wound care & suture techniques - cdn.ymaws.com · healing after flap surgery • secondary...
TRANSCRIPT
7/16/18
1
Wound Care & Suture Techniques
• M ic h a e l H a z e l , D N P, R N , F N P - B C
• S t e v e B r a n h a m , P h D , R N , F N P, A C N P
• T a r a L . R o b e r t s M S N , R N , A N P - B C
What to expect today..
• D iscuss different types of w ound healing techniques and assessm ents
• Identify different suture types and uses in the clinical setting
• D iscuss several w ound considerations and/or com plications that can arise during
healing process
• Practice – Practice - Practice
• (1) H em ostasis : w ithin m inutes post-in jury, platelets aggregate at the in jury site to form a fibrin clot.
• (2) Inflam m atory : bacteria and debris are phagocytosed and rem oved, and factors are released that cause the m igration and division of cells involved in the proliferative phase.
• (3) Proliferative : angiogenesis, collagen deposition, granulation tissue form ation, epithelialization, and w ound contraction
• (4) R em odeling : collagen is rem odeled and realigned along tension lines and cells that are no longer needed are rem oved by apoptosis.
Model of Wound Healing
7/16/18
2
Factors Affecting Wound Healing
L o c a l F a c t o r s
• O xygenation
• Infection
• Foreign body
• Venous sufficiency
S y s t e m ic F a c t o r s
•Age and gender•Sex hormones
•Stress•Ischemia•Diseases: DM, keloids, fibrosis, hereditary healing disorders, jaundice, uremia
•Obesity•Medications: glucocorticoid steroids, NSAIDS, chemo agents
•Alcoholism and smoking•Immunocompromised conditions
•Nutrition
CDC Surgical Wound Classification• C o n t a m i n a t e d : ( 1 0 - 1 7 % r i s k ) open, fresh, accidental w ounds, operations
w ith m ajor breaks in sterile technique or gross spillage from the gastrointestinal
tract, and incisions in w hich acute, non-purulent inflam m ation is encountered.
• D i r t y o r i n f e c t e d : ( > 2 7 % r i s k ) old traum atic w ounds w ith retained devitalized tissue and those that involve existing clinical infection or perforated
viscera. This definition suggests that the organism s causing postoperative infection w ere present in the operative field before the operation.
Wound Cleaning•Consider…– H a n d w a s h in g
– P e r s o n n e l p r e c a u t io n s
– H a ir r e m o v a l
– A n e s t h e s ia
– F o r e ig n m a t e r ia l
– W o u n d s o a k in g

7/16/18
3
Wound Cleaning
• “The solution to pollution is dilution”
• Scrubbing-controversial (be wary of too m uch on cosm etic areas)
Wound Preparation• M o s t im p o r t a n t s t e p f o r r e d u c in g t h e r i s k o f w o u n d in f e c t io n .
• R e m o v e a l l c o n t a m in a n t s a n d d e v i t a l iz e d t i s s u e b e f o r e w o u n d c lo s u r e .
– I R R I G A T E w / N S o r T A P W A T E R ( A V O I D H 2 O 2 , P O V I D O N E -I O D I N E )
– C U T O U T D E A D , F R A G M E N T E D T I S S U E
• I f n o t , t h e r i s k o f in f e c t io n a n d o f a c o s m e t i c a l ly p o o r s c a r a r e g r e a t ly in c r e a s e d
• P e r s o n a l P r e c a u t io n s
Anesthetic Solutions•CAUTIONS: due to its vasoconstriction properties never
use Lidocaine with epinephrine on: – Eyes, Ears, Nose – Fingers, Toes
– Penis, Scrotum
7/16/18
4
Anesthetic Solutions
• Lidocaine (Xylocaine® ) – Most commonly used
– Rapid onset
– Strength: 0.5%, 1.0%, & 2.0% – Maximum dose:• 5 mg / kg, or
• 300 mg – 1.0% lidocaine = 1 g lidocaine / 100 cc
= 1,000mg/100cc– 300 mg = 0.03 liter = 30 ml
• Lidocaine (Xylocaine® ) w ith epinephrine
– Vasoconstriction– Decreased bleeding
– Prolongs duration – Strength: 0.5% & 1.0%
– Maximum individual dose:• 7mg/kg, or• 500mg
Anesthetic Solutions
• BU PIVA CA IN E (M A RCA IN E):– Slow onset
– Long duration
– Strength: 0.25% or 0.50%– DOSE: maximum individual dose 3mg/kg
Local Anesthetics

