 respondents: 11 Type 1 & 8 type 2 IDDM, • 13 (70%) reported any metabolic dysregulation (10 Type 1 DM).
– 55 % of Type 1 diabetics reported to have dysregulated more often than in the preceding period at home.
– Critical dysregulations occurred in 2 /19 study patients. • Only 4 out of 11 (36%) type 1 DM patients increased frequency of
blood glucose monitoring while traveling. • 3 had febrile illness which resulted in hyperglycemic
dysregulation. • 5 had difficulties in the adjustment of their insulin dosage due to
the unfamiliar circumstances of traveling in the tropics.

4/06/2015
11
DRIESSEN JTM 1999
• Five (26%) patients experienced difficulties in the adjustment of the changed insulin requirements – to the other,sometimes unknown, food and/or– circadian rhythm during their stay in the tropics.
• Passing time zones by intercontinental flight caused metabolic dysregulation for two patients.
• One reported difficulties at the customs because of carrying injection material.
DRIESSEN JTM 1999
• Eleven (58%) out of 19 respondents reported a non-DM related medical problem while traveling, including– gastroenteritis (4), – upper respiratory tract infection (1) – Q-fever (1).
• Fever occurred in 3 (16%) of these 19. • All 3 diabetics with fever reported hyperglycemic dysregulation
for which the insulin dosage had to be increased.• Of the 3 travelers suffering from diarrhea without fever, only
one reported a slight hypoglycemia. • Skin infections were reported by three respondents (16%), two
with pyoderma and one with dermatomycosis.• T here were no infections of the feet.

