wrong problem, wrong treatment unrecognised inappropriate referral to physiotherapy
TRANSCRIPT
322
Wrong Problem, Wrong Treatment U n recog n ised i na p p ro pr ia te referra I to physiotherapy
Summary A combination of increasing demand from primary care aRd limitations on the capacity of NHS physiotherapy services to respond is likely to re-open the debate about the appropriateness of referred cases. Musculoskeletal symptoms are the commonest, and an increasing, reason for direct referral from primary care to physiotherapy. However, evidence suggests that in primary care such symptoms often reflect somatisation of patients’ u n recog nised mental iI I ness.
In a study of primary care patients with persistent physical symptoms due to somatisation of mental illness, we found a substantial minority (45%) who had been referred for one or more courses of physiotherapy. We present case histories from a number of patients who had received physiotherapy to illustrate patterns of somatisation of mental illness. Physiotherapy does not appear .to benefit and may harm such patients by reinforcing their somatic orientation and delaying access to more appropriate interventions.
‘The absence of recent published accounts of inappropriate referral from general practice to physiotherapy suggests that the problem of somatisation is either not recognised or not acknowledged by the two professions. We consider approaches to reducing this type of inappropriate demand on physiotherapy services.
Rose, M, Stanley, I, Peters, S, Salmon, P, Stott, Rand Crook, P (1999). ‘Wrorifi problem,
I1 r 1 1-c c() gn i sc (1 i r ia 1) p pliysiotherapy’, l’li~~.sioih,(~/~~)y, 85, 6 , :’,22-32x.
\Vl-Ollg 1 ~ C ~ l l Y l C l l t :
p r i a lc rcfc rml to
, , , . . . . . . . Introduction Studies of direct access by general practitioners (GI‘s) to physiotherapy have confirmed its effectiveness (Gentle et al, 1984; Fordhani and Hodkinson, 1987) , capacity to reduce drug costs (Hackett et al, 1993) and acceptability to patients (Hackett el nl, 1987). A recent review of the published literaturc: (Robert and Stevens, 1997), while calling for ‘good quality evidence of the cost- effkctiveness of different models of physical therapy services’, concludes that there are distinct advantages to patients from direct referral by their GP for physical therapy. This conclusion supports GPs’ aspiration for practice-based physiotherapy (GMSC, 1992) and explains the sharp increase in demand from general practices adopting fund- holding status (Robert. and Stevens, 1997). In one study (O’Cathain el al, 1995) the
Key Words
provision of a practice-based physiotherapy service led to an increase of 164% in demand compared to that previously made upon a hospital-based service. This upward trend in demand is likely to be accelerated by more recent NHS reforms (DOH, 1997). The gradual transfer of lead responsibility for commissioning from Health Authorities to Primary Care Groups (PCGs) and the capacity of PCGs to vire funds between previously ring-fenced budgets could lead to significantly greater investment in primary care physiotherapy services.
However, there are factors limiting the capacity of NHS services to respond, for example the availability of enough physiotherapists (Palastanga, 1995). s’ ince at least some of the advantages of direct access are likely to arise from prompt treatment (Robert and Stevens, 1997), waiting li for primary care patients referred t o physiotherapy are undesirable, and probably unacceptable to their GPs. Elsewhere (Crook el al, 1998) we have suggested that these factors will lead to more groupwork with patients, with physiotherapists increasingly acting in the role of educators/advisers (Worsfold et al, 1996).
It has often been asserted (Ellman el al, 1982; Mackett et al , 1993; Robert and Stevens, 1997) that rising demand for physiotherapy from primary care does not imply an increased level of inappropriate referral. However, the issue of‘ appro- priateness, which has remained dormant since initial recommendations on direct access by GPs to physiotherapy (Partridge, 1976), is likely to be reactivated by rising demand coupled with the limited capacity of NHS services to respond. In early accounts (Partridge and Warren, 1977), while physiotherapists reported inappropriate referrals, particularly from a minority of doctors, they found that the proportion progressively diminished. We have been
Physiotherapy,Jrinc 199Y/vol 85/no 6

Prof essiona I articles 323
unable to confirm the generalisability of this observation or find current estimates of the level of inappropriate referral; a recent literature search failed to find published evidence on this topic in the last five years.