7/16/18
5
Injection Techniques• 25, 27, or 30-gauge needle
• 6 or 10 cc syringe
• Check for allergies
• Insert the needle at the inner w ound edge
• A spirate
• In ject agent into tissue SLO W LY
• Wait…
• A fter anesthesia has taken effect, suturing m ay begin
Types of Sutures• A b s o r b a b le o r n o n - a b s o r b a b le ( n a t u r a l o r s y n t h e t i c )
• M o n o f i la m e n t o r m u l t i f i l a m e n t ( b r a id e d )
• D y e d o r u n d y e d
• S iz e s 3 t o 1 2 - 0 ( n u m b e r s a lo n e in d ic a t e p r o g r e s s iv e ly
la r g e r s u t u r e s , w h e r e a s n u m b e r s f o l lo w e d b y 0 in d ic a t e p r o g r e s s iv e ly s m a l le r )
• N e w a n t ib a c t e r ia l s u t u r e s

7/16/18
6
Suture
Natural Suture• Biological• Cause inflammatory reaction
–Catgut (connective from cow or sheep)
–Silk (from silkworm fibers)–Chromic catgut
Synthetic• Synthetic polymers• Do not cause inflammatory response
–Nylon–Vicryl–Monocryl–PDS–Prolene
Monofilament• Single strand of suture m aterial
• M inim al tissue traum a
• Sm ooth tying but m ore knots
needed
• H arder to handle due to m em ory
• Exam ples: nylon, m onocryl, prolene, PD S
Multifilament (braided)• Fibers are braided or tw isted
together
• M ore tissue resistance
• Easier to handle
• Few er knots needed
• Exam ples: vicryl, silk, chrom ic
SutureA b s o r b a b le
• N ot biodegradable and perm anent
–Nylon–Prolene–Stainless steel–Silk (natural, can
break down over years)
N o n - A b s o r b a b le
• D egraded via inflam m atory response
–Vicryl–Monocryl–PDS–Chromic–Cat gut (natural)