4/06/2015
12
BURNETT JTM 2006
• 493 patients using insulin• 10% experienced problems while traveling,
mostly due to hypoglycemia.• 37 travelled alone - 15% of them told no one
that they were using insulin therapy• 8 did not carry any form of identification on
their person that they had diabetes mellitus.
BAATEN JTM 2010
4/06/2015
13
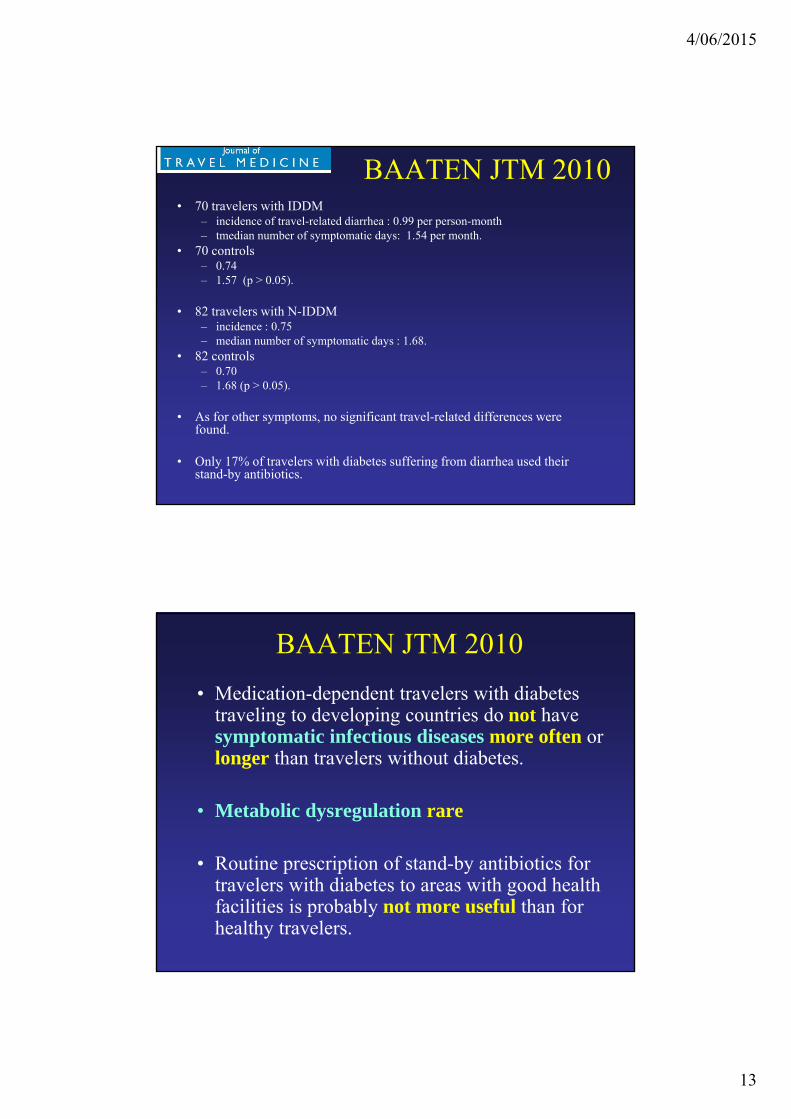
BAATEN JTM 2010• 70 travelers with IDDM
– incidence of travel-related diarrhea : 0.99 per person-month– tmedian number of symptomatic days: 1.54 per month.
• 70 controls – 0.74 – 1.57 (p > 0.05).
• 82 travelers with N-IDDM– incidence : 0.75– median number of symptomatic days : 1.68.
• 82 controls– 0.70 – 1.68 (p > 0.05).
• As for other symptoms, no significant travel-related differences were found.
• Only 17% of travelers with diabetes suffering from diarrhea used their stand-by antibiotics.
BAATEN JTM 2010• Medication-dependent travelers with diabetes
traveling to developing countries do not have symptomatic infectious diseases more often or longer than travelers without diabetes.
• Metabolic dysregulation rare
• Routine prescription of stand-by antibiotics for travelers with diabetes to areas with good health facilities is probably not more useful than for healthy travelers.
4/06/2015
14
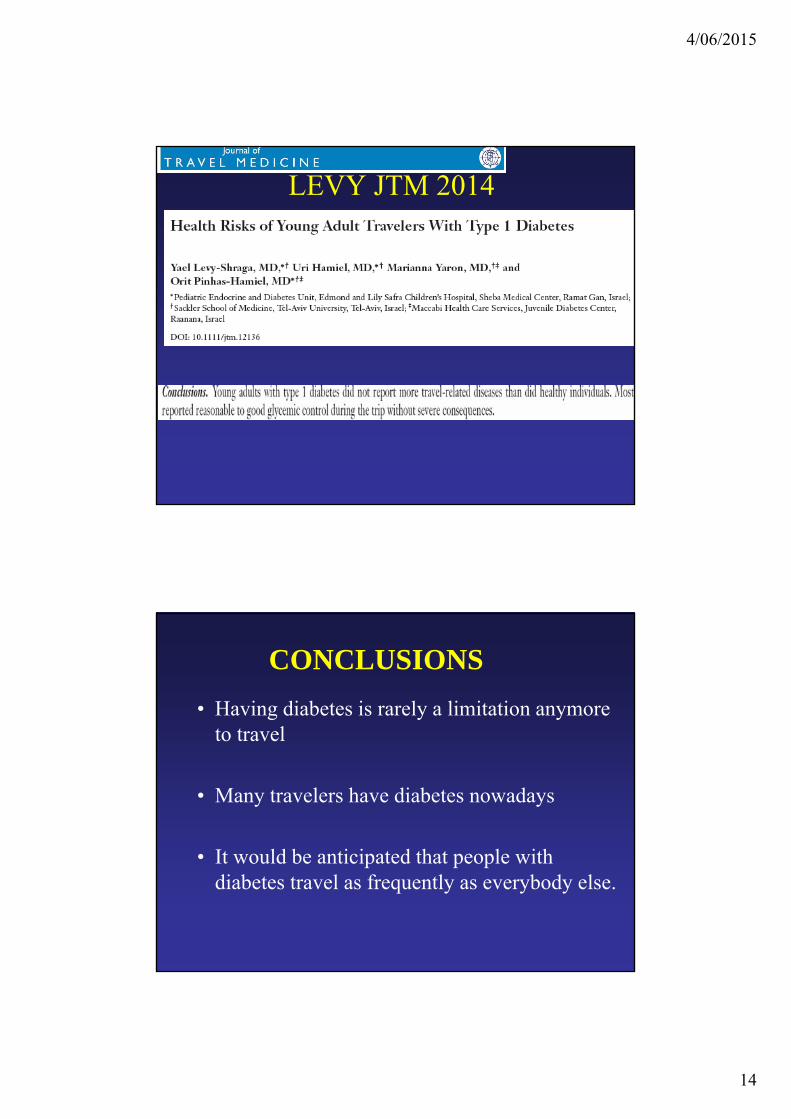
LEVY JTM 2014
CONCLUSIONS• Having diabetes is rarely a limitation anymore
to travel
• Many travelers have diabetes nowadays
• It would be anticipated that people with diabetes travel as frequently as everybody else.