T h e majority of referrals to physio- therapists from GPs are for musculoskeletal symptoms (Croft, 1993; Hackett et al, 1993). During the most recent decade for which data are available, the proportion of patients consulting their GPs for problems of this kind increased from 13% to 15% (McCormick et nl, 1995). In primary care patients, musculoskeletal symptoms are frequently an expression of mental illness (Wright, 1990) , a process known as soniatisation (Craig and Boardman, 1990; Shorter, 1992; Weich et al, 1995). However, failure by GPs to detect psychological morbidity in their patients is well documented (Freeling el al, 1985; Howe, 1996). Moreover, persistent somatising patients can cause ‘heart-sink’ in GPs (O’Dowd, 1988) and trigger a wide range of more or less appropriate referrals (Stanley et al, 1999). O n this basis, it is likely that a proportion of referrals by GPs to physio- therapists will be somatising patients who have no physical basis for their niusculo- skeletal symptoms.
Physiotherapy has a traditional allegiance to explanatory models in which a direct causal relationship exists between disease or trauma and patients’ symptoms. Moreover, in physiotherapy practice this cause-and- effect relationship may be applied in a reductionist way: physical examination of the presenting part is used to identify anatomical structures that call for local treatment. However, physical signs may be present in somatising patients. In low back pain, for example, restriction of movement by pain, muscle wasting and local tenderness can arise from disuse consequent upon psychosocial factors alone (Troup and Videman, 1989). Thus, in isolation, physical assessment may lead to patients with u n re c o g n is e d re c e ivi n g inappropriate physical treatment.
The paucity of published inforniation on this issue may reflect a failure by general practice and physiotherapy to recognise or acknowledge an aspect of’ shared care which, potenlially, has significant implications for patients, for both professions and, in terms of resource use, for the NHS. During recruitment to a controlled trial of aerobic exercise for primary care patients with persistent, unexplained physical symptoms
so mat i s a t i o n
(Crook et al, 1998), we explored patients’ treatment histories including previous courses of physiotherapy. In this way we sought retrospective evidence of demand on physiotherapy from primary care for patients with somatising disorders. In the present paper we report our findings and illustrate with case histories the somatisation of psychosocial problems for which physio- therapy had been sought and administered.
Method Recruitment All GPs in Liverpool and St Helens and Knowsley were invited to refer patients with physical symptoms which had persisted for at least one year and remained unexplained despite specialist referral and investigation. A total of 323 patients was referred. Fifteen patients were excluded because of ischaemic heart disease and /o r hypertension ( 9 ) , asthma (4) or a history of psychosis (2) , and 228 agreed to take part . Of these, GP records were available for 198.
Data Collection Socio-demographic data were recorded and individuals’ post codes used to allocate a score on the index of local conditions (deprivation index; DOE, 1995). Analyses used deciles of the index for Merseyside. Health care utilisation data were collected from GP records.
All patients completed the Hospital Anxiety and Depression (HAD) scale (Zigmond and Snaith, 1983); a score above eight on either of the subscales representing ‘caseness’ ie a high probability of clinically significant anxiety or depression being detected at formal psychiatric assessment. The HAD sub-scales are designed to exclude physical symptoms of anxiety and depression, and are well validated among primary care patients (Wilkinson and BarcLak, 1988; Upadhyaya and Stanley, 1993, 1995).
All patients were interviewed by a research assistant (SP) and asked to describe current symptoms and their history of illness, medical investigation and treatment. Qualitative thematic analyses of patient interview transcripts, including an account of our methods, have already been reported (Peters e t al , 1998). Following random allocation of patients to one of two group exercise programmes, the physiotherapists leading the programmes (RS and PC) recorded participants’ clinical histories. The experiences captured in these histories are
Authors Michael Rose PhD MCSP is an honorary Senior restxrch fellow in thr University of Kecle, Dtprtmerit of Physio therapy.