7/16/18
7
Suture Materials
Suture Sizes
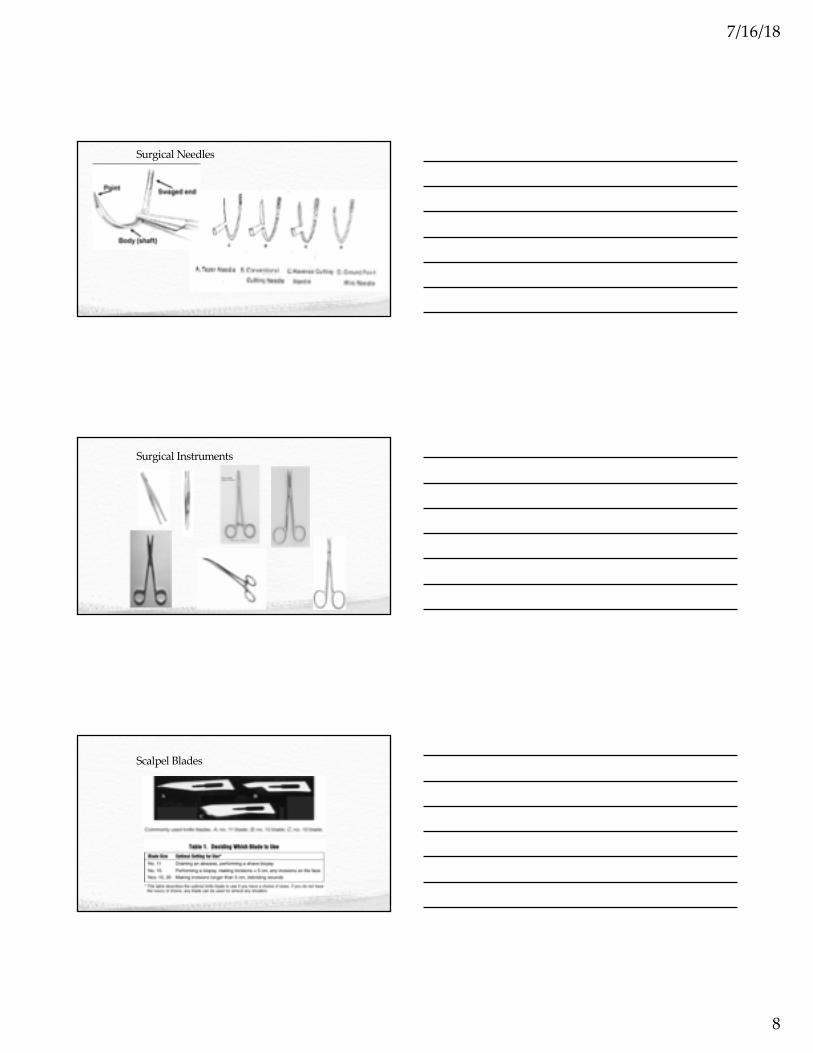
Surgical Needles• W ide variety w ith different com pany’s nam ing system s
• 2 basic configurations for curved needles
Cutting: cutting edge can cut through tough tissue, such as skin
Tapered: no cutting edge. For softer tissue inside the body
7/16/18
8
Surgical Needles
Surgical Instruments
Scalpel Blades
7/16/18
9
Langer’s Lines
Wound Evaluation• Tim e of incident
• Size of w ound
• D epth of w ound
• Tendon / nerve involvem ent
• Bleeding at site
When to Refer•Deep wounds of hands or feet, or unknown depth of penetration• Full thickness lacerations of eyelids, lips or ears• Injuries involving nerves, larger arteries, bones,
joints or tendons•Crush injuries•Markedly contaminated wounds requiring
drainage•Concern about cosmesis
7/16/18
10
Contraindications to Suturing
• R e d n e s s
• E d e m a o f th e w o u n d m a rg in s
• In fe c tio n
• F e v e r
• P u n c tu re w o u n d s
• A n im a l b ite s
• Te n d o n , n e rv e , o r v e s s e l in v o lv e m e n t
• W o u n d m o re th a n 1 2 h o u rs o ld (b o d y ) a n d 2 4 h rs (fa c e )
• S o m e re p o r ts n o w a re th a t b o d y w o u n d s c a n b e c lo s e d u p to 1 8 h rs la te r a n d fa c ia l w o u n d s u p to 4 8 -7 2 if n o s ig n o f in fe c tio n o r c o n ta m in a tio n .
Closure Types
• Primary closure (primary intention)– Wound edges are brought together so that they are adjacent to each
other (re-approximated) – Examples: well-repaired lacerations, well reduced bone fractures,
healing after flap surgery
• Secondary closure (secondary intention)
– Wound is left open and closes naturally (granulation)– Examples: gingivectomy, gingivoplasty,tooth extraction sockets,
poorly reduced fractures
• Tertiary closure (delayed primary closure)– Wound is left open for a number of days and then closed if it is
found to be clean
– Examples: healing of wounds by use of tissue grafts.
Basic Laceration Repair
Principles And Techniques
7/16/18
11
Principles And Techniques• M in im iz e t r a u m a in s k in
h a n d l in g
• G e n t le a p p o s i t io n w i t h s l ig h t e v e r s io n o f w o u n d
e d g e s– Visualize an Erlenmeyer flask
• M a k e y o u r s e l f c o m f o r t a b le– Adjust the chair and the light
• C h a n g e t h e la c e r a t io n – Debride crushed tissue
Types of Closures● Sim ple interrupted closure – m ost com m only used, good for
shallow w ounds w ithout edge tension
● Continuous closure (running sutures) – good for hem ostasis (scalp w ounds) and long w ounds w ith m inim al tension
● Subcuticular – good for cosm etic results● Vertical m attress – useful in m axim izing w ound eversion, reducing
dead space, and m inim izing tension across the w ound
● H orizontal m attress – good for fragile skin and high tension w ounds
● Percutaneous (deep) closure – good to close dead space and decrease w ound tension
Simple Interrupted Suturing• A pply the needle to the needle driver– Clasp needle 1/2 to 2/3 back from tip
• Rule of halves:– Matches wound edges better; avoids dog ears
– Vary from rule when too much tension across wound
7/16/18
12
Suturing• The needle enters the skin
w ith a 1/4-inch bite from the w ound edge at 90 degrees
– Visualize Erlenmeyer flask– Evert wound edges
• Because scars contract over time
Suturing• Release the needle from the needle driver, reach into the w ound
and grasp the needle w ith the needle driver. Pull it free to give enough suture m aterial to enter the opposite side of the w ound.
• U se the forceps and lightly grasp the skin edge and arc the needle through the opposite edge inside the w ound edge taking equal bites.
• Rotate your w rist to follow the arc of the needle.
• Principle: m inim ize traum a to the skin, and don’t bend the needle. Follow the path of least resistance.
Suturing•Release the needle and grasp the portion of the needle
protruding from the skin with the needle driver. Pull the needle through the skin until you have approximately 1 to 1/2-inch suture strand protruding form the bites site.
•Release the needle from the needle driver and wrap the suture around the needle driver two times.

7/16/18
13
Simple Interrupted SuturingRule of halves
Simple Interrupted SuturingRule of halves
Simple, Interrupted
http://www.youtube.com/watch?v=PFQ5-tquFqY
7/16/18
14
7/16/18
15
Suturing
Examples
Staples….
ThanksP r a c t i c e , P r a c t i c e , P r a c t i c e