4/06/2015
15
CONCLUSIONS
• Although those with diabetes may face special challenges during travel, they can usually anticipate or avoid serious problems by meticulous advance planning
• Medication-dependent travelers with diabetes traveling to developing countries do not have symptomatic infectious diseases more often or longer than travelers without diabetes
Outline Introduction
• Some Numbers of traveling diabetic persons• Some Studies on traveling diabetic persons • Some basics :
– oral medications– insuline therapy - different regimens– Glucometers– Frio
• Advices

4/06/2015
16

4/06/2015
17
4/06/2015
18
http://www.diabetesmonitor.com/
http://www.diabetesmonitor.com/
4/06/2015
19
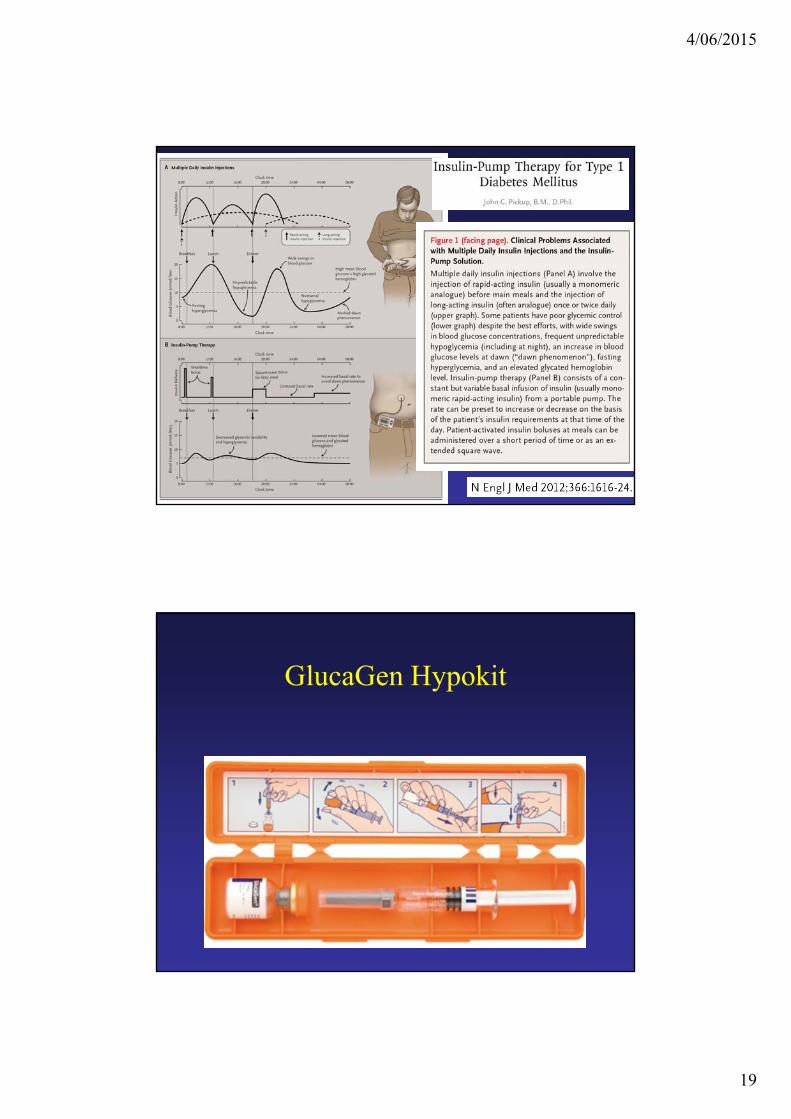
GlucaGen Hypokit

4/06/2015
20
Frio cooling wallet
GENERAL PREPARATIONS

4/06/2015
21
Diabetes and travelSome sources used
Medical Preparation• General health status • Is the diabetes stable ? well controlled ?
…. is a must !!– IDDM – NIDDM ?– late organ-complications or co-morbidities ?
neuropathy, nephropathy, retinopathy, macro-angiopathic ischemia, diabetic foot, …
• General precautions as for everybody traveling with a chronic disease / ailment

4/06/2015
22
Changes …Patients traveling with diabetes need to consider how to adapt their treatment programs to
• irregular schedules & day rythm, waiting times, time shift
• unfamiliar foods, more alcohol ?• varying amounts of exercise, stress, • varying climate, temperature• risk for motion sickness, TD, febrile infections, skin
problems, etc, etc
WITH RISK FOR METABOLIC DYSREGREGULATION
Medical Preparation• Good planning and advance preparation are key to avoiding stress and problems arising as a result of traveling with diabetes.
• It is important to make plane and hotel reservations in advance and to allow reasonable time between connecting flights.
• Organize assistance ahead of time if the connection time will be a problem.
• Preferably no rudimentary circumstances in remote destinations …

4/06/2015
23
Who gives advice ? Who gives advice ?• GP, endocrinologist/diabetes nurse –
nutriotionist / dietician• national diabetes organizations • Role travel medicine specialist ? = “co-coach”• Patient is partner !!
Every input is useful, as long as specific advice is given, & better to much than to less, if consistent ?
In advance …• Good planning and advance preparation are key to avoiding stress and problems arising as a result of traveling with diabetes.
• It is important to make plane and hotel reservations in advance and to allow reasonable time between connecting flights.
• Organize assistance ahead of time if the connection time will be a problem.