Ian Stanley FRCGP is emeritus professor in thr Department of Primary Care, University of‘ Liverpool.
Sarah Peters MA is a rcsearcli assistant ir i the Departments of Prirnary Care and Clinical Psychology at the University of Iivcrpool.
Peter Salmon PhD is professor of clinical psychology at the University of‘Liverpoo1.
Rachel Stott MCSP arid Pat Crook MCSP arc physiotherapists in Whistori Hospital N H S Trusl.
‘This article was rcceivrtl on September 3, 1998, arid acccpted on March 5, 1999.
Contribution Sarah Peters was responsible for thc operational rnanagcnient of the study, data collection and arialysis and played a m+jor part in the study’s cvolution. Rachel Stotl and Pat Crook were the study’s resrarch physiotherapists. Professor Stanley, Professor Salmon arid Dr Rose were grant holders for the study. This paper is a result of cqual contributions by all the authors.
Address for Correspondence I>r M J Rose, Back Pain I’rograrnnie, Wirral Hospital NHS Trust, Clatterbridge Koad, Bebbington, Wirral, Merseysidc I,63 4]Y.
Physiotherapy Junc iSYS/vol %/no 6
324
the basis of this paper. Details of the aerobic exercise and stretching/relaxation pro- grammes have also been published previously (Crook et al, 1998).
Findings Patient Characteristics The ages of the 228 participants ranged from 19 to 73 years (mean = 43.6 years) and 121 (53%) were women. Typically, particip- ants reported multiple symptoms (range =
0-12, mode = 3, mean = 4.23); of which a detailed analysis has already been reported (Stanley Pt al, 1999). While back pain was the most frequent single symptom (25%), 70 participants (31%) reported musculoskeletal pain as their main complaint. Whereas only 31 patients (14%) reported depression or anxiety as their primary problem, 154 (68%) scored above eight on the depression subscale and 166 (73%) on the anxiety sub- scale of the HAD; 124 (54%) were both anxious and depressed.
Health Care Use Analysis of GP records revealed high levels of patient contact with health care: in the six months before recruitment, GP consult- ations ranged from 0 to 43 (mean = 7.9, sd = 5.7, mode = 7) compared with the national mean of two (OPCS, 1995); and 55% of the sample (125) had been referred to hospital.
Of the 228 participants, 49 men and 53 women (45%) reported having received a course of physiotherapy during their present illness.
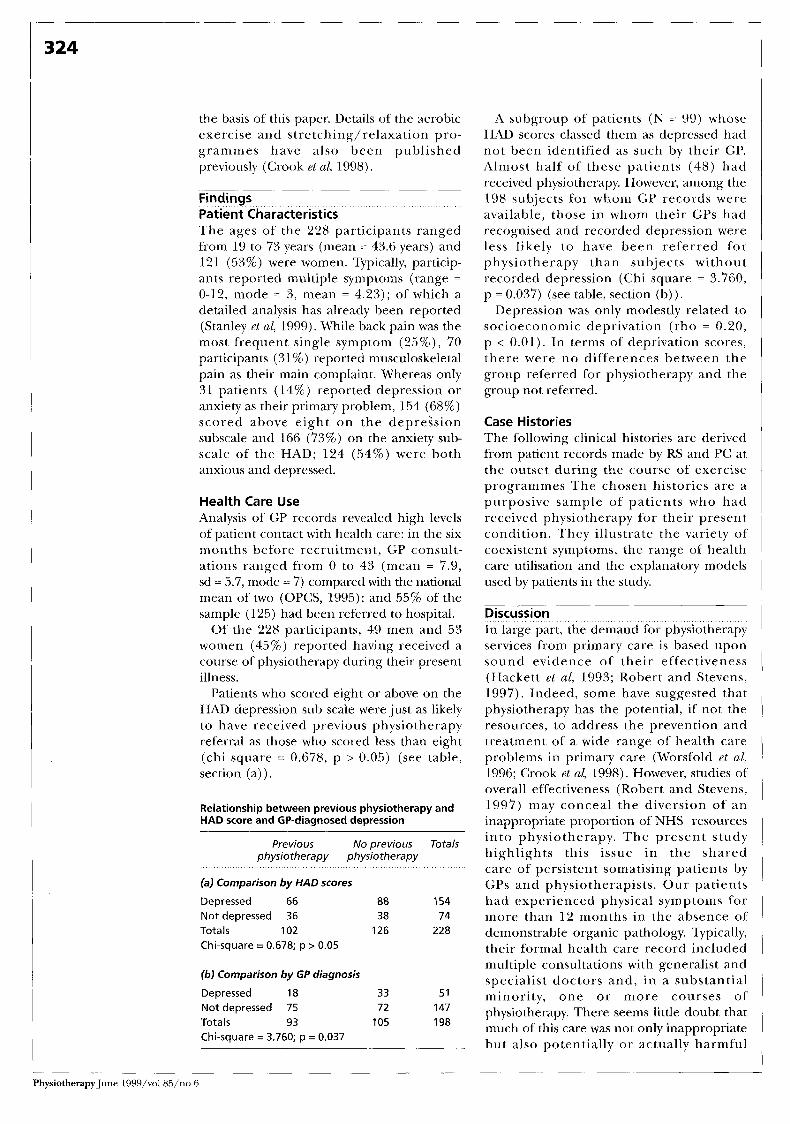
Patients who scored eight or above on the HAD depression sub scale were just as likely to have received previous physiotherapy referral as those who scored less than eight (chi square = 0.678, p > 0.05) (see table, section (a)) .
Relationship between previous physiotherapy and HAD score and GP-diagnosed depression
Previous No previous Totals physiotherapy physiotherapy
(a) Comparison by HAD scores
Depressed 66 88 154
Totals 102 126 228 Chi-square = 0.678; p > 0.05
Not depressed 36 38 74
(b) Comparison by GP diagnosis
Depressed 18 33 51 Not depressed 75 72 147 Totals 93 105 198 Chi-square = 3.760; p = 0.037
A subgroup of patients (N = 99) whose HAD scores classed them as depressed had not been identified as such by their GP. Almost half of these patients (48) had received physiotherapy. However, among the 198 sub,jects for whom GP records were available, those in whom their GPs had recognised and recorded depression were less likely to have been referred for physiotherapy than subjects without recorded depression (Chi square = 3.760, p = 0.037) (see table, section (b)) .
Depression was only modestly related to socioeconomic deprivation (rho = 0.20, p < 0.01). In terms of deprivation scores, there were no differences between the group referred for physiotherapy and the group not referred.
Case Histories The following clinical histories are derived from patient records made by RS and PC at the outset during the course of exercise programmes The chosen histories are a purposive sample of patients who had received physiotherapy for their present condition. They illustrate the variety of coexistent symptoms, the range of health care utilisation and the explanatory models used by patients in the study.
Discussion In large part, the demand for physiotherapy services from primary care is based upon sound evidence of their effectiveness (Hackett et al, 1993; Robert and Stevens, 1997). Indeed, some have suggested that physiotherapy has the potential, if not the resources, to address the prevention and treatment of a wide range of health care problems in primary care (Worsfold et nl, 1996; Crook et al, 1998). However, studies of overall effectiveness (Robert and Stevens, 1997) may conceal the diversion of an inappropriate proportion of NHS resources into physiotherapy. The present study highlights this issue in the shared care of persistent somatising patients by GPs and physiotherapists. Our patients had experienced physical symptoms for more than 12 months in the absence of demonstrable organic pathology. Typically, their formal health care record included multiple consultations with generalist and qpecialist doctors and , in a substantial minority, one or more courses of physiotherapy. There seems little doubt that much of’ this care was not only inappropriate but also potentially o r actually harmful
Physiotherapy June 1 YSY/vol85/no 6
Professional articles 325
'Mary' (45 years old) presented with a burning pain of several years duration in her neck, shoulder girdle, low back and both legs. A range of diagnostic tests had failed to identify inflammatory or orthopaedic pathology. Analgesic and anti-inflammatory medication had been prescribed for her pain and she had completed several courses of musculoskeletal physiotherapy.