4/06/2015
24
Insurance .. Papers ..Companions• Appropriate Insurance (National Diabetes Association)• Mmedical passport, Diabetes identification tag or
bracelet (MedicAlert)• Billfold card detailing insulin dose and doctor's name
and telephone number• Signed statement from personal physician on letterhead
stationary documenting – medical diagnosis and – necessity for carrying supply of insulin, syringes, and
needles for diabetic treatment, – as well as original prescription (Rx) labels on syringes and
medications• Extra Prescriptions
• Travel with two or in group• Inform the traveling companion(s), the
personnel / staff, …
• Accessibility by phone or email in case of problems, questions
Insurance .. Papers ..Companions

4/06/2015
25
VACCINATIONS
VACCINATIONS

4/06/2015
26
X, Contraindicated (per the Advisory Committee on Immunization Practices [ACIP]);
U, Use as indicated for normal hosts;
R, Recommended for all in this patient category;
P, Precaution (per ACIP);
W, Warning —medical conditions for which no data regarding YF vaccine exist but for which varying degrees of immune deficit might be present and could increase the risk of serious adverse events following vaccination; providers should carefully weigh vaccine risks and benefits before deciding to vaccinate such patients;
C, Consider; PCV13, 13-valent pneumococcal conjugate vaccine; PPSV23, 23-valent pneumococcal polysaccharide vaccine.
X, Contraindicated (per the Advisory Committee on Immunization Practices [ACIP]);
U, Use as indicated for normal hosts;
R, Recommended for all in this patient category;
P, Precaution (per ACIP);
W, Warning—medical conditions for which no data regarding YF vaccine exist but for which varying degrees of immune deficit might be present and could increase the risk of serious adverse events following vaccination; providers should carefully weigh vaccine risks and benefits before deciding to vaccinate such patients;
C, Consider; PCV13, 13-valent pneumococcal conjugate vaccine; PPSV23, 23-valent pneumococcal polysaccharide vaccine.
4/06/2015
27
INFECTIONS

4/06/2015
28
Conclusions. Patients with DM1 and DM2 are at increased risk for• lower respiratory tract infection, • urinary tract infection, • skin and mucous membrane infection.
The risk of developing tuberculosis increased among those with increasing diabetes severity.

4/06/2015
29
• Diabetes in general and treated diabetes were significantly associated with tuberculosis (adjusted hazard ratio, 2.09 [95% confidence interval {CI}, 1.10–3.95] and 2.60 [95% CI, 1.34–5.03], respectively).
• Compared with persons without treated diabetes, participants’ risk of tuberculosis increased as the number of complications of diabetes mellitus increased (P 5 .0016), with .3-fold risk among those with $2 diabetes-related complications (odds ratio, 3.45; 95% CI, 1.59–7.50).
• Similarly, the risk increased among those with higher Diabetes Complications Severity Index scores (P 5 .0002).
• The risk of developing tuberculosis increased among those with increasing diabetes severity.
Melioidosis …
4/06/2015
30
The currently available epidemiological evidence is very limited and only suggestive.
• Large prospective studies that systematically and objectively obtain relevant signs and symptoms of dengue fever episodes as well as of hyperglycemia in the past, and at the time of dengue diagnosis, are needed to properly address the effect of diabetes on the clinical presentation of an acute dengue fever episode.
• The currently available epidemiological evidence is very limited and only suggestive.
• The increasing global prevalence of both dengue and diabetes justifies further studies.
• At this point, confirmation of dengue infection as early as possible in diabetes patients with fever if living in dengue endemic regions seems justified. The presence of this co-morbidity may warrant closer observation for glycemic control and adapted fluid management to diminish the risk for a severe clinical presentation of dengue.

4/06/2015
31
MALARIA
• As for everybody• Rarely or no interactions with diabetes
treatment• Malaria not necessarily more severe, but in
case of fever …metabolic dysregulation
• “The risk of vaginal candidiasis is also increased, particularly if taking an antibiotic such as doxycycline for malaria prevention.”
TD• Vulnerable for
dehydration • dehydration can
affect blood glucose levels
adequate hydration should be maintained.
• ORS, loperamide, antibiotics

4/06/2015
32
Skin health• Travellers with diabetes, especially those with
peripheral neuropathy, should avoid injury to their feet. They should wear comfortable, well-fitting shoes and avoid walking barefoot.
• Feet should be checked regularly for injury, and kept clean, dry and moisturised.
• Toenails should be well-trimmed and broken skin covered with a sterile dressing.
• Insect bite avoidance is important; bites should be kept clean and no scratched. An antihistamine can reduce itching.

4/06/2015
33
Infections ….
• not only the fact that they are yes or no more vulnerable for infectious diseases or for more severe, complicated forms,
• but also the fact that in case of infection serious dysregulation of the glycemia - especially for hyperglycemia with risk for ketoacidosis, & hyperosmolar coma may occur = combination of serious morbidity
• especially in case of high fever, vomiting & diarrhea• in case of infections : extra controls of the blood
sugar & good hydration (keep drinking)
Middle East Respiratory Syndrome Coronavirus (MERS-CoV)
4/06/2015
34
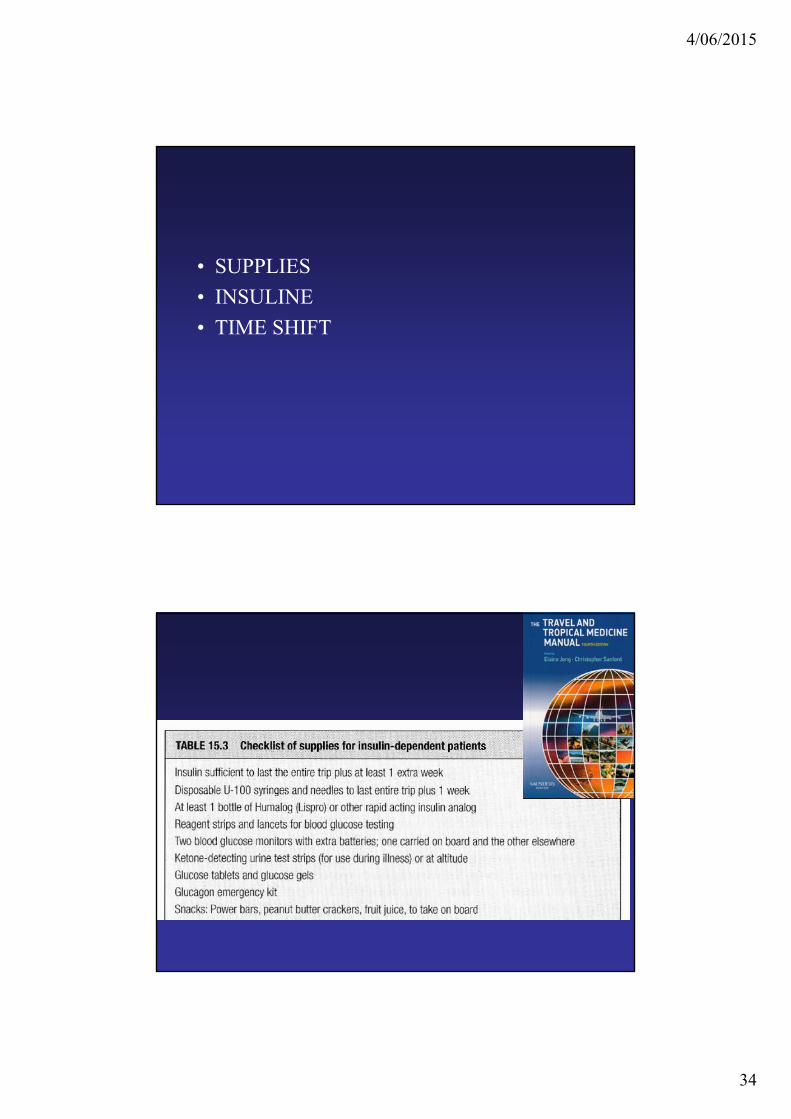
• SUPPLIES• INSULINE• TIME SHIFT
4/06/2015
35
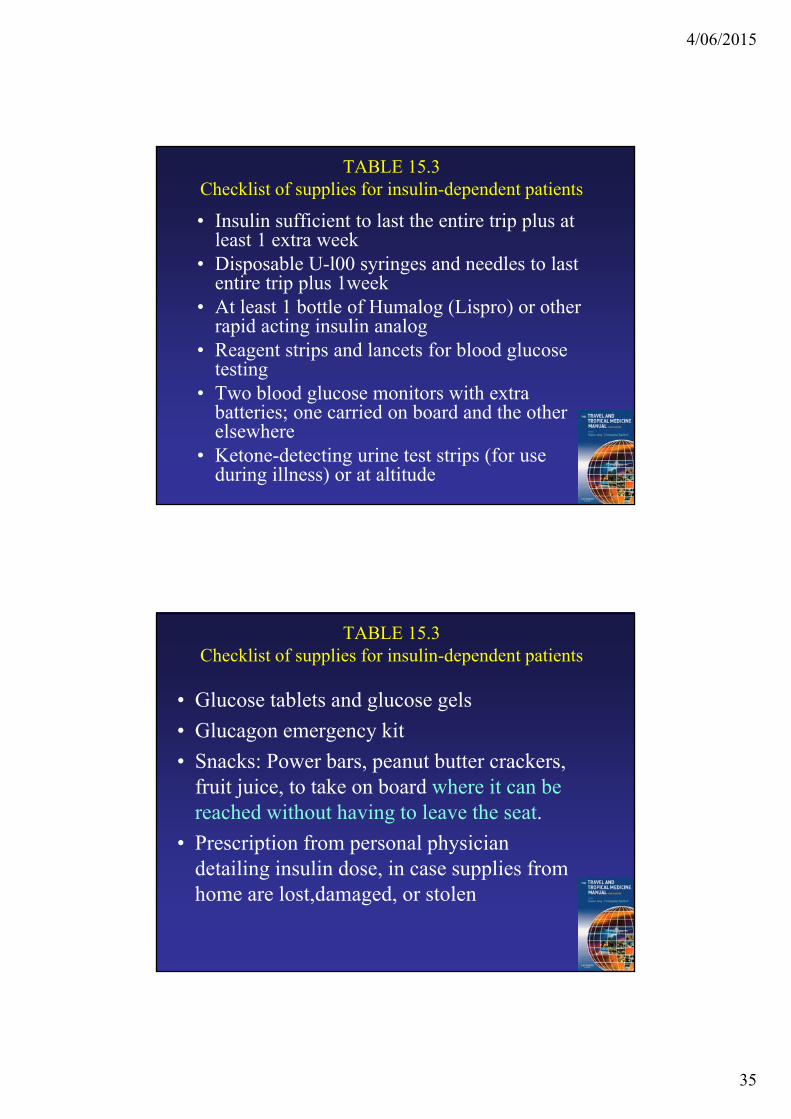
TABLE 15.3 Checklist of supplies for insulin-dependent patients
• Insulin sufficient to last the entire trip plus at least 1 extra week
• Disposable U-l00 syringes and needles to last entire trip plus 1week
• At least 1 bottle of Humalog (Lispro) or other rapid acting insulin analog
• Reagent strips and lancets for blood glucose testing
• Two blood glucose monitors with extra batteries; one carried on board and the other elsewhere
• Ketone-detecting urine test strips (for use during illness) or at altitude
TABLE 15.3 Checklist of supplies for insulin-dependent patients
• Glucose tablets and glucose gels• Glucagon emergency kit• Snacks: Power bars, peanut butter crackers,
fruit juice, to take on board where it can be reached without having to leave the seat.
• Prescription from personal physician detailing insulin dose, in case supplies from home are lost,damaged, or stolen