Mary is cautious of exercise and manages the problem by resting. She also experiences fatigue symptoms and believes that her problems are caused by myalgic encephalitis (ME) which resulted from a series of infections following the death of her husband. Mental state assessment suggests that she has moderate depression and anxiety.
'John' (44) has a long history of incapacitating multiple joint pains. Investigations u nd ert a ke n by d e pa rt m e n t s of g ast roe n tero I og y, n e u rol og y, o r t h o paed ics a nd rheumatology were negative. A course of physiotherapy, which included therapeutic exercises and passive physical modalities, was unhelpful.
John maintains the belief that his symptoms are caused by an unidentified food allergy. He spends most of the time resting. He has a high depression score.
'David' (39) has a 13-year history of low back and neck pain accompanied by paraesthesiae in the right arm ('bubbles in the blood, fizzing'). More recently he has been diagnosed as having irritable bowel syndrome and ME, In addition, he experiences lack of concentration, muscle pain and fatigue. Despite investigation by departments of gastroenterology, medicine, orthopaedics, surgery, infectious diseases and rheumatology, no physical pathology has been demonstrated.
He asserts that a course of physiotherapy made his symptoms worse. His response to the problem is to rest either in bed or on a chair for most of the day and consume homoeopathic remedies and vitamin supplements. He is a member of the ME Society. He acknowledges that his symptoms are increased by stress and that the onset of these problems followed business failure and marital breakdown. He has high anxiety and depression scores.
'Susan' (45) has a 12-month history of pains in her legs, spine and shoulders which are made worse by activity. She also complains of poor co-ordination and vomiting after exercise. She traces the onset of her symptoms to a series of 'viral infections' which followed the death of her husband three years ago.
Susan believes that the infections have attacked her immune system resulting in ME, a diagnosis which is supported by her general practitioner. Investigations performed by departments of medicine and rheumatology have been unhelpful and physiotherapy was unsuccessful. Susan manages her condition by continued inactivity. She has moderate anxiety and depression scores.
'Philip' (45) dates his symptoms from a back injury five years ago. In addition to his back problem, he experiences neck and arm pain and is dizzy on exertion. He wears a corset and can only walk short distances with the aid of two sticks. Referral by his GP to a pain clinic, to departments of homoeopathy and psychiatry and for physiotherapy have not helped to relieve his symptoms. He manages his pain by avoidance of activity and heavy use of opiates. He has high anxiety and depression scores.
I
'Mildred' (58) has had pain in her neck, low back and coccyx for five years following a fall a t work. Radiographs are unremarkable and her local pain clinic diagnosed anxiety disorder. In addition, she has had abdominal pain for some years which she attributes to an ulcer, despite negative gastroenterology investigations. Remarkably, she has had three separate courses of physiotherapy which have included manipulation and passive electrical modalities. Mildred has high anxiety and depression scores.
Acknowledgement We are gratetirl to the MetLic:al Kesearch (huiicil whidi fiinded the study and t o thc h l lowing for their hclp and support: Anne O'Ryan, lorrnc-rly physiotherapy rriariager at St Helen's and Knowsley NHS Trnst; Eilcen Thornton, head of thc Departrrierit of Physiotherapy, Liverpool University, and Dr Cecily Partridge.
PhysiotherapyJune 1999/vol85/no 6
326
(Mayou, 1991; Mayou and Sharpe, 1997; Peters et al, 1998).
On the basis of their HAD scores, 68% of our patients were depressed. The issue of whether depression is primary or secondary to perceived disability in persistent, unexplained physical symptoms remains open to debate (Simon et al, 1996; Stanley et al, 1999). In the present study, the minority of patients identified as depressed by their GPs were significantly less likely than the remainder to have been referred to physiotherapy. This finding fits the prevailing medical view of somatisation that depression is primary (Wright, 1990; Weich et al, 1995) and , where i t is detected, recourse to psychotropic drugs or cognitive therapy (Speckens et al, 1995) is more appropriate than referral to physiotherapy. However, the corollary of this finding almost certainly carries wider implications: failure by GPs to detect depression led to almost half of these patients being referred to physiotherapy.
Unlike persistent somatisation, episodic depression with or without somatic symptoms is commonplace in primary care, with an overall prevalence in general practice attenders of between 30% and 40% (Freeling f t al, 1985; Paykel and Priest, 1992). Physical symptoms are central to patients’ experience of depression (Wright, 1990) and musculoskeletal complaints among the most f requent (Katon et at, 1982). Moreover, depression is less likely to be detected by GPs when the presenting symptoms are physical rather than emotional (Weich et al, 1995). Our findings in persistent somatising patients lead us to conclude that a larger group of primary care patients with depression is almost certainly being referred to and treated by NHS physiotherapists: those with musculoskeletal symptoms arising from somatisation of an unrecognised episode of depression.
While aerobic exercise training has been shown to benefit patients with chronic fatigue syndrome (Fulcher and White, 1997) and fibromyalgia (McCain et al, 1998), there is no evidence that conventional physio- therapy is effective for patients with musculoskeletal symptoms arising from the somatisation of mental illness. Indeed, a key lesson to be drawn from our experience of persistent somatisation is that physical therapy may do patients more harm than good. Embarking on physical treatment carries a number of risks, including reinforcement of inappropriate explanatory
models, legitimisation of somatic symptoms, and delayed access to more appropriate care. As our case histories illustrate, despite a wide range of interventions including physiotherapy, patients in the present study typically remained both symptomatic and dissatisfied with their care (Salmon et al,
At present, patients with musculoskeletal symptoms due to somatisation of mental illness represent an unquantifiable element in the demand for physiotherapy services from primary care. There is evidence to suggest that it may prove to be a significant element. High levels of health care utilisation by persistent somatising patients previously reported (Smith et al , 1986; Smith, 1994; Speckens et al, 1996) were confirmed by the present study. To this must be added any demand for physiotherapy arising from the much more prevalent musculoskeletal somatisation of episodes of depression presenting to, but unrecognised by, GPs.
For physiotherapy services, an obvious solution might appear to be to screen the mental state of referred patients with an instrument such as the HAD scale (Wilkinson and Barczak, 1988) o r the Distress Risk Assessment Method (Main et al, 1992). However, this approach would almost certainly not be specific enough; it would generate false positives by identifying those with clear-cut physical pathology who were also depressed. One aim of the present paper is increase awareness by physiother- apists of somatisation among primary care patients, alerting them to signs of mental illness and the need to return such patients to GPs for reassessment and management which is more appropriate. However, we recognise that this option, too, carries disadvantages: patients may construe it as rejection of their problem (Salmon et al, 1999); and GPs may feel challenged by re-referral based on physiotherapists’ assessment of patients’ psychological problems.
Thus, over and above any harm to patients, a clear implication of inappropriate referrals of this kind is that, unrecognised, they generate unproductive work, while their detection risks damaging the working relationship between GPs and physiother- apists. One approach to this dilemma would be for the professions to define, locally, appropriate demand for physiotherapy from general practice. This might take the form of a protocol which lists the indications for
1999).
PhysiotherapyJune 1999/vol85/no 6
Prof essiona I articles
referral a n d , as important , criteria for returning patients to their GP. By enabling issues to be considered outwith the care of individual patients, this might be seen as a test of the maturity of working relationships between the professions (Lee et al, 1990).
However, our experience of primary care teams suggests that agreement on criteria is not enough; the protocol needs also to define, explicitly, the process of returning patients to the care of thc GP. For example, how a r e the findings which suggest somatisation to be conveyed to the GP? And
how is the change in management to be explained to patients? Such questions are best resolved between the professions locally, and adherence to the protocol audited over time. Collaboration of this kind should not only limit inappropriate demand but also promote the sharing of skills, the convergence of explanatory models, and rapid redirection of somatising patients to more appropriate care (Goldberg et al, 1989; Speckens et al, 1995; M ~ Y O L I and Sharp, 1997).