4/06/2015
36
INSULIN
• Transportation• Prevention metabolic dysregulation• Time shift • Problems in airports, on in flight on the
airplanes• Problems in hot climates• Problems on altitude, cold
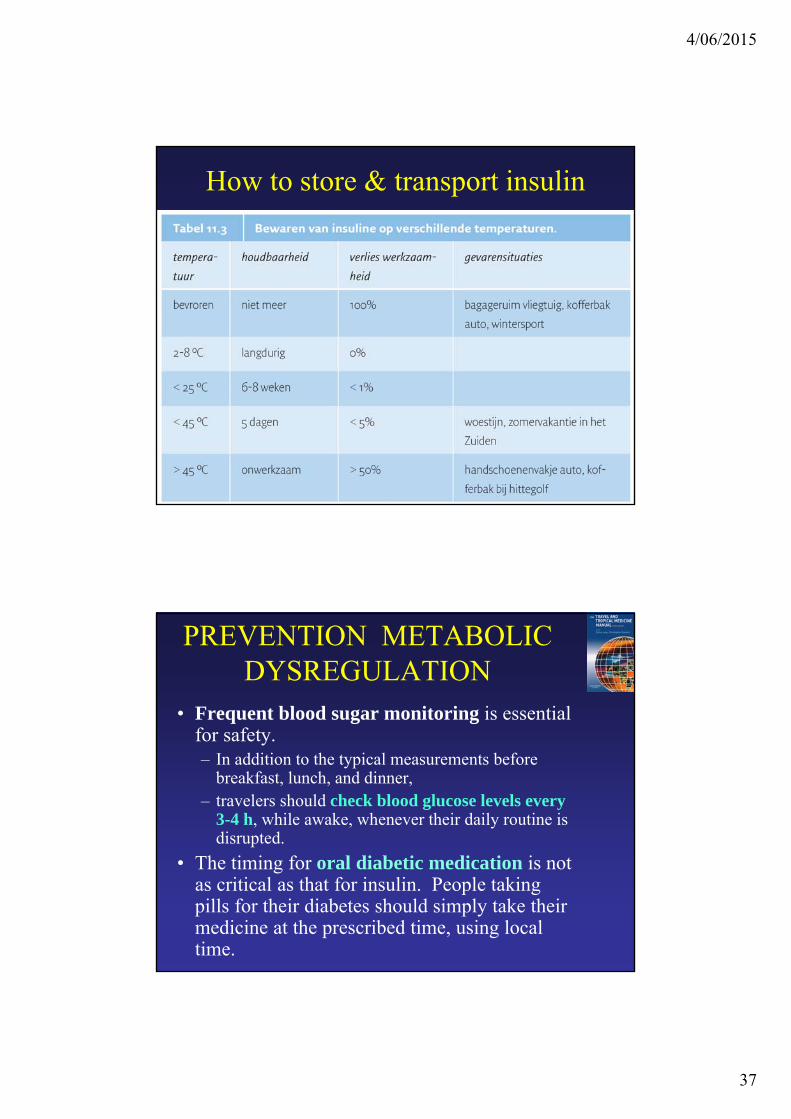
How to store & transport insulin
• Insulin should be stored away from direct sunlight and protected from temperature variations by use of a thermal insulated bag / flask.
• Insulin remains stable for up to 1 month when stored at room temperature (20°C). It will deteriorate more rapidly in warmer climates
4/06/2015
37
How to store & transport insulin
PREVENTION METABOLIC DYSREGULATION
• Frequent blood sugar monitoring is essential for safety. – In addition to the typical measurements before
breakfast, lunch, and dinner, – travelers should check blood glucose levels every
3-4 h, while awake, whenever their daily routine is disrupted.
• The timing for oral diabetic medication is not as critical as that for insulin. People taking pills for their diabetes should simply take their medicine at the prescribed time, using local time.
4/06/2015
38
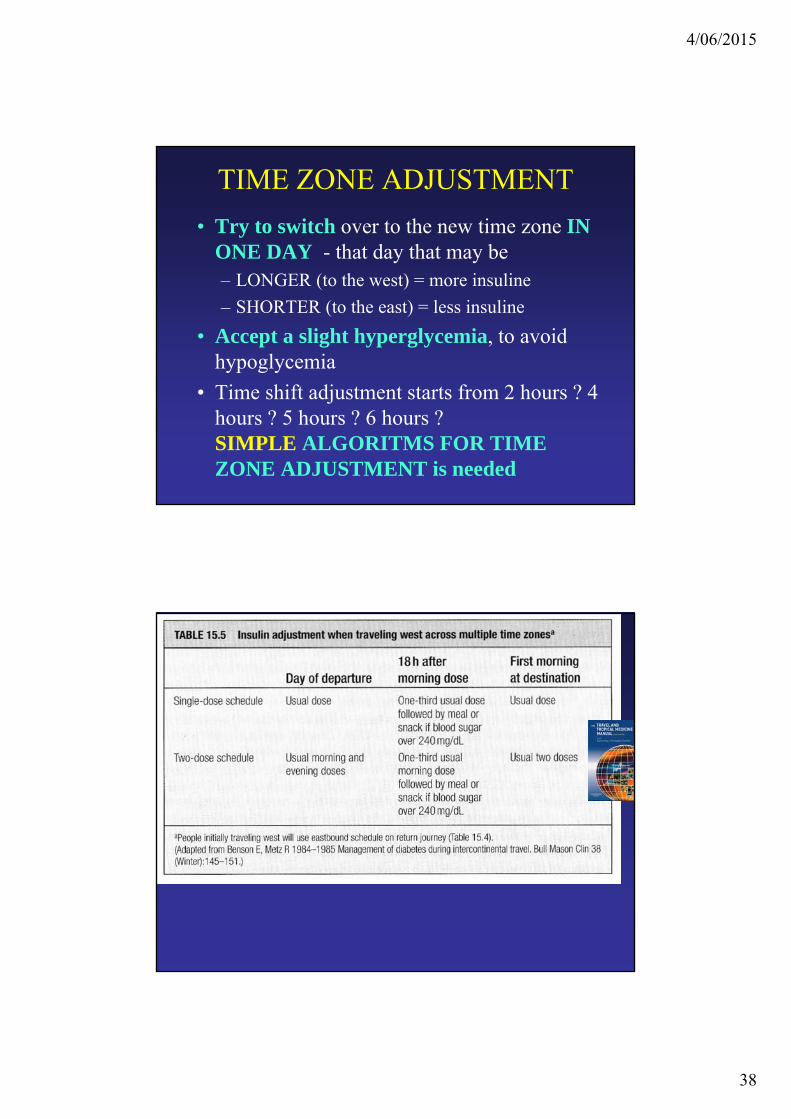
TIME ZONE ADJUSTMENT• Try to switch over to the new time zone IN
ONE DAY - that day that may be – LONGER (to the west) = more insuline– SHORTER (to the east) = less insuline
• Accept a slight hyperglycemia, to avoid hypoglycemia
• Time shift adjustment starts from 2 hours ? 4 hours ? 5 hours ? 6 hours ? SIMPLE ALGORITMS FOR TIME ZONE ADJUSTMENT is needed

4/06/2015
39
Airport security
• Most airport security personnel in major international airports are familiar with insulin pumps.
• Best wearing the pump in an easily accessible place, such as a front pants or skirt pocket.

4/06/2015
40
Warm – Cold• Insulin is absorbed
– more quickly in warm temperatures – more slowly In cold temperatures.
• The performance of glucometers, test strips and insulin delivery device can be affected by – temperature, – humidity and – altitude.
• Urine dipsticks may provide a more reliable method of basic monitoring whilst at altitude.
• Specialist advice should be received prior to travel to these environment.
• ALTITUDE• DIVING• SAILING
4/06/2015
41
ALTITUDE
Travel to high altitude
Expeditions with diabetics have had both positive and negative feedback regarding the health of these individuals.
Problems encountered have included • poorly functioning glucometers, possibly related to the cold
& hypoxia • confusion between AMS and hypoglycemia, • ketoacidosis secondary to anorexia / nausea and vomiting of
AMS• side-effects of medications • remoteness of medical care.

4/06/2015
42
… the glucose-dye-oxi-reductase (non O2 dependent) meters appeared to give more accuratereadings than the O2 dependent glucose oxidasemeters, giving an underestmation of glucose levels by 1-2% per 1000 ft / 300 mMy own Accucheck Active seemed to work well and indeed was specified by the manufacturers to 6500m, but is now off the market
Temperature.• Blood glucose meters are specified within a given temperature
range (typically +10 to +40C) and modern ones often contain a temperature sensor and will refuse to operate if outside set parameters.
• Temperature of sticks is also important as is their storage conditions (eg +2 to +30C)
• The mountaineers on IDEA 2000 Diabetic Acongaguaexpedition kept their test kit in insulated pouches worn under clothing near the skin to maintain temperatures.
Humidity• May be a factor.(Fink 2002) Altitude air tends to be dry
Wind• Can cause rapid drying of the blood sample

4/06/2015
43
keep the meter and test sticks warm, take the readings in shade and away from winds and use a large drop of blood to prevent rapid drying.
Best wishes Paul Richards / Medical Expeditions UK / [email protected]
DIVING

4/06/2015
44
Chpt 40 Diving Medicine Karen J. Marienau & Paul M. Arguin
P 374 Diabetes MellitusGuidelines developed in 2005 recommend that adults with diabetes mellitus may dive provided they • have been on a stable dose of insulin for 1 year or
oral hypoglycemic agents for at least 3 months; • have a glycosylated hemoglobin level of ≤9%; • have had no significant episodes of hypo- or
hyperglycemia for 1 year; • have no secondary complications of diabetes; and
have hypoglycemia awareness.Pollock et al. Diabetes and recreational diving: guidelines for the future. Proceedings of the UHMS/DAN 2005 June 19 Workshop. Durham, NC: Divers Alert Network; 2005. www.diversalertnetwork.org

4/06/2015
45
SAILINGLook at : www.forcedouce.org