Goldberg, I), Gask, L and O’Dowd, T (1989). ‘ ‘ I ’ l i c ~ t r c x t i i i c i i t 01’ sortlilt isai ion: Tcacliiiig 1 1 1 ~ ski 1 1 s ( ) I ’ r c.a t t r i I 1 I I t i ( ) n ’ , , J oltmwcl 01’ /<syh,o.wrn a/ i c / ~ ‘ e s m ~ ( h, 33, (iX!)-liS5.
Hackett, G, Hudson, M, Wylie, J et aZ(1987). Iiiiitiori ol 11ic. c~f’l ic;q and ac.cc:ptiildi(y l o
iysiotlicr;il)ist working in a health i\hdi,al,/oit I r i d , 294, 2 4-2 6.
Hackett, G, Bundred, P, Hutton, J, O’Brien, J and Stanley, I M (1993). ‘Mari:igcmerit ol’joint antl rol i tiasiic‘ iii,jiii-irs iri thrcc grnr r
(;an gc.ncrii1 prictitioncrs improve their ow
46,107-1 1 0 .
Katon, W, Kleinman, A and Rosen, G (1982). ‘1)c:pressioii antl soniali/ation: A review. Part 1 ’, Anieticcrtt. / / iwrtuL r?/ Mr&:zrtt, 72, 127-135.
Lee, J, Yorke, R A, Membrey, T and May, R (1990). ‘Rcliitionships hctwccn (;Ps and cliai.tei.cti physiothrrapi workiiig party’, l<o)..al (hllcgc of‘ (knc.ra1 I’ractitioncrs ;tiid ‘l’lir (:hartcrcd Socirty of‘ l’liysiotlic.rapy, 1 , o r i d o r i .
Main, C J, Wood, P L R, Hollis, S, Spanswick, C C and Waddell, G (1992). ‘The distress risk
I isk 01’ poor oiitcoiri
Mayou, K ( I 991). ‘Medically rrnc:xplained pliysic;il syiriptotns: 110 not over-iiivestigatc’, W l r ’ / r s / i /\/l~tlic nl, Joitmnl, 303, 534- Mayou, Rand Sharpe, M (1997). ‘Treating rncdically iiricxpl;iiiicd physical syiiipoins’ (cdi1ori:iI) /:ri/ish / l / l r d i ~ ~ ~ ~ , / / i ? ~ ~ ~ r i l , 315, 56 1-562.
McCain, G, Bell, I), Mai, F and Halliday, P (1998). ‘A coritrolletl stiidy of the ellects of a
McCormick, A, Fleming, D and Charlton, J ( 1995). M o d d i t y S&distic; /iom (;mr.?r~l PracLice hiiurtli i a r r / , i o l l a l .s/,~.~rly, 1991-IY92, Office 0 1 1’opul;rtiori (krisuses and Slatistics, EIMSC).
Physiotherapyjune 1999/vol85/no 6
328
O’Cathain, A, Froggett, M and Taylor, M (1995). ‘(kncral practice basctl physiotherapy: Its use
t on referrals to hospital ortliopaedics matology outpaticnt departirients’,
Ilrilish , Jou,rnccl or Gunural Practice, 45, 35 2-35 4.
O’Dowd, ‘r C (1998). ‘Five years of lieartsink patients in gmera1 practice’, fj /own al, 297, 5 28-5 30.
Palastanga, N (1995). ‘Manpower plaririing and tlie ph ysio t h crapy prol‘ession ’ , l’/zys%otheru@y, 8 1 , 7,
Partridge, C (1976). ‘I’lanning for physiotherapy in tlie corrirriii n i ty ’ , I’h,yhytiothrrcxpy, 62, 8 , 268.
Partridge, C and Warren, M (1977). f’/iysiothrrupy in t h ~ (,“ommun,ify, Heal th Services Research Unit, University of Kent, Canterbury.
Paykel, E S and Priest, R G (1992). ‘Rccognitiori and management of depression iri general practice’, Bt-itzsh Me~i( ; /~ l , / (~ / i~r t ,u l , 305, 1 198-1202.
Peters, S, Stanley, I M, Rose, M J and Salmon, P (1998). ‘The Intcraction of lay and medical rriodcls in patients’ accounts of mcdically uriexplained physical symptoms’, Social Sciurice
Robert, G and Stevens, A (1997). ‘Should GPs refer patierits directly to physical therapists?’ British Jourrinl o/ Gpnercrl I’ruclioe, 47, 3 14-3 18.
Salmon, P, Peters, S and Stanley, I (1999). ‘Patients’ perceptio somatisation disord British Medicccl,Jo,ii rri
Shorter, E (1992). from J’cmzlysis to f i l i p ~ e . A hislorj q/p~ycychosorncctic i l h s s , Free Press, New York.
Smith, G (1994). ‘The course of’ sornatization and its ef‘fects on the litilisatiori of health care reso urws ’ , I’.sychosomaticc, 35, 2 6 3-2 6 7.
Smith, G, Monson, R and Ray, D (1986). ‘Patients with multiple unexplained symptoms: Their characteristics, furictioiial hcaltli and hcalth care utilisatiori’, Archi7m o/Ziztern,nl M 69-72.
Speckens, A, Van Hemert, A, Spinhoven, P et a1 (1995). ‘Cogriitivc: beliavioriral therapy for rrietlically rrncxplainctl syniptorris: A raiidomisetl
-3117.
c:ontrolled trial’, fl?.itish MPrl%crcl,/oui-irnI, 31 1, 1328-32.
Speckens, A, Van Hemert, A, Bolk, J et aZ(1996). ‘Unexplained physical symptoms: outcome, irtilization of medical care arid associated factors’, P.sychological Medicine, 26, 745-752.
Stanley, I, Peters, S, Rose, M and Salmon, P (1999). ‘I’ersistent unexplained physical symptoms: (:hallenging the expha to ry ualidity o f somatization in primary care’, Briti.tk,/out-rial qf
Troup, J D G and Videman, Y (1989). ‘Inactivity and aetiopathogenesis of‘ rnusculoskelctal disorders’, CLi,iical f3iomtxhanic.,, 4, 173- 178
Upadhyaya, A and Stanley, I (1993). ‘Hospital anxiety depression s~a lc ’ , Brili~h Journal 1fGertrrni Practicp, 43, 349-350.
Upadhyaya, A and Stanley, I (1995). ‘Detection of depression in primary care: (:omparison of two selEadministercd scales’, Intrrricctionnl,~ourrialo/ (hiutrar Psychiatry, 12, I , 35-37.
Weich, S, Lewis, G, Donmall, R and Mann, A (1995). ‘Somatic presentation of psychiatric morbidity in general practice’, British ,/ourrial OJ (;enera1 Practice, 45, 143-1 47.
Wilkinson, M and Barczak, P (1988). ‘Psychiatric screening in gcrieral practice: Comparison of the gencr.al health questionnaire and the hospital anxiety arid depression scale’,,/ournal oJ’the Royal Collegu of Gwierul I’raclice, 38, 3 1 1-31 3 .
Worsfold, C, Langidge, J, Spalding, A and Mullee M (1996). ‘Comparison between primary care physiotherapy cducatiori/advicc clinics arid traditiorial hospital based physiotherapy treatment: A raxidomiscd trial’, Nriti,sh,/ournd q / Grneral Practice, 43, 61-64
Wright, A (1990). ‘A study of t.he presentation of somatic symptoms in general practice by patients with psychiatric ctisturbancc’, I9ritish,/ourn,cil OJ (:enural I’ructire, 40, 459-46:3.
Zigmond, A and Snaith, R (1983). ‘The Hospital Anxiety and Depressiori scale’, Acta f’,~yrchialm‘ccr Scnrirlini~viccc, 67, 36 1-370.
1 f’racticc: in press.
PhysiotherapyJunr lSSS/vol Xli/no 6